
Acute Myocardial Infarction due to Coronary Artery ... · Acute Myocardial Infarction due to...
5
82 The Permanente Journal/ Summer 2011/ Volume 15 No. 3 CASE STUDY Acute Myocardial Infarction due to Coronary Artery Embolism in a Patient with a Tissue AorticValve Replacement Joel T Levis, MD, PhD, FACEP, FAAEM Geoffrey Schultz, MD Philip C Lee, MD, FACC Case Report A 50-year-old man who underwent a tissue aortic valve replacement (AVR) (23 mm Magna pericardial tissue heart valve) four years earlier for bicuspid aortic valve and aortic stenosis, presented to the Emergency Department (ED) complaining of sudden onset chest discomfort with radiation to his left arm. The dis- comfort began 20 minutes before arrival in the ED while he was lifting heavy weights. Medical history was notable for a coronary angiogram immediately prior to his AVR without significant coronary artery disease, Joel T Levis, MD, PhD, FACEP, FAAEM, is a Senior Emergency Physician at the Santa Clara Medical Center in CA. He is a Clinical Instructor of Emergency Medicine (Surgery) at Stanford University and the Medical Director for the Foothill College Paramedic Program. E-mail: [email protected]. Geoffrey Schultz, MD, is a First-Year Resident in the Stanford/Kaiser Emergency Medicine Residency Program in Stanford, CA. E-mail: [email protected]. Philip C Lee, MD, FACC, is a Senior Cardiologist and Director of the EKG/Treadmill/Pacemaker Laboratory at the Santa Clara Medical Center in CA. E-mail: [email protected]. Abstract Acute occlusive embolism to the coronary arteries resulting in acute myocardial infarction (AMI) is an uncommon occurrence. Although cases of patients with mechanical prosthetic heart valves resulting in this phenomenon have been re- ported in the setting of inadequate anticoagulation, reported cases resulting years after tissue aortic valve replacement (AVR) are rare. We report the case of a 50-year-old man who underwent a tissue AVR four years earlier and presented to the Emergency Department (ED) with an ST-segment elevation myocardial infarction. ED door-to- balloon time was delayed (at 115 minutes) because of pre-existing left bundle branch block on elec- trocardiogram. Emergent coronary angiography demonstrated com- plete occlusion of the left anterior descending coronary artery by a coronary embolus.The patient was successfully treated with percuta- neous transluminal coronary an- gioplasty and aspiration thrombec- tomy, and subsequently underwent a transesophageal echocardiogram demonstrating thrombus on the tissue aortic valve prosthesis. This case demonstrates that coronary embolism resulting in AMI, while rare, can occur in patients years after tissue AVR surgery. Figure 1. 12-lead electrocardiogram (ECG) from a 50-year-old man presenting to the Emergency Department with chest discomfort (panel A), compared with a previous ECG obtained from the same patient four years earlier (panel B).
-
Upload
nguyenminh -
Category
Documents
-
view
230 -
download
0
Transcript of Acute Myocardial Infarction due to Coronary Artery ... · Acute Myocardial Infarction due to...
82 The Permanente Journal/ Summer 2011/ Volume 15 No. 3
CASE STUDY
AcuteMyocardialInfarctionduetoCoronaryArteryEmbolisminaPatientwithaTissueAorticValveReplacementJoel T Levis, MD, PhD, FACEP, FAAEM Geoffrey Schultz, MDPhilip C Lee, MD, FACC Case Report
A 50-year-old man who underwent a tissue aortic valve replacement (AVR) (23 mm Magna pericardial tissue heart valve) four years earlier for bicuspid aortic valve and aortic stenosis, presented to the Emergency Department (ED) complaining of
sudden onset chest discomfort with radiation to his left arm. The dis-comfort began 20 minutes before arrival in the ED while he was lifting heavy weights. Medical history was notable for a coronary angiogram immediately prior to his AVR without significant coronary artery disease,
Joel T Levis, MD, PhD, FACEP, FAAEM, is a Senior Emergency Physician at the Santa Clara Medical Center in CA. He is a Clinical Instructor of Emergency Medicine (Surgery) at Stanford University and the Medical Director for the Foothill College Paramedic Program. E-mail: [email protected]. Geoffrey Schultz, MD, is a First-Year Resident in the Stanford/Kaiser Emergency Medicine Residency Program in Stanford, CA. E-mail: [email protected]. Philip C Lee, MD, FACC, is a Senior Cardiologist and Director of the EKG/Treadmill/Pacemaker Laboratory at the Santa Clara Medical Center in CA. E-mail: [email protected].
AbstractAcuteocclusiveembolismtothe
coronaryarteriesresultinginacutemyocardial infarction (AMI) isanuncommonoccurrence.Althoughcasesofpatientswithmechanicalprostheticheartvalvesresultinginthisphenomenonhavebeen re-portedinthesettingofinadequateanticoagulation, reported casesresulting years after tissueaorticvalvereplacement(AVR)arerare.Wereportthecaseofa50-year-oldmanwhounderwentatissueAVRfour years earlier andpresentedto the Emergency Department(ED)withanST-segmentelevationmyocardialinfarction.EDdoor-to-balloontimewasdelayed(at115minutes)becauseofpre-existingleftbundlebranchblockonelec-trocardiogram.Emergentcoronaryangiographydemonstratedcom-pleteocclusionoftheleftanteriordescendingcoronaryarterybyacoronaryembolus.Thepatientwassuccessfullytreatedwithpercuta-neous transluminal coronaryan-gioplastyandaspirationthrombec-tomy,andsubsequentlyunderwentatransesophagealechocardiogramdemonstrating thrombus on thetissueaorticvalveprosthesis.Thiscasedemonstrates that coronaryembolismresultinginAMI,whilerare, canoccur inpatients yearsaftertissueAVRsurgery.
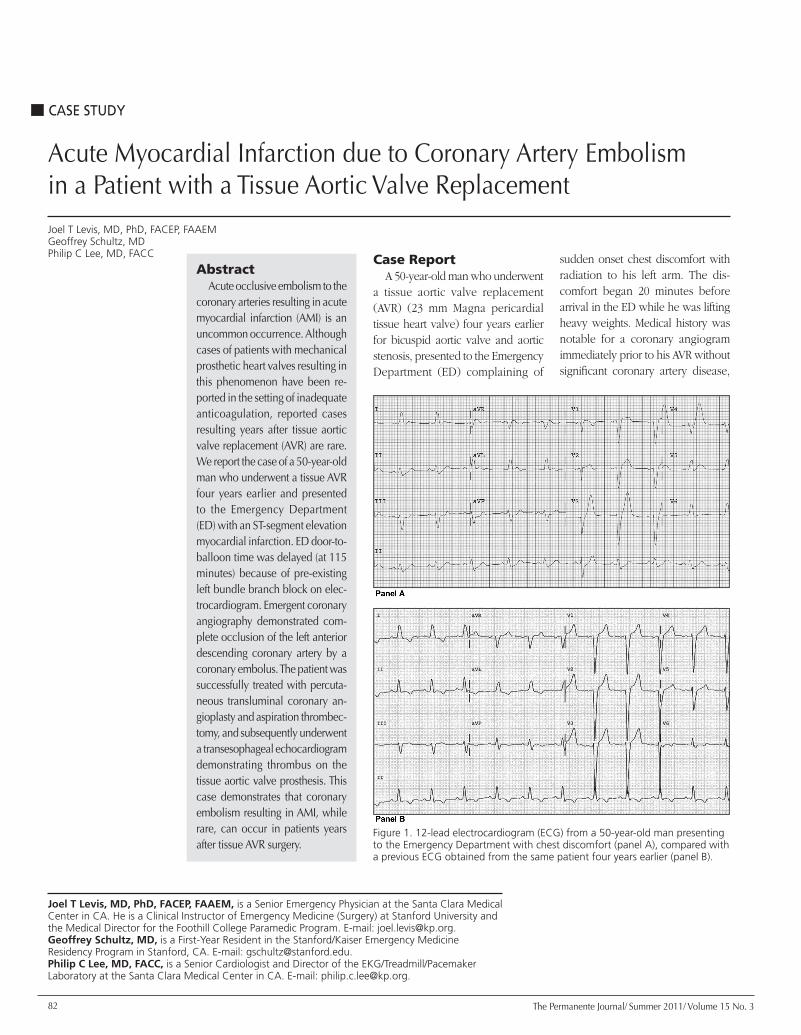
Figure 1. 12-lead electrocardiogram (ECG) from a 50-year-old man presenting to the Emergency Department with chest discomfort (panel A), compared with a previous ECG obtained from the same patient four years earlier (panel B).
83The Permanente Journal/ Summer 2011/ Volume 15 No. 3
CASE STUDYAcuteMyocardialInfarctionduetoCoronaryArteryEmbolisminaPatientwithaTissueAorticValveReplacement
paroxysmal atrial fibrillation prior to surgery that was treated with a MAZE procedure at the time of AVR (without recurrence of atrial fibrillation), hypertension, and gout. His medications included losartan and allopurinol (but not aspirin for unclear reasons).
The patient was a well-devel-oped, middle-aged man who ap-peared to be in no acute distress. Vital signs demonstrated an oral temperature of 98.6°F (37°C), pulse 60 beats/minute, blood pressure 115/72 mm Hg, respirations 20 breaths/minute, with an oxygen sat-uration of 100% on room air. Physi-cal examination, including the heart and lungs, was entirely normal. A 12-lead electrocardiogram (ECG) was obtained in the ED (Figure 1, panel A), which demonstrated a normal sinus rhythm, left bundle branch block (LBBB) (present on previous ECG, figure 1, panel B) with new ST-segment concordance with the QRS waves and slightly more prominent ST-segment elevations in leads aVL and V5. The patient was initially felt not to meet criteria for an ST-segment elevation myocardial infarction (STEMI). Laboratory tests were significant for a troponin I of 0.45 ng/mL (normal range 0.00-0.09 ng/mL). Treatment for presumed acute coronary syndrome was initi-ated with oral aspirin, clopidogrel, and sublingual nitroglycerin. The patient was started on intrave-nous unfractionated heparin and eptifibatide and considered for expeditious cardiac catheterization. Approximately 90 minutes follow-ing ED arrival, the patient went into cardiac arrest with the monitor demonstrating ventricular fibrilla-tion. Cardiopulmonary resuscita-tion immediately commenced, and he was successfully defibrillated to normal sinus rhythm with one biphasic shock of 200 joules with
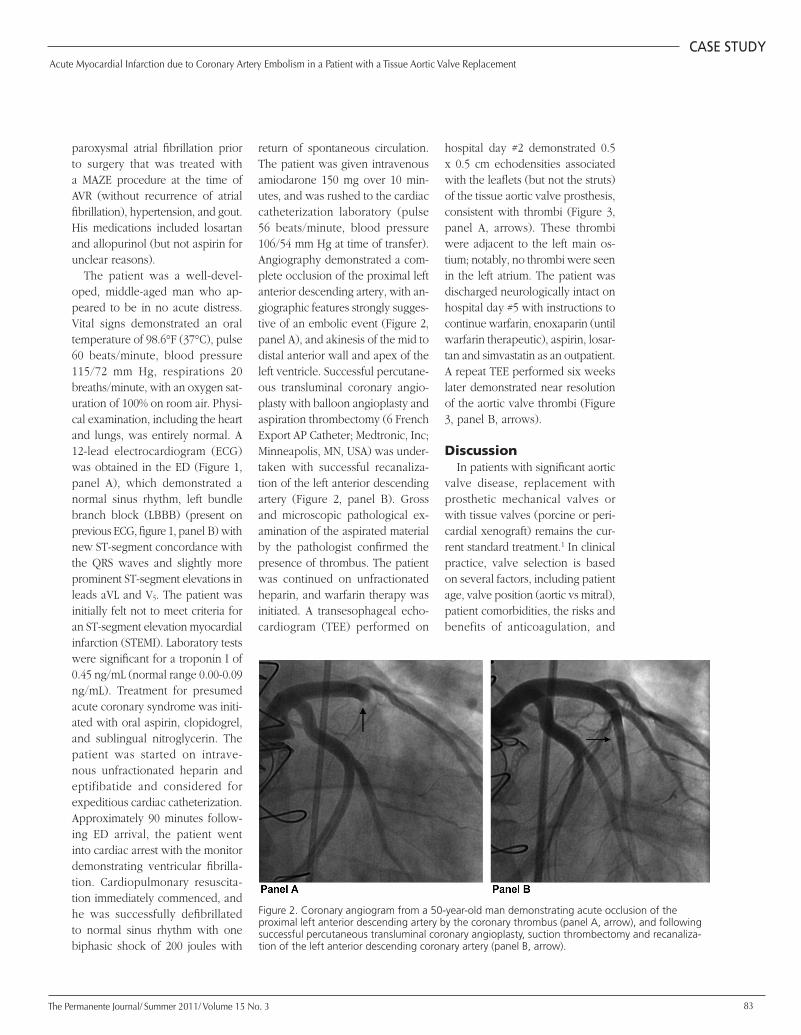
return of spontaneous circulation. The patient was given intravenous amiodarone 150 mg over 10 min-utes, and was rushed to the cardiac catheterization laboratory (pulse 56 beats/minute, blood pressure 106/54 mm Hg at time of transfer). Angiography demonstrated a com-plete occlusion of the proximal left anterior descending artery, with an-giographic features strongly sugges-tive of an embolic event (Figure 2, panel A), and akinesis of the mid to distal anterior wall and apex of the left ventricle. Successful percutane-ous transluminal coronary angio-plasty with balloon angioplasty and aspiration thrombectomy (6 French Export AP Catheter; Medtronic, Inc; Minneapolis, MN, USA) was under-taken with successful recanaliza-tion of the left anterior descending artery (Figure 2, panel B). Gross and microscopic pathological ex-amination of the aspirated material by the pathologist confirmed the presence of thrombus. The patient was continued on unfractionated heparin, and warfarin therapy was initiated. A transesophageal echo-cardiogram (TEE) performed on
hospital day #2 demonstrated 0.5 x 0.5 cm echodensities associated with the leaflets (but not the struts) of the tissue aortic valve prosthesis, consistent with thrombi (Figure 3, panel A, arrows). These thrombi were adjacent to the left main os-tium; notably, no thrombi were seen in the left atrium. The patient was discharged neurologically intact on hospital day #5 with instructions to continue warfarin, enoxaparin (until warfarin therapeutic), aspirin, losar-tan and simvastatin as an outpatient. A repeat TEE performed six weeks later demonstrated near resolution of the aortic valve thrombi (Figure 3, panel B, arrows).
DiscussionIn patients with significant aortic
valve disease, replacement with prosthetic mechanical valves or with tissue valves (porcine or peri-cardial xenograft) remains the cur-rent standard treatment.1 In clinical practice, valve selection is based on several factors, including patient age, valve position (aortic vs mitral), patient comorbidities, the risks and benefits of anticoagulation, and
Figure 2. Coronary angiogram from a 50-year-old man demonstrating acute occlusion of the proximal left anterior descending artery by the coronary thrombus (panel A, arrow), and following successful percutaneous transluminal coronary angioplasty, suction thrombectomy and recanaliza-tion of the left anterior descending coronary artery (panel B, arrow).

84 The Permanente Journal/ Summer 2011/ Volume 15 No. 3
CASE STUDYAcuteMyocardialInfarctionduetoCoronaryArteryEmbolisminaPatientwithaTissueAorticValveReplacement
patient preferences.1,2 Mechanical prosthetic valves are thrombogenic, and patients who receive them require long-term anticoagulation with warfarin (with its associated increased risk of bleeding).3 Bio-prosthetic (tissue) valves are felt to be less thrombogenic and usually do not require patients to continue chronic anticoagulation therapy; however, structural degeneration of these valves limits their durability.3,4
Coronary artery embolism is an uncommon cause of acute myo-cardial infarction (AMI).5 Several recent case reports cite prosthetic
mechanical heart valves (in the aortic or mitral posi-tions) in the setting of sub-therapeutic anticoagulation as the cause of the coronary artery emboli and AMI.6-9 Other causes of coronary embolism resulting in AMI include infective endocardi-tis,10,11 atrial thrombus in the setting of atrial fibrillation,12 atrial myxomas,13 embolism of cotton pledgets following insertion of porcine valve bioprosthesis,14 calcific em-boli from calcific aortic ste-
nosis,15 and even emboli originating from biologic glues used in surgical repair of acute aortic dissection.16
Chronic tissue AVR thrombosis, while rare, has been reported.17-19 However, to our knowledge, such thrombotic involvement of a chronic tissue valve resulting in coronary embolism and AMI has yet to be reported in the literature. In our case the coronary embolism was found to be thrombus by angiographic and pathological examination, demon-strated to be related to a tissue AVR (by TEE), resolved after treatment with anticoagulation, and not as-sociated with clinical or pathologic findings consistent with aortic valve endocarditis.
The prevalence of coronary artery embolism resulting in AMI is unknown, but is believed to be relatively uncommon.20 In one study, 55 out of 419 patients (13%) with autopsy-studied infarcts showed evidence of coronary artery em-bolism.21 It has been observed that most emboli involve the left coronary system, which could be because of the preferential flow into the artery related to coronary flow volume characteristics and aortic valve morphology.22 In patients with a presumed embolic coronary event, TEE has been recommended to identify any potential endocardial source of emboli.23 Percutaneous transluminal coronary angioplasty
and stenting have been successfully used to treat patients with AMI result-ing from coronary artery embolism.24 Conversely, catheter aspiration embolectomy (as used in this case), has been successfully employed by several authors to aspirate thrombus from a native coronary artery.8,25-28 In our case, following successful aspiration thrombectomy of the clot, the patient was continued on unfractionated heparin (as a bridge to anticoagulation) and started on warfarin to decrease the risk of further thromboembolic events.
Our patient presented with STE-MI in the setting of a known LBBB. The presence of a preexisting LBBB on the ECG may conceal the changes of AMI, and delay both its recognition and treatment.29 The Sgarbossa criteria are the most validated ECG criteria for diag-nosing STEMI in the presence of LBBB.29,30 These ECG criteria include: 1) ST-segment elevation >1 mm concordant with QRS complexes; 2) ST-segment depression >1 mm in lead V1, V2; and 3) ST-segment elevation >5 mm discordant with QRS complex. The application of the Sgarbossa criteria has resulted in low sensitivities and high speci-ficities for identifying patients with known LBBB and STEMI.29-31 The
Figure 3. Transesophageal echocardiogram from 50-year-old man demonstrating echodensities associated with the aortic valve leaflets consistent with thrombus (panel A, arrows), compared with the same view following six weeks of warfarin anticoagulation, now demonstrating near resolution of the thrombi (panel B, arrows).
In patients with a
presumed embolic coronary
event, TEE has been
recommended to identify
any potential endocardial
source of emboli.23
85The Permanente Journal/ Summer 2011/ Volume 15 No. 3
CASE STUDYAcuteMyocardialInfarctionduetoCoronaryArteryEmbolisminaPatientwithaTissueAorticValveReplacement
low sensitivity limits their utility in clinical practice, as diagnostic tests for AMI need to be highly sensitive to detect most cases.29
Our patient was not taking aspi-rin or any antiplatelet agent at the time of his STEMI. The 2006 Ameri-can Heart Association/American College of Cardiology Guidelines for Management of Patients with Valvular Heart Disease recommend long-term aspirin for all recipients of bioprosthetic heart valves (Class I, level of evidence C).32 The fact that our patient was not using an antiplatelet agent may have played a role in development of the AVR thrombus and subsequent coronary artery embolism.
We report the case of a man pre-senting with a STEMI resulting from acute coronary embolism in the set-ting of a tissue AVR performed four years earlier. The thrombus was suc-cessfully aspirated during coronary angiography, with the source of the coronary thrombus arising from the tissue AVR leaflets, as visualized by TEE. Following warfarin antico-agulation for six weeks, repeat TEE demonstrated near resolution of the AVR thrombi. Our case demon-strates that although rare, embolism from tissue prosthetic valves to the coronary artery can occur, result-ing in life-threatening AMI. In such cases, emergent coronary angiogra-phy (with aspiration thrombectomy, percutaneous transluminal coronary angioplasty, and/or coronary artery stenting), TEE, and treatment with anticoagulation therapy are effective management strategies. v
Disclosure StatementThe author(s) have no conflicts of
interest to disclose.
References 1. Khan SS, Trento A, DeRobertis M, et
al. Twenty-year comparison of tissue and mechanical valve replacement.
J Thorac Cardiovasc Surg 2001 Aug;122(2):257-69.
2. Khan S, Gray R. Selection of a valve prosthesis in the elderly patient. In: Emery RW, Arom KV, editors. The aortic valve. Philadelphia, PA: Hanley and Belfus; 1991. p 149-60.
3. Hammermeister KE, Sethi GK, Hen-derson WG, Oprian C, Kim T, Rahim-toola S. A comparison of outcomes in men 11 years after heart-valve replacement with a mechanical valve or bioprosthesis. Veterans Affairs Cooperative Study on Valvular Heart Disease. N Engl J Med 1993 May 6;328(18):1289-96.
4. Bloomfield P, Wheatley DJ, Prescott RJ, Miller HC. Twelve-year com-parison of a Bjork-Shiley mechanical heart valve with porcine biopros-thesis. N Engl J Med 1991 Feb 28;324(9):573-9.
5. Cheng TO. Coronary embolism. Int J Cardiol 2009 Jul 24;136(1):1-3.
6. Sial JA, Ferman MT, Saghir T, Rasool SI. Coronary embolism causing acute myocardial infarction in a patient with mitral valve prosthesis: successful management with angioplasty. J Pak Med Assoc 2009 Jun;59(6):409-11.
7. Nakazone MA, Tavares BG, Machado MN, Maia LN. Acute myo-cardial infarction due to coronary artery embolism in a patient with mechanical aortic valve prosthesis. Case Report Med 2010:751857. Epub 2010 Jun 14.
8. Ranasinghe I, Yiannikas J, Brieger D. Letter to the Editor: Acute left main occlusion secondary to embolism from an aortic valve prosthesis: Suc-cessful treatment with embolectomy and percutaneous coronary interven-tion. Int J Cardiol 2009;doi:10.1016/j.ijcard.2009.05.049 Jun 14. In Press. [Epub ahead of print].
9. Karabinos IK, Kranidis A, Spanos VN. Acute myocardial infarction presum-ably embolic, in a patient with a mechanical aortic valve: a rare cause of non-atherosclerotic coronary artery occlusion. Hospital Chronicles 2010;5(1):1-5.
10. Glazier JJ, McGinnity JG, Spears JR. Coronary embolism complicating aortic valve endocarditis: treatment with placement of an intra-coronary stent. Clin Cardiol 1997 Oct;20(10):885-8.
11. Roxas CJ, Weekes AJ. Acute
myocardial infarction caused by coronary embolism from infective endocarditis. J Emerg Med 2011 May;40(5):509-14.
12. Noto N, Osaka T, Yamanaka O, Kobayashi S, Ozaki H, Kanoh T. [A case of acute myocardial infarction due to coronary embolism from left atrial thrombus with atrial fibrilla-tion]. [Article in Japanese]. Kokyu To Junkan 1990 May;38(5):483-7.
13. Taşdemir K, Andaç MH, Ceyran H, Yasim A. Myxomas causing coronary emboli resulting in acute myocardial infarction. Asian Cardiovasc Thorac Ann 1999;7(2):150-2.
14. Lifschultz BD, Donoghue ER, Leestma JE, Boade WA. Emboliza-tion of cotton pledgets following insertion of porcine cardiac valve bioprosthesis. J Forensic Sci 1987 Nov;32(6):1796-800.
15. Mansur AJ, de Miranda RC, Grinberg M, Bellotti G, Pileggi F. Calcific aortic stenosis presenting as acute myo-cardial infarction. J Cardiovasc Surg (Torino) 1990 May;31(3):310-2.
16. Mahmood Z, Cook DS, Luckraz H, O’Keefe P. Fatal right ventricular in-farction caused by Bioglue coronary embolism. J Thorac Cardiovasc Surg 2004 Nov;128(5):770-1.
17. Logeais Y, Langanay T, Leguerrier A, Rioux C, Chaperon J Coutté MB. Aortic Carpenter-Edwards supraanu-lar porcine biprosthesis: a 12-year experience. Ann Thorac Surg 1999 Aug;68(2):421-5.
18. Selleslagh P, Hamerlijnck R, De Sutter J. A rare case of aortic bioproth-esis thrombosis. Acta Cardiol 2010 Apr;65(2):253-4.
19. Jamieson WRE, Lewis CTP, Sakwa MP, et al. St Jude Epic porcine bio-prosthesis: Results of the regulatory evaluation. J Thorac Cardiovasc Surg 2011 Jun;141(6):1449-54.e2.
20. Camaro C, Aengevaeren WR. Acute myocardial infarction due to coronary artery embolism in a patient with atrial fibrillation. Neth Heart J 2009 Aug;17(7-8):297-9.
21. Prizel KR, Hutchins GM, Bulkley BH. Coronary artery embolism and myo-cardial infarction. Ann Intern Med 1978;88:155-61.
22. Prizel KR, Hutchins GM, Bulkley BH. Coronary artery embolism and myo-cardial infarction. Ann Intern Med 1978 Feb;88(2):155-61.
86 The Permanente Journal/ Summer 2011/ Volume 15 No. 3
CASE STUDYAcuteMyocardialInfarctionduetoCoronaryArteryEmbolisminaPatientwithaTissueAorticValveReplacement
23. Meier B. Catheter-based closure of the patent foramen ovale. Circula-tion 2009 Nov;120(18):1837-41.
24. Hernández F, Pombo M, Dalmau R, et al. Acute coronary embolism: angio-graphic diagnosis and treatment with primary angioplasty. Catheter Cardio-vasc Interv 2002 Apr;55(4):491-4.
25. Kiernan TJ, Flynn AM, Kearney P. Coronary embolism causing myocar-dial infarction in a patient with me-chanical aortic valve prosthesis. Int J Cardiol 2006 Sep 20;112(2):E14-6.
26. Hung WC, Wu CJ, Chen WJ, Yang CH, Chang JP. Transradial intracoro-nary catheter-aspiration embolec-tomy: for acute coronary embolism after mitral valve replacement. Tex Heart Inst J 2003;30(4):316-8.
27. Belli G, Pezzano A, De Biase AM, et al. Adjunctive thrombus aspira-tion and mechanical protection from distal embolization in primary percutaneous intervention for acute myocardial infarction. Catheter Car-diovasc Interv 2000 Jul;50(3):362-70.
28. Beran G, Lang I, Schreiber W, et al. Intracoronary thrombectomy with
the X-sizer catheter system improves epicardial flow and accelerates ST-segment resolution in patients with acute coronary syndromes: a prospective, randomized, con-trolled study. Circulation 2002 May 21;105(20):2355-60.
29. Sgarbossa EB, Pinski SL, Barbagelata A, et al. Electrocardiographic diag-nosis of evolving acute myocardial infarction in the presence of left bundle-branch block. GUSTO-1 (Global Utilization of Streptokinase and tissue Plasminogen Activator for Occluded Coronary Arteries) Investigators. N Engl J Med 1996 Feb 22;334(8):481-7. Erratum in: N Engl J Med 1996 Apr 4;334(14):931.
30. Jain S, Ting HT, Bell M, et al. Utility of left bundle branch block as a diag-nostic criterion for acute myocardial infarction. Am J Cardiol 2011 Apr 15;107(8):1111-6.
31. Tabas JA, Rodriquez RM, Seligman HK, Golschlager NF. Electrocardio-graphic criteria for detecting acute myocardial infarction in patients with left bundle branch block: a meta-
analysis. Ann Emerg Med 2008 Oct;52(4):329-36.e1.
32. American College of Cardiology; American Heart Association Task Force on Practice Guidelines (Writing Committee to revise the 1998 guide-lines for the management of patients with valvular heart disease); Society of Cardiovascular Anesthesiologists, Bonow RO, Carabello BA, Chatterjee K, et al. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (writ-ing Committee to Revise the 1998 guidelines for the management of patients with valvular heart disease) developed in collaboration with the Society of Cardiovascular Anesthe-siologists endorsed by the Society for Cardiovascular Angiography and Interventions and the Society of Thoracic Surgeons. J Am Coll Cardiol 2006 Aug 1;48(3):e1-148. Erratum in J Am Coll Cardiol 2007 Mar 6;49(9):1014.
The Hot OrganInthemidstof[thelungs]isseatedahotorgan,theheart,
whichistheoriginoflifeandrespiration.Itimpartstothelungsthedesireofdrawingincoldair,
foritraisesaheatinthem;butitistheheartwhichattracts.If,therefore,theheartsufferprimarily,deathisnotfaroff.
— OnPneumonia, Aretaeus, the Cappadocian, 2nd Century AD Greek physician


















