
2015 Health Trends
59
HE AL TH 20 15 HEALTH TRENDS MARKETING CONSUMER DIGITAL HEALTH
description
2015 Health Trends: New challenges for a changing industry In the second of their 4-part annual trend report series, GSW takes a closer look at healthcare. From evolutions in doctor-patient relationships to strategies in benefit design to the changing mind-set of physicians, a new landscape takes shape.
Transcript of 2015 Health Trends

HEALTH
20
15
HEALTHTRENDS
MARKETING
CONSUMER
DIGITAL
HEALTH

20
15
HEALTHTRENDS
Our fifth annual series of trends reports includes insights into the
big shifts that are changing marketing, healthcare, digital
experience, and consumer expectations. In this report, you’ll find
the top eight trends in marketing, each with clues into new
possibilities and examples of brands that got there first.

20
15
HEALTHTRENDS
Abigail Schmelzer
Alex Brock
Andrea Evans
Angela Cua
Azul Ceballos
Bruce Rooke
Campbell Hooper
Charles DiSantis
Chelsea Bailey
Duncan Arbour
Eduardo Menendez
Eric Davis
Fred Harrison
James Tomasino
Jeffrey Giermek
Jeffrey Wilks
Jessie Brown
Joe DeSalvo
John Mucha
Joy Hart
Julie Valka
Kathryn Bernish-Fisher
Kevin Nalty
Leigh Householder
Luke Hebblethwaite
Matt Groom
Mike Martins
Nick Bartlett
Nicole Sordell
Pavithra Selvam
Phil Storer
Richard Martin
Rick Summa
Sam Cannizzaro
Sarah Brown
Sayeed Anwar
Scott Raidel
Stefanie Jones
Zach Gerber
CORE
CONTRIBUTORS

At the core of our innovation
practice is a simple idea:Knowing how people’s expectations are changing lets us capture new
market opportunities, take smart risks, and spur innovation
We start by uncovering clues. Clues are data points, great stories,
quotes, and pictures that shift our understanding of what people want
right now. We find them in practices around the world and in the
technologies, brands, and experiences that doctors and patients
encounter in their everyday lives.
Over time, those clues combine and connect to reveal trends, a new
kind of inspiration for creating experiences in the moments before our
customers realize they need them. And months and years before our
competitors realize the same thing.
20
15
HEALTHTRENDS

Innovation From Insiders
Patient 1’s and 0’s
Carrot and Stick Healthcare
Remote Attention
Disillusioned Doctors
Wedging Learning In
DIY Diagnosis
The New Competition
We’re following eight trends that show how
healthcare experiences will change.
THE
TRENDS
1.
2.
3.
4.
5.
6.
7.
8.

1.
IN SHORT
Last year it looked like
pharma might be left behind
in the wave of innovation
changing healthcare
experience. Now, more and
more industry leaders are
getting in the game.
1.INNOVATION FROM
INSIDERS
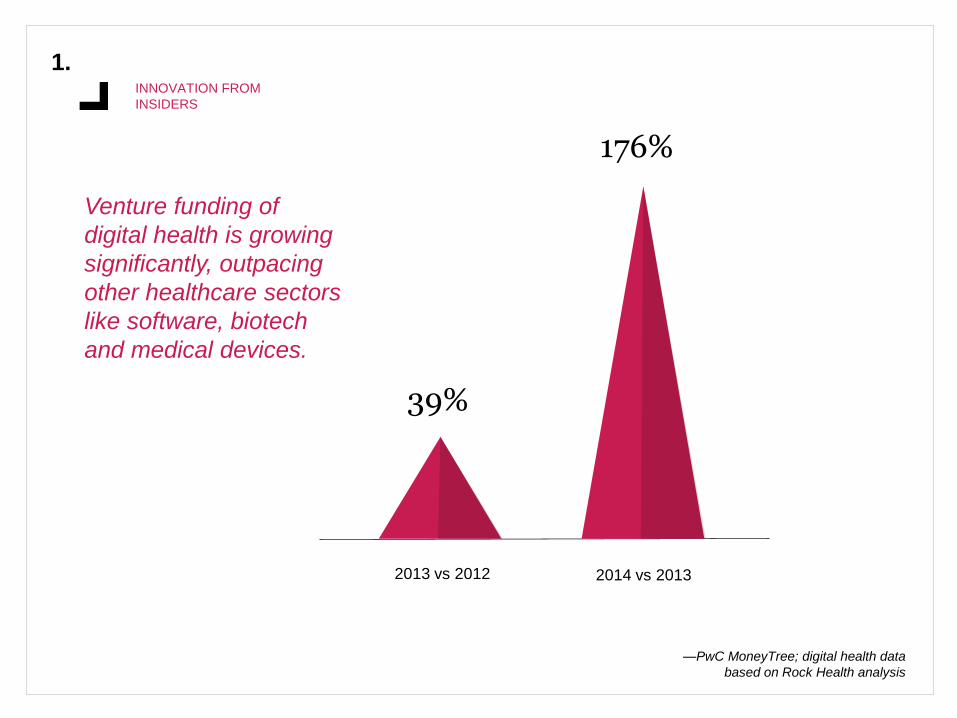
39%
2013 vs 2012
176%
2014 vs 2013
Venture funding of
digital health is growing
significantly, outpacing
other healthcare sectors
like software, biotech
and medical devices.
—PwC MoneyTree; digital health data
based on Rock Health analysis
ACCELERATING EXPERIENCE INNOVATION
1.INNOVATION FROM
INSIDERS
The industry that has long invested in early biotech innovation is now in the market for early
experience innovation. In 2014, Abbott, Boehringer Ingelheim, Genentech, and GE
partnered with Rock Health, a leading funder of healthcare technology startups.
In Germany, Bayer went even farther, evolving their Grants4Apps crowdsourcing initiative
into a true digital health accelerator. Each of five startups will receive 50,000€ and 3.5
months in-house at Bayer for less than a 10% loss in equity. The accelerator’s first
investments included wearable health sensors, a smart pill bottle, and home monitoring
systems.
—VentureBeat, 2014
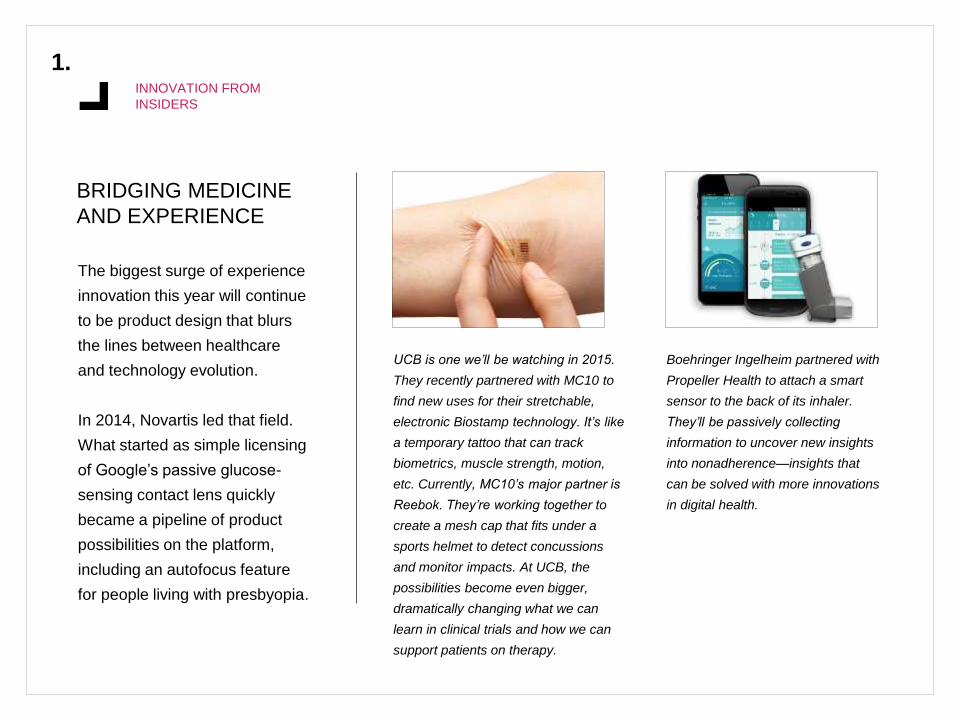
BRIDGING MEDICINE
AND EXPERIENCE
1.INNOVATION FROM
INSIDERS
The biggest surge of experience
innovation this year will continue
to be product design that blurs
the lines between healthcare
and technology evolution.
In 2014, Novartis led that field.
What started as simple licensing
of Google’s passive glucose-
sensing contact lens quickly
became a pipeline of product
possibilities on the platform,
including an autofocus feature
for people living with presbyopia.
UCB is one we’ll be watching in 2015.
They recently partnered with MC10 to
find new uses for their stretchable,
electronic Biostamp technology. It’s like
a temporary tattoo that can track
biometrics, muscle strength, motion,
etc. Currently, MC10’s major partner is
Reebok. They’re working together to
create a mesh cap that fits under a
sports helmet to detect concussions
and monitor impacts. At UCB, the
possibilities become even bigger,
dramatically changing what we can
learn in clinical trials and how we can
support patients on therapy.
Boehringer Ingelheim partnered with
Propeller Health to attach a smart
sensor to the back of its inhaler.
They’ll be passively collecting
information to uncover new insights
into nonadherence—insights that
can be solved with more innovations
in digital health.

(FINALLY) CO-CREATING
WITH OUR CUSTOMERS
1.INNOVATION FROM
INSIDERS
In 2015, we predict market research
budgets will start to decline as co-
creation becomes more and more
central to how pharma creates new
experiences.
Genentech was one of the biggest first
movers, working actively with patient
communities from PatientsLikeMe to
Crohnology to MediGuard to improve
their clinical trials.
Sanofi has a really compelling program for nurses that is
focused on listening to how its customers solve their own
challenges. The Connecting Nurses website has brought
together 14 million nurses from over 130 countries to share
their ideas on how to bridge the gaps in healthcare and
resources that happen around the world.
We have a new, intriguing opportunity to listen to those
customers with the latest Rx rating and review site, which
launched in mid-2014. Wired editor Thomas Goetz created
the site called Iodine to crowdsource effectiveness data on
drugs and guide consumers about drug purchasing decisions.

IN SHORT
Today’s doctor-patient relationships include emails,
text, electronic medical records, website portals,
and, oh yeah, the occasional conversation.
“My impressions from
speaking to friends who
have been patients is that
nowadays they rarely get
the doctor’s undivided
attention because of
doctor focus on the
computer.”
—Dr. Ken Grauer,
a family practitioner
2.
2.PATIENT 1’S
AND 0’S
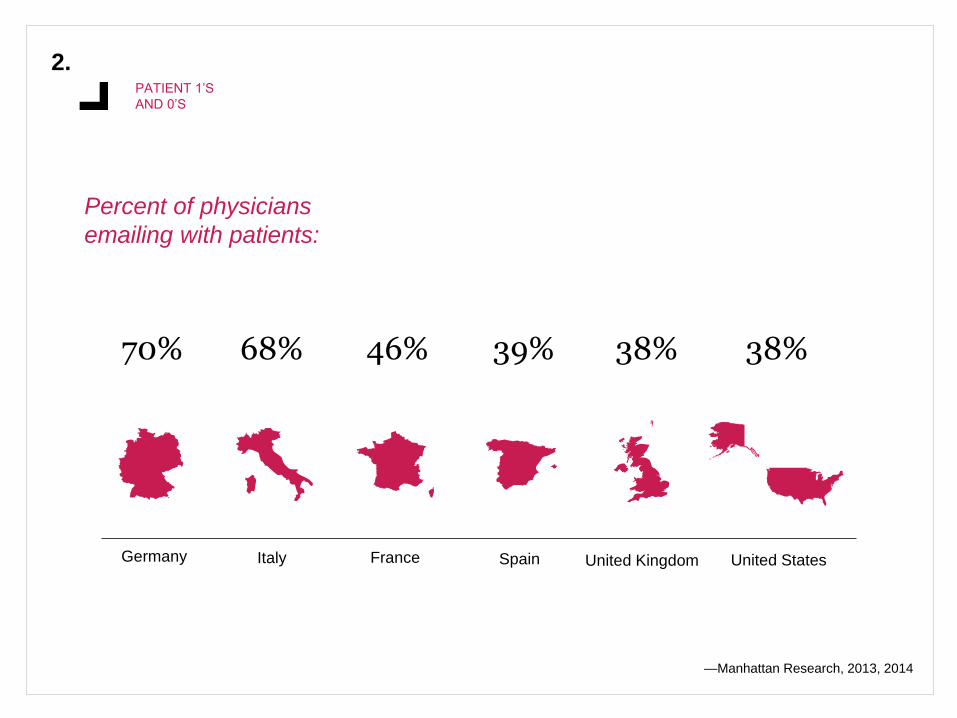
Italy France Spain United Kingdom United StatesGermany
70% 68% 46% 39% 38% 38%
Percent of physicians
emailing with patients:
—Manhattan Research, 2013, 2014

THE DOCTOR WILL SEE YOU IN YOUR INBOX NOW
2.PATIENT 1’S
AND 0’S
It turns out not every interaction with your doctor
requires a paper gown. More and more physicians
are connecting with their patients pre- and post-visit
via email, text message, and secure portal.
No surprise, patients prefer it. In fact, a recent
survey by Catalyst Healthcare found that 93% of
adults prefer to go to a doctor who offers email
communication. Many would even pay more for it:
25% said they would still prefer a doctor that uses
email communication even if there was a $25 fee per
episode.
Dr. Joseph C. Kvedar, a dermatologist and founder
of the Center for Connected Health, a Harvard-
affiliated organization that aims to move healthcare
from the hospital and doctor’s office into the day-to-
day lives of people who need help, explains that
email improves efficiency for doctors and removes
the frustration of phone tag. “Making myself available
via email gives my patients a sense of direct access
to me,” he said. It sends a message that I care and
that I’m available to answer questions in a timely
manner. It builds a bond between us that has
tangible benefits for my patients’ health.”
In a recent survey from Catalyst Healthcare
found that 93% of adults prefer to go to a
doctor that offers email communication.
93%

2.PATIENT 1’S
AND 0’S
A recent study from Kantar Media found that nurse
practitioners are even more likely than doctors to
reach out to their patients in the inbox.
These interactions are truly incremental, supportive
healthcare. In a retrospective study of 2,357 primary
care patients who connected with their doctors
through an online patient portal, the Mayo Clinic
found that there was no significant change in the
frequency of office visits.
In large networks, many of these personal messages
go through portals. Kaiser Permanente has one of
the largest. 4 million of its 9.1 million member
network use Kaiser’s online health management
platform, called My Health Manager. According to
their annual report, 34.4 million lab test results were
viewed online, 14.7 million secure emails were sent,
3.6 million online appointment requests were made,
and 14.8 million online prescriptions were refilled.
But Kaiser expects the platform to do more than
improve communications. They’re after improving
outcomes, too. Of the members who used the
lifestyle features of the portal 56% said they lost
weight and 58% said that they quit smoking.
Insomniacs even reporting increasing their nightly
sleep by 32 minutes on average.
Lost Weight
56%
Quit Smoking
58%
Of the members who used the
lifestyle features of the Kaiser
portal, 56% said they lost
weight and 58% said they quit
smoking.

2.PATIENT 1’S
AND 0’S
"Aspects of current EHRs that were particularly
common sources of dissatisfaction included poor
usability, time-consuming data entry, interference with
face-to-face patient care, inefficient and less fulfilling
work content, inability to exchange health information,
and degradation of clinical documentation."
—RAND Corporation for the American Medical Association, 2013

A NEW SCREEN, A NEW BARRIER
2.PATIENT 1’S
AND 0’S
Electronic health records may increase the long view
that doctors have into their patients’ health, but they
can really decrease the short view across the exam
room. Physicians and patients alike report that the
computers and tablets used to operate EHR systems
create a new barrier between doctor and patient.
Many, including Kevin R. Campbell, a cardiac
electrophysiologist who blogs as KevinMD, worry
that the new focus on data input will interrupt the
doctor-patient relationship. “We must continue to
practice the art of medicine, which requires that we
actually talk and listen to our patients,” Campbell
said. “We must not forget the value of interacting
with patients, looking them in the eye, and providing
them undivided attention. Computers, laptops, and
iPads in exam rooms foster distractions.”
But a new role could change all of that.
A growing number of physicians are hiring scribes to
do the data entry for them. Those scribes team up
with the physician throughout the day—seeing
patients, suggesting which codes to use, sending
electronic prescriptions to the patient’s pharmacy on
the doctor’s behalf, and generating referral letters to
specialists.
The impact is positive for both sides of the exam.
Patient satisfaction scores increase, physicians see
an average of one additional patient per hour, and all
the charts are completed by the end of the day
(which means no homework).
—Medscape, 2014

THE TEXT RX
2.PATIENT 1’S
AND 0’S
One of the longest-running and most
well-known health text initiatives is the
Text4Baby program created by a public-
private partnership that includes
Johnson & Johnson, the National
Healthy Mothers, the Healthy Babies
Coalition, and others. Women can sign
up for the service by texting BABY (or
BEBE for Spanish) to 511411. Then they
receive text messages, timed to their
due date, with helpful tips that educate
them about their pregnancy and getting
ready for the new baby.

2.PATIENT 1’S
AND 0’S
Like many other healthcare text programs, the short messages showed an
impact. And, they broke through to underserved communities:
82% learned about
medical warning signs
they did not know.
82% 65%
65% reported
they talked to
their doctor about
a topic they read
on a Text4Baby
message.
Text4Baby moms
were 3x more
likely to believe
that they were
prepared to be
new mothers
compared to
nonusers.
A higher percentage of
Text4baby participants live in
zip codes with the highest
levels of poverty compared to
the overall US distribution.
Nearly half reported their
household income was
$16,000 or less.

2.PATIENT 1’S
AND 0’S
Teams at practices and hospitals, like the Montefiore Medical
Center, are using texting to support patient relationships. An
interactive text message-based care management system at
Montefiore was able to create a 40% improvement in
appointment adherence and modest improvement in
medication and care plan adherence.
They extended the Sense Health platform to pre-scripted but
customizable messages that busy Medicaid care managers
could send to patients to make them feel like they were getting
more of the individual attention they wanted.
—California State University San Marcos National Latino
Research Center survey, 2013
Sense Health, 2014
IT’S NOT JUST YOUNG MOTHERS WHO ARE
BENEFITING FROM SMS SUPPORT. 40%
Montefiore’s text message system
created a 40% improvement in
appointment adherence

3.
IN SHORT
Financial incentives changed
how doctors practice medicine.
Now brands from insurers to
retail are betting they can use
them to shift something even
bigger: everyday human
behavior.
3.CARROT AND STICK
HEALTHCARE
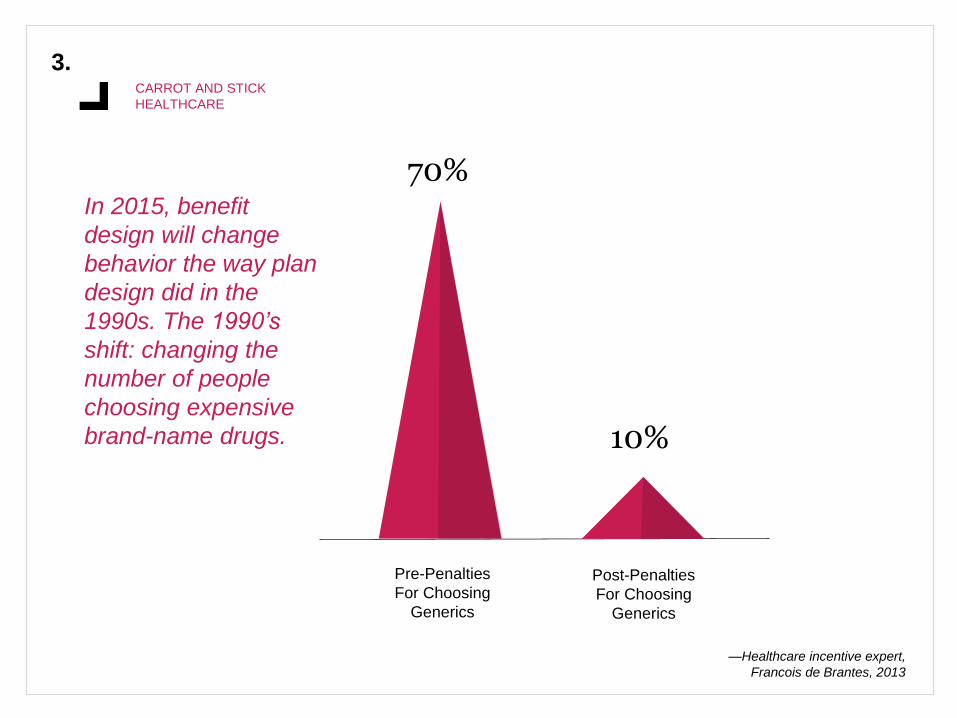
70%
Pre-Penalties
For Choosing
Generics
10%
Post-Penalties
For Choosing
Generics
In 2015, benefit
design will change
behavior the way plan
design did in the
1990s. The 1990’s
shift: changing the
number of people
choosing expensive
brand-name drugs.
—Healthcare incentive expert,
Francois de Brantes, 2013

THE BIGGEST LEVER IN HEALTHCARE
Governments, payers, and employers are using both
financial rewards and penalties to try to encourage
healthier behaviors. At Cigna, that means engaging 14
million members in a digital health coaching program
that offers mobile tools, social media engagement,
gamification, and rewards. At Pennsylvania State
University, it’s a $100 monthly surcharge for employees
who don’t complete a biometric screening and an online
wellness profile. One Midwestern hospital chain even
announced it would deduct money from employees’
paychecks for unhealthy behavior, such as being
overweight.
—Partnership to Fight Chronic Disease, 2014
Treating people
with chronic
conditions
accounts for 84%
of healthcare
costs.
84%
3.CARROT AND STICK
HEALTHCARE
CHANGING ROLE OF RETAIL
3.CARROT AND STICK
HEALTHCARE
One unexpected location for these new
rewarding programs is the local drug
store. Those stores increasingly want to
be seen as a healthcare destination. That
means they’re evolving their “minute
clinics” designed to deliver fast-pass
healthcare into full primary care suites
offering everything from pain management
clinics in the UK to chronic disease care in
the US.
And, they’re changing their rewards to
match. What were once simple savings
cards that rewarded shoppers with
coupons and discounts for their shopping
behavior are now delivering rewards
based on shoppers’ health behaviors. If
you walk those aisles enough, you might
even get a step-based reward in store!
FAT TAX OR SKINNY SPIF?
3.CARROT AND STICK
HEALTHCARE
The much discussed question is: Which one works
better? How these incentives are framed—as
benefits for healthy-weight people or penalties for
overweight people—makes a big difference.
Rewards become less effective over time, but
penalties can be seen as stigmatizing and punishing,
making it even harder for people to make a healthy
change.
While people prefer the carrot design, the sticks do
seem to have an impact. Researchers from the
University of Michigan Health System found that
when faced with having to pay up to 20% more for
health insurance or do more exercise, most of the
enrollees gradually met their fitness goal of walking
5,000 steps per day through an Internet-tracked
walking program.
Another approach may be reaching across industries
to punish food instead of people. A growing number
of European countries, including Denmark and
France, have already imposed a tax on unhealthy
food and drinks. A tax of at least 20% placed on
sugar-sweetened drinks could drop obesity rates by
3.5% and prevent 2,700 heart-related deaths each
year, according to the study.

3.CARROT AND STICK
HEALTHCARE
-3.5% +2,700
A recent study found that a tax of at least 20% placed on
sugar-sweetened drinks could drop obesity rates by 3.5%
and prevent 2,700 heart-related deaths each year.
—Association of Psychological Science, 2013
—Behavioral Translational Medicine, 2013
—British Medical Journal, 2012

4.
IN SHORT
For years, patients have complained that their medical
interactions were rushed and impersonal. Today they’re
finding the kind of attention they want at home from a
growing number of remote and telesupport services.

4.REMOTE
ATTENTION
5.7M
2014
The number of doctor-patient video
consults in the US will nearly triple over
the next year.
2015 2018
16M
130M

4.REMOTE
ATTENTION
FILLING THE GAPS IN MODERN MEDICINE
The eHealth Stakeholder Group in Europe has been one of many to clarify the need for
new kinds of healthcare interactions. Their “Widespread Deployment of Telemedicine
Services in Europe” report pointed to three shifts creating new gaps:
More people living
with (multiple)
chronic conditions,
often starting at a
younger age
Growing elderly
population,
supported by fewer
resources paid for
by the shrinking
tax base
Not enough
healthcare
workers (the total
number is actually
falling in
European states)
Urgent need for
more efficient,
impactful
healthcare
Beyond the demographic shifts, there are real experience gaps in medicine, ones that leave
patients feeling disconnected and unready to manage their own care.
+ + =

4.REMOTE
ATTENTION
46%
Primary
Care
Urgent
Care
Nothing
35%
7%
ER
12%
Video Visits Are Replacing
Traditional Healthcare“Doctor On Demand” users were
asked what services they would
have used if they didn’t have
access to the DOD app.

4.REMOTE
ATTENTION
FACE-TO-FACE VIDEO MEDICINE
Nearly one million US families used video
consultations with physicians last year. That number
is expected to explode in the next few years.
The consumer preference for video connections with
doctors over phone calls is staggering. American
Well, one of the leading providers of telehealth,
reported that 94% of its customers chose video over
telephone. This isn’t a trend limited to young families:
American Well’s core customer base includes the US
Department of Veterans Affairs, Rite Aid, United
Healthcare, WellPoint and various Blues plans.
Mobile may have been the tipping point for the
switch. A quick click of a camera phone is infinitely
easier to figure out than installing a webcam ever
was. In that same report, American Well calculated
that 60% of its customers used their smartphone or
tablet for their video visits.
The overall reach of telehealth has grown
substantially. In 2014, Parks Associates reported that
42% of broadband households in the United States
had used some type of online healthcare
communications and that many had used it multiple
times. Gartner believes we’re at a real tipping point,
predicting the global telehealth market will be more
than $27 billion by 2016, tripling in growth since 2010.
Many urgent care systems and primary care
practices are integrating telehealth into their offerings.
Even Google is making telehealth part of its search
service through Helpouts, its video chat service and
directory. Helpouts makes it easy for all kinds of
experts to offer a live consultation to searchers.
Increasingly, those experts are doctors, like the One
Medical Group.

4.REMOTE
ATTENTION
TAKE-HOME SUPPORT
Health systems around the world are looking to
telemonitoring to support patients—and outcomes—
at home.
Dr. Ed Brown, CEO of the Ontario Telemedicine
Network (OTN), has partnered with regional
healthcare authorities in Ontario to enroll patients
with congestive heart failure and COPD into a remote
monitoring program. “We’re providing them with
remote monitoring tools in their homes and asking
them questions based on clinical guidelines to track
their progress on a daily basis. Then their nurses
track that data,” he explained. The tools include
devices like remote pulse oximeters and blood
pressure cuffs.
The nurses are also trained to be health coaches
who can help patients understand their disease and
set goals to improve their health status. “Nurses are
pretty used to telling people what to do,” Brown said.
“This is different because they’re empowering
patients to set their own goals.”
The program has reduced hospitalization rates by two-
thirds and reduced emergency room visits by 70%.
In the US, the Geisinger Health Plan was able to use
remote monitoring to reduce readmissions by 38% for
congestive heart failure patients and deliver an ROI
of $3.30 on the dollar for the system.
Patients used a Bluetooth-connected weight scale that
included interactive voice surveys about shortness of
breath, swelling, appetite and prescription medication
management designed to detect acute events before
they happen. Weight data and survey answers were
transmitted to the patients’ care team, allowing them to
respond to warning signs.
66%Ontario Telemedicine
Network’s remote monitoring
program has reduced
hospitalization rates by 66%.
—PwC, 2013
—AMC Health, 2014
4.REMOTE
ATTENTION
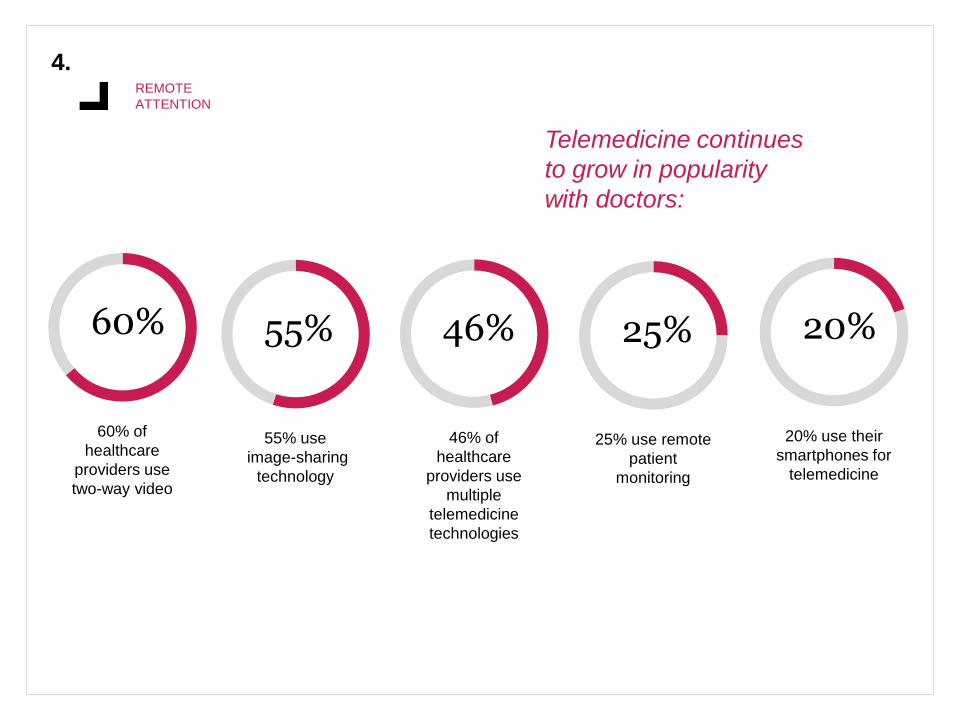
Telemedicine continues
to grow in popularity
with doctors:
60%
60% of
healthcare
providers use
two-way video
55%
55% use
image-sharing
technology
46%
46% of
healthcare
providers use
multiple
telemedicine
technologies
25%
25% use remote
patient
monitoring
20%
20% use their
smartphones for
telemedicine
5.
IN SHORT
Who wouldn’t want to be a doctor? Most
doctors. This once aspirational
profession is now shouldered with
growing levels of unhappiness,
disillusionment and burnout.
“The rate of severe diabetes complications
in patients of doctors who rate high on a
standard empathy scale is 40% lower than
in patients with low-empathy doctors.”
—”What Doctors Feel,” Dr. Danielle Ofri, MD

5.DISILLUSIONED
DOCTORS
Cardiologist Sandeep Jauhar says
today’s physicians see themselves not
as the “pillars of any community” but as
“technicians on an assembly line,” or
“pawns in a money-making game for
hospital administrators.”
—”Doctored,” Dr. Sandeep Jauhar, MD

5.DISILLUSIONED
DOCTORS
THE EMPLOYEE PHYSICIAN
Remember the doctors many of today’s practicing
physicians grew up with? It was a golden age of
medicine. They were heroes. Life expectancy was
increasing. There were huge firsts, like the heart-lung
bypass. And doctors generally set their own course—
customizing their practice, fees and hours around
their communities and the lives they wanted to lead.
Then things started to change.
Questions about fraud and waste sparked new rules
and bureaucracies designed to make medicine less
expensive and more uniform. Governments have
issued more mandates for record keeping and
reporting. Payers have set fees lower and lower. The
only way to keep up is to join up.
Doctors tend to have access to more support and get
reimbursed at a higher rate when they’re in a network
or physician group. So, many have left solo and small
practices and moved into big ones.
A recent survey by healthcare staffing firm Jackson
Healthcare found that not only are hospital
acquisitions of physician practices up (52% of
hospitals plan to acquire practices in 2013 compared
with 44% in 2012), the majority of those deals—70%,
in fact—are initiated by doctors looking to sell.
Many of these new mega employers set factory-like
goals for their employee physicians, like seeing a set
number of patients per day.
70%70% of acquisitions of
physician practices are
inititated by doctors
looking to sell.

5.DISILLUSIONED
DOCTORS
MODERN MEDICAL CONVEYOR BELT
Lots of new medical professionals are entering the
practice, and fewer and fewer of them are MDs. Instead
a growing number of physician assistants and nurse
practitioners are helping those MDs make the medical
home model real. They’re each working to the top of
their skill sets and then handing a patient off when she
needs even more expertise or speciality care.
In “The Physician Assistant Will See You,” Barbara
Moran looked into this in-practice referral system, ‘Like
it or not, medicine is now a team sport,’ observes Dr.
Reid B. Blackwelder, president of the American
Academy of Family Physicians. As his practice moves
to team-based care, he may delegate more well-child
visits to P.A.s or nurse practitioners. He enjoys seeing
his healthy patients, he said, ‘but the paperwork takes
a lot of time — as a physician, my time may be better
spent with a patient who is critically ill.’ And he can still
keep his relationship with the healthier children, he
said, ‘by a quick visit at the end.’”
That balancing act is tricky across specialties. In a
recent essay, “Doctors Tell All—and It’s Bad,” The
Atlantic’s Meghan O’Rourke wrote, “Studies estimate
that today’s doctors and ‘hospitalists’—medical
practitioners who do most of their work in hospitals—
spend just 12 to 17 percent of their day with patients.
The rest of the time is devoted to processing forms,
reviewing lab results, maintaining electronic medical
records, dealing with other staff.”
For patients, what’s missing is missed. Atul
Gawande, a surgeon and professor at Harvard
Medical School, explains that how patients feel about
their medical interactions really does influence the
efficacy of the care they receive and that doctors’
emotions about their work in turn influence the quality
of the care they provide. The patient-doctor
relationship is still the heart of medicine.
5.DISILLUSIONED
DOCTORS
"I wouldn't do it again, and it has nothing to do with the money. I get too little
respect from patients, physician colleagues, and administrators, despite good
clinical judgment, hard work, and compassion for my patients. Working up patients
in the ER these days involves shotgunning multiple unnecessary tests (everybody
gets a CT!) despite the fact that we know they don't need them, and being aware
of the wastefulness of it all really sucks the love out of what you do. I feel like a
pawn in a moneymaking game for hospital administrators. There are so many
other ways I could have made my living and been more fulfilled. The sad part is we
chose medicine because we thought it was worthwhile and noble, but from what I
have seen in my short career, it is a charade."
—Doctor on Sermo

5.DISILLUSIONED
DOCTORS
12-17%
It’s estimated that medical
practitioners who do most of
their work in hospitals spend
just 12 to 17% of their day
with patients.
78%
78% of 13,500 physicians
surveyed are “somewhat
pessimistic or very
pessimistic about the future
of the medical profession.”
84%
84% of physicians agree
that the medical profession
is in decline.

5.DISILLUSIONED
DOCTORS
JUST SICK OF IT
Here’s the big number: 78% of 13,500 physicians
surveyed are “somewhat pessimistic or very pessimistic
about the future of the medical profession.” And, 84% of
physicians agree that the medical profession is in
decline.
In “A Doctor’s Declaration of Independence,”
Dr. Daniel Craviotto wrote about the daily struggle: “I
don’t know about other physicians but I am tired—tired
of the mandates, tired of outside interference, tired of
anything that unnecessarily interferes with the way I
practice medicine. No other profession would put up
with this kind of scrutiny and coercion from outside
forces. The legal profession would not. The labor
unions would not. We as physicians continue to plod
along and take care of our patients while those on the
outside continue to intrude and interfere with the
practice of medicine.”
Almost 50% of doctors report symptoms of burnout —
emotional exhaustion, low sense of accomplishment,
detachment. In “Burnout and Satisfaction With Work-
Life Balance Among US Physicians Relative to the
General US Population,” the authors found that
“Burnout is more common among physicians than
among other US workers. Physicians in specialties at
the front line of care access seem to be at greatest
risk.”

6.
IN SHORT
The world of medicine is changing faster
than ever. Busy healthcare
professionals are left to try to find a way
to fit it all in.
The moments they do make
for new education are wedged
in between appointments or
surrounded by distraction.
6.WEDGING
LEARNING IN
CME ON THE COUCH
Our collaborators at Palio-Ignite created an interesting
healthcare professional layer over some recent data
from Google about when people use their various
devices. The new curves show traffic to healthcare
professional websites by device and time of day. Look
at that big spike in tablet usage right around 8PM in the
chart above.
It coincides with how we’re increasingly seeing those
doctors use different screens for different behaviors.
But it also shows the new environment doctors are
learning in. They likely are browsing healthcare content,
but in what context? At that hour, for many, it’s
potentially surrounded by the welcome distraction of
family life. (Perhaps Frozen is playing for the 30th time
in the background?) Not exactly study hall.
It’s a behavior we originally called multitasking, but
today that always-on, anywhere, anytime behavior has
left our culture in a permanent state of mild (to major)
distraction. The challenge is even greater in medicine,
where new screens, new tools, new requirements, and
the fast growth of information are leaving doctors
overloaded and only partially connected.

6.WEDGING
LEARNING IN
Web traffic to HCP sites
for digital devices

6.WEDGING
LEARNING IN
THE RESEARCH MOUNTAIN
These multitasking healthcare providers are up against pretty big odds. It
turns out new medical knowledge is already doubling every three years
and is projected to double every 73 days by 2020.
That’s a lot of information!
EHR and genomic data are amplifying the growth of data sets, publications
and possibilities. Just 10 years after the completion of the Human Genome
Project, 2014 brought the $1,000 genome. That cost decreased five orders
of magnitude in 10 years. That’s not linear, it’s logarithmic. In the next year
we’ll produce more genomic data than ever before in human history. (No
pressure.) And, that’s just one kind of medical information—so many more
are exploding, too.
6.WEDGING
LEARNING IN
REAL QUICK: ABOUT THIS RX
Let’s start with the biggest number: 10 minutes. When
Verilogue reviewed 70,000 exam room conversations, it
found that’s how long the average physician spends
with a patient. That 10 minutes is largely dominated by
the physician. In fact, 64% of the conversation is
physician-led; 33% is patient-led—with the small
balance owned by a caregiver or partner. How much of
it is dedicated to the new prescription? 99 seconds—or
13.7% of the conversation. Previous studies have
pegged that Rx discussion time as even shorter.
Think how many months and years we spend
perfecting the messages, the Q&A, the story, all to have
it boiled down into a 99-second Rush to the Rx. Beyond
the minor marketing injustice, there are real reasons to
wonder about the efficacy of those conversations. Our
collaborator George Van Antwerp recently reminded us
of the biggest one: the leaky bucket of good intentions.
The entire slippery slope of adherence starts with that
conversation between doctor and patient. Steve
Wilkins, MPH, one of the authors of the Verilogue study,
says nonadherence is “often a rational response on the
patient’s part when faced with a recommendation to do
something they don’t agree with—namely take a
medication.” He says 50% of patients disagree at one
time or another with a doctor regarding the diagnosis,
severity of a condition or particular treatment.
—2013 Physician-Patient Communications Benchmark from Verilogue and Steve Wilkins, MPH, of Mind the Gap and Smart Health Messaging
—”Pharmacies: Improving Health, Reducing Costs,” National Association of Chain Drugstores, 2010 (based on IMS data)

6.WEDGING
LEARNING IN
For every 100
prescriptions
written
50-70
go to a
pharmacy
48-66 come
out of the
pharmacy
25-30 are
taken
properly
15-20
are refilled as
prescribed
6.WEDGING
LEARNING IN
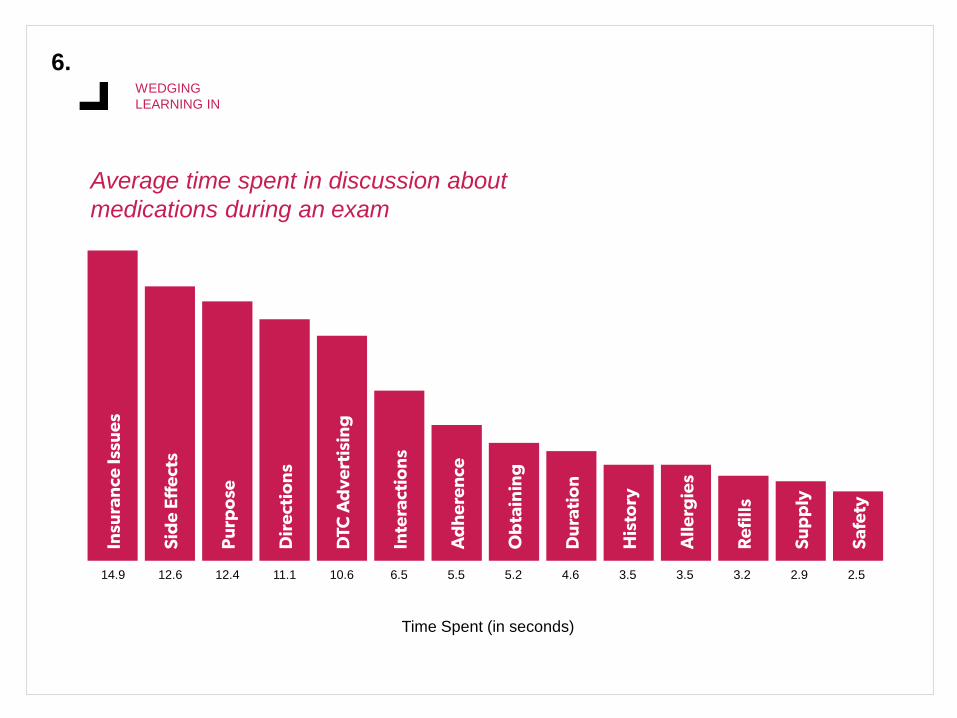
Average time spent in discussion about
medications during an exam
14.9 12.6 12.4 11.1 10.6 6.5 5.5 5.2 4.6 3.5 3.5 3.2 2.9 2.5
Time Spent (in seconds)

7.
IN SHORT
WebMD was training wheels.
This new era of at-home
diagnosis and health
management will make experts
of us all.

7.DIY
DIAGNOSIS
69%
69% of physicians said
patients should use tech tools
to help them form a diagnosis.
84%
84% of patients said
they should be able to use
the self-diagnosis tools.
—WebMD/Medscape, 2014

7.DIY
DIAGNOSIS
BRINGING THE LAB HOME
Today you can order an at-home self-screening
kit to test for everything from bowel disease to
meningitis to cholesterol. New entrants go even
further, letting users look at their own biology
on a molecular level and basically tinker with
activity, nutrition, sleep and more until they get
the consistent results they want. It’s more
health hacking then quantified tracking.
One of our favorites is Cue. It’s a small,
modular hardware system that works with iOS
to let users create a simple home diagnostics
lab. When it launches in early 2015, users will
be able to collect tiny samples of their own
saliva, blood or nasal fluid to test for five
distinct molecular indicators related to
inflammation, vitamin D, fertility, influenza and
testosterone. Each metric has a different
marker that, when measured and tracked, can
be used to discover trends, monitor progress
and help users gain realtime insight into their
bodies. Those numbers correlate with some of
the most basic questions people have about
health: Why don’t I have more energy? Is it a
cold or really the flu? What’s the best way to
recover from an injury or live your best life with
chronic disease?

7.DIY
DIAGNOSIS
Like other trackers, Cue pulls the data into great dashboards that let users compete against
themselves or collaborate with friends and strangers.

7.DIY
DIAGNOSIS
SHIFT IN RESPONSIBILITY
For people who believe that
healthcare is expensive and difficult
to use, DIY tools are a way to take
control back. They replace “What
could it be?” conversations in
healthcare social media with the
wisdom of science. Now a sensor on
your mattress can diagnose a sleep
issue. A blood pressure cuff
connected to your iPhone cannot
only spot a problem, it can identify its
triggers.
We predict this new at-home
medicine will be particularly
interesting to adult Millennials. Our
recent “The Worried Well” report,
published with Allidura and Harris
Poll, pointed to a strong desire
among that generation to take
healthcare into their own hands: “It
turns out that our hulking healthcare
system–with its confusing cost
structures and white-coated experts–
isn’t what Millennials are pursuing,
even as they express worry about
their health. For them the question
seems to be, not, who can help me
but what can help me. They’re
mashing up food trends with high-
profile cleanses and intriguing new
exercise offers to proactively live
healthier lives—and keep the doctor
away. In fact, 71% believe they’re
already doing everything they can to
maintain a healthy lifestyle. These
efforts show some indication that
they may be attempting to avoid
traditional healthcare altogether.”
Millennial Mindset: “The Worried Well”
allidura.com/millennialhealth

7.DIY
DIAGNOSIS
THE NEW PRIVACY QUESTION
People think the great debate of this decade is
about privacy—what we want other people and
companies to know about us. We disagree. We
think it’s about transparency—how much we’re
actually comfortable knowing about ourselves.
This new generation of products from both startups
and category leaders are going to push all of us to
answer this simple question: Do you really want to
know?
The question becomes even more difficult when it’s
connected to “real” healthcare. Both healthcare and
technology experts are pointing to Apple’s HealthKit
as the catalyst that finally brings patient-generated
data into the healthcare ecosystem—if patients are
really ready to share it there.
Apple’s HealthKit Platform

8.
IN SHORT
We’re just a few years away from
digital therapies taking on
traditional medicines on their own
turf: clinical trials, formularies, and
prescription pads.
8.THE NEW
COMPETITION
—WebMD/Medscape, 2014
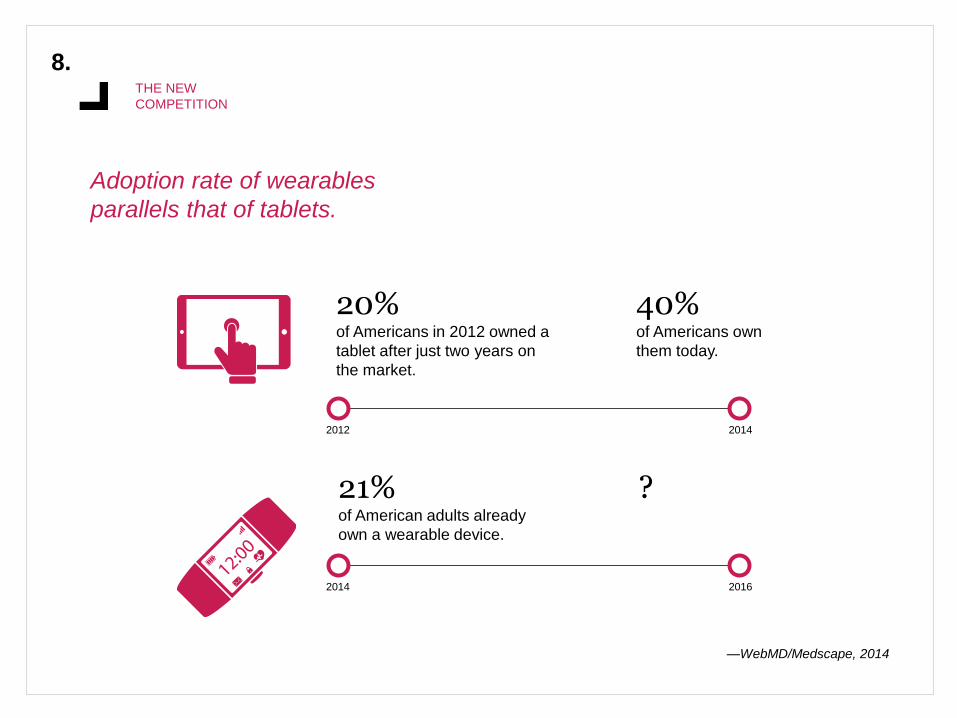
Adoption rate of wearables
parallels that of tablets.
20%of Americans in 2012 owned a
tablet after just two years on
the market.
40%of Americans own
them today.
21%of American adults already
own a wearable device.
?
2012 2014
2014 2016
8.THE NEW
COMPETITION
BOUNCING BACK FROM THE
BACKLASH
In 2013, we were all calling wearables the next big
thing in healthcare. Then in 2014, Nike fired the
majority of its FuelBand team. The New York Times
called wearables “digital snake oil.”
A lot of us chucked out Fitbits.
But, investors haven’t backed off. They think the first
generation just wasn’t good enough. The new
wearables will be more clinically valid, smarter,
more convenient, and more relevant to our lives.
Nike’s Fuel Band

8.THE NEW
COMPETITION
THAT’S JUST THE BEGINNING
Real digital therapies are just beginning to
take shape. In three years, the investment in
digital therapies has experienced 20x
growth. These are behavioral software tools
that are backed by published clinical data.
Real-world outcomes. This isn’t pill+ to
improve the bottom line, it is the bottom line.
Within a few years, these solutions will be
listed on formulary next to pills.
Investment in digital
therapies has experienced
20x growth in three years.
20X
8.THE NEW
COMPETITION
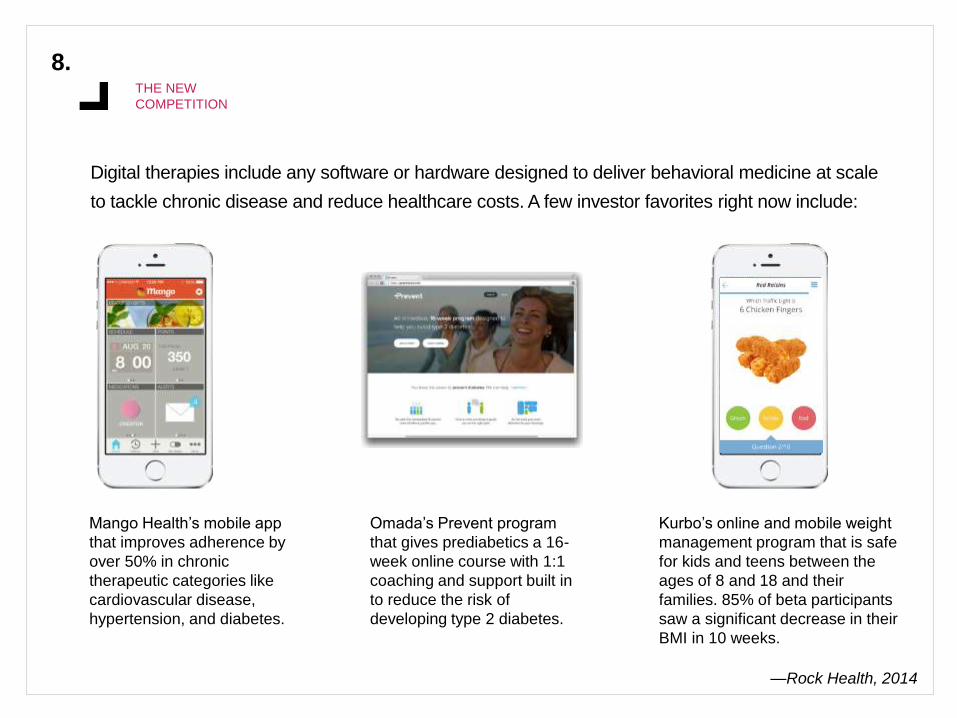
Digital therapies include any software or hardware designed to deliver behavioral medicine at scale
to tackle chronic disease and reduce healthcare costs. A few investor favorites right now include:
Mango Health’s mobile app
that improves adherence by
over 50% in chronic
therapeutic categories like
cardiovascular disease,
hypertension, and diabetes.
Omada’s Prevent program
that gives prediabetics a 16-
week online course with 1:1
coaching and support built in
to reduce the risk of
developing type 2 diabetes.
Kurbo’s online and mobile weight
management program that is safe
for kids and teens between the
ages of 8 and 18 and their
families. 85% of beta participants
saw a significant decrease in their
BMI in 10 weeks.
—Rock Health, 2014

8.THE NEW
COMPETITION
A SPOON MIGHT POINT THE WAY
This year, Google bought a spoon. One from Lift Labs,
a company that is developing smart utensils for people
with Parkinson’s and essential tremor. It competes
head-on with medicines that treat the symptoms of
those diseases, but does it with absolutely no side
effects. Instead, it uses active cancellation (which is
currently in noise-cancelling headphones) to stabilize
larger-scale motion. They’re also looking at solutions
for drinking and grooming. We might not hear more for
a while, though. After the acquisition, the team went
into Google’s notoriously secretive labs.
Governments and payers are looking carefully at the
potential of these new solutions. Long a first mover on
digital health, the US Department of Veterans Affairs
changed its contracting template in such a way that
enables it to soon begin reimbursing its doctors for
clinical grade activity trackers in some limited
circumstances.
They’re focused on a number of highly specific metrics
such as stance and swing time, gait symmetry,
dynamic function, cadence and cadence variability,
step count, numbers of steps per time interval, peak
performance, and functional level assessment.
Google bought Lift Labs, a company developing smart utensil
20
15
HEALTHTRENDS
To discuss this report live, request another module, or schedule a
presentation of trends, please contact Leigh Householder at
614-543-6496 or [email protected]


















