





Languages
Pages
Legal

Infectious Pediatric Pneumonia
Author: Roberta D. Hood, HBSc, MD, CCFP Lecturer, University of Toronto Date Created: December 2011
Global Health Emergency Medicine Teachi ng Modules by GHEM is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 3.0 Unported License.
Learning Objectives
To describe the presentation of pediatric pneumonia
To outline the management of pediatric pneumonia
To summarize the complications of pediatric pneumonia
To highlight interventions to prevent and protect against pediatric pneumonia

Outline Quiz Epidemiology and Pathophysiology Patient History Presentation and Diagnosis Management and Disposition Further Testing Complications Treatment Interventions to Protect Interventions to Prevent Summary Key Points Case Quiz Results

Quiz Question 1
What illness is the number one killer of
children? A. Diarrheal Disease B. HIV/AIDS C. Malaria D. Pneumonia
Quiz Question 2
What is the most sensitive and specific sign of
pneumonia in children? A. Difficulty breathing B. Fever C. Tachypnea D. Tachycardia

Quiz Question 3
If available, a chest x-ray should be done for
children with possible pneumonia: A. When a diagnosis is made B. When a history of tachypnea is present C. When antibiotics are started D. When complications are suspected

Quiz Question 4
Which of the following immunization
effectively reduce pneumonia mortality in
children? A. Haemophilus influenzae b Vaccine B. Pneumococcal Conjugate Vaccine C. Measles Vaccine D. All of the above

What is Pneumonia?
Pneumonia: an acute infection of the pulmonary parenchyma
The term “Lower Respiratory Tract Infection” (LRTI) may include pneumonia, bronchiolitis and/or bronchitis

Epidemiology and Pathophysiology

Epidemiology
Pneumonia kills more children under the age of five than any other illness in every region of the world.
It is estimated that of the 9 million child deaths in 2007, 20% (1.8 million) were due to pneumonia
Approximately 98% of children who die of pneumonia are in developing countries.

Epidemiology – Dadaab and Kakuma Refugee Camps (Kenya)
Data collected from 2007-2011 revealed that acute respiratory infections are the leading cause of morbidity and mortality in the camps.
In Dadaab camp acute respiratory infections were associated with 30% to 40% of deaths of children less than 5 years of age and up to 45% of morbidity in the same age group.

Millennium Development Goal
In 2000, the United Nations Member States committed to Millennium Development Goal 4 – to reduce the under five mortality rate by two thirds by 2015, compared to 1990.
Millennium Development Goal 4 can only be achieved by an intensified effort to reduce pneumonia deaths.

Question:
Is reducing the incidence, morbidity, and mortality of pneumonia in children a high priority in the region where you practice?
What is being done in your area?
Basic Pathophysiology
Most cases of pneumonia are caused by the aspiration of infective particles into the lower respiratory tract.
Organisms that colonize a child’s upper airway can cause pneumonia.
Pneumonia can be caused by person to person transmission via airborne droplets.

Etiology
• The common pathogens are a function of the patient’s age.
• The specific agent causing pneumonia can be determined in 1/3 to 2/3 of cases when cultures, antigen detection and serologic techniques are available.
• It is helpful to be aware of local outbreaks as clustering of cases is common.

Pneumonia - Common PathogensAge Group Common Pathogens (in Order of Frequency)
Newborn Group B StreptococciGram-negative bacilliListeria monocytogenesHerpes SimplexCytomegalovirusRubella
1-3 months Chlamydia trachomatisRespiratory Syncytial virusOther respiratory viruses
3-12 months Respiratory Syncytial virusOther respiratory virusesStreptococcus pneumoniaeHaemophilus influenzaeChlamydia trachomatisMycoplasma pneumoniae
From: Tintinalli JE et al. (2004). Emergency Medicine, A Comprehensive Study Guide, Sixth Edition. American College of Emergency Physicians. (pp. 784-789). McGraw-Hill. Toronto, ON.

Pneumonia - Common PathogensAge Group Common Pathogens (in Order of Frequency)
2-5 years Respiratory VirusesStreptococcus pneumoniaeHaemophilus influenzaeMycoplasma pneumoniaeChlamydia pneumoniae
5-18 years Mycoplasma pneumoniaeStreptococcus pneumoniaeChlamydia pneumoniaeHaemophilus influenzaeInfluenza viruses A and BAdenovirusesOther respiratory viruses
From: Tintinalli JE et al. (2004). Emergency Medicine, A Comprehensive Study Guide, Sixth Edition. American College of Emergency Physicians. (pp. 784-789). McGraw-Hill. Toronto, ON.
Pneumonia History

Pneumonia History Fundamentals Age Presence of cough, difficulty breathing,
shortness of breath, chest pain Fever Recent upper respiratory tract infections Associated symptoms (e.g.. headache,
lethargy, pharyngitis, nausea, vomiting, diarrhea, abdominal pain, rash)
Duration of symptoms

Pneumonia History
Immunizations status TB exposure Maternal Chlamydia, Group B Strep status
during pregnancy Choking episodes Previous episodes Previous antibiotics
Pneumonia History
• Ill contacts• Travel history• Day care attendance• Animal exposure
Dehydration is a sign of severe infection thatmay require hospitalization. Inquire about:• Fluid and nutrition intake• Urine output

History Fundamentals
• Past Medical History• Birth History• Medications• Allergies• Immunization Status• Home Environment• Social History• Family History

Diagnosis

Diagnosis Objectives
Recognition of the signs of pneumonia Diagnosis in a community setting Diagnosis in a health care setting Differential Diagnosis RSV and TB Diagnosis in the context of malnutrition,
and considering HIV

Recognition of Signs of Pneumonia
Tachypnea is the most sensitive and specific sign of pneumonia
Tachypnea had a Sensitivity of 61% and 79% and Specificity of 79% and 65% for pneumonia in malnourished and well-nourished Gambian children respectively

WHO Definition of TachypneaAge Respiratory
Rate(breaths/min)
Indication of severe infection (breaths/min)
< 2 months > 60 >70
2 to 12 months > 50
12 months to 5 years
> 40 >50
Greater than 5 years
> 20

Other signs of pneumonia -Indrawing
out---breathing---in Lower chest wall indrawing: with inspiration,
the lower chest wall moves in
From: Integrated Management of Childhood Illness. Chapter Three: Cough or difficulty breathing. World Health Organization. 2000”https://apps.who.int/chd/publications/referral_care/chap3/chap31.htm. Accessed February 2, 2012

Other signs of pneumonia - Nasal Flare
Nasal flaring: with inspiration, the side of the nostrils flares outwards
From: Integrated Management of Childhood Illness. Chapter Three: Cough or difficulty breathing. World Health Organization. 2000”https://apps.who.int/chd/publications/referral_care/chap3/chap31.htm. Accessed February 2, 2012

Diagnosis in Community Setting
SIGNS Classify AS Treatment
•Tachypnea•Lower chest wall indrawing•Stridor in a calm child
Severe Pneumonia •Refer urgently to hospital for injectable antibiotics and oxygen if needed•Give first dose of appropriate antibiotic
•Tachypnea Non-Severe Pneumonia
•Prescribe appropriate antibiotic•Advise caregiver of other supportive measure and when to return for a follow-up visit
•Normal respiratory rate Other respiratory illness
•Advise caregiver on other supportive measures and when to return if symptoms persist or worsen
From: Pneumonia The Forgotten Killer of Children. Geneva: World Health Organization (WHO)/United Nations Children’s Fund (UNICEF), 2006.
Infants at Risk of Pneumonia
Infants less than 3 months old with signs of pneumonia should be referred immediately to the nearest health facility because they are at high risk of severe illness and death.
Infants who were premature, and those with congenital heart disease or chronic lung disease are also at increased risk.

Diagnosis in a Health Care Setting• Vital signs that should routinely be taken in an
Emergency Care setting include:• Respiratory Rate• Heart Rate• Temperature• Oxygen saturation (if available)
• Any child with an increased respiratory rate should be immediately identified as having possible pneumonia.

Vital Signs
Both heart rate and respiratory rate are influenced by the presence of fever.
Heart rate increases by approximately 10 beats per minute for each 1 degree Celsius.
Respiratory Rate has been estimated to vary by 0.5-2 breath per minute to 5-11 breaths per minute for each 1 degree Celsius.

Does this infant child have pneumonia?
The Rational Clinical Exam, Journal of the American Medical Association
Observation of the infant is the most important part of the examination – does the child look sick?
Respiratory rate should be calculated over two thirty second intervals, or one minute due to moment to moment variability.
Auscultation is unreliable when examining infants.

Does this infant child have pneumonia?
Absence of tachypnea is the best individual finding for ruling out pneumonia.
Chest indrawing, other signs of increased work of breathing and abnormal findings on auscultation can be used toward ruling in pneumonia.
If clinical signs are negative (respiratory rate, auscultation, and work of breathing), it is unlikely that there will be chest x-ray findings.
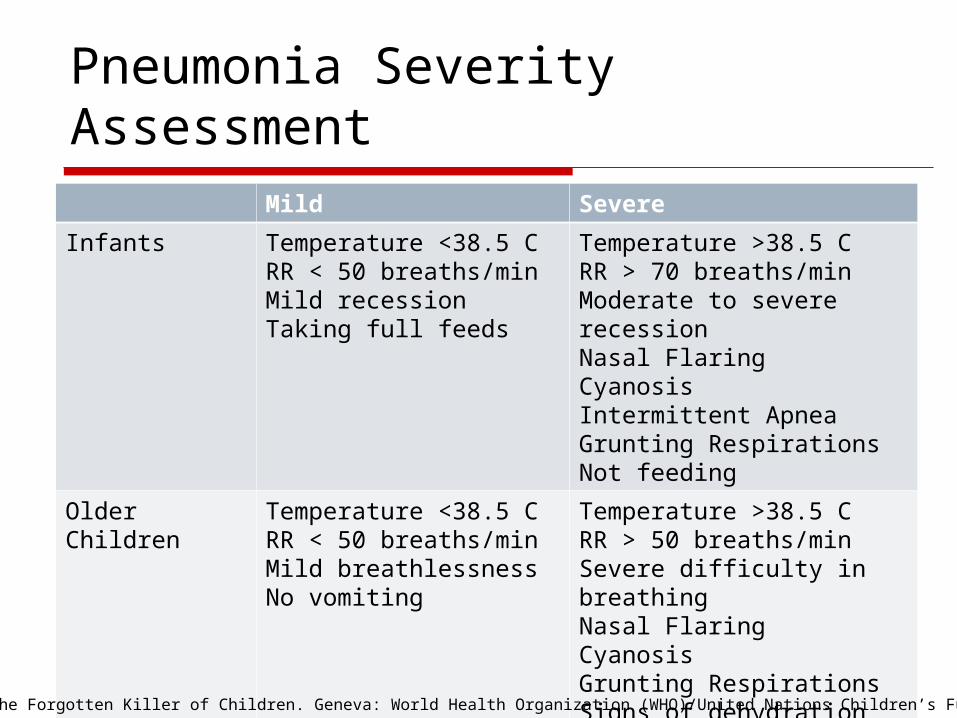
Pneumonia Severity AssessmentMild Severe
Infants Temperature <38.5 CRR < 50 breaths/minMild recessionTaking full feeds
Temperature >38.5 CRR > 70 breaths/minModerate to severe recessionNasal FlaringCyanosisIntermittent ApneaGrunting RespirationsNot feeding
Older Children Temperature <38.5 CRR < 50 breaths/minMild breathlessnessNo vomiting
Temperature >38.5 CRR > 50 breaths/minSevere difficulty in breathingNasal FlaringCyanosisGrunting RespirationsSigns of dehydration
From: Pneumonia The Forgotten Killer of Children. Geneva: World Health Organization (WHO)/United Nations Children’s Fund (UNICEF), 2006.

Differential Diagnosis: A Focus on Respiratory Syncytial Virus (RSV)

Respiratory Syncytial Virus (RSV)
RSV is the most common cause of LRTIs in children less than 1.
Infants and young children typically present with pneumonia or bronchiolitis.
Older children may have upper respiratory tract infection symptoms.
RSV is associated with apnea in infants. Wheezing is common.

RSV Seasonality
Seasonal outbreaks occur throughout the world.
In the northern hemisphere outbreaks peak in January and February.
In the southern hemisphere outbreaks peak in May, June and July.
In tropical climates outbreaks are often associated with the rainy season.

Differential Diagnosis: Consider Tuberculosis

Tuberculosis
Common symptoms of tuberculosis include: Chronic cough that has been present for
more than 3 weeks and is not improving Fever greater than 38°C for at least two
weeks, not attributable to other common causes
Weight loss or failure to thrive
Tuberculosis Physical exam findings of children with
pulmonary tuberculosis are similar to those of a lower respiratory tract infection.
In children less than age five tuberculosis can progress rapidly from latent infection to active disease and serve as a sentinel case in the community.
Consider the diagnosis of tuberculosis, especially in those children who fail to respond appropriately to routine treatment for pneumonia.

Pneumonia in Malnourished Children

Pneumonia in Malnourished Children
History of cough, fast breathing and difficulty breathing were significant predictors of pneumonia in malnourished children.
Only difficulty breathing was a significant predictor of pneumonia in well-nourished children.
As malnourished children are a high risk group, those who present with a history of cough, fast breathing, or difficulty breathing should be treated with antibiotics.
Fast breathing and lower chest wall indrawing are not specific predictors of pneumonia in malnourished children.

Pneumonia and HIV infected Children

Pneumonia and HIV infected Children
The prevalence of HIV-1 in children admitted with severe pneumonia (by WHO criteria) in Africa is 55-65%.
The case fatality rate is 20-34%. This case fatality rate is 3-6 times higher for children
infected with HIV compared to those not infected with HIV.
Pneumonia caused by Pneumocystis jiroveci may be the first indicator of HIV infection, and lead to HIV testing and diagnosis.

Question:
How are children who may have pulmonary tuberculosis identified and treated?
Malnourished children, and children with HIV are at high-risk for complications associated with pneumonia. How are these children managed where you practice?

Management and Disposition

Disposition The decision whether the patient would be best
managed at home or in a heath care setting is based on many factors, including the resources available.

Admission Considerations
If caregivers are unable to care for the child, or to commit to following a treatment plan, the child should be admitted to a health care facility.
Any child less than three months of age. Failure of outpatient treatment (worsening or
no response to treatment after 24 to 72 hours).
Family lives in a remote area.

Indications for Admission - IMCI
All Children with Very Severe Pneumonia need admission
Very Severe Pneumonia includes any of: Cough or difficult breathing plus at least one of the following: Central cyanosis Inability to breastfeed or drink, or vomiting everything Convulsions, lethargy or unconsciousness Severe respiratory distress (e.g. head nodding) Some or all of the other signs of pneumonia (tachypnea,
grunting, nasal flare, indrawing, changes in auscultation)

Indications for Admission
Age Group Indications for Admission to Hospital
Infants Oxygen Saturation <= 92%, cyanosisRR > 70 breaths /minDifficulty in breathingIntermittent apnea, gruntingNot feedingFamily not able to provide appropriate observation or supervision
Older Children Oxygen Saturation <= 92%, cyanosisRR > 50 breaths /minDifficulty in breathingGruntingSigns of DehydrationFamily not able to provide appropriate observation or supervision
From: British Thoracic Society (BTS) of Standards of Care Committee. BTS Guidelines for the Management of Community Acquired Pneumonia in Childhood. Thorax. 2002;57: i1-i24.

In-Patient Management
Consideration must be given to the provision of adequate hydration, oxygenation, nutrition, antipyretics and pain control.
Monitoring should include: Respiratory rate Work of breathing Temperature Heart rate Oxygen saturation (if available) Findings on auscultation.

In-Patient Considerations
Due to the risk of transmission, a child suspected of having pneumonia should be cared for in an area that is isolated from others to who are at risk of becoming infected.
Contact precautions by health care workers such as hand washing, gloves, gowns and masks to prevent transmission between patients are often appropriate.

Criteria for Intensive Care
If intensive care is available consider the following: The patient is failing to maintain an oxygen
saturation of > 92% in FiO2 of > 0.6. The patient is in shock. There is a rising respiratory rate and rising pulse
rate with clinical evidence of severe respiratory distress and exhaustion, with or without a raised arterial carbon dioxide tension (PaCO2).
There is recurrent apnea or slow irregular breathing.
Management of Respiratory Distress and Respiratory Failure: ABC’s and Intubation
Airway
Support the airway (position of comfort for the child) or open the airway (chin lift or jaw thrust).
Clear the airway (suction nose and mouth, remove any foreign body).
Insert an oropharyngeal or nasopharyngeal airway as indicated.

Breathing
Assist ventilation (e.g., bag-mask ventilation) as needed
Provide oxygen Continuously monitor oxygen saturation Consider use of CPAP or BIPAP Prepare for endotracheal intubation as
needed Administer medications as needed
Circulation
Monitor heart rate and rhythm Establish vascular access as indicated (for
fluid therapy and medications)

Indications for Intubation
Inadequate oxygenation or ventilation Inability to maintain and/or protect the
airway Potential for clinical deterioration Prolonged patient transport or diagnostic
studies

Indications for Intubation Respiratory failure is the most common indication for
intubation in children with pneumonia
Clinical evidence of respiratory failure: Poor or absent respiratory effort Poor colour Obtunded mental status
Oxygen saturation and end-tidal carbon dioxide can be used to support the decision to intubate, but intubation should not be delayed if there is clinical evidence of respiratory failure

Relative Contraindications to Intubation
No absolute contraindications
Caution using rapid sequence intubation with neuromuscular blockade in a child difficult to bag and mask
High-risk intubation (e.g.. suspected epiglottitis)
Airway trauma that may require a surgical airway

Intubation Pointers
Detailed Pediatric Airway management is beyond the scope of this module
Endotracheal tube size calculations:Uncuffed tube = 4 + (age in years/4)Cuffed tube = 3.5 + (age in years/4)
Ventilation: begin with 8-10 breaths per minute

Question:
What resources do you have available to care for children with pneumonia?
What are the criteria for hospital admission/ transfer to another facility/intensive care where you practice?

Further Testing

Chest X-ray
Confirmation of pneumonia by chest x-ray is not indicated in children with mild, uncomplicated lower respiratory tract infections who will be treated at outpatients.

Chest X-ray A study in South Africa randomized children
age 2-59 months who met the WHO case definition of pneumonia to have a chest x-ray, or not.
There was no clinically identifiable subgroup of children within the WHO case definition who were found to benefit from a chest x-ray.
It was concluded that there was no benefit in routine chest x-ray of ambulatory children with lower respiratory-tract infection over two months of age.

Chest X-ray
Consider if available and: Infection is severe Diagnosis is otherwise inconclusive To exclude other causes of shortness of
breath (e.g.. foreign body, heart failure) To look for complications of pneumonia
unresponsive to treatment (e.g.. empyema, pleural effusion)
To exclude pneumonia in an infant less than three months with fever

Right Upper Lobe Pneumonia

Right Middle Lobe Pneumonia

Laboratory Investigations
Routine blood work is not required in children with uncomplicated lower respiratory tract infections who will be treated as outpatients
Tests to consider if available: CBC, particularly WBC Electrolytes, particularly Sodium Consider blood cultures, sputum cultures HIV and TB testing as appropriate

Question:
What tests do you have readily available to assist in the management of a child with complications of pneumonia?
What other testing could reasonably be arranged?

Complications

Complications of Pneumonia
Pleural effusion – fluid in the pleural space as the result of inflammation.
Empyema – bacterial infection in the pleural space.
Parapneumonic effusions develop in approximately 40% of patients admitted to hospital with bacterial pneumonia.
If an effusion is present and the patient is persistently febrile, the pleural space should be drained.

Complications of Pneumonia
Necrotizing Pneumonia – necrosis or liquefaction of lung parenchyma.
Lung Abscess – A collection of inflammatory cells leading to tissue destruction resulting in one or more cavities in the lungs. A rare complication.
Treatment of both Necrotizing Pneumonia and Lung Abscess involves long term parenteral antibiotics for 2-4 weeks, or 2 weeks after the patient is afebrile, and has clinically improved.

Complications of Pneumonia
Pneumatocele – thin walled, air filled cysts of the lung, often occurs with empyema.
Pneumatoceles often resolve spontaneously, but may lead to pneumothorax.
Complications of Pneumonia Hyponatremia:
Serum sodium <135 mmol/L. Studies in India (1992) revealed that in children
hospitalized with pneumonia, 27% had hyponatremia and 4% had hypernatremia.
SIADH was the most common cause of hyponatremia.
Hyponatremia is associated with increased hospital stay, complications and increased mortality, however most cases were found to be mild.
Treatment

Treatment - Epidemiology Antibiotics serve an essential role in reducing
child deaths from pneumonia.
Limited data suggest that in the early 1990’s less than one in five children with pneumonia received antibiotics.
Children in urban areas, and those with well educated mothers were more likely to receive antibiotics.
Treatment – Oral Antibiotics
Common medications for treating pneumonia: Penicillins: Amoxicillin, Amoxicillin-
Clavulanate Sulfonamides: Co-trimoxazole Macrolides: Azithromycin, Clarithromycin,
Erythromycin 2nd generation Cephalosporins: Cefaclor Dose according to child’s weight

Treatment – IV Antibiotics
Common medications for treating pneumonia: Penicillins: Amoxicillin, Ampicillin, Benzyl
Penicillin 2nd generation Cephalosporins: Cefuroxime 3rd generation Cephalosporins: Cefotaxime Dose according to child’s weight

Treatment – IMCI Guidelines
Antibiotic therapy Chloramphenicol (25 mg/kg IM or IV every 8
hours) until the child has improved. Then continue orally 3 x/ day for a total course of 10 days.
If chloramphenicol is not available, give benzylpenicillin (50 000 units/kg IM or IV every 6 hours) and gentamicin (7.5 mg/kg IM once a day) for 10 days.

Treatment – IMCI Guidelines
If the child does not improve within 48 hours, Switch to gentamicin (7.5 mg/kg IM once a
day) and cloxacillin (50 mg/kg IM or IV every 6 hours), for staphylococcal pneumonia.
When the child improves, continue cloxacillin (or dicloxacillin) orally 4 times a day for a total course of 3 weeks.

Outpatient Antibiotic Choice
The British Thoracic Society suggests amoxicillin as the first line outpatient antibiotic for community acquired pneumonia in children of all ages.
For children age 5 and older who can be managed as outpatients, atypical bacteria mycoplasma pneumoniae and chlamydia pneumoniae are the most common cause. A macrolide can be considered as the first line treatment in these children.

Treatment
In a study conducted in areas of Pakistan with high levels of Streptococcus pneumoniae and Haemophilus Influenzae b resistance to co-trimoxazole, co-trimoxazole was found to be over 90% effective in treating cases of non-severe pneumonia.
In cases of severe pneumonia, amoxicillin was more effective than co-trimoxazole.
Inpatient Antibiotic Choice
Consider IV 3rd Generation Cephalosporin in a child less than 1 year of age, or who is not fully immunized, or with severe illness.
Consider IV Ampicillin or Penicillin in a child over 1 year of age in areas that do not have a high prevalence of penicillin-resistant Streptococcus Pneumoniae.

Oral vs. IV Antibiotics
A non-blinded randomized controlled trial in England found that oral amoxicillin was equivalent to IV benzyl penicillin for children admitted to hospital, although the sickest children were excluded from the study.
Patients were excluded for: wheezing, hypotension, chronic pulmonary conditions (other than asthma), immunodeficiency, pleural effusion requiring drainage, oxygen saturation <85% on room air.

Treatment
Three studies (two in Gambia, one in Turkey) published between 1988 and 1995 comparing co-trimoxazole treatment with parenteral procaine penicillin G, ampicillin, or chloramphenicol showed no significant improvement in efficacy with the alternative antibiotic regimens.

Antibiotic Resistance
Expanded and continued use of antibiotics to treat pneumonia could make antibiotic resistance an increasing challenge in the future.
Increased treatment of pneumonia with antibiotics must be accompanied by appropriate training of health care workers to ensure proper diagnosis and treatment of pneumonia.

Question:
What antibiotics are commonly used and/or readily available where you practice?
What are the costs?
What is the antibiotic resistance in your local area?

Supportive Treatment – IMCI Guidelines
Oxygen therapy
If fever (=>39oC) causing distress, give paracetamol
If wheeze is present, give a rapid-acting broncho-dilator
Gentle suction any thick secretions in the throat, which the child cannot clear.

Supportive Treatment – IMCI Guidelines Ensure that the child receives daily maintenance fluids for
the child's age - avoid overhydration. Encourage breastfeeding and oral fluids. If the child cannot drink, insert a NG tube and give
maintenance fluids in frequent small amounts. If the child is taking fluids adequately by mouth, do not use a
NG tube as it increases the risk of aspiration pneumonia. If oxygen is given by nasopharyngeal catheter at the same time
as NG fluids, pass both tubes through the same nostril.
Encourage the child to eat as soon as food can be taken.

Interventions to Protect Against Pneumonia

Interventions to Protect Against Pneumonia
It is estimated that hand washing, when combined with improved water and sanitation could lead to a 3% reduction in all child deaths.
Promote exclusive breast feeding for 6 months. Impact 15-23% reduction in pneumonia incidence. 13% reduction in all child deaths. Shown to be cost effective.

Interventions to Protect Against Pneumonia
Adequate nutrition throughout the first five years of life, including adequate micronutrient intake. Impact 6% reduction in all child deaths for adequate complementary feeding (age 6-23 months).
Reduce incidence of low birth weight.

Public Awareness
Tachypnea and respiratory distress are considered the most important signs in the diagnosis of pneumonia.
Only 1 in 5 caregivers know that fast breathing and respiratory distress are a reason to seek care immediately.

Care Seeking Behaviour
In developing countries only half of the children with pneumonia are taken to an appropriate health care provider.
Rates are similar between boys and girls. Children who are rural, poorer, and those
with less educated mothers are less likely to be taken to an appropriate health care provider.

Question:
Are parents and/or caregivers in your area aware of the signs that indicate their child should see a health care provider?

Intervention to Protect Against Pneumonia
Reducing indoor air pollution, by changing to cleaner gas or liquid fuels or high-quality, well maintained biomass stoves, may reduce the incidence of pneumonia by 22 to 46% in appropriate settings. This intervention may be cost-effective in low-income settings.

Intervention to Protect Against Pneumonia
Reduce Exposure to Second-Hand Tobacco Smoke.
Both maternal and paternal smoking cause lower respiratory tract illnesses such as pneumonia and bronchitis, particularly during the first year of life.
Question:
Would changing to cleaner cooking options be helpful in the region where you practice? Are there cultural barriers to change?
Would education on smoking cessation be helpful in your area?
Interventions to Prevent Pneumonia

Prevention Strategies Vaccination against measles, Streptococcus
pneumoniae, and Haemophilus influenzae type b
Zinc supplementation Prevention of HIV in Children Co-trimoxazole prophylaxis for HIV-infected
children

Prevention - Vaccination
Three vaccinations have the potential to significantly reduce childhood deaths from pneumonia
Haemophilus Influenzae type B (Hib) vaccine and Pneumococcal conjugate vaccine prevent infections that directly cause pneumonia
Pneumonia is a possible complication of Measles, thus prevention of measles would decrease the incidence of pneumonia.

Prevention - Vaccination
The implementation of Haemophilus influenzae type b (Hib) and Streptococcus pneumoniae immunization through an existing immunization program has been shown to be cost effective in reducing pneumonia mortality.
Measles immunization coverage is high (making cost effectiveness estimates difficult).

Measles Vaccine 2010
From: WHO. Immunization Surveillance Assessment and Monitoring.
[http://www.who.int/immunization_monitoring/diseases/measles/en/index.html]. Accessed on December 9,2011.

HIB Vaccine 2008
From: GAPP. Geneva: WHO/UNICEF, 2009.

Pneumococcal Conjugate Vaccine 2008
From: GAPP. Geneva: WHO/UNICEF, 2009.

Question:
What immunizations are given in your area?
Are there plans to expand immunization programs in your area?

Prevention – Zinc Supplementation
Zinc supplementation in Bangladesh has been shown to reduce pneumonia mortality in children in children less than 2 years.
Zinc supplementation was also shown to reduce the incidence of pneumonia, other upper and lower respiratory tract infections and diarrhea.
Doses of 70 mg per week have been found to be effective.

Prevention – Zinc Supplementation
Zinc supplementation had been shown to be cost-effective in reducing pneumonia mortality.
Prevention of HIV in Children
It is estimated that prevention of HIV in children would lead to a 2% reduction in all child deaths.

Prevention – Co-trimoxazole Prophylaxis for HIV-infected Children
Children with features of HIV should receive daily Co-trimoxazole even in areas of high bacterial resistance this medicine.
Daily Co-trimoxazole prophylaxis has been shown to decrease mortality in HIV infected children.

Co-trimoxazole Prophylaxis
In the CHAP study in Zambia (Lancet, 2004), a double-blind, randomized placebo controlled trial, at 19 months the mortality rate for enrolled children was 28% in the Co-trimoxazole group and 42% in the placebo group.
The study was stopped early with the conclusion that all HIV infected children in resource poor areas should receive Co-trimoxazole prophylaxis.
Summary

Key Points
Pneumonia is an acute infection of the pulmonary parenchyma
Pneumonia kills more children under the age of five than any other illness.
A diagnosis of pneumonia should be considered in all children with tachypnea and difficulty breathing.
Common first-line antibiotics include amoxicillin and co-trimoxazole .

A Complicated Case from Gambia
Based on a true story

Case – Chief Complaints
A 1 year old child is brought in for fever, cough, lethargy, and mild respiratory distress increasing over 2 weeks.
You take a focused medical history from the child’s mother.
What are the patient’s vital signs?

Vital Signs
Vital signs are as follows: Temperature 38.7, Pulse 150, Respiratory Rate 54, Oxygen Saturation 94% on room air.
What is observed on physical examination?

Physical Examination
On observation the patient clearly appears septic. Mild respiratory distress is present. Skin is mottled.
What is the likely diagnosis?
Diagnosis
It is reasonable to make a presumptive diagnosis of pneumonia based on the history and vital signs.
What other physical examination information is immediately relevant to forming an initial treatment plan for this patient?
Weight and Hydration Status
The child’s weight is z score was minus 2
(but 1 lb more and would have been minus 3 i.e.. severe malnutrition)
The patient appears mildly dehydrated.
What interventions should be started?

Initial Treatment
A presumptive diagnosis of pneumonia is made. The patient is admitted to the hospital and started on broad spectrum IV antibiotics and appropriate hydration and re-feeding.
The patient does not seem to improve initially.
What is your differential diagnosis?

Differential Diagnosis
Differential Diagnosis includes:Pneumonia +/- complications (e.g. Empyema)Pneumonia in a patient with HIVTuberculosis
What is the first investigation you would order? (assume first choice investigation is available).
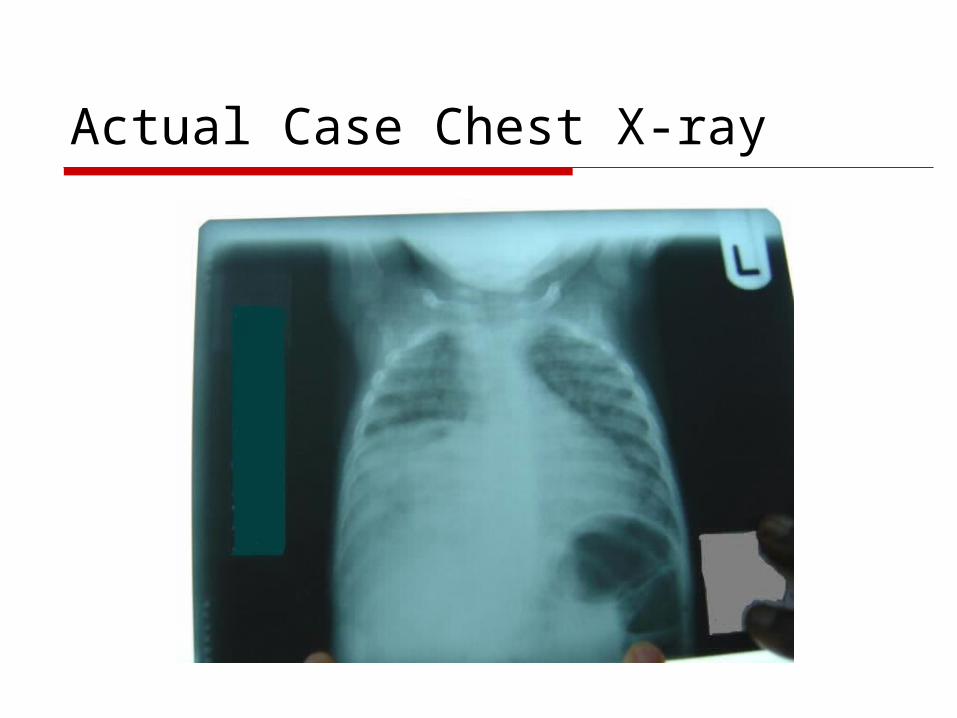
Actual Case Chest X-ray

Chest X-ray Interpretation
The chest x-ray reveals a right sided lobar infiltrate.
What is the clinical correlation?

Clinical Course
The patient begins to improve clinically. Fever, cough and respiratory distress resolve. However, over the next few weeks of
appropriate re-feeding, the patient fails to gain weight despite remaining on broad spectrum antibiotics.
What other investigations would you consider?

Other Investigations HIV test – negative TB skin test – unreactive Sputum culture – unable to induce sputum
*Important Note: The mother is no longer with the patient. Another family member reports that she is sick with a cough, fever, and weight loss.*
What other courses of treatment should be considered in this case?
Treatment and Outcome
The patient was started on treatment for tuberculosis and began to improve and gain weight.
This patient did well. The mother and other close contacts were also treated for tuberculosis.

Learning Point
This patient’s x-ray revealed a lobar infiltrate. Pneumonia commonly presents as a lobar
infiltrate. Reactivation of TB tends to be apical, but
acute TB can present as a lobar infiltrate. TB should remain as a differential diagnosis
and be reconsidered if there is a poor response to treatment, or a possible exposure history.

Post-Test

Quiz Question 1
What illness is the number one killer of children?
A. Diarrheal Disease B. HIV/AIDS C. Malaria D. Pneumonia

Quiz Question 2
What is the most sensitive and specific sign of pneumonia in children?
A. Difficulty breathing B. Fever C. Tachypnea D. Tachycardia

Quiz Question 3
If available, a chest x-ray should be done for children with possible pneumonia
A. When a diagnosis is made B. When a history of tachypnea is present C. When antibiotics are started D. When complications are suspected

Quiz Question 4
Which of the following immunizations effectively reduce pneumonia mortality in children?
A. Haemophilus influenzae b Vaccine B. Pneumococcal Conjugate Vaccine C. Measles Vaccine D. All of the above

Quiz Answers:
1. D. Pneumonia 2. C. Tachypnea 3. D. When complications are suspected 4. D. All of the above

Millennium Development Goal
Please use the information in this presentation to help achieve Millennium Development Goal 4 – to reduce the under five mortality rate by two thirds by 2015, compared to 1990.
Millennium Development Goal 4 can only be achieved by an intensified effort to reduce pneumonia deaths

Further Reading Considerable content and structure for this presentation
is based on the following reports, which are recommended for further reading:
Global Action Plan for Prevention and Control of Pneumonia (GAPP). Geneva: World Health Organization (WHO)/United Nations Children’s Fund (UNICEF), 2009.
Pneumonia The Forgotten Killer of Children. Geneva: World Health Organization (WHO)/United Nations Children’s Fund (UNICEF), 2006.
Top Related