







Languages
Pages
Legal


Environmental Issues in Sports MedicineJeremiah Penn, MDSanford Orthopedics and Sports MedicineBismarck, ND

Lecture Objectives
� Identify common environmental illnesses
� Describe prevention of environmental illness
� Describe treatment for life-threatening and non-emergent environmental illness

Mt Everest 29,029 ft above sea level
First climbed by Edmund Hillary and Tenzing Norgay on May 29, 1953
Number of summits in 1975: 15
Number of summits in 1995: 83
Number of summits in 2004: 330
Number of summits in 2010: 513
Introduction
� Outdoor sports are increasing in popularity
� Participants are becoming more “extreme”
� Family physicians need to be able to recognize and treat these problems in their patient population
Environmental Illness
� Heat related Illness
� Cold injury
� Altitude
� UV Light
� Lightning

Heat related Illness
� Heat edema
� Heat rash
� Heat syncope
� Heat cramps
� Heat exhaustion
� Heat stroke

Human Heat Loss
� Convection
� Conduction
� Evaporation
� Radiation

Chicago Marathon 2007

Wet Bulb Globe Temperature
� Developed by USMC in 1956 at Parris Island, SC
� Takes into account temperature, humidity, wind speed, and solar radiation
� WBGT = 0.7Tw + 0.2Tg + 0.1Td

Wet Bulb Globe Temperature
Category Temperature (°F) Flag
1 <79.9 None
2 80 – 84.9 Green
3 85 – 87.9 Yellow
4 88 – 89.9 Red
5 ≥90 Black

Heat Index Chart
� Developed by RG Steadman in 1979
� Takes into account temperature and relative humidity
� Much easier to calculate, don’t need special equipment

Heat Edema
� Transient venodilation to facilitate core heat loss
� Normal body temperature
� Dependant edema
� Treat with hydration, elevation of lower extremities, and cooling

Heat Rash
� Also called prickly heat, miliaria rubra
� Profuse sweating saturates skin and clogs sweat ducts
� Pruritic rash, normal body temperature
� Treat with cooling, reduced clothing, antihistamines, lotions

Heat Syncope
� Occurs at end of activity in elevated temperatures
� Decrease in muscle contractions combined with peripheral vasodilation
� Normal body temperature
� Present with orthostasis, syncope, rapid mental status recovery when supine
� Treat with cool environment, supine position, elevated legs, fluid replacement, untie shoes

Heat Cramps
� Generally not acclimated to conditions
� Excess heat exposure with profuse sweating
� Generally inadequate fluid and electrolyte intake
� Temp <104 °F
� Painful muscle spasms, usually calves, quads, abdominal muscles
� Treat with stretching, cooling, fluid and electrolyte replacement
� Pickle juice, Gatorade with extra salt


Korey Stringer
May 8, 1974 – August 1, 2001

Heat Exhaustion
� May be initial presentation of heat illness
� Body temperature between 98.6 °F and 104 °F
� Malaise, fatigue, dizziness
� May have profuse sweating, nausea/vomiting, headache, fainting, weakness, cold/clammy skin, tachycardia
� Normal mental status
� Stable neurologic status
� May progress to heat stroke if not recognized and treated

Heat Stroke
� Symptoms of heat exhaustion along with the following
� Core temp >104 °F
� Hot skin with or without sweating
� CNS disturbance (Confusion, ataxia, irritability, coma)
� May have hypotension, seizure, hyperventilation
� Classic vs. Exertional

Risk Factors
� Age <15 or >65
� EtOH, medications
� Dehydration**
� Prev. heat illness
� Poor acclimatization
� Overmotivation
� Sickle cell trait
� Activity level
� Obesity
� Excessive clothing
� Lack of water/shade
� Temperature
� Humidity
� WBGT

Medications
� Alpha adrenergic agents
� Amphetamines
� Anticholinergics
� Antihistamines
� Antihypertensives
� Benzodiazepines
� Illicit drugs
� Laxatives
� MAOIs
� Thyroid agonists
� TCAs
� Typical antipsychotics
� Dietary supplements
� EtOH

Prevention
� Education (athletes, coaches, trainers)
� Acclimatization (NCAA, ACSM guidelines)
� Daily weights to monitor for dehydration
� Proper uniforms
� Condition monitoring
� Adjusting practice times

Treatment
� Medical Emergency!
� Rectal Temp
� ABCs
� Cool first, then transport
� Ice bath
� Cool mist and fan
� Ice at groin/axilla

Complications
� Seizures
� benzodiazepines
� Hypotension
� IV fluids, may need pressors
� Rhabdomyolysis
� IV fluids, diuretics, alkalinize urine (pH > 7)
� Liver damage
� Avoid acetaminophen
� Arrythmias
� Avoid cardioversion until myocardium has cooled

Return to Play
� Mild illness – 24 hours post event with proper rest and rehydration
� Heat stroke – at least one week
� Monitor daily weights
� Normalization of lab values
� Graduated return to activity
� Address all risk factors

Cold Injury
� Hypothermia
� Frostbite
� Trenchfoot

Hypothermia
� Normal core temperature 99.6 °F(+/- 4 °F)
� Thermoregulation through hypothalamus
� Voluntary muscular activity
� Involuntary shivering
� Increased metabolic rate (higher epi and norepi)
� Peripheral vasoconstriction

Hypothermia
� Risk factors
� CNS depressants
� Phenothiazines
� Hypoglycemia, peripheral neuropathy, hypothyroidism, adrenal insufficiency
� Ethanol
� Age
� Exhaustion
� Malnutrition

Hypothermia
� Core temp <95 °F
� 1.8% increase in mortality rate with each 1.8 °F drop in core temperature
� Need a true core temperature (rectal temp with appropriate thermometer)
Mild Hypothermia
� Core temp 90° -95° F
� Cool, pale, core
� Uncontrolled shivering
� Dysarthria
� Ataxia
� Confusion
� Tachycardia
� Maximal peripheral vasoconstrictions
Moderate Hypothermia
� Core temp 82 ° - 90° F
� Loss of shivering
� Cardiac conduction irregularities
� Afib
� J waves

Severe Hypothermia
� Looks dead, core temp <82 °F
� No pulse or blood pressure
� Agonal or absent respirations
� Dilated pupils, areflexic
� Ventricular arrhythmia on EKG
Hypothermia
� Prevent further heat loss
� Passive external rewarming
� Active external rewarming
� Warm blankets
� hot water bottles
� Warmed forced air
� Active Core rewarming
� Warmed IV fluids
� Warmed oxygen
� NG, colonic, bladder irrigations
� Peritoneal dialysis
� Cardiopulmonary bypass
� Hemodialysis
Hypothermia
� ABCs
� Limit movement
� Avoid chest compressions if any cardiac or respiratory activity
� A patient isn’t dead until he’s warm and dead


Frostbite
� Direct freezing of tissues
� Ambient temp < 32° F
� Exposed areas and distal extremities most at risk
� Risk factors include
� Raynauds, PAD, constrictive clothing, nicotine

Frostbite
� Tissue cooling, vasoconstriction, hyperviscosity
� Extracellular ice formation
� Intracellular dehydration and hyperosmolality
� Cell membrane damage
� Microcirculatory stasis, sludging, thrombosis, leads to hypoxia
� Thawing leads to capillary leakage and tissue edema, causing more ischemia
� Usually several freeze thaw cycles in severe injuries

1st Degree Frostbite
� Partial skin freezing
� Erythema, edema, hyperemia, no blisters
� No necrosis
� Skin may peel a week or two later
� Stings, throbs, aches, burns, hyperhidrosis

2nd Degree Frostbite
� Full thickness injury
� Erythema, edema
� Vesicles with clear fluid
� May form blackened eschar
� Numbness, vasomotor dysfunction if severe

3rd Degree Frostbite
� Full thickness skin and subQ freezing
� Hemorrhagic blisters
� Skin necrosis
� Blue-gray discolorations

4th Degree Frostbite
� Full thickness, skin, subQ, muscle, tendon, and bone freezing
� Little edema
� Mottled, deep red, or cyanotic
� Becomes dry, black, and mummified

Frostbite
� Rewarm in 104 -108 F water bath
� Ensure no refreezing
� Very painful process (narcotics and NSAIDs)
� Tetanus immunization
� After rewarming, separate digits and splint

Frostbite
� Debride clear blisters but not hemorrhagic ones
� Early surgery for compartment syndrome or escharotomy
� Amputation after tissue injury demarcates unless infected (may take several weeks)
� Physeal injury may develop in children with frostbite

Trenchfoot
� Lengthy exposure to cold water (32 °-50° F)
� Prolonged vasoconstriction leads to ischemia
� Appears hyperemic, then cyanotic mottling and swelling
� May have persistant paresthesias
� Prevent with frequent sock changes and keeping shoes dry

Altitude Ilness
White Butte, ND Elevation 3,506 ftMt. Whitney, CA Elevation 14,505 ft
Altitude Illness
� Exponential drop in partial pressure of oxygen
� At 10,000 ft, 42% of people with experience altitude illness
� Risk factors include increasing altitude, rate of ascent, sleeping altitude, previous hx of altitude illness, permanent residence at low altitude, level of exertion at high altitude
Altitude Illness
� High Altitude Headache
� Acute Mountain Sickness
� High Altitude Cerebral Edema
� High Altitude Pulmonary Edema

HAH/AMS
� High altitude headache – usually attributed to lack of sleep, poor nutrition, or dehydration
� Treat with NSAIDs or acetominophen
� Acute mountain sickness – HAH plus 1 of the following: GI irritation, dizziness, fatigue, or sleep disturbance
� Treat with stopping ascent (rare), descent, oxygen, dexamethasone, acetazolamide

High Altitude Cerebral Edema
� Defined as altered conciousness or ataxia in someone with AMS or HAPE
� Drowsiness, poor decision making, pyschomotorslowing, stupor
� Exam may reveal papilledema, retinal hemorrhages, global encephalopathy
� Untreated, leads to death via cerebral herniation
High Altitude Pulmonary Edema
� Most common cause of death from altitude related illness
� Dry cough and decreased exercise tolerance
� Progresses to tachycardia, resting tachypnea, hemoptysis, respiratory distress and fever
� Treat with descent, supplemental oxygen, nifedipine, nitric oxide
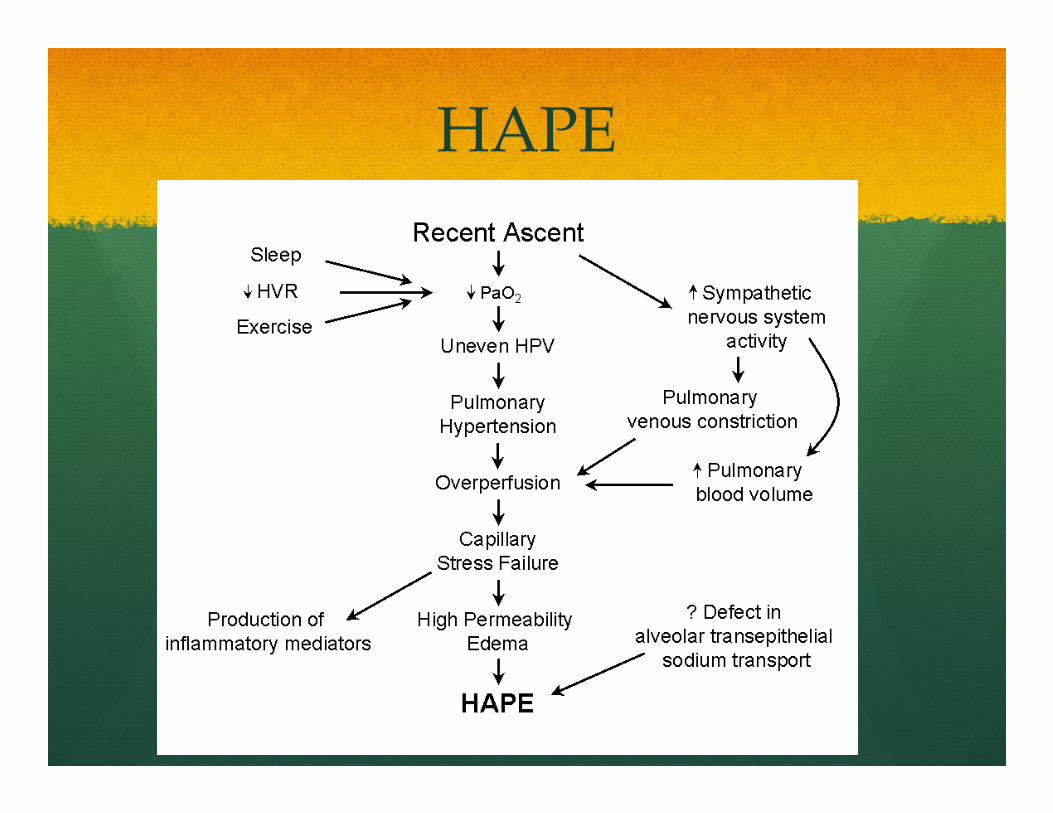
HAPE

Altitude Illness


UV Light
� Outdoor competition increases UV exposure
� Short term consequences of sunburn
� Long term consequences of melanoma, basal cell cancer and squamous cell cancer

UV Light
� UVA - makes up 90% of UV light, wavelength of 320-400 nm, penetrates to deep cutaneous tissue, damages DNA through free radical formation
� UVB – wavelength of 290 to 320 nm, primary cause of sunburn
� UVC – wavelength of 200-290 nm, blocked by ozone

Sunburn
� Direct injury from UV radiation
� Vasodilation leading to erythema, edema, vesicles, and bullae
� Initial symptoms at 3-5 hours post exposure, peaking at 24 hours

Skin Cancer
� Frequent severe sunburns as a youth increase risk of melanoma and basal cell cancer
� Prolonged exposure at lower levels increases risk of squamous cell CA

UV Light
� Treat sunburns with moisturizers and pain medications
� Options include topical and systemic steroids, NSAIDS, antihistamines, antioxidants, emollients
� Prevent sun damage with UVA/UVB sunscreen with SPF between 15-30
� SPF 15 filters 92% of UVB exposure
� Participate at low sun times and wear protective clothing

Lightning
� About 300 injuries per year in the US
� 70-90 % of victims survive but 75% have permanent injuries
� Highest incidence of injury in areas of highest lightning flashes (Central Florida in US)

Lightning
� 3 sources of injury
� Electrical current
� Heat production
� Concussive force
� 3 forms of human contact
� Direct Strike (3-5%)
� Contact (1-2%)
� Side flash/splash (35%)
Lightning
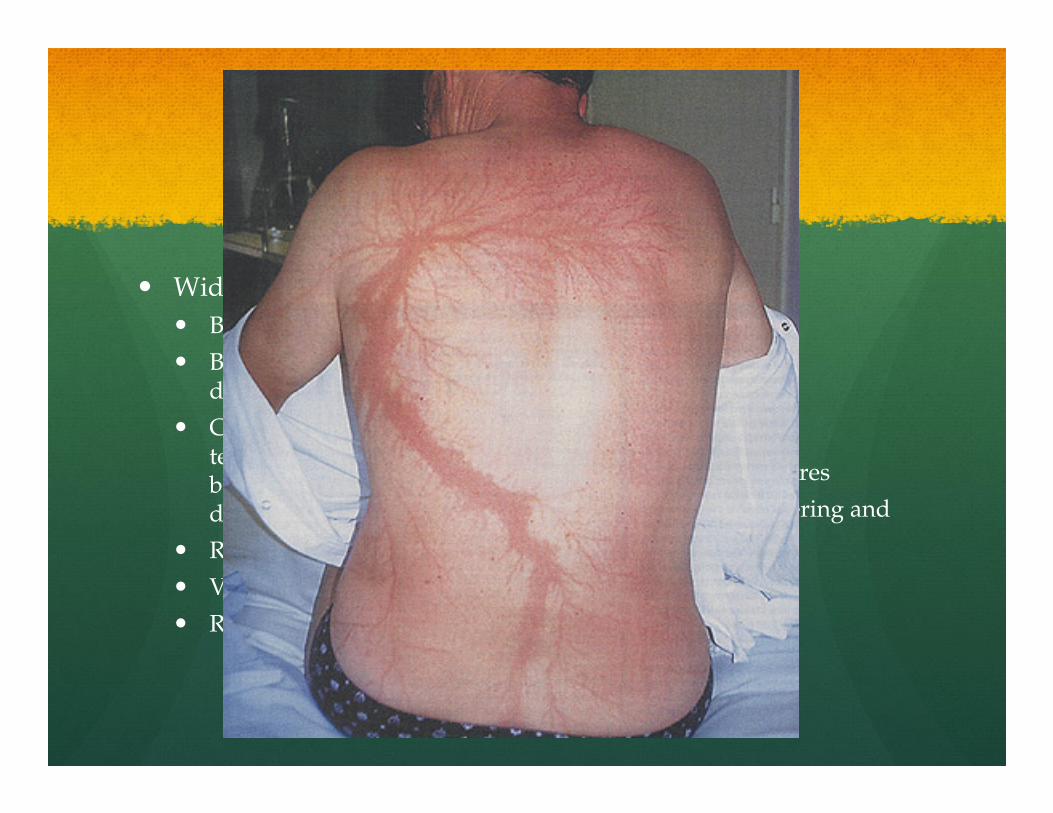
� Wide spectrum of injuries
� Blunt force trauma
� Bilateral shoulder dislocation and cervical fx
� Confusion, amnesia, temporary deafness or blindness, LOC, dysesthesia or paralysis
� Respiratory arrest
� Vfib/cardiac arrest
� Rhabdomyolysis (rare)
� Burns
� Contact
� Flash
� Linear
� Punctate
� Lichtenberg figures
� Superficial blistering and erythema

Lightning
� ATLS protocol
� EKG, C-spine films
� UA, chem 14, cardiac profile
� Burn treatment/referral
� Post-injury support network
Lightning
� 30 seconds - 30 minutes rule
� Shelter in substantial building or metal roofed automobile
� Increased storm activity on summer afternoons, also peak time for sporting events
Thank You
Top Related