







Languages
Pages
Legal


1
“All drugs known to humans are poisons, only the amount or dose determine the effects.”
Paracelsus, 1490 - 1541
Drug-induced nephrotoxicity

Definition and epidemiology Risk factors of ICU nephrotoxicity
Pharmacology in ICU patientsMechanisms of toxicity
Biomarkers Prevention of ICU nephrotoxicity

AKI definition: increase in S. Cr. By ≥ 0.3 mg/dl (≥ 26.5 µmol/l) in 48 h.
Or increase in SCr to ≥ 1.5 times baseline, which is known
Or Urine volume < 0.5 ml/kg/h for 6 hours.
Nephrotoxic Injury DefinitionNephrotoxic injury is damage to one or both of the kidneys that results from exposure to a toxic substance.Deterioration of renal function alters the drugs and metabolites clearance leading to :
More side effects Increase nephrotoxicity Change in the drug metabolism (volume distribution)
Introduction


Epidemiology: The rates of AKI have been reported in hospitalized patients to be between 3.2%-
20% and in ICUs. This rate rises up to 22% and even to 67% depending on the population studied and the definition of AKI used
– Murugan R et all, Nat Rev Nephrol 2011 7:209 - 2179
Nephrotoxicity due to drugs contributes to between 8-60% of AKI cases in hospitalized patients.
– Schetz M, et allCurr Opin Crit Care 11:555-565.– Hou SH, et all Am J Med 74:243-248.
In the ICU setting the incidence of AKI from drug nephrotoxicity ranges between 1-23%.
– Mehta RL, et all Kidney Int 66:1613-1621.– Silvester W, et all Crit Care Med 29:1910-1915.– Liano F, et all Kidney Int Suppl 66:S16-24.

Continue: Based on 75,000 critically ill adults, more severe AKI occurs in 4% to 25% of all ICU admissions . On average, 5% to 6% of ICU patients with AKI require renal replacement therapy (RRT).
Uchino S, et al: Jama 2005; 294:813–818Uchino S, et al: Critical care medicine 2006; 34:1913–1917Ostermann M, Chang RW:Critical care medicine 2007; 35: 1837–1843; quiz 1852
Elderly patients are likely more susceptible to AKI from nephrotoxic agents due to the age related decline in GFR or renal blood leading to reduced clearance of the drug, decline in hepatic clearance, altered free drug concentration.
Henrich WL. Kidney Int Suppl:S107-109.


Common risk factors associated with the development of AKI
Clinical settingsICU/multiple organ failure Sepsis/infectionDMPreexisting CKD defined as eGFR < 60 ml/min/m2Nephrotic syndromePostoperative especially cardiac and vascular surgery TraumaBurnsHIVNon-renal solid organ transplantation Bone marrow transplantation Liver disease MalignancyHypertension Morbid obesity

Patient – specific factors Advanced age Volume depletion Sepsis, Preexisting renal hepatic and cardiac diseasesDMMultiple nephrotoxic drugsRadiocontrast agent
Common risk factors associated with the development of AKI
Medications NSAIDs /cox-2 inhibitorsAminoglycoside antibioticsAmphotericin B RAS blockers Calcineurin inhibitors Chemotherapeutic agents CocaineEthylene glycol Occupational toxins (heavy metals, organic solvents)Herbal remedies

Pharmacokinetic changes in ICU patients
Altered oral drug bioavailability (decreased> increased)Increased gastric pH, insoluble drug complexes Intestinal atrophy, dysmotility and reduced transport function (intestinal edema, or hypoperfusion ) Reduced intestinal and hepatic metabolism Risk factors: acute heart decomposition, liver diseases)
Boucher BA et el, Cri Care Clin 2006: 255 – 271Chan LMS, et al, Eur J Pharmaceut Sci 2004, 21: 25 – 51.
Altered volume of distribution (decreased or increased) Decreased or increased extracellular fluid space (volume distribution)
Liver diseases, nephrotic syndrome, and heart failureDecreased protein concentration or binding and lipid solubility of drugs Altered tissue permeability pH disturbances
Boucher BA et el, Cri Care Clin 2006: 255 – 271Schmith VD, et al, Clin Pharmacol Ther 2010; 87: 488 - 491

Altered drug metabolism:Liver, kidney, intestine,
Hypoperfusion of these organsAltered drug cellular transportAltered CYP-450 drug metabolism
Vily AM et al, Crit Care, 2008, 12: 235 – 243 Chan LMS, et al, EurJ Pharmaceut Sci 2004; 12 25 – 51.
Altered renal drug clearance: Reduced GFR Reduced proximal tubular drug secretion
Dialysis clearanceModality of RRT (PD, HD, CVVH)
Perazella, Kidney Int. 2012; 81: 1172 – 1178
Continue:

Mechanisms of Nephrotoxicity
Intraglomerular hemodynamics Tubular cell toxicity InflammationCrystal nephropathyThrombotic microangiopathyRhabdomylosis

prostaglandins
Filtration of 120ml plasma/ min
Ang II
Afferent Arteriolar Vasoconstrictors:Vasodilatory PG Inhibitors: NSAIDsDirect Afferent Vasoconstrictors:CyA, Tacrolimus, Radioconstrast Media, Vasopressors
Efferent Arteriolar Vasodilators:RAAS: ACEI, ARBDirect Efferent Vasodilators:Diltiazem, Verapamil
Risk Factors:Decreased intravascular volume (dehydration, diuretic overuse, CHF, vomiting, diarrhea)SepsisRenal-artery stenosisPolycystic kidney disease
FENa <1%, Uosm > 500
AKI : 3% - 23% in Bilateral RAS or 38% in solitary RAS

NSAIDs: Anti-prostaglandins activity Vasoconstriction of afferent arterioles
RAS blockers: Decreasing efferent arteriolar tone Decreasing intraglom. Capillary pressure
Calcineurin inhibitors: AKI and oliguria <50ml/h Dose-depend vasoconstruction of afferent arterioles:
Endothelium Increase sympathetic activity Increase in adenosine Relative decrease in nitric oxide and transforming GF-β-1 Increase in endothelin -1
Dugs affecting the CsA concentration (Ketoconazole, etc).

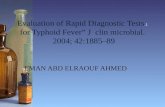
ACUTE PRE-RENAL FAILURE
AMPHOTERICIN, ANTIHYPERTENSIVES,
DIURETICS, DOXORUBICIN, NSAIDS,
CYCLOSPORIN-A
CHRONIC INTERSTITIAL NEPHRITIS ANALGESIC COMBINATIONS, CHINESE HERBS, CYCLOSPORINE,
METALS (PB, Cd, Li, Ge), METHYL-CCNU
------------------------------------------------------------
-----------------------------------------------------------
OBSTRUCTION
ACYCLOVIR, ANTICHOLINERGICS, BROMOCRIPTINE, ERGOT ALKALOIDS,
FLUOROQUINOLONE, MTX
OUTER MEDULLA
INNER MEDULLA
VASCULITIS AMPHETAMINES, NSAIDS,
PENICILLINS,SULFONAMIDES
NEPHROTIC SYNDROME
NSAIDS, PENICILLAMINECAPTOPRIL
HEROIN/COCAINEMETALS (Au, Hg)
ATN(P): ACUTE TUBULAR NECROSIS AMINOGLYCOSIDES, ANTINEOPLASTICS,
GLYCOLS, RADIOCONTRAST AGENTS
ATN(D): ACUTE TUBULAR NECROSIS AMPHOTERICIN,
CISPLATIN, GLYCOLS
ACUTE INTERSTITIAL NEPHRITIS
ALLOPURINOL, RIFAMPIN, VANCOMYCIN, NSAIDS
CORTEX

Tubular cells injury/necrosis : Proximal tubular cells Concentrating and reabsorbing Expose to high concentration of toxins Toxins cause impairing metochondrial function, interfering with tubular transports,
increasing oxidative stress, or free radicals. Swollen cells and filled with abundant lysosomal vacuoles aminoglycosides, amphotericin B, antiretrovirals (adefovir , cidofovir, tenofovir), cisplatin,
contrast dye

Acute Tubular Necrosis:
Cidofovir or tenovir, dose dependent AKI 14-24% Fanconi syndrome (proteinuria, glucosuria, and bicarbonate wasting. RF improve upon discontinuation but can leads to ESKD
Aminoglycosides with AKI 7-9 - 15% The renal toxicity was reported to be 3.9%,30% in the 1st week and after 1 month
respectively Cephalosporins, Am-B, rifampicin, NSAIDs, contrast media, CsA, FENa > 2%, Uosm < 350, urinary sediment: granular casts, renal epithelial cells Elevated CPK (statins and barbiturates) Elevated LDH and decrease haptoglobin (nitrofurantion, quinine, sulfanamide,hydralazine)
Joannidis M. et all, 2004. Int J Artif Organs 27:1034-1042.Verhelst D, et all, 2002. Am J Kidney Dis 40:1331-1333.Bertino JS Jr, et all. 1993.J Infect Dis 167:173-179.
Baciewicz AM, et all. 2003. Ann Pharmacother 37:182-186.

Allergic Interstitial Nephritis: Dugs produce allergic reaction leading to inflammation and infiltration of immune cells
(lymphocytes, monocytes, eosinophils), leading to fibrosis and scaring AKI is 3 – 15% of all cases. Drugs: β-lactams, quinolones, sulfonamides, rifampin, diuretics, NSAIDs, cimitedine,
ranitidine, recombinant humanized monoclonal immunoglobulin G. Clinical: rash, fever, eosinophilia, eosinophiluria, pyuria.
Michel DM, et all. 1998. J Am Soc Nephrol 9:506-515.Toto RD. 1990. Am J Med Sci 299:392-410.Barakat RK, et all, 2007.Ann Pharmacother 41:707-710.

Crystal Nephropathy: Distal tubular lumen Insolubility of drugs in urine pH dependent 49 Produced crystals precipitate in the distal tubular lumen, leading to obstruction and eliciting
an interstitial reaction 21 48 The risk increased with volume depletion, dose dependent, CKD, Ciprofloxacin, sulfonamides , ampicilin, acyclovir (mealy in 500mg/m2) , ganciclovir,
indinavir; methotrexate 55 Tumor lysis syndrome leading to uric acid and calcium phosphate crystals Urine test: Hematuria, renal tissue,
Perazella MA. 1999. Am J Med 106:459-465.Fogazzi GB. 1996. Nephrol Dial Transplant 11:379-387.Martinez F, et all. 1998. Nephrol Dial Transplant 13:750-753.

Rhabdomyolysis: Muscle injury leads to lysis of myocyte releasing of intracellular contents including
myoglobin and creatine kinase into plasma Drugs may induce rhabdomyolysis directly secondary to a toxic effect on myocyte
function, or indirectly by predisposing the myocyte to injury Drug rhabdomyolysis charactarised by weakness, myalgia, tea-colored urine Combination with clarythromicin, erythromicn, fibrate Statins, cocaine heroin and ketamine Alkalinization to keep urine pH > 6.5 by mannitol and bicarbonte which are effective
than saline.
Thrombotic microangiopathy: Platelet thrombi in the microcirculation as in TTP. Immune-mediated reaction or direct endothelial toxicity Clopidogrel, ticlopidine, cyclosporine, mitomycin-C, and quinine. low Hb, haptoglobin, high LDH ADAMTS 13 not indicated here

Biomarkers

Traditional tools: Traditional tools to diagnose AKI (SCr) and determine etiology of AKI (clinical history,
physical examination, renal ultrasound, fractional excretion of sodium [FeNa], fractional excretion of urea, blood urea nitrogen [BUN], and urine microscopy) remain the cornerstone of diagnostic tools available to the clinician in the ICU
Urine microscopy can be helpful in differential diagnosis• granular casts and renal tubular epithelial cells in acute tubular necrosis,• cellular casts in glomerular injury, • Eosinophiluria in acute interstitial nephritis, or atheroembolic AKI).
S. Creatinine : • Tubular secretion • Age, sex muscle mass, metabolism and volume status.• Increased when GFR is low 2 -3 days after insulting the nephron

New biomarkers: Enthusiasm about their usefulness seems unwarranted at present, in ICU or surgical
ICU. Poor performance in patients with sepsis or with acute-on-chronic kidney disease The inability of biomarkers to improve classification of 'unclassifiable' (structural or
functional) AKI, in which accurate differential diagnosis of pre-renal versus intrinsic renal AKI has the most value, illustrates another problem.
Future research is necessary to clarify whether serial measurements of a specific biomarker or the use of a panel of biomarkers may be more useful in critically ill patients at risk of AKI.
Mol Diagn Ther. 2012 Aug 1;16(4):199-207

Cystatin C marker: • able to predict AKI 1-2 days earlier than SCr. But also increased when GFR is low too• Cystatin C is a low molecular weight protein produced by all nucleated cells that is
freely filtered by the glomerulus and then reabsorbed and metabolized by the proximal tubule
• Serum level of Cystatin C dependents on – Clearance– Production – Volume of distribution. – Increased by higher dose of corticosteroids and hyperthyriodism– and hyperthyroidsm and decreased by hypothyroidism.– Smoking – Immunosuppressive therapy and malignanacy
• There is plasma Cystatin C which affected by and urinary cystatin C which reflect tubuar damage
Hilde R. et al Clin Kidney J (2012) 5: 102–108Knight EL, et al, Kidney Int 2004; 65: 1416–1421Okura T, Jotoku M, Irita J et al. Clin Exp Nephrol 2010; 14: 584–588

NAGL Neutrophil Gelatinase- Associated Lipocaline ( Lipocalin-2 or siderocalin) • Superior to s.cr and cystatin C.• In the normal kidney, only the distal tubules and collecting ducts stain for NGAL
expression.• Response to ischemic injury in proximal tubule cells. • Its appearance in urine is independent of the GFR• uNGAL excretion is proportional to albumin excretion in mouse
Mishra J, et al J Am Soc Nephrol 2003,14:2534-43Hilde R. et al Clin Kidney J (2012) 5: 102–108
A pro-inflamatory cytokine IL-18:
Urine IL-18 levels were found markedly increased in patient with AKInot in patients with UTI, CKD, nephrotic syndrome sensitivty > 90% and specifity>95% for the diagnosis of AKI.
Parikh CR & Devarajan . Crit Care Med 2008,364):S159-S16

Kidney injury molecule KIM-1 :
• Ischemia and nephrotoxic injuryof proximal tubule cells. • It is more useful in toxic renal injury like rhabdomyolysis• KIM-1 levels peaked 12 hours after injury in AKI in post cardiac operation.• KIM-1 more specific to ischemic and nephrotoxic kidney injury than NGAL • it is not significantly affected by chronic kidney disease or urinary tract
infection
Liangos O, et al. J Am Soc Nephrol 2007:18:904-912

Author Estimation formula PurposeMDRD eGFR = 186 × serum creatinine (mg per
dL) −1.154 × age (years) −0.203 × (0.742 if patient is female) × (1.210 if patient is black)
To assess renal function and stage chronic kidney disease
Cockcroft and Gault
Male: eCrCl = ([140 – age (years)] × ideal body weight [kg]) ÷ (serum creatinine [mg per dL] × 72)
To adjust drug dosing for renal function in adults
Female: male eCrCl × 0.85Schwartz eCrCl = (length [cm] × k) ÷ serum
creatinine (mg per dL)To adjust drug dosing for renal function in children
k = 0.45 (infants one to 52 weeks of age)
0.55 (children one to 13 years of age)
0.70 (males 14 to 17 years of age)0.55 (females 14 to 17 years of age)
Formulas to assess renal function and adjust medication dosages

General approaches for the prevention of AKIAvoidance of nephrotoxins Recognition of potential nephrotoxic agentsRecognition of high risk high risk patients and clinical stetting sAvoidance of concomitant use of multiple nephrotoxins Maintain euvolemia :
CVP 8 – 12 mmHg or to 15 mmHg in patient with positive pressure ventilation Early rehydration Mean arterial pressure > 65mmHg Third space
If applicable monitoring drug dose and levelsUse of lowest dose for shortest time
Minimization of nosocomial infection
Urine output hourly measurement
Monitoring kidney function closely and evaluation of GFR Dose adjustment accordingly
Controlling BPControlling DM : tight is associated with hypoglycemia and no difference in moratlity copre to conventional glucose control

Example of specific renal protective strategies Exposure Strategy
Aminoglycoside antibiotics Once – daily dosing Monitoring of drug levels Avoiding in CKD and pts at risks. Maintain trough levels < 1mcg /ml.
Tumor lysis (uric acid) Allopurinol/rasburicase IV hydration/urine alkaliniation
Amphotericin B Use lipid formulation Saline hydration pre and post administrationAvoid high or rapid dose or prolonged duration
Ethylene glycol ingestion Ethanol/fomepizole hemodialysis
rhabdomyolysis IV hydration/urine alkalinization ± mannitol
Methotrexate IV hydration/urine alkalinization
Acyclovir IV hydration
Calcineurin inhibitors Monitoring drug levelsLowering the doses ± CCB

Strategy Exposure
Avoid long-term use, More than one drug Avoid in old ageMonitor cumulative consumptions and avoid it Avoid combination wit RAS blockers
Acetaminophen, Aspirin, NSAIDs
Fluid correction before drugs initiation Monitoring s.creatinine
RAS inhibitors
Discontinue or reduce dose Hydration Oral route Establish high urine flow
Acyclovir MethotrexateSulfa ATBTriamterene

Definition:• The impairment of renal function and is measured as either a 25% increase in serum
creatinine (SCr) from baseline or 0.5 mg/dL (44 µmol/L) increase in absolute value, within 48-72 hours (max 7 days) of IV administration.
• The SCr levels peak between 2 and 5 days and usually return to normal in 14 days.Patient related risk factors:• Age • CKD• Coexisting diseases: Diabetes mellitus, Hypertension, Metabolic syndrome, Anemia,
Multiple myeloma Hypoalbuminemia, • Renal transplant• Hypovolemia and decreased effective circulating volumes . Contrast-related risk factors are as follows:• Volume of contrast• Contrast characteristics, including osmolarity, molecular weight, volume, and viscosity.• Ultra-low dose <50 ml was effective in reducing CIN .
Norbert Lameire, NDT Plus, 2008, 6:392 – 402.
Contrast – Associated Nephropathy

Complications: • CIN is one of the leading causes of hospital-acquired acute renal failure. • Nonrenal complications include
– Procedural cardiac complications (eg, Q-wave MI, coronary artery bypass graft [CABG], hypotension, shock),
– Vascular complications (eg, femoral bleeding, hematoma, pseudoaneurysm, stroke), – Systemic complications (eg, acute respiratory distress syndrome [ARDS], pulmonary
embolism).
Clinical presentation:
Acute renal failure : There may also be associated dehydration from aggressive diuresis, exacerbated by preexisting fluid depletion; the acute renal failure is usually oliguric, and recovery is anticipated in 2-3 weeks Acute interstitial nephritis : is usually from drugs such as penicillin, cephalosporins, and nonsteroidal anti-inflammatory drugs (NSAIDs) Acute tubular necrosis - Ischemia from prerenal causes; endogenous toxins, such as hemoglobin, myoglobin, and light chains; exogenous toxins, such as antibiotics, chemotherapeutic agents, organic solvents, and heavy metals

Advanced algorithm for the management of patients receiving iodinated contrast media (taken from reference 86 after permission).
Lameire N et al. NDT Plus 2009;2:1-10
© The Author [2009]. Published by Oxford University Press on behalf of ERA-EDTA. All rights reserved. For Permissions, please email: [email protected]

• Steroid use in controversial but may be used for:– Glomerular proteinuria with intake of NSAIDs, gold, penicillamine not respoding
to cessation of drug.– All patients of hypersensitivity vasculitis due to drugs– AIN unresponsive to drug cessation with granulomatous reaction.– In patients with cisplatin toxicity
• Dialysis: – Persistent azotemia– Plasmapharesis in HUS– PD for dug protein – bound (cisplatin, CsA, beta-lactams)
Next steps

36
"The person who takes medicine must recover twice, once from the disease and once from the medicine."
- William Osler, M.D.

Case 2: 52 yo male with Type 2 DMbaseline creatinine 159umol/L; BP 148/96 Ramipril 5 mg daily started and 2 weeks later: BP 138/82 Serum creatinine 194umol/L
accept 20-30% increase in serum creatinine within 1-2 months of initiation in fact, this could be an indication that the drugs are exerting their desired actions to help preserve renal functioncheck serum creatinine 1-2 weeks after initiation, then in 2-4 weeks if > 30% change, decrease ACEI/ARB dose by 50% andrepeat Ser Cr in 4 weeks (exclude hypovolemia/NSAIDs, etc)if > 50% rise in Ser Cr – rule out RAS repeat serum creatinine in this patient in 1-2 weeks to ensure it has stabilized
Case 1: 82 yo female with osteoarthritis and HTNAdmitted to hospital for CAP & dehydrationMeds: Losartan 100mg daily + Naproxen 250mg BIDSerum creatinine 250 umol/L
Discontinue NSAID and hold ARB until infection treated and patient is rehydrated/creatinine reducedresume ARB and monitor serum creatinine

Sepsis:Up to 50% of ICU AKI (tubular injury/necrosis).Systemic vasodilatationRenal vasoconstruction Intravascular volume depletionAnorexia Third spacing of fluid Apoptosis rather than necrosis
Heart failure:Cardiorenal syndromeNeurohormonal response Reduce cardiac outputElevated renal venous pressure Systemic hypotension
Preexisting CKD :Reduced volume of functional parenchymaeGFRAcute in top of Chronic
Liver diseases :Acute hepatic failureDecompensated cirrhosisVasodilated systemic circulation Renal arteriolar vasoconstriction Ascites (intraabdomenal compartement
syndrome)

EXCRETION PATHWAYS, TRANSPORT MECHANISMS & DRUG EXCRETED.
Excretory route
Mechanism Drug Excreted
Urine GF/ ATS/ ATR, PTR Free, hydrophilic, unchanged drugs/ metabolites of MW< 500
Bile Active secretion Hydrophilic, unchanged drugs/ metabolites/ conjugates of MW >500
Lung Passive diffusion Gaseous &volatile, blood & tissue insoluble drugs
Saliva Passive diffusionActive transport
Free, unionized, lipophilic drugs. Some polar drugs
Milk Passive diffusion Free, unionized, lipophilic drugs (basic)
Sweat/ skin
Passive diffusion Free, unionized lipophilic drugs
Intestine Passive diffusion Water soluble. Ionized drugs
09-12-2010 39KLECOP, Nipani



SLOUGHING-OFF OF VIABLE & NON-VIABLE CELLS WITH INTRALUMINAL CELL-CELL ADHESION
INTACT TUBULAR EPITHELIUM I) LOSS OF CELL POLARITYII) TIGHT JUNCTION INTEGRITY III) CELL-SUBSTRATE ADHESION
CAST FORMATION & TUBULAR OBSTRUCTION
TOXIC INJURY

Top Related