![Hospital Acquired Infections, Sources, Route of …...hospital acquired infections worldwide is Enterococci [17]. Three to seven percent of hospital-acquired bacterial infections are](https://static.fdocuments.in/doc/165x107/5e8d2da3c3edfd174827a4ae/hospital-acquired-infections-sources-route-of-hospital-acquired-infections.jpg)
2. hospital acquired infections
77
Hospital Acquired Infections ( Nosocomial Infections) Dr Soni Rani PGT-I Department of Community Medicine Katihar Medical College & Hospital
-
Upload
dr-arun-kumar-pandey -
Category
Health & Medicine
-
view
210 -
download
4
Transcript of 2. hospital acquired infections

Hospital Acquired Infections( Nosocomial Infections)
Dr Soni RaniPGT-I
Department of Community MedicineKatihar Medical College & Hospital

Hospital Acquired Infections(Nosocomial Infections)
• Hospital-acquired infections (HAIs) is defined as acquiring an infection in the hospital by the patients or others during their stay and manifesting either during the hospital stay itself or after discharge.
Hospital Acquired Infections(Nosocomial Infections)

Definition of Nosocomial Infection
• An infection acquired in hospital by a patient who was admitted for a reason other than that infection .
• An infection occurring in a patient in a hospital or other health care facility in whom the infection was not present or not incubating at the time of admission.
• This includes infections acquired in the hospital but appearing after discharge, and also occupational infections among staff of the facility.

• Infections occurring more than 48 hours after admission are usually considered nosocomial.
• Infections acquired by Staff/Visitors to Hospital for OPD services also considered as Nosocomial infections.
Definition of Nosocomial Infection
Prevalence of HAI
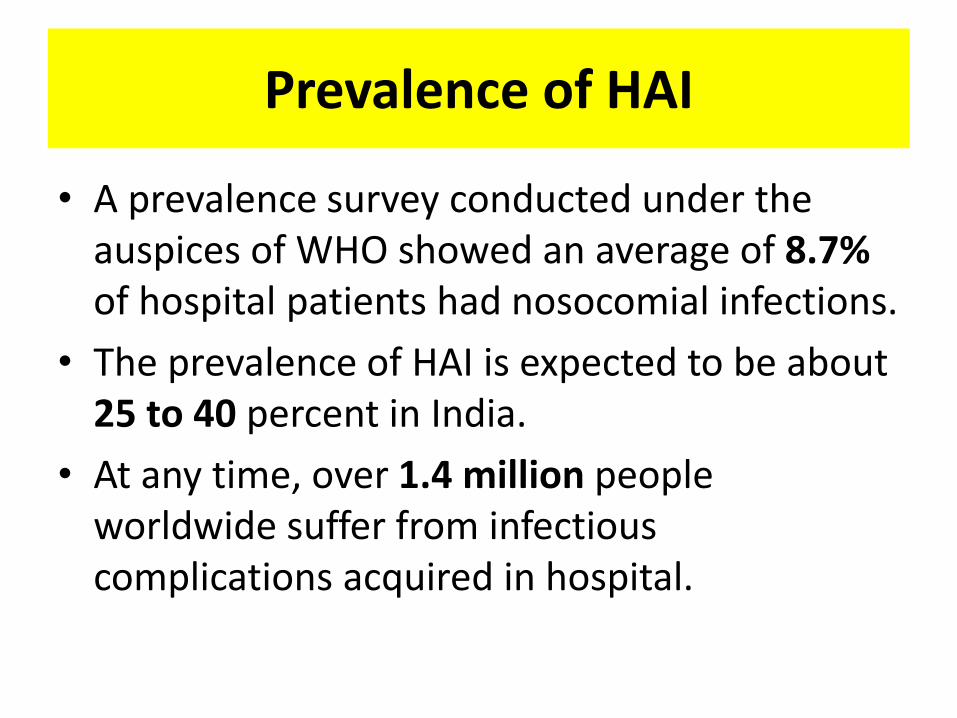
• A prevalence survey conducted under the auspices of WHO showed an average of 8.7%of hospital patients had nosocomial infections.
• The prevalence of HAI is expected to be about 25 to 40 percent in India.
• At any time, over 1.4 million people worldwide suffer from infectious complications acquired in hospital.
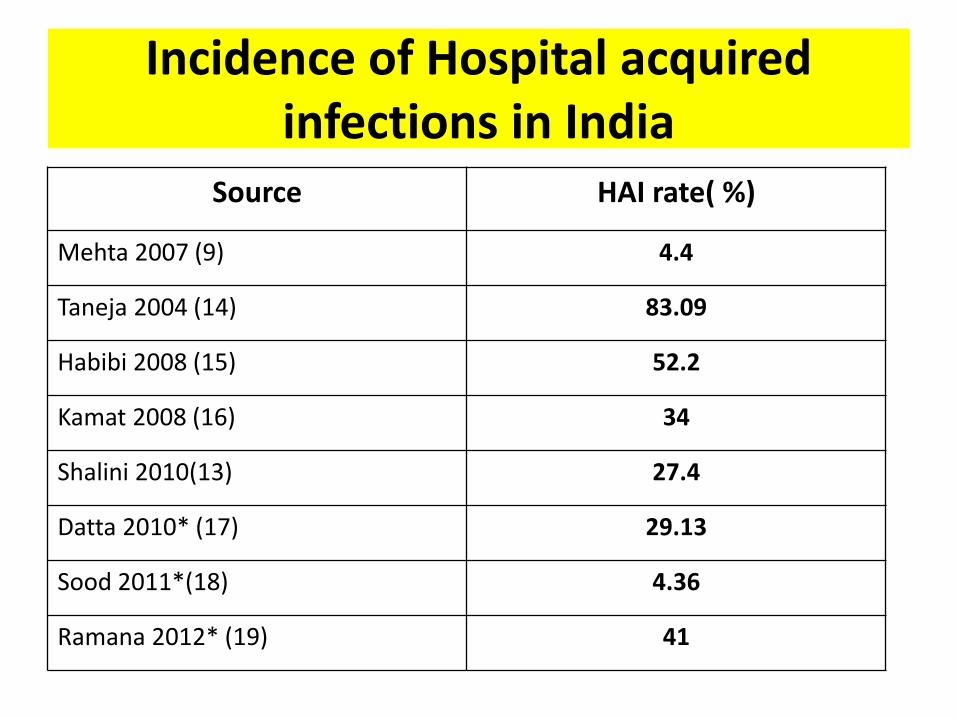
Incidence of Hospital acquired infections in India
Source HAI rate( %)
Mehta 2007 (9) 4.4
Taneja 2004 (14) 83.09
Habibi 2008 (15) 52.2
Kamat 2008 (16) 34
Shalini 2010(13) 27.4
Datta 2010* (17) 29.13
Sood 2011*(18) 4.36
Ramana 2012* (19) 41

Impact of Nosocomial Infection

compromised patients
ward and inter-hospital transfers
antibiotic resistance (MRSA, resistant Gram negatives)
increasing workload
staff pressures
lack of facilities
? lack of concernHAI is inevitable but some is preventable (irreducible minimum)
realistically reducible by 10-30%
H.A.I. IS INCREASING

Most Common Sites of NosocomialInfections

Causes of HAI
• Hospital-acquired infections is usually due to failure to observe aseptic precautions while carrying out the hospital procedures such as surgical operations, IV infusions, catheterization, dressings of the wounds, lumber puncture, giving injections, etc.

Predisposing Factors
• Development of the resistance by the organisms to the commonly used drugs
• Overcrowding of the hospitals
• Poor environment of the hospitals, both inside and outside
• Decreased resistance and increased susceptibility of the vulnerable groups of patients such as those suffering from tuberculosis, leprosy, diabetes, severe PEM, anemia, cardiac patients, old age of the patients, those who have undergone major surgery, those who are on steroids, cytotoxic drugs, etc.
Cross infection organisms
• METHICILLIN RESISTANT STAPH AUREUS (MRSA) • Causes about 50% of HAI
• Resistant to Flucoxacillin and usually others
May cause -Wound infection Bacteraemia Skin/soft tissue infection U.T.I. Pneumonia etc.
Etiological agents

• RESISTANT GRAM NEGATIVE ORGANISMS• Causes about 45% of HAI
• Resistance to multiple antibiotics
Organisms:E .coli Proteus EnterobacterAcinetobacterPseudomonas aeruginosa
Etiological agents

• TUBERCULOSIS• Open pulmonary TB (Sputum smear positive for AFB)
• VIRAL INFECTIONS
Chicken Pox, (Hepatitis B HIV)
• Both are responsible for about 5% of HAI.
Etiological agents

Important means of monitoring HAI Early detection of trends outbreaks
1. Laboratory BasedMicrobiology Laboratory lists +ve organisms ICN reviews ‘Alert organisms’ reported
2. Ward BasedWard staff monitor patientsICN reviews ICN visits wards
HAI Surveillance

Diagnostic criteria for Surveillance of Nosocomial Infections
Type of Nosocomial Infections Simplified Criteria
Surgical site infection
Any purulent discharge, abscess, orspreading cellulitis at the surgicalsite during the month after theoperation.
Urinary infection
Positive urine culture(1 or 2 species) with at least105bacteria/ml, with or withoutclinical symptoms.
Respiratory infection
Respiratory symptoms with atleast two of the following signsappearing during hospitalization:— cough— purulent sputum— new infiltrate on chestradiograph consistent withinfection

Type of NosocomialInfections
Simplified Criteria
Vascular Catheter InfectionInflammation, lymphangitis or purulent discharge at the insertion site of the catheter
SepticaemiaFever or rigours and at least onepositive blood culture
Criteria for Surveillance of NosocomialInfections

Hospital acquired infection
1. Sources and reservoir of HAI
2. Recipients
3. Route of spread
Hospital Acquired Infections(Nosocomial Infections)
Sources and Reservoirs of HAI
The sources are patients, hospital staff and the environment.
PATIENTS:
• Patients suffering from infectious diseases are potential sources of infection.
• These cases may be certain viral infections (measles, german measles, influenza, viral hepatitis);

• Skin infections (discharging wounds, infected skin lesions, eczema, psoriasis, boils, bed sores)
• respiratory infections (sore throat, pulmonary tuberculosis, chest infection)
• urinary tract infection (E. coli infection).
• All these are very common sources of hospital acquired infection
Sources and Reservoirs of HAI

• STAFF:
• The hospital staff (viz doctors, nurses, ward boys) who come in close contact with patients may often be an important source of cross infection.
• For example, staphylococcus aureus is commonly carried in the nose or on the skin.
• Haemolytic streptococci may be carried in the throat and salmonella in the gut.
Sources and Reservoirs of HAI
• ENVIRONMENT:
a) Air: Hospital air and dust usually harbors more bacteriae, which are often pathogenic an multidrug resistant.
b) Surfaces contaminated by patient’s secretions, excretions, blood and body-fluids, animals and insects.
Sources and Reservoirs of HAI

c) Inanimate objects:
– Contaminated by the patients: Hospital equipment, such as thermometer, linen, bed, table, cot, sanitary installations, etc. medical equipment such as endoscopes, catheters, needles, lancets, spatula, vesical probes, etc.
– Contaminated by the hands of any hospital staff in any part of the hospital (kitchen, laundry, treatment room, etc.)
Sources and Reservoirs of HAI

– Contaminated by visitors
– Contaminated by staff who are ill or are carriers of microorganisms
– Contaminated by food or contaminated water
– Contaminated by animals and insects.
Sources and Reservoirs of HAI
• Thus, man occupies a central position:
a. As reservoir and source of microorganisms
b. As disseminator (communication routes)
c. As recipient or target, thus becoming a new reservoir.
• All patients in the hospital are potential recipients of crossinfection.
• Those who are severely ill, chronically ill and on steroid therapy are all highly susceptible.
Recipients
Route of Spread
• The common routes of spread of cross infection are:
a) Direct contact- the organism may be transferred directly from the hands of a nurse or doctor to a susceptible patient;
b) Droplet infection- droplets released from nose and throat through coughing or sneezing:
c) Air-borne particles; d) Release of hospital dust into the air;e) Through various hospital procedures, viz, catheterisation,
intravenous procedures, infected cat gut, dressings, sputum cups, bed pans, urinals etc.

Prevention and Control of Nosocomial Infections
Preventions and Control
• Elimination of the Reservoirs or Sources
• Breaking the Channel of Transmission
• Protection of Susceptible Persons
• Administrative Measures

Elimination of the Reservoirs or Sources
1) Care of the staff
2) Care of the Patient
3) Treatment
4) Nursing care

Care of the staff
• Hospital staff suffering from any infectious disease (respiratory or alimentary or any septic skin lesions) should not attend to their duties until complete recovery.

Care of the Patient
• All acute infectious cases must be admitted in the isolation ward only. There are three types of wards.
i. Chamber ward (cell ward): This is a separate ward for separate (individual) patients.
• It is also called isolation ward.• It has its own ventilation. • The partition extends from floor to ceiling.ii. Cubicle ward: In this type, the partition extends from floor
but does not reach ceiling, giving provision for cross-ventilation.
iii. Open wards: These are general wards wherein manypatients are admitted.
Treatment and Nursing care
• Treatment: This should be given correctly and completely with specific antibiotics.
• Nursing care:i. Barrier nursing: This means that the hospital staff must
act as barriers to prevent cross-infection by wearing gowns, gloves, masks, etc. while touching or examining certain acute infectious cases.
ii. Task nursing: This means posting special nurses for special duties. For example, a nurse attending to feeding of a premature child should not attend to the toilet of the child. Such care is essential in intensive care unit, premature baby-ward, etc.

• Hand washing
• Personal hygiene
• Clothing
• Mask
• Gloves
• Safe injection practices .
Breaking the chain of transmission

Why
Don’t Staff Wash their Hands
(Compliance estimated at less than 50%)

Why Not?
• Skin irritation
• Inaccessible hand washing facilities
• Wearing gloves
• Too busy
• Lack of appropriate staff
• Being a physician
(“Improving Compliance with Hand Hygiene in Hospitals” Didier Pittet. Infection
Control and Hospital Epidemiology. Vol. 21 No. 6 Page 381)

Why Not?
• Working in high-risk areas
• Lack of hand hygiene promotion
• Lack of role model
• Lack of institutional priority
• Lack of sanction of non-compliers

Successful Promotion
• Education
• Routine observation & feedback
• Engineering controls
– Location of hand basins
–Possible, easy & convenient
–Alcohol-based hand rubs available
• Patient education
(Improving Compliance with Hand Hygiene in Hospitals. Didier Pittet. Infection Control and Hospital Epidemiology. Vol. 21 No. 6 Page 381)

Successful Promotion
• Reminders in the workplace
• Promote and facilitate skin care
• Avoid understaffing and excessive workload; Nursing shortages have caused
Successful Promotion

Hand Hygiene
• Easy, timely access to both hand hygiene and skin protection is necessary for satisfactory hand hygiene.
• A study by Pittet showed a 20% increase in compliance by using feedback and encouraging the use of alcohol hand rubs

Hand Hygiene Techniques
1. Alcohol hand rub
2. Routine hand wash 10-15 seconds
3. Aseptic procedures 1 minute
4. Surgical wash 3-5 minutes

Repeat procedures until hands are clean
Routine Hand Wash
Alcohol Hand Rubs
• Require less time
• Can be strategically placed
• Readily accessible
• Multiple sites
• All patient care areas

Alcohol Hand Rubs
• Acts faster
• Excellent bactericidal activity
• Less irritating (??)
• Sustained improvement

Alcohol Hand Rubs
Choose agent carefully:
–Adequate antimicrobial efficacy
–Compatibility with other hand hygiene products

Visible soiling
• Hands that are visibly soiled or potentially grossly contaminated with dirt or organic material MUST by washed with liquid soap and water
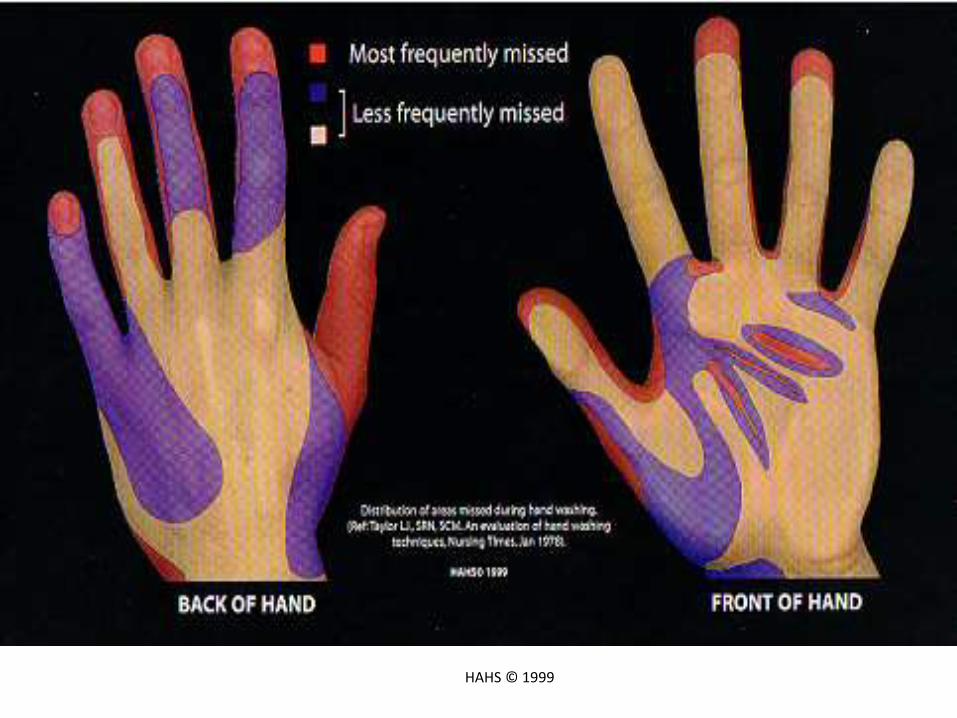
Areas Most Frequently Missed
HAHS © 1999

Hand Care• Nails
• Rings
• Hand creams
• Cuts & abrasions
• “Chapping”
• Skin Problems
Hand hygiene is the simplest, most effective measure for preventing
hospital-acquired infections.

Personal hygiene
• All staff must maintain good personal hygiene.
• Nails must be clean and kept short.
• False nails should not be worn.
• Hair must be worn short or pinned up.
• Beard and moustaches must be kept trimmed short and clean.

Clothing
• Working cloth
• Shoes
• Caps
Mask
• Masks of cotton wool, gauze, or paper are ineffective.
• Paper masks with synthetic material for filtration are an effective barrier against microorganisms.
• For patient protection surgical mask is recommended.
• For staff protection a high efficiency mask is recommended.

Gloves
• Hands must be washed when gloves are removed or changed.
• Disposable gloves should not be reused.• Latex or polyvinyl-chloride are the materials
most frequently used for gloves. • Quality, i.e. absence of porosity or holes and
duration of use vary considerably from one glove type to another.
• Sensitivity to latex may occur, and the occupational health programme must have policies to evaluate and manage this problem.

Safe injection practices
• eliminate unnecessary injections
• use sterile needle and syringe
• use disposable needle and syringes, if possible
• prevent contamination of medications
• follow safe sharps disposal practices
Preventing transmission from theenvironment
1) Cleaning of the hospital environment
2) Use of hot/superheated water
3) Disinfection of patient equipment
4) Sterilization

Cleaning of the hospital environment
• Ninety per cent of microorganisms are present within “visible dirt”, and the purpose of routine cleaning is to eliminate this dirt.
• This may be achieved by classifying areas into one of four hospital zones
— Zone A: no patient contact. Normal domestic cleaning (e.g. administration, library).

• Zone B:• care of patients who are not infected, and not
highly susceptible, cleaned by a procedure that does not raise dust.
• Dry sweeping or vacuum cleaners are not recommended.
• The use of a detergent solution improves the quality of cleaning.
• Disinfect any areas with visible contamination with blood or body fluids prior to cleaning.
Cleaning of the hospital environment

• Zone C:
• infected patients (isolation wards).
• Clean with a detergent/disinfectant solution, with separate cleaning equipment for each room.
Cleaning of the hospital environment
— Zone D:
highly-susceptible patients (protective isolation) or protected areas such as operating suites, delivery rooms, intensive care units, premature baby units, casualty departments and haemodialysis units.
• Clean using a detergent/ disinfectant solution and separate cleaning equipment.
Cleaning of the hospital environment

Disinfection with hot water
Temperature Duration
Sanitary equipment 80 °C 45–60 seconds
Cooking utensils 80 °C 1 minute
Linen 70 °C 25 minute
95 °C 10 Minutes

Disinfection of patient equipment
• High-level disinfection (critical) —
• this will destroy all microorganisms, with the exception of heavy contamination by bacterial spores.
• Intermediate disinfection (semi-critical) —this inactivates Mycobacterium tuberculosis vegetative bacteria, most viruses and most fungi, but does not necessarily kill bacterial spores.

• Low-level disinfection (non-critical) — this can kill most bacteria, some viruses and some fungi, but cannot be relied on for killing more resistant bacteria such as M. tuberculosis or bacterial spores.
Disinfection of patient equipment

Sterilization
• Sterilization is the destruction of all microorganisms.
• Operationally this is defined as a decrease in the microbial load. sterilization can be achieved by either physical or chemical means .
• Heat (Thermal ) sterilization
• Chemical sterilization
• Radiation sterilization
Sterilization

Thermal sterilization
• Wet sterilization( Autoclave) : exposure to steam saturated with water at 121 °C for 30 minutes, or 134 °C for 13 minutes in an autoclave; (134 °C for 18 minutes for prions).
• Dry sterilization: exposure to 160 °C for 120 minutes, or 170 °C for 60 minutes; Dry sterilization process is often considered less reliable than the wet process, particularly for hollow medical devices.
• Other methods are Flaming, incineration, tyndallization , glass blade sterilizer

Chemical sterilization
• Ethylene oxide and formaldehyde for sterilization are being phased out in many countries because of safety and greenhouse gas emission concerns.
• Peracetic acid is widely used in the United States and some other countries in automatic processing systems.

Radiation sterilization
• Non-ionizing radiation sterilization- ( UV Radtiation)
• Ionizing radiation sterilization(Gamma radiation, X-Ray, Electron Beam Radiation)

Protection of Susceptible Persons
1. Highly susceptible persons should be admitted preferably in the isolation wards.
2. They are protected with vaccinations, e.g. tetanus, hepatitis B, gas gangrene, etc.
3. Universal blood and body fluid precautions to be adopted by all the health care workers.

Administrative Measures
• There should be a Hospital Infection Control Committee for surveillance of HAIs, to draw guidelines for different high risk procedures, early detection and control of outbreak of HAI and also to formulate policies (regarding admission of infectious cases, isolation facilities, disinfection procedures,etc.) and to implement them.

Infection control committee
• The Hospital-acquired Infection Control Committee consists of the following administrative set-up:
• Chairperson: Medical Superintendent
• Member Secretary: Infection Control Officer (Microbiologist)
• Members: Chiefs of all Clinical Units/Heads of Deptartment
• Chief of Blood Bank Service

• Microbiologist
• Medical Record Officer
• Chief of Nursing Services
• Infection Control Sister
• Invited members: Chiefs of all Supportive Services (OT, kitchen, laundry, etc.)
Infection control committee
• The Committee must meet at least once a month. Similarly there must be a ‘Control Board’ at the state level and national level.
Infection control committee
Task of ICC
• To review and approve a yearly programme of activity for surveillance and prevention
• To review epidemiological surveillance data and identify areas for intervention
• To assess and promote improved practice at all levels of the health facility
• To ensure appropriate staff training in infection control and safety

• to review risks associated with new technologies, and monitor infectious risks of new devices and products, prior to their approval for use
• to review and provide input into investigation of epidemics
• to communicate and cooperate with other committees of the hospital with common interests such as Pharmacy and Therapeutics or Antimicrobial Use Committee, Biosafety or Health and Safety Committees, and Blood Transfusion Committee.
Task of ICC


References
• PREVENTION OF HOSPITAL-ACQUIRED INFECTIONS: A PRACTICAL GUIDE — WHO/CDS/CSR/EPH/2002.12
• Park’s textbook of preventive and social medicine (23rd Edition)
• Community medicine with recent advances ( A.H.Suryakantha). 3rd Edition.
• Textbook of community medicine ( Preventive and social medicine) 4th Edition by Sundarlaal.
• https://en.wikipedia.org/wiki/Hospital-acquired_infection

Any Questions???
• Thank you for not asking!!!