







Languages
Pages
Legal


Primary Health Care & HR for Health
Prof. Jan De Maeseneer, M.D., Ph D. 1
Chairman European Forum for Primary Care
Secretary General The Network “Towards Unity for Health”
Family Physician (part-time), Community Health Center – Ledeberg – Ghent
Vice-Dean Strategic Planning, Faculty of Medicine and Health Sciences – Ghent University
Pretoria, 22 June 2014

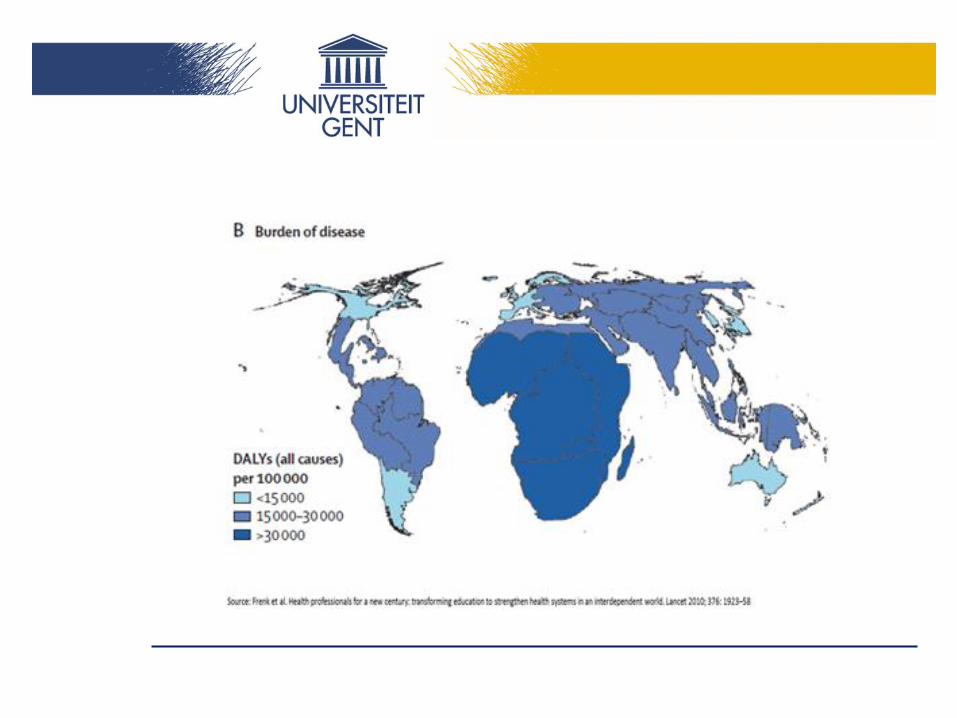
The Lancet 2010;376:1923-58



AN international FP7 collaborative research project.
Aims at developing and assessing policies and key interventions to address the personnel crisis in (PRIMARY) health, in Africa.
Human Resources for Primary Health Care
in Africa (HURAPRIM)

Partners Research objectives
• UNIVERSITY OF WITWATERSRAND, SOUTH AFRICA
• MBARARA UNIVERSITY, UGANDA
• UNIVERSITY OF BOTSWANA, BOTSWANA
• AHFAD UNIVERSITY OF WOMEN, SUDAN
• UNIVERSITY OF BAMAKO, MALI
• AIDEMET NGO, MALI
• OXFORD UNIVERSITY, UK
• MEDICAL UNIVERSITY OF VIENNA, AUSTRIA
• GHENT UNIVERSITY, BELGIUM
assess the scope of the deficit
identify and analyse the main causes
review the effects of related interventions and policies
implement improved or new interventions and/or policies and valuate them
formulate scientifically sound, acceptable and feasible policy directions for the future
March 2011 – February 2015
Coordinator: UGent

Health workers per 10 000 in HURAPRIM countries
0 20 40 60
Mali
Uganda
N. Sudan
Botswana
South Africa
Doctors
Nurses
Midwives

And from those who have not,…
0
5000
10000
15000
20000
25000
30000
35000
40000
2005 2011
Population (000)
Doctors
Nurses+Midwives
Uganda:

Uganda MoH staffing norms: filled and
vacant positions at public facilities
0 5000 10000 15000
Ministry of Health…
Mulago Hospital
Butabika Hospital
Regional Referral Hospitals
General Hospitals
Health center IVs
Health center IIIs
Health center IIs
Vacant (%)
Filled (%)
Source: Uganda Capacity program data 2009
These posts

District staffing, Uganda March 2012
Key: % of
posts filled

% of birth assisted by “skilled” provider (Uganda DHS, 2011)
31%
94%

Distribution of MUST* Alumni Currently in Uganda 687 (88%)
Work for:
Government
NGO or Private
270 (35%)
510 (65%)
HIV related NGO 383 (51%)
Effort dedicated to HIV
None
Less than 50%
Over 50%
119 (15.8%)
317 (42.2%)
314 (42.0%)
Donor program not HIV 169 (22.5)
*Faculty of Medicine n=790

Brain-drain
Internal:
- From PHC to specialist care
- From horizontal to vertical
- From public to private
- From rural to urban
External:
- Within Africa
- Intercontinental

Vertical programmes and internal brain drain
• Well-financed, vertical programs
• Example: Ethiopia
“The implementation of the Global Fund
proposal required human resources: local
medical staff was hired on consultancy
contracts at triple the salary available in
the public sector. This has “diverted”
skilled local health personnel from the
poor local (primary) health care system.”

Brain drain



26/06/2014
3. Strategies for change
A confidential enquiry into maternal and child
deaths in Mali and Uganda*
1. To adapt the confidential enquiry as a tool which could be
used in Africa
2. To test whether this tool could help to reduce under five and
maternal mortality, by:
• Identifying avoidable factors
• Suggesting and prioritising possible interventions
• Making and implementing recommendations
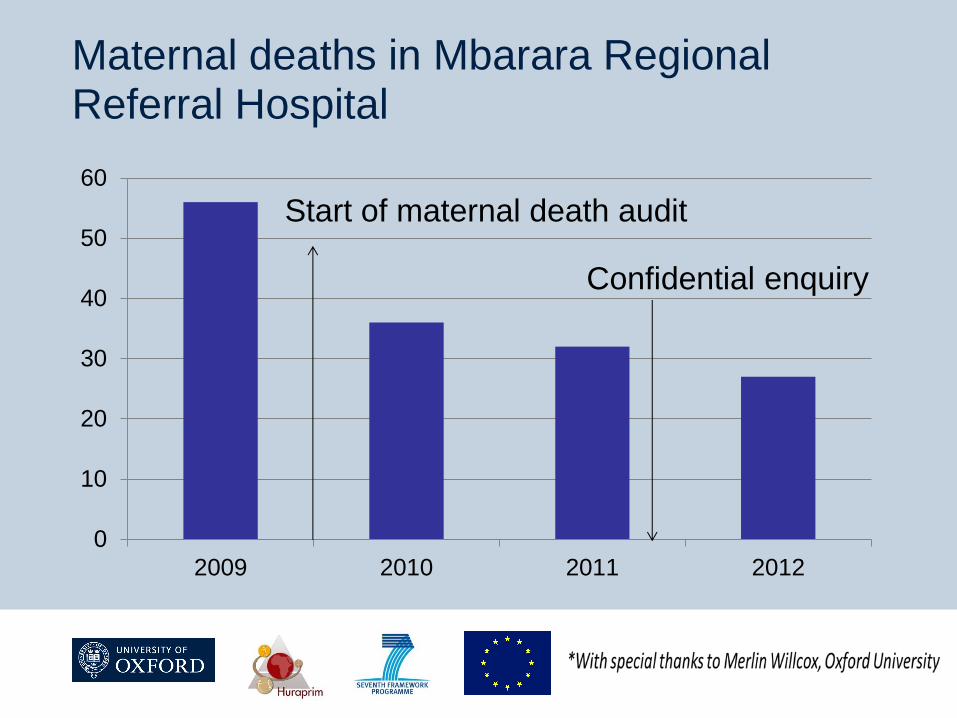
*With special thanks to Merlin Willcox, Oxford University

Results: child deaths in 12 months
0
20
40
60
80
100
120
140
160
Rugando Nyakayojo Kibuli Finkolo Kolokani
Expected deaths
Observed deaths

Results: child deaths in 12 months
0
20
40
60
80
100
120
140
160
Rugando Nyakayojo Kibuli Finkolo Kolokani
Expected deaths
Observed deaths

All deaths of babies and children aged <5 years are reported
by Village Health Teams (VHTs) in the included subcounties
A fieldworker visits the family, presents condolences, and
invites them to be interviewed
Informed consent
Methods: Identifying child deaths

VHTs were asked to report any maternal deaths in the included
subcounties
A fieldworker visits the family, presents condolences, and
invites them to be interviewed
Informed consent
Methods: Identifying maternal deaths

Interviews
“Verbal autopsy” interviews with families
Interviews with any health workers involved at any levelel

Example : 2 ½ year old girl from Uganda
Fever, cough, abdominal pain
Morning: taken to a church for prayers
no improvement
Around 2pm: taken to Health Centre - no staff
Taken to private drug shop:
given paracetamol + mebendazole + injection
Parents borrowed money from extended family
Child died while returning to drug shop the
same evening
Do you think this death could have been
avoided? How?

Monthly panel review meeting
Fieldworkers present case summary
Panel includes doctors, nurses, village health workers
Agrees on most likely cause of death (diagnosis)
Identifies avoidable factors
Makes recommendations
External review for quality assurance

How many deaths could be avoided?
Almost all deaths had at least 1 avoidable
factor
Missed opportunities to prevent illness
Problems in getting treatment

Biannual “Grand Committee” meeting:
Local politicians and decision-makers are invited
Summary of results and recommendations presented
Feedback is invited

What has been the impact of the confidential enquiry?
Number of child deaths per month,
Finkolo (Mali)
0
5
10
15
20
25
30
Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul
2011-12 2012-13

What has been the impact of the confidential enquiry?
Number of child deaths per month,
Finkolo (Mali)
0
5
10
15
20
25
30
Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul
2011-12 2012-13
Overall 27% reduction (158 to 116)

Under-5 deaths in Nyakayojo subcounty, Uganda
0
2
4
6
8
10
12
Jan-Mar Apr-Jun Jul-Sep Oct-Dec
2012
2013

Under-5 deaths in Nyakayojo subcounty, Uganda
0
2
4
6
8
10
12
Jan-Mar Apr-Jun Jul-Sep Oct-Dec
2012
2013
Overall 66% reduction (36 to 12)

Maternal deaths in Mbarara Regional Referral Hospital
0
10
20
30
40
50
60
2009 2010 2011 2012
Start of maternal death audit

Maternal deaths in Mbarara Regional Referral Hospital
0
10
20
30
40
50
60
2009 2010 2011 2012
Start of maternal death audit

Maternal deaths in Mbarara Regional Referral Hospital
0
10
20
30
40
50
60
2009 2010 2011 2012
Confidential enquiry
Start of maternal death audit
Maternal deaths in Mbarara Regional Referral Hospital
0
10
20
30
40
50
60
2009 2010 2011 2012
Confidential enquiry
Start of maternal death audit

Recommendations
Training of health care providers on resuscitation and basic life
saving skills and making necessary follow-up
Health workers should monitor patients
Health centres should be made functional to offer emergency
obstetric care
Emergency ambulance service should be functional

Discussion of pertinent cases with Village Health Workers and Traditional Birth Attendants

Training of Village Health Workers -> improved recognition and referral of serious illness

Training of Traditional Birth Attendants -> Care of newborn babies

Discussion of cases with health workers in Health Centres - Continuing professional education - to improve quality of care

Challenges…
Improve functioning of Village Health Teams
Child protection
Supervision of private clinics
More, better motivated health workers in government
facilities
Improve Management of health centres
Scaling up the intervention and improve cost-
effectiveness: need for funding!

An African wide plan is needed to scale
up the capacity of family medicine
training:
By 2020 Africa should have 30,000
more trained family/primary care
physicians!
How to make this happen?
“The data suggest an estimated
10,000-11,000 graduates per year from
medical schools in sub-Saharan Africa”
(Mullan F et al. Medical schools in sub-Saharan Africa. The Lancet
2011:377:1113-1121)
What happens if 50 % of these graduates
are from now onwards trained in a 2-years
program in Family Medicine?

2015
2016
2017
2018
2019
2020

The future: campaign “30by20” ?
• From 2013 onwards 50 % of all African
graduates (MD), should be trained to become
Family Physicians
• By doing so Africa will have 30000 new Family
Physicians by 2020

2015
2016
2017
2018
2019
2020
WHO
Collaborating
Centre on PHC
Thank you !
Top Related