







Languages
Pages
Legal


RAPPORTEUR SESSION
HIV/STD/TB/VIRAL HEPATITIS SYMPOSIUM
SEPTEMBER 17-18, 2014

What Is PCSI?
A mechanism for organizing and blending interrelated health issues, activities, and prevention strategies to facilitate comprehensive delivery of services that are based on five principles:
• Appropriateness• Effectiveness• Flexibility• Accountability• Acceptability
2
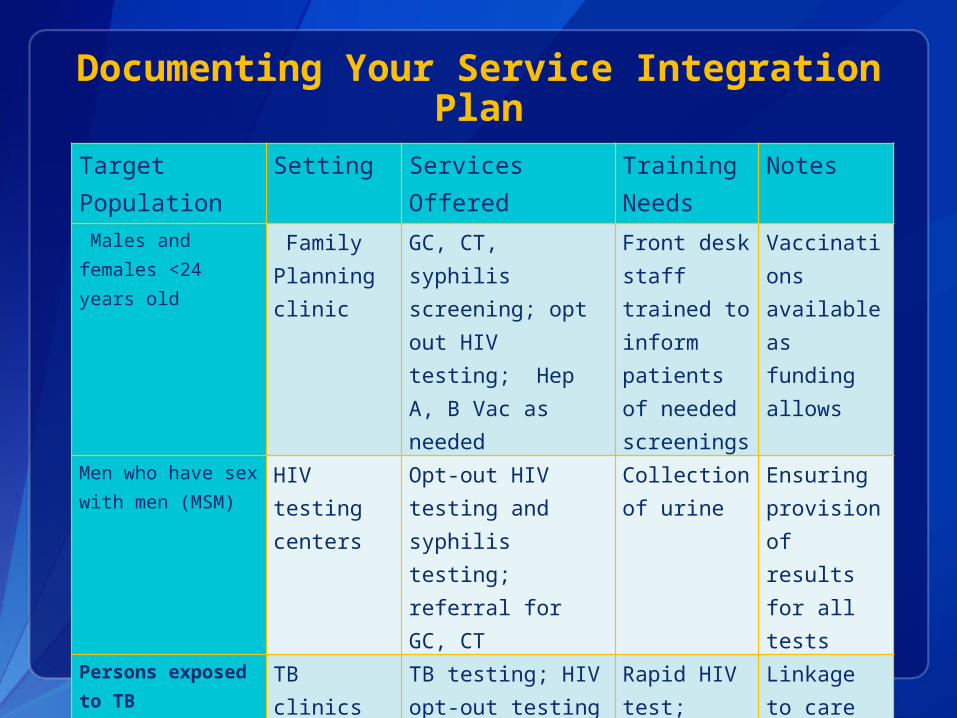
Documenting Your Service Integration Plan
Target Population Setting Services Offered Training Needs
Notes
Males and females <24 years old
Family Planning clinic
GC, CT, syphilis screening; opt out HIV testing; Hep A, B Vac as needed
Front desk staff trained to inform patients of needed screenings
Vaccinations available as funding allows
Men who have sex with men (MSM)
HIV testing centers
Opt-out HIV testing and syphilis testing; referral for GC, CT
Collection of urine
Ensuring provision of results for all tests
Persons exposed to TB
TB clinics TB testing; HIV opt-out testing
Rapid HIV test; providing positive results
Linkage to care plan needed for HIV+ results
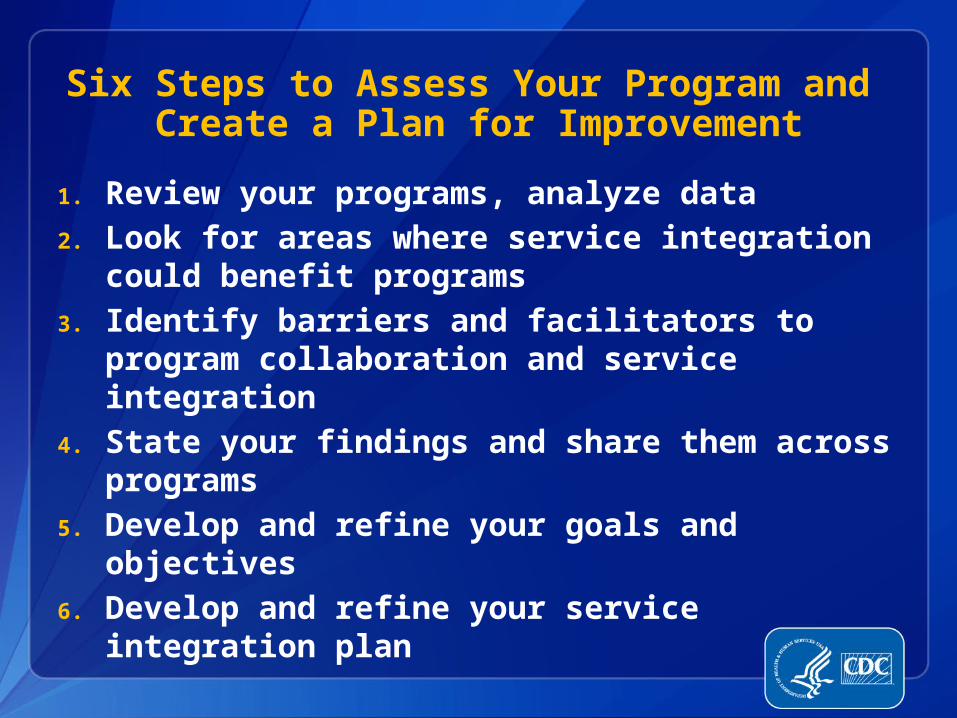
Six Steps to Assess Your Program and Create a Plan for Improvement
1. Review your programs, analyze data2. Look for areas where service integration
could benefit programs3. Identify barriers and facilitators to program
collaboration and service integration4. State your findings and share them across
programs5. Develop and refine your goals and
objectives6. Develop and refine your service integration
plan

Coordination Across Payers:Translating Coverage into Care and Treatment
SERVICE QHP MEDICAID RW/ ADAP/CDC
HIV Testing Continue to cover in certain settings
RX Cost-sharing assistance
MEDICAL CASE MANAGEMENT
ORAL HEALTH
LABS Cost-sharing assistance
MENTAL HEALTH SERVICES
Cost-sharing assistance
SUBSTANCE ABUSE TREATMENT
Cost-sharing assistance
HIV PRIMARY CARE Cost-sharing assistance
MEDICAL TRANSPORTATION Limited Coverage
INPATIENT HOSPITAL SERVICES
Adapted from West Virginia Ryan White Part B Program

Leveraging New Resources/Payers: It’s Complicated!
Service covered?
Provider in network and credentialed with payer?
Does reimbursement
cover cost of service?
What is impact on
client/patient?
Translate public health service into language of payers/insurance (e.g., CPT codes)
Assess provider requirements (licensed provider; provider supervision; provider recommendation; setting)
Compare reimbursement rate (within capitation or FFS) with cost of providing service
Are privacy and confidentiality concerns addressed?
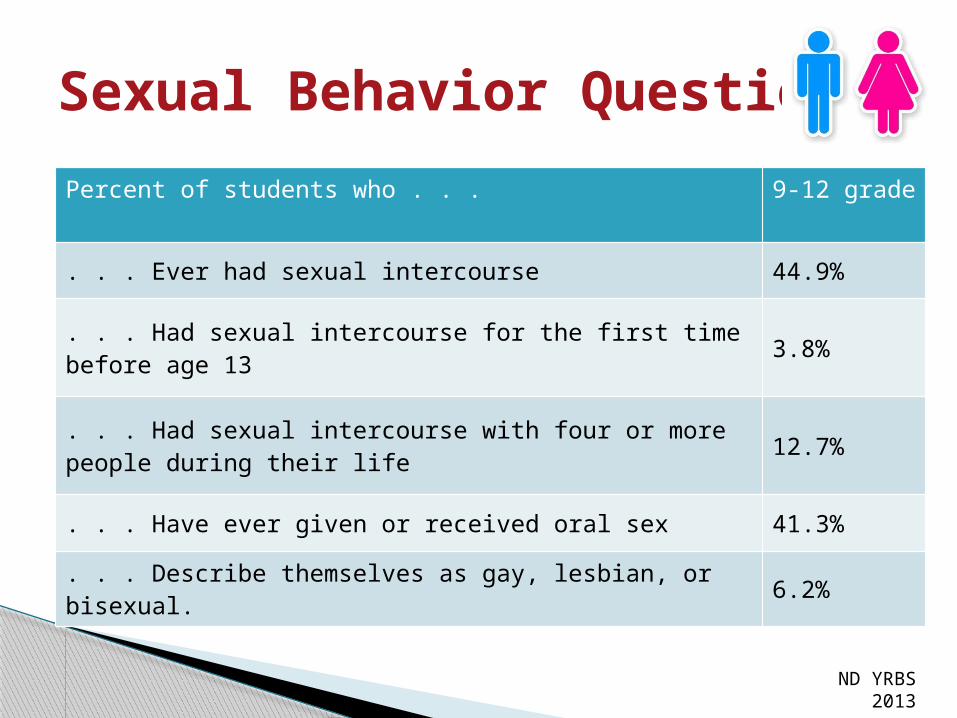
Sexual Behavior Questions
Percent of students who . . . 9-12 grade
. . . Ever had sexual intercourse 44.9%
. . . Had sexual intercourse for the first time before age 13 3.8%
. . . Had sexual intercourse with four or more people during their life 12.7%
. . . Have ever given or received oral sex 41.3%
. . . Describe themselves as gay, lesbian, or bisexual. 6.2%
ND YRBS 2013

Sexual Behavior QuestionsPercent of students who . . . 9-12 grade
. . . Have ever been tested for a sexually transmitted disease (STD) including HIV, the virus that causes AIDS. 12.8%
. . . Have ever had the HPV vaccine, a vaccine to prevent human papillomavirus or HPV infection. 35.6%
. . . Whose parents or other adults in their family talked with them about what they expect them to do or not do when it comes to sex.
58.4%
. . . Have ever had sex education in school. 74.0%
ND YRBS 2013
OUTBREAK THEMES
1. Contact Investigation
2. Training
3. Continuing Education
4. Incentives – No Walmart
5. Collaboration & Communication
PARTNERSHIP DEVELOPMENT
North Dakota Department of Agriculture
Youth Services – Police Department
North Dakota Department of Health
Emergency Preparedness and Response Immunization Program
Refugee Health Providers
Schools and Health Educators
North Dakota Department of Health Immunization Program
HPV Vaccine: Cancer prevention
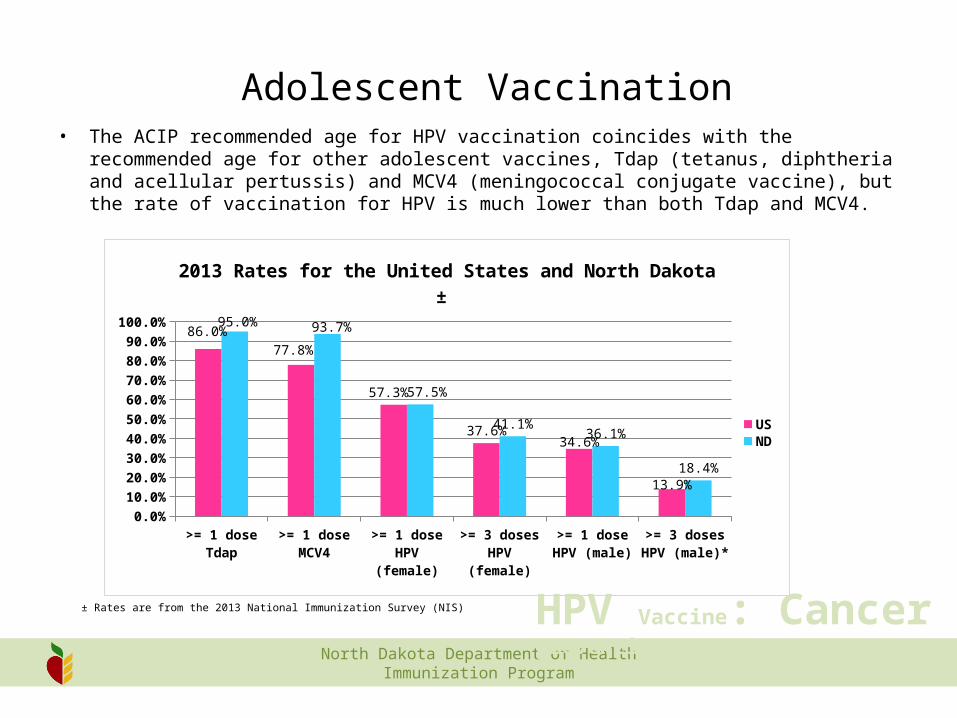
Adolescent Vaccination• The ACIP recommended age for HPV vaccination coincides with the recommended age for
other adolescent vaccines, Tdap (tetanus, diphtheria and acellular pertussis) and MCV4 (meningococcal conjugate vaccine), but the rate of vaccination for HPV is much lower than both Tdap and MCV4.
>= 1 dose Tdap >= 1 dose MCV4 >= 1 dose HPV (female)
>= 3 doses HPV (female)
>= 1 dose HPV (male)
>= 3 doses HPV (male)*
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
86.0%
77.8%
57.3%
37.6%34.6%
13.9%
95.0% 93.7%
57.5%
41.1%36.1%
18.4%
2013 Rates for the United States and North Dakota ±
USND
± Rates are from the 2013 National Immunization Survey (NIS)
North Dakota Department of Health Immunization Program
HPV Vaccine: Cancer prevention
Coming up! New HPV vaccine
o Merck is in the process of licensing a new HPV vaccine.9-valent HPV vaccine (V503) o V503 includes five more HPV types (31, 33, 45, 52, 58) in
addition to the four original HPV types (6, 11, 16, 18) in GARDASIL.
o In clinical trials it prevented approximately 97 percent of cervical, vaginal and vulvar pre-cancers caused by HPV types 31, 33, 45, 52, and 58.
o ACIP may recommend the vaccine in 2015.

North Dakota Department of Health Immunization Program
HPV Vaccine: Cancer prevention
Number of TB Cases inU.S.-born vs. Foreign-born Persons,
United States, 1993–2013*
*Updated as of June 11, 2014.
No.
of C
ases
19931994
19951996
19971998
19992000
20012002
20032004
20052006
20072008
20092010
20112012
20130
5,000
10,000
15,000
20,000
U.S.-born Foreign-born

National Veterinary Services Laboratories – Suelee Robbe Austerman
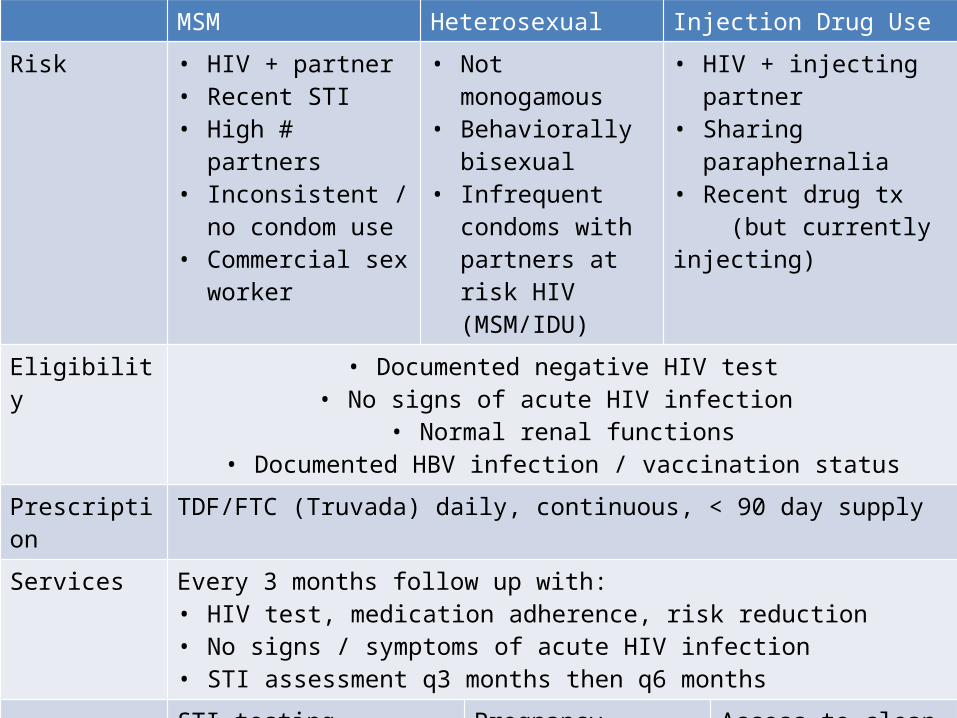
MSM Heterosexual Injection Drug Use
Risk • HIV + partner• Recent STI• High # partners• Inconsistent / no
condom use • Commercial sex
worker
• Not monogamous• Behaviorally
bisexual• Infrequent
condoms with partners at risk HIV (MSM/IDU)
• HIV + injecting partner• Sharing paraphernalia• Recent drug tx (but currently injecting)
Eligibility • Documented negative HIV test• No signs of acute HIV infection
• Normal renal functions• Documented HBV infection / vaccination status
Prescription TDF/FTC (Truvada) daily, continuous, < 90 day supply
Services Every 3 months follow up with: • HIV test, medication adherence, risk reduction • No signs / symptoms of acute HIV infection • STI assessment q3 months then q6 months
STI testing Pregnancy test / intent q-3 mos
Access to clean needlesDrug rx services
NDDOH FUTURE ACTIVITIES Educate Providers: Website, Fundamentals Online
ACA – Resources for Building Billing Capacity
Support on how best to integrate services within your facility to leverage new funding source opportunities
Work to overcome issues related to how EOB and insurance utilization information is sent for covered services
Evaluation – Program Improvement and Policy Decision
Data Reporting Resource for Local Epidemiological and Data Needs
Outbreak Response Plans for HIV.STD.TB.Viral Hepatitis
Working with DPI on Opportunities to Provide Resources for Schools and Policy Initiatives

CLOSING REMINDERS CEUs
Turn in on Registration Desk Certificate will be emailed
Our Program Information on the Back of Agenda
Please Turn in Evaluation Form
Parking Validation – Yellow Cards
Lunch N’ Learn – September 24th: HIV (CME Credits)
THANK YOU for Coming and Safe Travels!