







Languages
Pages
Legal


The Cirrhosis Tsunamiare we ready?
Mary Patricia Pauly MD FACP AGAF
Kaiser Permanente
Sacramento Medical Center


Diagnosis Diagnosis

• 45 year old elementary school teacher with cirrhosis calls in to clinic – Trouble focusing – Slow – Slurred speech – Confused

Outline• Cirrhosis
– Definition , • Survival w and wo Decompensation• causes
– Physical signs and lab signs • Portal hypertension--Anatomy and physiology• Manifestation of decompensated cirrhosis – how it fits with portal
hypertension – Ascites, variceal bleed , encephalopathy
• Only a certain percentage,
– TREATMENT OF complications of cirrhosis and portal hypertension- cancer surveillance
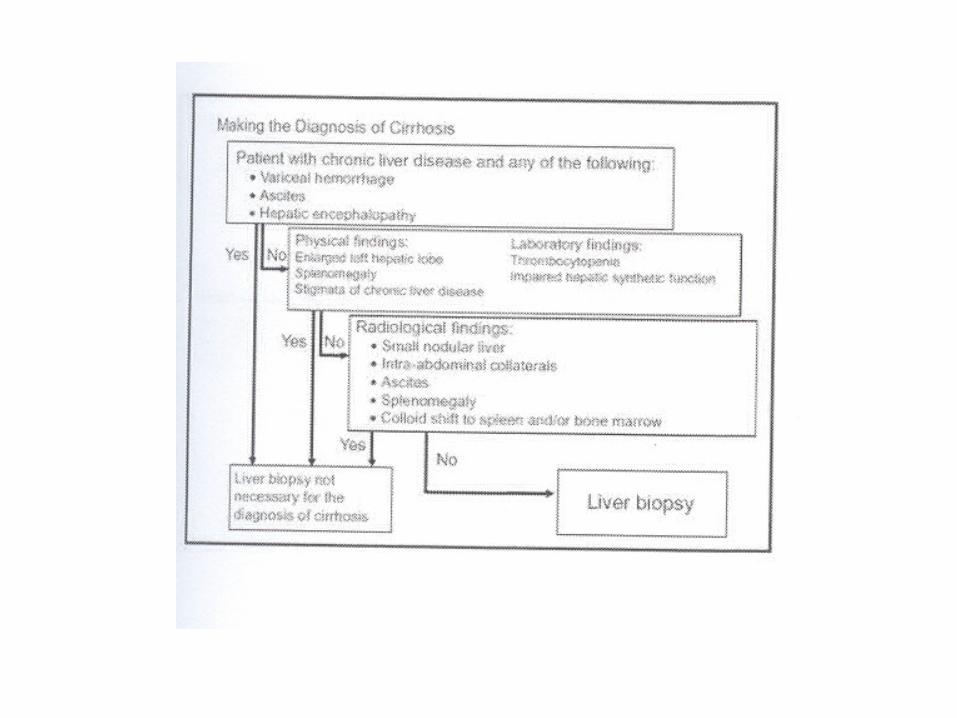
– Making the diagnosis– Prognosis –
• Childs class, MELD – Treatment may decrease incidence of cirrhosis

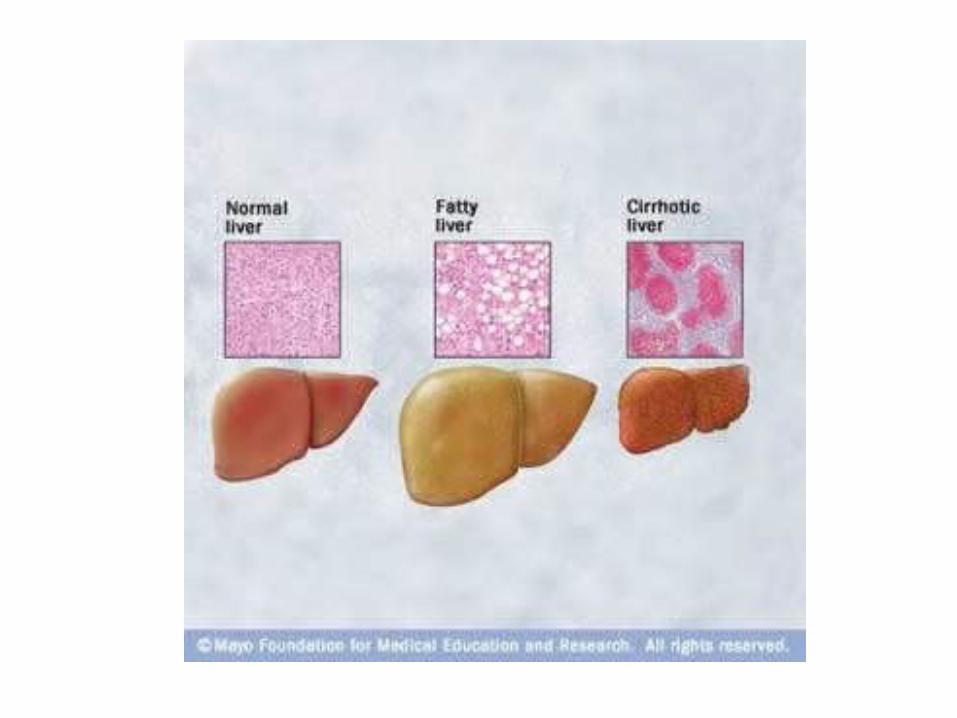
Cirrhosis
• Late stage of progressive hepatic fibrosis – Distortion of hepatic architecture – Regenerative nodules – Irreversible in advanced stages
• Patients with cirrhosis – Decreased life expectancy – Susceptible to complications
• Decompensation – Ascites, Variceal bleeding and encephalopathy
• Cancer– HCC and – Cholangiocarcinoma

Survival in Cirrhosis
Fattovich G, et al. Gastroenterology. 1997;112:463-472.
Compensated
After first major complication
Survival Probability
100
Pat
ien
ts (
%)
80
60
40
20
01200 12 24 36 48 60 72 84 96 108
Mos
384 65
Pts at Risk, n 376 39
34221
28811
2367
1654
1264
793
523
392
251
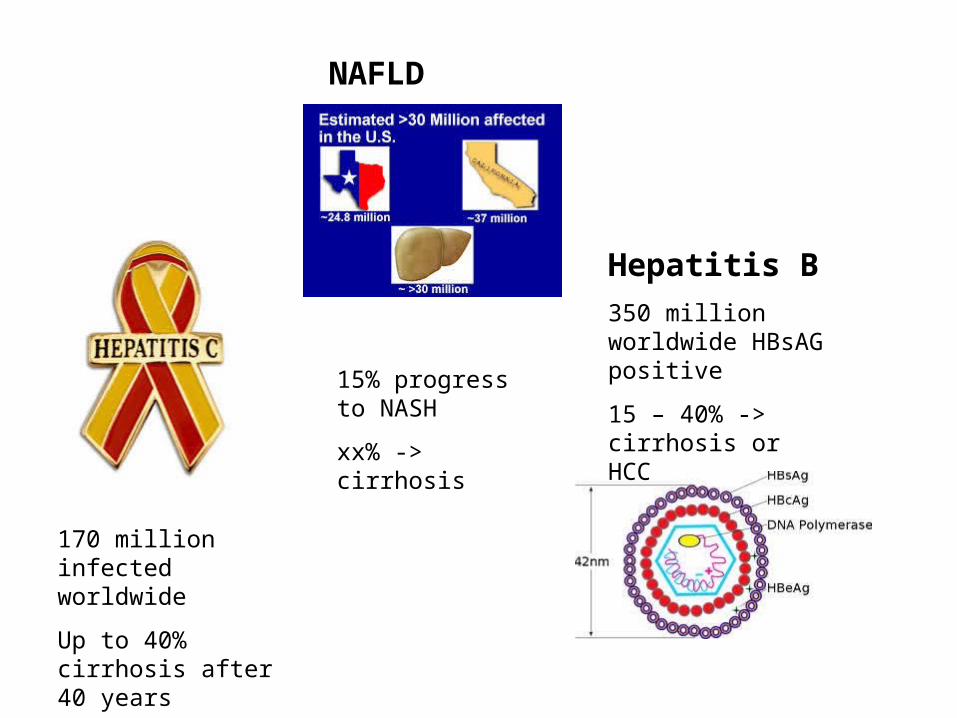
170 million infected worldwide
Up to 40% cirrhosis after 40 years
Hepatitis B
350 million worldwide HBsAG positive
15 – 40% -> cirrhosis or HCC
NAFLD
15% progress to NASH
xx% -> cirrhosis

The Cirrhosis Tsunami

Spider angiomata
Note the central pulsating arteriole surrounded by many smaller vessels or “legs.”
Pathogenesis incompletely understood
Possibilities: Alterations in sex hormone metabolism- increase in estradiol to free testosterone ratio in men.
Number and size correlate with severity of disease

Palmar erythema
Pathogenesis: It is thought to be caused by altered sex hormone metabolism

Gynecomastia
Pathogenesis: increased conversion of androstenedione ( produced in adrenals) -> estrone -> estradiol.

Dupuytren’s contractures
Due to thickening and shortening of the palmar fascia
Fibroblastic proliferation and disorderly collage deposition --> fascial thickening and flexion deformities of the fingers.
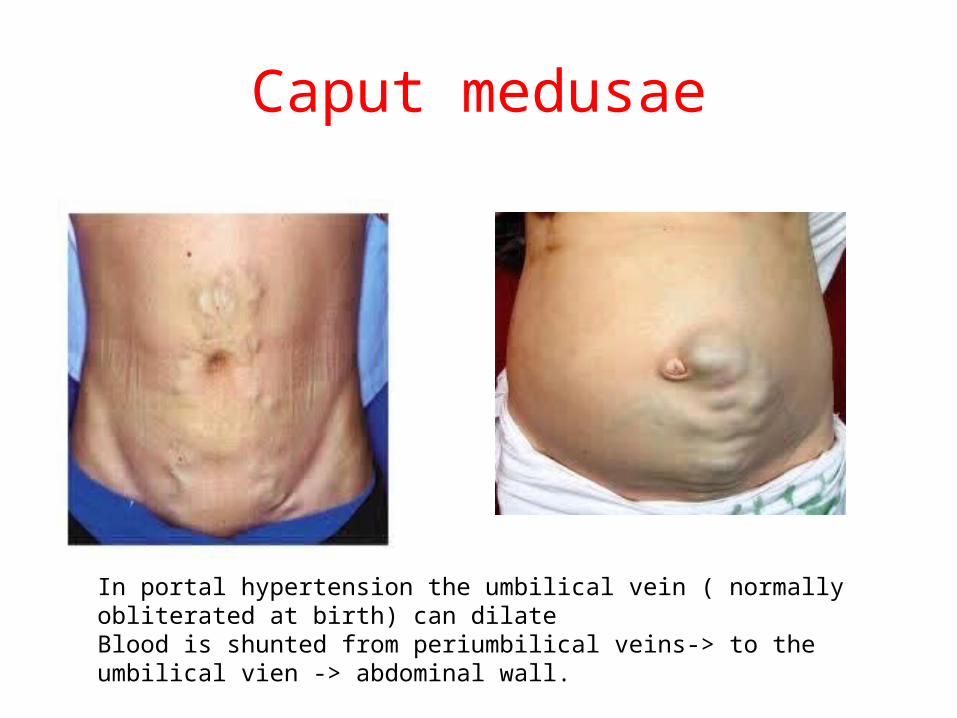
Caput medusae
In portal hypertension the umbilical vein ( normally obliterated at birth) can dilate Blood is shunted from periumbilical veins-> to the umbilical vien -> abdominal wall.

Physicial findings in cirrhosis•Physical findings
–Stigmata of portal hypertension:• Spider angiomata
• Caput medusae
• Palmar erythema
• Dupuytren’s contracture
• Gynecomastia
• Ascites
• Signs of encephalopathy– Jaundice --- does not necessarily indicate cirrhosis
» acute hepatitis
» CBD obstruction

Laboratory Finding consistent with cirrhosis
• Laboratory findings–Low platelet count
< 100 K
Low WBC and Anemia. – Splenic sequestration
–Low albumin–Elevated prothrombin
time –Elevated Bilirubin
– Liver biopsy – Non invasive markers
of Fibrosis • Fibrosure/fibrospect
F3-4• Fibroscan and similar
technologies measures elasticity
– >12.5 Kpa
• APRI > 2
APRI
• APRI = • (AST elevation/platelet
count) x 100• Example
– AST = 90 IU/L • ULN = 45 IU/L
– Platelet count =120,000/mm3
• APRI =• 90/45=2• (2/120) x 100 = 1.67• APRI > 2 correlates
with cirrhosis • <0.5 correlates with
no cirrhosis.


The Liver: Progression of Disease
TIME course 10 --> 40 years .

Hepatic Fibrosis: Metavir score


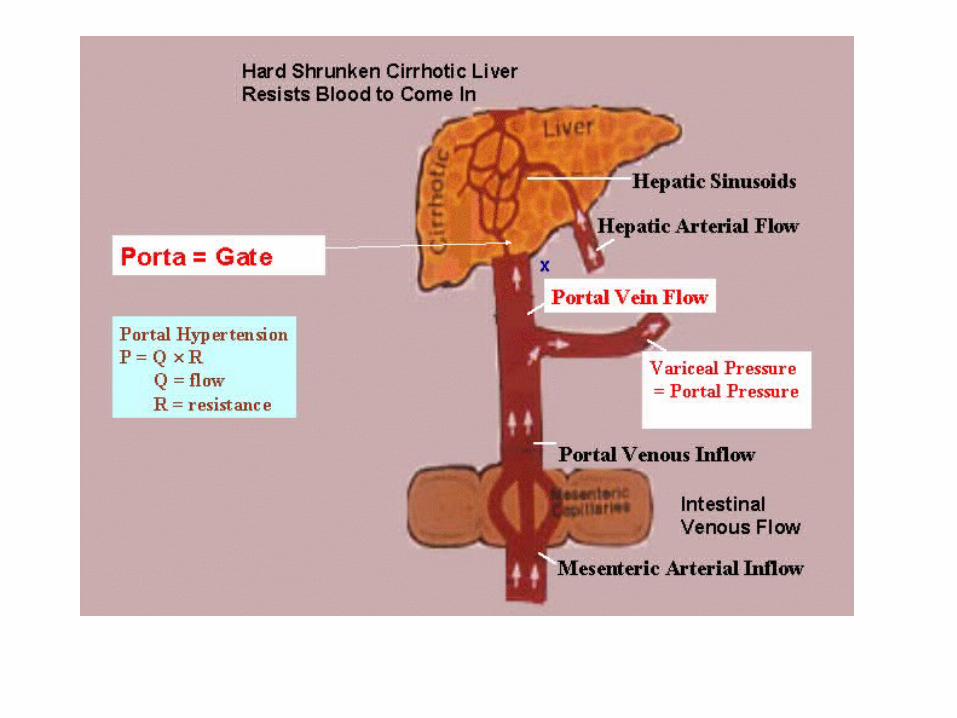

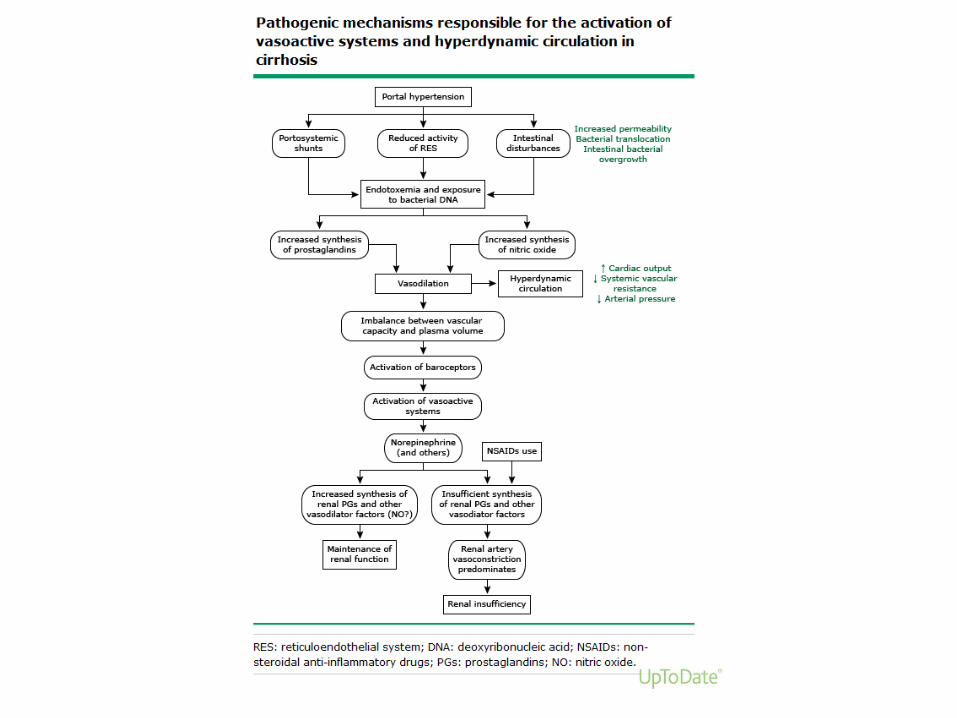
Portal Hypertension
• More than mechanical obstruction • Vasodilation
– increased
» Glucagon
» Nitrous oxide
– Decreased SVR
– Decreased MAP
– Increased collaterals
• Increased CO– Increased portal blood
flow
– Hyperdynamic circulation

Cirrhosis
Increased resistance to portal flow
Increased portal pressure
Varices
Decreased splanchnic arteriolar resistance
Increased portal blood flow
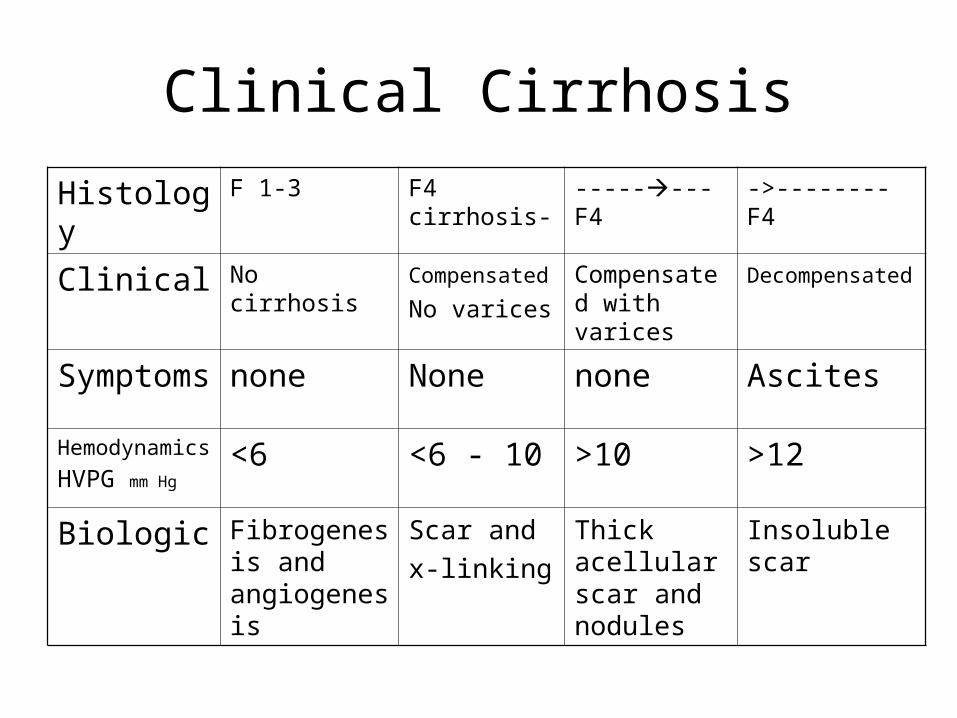
Clinical Cirrhosis
Histology F 1-3 F4 cirrhosis- --------F4 ->--------F4
Clinical No cirrhosis Compensated
No varices
Compensated with varices
Decompensated
Symptoms none None none Ascites
Hemodynamics
HVPG mm Hg<6 <6 - 10 >10 >12
Biologic Fibrogenesis and angiogenesis
Scar and
x-linking
Thick acellular scar and nodules
Insoluble scar

Gastro esophageal varices
• 50% of patients with cirrhosis
• 5-15% Risk of bleeding per year – Directly related to
portal pressure– SIZE if most important
predictor of bleeding *• Large varices 30%• Small varices 7%
• Recommended EGD• Surveillance for varices
in cirrhosis
– If no varices –• Recheck 2-3 y
– If small varices • Recheck 1-2 y
– If large varices • Primary prophylaxis
*over 2 years

Esophageal varices
Varices 2 y risk of bleeding without BB
2 y risk of bleeding with BB
Small 7% 2%
Large 30% 14%
• Non bleeding varices• Primary prophylaxis
– Non cardioselective beta- blockers
• Propranolol• Nadolol
• Titrate to 25% decrease in HR from baseline
– EVBL• if intolerant of BB

Treatment of varices
• Actively bleeding– Band ligation– Octreotide
• ->Splanchnic vasoconstriction and Decreased portal blood flow
– Inhibits release of vasodilator hormones (glucagon)
– IV Antibiotics
• Active variceal bleed – 20% mortality – 60 – 80% rebleeding
within 2 years
• Secondary prophylaxis – Band ligation – Non cardioselective
beta blockers

Prophylactic antibiotics improve outcomes in
cirrhotic patients with GI Hemorrhage
Control antibiotic Absolute rate difference
(95% CI)
Infection 45% 14% - 32%-42-23%
SBP/
Bacteremia
27% 8% -18%-26-11%
Death 24% 15% -9%-15-3%
Barnard et al J Hepatology 1998; 29: 1685

Ascites
• Increased vasodilaton affects the kidneys – Increased CO and
decreased MAP->– Stimulates
endogenous vasoconstrictors ->
• Salt and water retention– Ascites and edema
» Dilutional hyponatremia
–

Ascites
• Most common complication of cirrhosis– Pathologic
accumulation of fluid in peritoneal cavity
– Risk of developing ascites
• 50% - 70% within 10 years of diagnosis of cirrhosis
• Requirements for Ascites in cirrhosis
– Portal hypertension
• Actually sinusoidal Hypertension

Management of Ascites
• Dietary Sodium restriction – 88 meq sodium daily – 2000 mg sodium daily
• Diuretics• Combination of lasix
and spironolactone
• Spironolactone (aldactone)– Aldosterone antagonist
– Weak diuretic
– More effective than lasix alone in cirrhosis
• Furosemide (Lasix) – Loop diuretic
• Must enter the lumen of the tubule to work
– Proximal tubular secretion is impaired in cirrhosis

Refractory ascites
• Diuretic resistant• No weight loss
– Despite adequate doses of diuretics
– And salt restriction
•
• Diuretic intractable– Something precludes the use
of effective doses of diuretics• Hyponatremia • Elevated creatinine
Hepatorenal syndrome

Treatment of Refractory Ascites
• Large Volume Paracentesis– Beware of post
paracentesis circulatory dysfunction
– Can cause renal failure and
• Decreased survival
– Many advocate IV Albumin
• to prevent PPCD.
• Terlipressin *– Vasoconstrictor
• Splanchnic and systemic
– Increases effective blood volume
• Decreases renin and angiotensin secretion
• Increases renal vasodilation and perfusion
– Improves creatinine
* Not yet approved in US
Presence of VARICES and ASCITES determines prognosis
patients with cirrhosis


Hepatic Encephalopathy
• Definition– A spectrum of potentially reversible
neuropsychiatric abnormalities seen in patient with liver dysfunction and / or porto systemic shunting.
• Overt Hepatic Encephalopathy – 30-45% of patients with cirrhosis
• Minimal Hepatic Encephalopathy– Up to 80% with cirrhosis


Encephalopathy work up and diagnosis
• High index of suspicion – Physical exam – Clinical setting
• Rule out other causes of mental status changes – Intracranial process
• Check for precipitating factor– Infection
• SBP
– GI Bleed– Drugs – Renal Insufficiency – Worsening liver
function

Lactulose
• Increases stool volume
• Increased acetate and lactate change acid base balance
• pH = 5– NH3 -> NH4– Increases excretion of
fecal nitrogen
• Problems• Side effects ->
– Increased number of BMs
– Loose stools – Gas
Non compliance
Treatment of encephalopathy
Rifaximin Nonabsorbable antibiotic
Comparable efficacy to lactuloseWide bacterial activity against
aerobic and anaerobic gram-negativeand gram-positive
Superior safety profile compared with neomycin
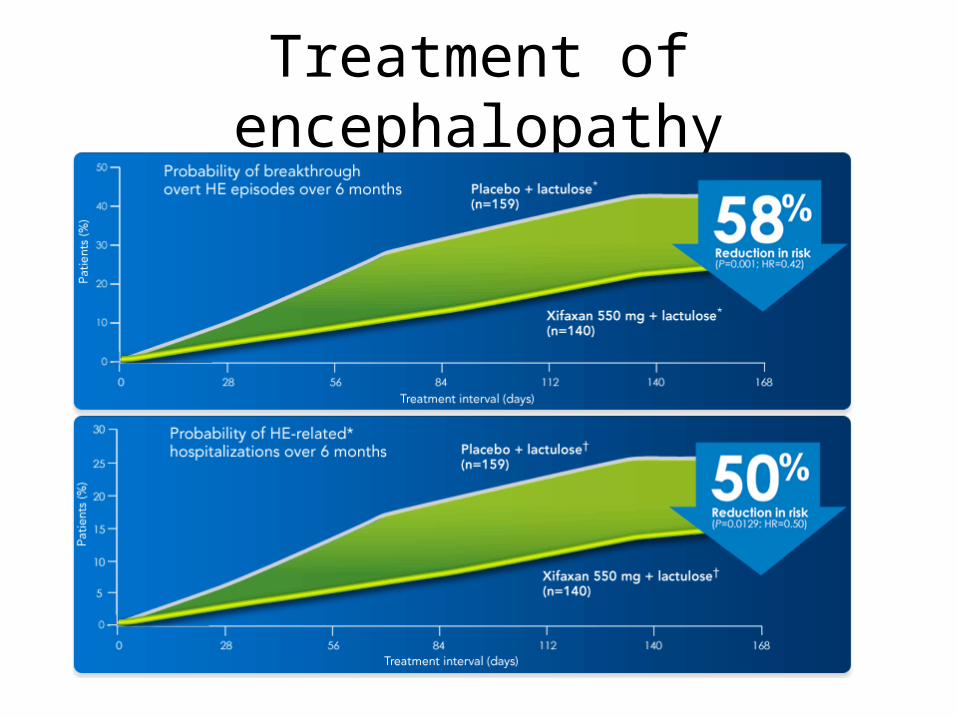
Treatment of encephalopathy

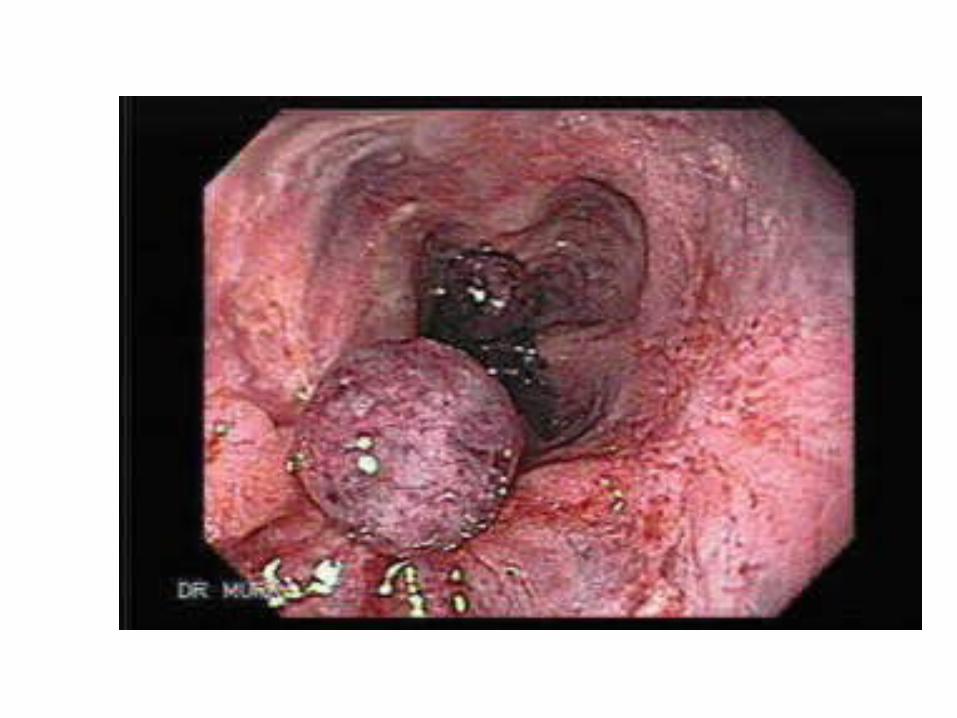
Hepatocellular carcinoma
• Surveillance recommended in all with cirrhosis– Incidence HCC varies with
cause of cirrhosis• Up to 5% per year
• Surveillance decreases mortality– detects small HCC– HCC 1-2 cm can be cured
in >50% of cases
• Patients listed for transplant with HCC– Get Priority on list – Exception points for certain
cases are available
• Must be small – One lesion < 5 cm – or < 3 lesions
• None greater than 3 cm
• No vascular invasion
• No extrahepatic lesions

Causes of Cirrhosis
• Most common • Chronic viral hepatitis
– HBV– HCV
• Alcoholic liver disease
• Hemochromatosis
• NASH– Non alcoholic
steatohepatitis
• Less common causes– Autoimmune hepatitis– Primary and secondary
biliary cirrhosis– Primary sclerosing
cholangitis– Medications– Wilson disease– Alpha-1 antitrypsin
deficiency– Granulomatous liver
disease– Polycystic liver disease– Right-sided heart failure– Veno-occlusive disease.
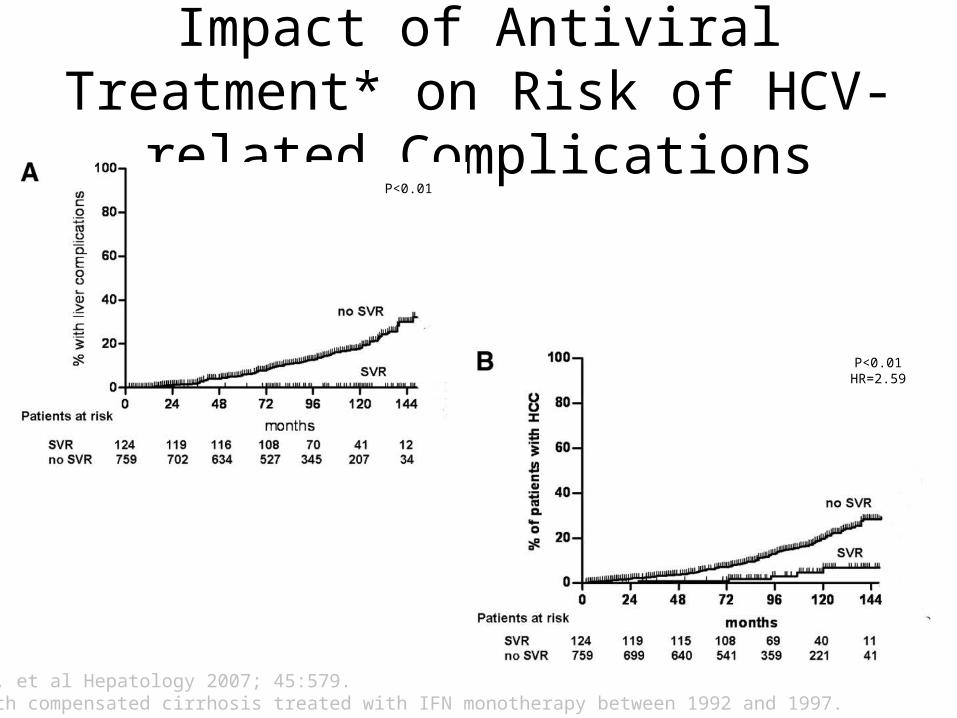
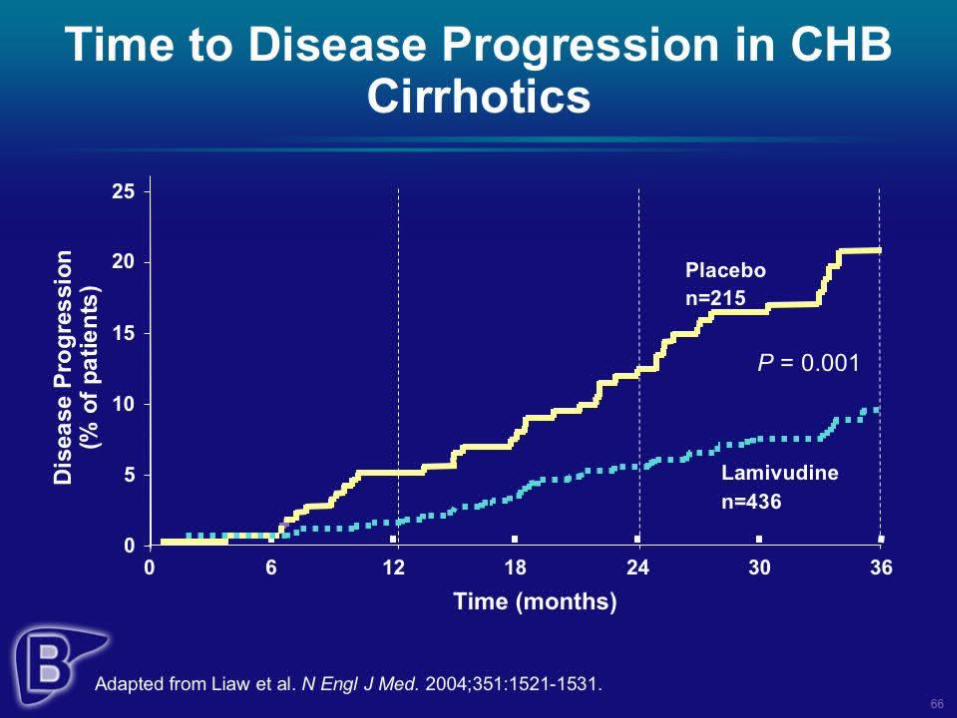
Impact of Antiviral Treatment* on Risk of HCV-related Complications
Bruno S, et al Hepatology 2007; 45:579.*Pts with compensated cirrhosis treated with IFN monotherapy between 1992 and 1997.
P<0.01
P<0.01HR=2.59

Hereditary Hemochromatosis
• Genetic disorder – Autosomal recessive– increased intestinal
iron absorption – Increased iron
deposition in • Liver • Heart • Pancreas • pituitary
• Diagnosis can be made early – Good family history – High index of
suspicion • Serum iron /TIBC• Ferritin • +/- liver biopsy

Survival in HHC
• Survival in those pre cirrhosis– if you start treatment before a person
develops cirrhosis• Is the same as control population without HHC
– 65% 20 year survival
– After cirrhosis survival is decreased• Due to complications of cirrhosis• And HCC
– From Niedarau et al. NEJM 1985

HCV: Effect of Weight Loss on Grade of Inflammation
• 19 pts HCV + steatosis• 3 month weight loss
– 5.9 kg – 16/19 ALT decrease– Decrease fasting insulin 16 –
11 mmoles/l. (p=<0.002)• 10 had paired liver biopsies ( 3-6
mos post)– Decreased Knodel fibrosis
score 3 to 1. (p=0.04)– Decreased activated stellate
cells (p=< 0.004)
Hickman IJ et al. Gut 2002;51: 89-94

Drug therapy for treatment of NASH
• Vitamin E**– Decreased hepatic
steatosis– Decreased
inflammation • No effect on fibrosis• Dose was 800 U daily
– Use with caution in pts with CAD and DM
• Obeticholic acid– Currently
investigational – Clinical trial halted
after 50% of the patients enrolled met endpoint.
• Statistically significant efficacy.*
•*Intercept press release
•**Sanyal AL et al NEJM. 2010. 362 (18) 1675

Summary
• Cirrhosis is end result of years of ongoing liver damage– We will be called on to manage complications of
cirrhosis in our daily practice• Ascites, varices, encephalopathy and HCC.
– Treatment of the most common causes of cirrhosis are emerging
• In the future we should seen decrease in cirrhosis• If we can manage the
– upcoming tsunami of NASH.


Top Related