






Languages
Pages
Legal


LearningNetwork
Facilit
ate
.
Edu
cate
.
Collaborate
.
ISS
UE
7,
DE
CE
MB
ER
2013
Vio
len
ce A
gain
st
Wo
men
wit
h
Dis
Ab
ilit
ies a
nd
Deaf
Wo
men
We a
re p
leased t
o h
ave p
art
nere
d w
ith D
AW
N-R
AF
H C
an
ad
a
for
this
exte
nded,
accessib
le n
ew
sle
tter
that
focuses o
n t
he
under-
recogniz
ed,
under-
researc
hed a
nd u
nder-
resourc
ed
socia
l concern
--
vio
lence a
gain
st
wom
en w
ith d
isA
bili
ties a
nd
Deaf
wom
en.
We h
ighlig
ht
the inte
rsectional conte
xt
of
vio
lence
experienced b
y w
om
en w
ith d
isA
bili
ties,
dra
w o
n liv
ed e
xperie
nce,
and p
rovid
e s
tatistics a
nd r
esourc
es.
Ab
leis
m –
A F
orm
of
Vio
len
ce A
gain
st
Wo
men
B
y F
ran
Od
ett
e
Able
ism
and a
ble
ist
vie
ws a
re ideas/b
elie
fs t
hat
are
based o
n t
he
assum
ption t
hat
the ‘able
-body’ is
favoure
d/p
refe
rred o
ver
the
dis
able
d b
ody.1
,2 S
imila
r to
the e
xperience o
f ra
cis
m,
hom
ophobia
/tr
ansphobia
and s
exis
m,
socia
lly c
onstr
ucte
d c
hara
cte
ristics o
f dis
Abili
ty p
ositio
n p
eople
with d
isA
bili
ties a
s a
n ‘in
ferior’ g
roup t
o
non-d
isable
d p
eople
.2,3 D
isable
d p
eople
have a
bili
ties t
hat
diffe
r fr
om
the m
ajo
rity
. T
his
doesn’t m
ean t
hat
we m
inim
ize o
r ig
nore
the
impairm
ent,
but
for
the m
ost
part
, if t
he r
ight
support
s a
re in
pla
ce,
all
people
can c
ontr
ibute
to t
heir c
om
munity.
Able
ism
adhere
s t
o t
he “
medic
al m
odel” w
here
by p
eople
/wom
en a
re
defined b
y t
heir d
isA
bili
ty a
nd w
here
the f
ocus is o
n t
he indiv
idual’s
devia
tion f
rom
the “
norm
”, r
ath
er
than r
ecogniz
ing e
very
one’s
in
div
idualit
y a
nd s
pecific
sets
of
experiences.
One o
f th
e p
rob
lem
s
with t
he m
edic
al m
odel is
that
we a
re e
ncoura
ged t
o d
efine
people
by t
heir im
pairm
ent
rath
er
than s
eein
g t
he p
ers
on f
irst.
“S
imila
rly,
audis
m c
an b
e d
efined a
s t
he d
evalu
ation o
f people
who a
re D
eaf,
deafe
ned o
r hard
of
hearing. A
n e
xam
ple
of
this
would
be a
ssum
ing
that
sig
n language is a
n infe
rior
language a
nd/o
r th
e c
ultura
l w
ays o
f D
eaf
people
are
som
ehow
infe
rior”
.4
Myth
olo
gie
s a
bout
dis
Abili
ty a
nd g
endere
d v
iole
nce a
bound f
or
wom
en liv
ing w
ith im
pairm
ents
and a
ble
ism
dic
tate
s t
he k
inds o
f serv
ices
wom
en w
ith d
isA
bili
tes h
ave a
vaila
ble
and a
re a
ble
to
access.
For
exam
ple
, lim
ited a
ccess t
o s
exual health info
rmation f
or
wom
en w
ith d
isA
bili
ties is b
ased o
n t
he b
elie
f th
at
dis
able
d w
om
en
CO
NT
INU
ED
ON
PA
GE
2,
SE
E A
BL
EIS
M
1 D
isabili
ty S
tudie
s f
or
Teachers
, “R
eassig
nin
g M
eanin
g”,
Cente
r on H
um
an P
olic
y,
2 L
into
n,
S.
(1998).
C
laim
ing D
isabili
ty.
New
York
, N
Y:
NY
U P
ress.
3 “
Reassig
nin
g M
eanin
g”,
pg.
14 N
elli
e’s
Positi
on P
aper
on A
ccessib
ility
: W
om
en w
ith D
isabili
ties a
nd D
eaf W
om
en (
Marc
h 2
013),
pg. 1
htt
p:/
/dev.
innovachannel.in
fo/n
elli
es.o
rg/w
p-c
onte
nt/
uplo
ads/2
013/0
3/N
elli
es-P
ositio
n-P
aper.
LearningNetwork
Funded b
y:
Gu
est
Ed
ito
rs f
rom
DA
WN
-RA
FH
Can
ad
a
Bo
nn
ie B
rayto
n, N
ational E
xecutive D
irecto
r
Fra
n O
dett
e, S
enio
r R
esearc
h C
onsultant
D
ori
s R
aja
n, S
enio
r P
roje
ct
Directo
r
Th
e L
earn
ing
Netw
ork
Team
Lin
da B
aker,
Learn
ing D
irecto
r
An
na-L
ee S
traatm
an
, R
esearc
h A
ssocia
te
Marc
ie C
am
pb
ell
, R
esearc
h A
ssocia
te
E
lsa B
arr
eto
, M
ulti-m
edia
Sp
ecia
list
Ple
ase e
valu
ate
us!!
!Let
us k
now
what
you t
hin
k.
Your
input
is im
port
ant
to u
s.
Ple
ase c
om
ple
te t
his
brief
surv
ey o
n y
our
thoughts
of
the c
urr
ent
new
sle
tter.
CLIC
K H
ER
E
vaw
learn
ing
netw
ork
.ca
facebook.c
om
/TheLearn
ingN
etw
ork
twitte
r.com
/learn
toendabuse
No
w A
vail
ab
le o
n v
aw
learn
ing
netw
ork
.ca
Ab
leis
m –
A F
orm
of
Vio
len
ce A
gain
st
Wo
men
:
Cri
tical
Refl
ecti
on
s b
y F
ran
Od
ett
eLearn
ing N
etw
ork
Brief
11
Vio
len
ce A
gain
st
Wo
men
wit
h D
isA
bil
itie
s a
nd
Deaf
Wo
men
:
An
Overv
iew
Learn
ing N
etw
ork
Brief
12
Vio
len
ce A
gain
st
Wo
men
wit
h D
isA
bil
itie
s a
nd
Deaf
Wo
men
Netw
ork
Are
a

Bu
ild
ing
th
e E
vid
en
ce.
A
report
on t
he s
tatu
s o
f polic
y a
nd p
ractice
in r
espondin
g t
o v
iole
nce a
gain
st
wom
en w
ith
dis
abili
ties in V
icto
ria.
This
2008 A
ustr
alia
n r
eport
dis
cusses h
ow
curr
ent
polic
ies a
nd p
ractices
recogniz
e a
nd p
rovid
e f
or
wom
en w
ith d
isA
bili
ties e
xperiencin
g v
iole
nce.
Recom
mendations inclu
de:
colla
bora
tion b
etw
een d
isA
bili
ty a
nd v
iole
nce
secto
rs;
accessib
le s
erv
ices;
education f
or
wom
en w
ith d
isA
bili
ties a
nd
the c
om
munity a
bout
vio
lence a
nd a
vaila
ble
serv
ices;
housin
g o
ptions;
and t
rain
ing v
iole
nce w
ork
ers
in d
isA
bili
ty a
ware
ness.
Do
ub
le O
pp
ressio
n:
V
iole
nce A
gain
st
Dis
able
d W
om
en.
A
resourc
e p
ack f
or
pra
ctitioners
.T
his
UK
resourc
e d
iscusses t
he c
onte
xt
and p
revale
nce o
f vio
lence
again
st
wom
en w
ith d
isA
bili
ties;
the m
edic
al and s
ocia
l m
od
els
of
dis
Abili
ty;
types o
f vio
lence e
xperienced b
y w
om
en w
ith d
isA
bili
ties;
how
to m
ake s
upport
serv
ices m
ore
accessib
le;
and s
afe
ty p
lannin
g.
Vio
len
ce A
gain
st
Wo
men
wit
h D
isab
ilit
ies –
V
iole
nce P
reven
tio
n R
evie
wT
his
2011 C
anadia
n r
eport
identifies k
ey b
arr
iers
and initia
tives
addre
ssin
g t
he n
eeds o
f w
om
en w
ith d
isA
bili
ties liv
ing w
ith v
iole
nce.
Recom
mendations inclu
de:
cre
ating p
rogra
ms;
mappin
g o
ut
support
serv
ices;
develo
pin
g b
est
pra
ctice t
ools
to e
ducate
, tr
ain
, and s
upport
w
om
en w
ith d
isA
bili
ties a
nd g
uid
e t
he w
ork
of
pro
fessio
nals
; and
develo
pin
g a
national str
ate
gy t
o a
ddre
ss v
iole
nce a
gain
st
wo
men w
ith
dis
Abili
ties.
Wo
men
wit
h D
isA
bil
itie
s a
nd
D
eaf
Wo
men
Pro
gra
mS
pringtide R
esourc
es d
evelo
ped t
he W
om
en w
ith D
isA
bili
ties a
nd D
eaf
Wom
en P
rogra
m t
o o
verc
om
e b
arr
iers
to s
erv
ices inclu
din
g a
ccessib
ility
audits,
agency c
onsultation,
train
ing,
resourc
e d
evelo
pm
ent,
an
d
leaders
hip
develo
pm
ent.
7
LearningNetwork
LearningNetwork
2
will
not
be s
exually
active a
nd t
here
fore
, do n
ot
need r
elia
ble
sexual health a
nd r
epro
ductive h
ealth info
rmation.
This
in
cre
ases o
ur
risk f
or
sexual and p
hysic
al abuse.
Able
ism
sig
nific
antly im
pacts
debate
s r
egard
ing e
uth
anasia
, w
hic
h h
as r
eceiv
ed a
gre
at
deal of
media
att
ention r
ecently,
because t
he e
xperience o
f liv
ing w
ith a
dis
Abili
ty is a
t w
ors
t de-v
alu
ed a
nd m
isunders
tood a
nd a
t best,
ignore
d in t
hese
dis
cussio
ns.
In Q
uebec,
eff
ort
s b
y d
isA
bili
ty o
rganiz
ations,
inclu
din
g T
oujo
urs
Viv
ant-
Not
Dead Y
et
(TV
ND
Y),
join
ed
togeth
er
to o
ppose t
he legaliz
ation o
f euth
anasia
. O
ur
so
cie
ty
is ‘dis
Abili
ty-p
hobic
’ and s
ees little v
alu
e in liv
ing a
life w
here
one is d
isable
d. A
my H
asbro
uck,
TV
ND
Y D
irecto
r says t
hat
“[p]e
ople
with d
isA
bili
ties a
re t
he p
opula
tions m
ost
directly
aff
ecte
d,
sin
ce n
early e
very
one w
ho a
sks f
or
euth
anasia
has a
dis
abili
ty.”
5 A
ble
ism
as a
form
of
vio
lence o
ccurs
when
som
eone liv
ing w
ith a
dis
Abili
ty c
om
es t
o t
he d
ecis
ion t
o
end t
heir life a
nd t
hat
decis
ion is n
ot
consid
ere
d a
‘suic
ide’.
Yet,
we a
ctively
engage w
ith o
thers
liv
ing w
ithout
dis
Abili
ty
to s
upport
them
to s
ee liv
ing a
s a
via
ble
option. A
ble
ist
and
sexis
t belie
fs influence w
hic
h liv
es a
re m
ore
valu
ed;
more
oft
en,
the liv
es o
f w
om
en w
ith d
isA
bili
ties a
re c
onsid
ere
d liv
es
not
wort
h liv
ing.
Able
ism
as a
form
of
vio
lence is s
een in d
ecis
ion m
akin
g
surr
oundin
g D
NR
(do n
ot
resuscitate
) ord
ers
. P
eople
with
dis
Abili
ties a
re o
ften c
oerc
ed t
o s
ign t
hese o
rders
befo
re
goin
g into
the h
ospital (e
.g.,
by f
am
ily/c
are
giv
er)
, or
to s
ign
under
conditio
ns w
here
lim
ited o
ptions f
or
ensuring a
ccess t
o
medic
al care
and s
upport
s a
re p
resente
d (
e.g
., d
eny s
urg
ery
/tr
eatm
ent
that
would
enhance q
ualit
y o
f lif
e/e
xte
nd life
). W
hen
lookin
g a
t th
e liv
es o
f w
om
en w
ith d
isA
bili
ties a
nd d
ecis
ion
makin
g s
urr
oundin
g D
NR
, it is c
ritical to
unders
tand t
hat
we
are
the o
nes w
ho a
re left
behin
d o
r negle
cte
d in o
ur
fam
ilies
of
origin
, and s
een a
s b
urd
ens o
n t
he s
yste
m b
ecause w
e
fail
to liv
e u
p t
o o
r confo
rm t
o g
ender-
role
ste
reoty
pes o
f w
hat
it m
eans t
o b
e ‘fe
male
’ in
this
culture
. T
he u
nderlyin
g
message s
urr
oundin
g ‘assis
ted s
uic
ide’, ‘D
NR
’ directives
and t
he d
enia
l of
medic
al care
for
wom
en w
ith d
isA
bili
tie
s,
reflects
larg
er
syste
mic
pre
judic
es a
nd o
ther
barr
iers
that
influence p
erc
eptions a
bout
whose life is v
alu
ed,
whic
h in
turn
, in
fluences w
ho h
as r
esponsib
ility
for
decis
ions a
bout
“endin
g life”
and h
ow
those d
ecis
ions a
re m
ade.
The b
inary
betw
een d
isable
d a
nd a
ble
-bodie
d is levera
ge f
or
the s
uic
ide
cele
bra
tion v
ers
us s
uic
ide p
revention
dic
hoto
my.
The r
eal
question is,
“Wh
o b
enefits
?”
– is it
the w
om
an w
ith d
isA
bili
ties
OR
her
‘care
giv
ers
’, s
erv
ice p
rovid
ers
, and t
he s
tate
?
LE
AR
N M
OR
E
Bett
y A
nn
e
Gag
no
n
In O
cto
ber
2013,
the
Edm
onto
n C
ourt
of
the
Queen’s
Bench a
nnounced
the s
ente
ncin
g in t
he c
ase
of
Bett
y A
nne G
agnon,
a
wom
an w
ith a
n inte
llectu
al
dis
abili
ty a
nd v
isual
impairm
ent
who d
ied u
nder
the “
care
” of
her
sis
ter
and
bro
ther-
in-law
in N
ovem
ber
2009.
Both
faced m
ultip
le
charg
es inclu
din
g
mansla
ughte
r, f
ailu
re t
o
pro
vid
e t
he n
ecessitie
s o
f
life,
crim
inal neglig
ence
causin
g d
eath
, unla
wfu
l
confinem
ent
and a
ssault,
and c
onspiracy t
o c
om
mit
exto
rtio
n.
Bett
y A
nne’s
experience e
xem
plif
ies
syste
mic
and indiv
idual
able
ism
in r
ela
tion t
o h
er
treatm
ent
by h
er
fam
ily
prior
to h
er
death
in 2
009.
Bett
y A
nne d
ied b
ecause
her
care
giv
ers
faile
d
to p
rovid
e h
er
with t
he
necessitie
s o
f lif
e –
to s
ee
her
life a
s o
ne w
ort
h liv
ing.
Dis
Abili
ty a
ctivis
ts identify
this
as a
tra
vesty
of ju
stice
for
a y
oung w
om
an w
ho
had n
o v
oic
e.
Despite c
alls
made b
y B
ett
y A
nne’s
nie
ce r
egard
ing h
er
safe
ty
and w
ellb
ein
g,
the s
yste
m
that
is t
here
to s
erv
e a
nd
pro
tect
us a
ll, f
aile
d h
er.
5 N
ew
sle
tter,
“E
uth
anasia
, N
o T
hanks!”
, Toujo
urs
Viv
ant-
Not
Dead Y
et,
April 2013,
pg.
1.
AB
LE
ISM
CO
NT
INU
ED

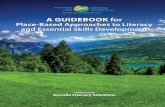
More
than 1
out
of
6 w
om
en in C
anada
lives w
ith a
dis
abili
ty*
(15 y
ears
and o
lder)
of
incid
ents
of
sexual
assault o
f w
om
en w
ith
menta
l dis
abili
ties involv
e
recurr
ing e
pis
odes
75
%
1 in
10O
ver
Most often the a
busiv
e
pers
on is a
care
giv
er
Wom
en liv
ing w
ith d
isabili
ties*
are
more
lik
ely
to b
e v
ictim
s
of
the m
ost
severe
form
s
of
spousal vio
lence
of
hom
ele
ss
wom
en liv
ing in T
oro
nto
have a
his
tory
of
traum
atic b
rain
inju
ry
wom
en r
esid
ing in s
helters
on
April 16,
2008 liv
ed w
ith s
om
e
form
of
dis
abili
ty
Availa
bili
ty o
f accessib
le s
erv
ices
as r
eport
ed b
y C
anadia
n
Shelters
in 2
008:
Over
½ b
illi
on
wo
men
an
d g
irls
in t
he w
orld h
ave a
dis
abili
ty
2/3
of
shelters
had w
heelc
hair-a
ccessib
le b
edro
om
s
22%
pro
vid
ed T
TY
/TD
D e
quip
ment
(i.e
., s
pecia
lly
equip
ped t
ele
phones)
for
wom
en w
ith h
earing im
pairm
ents
17%
pro
vid
ed s
ign language o
r in
terp
reta
tion s
erv
ices
17%
pro
vid
ed larg
e p
rint
readin
g m
ate
rials
for
wom
en
who a
re v
isually
im
paired
5%
pro
vid
ed B
raill
e r
eadin
g m
ate
rials
42
%W
o
3
Clic
k t
ext
for
refe
rence s
ourc
es.
LearningNetwork
Reso
urc
es
Lead
ing
th
e w
ay –
DA
WN
-RA
FH
Can
ad
a a
nd
ou
r P
art
ners
DA
WN
-RA
FH
Can
ad
a,
the D
isA
ble
d W
om
en’s
Netw
ork
(D
AW
N)
of
Canada/R
éseau
d’a
ction d
e f
em
mes h
andic
apées (
RA
FH
) C
anada,
esta
blis
hed in 1
985 is t
he o
nly
national
org
aniz
ation f
or
wom
en w
ith d
isA
bili
ties a
nd D
eaf
wom
en –
wom
an a
buse h
as b
een
TH
E c
entr
al fo
cus o
f our
work
sin
ce o
ur
inception.
DA
WN
’s o
rganiz
ational m
an
tra
is
LE
AD
ER
SH
IP,
PA
RT
NE
RS
HIP
and N
ET
WO
RK
ING
and is t
he w
ay w
e a
re w
ork
ing t
o
‘tra
nsfo
rm’ our
world t
o o
ne t
hat
inclu
des.
In n
am
ing a
ble
ism
as a
form
of
vio
lence w
e a
re
indeed c
alli
ng u
pon y
ou a
s a
Leader
in y
our
work
, in
your
worl
d,
to identify
it,
nam
e it
and
work
with y
our
Part
ners
to c
hange it.
ww
w.d
aw
ncan
ad
a.n
et
A m
antr
a is a
sound,
sylla
ble
, w
ord
, or
gro
up o
f w
ord
s t
hat
is
consid
ere
d c
apable
of
“cre
ating t
ransfo
rmation”.
A F
irst
Nati
on
s W
om
an
wit
h D
isA
bil
itie
s:
“L
iste
n t
o w
hat
I am
sayin
g!”
This
explo
rato
ry a
nd q
ualit
ative s
tudy d
escribes t
he c
oura
geous s
tory
of
Hope,
a F
irst
Nations w
om
an liv
ing w
ith s
evere
dis
Abili
ties in a
n u
rban c
ity.
Hope e
xperiences g
rief,
ra
cis
m,
verb
al and s
exual abuse,
healthcare
concern
s,
isola
tion,
po
vert
y,
and r
esis
ting c
hild
w
elfare
. H
ope’s
sto
ry is a
learn
ing o
pport
unity f
or
all
health a
nd s
ocia
l serv
ice p
rovid
ers
.
Urb
an
Ab
ori
gin
al
Pers
on
s w
ith
Dis
ab
ilit
ies:
Tri
ple
Jeo
pard
y!
This
resourc
e f
ocuses o
n c
halle
nges o
f F
irst
Nations,
urb
an,
dis
ab
led p
ers
ons a
nd s
olu
tions
to o
verc
om
e o
bsta
cle
s. A
borigin
al pers
ons liv
ing w
ith d
isA
bili
ties a
nd s
erv
ice p
rovid
ers
share
their e
xperiences.
Wo
rld
Rep
ort
on
Dis
ab
ilit
yT
his
2011 W
orld H
ealth O
rganiz
ation r
eport
pro
vid
es a
glo
bal pic
ture
of
dis
Abili
ty.
Topic
s inclu
de:
pre
vale
nce,
health c
are
, re
hab
ilita
tion,
enablin
g e
nvironm
ents
, education,
em
plo
ym
ent
and r
ecom
mendation
s
focused o
n a
llevia
ting b
arr
iers
.
6

Po
ten
tial
Co
nseq
uen
ces
Wom
en w
ith d
isA
bili
ties e
xperience a
range
of
consequences s
haped b
y s
uch f
acto
rs
as r
ace,
abili
ty,
sexual orienta
tion a
nd
gender
identity
, in
com
e level, a
nd t
he s
ocia
l in
equitie
s r
ela
ted t
o s
uch f
acto
rs.
Im
pacts
in
clu
de:
fe
ar
of
rem
oval/destr
uction o
f serv
ice
anim
als
or
assis
tive d
evic
es (
e.g
.,
dis
ablin
g t
ele
typew
rite
r, b
reakin
g c
ane)
fe
arf
ul of
leavin
g t
he h
ouse
chro
nic
health c
onditio
ns lin
ked t
o t
he
long t
erm
str
ess o
f liv
ing w
ith a
buse b
y
care
giv
ers
/part
ners
experiencin
g a
dditio
nal dis
Abili
ty c
aused
by a
buse (
e.g
., c
ognitiv
e im
pairm
ent
due
to t
raum
atic b
rain
inju
ry)
very
low
self-e
ste
em
is
ola
tion
alc
oholis
m
engagin
g in o
ther
destr
uctive r
ela
tionship
s
or
behavio
ur
All
wom
en e
xperience b
arr
iers
to d
isclo
sure
(e
.g.,
sham
e,
em
barr
assm
ent)
. S
om
e b
arr
iers
are
rela
ted t
o s
ocia
l lo
cation a
nd p
ers
onal
experience (
e.g
., im
mig
rant
wom
an liv
ing
with d
isA
bili
ty,
povert
y a
nd v
iole
nce).
Wom
en
with d
isA
bili
ties m
ay e
xperience s
om
e o
f th
e
follo
win
g b
arr
iers
:
a
ble
ism
and o
ther
form
s o
f oppre
ssio
n
n
ot
know
ing t
hat
what
they w
ere
experiencin
g w
as a
buse
la
ck o
f m
oney
la
ck o
f accessib
le s
erv
ices a
nd o
utr
each
eff
ort
s
n
ot
know
ing w
here
to s
eek h
elp
or
not
seein
g them
selv
es r
epre
sente
d in s
erv
ices
n
ot
bein
g b
elie
ved o
r havin
g t
he a
buse
min
imiz
ed
n
eedin
g c
are
giv
ing s
upport
the a
busiv
e
pers
on p
rovid
es
la
ck o
f accessib
le/a
fford
able
tra
nsport
ation
to leave a
n a
busiv
e s
ituation o
r to
access
serv
ices in t
he c
om
munity
LE
AR
N M
OR
E
Fo
r S
erv
ice P
rovid
ers
…
non-judgm
enta
l lis
tenin
g
belie
vin
g d
isclo
sure
s
tr
eating w
om
en w
ith c
om
passio
n &
respect
a
skin
g a
bout
abuse a
nd p
rovid
ing a
support
ive s
ett
ing f
or
dis
cussio
n
connecting t
he w
om
an t
o t
he larg
er
com
munity (
e.g
., v
olu
nte
ering,
recre
ational activitie
s)
addre
ssin
g w
om
an’s
health c
oncern
s
Fo
r w
om
en
wit
h d
isA
bil
itie
s…
esta
blis
hin
g f
inancia
l security
in
form
ation,
aw
are
ness,
and
em
pow
erm
ent
holis
tic h
ealth s
erv
ices
in
form
al and f
orm
al support
s
w
om
an-c
entr
ed c
olla
bora
tive s
erv
ices
gett
ing c
onnecte
d t
o t
he larg
er
com
munity
abuse a
ware
ness e
ducation
LE
AR
N M
OR
E
Learn
ing
fro
m W
om
en
wit
h L
ived
Exp
eri
en
ce
Wom
en w
ith d
isA
bili
ties h
ave s
hare
d s
trate
gie
s t
hat
help
ed t
hem
heal and m
ove f
orw
ard
fro
m
their liv
ed e
xperiences o
f vio
lence.
Barr
iers
to
Dis
clo
su
re a
nd
Accessin
g S
up
po
rt
LearningNetwork
5
LearningNetwork
Exp
eri
en
ces o
f V
iole
nce
While
all
wom
en e
xperience v
iole
nce
diffe
rently,
there
are
com
monalit
ies b
etw
een
the e
xperiences o
f w
om
en w
ith a
nd w
ithout
dis
Abili
ties.
How
ever,
vio
lence a
gain
st
wom
en w
ith d
isA
bili
ties m
ay b
e r
ela
ted t
o
their d
isA
bili
ty s
upport
needs a
nd is r
oote
d
in a
ble
ism
and o
ther
form
s o
f dis
crim
ination.
Abusiv
e p
ers
ons a
re o
ften c
are
giv
ers
, w
hic
h
can b
e a
fam
ily m
em
ber,
health c
are
work
er,
or
an in
tim
ate
part
ner/
spouse. A
buse in
clu
des:
p
sych
olo
gic
al
& v
erb
al
(e.g
., n
am
e c
alli
ng r
ela
ted t
o d
isA
bili
ty;
thre
ate
nin
g h
arm
to a
ssis
tive d
evic
e o
r serv
ice a
nim
al; t
hre
ate
nin
g t
o w
ithhold
essential care
support
s)
syste
ms a
bu
se
(e
.g.,
unw
illin
gness t
o p
rovid
e s
erv
ice
and s
upport
; ru
de a
nd d
isre
spectf
ul
treatm
ent)
d
estr
ucti
on
of
pro
pert
y
(e.g
., d
am
agin
g h
earing a
id o
r oth
er
assis
tive d
evic
es)
d
en
ial
of
serv
ices a
nd
/or
inap
pro
pri
ate
tr
eatm
en
t b
y c
are
giv
ers
(e.g
., f
orc
ed t
o
live in inaccessib
le h
om
es)
d
iscri
min
ati
on
on
th
e b
asis
o
f th
eir
dis
Ab
ilit
y
(e.g
., r
efu
sed s
erv
ice o
r could
n’t b
e
accom
modate
d a
t a s
helter
because o
f m
enta
l health d
isA
bili
ty)
ra
cis
m a
nd
ab
leis
m
(e.g
., f
earing t
he r
evokin
g o
f sponsors
hip
fo
r im
mig
ration b
ecause o
f re
lationship
vio
lence a
nd d
isclo
sure
of
one’s
dis
Abili
ty
sta
tus)
fi
nan
cia
l
(e.g
., c
ontr
olli
ng b
ank a
ccounts
; ste
alin
g
dis
Abili
ty s
ocia
l assis
tance c
heques)
p
hysic
al
(e
.g.,
vio
lently t
ransfe
rrin
g a
wom
an t
o
and f
rom
her
wheelc
hair;
withhold
ing o
r denyin
g s
erv
ices;
usin
g s
evere
vio
lence
that
can c
ause b
rain
inju
ries)
sexu
al
(e
.g.,
forc
ed s
ex;
forc
ed s
teriliz
ation o
r abort
ions;
vio
lations o
f privacy;
sexual
touchin
g d
uring p
rim
ary
care
)
te
ch
no
log
y-r
ela
ted
vio
len
ce
(e.g
., im
pers
onating a
Deaf
wom
an b
y
usin
g t
heir t
ele
typew
rite
r; c
yber-
bully
ing)
MY
TH
S
W
om
en w
ith d
isA
bili
ties a
re s
een a
s
sexually
undesirable
or
asexual and
can’t b
e s
exually
vio
late
d
W
om
en w
ith d
isA
bili
ties a
re m
ost
oft
en
abused b
y s
trangers
especia
lly g
iven
that
no p
ers
on w
ho c
om
mits t
heir life
to c
aring f
or
som
eone w
ith a
dis
Abili
ty
would
abuse t
hem
RE
AL
ITIE
S
W
om
en w
ith d
isA
bili
ties e
xperience r
ate
s
of sexual vio
lence that are
hig
her
than
wom
en liv
ing w
ithout dis
abili
ties. S
exual
vio
lence is a
bout pow
er
and c
ontr
ol and
not sexual attra
ctiveness a
nd d
esirabili
ty
of th
e v
ictim
P
erp
etr
ato
rs m
ost
oft
en inclu
de f
am
ily
mem
bers
, in
tim
ate
part
ner,
peers
, and
care
giv
ers
(e.g
., institu
tional sta
ff,
docto
r)
Myth
s a
nd
Reali
ties
4
LE
AR
N M
OR
E
Top Related