28 DAVID SUTTON PICTURES THE PEDIATRIC ABDOMEN
89
28 THE PAEDIATRIC ABDOMEN DAVID SUTTON
-
Upload
muhammad-bin-zulfiqar -
Category
Education
-
view
40 -
download
3
Transcript of 28 DAVID SUTTON PICTURES THE PEDIATRIC ABDOMEN

28THE PAEDIATRIC ABDOMEN
DAVID SUTTON

DAVID SUTTON PICTURES
DR. Muhammad Bin Zulfiqar PGR-FCPS III SIMS/SHL

• Fig. 28.1 Barium aspiration. CXR in a 2-month-old boy with congenital varicella and bulbar palsy demonstrating high-density opacities throughout the right lung secondary to aspiration during a barium meal examination performed at 2 days of age. Gastrostomy feeding was instituted.

• Fig. 28.2 Gadolinium-enhanced 3D MR angiogram in a 6-year-old girl following liver transplantation demonstrating stenosis of the portal venous anastomosis with poststenotic dilatation.

• Fig. 28.3 Oesophageal atresia with tracheo-oesophageal fistula. A coiled nasogastric tube is seen in the dilated proximal oesophageal pouch (top arrow). The presence of distal air-filled bowel implies an associated tracheoesophageal fistula. Thirteen pairs of ribs are noted, compatible with VATER syndrome (lower arrow).

• Fig. 28.4 Contrast oesophagram demonstrating oblique track (arrows) of a tracheo-oesophageal fistula with contrast filling the tracheobronchial tree.

• Fig. 28.5 Double aortic arch. AP barium swallow (A) demonstrating bilaterality are much reduced. smooth extrinsic filling defects with a posterior oesophageal impression on lateral image (B). Axial T,-weighted MRI (C) confirming double aortic arch.

• Fig. 28.6 Pyloric stenosis. AXR showing distended gastric air bubble.

• Fig. 28.7 Pyloric stenosis. Longitudinal US image (A) showing an elongated thickened pylorus, muscle length 1 7 mm and width 3.8 mm. Transverse image (B) in another patient with muscle width 6 mm. No transit of gastric contents into the duodenum was observed.

• Fig. 28.8 Normal pylorus. Longitudinal US section demonstrating an open pyloric canal with transit of gastric contents observed on dynamic imaging. Wall thickness approximately 2 mm.

• Fig. 28.9 Pyloric stenosis. Barium meal showing an elongated pyloric canal and shouldering of the antrum due to the hypertrophied pyloric muscle.

• Fig. 28.10 Duodenal atresia. Erect (A) and supine (B) AXR demonstrating the 'double-bubble' sign.

• Fig. 28.11 Duodenal web. Barium meal demonstrating a curvilinear filling defect or 'wind-sock diverticulum' in the second part of the duodenum with proximal dilatation.

• Fig. 28.12 Malrotation and volvulus. AXR in a 12-month-old boy with bilious vomiting. The stomach is distended with a relative paucity of gas distally.

• Fig. 28.13 Malrotation. Contrast meal (A) demonstrating abnormally low position of the duodenojejunal junction (DJJ) (arrow). Further case (B) demonstrating both inferior and medial displacement of the DJJ (arrow). The normal DJJ should lie to the left of the midline (over or lateral to the left vertebral pedicle) at the level of the pylorus.

• Fig. 28.14 Midgut volvulus presenting as a classic 'corkscrew' appearance of the duodenum and proximal jejunum on lateral view (A) and in a further case as complete duodenal obstruction (B). The linear filling defect is likely to represent the superior mesenteric vessels and associated mesentery.

• Fig. 28.15 Contrast meal showing mild inferior displacement of the duodenojejunal junction (DJJ) in the presence of multiple dilated loops of bowel. In this case the cause of obstruction was an undiagnosed inguinal hernia. A repeat contrast meal after surgery showed a normal DJJ location.

• Fig. 28.16 Follow-through examination demonstrating an abnormal high and medial caecal position (arrow). Malrotation confirmed at surgery.

• Fig. 28.17 Transverse ultrasound images of the normal superior mesenteric artery: vein relationship (A) and a malrotated child (B) in whom the SMV lies to the left of the SMA.

• Fig. 28.18 Ultrasound 'whirlpool' sign of midgut volvulus. Twisting mesenteric vessels with concentric rings of echogenic mesentery.

• Fig. 28.19 Chronic volvulus. Doppler ultrasound showing large dilated mesenteric veins in an 8-year-old girl with a long history of intermittent abdominal pain. Barium meal confirmed malrotation, and chronic volvulus was found at laparotomy.

• Fig. 28.20 Neonatal low gastrointestinal obstruction. Multiple loops of distended air-filled bowel.

• Fig. 28.21 Meconium ileus. AXR showing loops of dilated bowel with a ' bubbly' appearance of meconium mixed with air in the right side of the abdomen. Free air is seen, indicating a perforation.

• Fig. 28.22 Meconium ileus. Contrast enema demonstrating a microcolon with reflux into dilated distal ileum. Multiple filling defects of inspissated meconium are seen within the distal ileum (superimposed over the transverse colon) and the colon.

• Fig. 28.23 Ileal atresia. Contrast enema with microcolon and reflux into non-dilated distal ileal segment with abrupt convex termination. A few meconium plugs are present.

• Fig. 28.24 Hirschsprung's disease. An abrupt transition zone is seen at the rectosigmoid junction on this lateral rectal view from a contrast enema performed on a 2-day-old boy with failure to pass meconium. The rectum was difficult to distend well and showed irregular contractions.

• Fig. 28.25 Functional immaturity (left colon syndrome). Contrast enema in a newborn term infant showing a relatively small left colon, transition zone at the splenic flexure and a large coiled meconium plug which was dislodged from the splenic flexure to the hepatic flexure during colonic filling. The patient established a regular bowel habit over the following week and was discharged uneventfully.

• Fig. 28.26 Colonic atresia. AXR (A) showing disproportionate dilatation of one bowel loop in a neonate with abdominal distension and failure to pass meconium. Contrast enema (B) showing a blind-ending colon with a convex distal border in the splenic flexure. The dilated air-filled proximal colonic segment can be seen. An isolated colonic atresia was confirmed at surgery.

Fig. 28.27 Anorectal atresia with urethral fistula. Micturating cystogram (A) demonstrating fistula from the distal rectal pouch to the posterior urethra and distal loopogram (B) showing a fistula to the anterior urethra in two newborn boys with high anorectal malformations.

• Fig. 28.28 Perineal ultrasound documenting an 8 mm rectoperineal distance consistent with a low anorectal malformation.

• Fig. 28.29 Portal venous air. AXR (A) and ultrasound (B) evidence of portal venous air in a premature infant with necrotising enterocolitis.

• Fig. 28.30 Free intraperitoneal air in perforated necrotising enterocolitis demonstrated by lucency over the entire abdomen (football sign), subdiaphragmatic air and outlining of both sides of the bowel wall (Rigler's sign).

• Fig. 28.31 Necrotising enterocolitis. Supine AXR (A) demonstrating extensive 'bubbly' pneumatosis in a 16-day-old premature infant born at 28 weeks gestation. No definite free air seen. However, lateral shoot-through radiograph (B) shows a small triangle of free air beneath the anterior abdominal wall (arrow). A localised ileal perforation was found at laparotomy.

• Fig. 28.32 Left congenital diaphragmatic hernia with associated mediastinal shift and pulmonary hypoplasia. The tips of the arteriovenous (AV) ECMO lines are positioned in the right atrium (radiodense dot distal to the opaque portion of the catheter) and in the origin of the right common carotid artery or aortic arch.

• Fig. 28.33 Diaphragmatic eventration. PA (A) and lateral (B) CXR demonstrating a focal bulge in the anteromedial portion of the right hemidiaphragm. Cardiomegaly and pulmonary plethora are due to a ventricular septal defect.
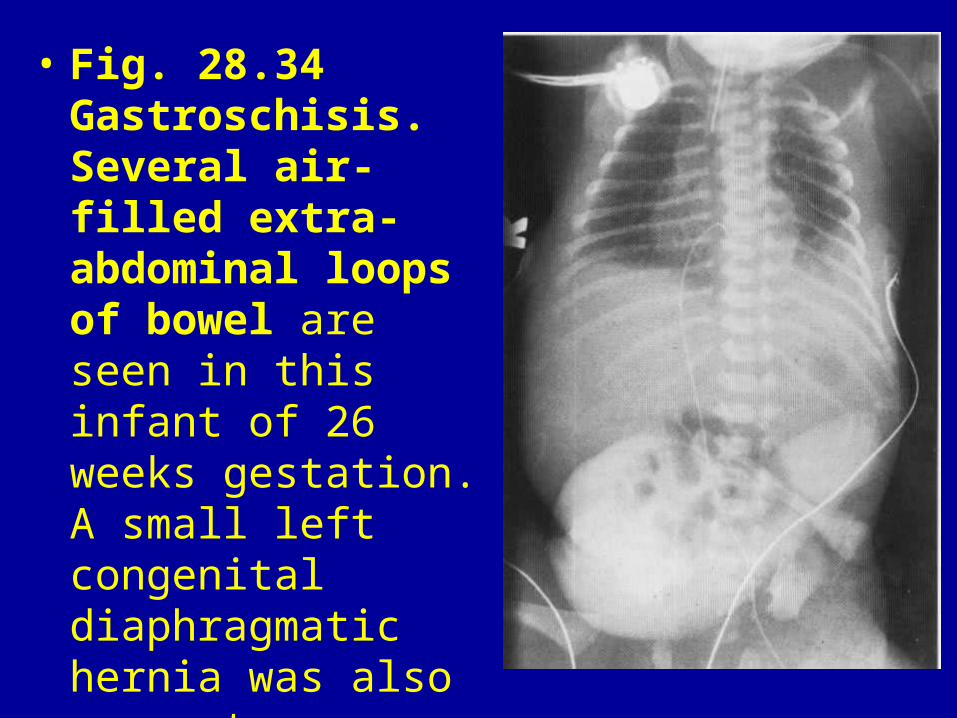
• Fig. 28.34 Gastroschisis. Several air-filled extra-abdominal loops of bowel are seen in this infant of 26 weeks gestation. A small left congenital diaphragmatic hernia was also present.

• Fig. 28.35 Ingested coin. PA CXR (A) demonstrating a coin impacted in the proximal oesophagus. Coins lodged within the oesophagus are seen ' en face' on PA CXR, whereas impaction within the trachea results in 'sideon‘ visualisation. Lateral cervical spine X-ray (B) confirming oesophageal location of the foreign body.

• Fig. 28.36 Duplication cyst. Hypoechoic cyst with double 'gut wall signature'. In this case the adjacent segment of bowel can be seen along the superior border of the cyst, confirming its origin.

• Fig. 28.37 Oesophageal duplication cyst. CXR (A) on a 6-month-old infant admitted to paediatric intensive care with upper airway obstruction showing deviation of the nasogastric tube to the right and a possible right paratracheal mass. AP (B) and lateral (C) views from contrast swallow showing smooth extrinsic compression and posterolateral deviation of the proximal oesophagus with narrowing and anterior bowing of the trachea. CT (D) confirmed the presence of a prevertebral tubular cystic mass with oesophageal and tracheal displacement. A proximal oesophageal duplication cyst was resected at thoracotomy.

• Fig. 28.37 Oesophageal duplication cyst. CXR (A) on a 6-month-old infant admitted to paediatric intensive care with upper airway obstruction showing deviation of the nasogastric tube to the right and a possible right paratracheal mass. AP (B) and lateral (C) views from contrast swallow showing smooth extrinsic compression and posterolateral deviation of the proximal oesophagus with narrowing and anterior bowing of the trachea. CT (D) confirmed the presence of a prevertebral tubular cystic mass with oesophageal and tracheal displacement. A proximal oesophageal duplication cyst was resected at thoracotomy.

• Fig. 28.38 Mesenteric cyst. CT demonstrating a large left-sided cystic abdominal mass with compression of the left kidney. Ultrasound showed multiple fine septations within the cyst (not illustrated).

• Fig. 28.39 Appendicolith. Rounded calcific density projected over the multiple fine septations within the cyst (not illustrated). right iliac fossa in a 7-year-old boy presenting with abdominal pain.

• Fig. 28.40 Acute appendicitis. Transverse ultrasound image demonstrating a hypoechoic tubular structure 7 mm (markers) in diameter adjacent to the iliac vessels. It was blind-ending and non-compressible.

• Fig. 28.41 Perforated appendicitis. Right iliac fossa mixed echogenicity inflammatory mass. A 6 mm echogenic focus with acoustic shadowing consistent with an appendicolith confirms the diagnosis.

• Fig. 28.42 CT pelvis (A) showing a large thick-walled pelvic abscess containing an air-fluid level in a 9-year-old girl presenting with a 10 day history of ill-defined abdominal pain and diarrhoea. An appendicolith was identified on a more superior slice (B). The patient was managed with percutaneous drainage and antibiotic therapy

• Fig. 28.43 Acute appendicitis. CT pelvis in a 12-year-old boy with a recent diagnosis of acute leukaemia and a 2 day history of abdominal pain. The appendix is identified medial to the iliac vessels (arrow). It is thick walled and associated with a small pocket of free fluid. An acutely inflammed appendix was found at laparotomy.

• Fig. 28.44 Henoch-Schönlein purpura. Ultrasound (A), barium follow-through (B) and CT abdomen (C) demonstrating jejunal bowel wall thickening in a 5-year-old boy. Thickening of the valvulae conniventes can also be seen on the barium study.

• Fig. 28.45 Graft-versus-host disease. CT abdomen demonstrating extensive thickening of the bowel wall, abnormal mucosal enhancement and mesenteric stranding in pancolitis due to GVHD after bone marrow transplantation.

• Fig. 28.46 Juvenile polyp. Barium enema demonstrating a pedunculated polyp in the descending colon (arrow).

• Fig. 28.47 Colitis. Ultrasound demonstrating thick-walled ascending colon, in this case due to Crohn's disease. Doppler examination showed hyperaemia of the bowel wall.

• Fig. 28.48 Gadolinium-enhanced fat saturated T 1 -weighted axial MRI pelvis showing diffuse mucosal enhancement and bowel wall thickening of the rectosigmoid colon in Crohn's disease.

• Fig. 28.49 Intussusception. Paucity of bowel gas in the right iliac fossa and a soft-tissue mass (arrows) strongly suggest intussusception in this 11-month old child. However, in many cases, AXR shows no definite abnormality.

• Fig. 28.50 Intussusception. Transverse ultrasound showing multiple hypoechoic concentric rings, central echogenic mesentery and a few small trapped lymph nodes.

• Fig. 28.51 Pathological lead point. Composite ultrasound image showing a cystic mass at the head of an intussusception in a 3-month-old boy. A duodenal duplication cyst was found at laparotomy.
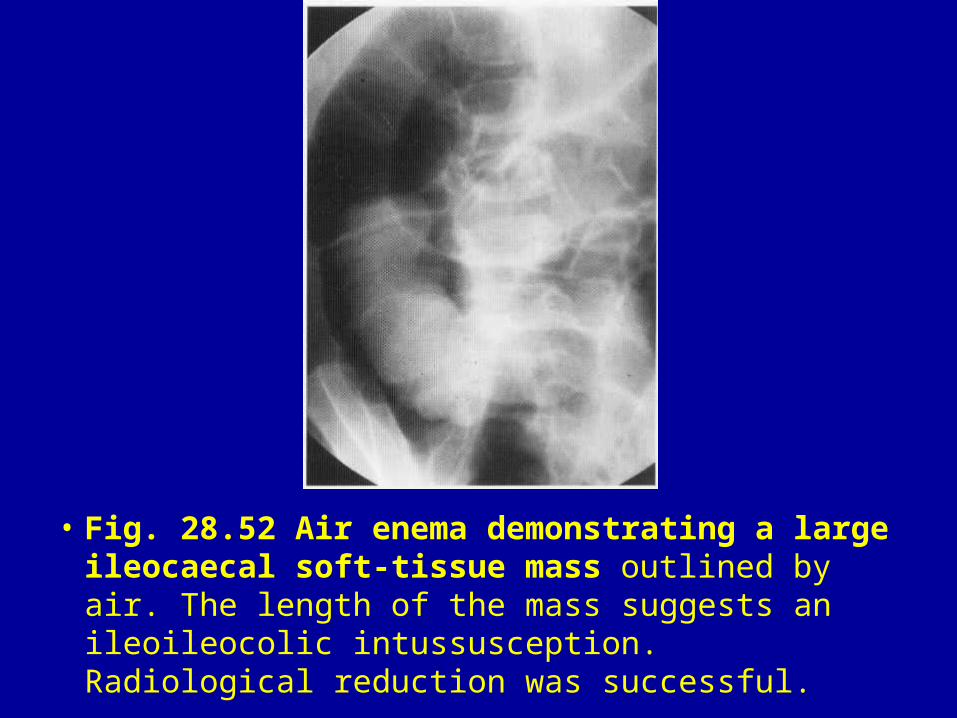
• Fig. 28.52 Air enema demonstrating a large ileocaecal soft-tissue mass outlined by air. The length of the mass suggests an ileoileocolic intussusception. Radiological reduction was successful.

• Fig. 28.53 Transverse (A) and longitudinal (B) ultrasound images demonstrating a small bowel intussusception around the tip of a gastrojejunostomy feeding tube.

• Fig. 28.54 Bilateral Wilms' tumours. CT showing bilateral large low attenuation renal masses filling the abdomen of this 5-month-old girl.

• Fig. 28.55 Wilms' tumour. Ultrasound (A) demonstrates a large heterogenous mass arising from the left kidney containing multiple low echogenicity areas of haemorrhage or necrosis. CT (B, C) demonstrates the ' claw sign' with renal parenchyma stretched around the mass, confirming its renal origin. The tumour displaces the retroperitoneal vessels without encasing them. The left renal vein lies over the anteromedial aspect of the mass. Small retroperitoneal lymph nodes are present.

• Fig. 28.55 Wilms' tumour. Ultrasound (A) demonstrates a large heterogenous mass arising from the left kidney containing multiple low echogenicity areas of haemorrhage or necrosis. CT (B, C) demonstrates the ' claw sign' with renal parenchyma stretched around the mass, confirming its renal origin. The tumour displaces the retroperitoneal vessels without encasing them. The left renal vein lies over the anteromedial aspect of the mass. Small retroperitoneal lymph nodes are present.

• Fig. 28.56 Non-Hodgkin's lymphoma of the kidneys. Longitudinal renal ultrasound (A) in a 5-year-old boy showing multiple isoechoic masses in a 17 cm kidney. Axial T,-weighted (B) and coronal STIR MRI (C) confirming gross enlargement of both kidneys with complete loss of normal renal architecture. Differential diagnoses include lymphoma, leukaemia and nephroblastomatosis. Biopsy yielded non-Hodgkin's lymphoma.

• Fig. 28.56 Non-Hodgkin's lymphoma of the kidneys. Longitudinal renal ultrasound (A) in a 5-year-old boy showing multiple isoechoic masses in a 17 cm kidney. Axial T,-weighted (B) and coronal STIR MRI (C) confirming gross enlargement of both kidneys with complete loss of normal renal architecture. Differential diagnoses include lymphoma, leukaemia and nephroblastomatosis. Biopsy yielded non-Hodgkin's lymphoma.

• Fig. 28.57 Angiomyolipoma. Longitudinal ultrasound showing a well-circumscribed echogenic mass in the upper pole of the right kidney.

• Fig. 28.58 Tuberous sclerosis. The architecture of both kidneys is distorted by multiple fat-containing angiomyolipoma. This CT was performed on a 15-year-old girl with tuberous sclerosis admitted with acute abdominal pain following haemorrhage into one of the right-sided lesions. Oedematous changes in the right abdominal wall followed removal of a percutaneous drain.

• Fig. 28.59 Neonatal adrenal haemorrhage. Ultrasound of a right adrenal haemorrhage on day 2 (A) and day 10 (B) of life. Decrease in size of the mass, often with cystic change (not shown in this example) confirms the nature of the lesion.


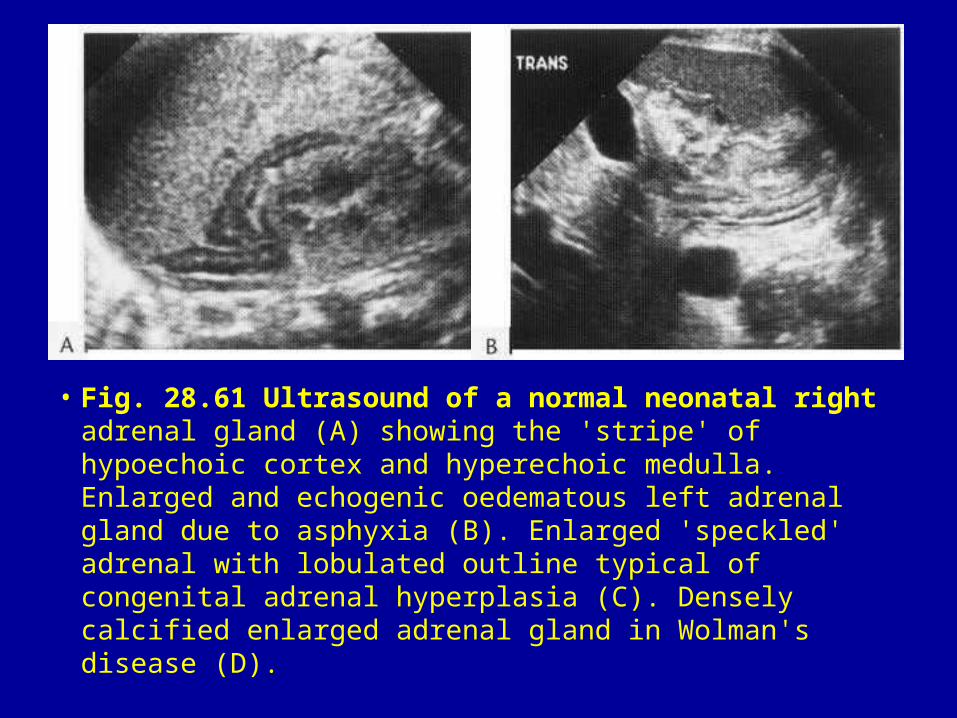
• Fig. 28.61 Ultrasound of a normal neonatal right adrenal gland (A) showing the 'stripe' of hypoechoic cortex and hyperechoic medulla. Enlarged and echogenic oedematous left adrenal gland due to asphyxia (B). Enlarged 'speckled' adrenal with lobulated outline typical of congenital adrenal hyperplasia (C). Densely calcified enlarged adrenal gland in Wolman's disease (D).

• Fig. 28.61 Ultrasound of a normal neonatal right adrenal gland (A) showing the 'stripe' of hypoechoic cortex and hyperechoic medulla. Enlarged and echogenic oedematous left adrenal gland due to asphyxia (B). Enlarged 'speckled' adrenal with lobulated outline typical of congenital adrenal hyperplasia (C). Densely calcified enlarged adrenal gland in Wolman's disease (D).

Fig. 28.62 Hepatoblastoma. Unenhanced (A) and enhanced (B) CT abdomen showing a large low-attenuation mass in the left lobe of the liver with small central calcific foci and heterogenous enhancement. delineated on ultrasound, CT or MRI and strongly suggest malignancy

• Fig. 28.64 Hepatic cyst. CT abdomen demonstrating a congenital hepatic cyst within the right lobe.

Fig. 28.63 Haemangioendotheliosis. Ultrasound (A) showing an ill defined, almost isoechoic mass with multiple vascular channels in the right lobe of the liver in a newborn infant with congestive cardiac failure. Axial T,-weighted (B) and T2 -weighted (C) MRI showing lesions within the right and left lobes (low signal on T1 , high signal on T 2 ) with tortuous dilated feeding vessels arising from the coeliac axis. Sagital 2D TOF MRA (D) showing large calibre proximal abdominal aorta with a reduction in calibre below the origins of the dilated coeliac axis and superior mesenteric artery.

• Fig. 28.63 Haemangioendotheliosis. Ultrasound (A) showing an ill defined, almost isoechoic mass with multiple vascular channels in the right lobe of the liver in a newborn infant with congestive cardiac failure. Axial T,-weighted (B) and T2 -weighted (C) MRI showing lesions within the right and left lobes (low signal on T1 , high signal on T 2 ) with tortuous dilated feeding vessels arising from the coeliac axis. Sagital 2D TOF MRA (D) showing large calibre proximal abdominal aorta with a reduction in calibre below the origins of the dilated coeliac axis and superior mesenteric artery.

• Fig. 28.65 Hepatic arteriovenous malformation. Ultrasound of the liver showing dilated portal venous and hepatic arterial vessels. Doppler spectral traces confirmed arterialisation of the portal venous system due to arteriovenous shunting. There was no associated soft-tissue mass.

• Fig. 28.66 Target lesion. Ultrasound showing a small target lesion with hypoechoic rim in the left lobe of the liver. Several other hepatic lesions were identified in this immunosuppressed patient and are highly suspicious for fungal infection in this clinical setting.

• Fig. 28.67 Ruptured choledochal cyst. This 2-year-old girl presented with clinical signs of peritonitis and echogenic ascites documented on ultrasound. CT abdomen shows a right upper quadrant cyst with a 'tail' directed towards the head of the pancreas and ascites. Laparotomy confirmed the diagnosis.

Fig. 28.68 Fusiform dilatation of the common hepatic and common bile ducts in a type 1 B choledochal cyst (A) and a large saccular type 2 choledochal cyst showing connection to the common bile duct (B).

Fig. 28.69 Gallstones. Multiple calculi within a collapsed gallbladder in a 13-year-old girl with sickle-cell anaemia.

• Fig. 28.70 Acalculous cholecystitis. Ultrasound demonstrating grossly thickened gallbladder wall in an 8-year-old girl admitted to paediatric intensive care with pneumonia and septicaemia

• Fig. 28.71 Pancreatic pseudocyst. CT abdomen (A) showing two large pseudocysts anterior to the body of the pancreas. This 3-year-old boy had sustained a laceration to the neck of the pancreas 9 days earlier (B) following a fall from a shopping trolley.

• Fig. 28.72 Solid papillary tumour of the pancreas. CT abdomen with a large low-attenuation mass in the region of the tail of the pancreas in a 16- year-old girl. Ultrasound demonstrated both solid and cystic components to the mass (not illustrated).

• Fig. 28.73 Polysplenia. Two spleens were identified on ultrasound in this newborn infant with left isomerism.

• Fig. 28.74 Wandering spleen. CT abdomen in a 4-year-old boy with acute abdominal pain demonstrating a low-attenuation mass in the pelvis. No spleen identified in the left upper quadrant. The echogenicity of the mass was similar to splenic tissue on ultrasound (not illustrated) but no Doppler flow was obtained, consistent with an infarcted wandering spleen.

• Fig. 28.75 Multiple small hypoechoic lesions within the spleen may be due to infections (fungal disease, granulomatous disease, bacterial microabscesses), diffuse infiltrative lymphocytosis syndrome in HIV-infected children (case illustrated), extramedullary haematopoesis or, rarely, metastases.
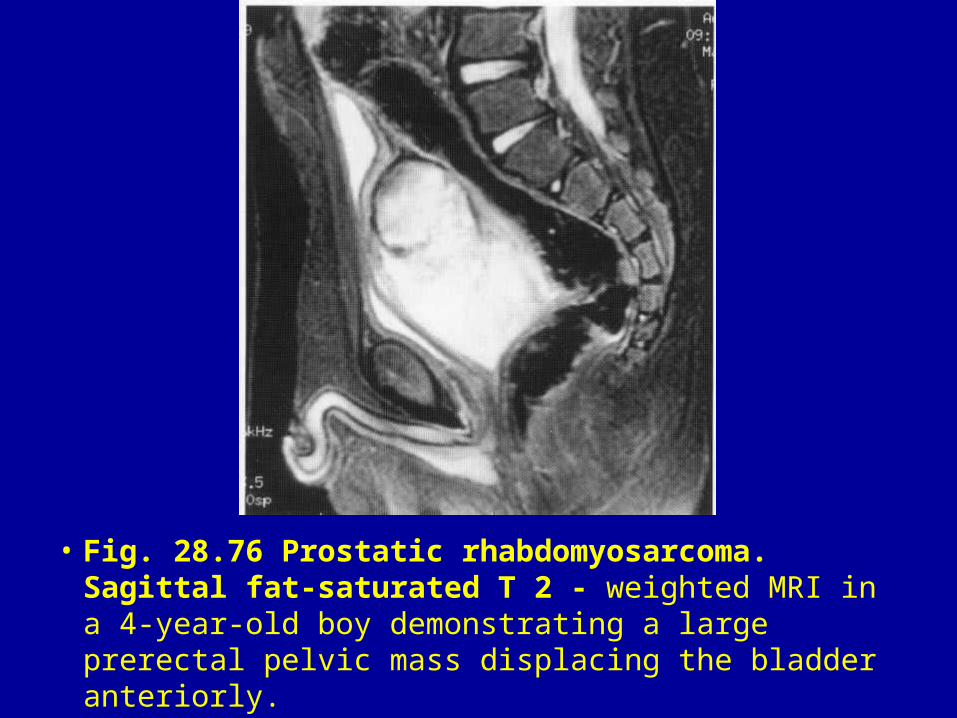
• Fig. 28.76 Prostatic rhabdomyosarcoma. Sagittal fat-saturated T 2 - weighted MRI in a 4-year-old boy demonstrating a large prerectal pelvic mass displacing the bladder anteriorly.

• Fig. 28.77 Type II sacrococcygeal teratoma. CT pelvis (A) in a newborn girl showing a presacral mass with a large external component (B) containing soft tissue, cystic, fat and calcific elements.

• Fig. 28.78 Ovarian cyst. Ultrasound of the pelvis in a 4-week-old girl demonstrating an ovarian cyst containing mobile debris. A crescent of ovarian tissue is seen laterally and confirms the origin of the cyst.

• Fig. 28.79 Mature ovarian teratoma in an 11-year-old girl. CT demonstrating a large mixed solid/cystic mass arising from the pelvis and containing fat and calcification.

• Fig. 28.80 Torted ovary. This infant girl presented with a tender left inguinal lump. Ultrasound showed a hypoechoic mass with peripheral cysts and absent Doppler flow. Surgical exploration revealed a torted left ovary that had herniated into the inguinal region.