The Cirrhosis Tsunami are we ready? Mary Patricia Pauly MD FACP AGAF Kaiser Permanente Sacramento...
59
The Cirrhosis Tsunami are we ready? Mary Patricia Pauly MD FACP AGAF Kaiser Permanente Sacramento Medical Center
-
Upload
audra-mills -
Category
Documents
-
view
214 -
download
1
Transcript of The Cirrhosis Tsunami are we ready? Mary Patricia Pauly MD FACP AGAF Kaiser Permanente Sacramento...

The Cirrhosis Tsunamiare we ready?
Mary Patricia Pauly MD FACP AGAF
Kaiser Permanente
Sacramento Medical Center


Diagnosis Diagnosis

• 45 year old elementary school teacher with cirrhosis calls in to clinic – Trouble focusing – Slow – Slurred speech – Confused

Outline• Cirrhosis
– Definition , • Survival w and wo Decompensation• causes
– Physical signs and lab signs • Portal hypertension--Anatomy and physiology• Manifestation of decompensated cirrhosis – how it fits with portal
hypertension – Ascites, variceal bleed , encephalopathy
• Only a certain percentage,
– TREATMENT OF complications of cirrhosis and portal hypertension- cancer surveillance
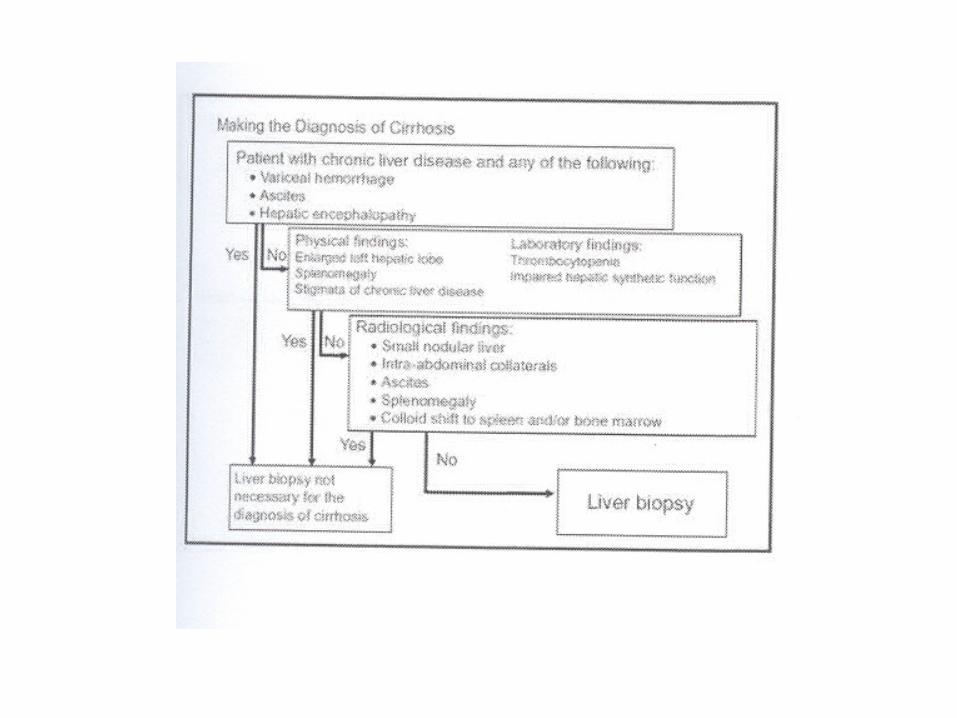
– Making the diagnosis– Prognosis –
• Childs class, MELD – Treatment may decrease incidence of cirrhosis

Cirrhosis
• Late stage of progressive hepatic fibrosis – Distortion of hepatic architecture – Regenerative nodules – Irreversible in advanced stages
• Patients with cirrhosis – Decreased life expectancy – Susceptible to complications
• Decompensation – Ascites, Variceal bleeding and encephalopathy
• Cancer– HCC and – Cholangiocarcinoma

Survival in Cirrhosis
Fattovich G, et al. Gastroenterology. 1997;112:463-472.
Compensated
After first major complication
Survival Probability
100
Pat
ien
ts (
%)
80
60
40
20
01200 12 24 36 48 60 72 84 96 108
Mos
384 65
Pts at Risk, n 376 39
34221
28811
2367
1654
1264
793
523
392
251
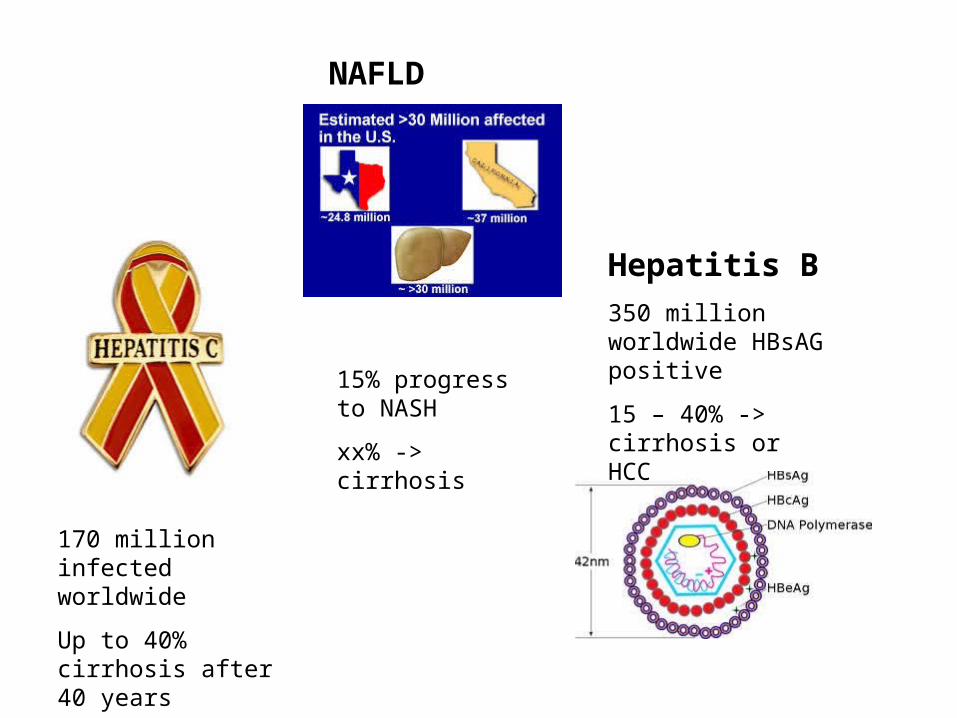
170 million infected worldwide
Up to 40% cirrhosis after 40 years
Hepatitis B
350 million worldwide HBsAG positive
15 – 40% -> cirrhosis or HCC
NAFLD
15% progress to NASH
xx% -> cirrhosis

The Cirrhosis Tsunami

Spider angiomata
Note the central pulsating arteriole surrounded by many smaller vessels or “legs.”
Pathogenesis incompletely understood
Possibilities: Alterations in sex hormone metabolism- increase in estradiol to free testosterone ratio in men.
Number and size correlate with severity of disease

Palmar erythema
Pathogenesis: It is thought to be caused by altered sex hormone metabolism

Gynecomastia
Pathogenesis: increased conversion of androstenedione ( produced in adrenals) -> estrone -> estradiol.

Dupuytren’s contractures
Due to thickening and shortening of the palmar fascia
Fibroblastic proliferation and disorderly collage deposition --> fascial thickening and flexion deformities of the fingers.
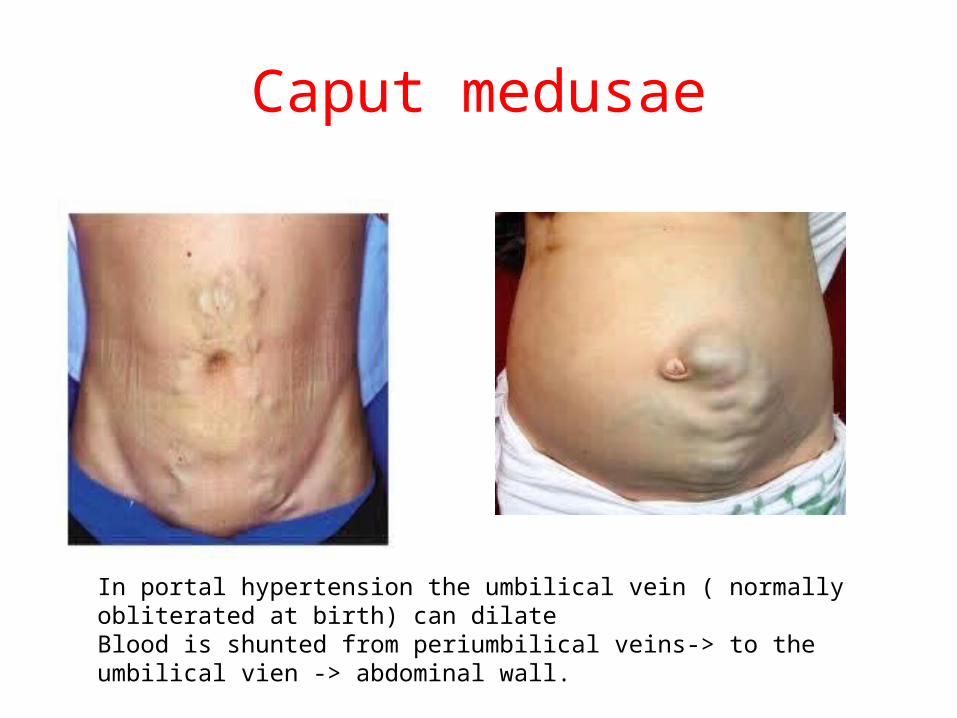
Caput medusae
In portal hypertension the umbilical vein ( normally obliterated at birth) can dilate Blood is shunted from periumbilical veins-> to the umbilical vien -> abdominal wall.

Physicial findings in cirrhosis•Physical findings
–Stigmata of portal hypertension:• Spider angiomata
• Caput medusae
• Palmar erythema
• Dupuytren’s contracture
• Gynecomastia
• Ascites
• Signs of encephalopathy– Jaundice --- does not necessarily indicate cirrhosis
» acute hepatitis
» CBD obstruction

Laboratory Finding consistent with cirrhosis
• Laboratory findings–Low platelet count
< 100 K
Low WBC and Anemia. – Splenic sequestration
–Low albumin–Elevated prothrombin
time –Elevated Bilirubin
– Liver biopsy – Non invasive markers
of Fibrosis • Fibrosure/fibrospect
F3-4• Fibroscan and similar
technologies measures elasticity
– >12.5 Kpa
• APRI > 2
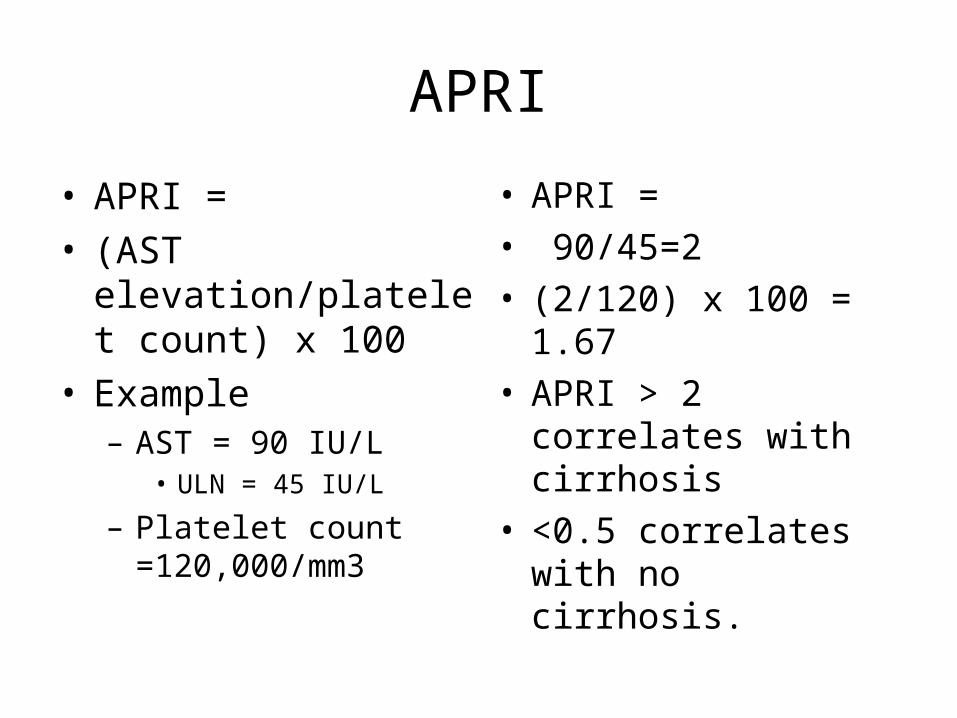
APRI
• APRI = • (AST elevation/platelet
count) x 100• Example
– AST = 90 IU/L • ULN = 45 IU/L
– Platelet count =120,000/mm3
• APRI =• 90/45=2• (2/120) x 100 = 1.67• APRI > 2 correlates
with cirrhosis • <0.5 correlates with
no cirrhosis.


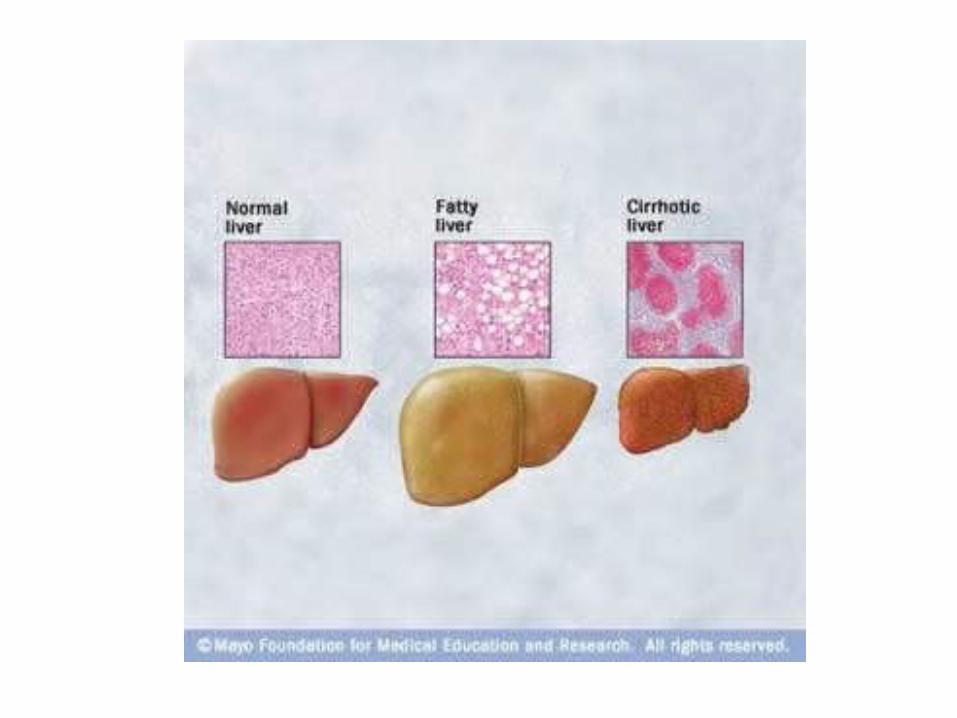
The Liver: Progression of Disease
TIME course 10 --> 40 years .

Hepatic Fibrosis: Metavir score


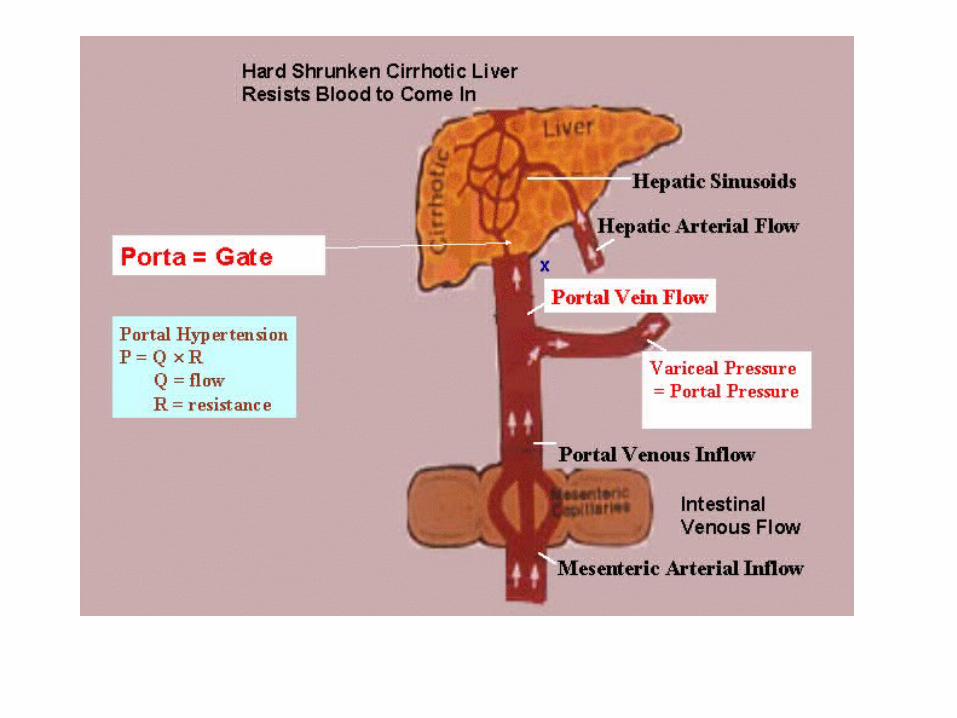

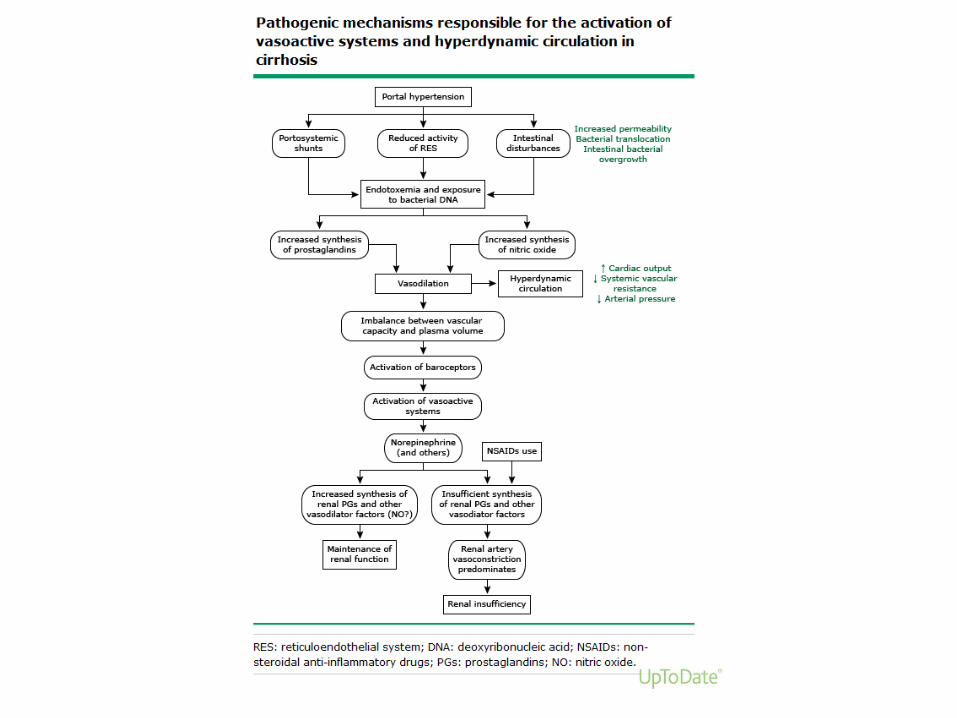
Portal Hypertension
• More than mechanical obstruction • Vasodilation
– increased
» Glucagon
» Nitrous oxide
– Decreased SVR
– Decreased MAP
– Increased collaterals
• Increased CO– Increased portal blood
flow
– Hyperdynamic circulation

Cirrhosis
Increased resistance to portal flow
Increased portal pressure
Varices
Decreased splanchnic arteriolar resistance
Increased portal blood flow
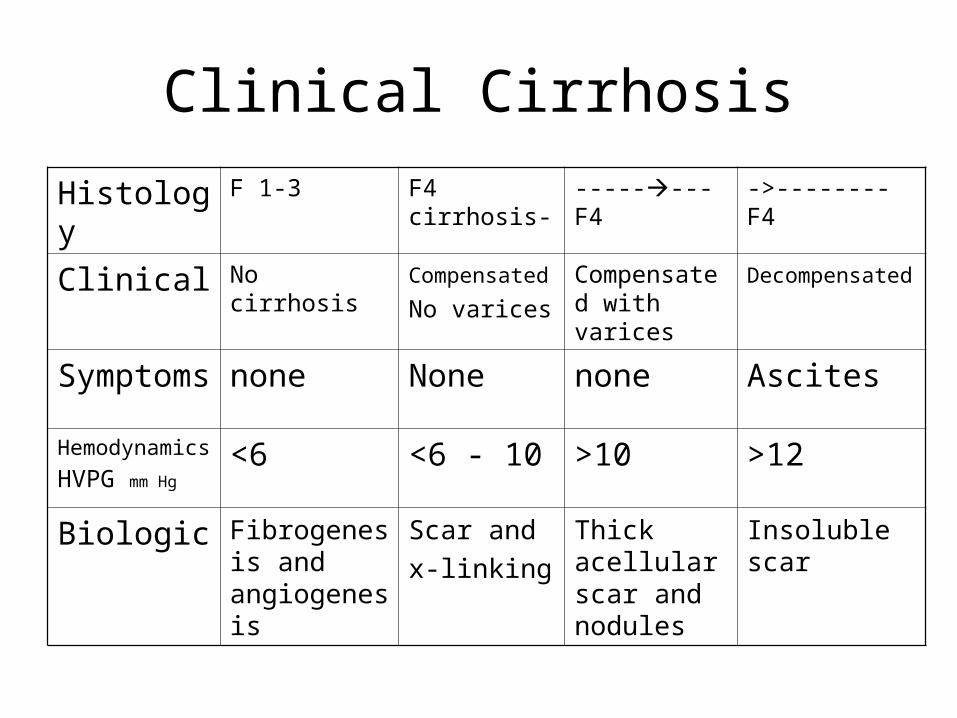
Clinical Cirrhosis
Histology F 1-3 F4 cirrhosis- --------F4 ->--------F4
Clinical No cirrhosis Compensated
No varices
Compensated with varices
Decompensated
Symptoms none None none Ascites
Hemodynamics
HVPG mm Hg<6 <6 - 10 >10 >12
Biologic Fibrogenesis and angiogenesis
Scar and
x-linking
Thick acellular scar and nodules
Insoluble scar

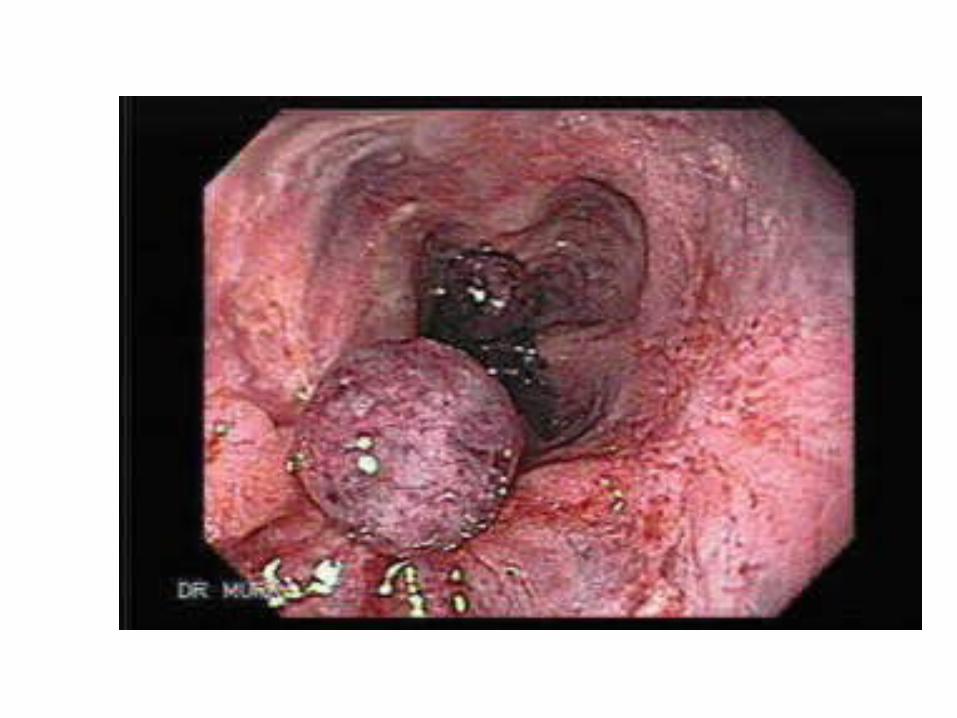
Gastro esophageal varices
• 50% of patients with cirrhosis
• 5-15% Risk of bleeding per year – Directly related to
portal pressure– SIZE if most important
predictor of bleeding *• Large varices 30%• Small varices 7%
• Recommended EGD• Surveillance for varices
in cirrhosis
– If no varices –• Recheck 2-3 y
– If small varices • Recheck 1-2 y
– If large varices • Primary prophylaxis
*over 2 years

Esophageal varices
Varices 2 y risk of bleeding without BB
2 y risk of bleeding with BB
Small 7% 2%
Large 30% 14%
• Non bleeding varices• Primary prophylaxis
– Non cardioselective beta- blockers
• Propranolol• Nadolol
• Titrate to 25% decrease in HR from baseline
– EVBL• if intolerant of BB

Treatment of varices
• Actively bleeding– Band ligation– Octreotide
• ->Splanchnic vasoconstriction and Decreased portal blood flow
– Inhibits release of vasodilator hormones (glucagon)
– IV Antibiotics
• Active variceal bleed – 20% mortality – 60 – 80% rebleeding
within 2 years
• Secondary prophylaxis – Band ligation – Non cardioselective
beta blockers

Prophylactic antibiotics improve outcomes in
cirrhotic patients with GI Hemorrhage
Control antibiotic Absolute rate difference
(95% CI)
Infection 45% 14% - 32%-42-23%
SBP/
Bacteremia
27% 8% -18%-26-11%
Death 24% 15% -9%-15-3%
Barnard et al J Hepatology 1998; 29: 1685

Ascites
• Increased vasodilaton affects the kidneys – Increased CO and
decreased MAP->– Stimulates
endogenous vasoconstrictors ->
• Salt and water retention– Ascites and edema
» Dilutional hyponatremia
–

Ascites
• Most common complication of cirrhosis– Pathologic
accumulation of fluid in peritoneal cavity
– Risk of developing ascites
• 50% - 70% within 10 years of diagnosis of cirrhosis
• Requirements for Ascites in cirrhosis
– Portal hypertension
• Actually sinusoidal Hypertension

Management of Ascites
• Dietary Sodium restriction – 88 meq sodium daily – 2000 mg sodium daily
• Diuretics• Combination of lasix
and spironolactone
• Spironolactone (aldactone)– Aldosterone antagonist
– Weak diuretic
– More effective than lasix alone in cirrhosis
• Furosemide (Lasix) – Loop diuretic
• Must enter the lumen of the tubule to work
– Proximal tubular secretion is impaired in cirrhosis

Refractory ascites
• Diuretic resistant• No weight loss
– Despite adequate doses of diuretics
– And salt restriction
•
• Diuretic intractable– Something precludes the use
of effective doses of diuretics• Hyponatremia • Elevated creatinine
Hepatorenal syndrome

Treatment of Refractory Ascites
• Large Volume Paracentesis– Beware of post
paracentesis circulatory dysfunction
– Can cause renal failure and
• Decreased survival
– Many advocate IV Albumin
• to prevent PPCD.
• Terlipressin *– Vasoconstrictor
• Splanchnic and systemic
– Increases effective blood volume
• Decreases renin and angiotensin secretion
• Increases renal vasodilation and perfusion
– Improves creatinine
* Not yet approved in US
Presence of VARICES and ASCITES determines prognosis
patients with cirrhosis


Hepatic Encephalopathy
• Definition– A spectrum of potentially reversible
neuropsychiatric abnormalities seen in patient with liver dysfunction and / or porto systemic shunting.
• Overt Hepatic Encephalopathy – 30-45% of patients with cirrhosis
• Minimal Hepatic Encephalopathy– Up to 80% with cirrhosis


Encephalopathy work up and diagnosis
• High index of suspicion – Physical exam – Clinical setting
• Rule out other causes of mental status changes – Intracranial process
• Check for precipitating factor– Infection
• SBP
– GI Bleed– Drugs – Renal Insufficiency – Worsening liver
function

Lactulose
• Increases stool volume
• Increased acetate and lactate change acid base balance
• pH = 5– NH3 -> NH4– Increases excretion of
fecal nitrogen
• Problems• Side effects ->
– Increased number of BMs
– Loose stools – Gas
Non compliance
Treatment of encephalopathy
Rifaximin Nonabsorbable antibiotic
Comparable efficacy to lactuloseWide bacterial activity against
aerobic and anaerobic gram-negativeand gram-positive
Superior safety profile compared with neomycin
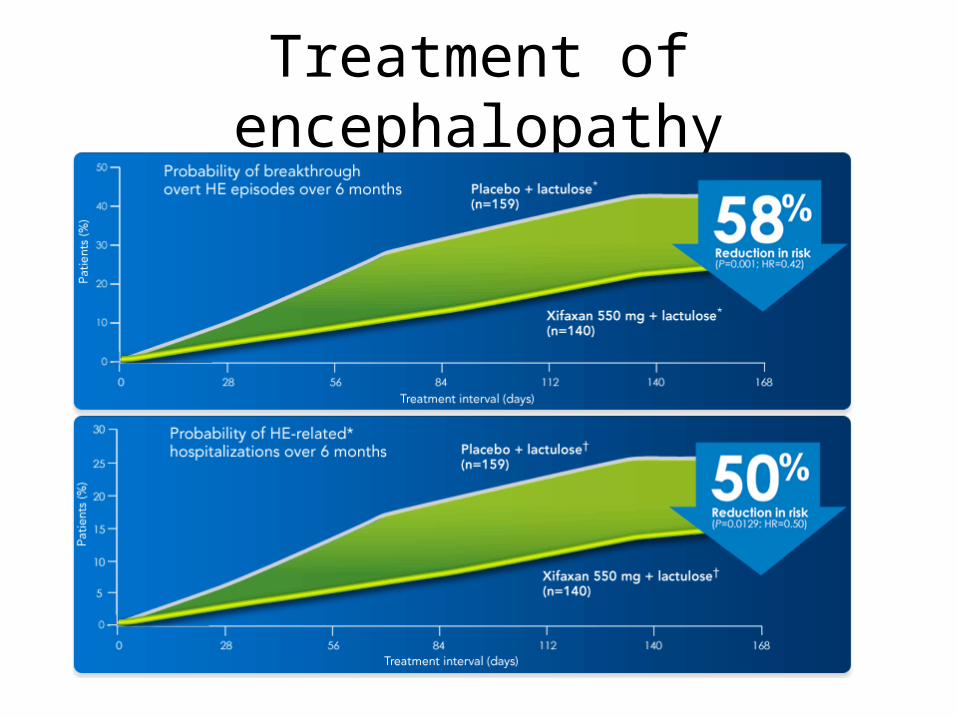
Treatment of encephalopathy

Hepatocellular carcinoma
• Surveillance recommended in all with cirrhosis– Incidence HCC varies with
cause of cirrhosis• Up to 5% per year
• Surveillance decreases mortality– detects small HCC– HCC 1-2 cm can be cured
in >50% of cases
• Patients listed for transplant with HCC– Get Priority on list – Exception points for certain
cases are available
• Must be small – One lesion < 5 cm – or < 3 lesions
• None greater than 3 cm
• No vascular invasion
• No extrahepatic lesions

Causes of Cirrhosis
• Most common • Chronic viral hepatitis
– HBV– HCV
• Alcoholic liver disease
• Hemochromatosis
• NASH– Non alcoholic
steatohepatitis
• Less common causes– Autoimmune hepatitis– Primary and secondary
biliary cirrhosis– Primary sclerosing
cholangitis– Medications– Wilson disease– Alpha-1 antitrypsin
deficiency– Granulomatous liver
disease– Polycystic liver disease– Right-sided heart failure– Veno-occlusive disease.
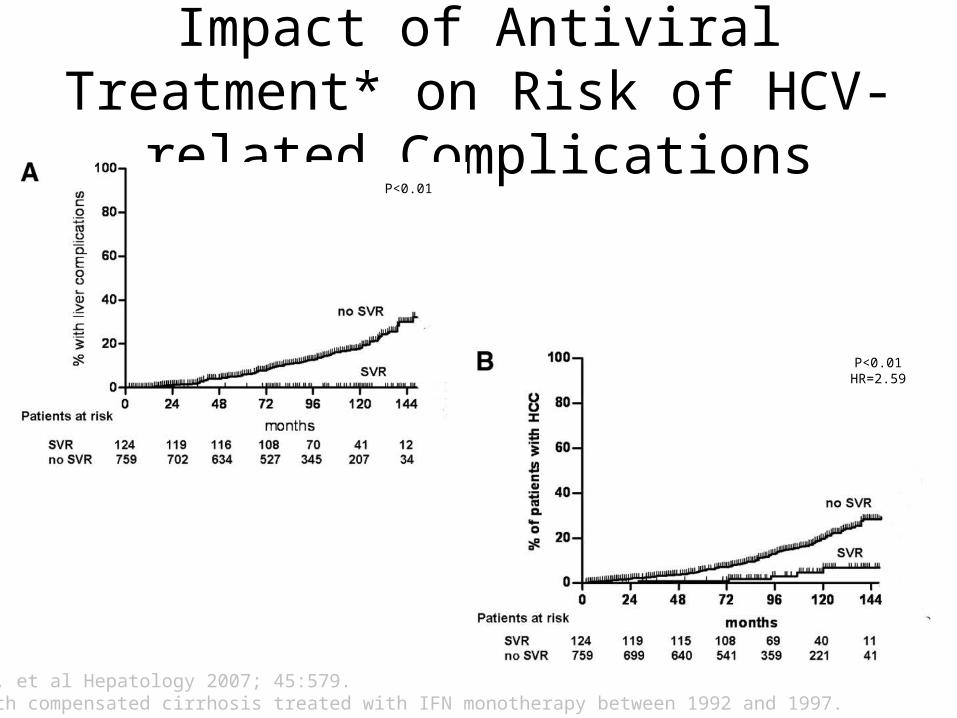
Impact of Antiviral Treatment* on Risk of HCV-related Complications
Bruno S, et al Hepatology 2007; 45:579.*Pts with compensated cirrhosis treated with IFN monotherapy between 1992 and 1997.
P<0.01
P<0.01HR=2.59

Hereditary Hemochromatosis
• Genetic disorder – Autosomal recessive– increased intestinal
iron absorption – Increased iron
deposition in • Liver • Heart • Pancreas • pituitary
• Diagnosis can be made early – Good family history – High index of
suspicion • Serum iron /TIBC• Ferritin • +/- liver biopsy

Survival in HHC
• Survival in those pre cirrhosis– if you start treatment before a person
develops cirrhosis• Is the same as control population without HHC
– 65% 20 year survival
– After cirrhosis survival is decreased• Due to complications of cirrhosis• And HCC
– From Niedarau et al. NEJM 1985

HCV: Effect of Weight Loss on Grade of Inflammation
• 19 pts HCV + steatosis• 3 month weight loss
– 5.9 kg – 16/19 ALT decrease– Decrease fasting insulin 16 –
11 mmoles/l. (p=<0.002)• 10 had paired liver biopsies ( 3-6
mos post)– Decreased Knodel fibrosis
score 3 to 1. (p=0.04)– Decreased activated stellate
cells (p=< 0.004)
Hickman IJ et al. Gut 2002;51: 89-94

Drug therapy for treatment of NASH
• Vitamin E**– Decreased hepatic
steatosis– Decreased
inflammation • No effect on fibrosis• Dose was 800 U daily
– Use with caution in pts with CAD and DM
• Obeticholic acid– Currently
investigational – Clinical trial halted
after 50% of the patients enrolled met endpoint.
• Statistically significant efficacy.*
•*Intercept press release
•**Sanyal AL et al NEJM. 2010. 362 (18) 1675

Summary
• Cirrhosis is end result of years of ongoing liver damage– We will be called on to manage complications of
cirrhosis in our daily practice• Ascites, varices, encephalopathy and HCC.
– Treatment of the most common causes of cirrhosis are emerging
• In the future we should seen decrease in cirrhosis• If we can manage the
– upcoming tsunami of NASH.