A n t i p l a t e l e t T h e r a p y

of 15
-
Upload
fernando-davalos-manzanares -
Category
Documents
-
view
219 -
download
0
Transcript of A n t i p l a t e l e t T h e r a p y
-
8/7/2019 A n t i p l a t e l e t T h e r a p y
1/15
-
8/7/2019 A n t i p l a t e l e t T h e r a p y
2/15
acute episodes of care, but whose efficacy in pre-ventingfurther ischemic events continues well afterthe precipitating event has quiesced, thus blurringformal definitions of prevention.
Aspirin
Aspirin is the most widely used antiplatelet agent.After ingestion, it reaches peak plasma levels in 30minutes.9 At low doses, it acetylates plateletCOX-1, resulting in irreversible, near total inhibition
of TXA2 production.10 Given platelets inability tosynthesize new COX-1, aspirins antiplatelet effectlong outlasts its plasma clearance, requiringregeneration of the platelet pool for return ofplatelet function (7e10 days for full repletion).13,14
Several trials have investigated aspirin use inCHD prevention and meta-analyses help shapeour understanding of its benefits and risks.15,16 Inpatients with prior myocardial infarction (MI), theAntithrombotic Trialists (ATT) Collaboration founda 25% relative risk reduction in recurrent vascularevents (MI, stroke, vascular death) with aspirinuse.15 Overall mortality decreased one-sixth withantiplatelet therapy.15 Similar relative risk reduc-tions persist in broader populations, such asin those with a history of unstable angina (UA)
or stroke.15,16 Aspirin is clearly indicated insecondary prevention of CHD.
The effect of aspirin in primary preventionsettings, where absolute cardiovascular eventrates are an order of magnitude lower (w1 per
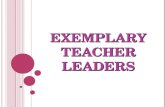
Fig. 1. Platelets are central mediators of atherothrombosis. (A) Inactive, they partition to the flow periphery,serving as efficient scouts of vascular integrity. On vascular disruption, as with acute plaque rupture or afterPCI, they tether and activate to reactive subendothelial components such as collagen and bound von WillebrandFactor (vWF). (B) They are further activated through a variety of signaling molecules such as thromboxane A2(TxA2), ADP, and thrombin through specialized receptors. (C) On activation, they release newly generated or pre-formed mediators into the thrombotic milieu that serve as autocrine and paracrine activators, amplifying theprocess. (D) In a final common step, glycoprotein (GP) IIb/IIIa receptors are activated, facilitating fibrinogenand vWF bridging and platelet aggregation. Antiplatelet agents act by inhibiting various steps in this complexprocess. (From Bhatt DL. Intensifying platelet inhibition e navigating between Scylla and Charybdis. N Engl JMed 2007;357:2079; with permission.)
Kolandaivelu & Bhatt72
-
8/7/2019 A n t i p l a t e l e t T h e r a p y
3/15
1000 patients versus w10e60 per 1000), is lessobvious.12,16 A recent analysis of data from95,000 participants from primary prevention trialsfound a 12% reduction in vascular events (abso-lute reduction from 0.57% to 0.51%), with an18% reduction in coronary events attributable
mostly to nonfatal MI.16 There was no mortalitybenefit and absolute major bleeding increasedfrom 0.07% to 0.10%.16
Balancing these competing risks of clotting andbleeding is essential for optimal antiplatelet use(Fig. 2A).8,9 As vascular risk increases, so doesthe absolute benefit of aspirin (see Fig. 2B).16
Moreover, benefit seems roughly proportional torisk.16 In contrast, bleeding risk is often assumedconstant or age dependent.11,12,15 Risk modelssuggest aspirin use is indicated in patients withcoronary event rates in excess of 0.6% andpossibly as high as 1.5% to 2% per year, whereasin those with annual risk less than 0.5%, bleedingrisk supersedes.10,11 Reality is far more complexbecause bleeding risks are not constant. Thesame factors that increase cardiovascular riskincrease propensity to bleed (Fig. 3A).16 Moreover,some individuals are at exceptional bleeding risk(eg, those with gastrointestinal complications,particularly the elderly; see Fig. 3B).9,12 Improvedrisk scores and paradigms are needed to helpproviders and patients make these difficult,
everyday treatment decisions.Choosing the right dose of antiplatelet therapy
can help maximize benefit and minimize risk, yetoptimal aspirin dose remains uncertain. At dosesof 30 to 50 mg, platelet TXA2 production iscompletely inhibited. However, there is a sugges-tion that doses less than 75 mg may be less effec-tive than doses greater than 75 mg.15 Becausesmall reductions in TXA2 inhibition yield largereductions in inhibitory effect, this lower limit mayin part reflect individual variability in pharmacoki-
netics or drug effect.
10
Although true biochemicalaspirin nonresponsiveness is now consideredrare, broader aspirin resistance can be attributedto several factors including variable pharmacoki-netics, increased platelet turnover, or drug-druginteractions.17 For example, enteric coatingssignificantly reduce absorption rate and bioavail-ability, and nonsteroidal antiinflammatory drugs(NSAIDs) directly compete for COX-1 binding,decreasing aspirins efficacy.9 That much of aspi-rins nonresponsiveness is lost in closely moni-tored settings indicates the important role of
patient adherence (discussed later).17Increasing dose can, in part, overcome antipla-
telet nonresponsiveness, yet there is an upperbound to efficacy and safety. Higher aspirin dosesresult in pleiotropic systemic effects through
broader COX-1 and less specific COX-2 inhibi-tion.9 Despite theoretic advantages in reducingvascular inflammation, higher dose aspirin (up to1500 mg) have not been found efficacious inCHD prevention, perhaps because of concurrentreductions in endothelial prostacyclin.4,9,15 More-
over, gastric prostaglandin suppression in combi-nation with platelet inhibition can increasebleeding risk.9,14 Given the aggregate findings,current recommendations are to use 162 to 325mg in acute settings, reducing to 75 to 162 mgfor longitudinal prevention in patients withsufficiently high risk of cardiovascular disease(>6%e10% over 10 years).18
Thienopyridine P2Y12 Inhibitors
Thienopyridines irreversibly block platelet P2Y12
receptors, inhibiting ADP-mediated activationfor a platelets lifespan.2,5 Ticlopidine (a first-generation agent) reduced vascular events andmortality in broad categories of patients.4
However, twice-daily dosing and its potential forsevere side effects (severe neutropenia and throm-botic thrombocytopenic purpura [TTP]) have led toits near-universal replacement with clopidogrel.2
ClopidogrelClopidogrel is intestinally absorbed as a prodrug,most of which is quickly degraded by plasma
esterases.17 The remainder is hepatically con-verted via sequential cytochrome P-450 (CYP)steps to a short-lived active metabolite.19 Depend-ing on loading dose administered (600 mg vs 300mg), platelet inhibition is achieved in 2 to 6 hoursin most patients. Higher loading doses were notconsistently more effective.20
CAPRIE investigated daily clopidogrel (75 mg)as an alternative to aspirin (325 mg) in high-riskpatients with manifest CHD, stroke, or symptom-atic peripheral artery disease (PAD) and found an
8.7% relative reduction in vascular events(Fig. 4A).21 Bleeding risk was unchanged. Thus,clopidogrel can be used safely for CHD preventionin aspirin-intolerant patients at sufficiently highrisk. Given the substantial cost differentialbetween aspirin (e$15 per year) and clopidogrel(e$1200 per year), universal application is not justi-fied, although as clopidogrel approaches genericavailability, this issue may be revisited.22
CURE showed that adding clopidogrel toaspirin therapy (dual antiplatelet therapy [DAPT])for up to 1 year reduced vascular events by
20% (11.4% to 9.3%) in patients presentingwith acute coronary syndromes (ACS), witheven greater benefits in those undergoing PCI(31% relative risk reduction; PCI-CURE).23,24
Although major bleeding increased with DAPT
Antiplatelet Therapy and Coronary Heart Disease 73
-
8/7/2019 A n t i p l a t e l e t T h e r a p y
4/15
Fig. 2. Balancing the risks of vascular events and major bleeding episodes is a central theme to antiplatelet use.(A) A plot of vascular and bleeding event rates observed in major primary prevention aspirin trials as a function ofuntreated vascular risk. Aspirin use is clearly indicated when vascular risks are greater than 2% per year (and aslow as 0.6% per year in some analyses). When vascular risk is less than 0.5% per year, bleeding risk supersedes. Inbetween these percentages, clinical uncertainty remains. (From Patrono C, Garcia Rodriguez LA, Landolfi R, et al.Low-dose aspirin for the prevention of atherothrombosis. N Engl J Med 2005;353:2380; with permission.) ( B) Arecent analysis performed by the Antithrombotic Trialists Collaboration found significant reductions in seriousvascular events when aspirin was used in secondary as well as primary prevention. However, as shown, theabsolute benefit in primary prevention was far smaller and must be balanced with major bleeding. ( Data fromBaigent C, Blackwell L, Collins R, et al. Aspirin in the primary and secondary prevention of vascular disease:collaborative meta-analysis of individual participant data from randomised trials. Lancet 2009; 373:1849e60.)
Kolandaivelu & Bhatt74
-
8/7/2019 A n t i p l a t e l e t T h e r a p y
5/15
(2.7% to 3.7%), life-threatening and intracranialbleeding were similar. Thus, clopidogrel use inconjunction with aspirin in ACS leads to long-term event reductions with or without PCI and
its use is indicated.23The benefits of DAPT do not apply to all high-
risk patients. CHARISMA investigated clopidogrelplus low-dose aspirin versus low-dose aspirinalone in stable patients for secondary or primary
prevention.25 Patients with ACS or recent stentingwere excluded. Although the primary end pointwas neutral in the overall population studied, therewas a significant increase in moderate bleeding
with dual therapy. Moreover, subgroup analysissuggested that patients on primary preventionhad no evidence for benefit, although were still atrisk for bleeding (see Fig. 4B). However, benefitwas suggested in the patients on secondary
Fig. 3. Bleeding risks, although often assumed constant or age dependent, are far more complex and better risk
scores are needed to help guide clinical decisions to use or not use antiplatelet therapy in patients at increasedrisk of bleeding. (A) Bleeding risk is highly dependent on cardiovascular risk factors. (Data from Baigent C, Black-well L, Collins R, et al. Aspirin in the primary and secondary prevention of vascular disease: collaborative meta-analysis of individual participant data from randomised trials. Lancet 2009; 373:1849e60.) (B) Bleeding riskincreases substantially as a function of age and gastrointestinal symptoms. (From Patrono C, Garcia RodriguezLA, Landolfi R, et al. Low-dose aspirin for the prevention of atherothrombosis. N Engl J Med 2005;353:2381;with permission.)
Antiplatelet Therapy and Coronary Heart Disease 75
-
8/7/2019 A n t i p l a t e l e t T h e r a p y
6/15
prevention, particularly those with prior ischemicevents (see Fig. 4C).26 Analysis of the CHARISMAdata also showed that the incremental risk ofbleeding with clopidogrel plus aspirin versusaspirin alone was largely during the first year oftherapy.26,27 In patients who tolerated therapy forthe first year without bleeding problems, thesubsequent risk of bleeding was similar to thatseen with aspirin alone. It is important that thesesubgroup hypotheses be confirmed through well-powered prospective testing, particularly asMATCH found that combined clopidogrel andaspirin use following ischemic stroke compared
with clopidogrel alone led to excessive life-threatening bleeding without significant benefit.28
The potential risk of DAPT, when applied toobroadly, and uncertainty about its use in long-term secondary prevention, raises the current
controversy in how long patients should remainon combination therapy once initiated.29 Althoughat least 1 month of therapy is required after baremetal stent implantation (ideally a year in thoseat low bleeding risk), a period of at least a year isrequired after drug-eluting stenting (DES) givenpersistent risks of late stent thrombosis.29 Thelatter issue requires further delineation and isactively being addressed by the DAPT trial. Furthercomplicating the issue is the observation thatsecond-generation DES may have a lower risk ofstent thrombosis than first-generation devices.
Variability in clopidogrel responsiveness
(Fig. 5A) and its association with worse clinicaloutcomes is a great concern, particularly afterstent placement.30,31 For example, gene-products derived from polymorphisms inCYP2C19 and ABCB1 lead to altered hepatic
Fig. 4. As vascular risk increases, more intense therapies become justified. ( A) CAPRIE found clopidogrel was moreeffective than aspirin in patients with established cardiovascular disease as shown in the 3-year Kaplan-Meiercurves, although these modest benefits do not justify routine aspirin replacement given the current increased
cost of clopidogrel. Dual therapy with aspirin and clopidogrel was not significantly better than aspirin alonein the main CHARISMA trial, which considered patients with established disease or multiple risk factors. Post-hoc subgroup analysis, found that although benefits were not seen in the primary prevention subgroup ( FromCAPRIE Steering Committee. A randomised, blinded, trial of clopidogrel versus aspirin in patients at risk of ischae-mic events (CAPRIE). Lancet 1996;348:1333, with permission.), (B) the group of patients receiving dual therapy forsecondary prevention for ischemic events did have a reduction in MI, stroke, or cardiovascular death; (C) shownare the Kaplan-Meier curves for patients with prior MI. These findings must be confirmed prospectively. ( FromBhatt DL, Flather MD, Hacke W, et al. Patients with prior myocardial infarction, stroke, or symptomatic peripheralarterial disease in the CHARISMA trial. J Am Coll Cardiol 2007;49:1987; with permission.)
Kolandaivelu & Bhatt76
-
8/7/2019 A n t i p l a t e l e t T h e r a p y
7/15
metabolism and intestinal absorption, respec-tively, decreased clopidogrel response, and areassociated with higher rates of vascularevents.19,32 Conversely, the CYP2C19*17 alleleaccelerates metabolism and was shown toincrease propensity to bleed.33 In addition to
genetic determinants, environmental factorsincluding hypertension, diabetes, hyperlipidemia,smoking, and increasing age influence clopidogrelresponse.32 Drug-drug interactions, for example,proton pump inhibitors (PPIs), statins, andcalcium-channel blockers, can alter clopidogrelmetabolism, generating controversy about thesafety of combined use. Often, these interactionshave been associated with decreased measuresof clopidogrel response, the clinical significanceof which is unclear.17 Given the lack of evidenceto suggest clinical harm when considered in largerandomized fashion, the beneficial effects of thesemedications seem to overshadow the theoreticrisks.34
The potential effect of clopidogrel nonrespon-siveness has led to approaches to overcome it,most simply through using higher doses of clopi-dogrel. Recently, CURRENT OASIS-7 showedthat higher clopidogrel doses (600 mg loading fol-lowed by 150 mg daily for 1 week, then 75 mgmaintenance) were better than standard regimensin preventing stent thrombosis, although when
applied indiscriminately to patients managedmedically, bleeding rates increased.35 Methodsof personalizing therapy may help to target moreintense therapies to those most likely to needthem (discussed later). However, clopidogrel non-responsiveness can be only partially overcomewith higher doses.35
PrasugrelPrasugrel (Effient) is rapidly converted to an activemetabolite via plasma esterases and a single CYP
activation step, thus shortening its time to onset (1hour) and increasing its potency.2 At maintenanceand loading doses of 60 mg and 10 mg, respec-tively, it exhibits less interindividual variabilitycompared with clopidogrel (either 300 or 600 mgloading and 75 or 150 mg maintenance).36
In TRITON-TIMI 38, prasugrel (60 mg/10 mg)reduced cardiovascular events 20% comparedwith clopidogrel (300 mg/75 mg) when added toaspirin in patients with ACS undergoing PCI.37
However, bleeding increased (including fatal andintracranial bleeds). In patients more than 75 years
old and those less than 60 kg, benefit of therapywas lost.37 Patients with prior transient ischemicattack or stroke suffered net harm.37 Prasugrelwas recently approved by the US Food and DrugAdministration for patients with ACS in planned
PCI, with a black-box warning in these subsets.TRILOGY-ACS should help define if lower dosesof prasugrel are beneficial in these high-riskgroups.2 Its use in clopidogrel nonrespondersremains to be studied (discussed later).
Nonthienopyridine P2Y12 Inhibitors
Direct reversible inhibitors of P2Y12 have recentlybeen tested in large clinical trials. Given theirshort-lived effect on platelet inhibition whenstopped, these agents may help dissociate inten-sity of therapy and risk of uncontrollable bleeding.
TicagrelorTicagrelor (Brilinta) is an adenosine triphosphateanalogue that reversibly blocks P2Y12 receptorswithout requiring metabolic conversion, thus
achieving consistent platelet inhibition within2 hours.13 When stopped, platelet function returnsto baseline within 1 to 2 days. This attractivefeature, however, requires ticagrelor be adminis-tered twice daily.13
PLATO compared ticagrelor (180 mg loading;90 mg twice daily maintenance) with clopidogrel(300e600 mg/75 mg) in combination with aspirinin patients with ACS.38 After 1 year, relativevascular events decreased 16% and there wasno difference in rates of major bleeding. Overallmortality decreased significantly (5.9% to 4.5%;P
-
8/7/2019 A n t i p l a t e l e t T h e r a p y
8/15
Kolandaivelu & Bhatt78
-
8/7/2019 A n t i p l a t e l e t T h e r a p y
9/15
with relevance to longitudinal management, itsequivalence with clopidogrel and dose-dependence makes it a potential bridging therapyin patients requiring invasive procedures (cardiacor otherwise), a prospect currently being testedin the BRIDGE study.2 Methods of transitioning
between IV and oral agents must be clarified; forexample, cangrelor/P2Y12 binding may affect clo-pidogrel loading.42 Elinogrel, also a direct, revers-ible P2Y12 inhibitor in phase II testing, is availablein both IV and oral formulations offering the poten-tial for seamless transitions between routes.3,13
GPIIB/IIIA Inhibitors
GPIIB/IIIA inhibitors block fibrinogen cross-linkingwith GPIIB/IIIA receptors. Three IV formulationshave been approved for management of high-risk
ACS and PCI.2,3 These agents effectively reducedcomposite vascular end points in large, random-ized clinical trials. However, most trials occurredbefore effective application of P2Y12 inhibitors,which have now largely supplanted the need forGPIIb/IIIa inhibitors.3 Currently, GPIIb/IIIa inhibi-tors are best reserved for provisional use. Earlypromise of GPIIb/IIIa antagonism led to develop-ment of various oral GPIIb/IIIa antagonists (of rele-vance to long-term prevention). Several have beentested, although as a class they resulted in excess
bleeding without cardiovascular benefits.43
Further development was abandoned.
Phosphodiesterase Inhibitors
Phosphodiesterase (PDE) inhibitors (dipyridamole[Persantine] and cilostazol [Pletal]) inhibit cyclicnucleotide PDE activity, thereby increasing intra-cellular cyclic nucleotides with pleiotropic effectson platelet inhibition and vasodilation.4,10 Earlyformulations of dipyridamole resulted in inconsis-tent absorption and poor bioavailability, potentially
accounting for variability in clinical effects.15,44Recent trials have focused on its use in cerebro-vascular disease. Extended-release formulations,when combined with aspirin, significantly reduce
vascular event rates more than aspirin alone(ESPS 2 and ESPRIT trials), with efficacy similarto clopidogrel although with a greater risk ofserious bleeding (PROFESS trial).45,46 Use of thesenewer formulations in CHD has yet to be defined.
Cilostazol has been studied as an adjunct to
standard DAPT regimens (so-called triple antipla-telet therapy [TAPT]).47 In small studies (bothACS and PCI), TAPT with cilostazol reducedvascular events, stent thrombosis, even totalmortality, without excess bleeding.47 Moreover,cilostazol was found to reduce variability in clopi-dogrel response and decrease restenosis afterstenting.2,47 Although intriguing, these findingsmust be replicated in larger, more diverse random-ized trials before being broadly applied, particu-larly given the high rate of side effectsassociated with cilostazol and mortality concernsassociated with PDE inhibitor use in patients withheart failure.48
Protease Activated Receptor Inhibitors
PAR inhibitors have the theoretic advantage oflocalizing antiplatelet effects to the vicinity ofactive thrombin generation and clot, potentiallyreducing the risk of systemic bleeding.10 Earlytesting demonstrated similar rates of bleedingwhen added as a third agent to standard DAPT.
Currently, there are 2 oral formulations beingtesting in secondary prevention trials: SCH530348with a half-life of 5 to 10 days resulting in plateletinhibition for around 1 month (through the TRA-2P-TIMI 50 trial) and E5555 with a significantlyshorter half-life (through the LANCELOT CADtrial).10
SPECIAL POPULATIONS
Parallel to novel antiplatelet development, muchremains to be done to realize the full benefit of
therapies that are already proven. Randomizedcontrolled trials serve as powerful proof of effi-cacy, yet strict inclusion and exclusion criteriacan produce significant bias. Thus, the
Fig. 5. (A) Significant variability exists in individual responses to clopidogrel, as shown in the distribution ofplatelet aggregation to 5 mM adenosine. Antiplatelet nonresponsiveness and its proven effect on clinicaloutcomes has led to pharmacogenomic and pharmacodynamic approaches to personalize therapy, typicallythrough the use of increased dosing, alternate antiplatelet agents, or added antiplatelet agents. ( From Sere-bruany VL, Steinhubl SR, Berger PB, et al. Variability in platelet responsiveness to clopidogrel among 544 individ-uals. J Am Coll Cardiol 2005;45:247; with permission.) (B) Despite proven biochemical nonresponsiveness,significant real-world barriers exist to achieving the full potential of these important medications. For example,patient nonadherence to antiplatelet therapy is an enormous issue, confounding measures of platelet responseand our understanding of evidence-based therapies. Treating nonadherent patients as if they were nonresponsivecould result in increased health care costs and net harm. (From Kolandaivelu K, Bhatt DL. Overcoming resistanceto antiplatelet therapy: targeting the issue of nonadherence. Nat Rev Cardiol 2010;7;464; with permission.)