2015 ACLS Review - cprclassespa.com · ACLS DRUGS Epinephrine (Bolus) • Hormone naturally...
38
2015 ACLS Review (877) 338-9286 www.CprClassesPA.com Serving PA & NJ
Transcript of 2015 ACLS Review - cprclassespa.com · ACLS DRUGS Epinephrine (Bolus) • Hormone naturally...

2015 ACLS Review
(877)338-9286www.CprClassesPA.comServingPA&NJ

DISCLAIMER• The following information is provided by
the American Heart Association. • Monies collected do not represent income
for the American Heart Association.• Please review and study your American
Heart Association ACLS Manual before attempting to complete the AHA ACLS
Course.
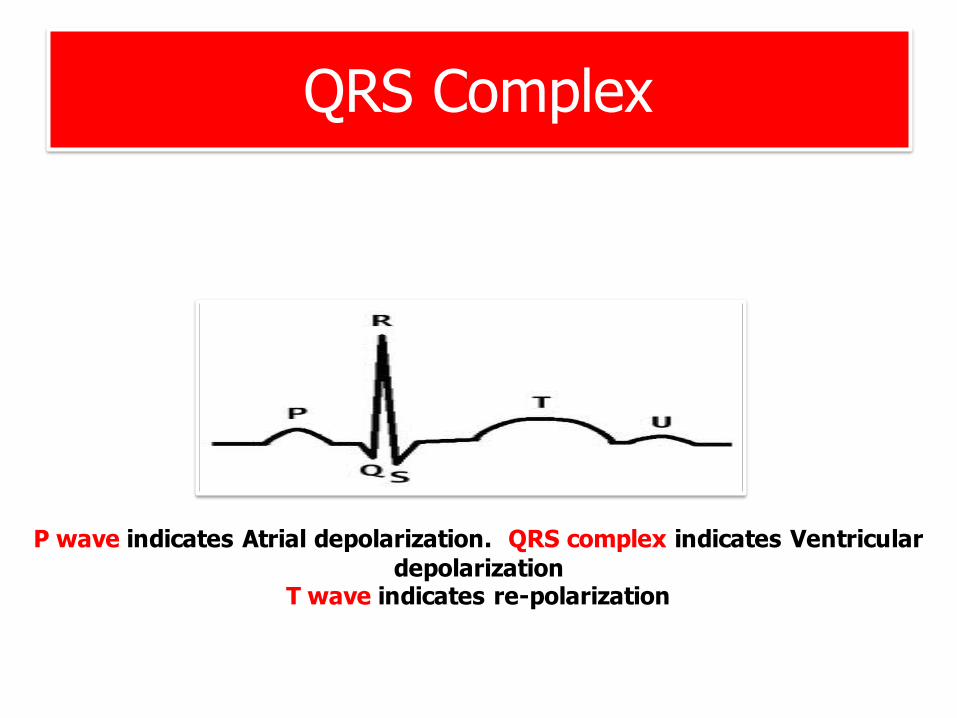
QRS Complex
P wave indicates Atrial depolarization. QRS complex indicates Ventricular depolarization
T wave indicates re-polarization

Rhythm Recognition• Fastorslow?• Regularorirregular?• QRSnarroworwide?• IsthereaPwave?• IsthePwavecloseorfarfromQRS?• IsthePwaveinthesameplace?

Normal Sinus Rhythm

1st Degree Heart Block• Usuallybenign,verycommon• NottreatableinACLSunlesssymptomatic• Notactuallyablock- justadelayinconduction• PRI- >20(4smallboxes)• IftheRs arefarfromPs,thenyouhavea1stDegree

2nd Degree Heart Block, type 1aka “Wenckebach”
• UsuallyIrregular• NottreatableinACLSunlesssymptomatic• PRI- Long,long,longer,DROP- mustbeaWenckebach!

2nd Degree, Type 2 Heart Block• BlockedPwaves/droppedQRSComplexes• IfsomePsdon’thaveQs,thenyouhaveaMobitz 2
• Thisisgettingworse…

3rd Degree Heart Block(Complete Heart Block)
• Malignant• UsuallyBradycardic,Irregular• Won’ttakelong…NEEDTOTREAT!• IfthePsandQsdonotagree,thenyouhavea3rd degree!

Supra Ventricular Tachycardia(SVT)
• Firingsomewhereabove theVentricles• Treatableover150BPMperACLS• RegularandFAST!

Ventricular Tachycardia(V- tach with or w/o Pulses)
• Extremelydangerousarrhythmia• Patientwontlastlong• WideandBizarrepattern,butregular• Shock-ablerhythm(ifnopulsepresent)

Torsades de Pointes• Translatesto:“TwistedoftheSpikes”• DescribedasPolymorphicTachycardia• MaydegeneratetoV-Fibifpersistent• CausedbyHYPOkalemia/HYPOmagnasemia

Ventricular Fibrillation(V-Fib)
• Won’thaveapulse• Fineorcoarse• Shock-ablerhythm• PatientisinCARDIACARRESTatthispoint

Pulseless Electrical Activity (PEA)
• ANY rhythmcanbePEA aslongasitdoesn’thaveaPULSE!
• YOUMUSTCHECKAPULSEWITHEVERYRHYTHM- InaCardiacArrest!

Asystole (Flat line)• HeartnotproducingANYelectricalactivity• NON-ShockableRhythm• PatientisDEAD

Acute M.I. (Where do you see STEMI?)

ACLS DRUGSAtropine
• DerivedfromtheNightshadePlant(deadly)• Dilatespupils,increasesheartrate• Usedtotreatsymptomaticbradycardia• NolongerusedforPEA
DOSE:0.5mgwithamaximumof3.0mg

ACLS DRUGS
Adenosine• Inhibitsneurotransmitters• “Resets”heart• Asystolefor3-5seconds• CausesatransientheartblockintheAVnode• UsedtotreatAsymptomaticSVTover150bpm• NOT forwidecomplexIRREGULARV-Tach
DOSE:6.0mgthen12.0mg

ACLS DRUGSAmiodaroneBolus
• Anti-arrhythmic• WorksontheAtriaandtheVentricles• Ifyoucanshock,useAmiodarone
DOSE:300mgthen150mg.MAX:450mg

ACLS DRUGSEpinephrine(Bolus)
• Hormonenaturallyoccurringinthebody• AffectstheSympatheticNervousSystem• Constrictsbloodvessels,increasesperipheralresistance
• IncreasesHeartRate(InotropiceffectsandChronotropiceffects)(contractilityandrate)
DOSE:1.0mgNOMAXDOSE!

ACLS DRUGSDopamine
• Second-linedrugforsymptomaticbradycardiawhenatropineisnoteffective
• Usedforcardiogenicshockintheabsenceofhypovolemia
Dose:2-20micrograms/kg/mininfusion

ACLS DRUGSEpinephrine(Infusion)
• Second-linedrugforsymptomaticbradycardiawhenatropineisnoteffective.ChooseEPIorDopamine
Dose:2-10micrograms/mininfusion

ACLS DRUGSMagnesiumSulfate
• ForthetreatmentofTorsades
Dose:1-2Grams(SlowPush)

H’s and T’s• Hypovolemia• Hypoxia• HydrogenIons(acidosis)
• Hyper/Hypokalemia• Hypothermia
• Toxins• Tamponade(cardiac)• TensionPneumothorax• Thrombosis(coronary)• Thrombosis(Pulmonary)

CircularAlgorithm

Treatment Modalities per ACLS• V-FIBor(V-TACHw/opulses)aretheonlyshock-ablerhythms.
• 360JMonophasicDefibrillator/200JBi-Phasic• HighQualityCPR100-120BPM• EPI1mg• Amiodarone- 300mg,then150mg(450mgMAX)

SVT• Treatableat150BPM• UseValsalva ManeuverFirst(ThinkBLS)• Stable=Drugs.Adenosine6mg,12mg,done• Unstable=Electricity.SynchronizedCardioversion.(sedatefirst)JouleSettingsdiscussedinclass
• MAKESUREYOUPUSHSYNCHBUTTON!

SVT Algorithm

V-TACH w/PULSES (Regular)• Dangerousarrhythmia- PT.wontlastlong• Stable= UseAdenosine• Unstable=Electricity(Cardioversion)• JouleSettingsdiscussedinclass• Trytosedatefirst.Don’tdelaytreatment.• PT.willusuallybeUNSTABLE!

V-TACH Algorithm

V-Tach (Irregular, Torsades)• Dangerousarrhythmia- PT.wontlastlong• Stable=Adenosine- notindicated.• MagnesiumSulfate• (DEFIBRILLATE-Won’tbeabletosync)

Bradycardias
• Lessthan50-60BPM
• Stable=DONOTAGGRESSIVELYTREAT-watchpatient
• Unstable=(1)Atropine(2)DopamineorEPIDrip(3)Pacing…

Bradycardia Algorithm

Pacing• ApplyD-FibPadsonPt• SetPacerat80BPM*• IncreasemAuntil1pacerspikeprecedesQRS• CheckFemoralArteryforpulsethatmatchesmonitor
• Ifisdoesn’t,increasemAuntilitdoes

PEA (Pulseless Electrical Activity)
• Arhythmthatappearsonamonitortohaveapulse,butdoesnotwhenthepulseischecked
• HighqualityCPR• Epinephrine,1.0mg• NON- SHOCKABLE!• PushEpiAlways

Complete Heart Block (3rd degree)
• TheuseofAtropineisnotindicated• Transcutaneouspacing• Fluids• Oxygen• Cardiologyconsult

Hypothermia Protocol (Targeted Temperature Management)
• PatientMUSTbeIntubatedandComatose• Coolto32-36Celsius• Atleast24hours• OptimizesNeurologicRecovery• MaintainHemodynamics

THE END!
THANKYOU!!!