2.8 Luteoma of Pregnancy. h.s. Cronje

of 2
Transcript of 2.8 Luteoma of Pregnancy. h.s. Cronje
-
8/3/2019 2.8 Luteoma of Pregnancy. h.s. Cronje
1/2
SA MEDIESE TYDSKRIF DEEL 66 14 JUUE 1984 59
Luteoma of pregnancyH. S. CRONJE
SummarySeven patients are presented. 6 with luteomas ofpregnancy and 1 with hyperreactio luteinalis. Themean age was 31,7 years and 4 patients had bilateraltumours. Only 1 of these patients was treated withbilateral salpingo-oophorectomy, while 1 patientwitha unilateral tumour had only a wedge biopsy. In allinstances the remaining 'tumour' regressed, supporting the thesis tha t luteomas represent an unusualresponse of ovarian stromal cells to the altered hor-monallevels of pregnancy. About30%of patientswithluteomasof pregnancywill be virilized. and about50%of.female infants from these patients will be masculinized. About 112patients with luteomasof pregnancyhave been reported in the l iterature. The differentialdiagnosis includes theca lutein cysts, the oedematousovarysyndromeand luteinized forms of ovarian stromaltumours.S Atr Med J 1984; 66: 59-60.
Luteoma of pregnancy was described by Sternberg I in 1963, andsince then a further 112 cases have been reported. The questionsurrounding this entity is whether it represents a true neoplasmor only an abnormal response to the hormones of pregnancy.These 'tumours' may be endocrinologically active, as initiallysuggested by Malinak and Miller.2In this article 7 patients are described , 6 with luteoma ofpregnancy and 1 with hyperreactio luteinalis. A review of theliterature on luteoma of pregnancy is presented and the aetiologyand differential diagnosis discussed.
Patients and methodsIn reviewing 477 patients classified under granulosa and thecacell tumours of the ovary in the Emil Novak Ovarian TumorRegistry and in the ftles of the Surgical Pathological Laboratoryof the Johns Hopkins Hospi ta l, 6 pat ients were found withluteoma of pregnancy and I with hyperreactio luteinalis. Thisgroup of7 patients is the subjectof analysis in this article. In eachcase clinical information and microscopic slides were available.
ResultsThe clinical data are summarized in Table 1. Five patients wereBlack, 2 White; the mean age was 31,7 years. They varied frompara 1to para 11 (parity unknown in 2) at the time of pregnancy.
Department ofObstetrics and Gynaecology, Johns HopkinsHospital, Balt imore , Md, USAH. S. CRONJE, F.CO.G. (SA), M.MED., (0 ET G), M.D. (Present address:Department of Obstetrics and Gynaecology, University of Stellenbosch and Tygerberg Hospital, Parowvallei, CP)
Maternal viri li sm occurred in 2 pat ients, both with bilateraltumours, but the fetal outcome is unknown.In 4 pat ients the tumour was found accidentally, in 3 atcaesarean section and in I at postpartum tuballigation. Bilateraltumourswere present in4 patients,one of them beingthe patientwith hyperreactio luteinalis. A unilateral salpingo-oophorectomywas done in 5 patients, including 3 of those with bilateraltumours. In one of them, a specimen was taken from the otherovary. The 4th patient with bilateral tumourswas treated by totalabdominal hysterectomy and bilateral salpingo-oophorectomy.Finally, in I patient only a wedge biopsy was done. There wereno recurrences or deaths after 2,3 and 13 years respectively in the3 patients who were followed up.The previous diagnoses in these pat ients were luteinizedgranulosa cell tumour (cases 2, 3, 5 and 6; seeTable I), luteoma of
pregnancy (cases 1 and 7) and luteinized Stein-Leventhalsyndrome (case 4).
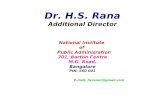
DiscussionIn 1975 Garcia-Bunuel et aP reported the iargest publishedseries ofluteoma of.pregnancy (20 patients). They reviewed theliterature and found 54previously recorded patients, 14 ofwhomwere masculinized. Jenkins et al.4 had reported 30 cases in 1968,but 29 were from the literature and only I their own. GarciaBunuel et aP included 22 of t hese 29 repor ted cases in the irseries. Since the latter report in 1975, 8 cases of luteoma ofpregnancy have been reported in the literature, 5 ofwhich wereassociated with maternal virilization. S- 12 Two of the latter,however, were probablyhyperreactio luteinalis since the tumourswere multicystic.s,7 These masculinized patients had maleinfants (sex unknown in I case).Clinical aspects of interest in pat ients with luteomas ofpregnancy include a predominance of Black. patients,3,4 anassociation w.ith pre-eclampsia and obesity, and a 30% prevalence .of maternal masculinization during pregnancy.3 About 50% offemale infants born to these masculinized mothers will bevirilized. 13 Conservative surgery such as amputation of anenlarged clitoris may be necessary in a female infant} Maleinfants suffer no untoward effects and all mothers with masculinization return to normal after delivery.Pre-operative hormonal s tudies in masculinized pat ientsrevealed high levels of 17-ketosteroids, plasma testosterone,dihydrotestosterone, androstenedione and dehydro-epiandrosterone.6- 9 These elevated levels returned to normal with in 3days of removal of the tumour. Both ~ - and ~ - pathways wereutilized in the synthesis of androgens. 8,9Luteomas of pregnancy are bilateral in 45% of cases. 3 Thetumours are usually smooth and solid, yellow to yellow-orangeand about 6 - 10 cm in diameter. 14 Microscopically, a markedlyuniform sheet of cells is seen, often composed of ill-defmed cordsand nests. Classically, a rwo-eell population is present (Fig. I).The first type is a cellwith deeply staining acidophilic cytoplasm,presumably of theca origin, which has invaded the granulosalayer during its luteinization. The second cell type is larger withless intense cytoplasmic eosinophilia, resembling luteinizedgranulosa cells. Reinke crystalloids have not been demonstratedin either cell.3Most tumours are not palpable during pregnancy and surgeryis generally performed for other reasons. In about 60% of all
-
8/3/2019 2.8 Luteoma of Pregnancy. h.s. Cronje
2/2
60 SA MEDICAL JOURNAL VOLUII.1E 66 14JULY 1984
TABLE I. LUTEOMA OF PREGNANCYAge
Case Race (yrs) Grav. Para Location, s ize Treatment Follow-up1 Black 42 ? ? Bilateral, 6 cm usa at C/S2 Black 20 ? ? Unilateral Wedge3 Black 22 4 2 Right, 13 cm usa at C/S 3 yrs4 White 38 2 1 Bilat., 6 and 10 cm usa5 Black 27 6 1 Bilat., 5 and 6 cm TAH,BSO6 White 31 2 1 Unilat., 7 cm usa at C/S 13 yrs7* Black 41 12 11 Bilat., bluish,
multicystic usa 2 yrsusa = unilateral salpingo-oophorectomy:850 = bilateral salpingo-oophorectomy; TAH= total abdominal hysterectomy;C/ S = caesarean section.""Hyperreactio luteinalis (see text).
Fig. 1. Luteoma of pregnancy. Note solid sheet of cells with dark(pink) and pale cells (X 400).
pat ients the tumour was found at caesarean section, withcephalopelvic disproportion as the indication in half of them.Unilateral salpingo-oophorectomy is the treatment most oftenapplied. Other forms of treatment vary from wedge biopsies> tototal abdominal hysterectomy and bilateral salpingo-oophorectomy. Tumours left behind regressed almost routinely. Thesepatients have no difficulty in becoming pregnant again and the'tumour' rarely recurs.3 The correct treatment, therefore, isbiopsy and conservation of the enlarged ovary.
The origin of luteomas of pregnancy is presumably the thecaand granulosa cells responding to the elevated hormonal levelsofpregnancy.3 Chorionic gonadotrophin was suspected as thepromoter, bu t administration of this hormone in late pregnancyhas resulted only in a dramatic hyperreactio luteinalis or thecalutein cyst. Luteomas of pregnancy have not been producedexperimentally. Theca lutein cysts, often seen in association withmolar pregnancies, mayrepresent a cysticform ofluteoma. Theyare characterized by similar clinical phenomena, although it hasbeen stated that the cystic form 'protects' a female infant againstmasculinization if the mother is masculinized. l3 Similar celltypes can be seen in both theca lutein cysts and in luteomas, andboth regress postpartum. These tumours, therefore, represent anon-neoplastic hyperplasia of certain stromal cells, althoughuncertainty exists as to whether some are preceded by minutelesions like thecomas. One of the Emil Novak Ovarian TumorRegistry patients (case 4) with bilateral luteomas had a history ofpossible Stein-Leventhal syndrome.
The differential diagnoses include the stromal luteoma,l>luteinized forms of thecoma, granulosa cell tumour and gonadalstromal tumour, and the large oedematous ovary syndrome. Thelatter, as well as the stromal luteoma, may consist of a two-cellpopulation as seen in luteomas of pregnancy. These patients arenot pregnant and the oedematous ovary syndrome has a distinctappearance with its oedematous stroma in contrast to the solidsheet of cells of the luteoma of pregnancy. Luteinized granulosaand theca cell tumours lack the two-cell population of theluteoma of pregnancy. The stromal luteoma and luteinizedgonadal stromal tumour are probably variants of the sameentity.
In conclusion, the luteoma of pregnancy is a rare conditionwhich probably represents an unusual response to the alteredhormonal environment in pregnancy. I t regresses in the postpartum period. About one-third of patients will become masculinized during pregnancy and half the female infants born tothese mothers will also be masculinized. Luteomas should bedifferentiated from the theca lutein cysts, the oedematous ovarysyndrome, and luteinized forms of ovarian stromal tumours.I wish to thank Professor J. D. Woodrufffor his assistance in themicroscopic evaluation of these tumours.
REFERENCES1. Sternberg WHo Nonfunctioning ovarian neoplasms. In: Grady HG , SmithDE, eds. The Ovary. (International AcademyofParhologisrs, Monograph No.3). Baltimore: Williams & Wilkins, 1963: 209.2. MaIinak LR, Miller GV. Bilateral multicentric ovarian luteomasof pregnancyassociated with masculinizationof a female infant. Am] Obs!er Gynecol 1965;91: 251-259.3. Garcia-Bunuel R, Berek JS, Woodruff JD. Luteomas of pregnancy. Obs!erGyneco/1975; 45: 407-414.4. Jenkins ME, Surana RB, Russell-Cutts CM. Ambiguous genitals in a femaleinfant associated with luteoma of pregnancy: report of a case. Am] ObslelGynecol 1968; 101: 923-928.5. Tucker S, Buell J , F isherHR. Luteoma of pregnancy: case reportAm] ObsrerGyneco11975; 121: 282.6. Forti G, Burarti R, Colafranceschi M er al. Hormonal studies in a virilizing'luteoma' of pregnancy ('nodular theca-Iuteinic hyperplasiaofpregnancy'). In:James VH er al., eds. The Endocrine Function of rhe Human Ovary. London:Academic Press, 1976: 417.7. Polansky S, de Papp EW, Ogden EB. Virilization associated with bilateralluteomas of pregnancy. Obmr Gyneco11975; 45: 516-522.8. Zander J, Mickan H. Luteoma of pregnancy with androgenic activity. In: deWatteville H er al., eds. Diagnosis and TTeatmenr of Ovarian NeoplasricAlrerations. Amsterdam: Excerpta Medica, 1975: 249-251.9. O'MalJey BW, LipsettMB, Jackson MA. Steroid content and synthesis in avirilizing luteoma.] Clin Endocrinoll967; 27: 311-319.10. RachmanR, TellemM. Bilateral ovarianluteomas withtubal pregnancy.Am]
Obmr GynecoI1964; 88: 132-134.11. B6hm W. Der Luteinzellrumordes Ovars bei Graviditiit.Zenrra/bl AlIgParhol1977; 121: 404-408.12. Fonseca JJS, QuesadaGZ. Luteomaof pregnancy: reportof a case and reviewof literaruse.] RepTodMed 1975; 14: 76-79.13. Hensleigh PA, Woodruff JD. Differential maternal-fetal response to andro-genizing luteoma or hyperreactio luteinalis. Obscer Gynecol Surv 1978; 33:262-271.14. Tulzer H, Vim R. A very large luteoma gravidarum.ZentTalbl Gynako/1976;98: 1659-1660.15. ScullyRE. Stromal luteomaof the ovary: a distinctivetype oflipoid-eelltumor.Cancer 1964; 17: 769-778.