2 Pattern Recognition in Muscle Misuse Voice Disorders - How to Do It
7
Journal of Voice Vol. 11, No. 1. pp. 108--114 © 1997 Lippincott-Raven Publishers,Philadelphia Pattern Recognition in Muscle Misuse Voice Disorders: How I Do It Murray Morrison Division of Otolaryngology, University of British Columbia, Vancouver Hospital and Health Sciences Centre, Vancouver, B.C., Canada Summary: The diagnosis of the patient with a muscle misuse voice disorder can be a complex process. The dysphonia is usually caused by problems stem- ming from a number of interacting factors that may include habitual vocal technique and postural use, vocal behavior, emotion, manifestations of gas- troesophageal reflux, neuromuscular abnormalities, and associated organic mucosal disease. Sorting out the relative importance of the various factors is the first step towards planning an effective treatment program. This article addresses the difficulties caused by trying to classify dysphonia too rigidly, and presents a strategy for collecting the necessary information in a manner that facilitates the development of effective tools for clinical decision making. For each dysphonic patient, a pattern of causation will emerge in a way that helps the clinician to disentangle the interrelated factors. Key Words: Dys- phonia--Functionai--Spasmodic--Muscle tension--Etiology patterns. Physicians like to classify things. This is reason- able since classification systems are a great aid to diagnosis and treatment in most clinical situations. The treatment plan for a particular cancer is di- rected by the histologic class or by the classification of depth of invasion. Hoarseness, in a similar way, can be etiologically classified into broad groups such as those due to tumors, infection, vocal fold paralysis, and so on, but many voice-disordered pa- tients do not fit into a single diagnosis format very well. For example, if a patient is given the diagnosis of vocal nodules then much of the therapeutic en- ergy is naturally directed at the nodules, possibly to the extent of early excision. Less time may be spent on treating the muscle misuse aspects, behavioral, and emotional factors or associated gastric reflux. In a similar way, these same factors may aggravate the spasmodic voice of the patient with laryngeal Accepted January 3, 1996. Address correspondence and reprint requests to Dr. Murray Morrison, Division of Otolaryngology, University of British Co- lumbia, Vancouver Hospital and Health Sciences Centre, 805 W. 12th Ave., Vancouver, B.C., V5Z IM9, Canada. dystonia, and attending to them may lessen the need for dependence on botulinum toxin. BACKGROUND In the early 1980s, our voice clinic group at the University of British Columbia studied clinical re- lationships in patients with mucosal abnormalities of the vocal folds, such as vocal nodules, and found that many had demonstrable muscle misuses and postural abnormalities, including suprahyoid mus- cle tension, jaw restrictions, and an open posterior glottis with voicing. The open posterior chink was attributed to retained abductor tension in the pos- terior cricoarytenoid muscles during phonation, part of a global hypertonicity of muscle systems in the phonatory apparatus. We felt that vocal nodules developed because extra glottic tension was used for voice production in a manner that added to the shearing forces on the vocal folds. We termed the process "muscle tension dysphonia" and became interested in developing a classification system for this and related vocal dysfunction (1,2). 108
description
muscular
Transcript of 2 Pattern Recognition in Muscle Misuse Voice Disorders - How to Do It

Journal of Voice Vol. 11, No. 1. pp. 108--114 © 1997 Lippincott-Raven Publishers, Philadelphia
Pattern Recognition in Muscle Misuse Voice Disorders: How I Do It
Murray Morrison
Division of Otolaryngology, University of British Columbia, Vancouver Hospital and Health Sciences Centre, Vancouver, B.C., Canada
Summary: The diagnosis of the patient with a muscle misuse voice disorder can be a complex process. The dysphonia is usually caused by problems stem- ming from a number of interacting factors that may include habitual vocal technique and postural use, vocal behavior, emotion, manifestations of gas- troesophageal reflux, neuromuscular abnormalities, and associated organic mucosal disease. Sorting out the relative importance of the various factors is the first step towards planning an effective treatment program. This article addresses the difficulties caused by trying to classify dysphonia too rigidly, and presents a strategy for collecting the necessary information in a manner that facilitates the development of effective tools for clinical decision making. For each dysphonic patient, a pattern of causation will emerge in a way that helps the clinician to disentangle the interrelated factors. Key Words: Dys- phonia--Functionai--Spasmodic--Muscle tension--Etiology patterns.
Physicians like to classify things. This is reason- able since classification systems are a great aid to diagnosis and t reatment in most clinical situations. The treatment plan for a particular cancer is di- rected by the histologic class or by the classification of depth of invasion. Hoarseness, in a similar way, can be etiologically classified into broad groups such as those due to tumors, infection, vocal fold paralysis, and so on, but many voice-disordered pa- tients do not fit into a single diagnosis format very well. For example, if a patient is given the diagnosis of vocal nodules then much of the therapeutic en- ergy is naturally directed at the nodules, possibly to the extent of early excision. Less time may be spent on treating the muscle misuse aspects, behavioral, and emotional factors or associated gastric reflux. In a similar way, these same factors may aggravate the spasmodic voice of the patient with laryngeal
Accepted January 3, 1996. Address correspondence and reprint requests to Dr. Murray
Morrison, Division of Otolaryngology, University of British Co- lumbia, Vancouver Hospital and Health Sciences Centre, 805 W. 12th Ave., Vancouver, B.C., V5Z IM9, Canada.
dystonia, and attending to them may lessen the need for dependence on botulinum toxin.
BACKGROUND
In the early 1980s, our voice clinic group at the University of British Columbia studied clinical re- lationships in patients with mucosal abnormalities of the vocal folds, such as vocal nodules, and found that many had demonstrable muscle misuses and postural abnormalities, including suprahyoid mus- cle tension, jaw restrictions, and an open posterior glottis with voicing. The open posterior chink was attributed to retained abductor tension in the pos- ter ior c r icoary tenoid muscles during phonat ion, part of a global hypertonici ty of muscle systems in the phonatory apparatus. We felt that vocal nodules developed because extra glottic tension was used for voice production in a manner that added to the shearing forces on the vocal folds. We termed the process "muscle tension dysphonia" and became interested in developing a classification system for this and related vocal dysfunction (1,2).
108

MUSCLE MISUSE VOICE DISORDERS 109
We initially "classified" types of muscle tension dysphonia (MTD) as being present without mucosal change (type 1) or with mucosal abnormalities, in- cluding nodules (type 2a), chronic laryngitis (type 2b), and polypoidal degeneration (type 2c). But there were other patients in the clinic who clearly had voice problems related to muscular tension but did not have the MTD pattern. These were then "classified" as having a "functional" dysphonia without using the muscle tension dysphonia title. Thus, we had functional dysphonia with ventricular band phonation (FDVB), with bowing (FDB), with hypoadducting states (FDHA), or a miscellaneous assortment of misuses that we called nonspecific (FDNS). We thus created classification confusion (3). This classification system of 1983 and the re- worked classification system of 1993 are summa- rized on Table 1.
Koufman's (4) work brought to our attention that supraglottic anteroposterior contraction states should also be brought into the relationship. So we reclassified the ways in which a laryngologist could group misuse of the laryngeal structures based on visual inspection during indirect or fiberoptic laryn- goscopy. Now all the patterns were included, with the original MTD being type 1, also called the "la- ryngeal isometric." Type 2 included lateral contrac- tion states at either a glottic or supraglottic location. Type 3 indicated varying severities of anteroposte- rior supraglottic contraction, type 4 hypoadducting or hysterical conversion aphonia, type 5 psycholog- ically based vocal fold bowing, and type 6 adoles- cent transitional dysphonia. We thus augmented our level of classification confusion (5).
We dropped the word "functional" from usage in
TABLE 1. Early muscle misuse dysphonia classifications
First (1983) Second (1993)
MTD 1 MTD2a (nodules) MTD2b (chronic laryngitis) MTD2c (polyp degeneration)
FDNS (nonspecific) FDVB (ventricular)
FDHA (hypoadducting) FDB (bowing) FMD (mutational)
mml laryngeal isometric mml plus vocal nodules mml plus chronic laryngitis mml plus polypoidal
degeneration mm2 glottic mm2 supraglottic mm3 (anteroposterior
contraction) mm4 (conversion aphonia) mm5 (psychogenic bowing) mm6 (adolescent transitional)
MTD, muscle tension dysphonia; mm, muscle misuse; FD, functional dysphonia.
describing the clinical features in muscle misuse voice disorders. The word can imply either a voice problem due to psychological factors or a simple disorder of physiological function; we found the term added confusion.
The detailed description and criteria for the use of each class in the second system still seems too ar- tificial and restrictive when one considers the com- plex clinical pattern usually present in any one pa- tient. We still use the system in our database to assist in organizing clinical detail, but prefer now to view each patient as presenting a pattern of clinical features beyond laryngeal postures and visible fea- tures of laryngoscopy.
CLINICAL PATTERN RECOGNITION IN MUSCLE MISUSE VOICE DISORDERS
Classification systems are more useful when there is a single disease state that accounts for the full range of clinical features observed. In voice dis- orders, we have found that impairment can be due to a collection of causative factors, including (a) habitual technical and postural misusage, (b) psy- chologically based muscular hypertonicity, (c) in- creased pharyngolaryngeal tone due to the reflux reflex, (d) neuromuscular abnormalities such as dystonia or tremor, and (e) organic processes, in- cluding nodules, polyps, cysts, or tumors.
Any classification that points a finger at one cause tends to ignore or undervalue the contribu- tion of others. We have found that successful treat- ment programs address each abnormal process in- volved. Each of the above factors plays a role in the production of dysphonia in a patient with a muscle misuse voice disorder, and the way in which these facts interact and interrelate presents a problem- solving challenge. Each of these patients has a pat- tern of causative factors, and many of these "pat- terns" are typical. For example, the person with long-standing poor postural habits and marginal vo- cal technical skill and who also has subclinical gas- troesophageal reflux disease often responds to emo- tional stressors with depression, vocal effort, fa- tigue, and voice loss. Another example may be the outgoing ebulent and vocally active teacher who is losing time at work. In order to sort out which of the etiological factors are most important to treat, the clinician must examine all aspects of the case. A clinical pattern will emerge for each.
Journal of Voice, Vol. 11, No. I, 1997
110 M. MORR1SON
IDENTIFICATION OF VARIOUS ASPECTS OF VOCAL MUSCLE MISUSE
Visual inputs Before getting into the details of pattern recogni-
tion, it will be helpful to review the ways in which we collect data from a voice-disordered patient. The classifications listed above have focused on laryngological appearance, which is only one part of the visual examination of the patient. Other visual observations that we make include the following:
1. General movement and posture: Patients with muscle misuse voice disorders (MMVD) tend to hold themselves rather rigidly and " s l o u c h . " Posture also is an expression about how one feels about oneself.
2. Mental state and personality: Many voice disorders are the result of the repression of negative emotion. Depression may be related to a suppressed cry or anger; jaw tension, to overactive neural activity with anxiety; and severe anxiety may convert to total voice loss. Persons with a hypochondriacal per- sonality may anticipate the poor voice and find it.
3. Shoulder and neck motion, and alignment: Free and easy voice use is difficult if the neck and shoulders are held tightly. The tension is often asymmetrical, and one shoulder may be at a higher level than the other. Cervical lor- dosis may be increased. Neck torsion injury, or " w h i p l a s h , " may trigger or cause a MMVD.
4. Head position and movement: With extra cervical lordosis, the head is extended at the atlantooccipital joint and the jaw juts for- ward. Spontaneous head movements are re- duced in MMVD.
5. Jaw excursion and freedom: In a person with a MMVD, the jaw does not move very much during phonation.
6. Scalloped tongue edges: Pressure against the teeth from a tense tongue creates a series of ridges that reflect the overall "held" nature of the voice and speech system.
7. Laryngeal movement with speech: In the nor- mal state, the larynx can be observed to move up and down freely during speech at various pitches, especially in untrained voice users. In trained professionals, decreased vertical variation with pitch is not necessarily a bad sign.
8. Strap muscle contraction: In MMVD, the strap muscles are tense and prominent during speech. This generally reflects the intensity of the "tug-of-war" that is going on in the neck, between the tongue and jaw muscles above and the infrahyoid straps below. Ob- serving the inferior bellys of the omohyoid muscles as they cross the supraclavicular fos- sae is often the easiest way to note this effect. It is helpful to ask the patient to change into a surgical scrub shirt during the interview if his/her attire makes it difficult to see the front of the neck.
9. Voice-related chest pressure: Chest and sub- glottic air pressure during speech are in- creased in patients with MMVD, due to the hypervalving effect of the tight laryngeal clo- sure. Jugular vein distension and overfilling of the supraclavicular fossae during voicing suggest the presence of this increased pres- sure.
I0. Breathing pattern: Optimal breathing for speech is present when a controlled flow of low pressure air passes up through a loosely adducted glottis. This control requires a push-pull interaction of some sort between the diaphragm and the other thoracic and ab- dominal muscles. For example, it can be achieved when abdominal muscles push air up against a degree of retained inspiratory force maintained by the diaphragm and inter- costals. Patients with MMVD may exhibit a lot of respiratory effort in the upper chest and shoulder areas, giving evidence to their breath control problem.
I 1. Level o f vocal effort: People with a muscle misuse voice problem generally have to work harder at talking than normal, and this effort is reflected in their complaints of fatigue and voice loss with use. This extra effort can also be observed by the clinician during the eval- uation.
Auditory inputs Listening to the voice is important in the evalua-
tion of a patient with a voice disorder. The follow- ing are a number of questions that the laryngologist may find useful in sorting out patterns of muscle misuse.
1. How "tight" & the voice? Just thinking this question will help the clinician, since much of the focus in muscle misuse voice disorders is
Journal of Voice, Vol. I1, No. I, 1997
MUSCLE MISUSE VOICE DISORDERS 111
on the degree and causation of tension. 2. Is the tightness "fry" or "spasm"? Effortful
pushing out of the voice in a low-pitched vo- cal fry register can sound to the uninitiated listener much the same as the spasmodic voice associated with focal dystonia or a psy- chologically based spasm.
3. How steady is the voice? The presence of tremor helps to confirm the neurological component of a voice misuse pattern. Tremor can be part of a spasmodic voice or be the central component in benign essential famil- ial tremor. Tremor is part of the core muscle function status upon which other factors act to shift the symptom severity up or down. Voice breaks are another form of unsteadi- ness and can be a component of almost any form of MMVD.
4. In what way is it "hoarse" or "clear"? This quality assessment refers to the amount of noise in the acoustic spectrum. Many de- scriptive terms are used, including harsh, strident, raspy, breathy, or rough. Other acoustic features such as diplophonia, which usually represents an asymmetry of the vocal fold mass or tension, have diagnostic value.
5. Are pitch and loudness appropriate? One way to get an idea of what the normal vocal pitch would be in the absence of the muscular misuse is to have the patient utter an abdom- inally supported "humph" repeatedly. This act tends to release the tightness rather well in many cases. Because laryngologists now regularly use a laryngeal stroboscope, they have easy access to a pitch-measuring de- vice. Even without a stroboscope, pitch can be estimated with an inexpensive keyboard or pitch pipe.
6. Where does the voice resonate? Effective voice production tends to sound somewhat nasal due to the "proper" use of the upper vocal tract resonators for amplification. In patients with MMVD, the voice may sound as if it is resonating further back in the throat.
7. Are modal and falsetto registers present? How well is the transition between registers achieved? A vocal register is a range of pitches that have a similar tonal quality and are produced by roughly similar phonatory dynamics and postures. In the pitch range where these registers are adjacent or overlap- ping, the vocalist needs greater technical skill
.
.
10.
to maintain a smooth transition of sound. As the voice tightens, the initial difficulty noted is often a problem with smooth transition be- tween modal (chest) register and the higher head (falsetto) register. When the MMVD is more advanced, the ability to sing in the up- per register may be lost, and the patient is restricted to modal voice usage. High notes must then be achieved by force, which is both injurious and aesthetically unpleasant. Does the voice fatigue? Sustaining constant vocal effort when the production forces are excessive leads to loss of quality, power, and projection, and it may be painful. How does the voice change with a hum, glide, or with movement o f the tongue, jaw, or head? These are some typical tools used in voice therapy for MMVD, and incorporating them into the evaluation will give the clini- cian insight into the nature of the disorder and may help estimate the likelihood of suc- cess in treatment. How does the voice change with emotion or with the topic o f conversation? The voice may become tight or dissonant when the topic of conversation moves into some spe- cific sphere and stay clear when the patient is distracted or more relaxed.
Tactile inputs: laryngeal palpation Palpation of the larynx at rest and during voice
gives useful information about its function and the degree of tension. In some patients, the larynx con- tracts to an abnormal degree and in an unphysio- logic way during voicing but returns to normal dur- ing rest. In others, the larynx is held tightly at all times, as if the person has forgotten to let go. There is also a difference between the "t ight" larynx, in which most of the tension is within the larynx itself, and the "held" larynx, where the larynx is splinted by the straps or, more importantly, held against the vertebral column by a tense inferior constrictor muscle.
Specifically, the laryngologist can assess these functional areas by palpating the following, at rest and with voicing:
1. Suprahyoid tension: The examiner should, from the patient's right side, lightly support the occiput in a neutral position while palpat- ing upward into the muscle region extend- ing from the body of the hyoid forward toward
Journal of Voice, Vol. 11, No. 1, 1997
112 M. MORRISON
the submental area. At rest this will be soft unless the tongue is being forced against the lower teeth. The intensity of contraction of muscles in this area with voice production is assessed.
2. Thyrohyoid space tension and tenderness: Still from the side, the examiner palpates the thyrohyoid membrane areas with the tip of the index finger on the left and thumb on the right. Is it open and relaxed? Are the thyrohyoid muscles tender to touch? Is pushing the hyoid bone to one side and the thyroid cartilage to the other easy? When the patient is asked to speak or phonate lightly on a vowel or "humph," does the thyrohyoid space disap- pear? Is there any relationship between ten- sion here and the degree of anteroposterior contraction of the supraglottis on laryngos- copy?
3. Cricothyroid space and mobility: The crico- thyroid space should be palpated with the in- dex fingertip. Is it open at rest? Does it open further when the voice glides down to the bot- tom of the range? Does it close with high pitches? The space that is held tightly closed at all times is particularly significant and un- desirable.
4. Cricoid displacement: Harris and Lieberman (6) have suggested that in MMVD the crico- thyroid muscles will eventually fatigue and let go, allowing the cricoid cartilage to slip for- ward and partly sublux the cricothyroid joint. This can be felt by relating the inferior midline edge of the thyroid cartilage to the cricoid arch.
5. Laryngeal excursion: The degree of up and down mobility of the larynx throughout the pitch range may be palpated or visualized.
6. Inferior constrictor tightness and freedom of the lateral laryngeal gutters: If the inferior constrictors are not holding the larynx tightly against the vertebral column, the larynx can be rotated and the fingertips insinuated behind the posterior edge of the thyroid lamina. If the area is very relaxed, then the movement of the arytenoid cartilage can be felt, and posterior cricoarytenoid muscle contraction can be pal- pated during an inspiratory sniff. If the larynx is tightly held, then the lateral gutters are not accessible at all. Great care must be taken to avoid carotid artery compression during this maneuver.
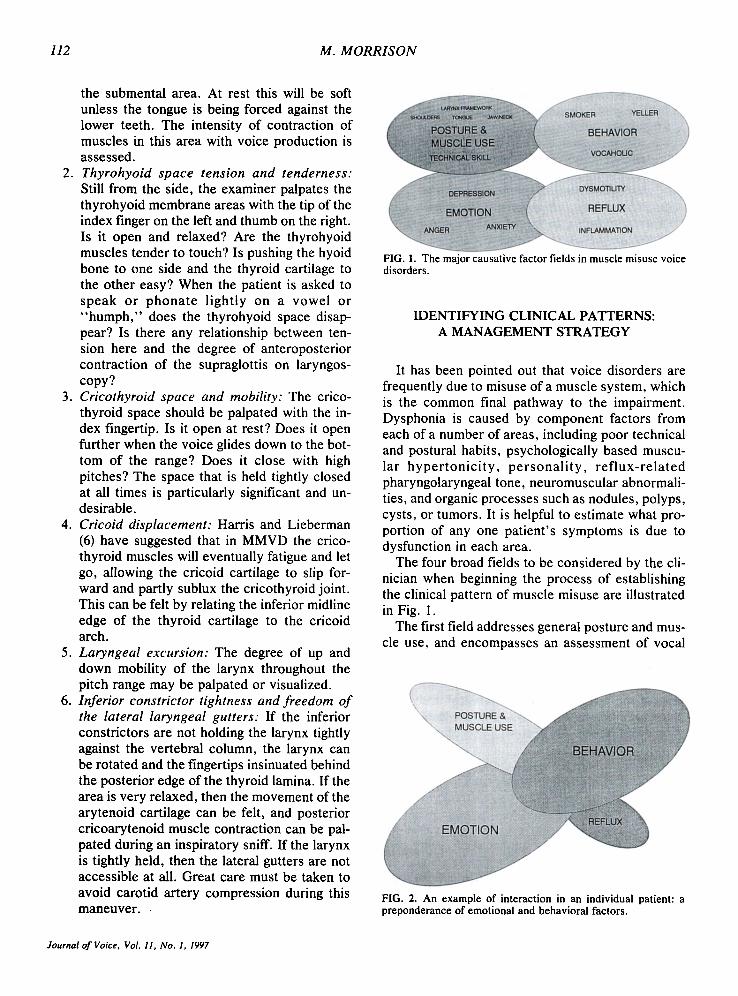
FIG. 1. The major causative factor fields in muscle misuse voice disorders.
IDENTIFYING CLINICAL PATTERNS: A MANAGEMENT STRATEGY
It has been pointed out that voice disorders are frequently due to misuse of a muscle system, which is the common final pathway to the impairment. Dysphonia is caused by component factors from each of a number of areas, including poor technical and postural habits, psychologically based muscu- lar hyper tonic i ty , personal i ty , ref lux-re la ted pharyngolaryngeal tone, neuromuscular abnormali- ties, and organic processes such as nodules, polyps, cysts, or tumors. It is helpful to estimate what pro- portion of any one patient's symptoms is due to dysfunction in each area.
The four broad fields to be considered by the cli- nician when beginning the process of establishing the clinical pattern of muscle misuse are illustrated in Fig. 1.
The first field addresses general posture and mus- cle use, and encompasses an assessment of vocal
FIG. 2. An example of interaction in an individual patient: a preponderance of emotional and behavioral factors.
Journal of Voice, Vol. 11, No. 1, 1997
MUSCLE MISUSE VOICE DISORDERS 113
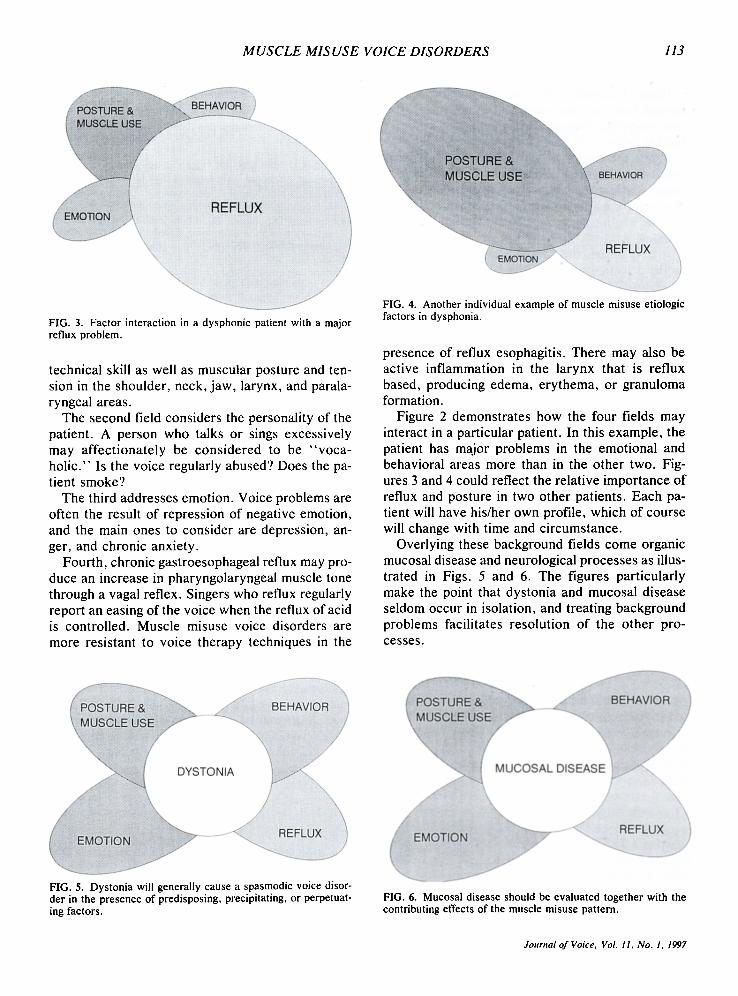
FIG. 3. Factor interaction in a dysphonic patient with a major reflux problem.
technical skill as well as muscular posture and ten- sion in the shoulder, neck, jaw, larynx, and parala- ryngeal areas.
The second field considers the personality of the patient. A person who talks or sings excessively may affectionately be considered to be "voca- holic." Is the voice regularly abused? Does the pa- tient smoke?
The third addresses emotion. Voice problems are often the result of repression of negative emotion, and the main ones to consider are depression, an- ger, and chronic anxiety.
Fourth, chronic gastroesophageal reflux may pro- duce an increase in pharyngolaryngeal muscle tone through a vagal reflex. Singers who reflux regularly report an easing of the voice when the reflux of acid is controlled. Muscle misuse voice disorders are more resistant to voice therapy techniques in the
FIG. 4. Another individual example of muscle misuse etiologic factors in dysphonia,
presence of reflux esophagitis. There may also be active inflammation in the larynx that is reflux based, producing edema, erythema, or granuloma formation.
Figure 2 demonstrates how the four fields may interact in a particular patient. In this example, the patient has major problems in the emotional and behavioral areas more than in the other two. Fig- ures 3 and 4 could reflect the relative importance of reflux and posture in two other patients. Each pa- tient will have his/her own profile, which of course will change with time and circumstance.
Overlying these background fields come organic mucosal disease and neurological processes as illus- trated in Figs. 5 and 6. The figures particularly make the point that dystonia and mucosal disease seldom occur in isolation, and treating background problems facilitates resolution of the other pro- cesses.
q/ 8 FIG. 5. Dystonia will generally cause a spasmodic voice disor- der in the presence of predisposing, precipitating, or perpetuat- ing factors.
FIG. 6. Mucosal disease should be evaluated together with the contributing effects of the muscle misuse pattern.
Journal of Voice, Vol. 11, No. 1, 1997

114 M. MORRISON
Figure 5 considers dystonia and tremor, the ab- normal baseline tone upon which background fac- tors exert their impact. Therapy directed at the al- terable factors can facilitate symptom resolution.
Figure 6 considers mucosal changes. These may result from misuse and abuse, or can activate and trigger the misuses themselves. It is easy to lay all blame for the symptom on a poor nodule, when it may be just a trigger, an effect, or an innocent by- stander.
In conclusion, this article presents my approach to the disentanglement of the complex factors that can cause a muscle misuse voice disorder in a way that may help the clinician treat patients more ef- fectively. It is hoped that this account will generate as many questions as solutions and encourage the research that is needed to better our understanding of this intriguing muscle use system.
More information on clinical recognition of fea- tures related to psychological, postural, reflux, or behavioral manifestations of voice disorders has been presented elsewhere, and the reader is encour- aged to explore further (7-10).
REFERENCES
1. Morrison MD, Rammage LA, Belisle GM, Nichol H, Pullan B. Muscular tension dysphonia. J Otolaryngol 1983;12: 302--6.
2. Belisle G, Morrison MD. Anatomic correlation for muscle tension dysphonia. J Otolaryngol 1983;12:319-21.
3. Morrison MD, Nichol H, Rammage LA. Diagnostic criteria in functional dysphonia. Laryngoscope 1986;96: I-8.
4. Koufman JA, Blalock PD. Classification and approach to patients with functional voice disorders. Ann Otol Rhinol Laryngol 1982;91:372-7.
5. Morrison MD, Rammage LA. Muscle misuse voice disor- ders: description and classification. Acta Otolaryngo! (Stockh) 1993;113:428-34.
6. Harris T, Lieberman J. The cricothyroid mechanism, its re- lation to vocal fatigue and vocal dysfunction. Voice Forum 1993 ;2:89-96.
7. Morrison MD, Rammage LA. The management of voice dis- orders. London: Chapman and Hall, 1994.
8. Rubin JS, Sataloff RT, Korovin GS, Gould WJ. Diagnosis and treatment of voice disorders. New York: Igaku-Shoin, 1995.
9. Colton RH, Casper JK. Understanding voice problems. Bal- timore: Williams & Wilkins, 1990.
10. Sataloff RT. Professional voice: the science and art o f clin- ical care. New York: Raven Press, 1991.
Journal of Voice, Vol. I1, No. 1, 1997