





Languages
Pages
Legal

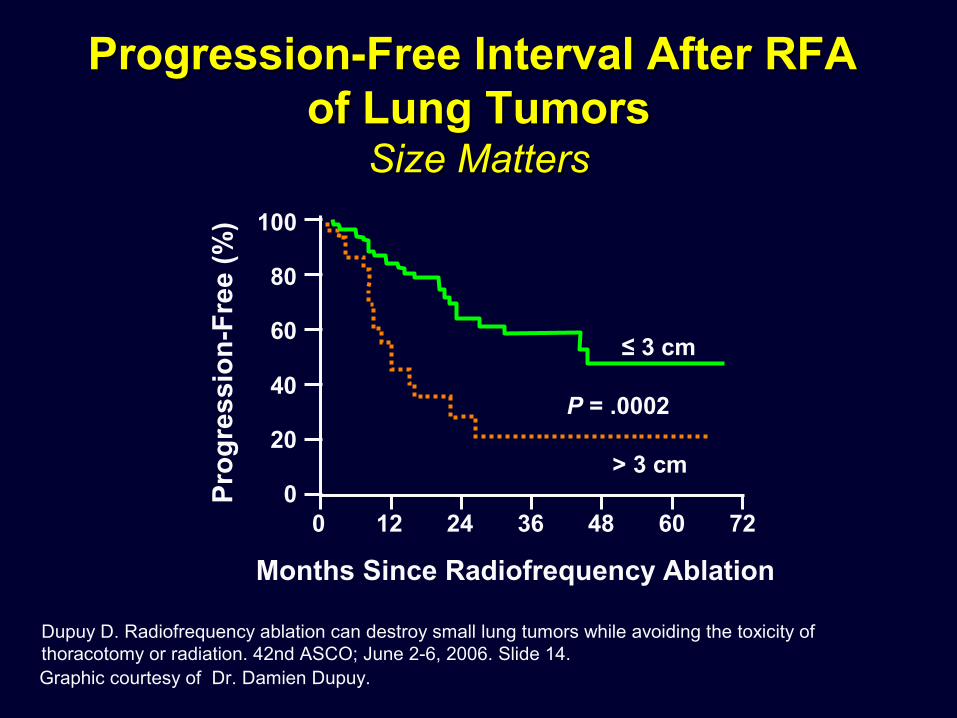
Graphic courtesy of Dr. Damien Dupuy.
Dupuy D. Radiofrequency ablation can destroy small lung tumors while avoiding the toxicity of thoracotomy or radiation. 42nd ASCO; June 2-6, 2006. Slide 14.
Progression-Free Interval After RFA Progression-Free Interval After RFA of Lung Tumorsof Lung Tumors
Size MattersSize Matters
100
80
60
40
20
00 12 24 36 48 60 72
≤ 3 cm
> 3 cm
P = .0002
Pro
gre
ssio
n-F
ree
(%)
Months Since Radiofrequency Ablation

Graphic courtesy of Dr. Damien Dupuy.
Dupuy D. Radiofrequency ablation can destroy small lung tumors while avoiding the toxicity of thoracotomy or radiation. 42nd ASCO; June 2-6, 2006. Slide 14.
Radiofrequency Ablation/Radiation Radiofrequency Ablation/Radiation Therapy in NSCLCTherapy in NSCLC
Pre-RFA 2 Weeks Post-RFA
6 Months Post-RFA/XRT
RFA = radiofrequency ablation; XRT = radiation therapy.

Copyright © Radiological Society of North America, 2005.
Wang H, et al. Radiology. 2005;235:289-298.
Before Cryotherapy After Cryotherapy
CT Images During Cryotherapy and at CT Images During Cryotherapy and at Follow-Up for Treatment of Small Follow-Up for Treatment of Small
Pulmonary MassPulmonary Mass
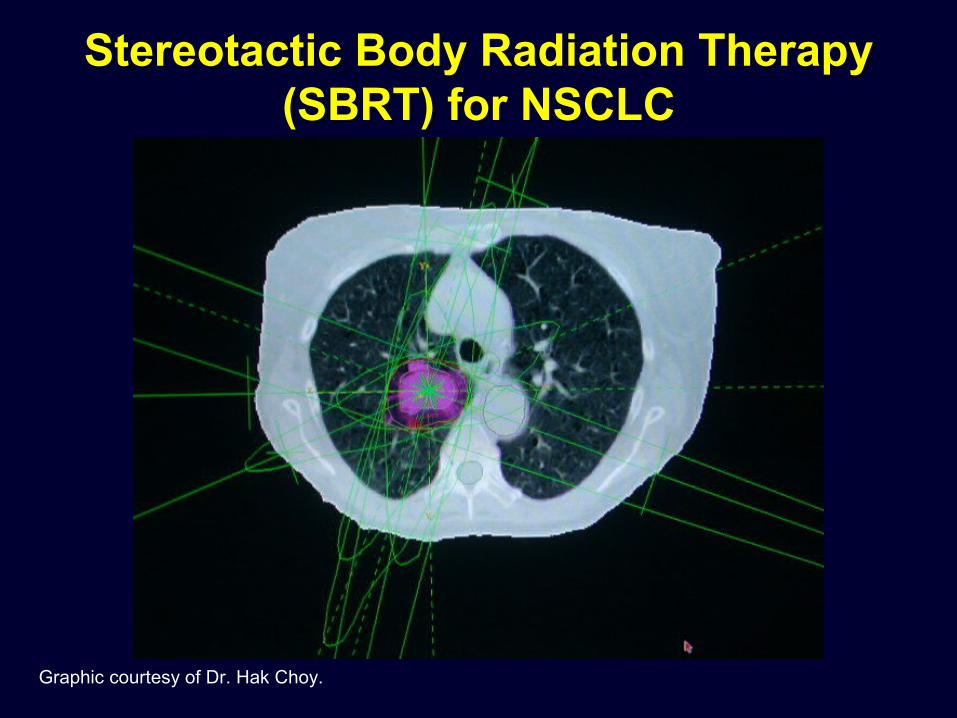
Stereotactic Body Radiation TherapyStereotactic Body Radiation Therapy(SBRT) for NSCLC(SBRT) for NSCLC
Graphic courtesy of Dr. Hak Choy.
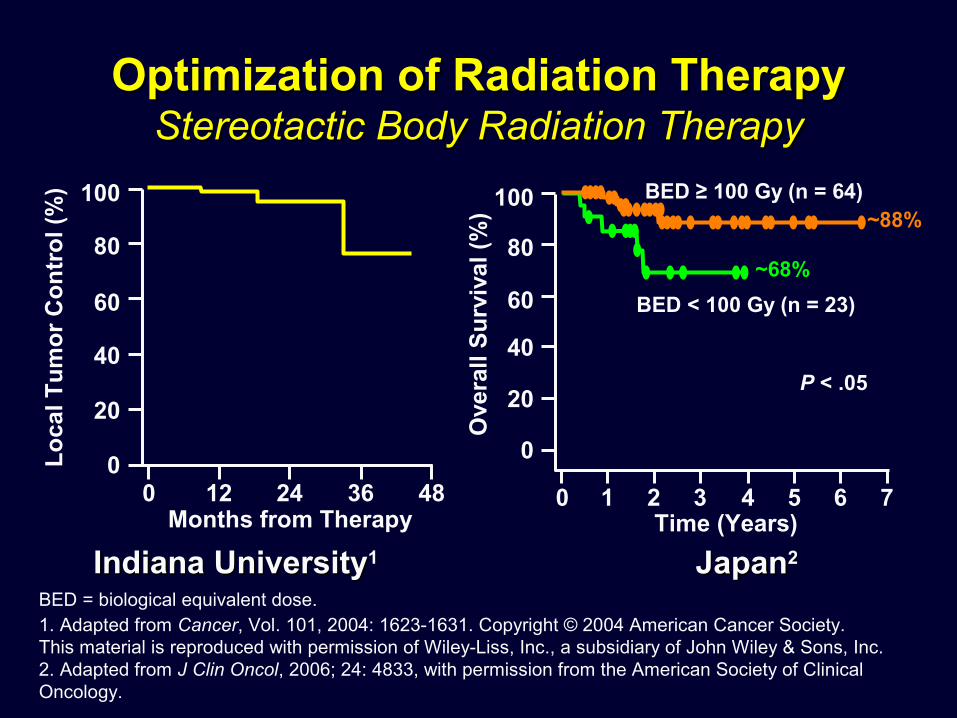
BED = biological equivalent dose.
Optimization of Radiation Therapy Optimization of Radiation Therapy Stereotactic Body Radiation TherapyStereotactic Body Radiation Therapy
Indiana UniversityIndiana University11 JapanJapan22
~88%
~68%
100
80
60
40
20
00 12 24 36 48
Lo
cal T
um
or
Co
ntr
ol (
%)
Months from Therapy
100
80
60
40
20
0
0 1 2 3 4 5 6 7Time (Years)
P < .05
Ove
rall
Su
rviv
al (
%)
BED < 100 Gy (n = 23)
BED ≥ 100 Gy (n = 64)
1. Adapted from Cancer, Vol. 101, 2004: 1623-1631. Copyright © 2004 American Cancer Society. This material is reproduced with permission of Wiley-Liss, Inc., a subsidiary of John Wiley & Sons, Inc. 2. Adapted from J Clin Oncol, 2006; 24: 4833, with permission from the American Society of Clinical Oncology.

Study DesignPCI
20–30 Gy in5–12 Fractions
No PCI
RandomAny response
Stratification: performance score and institute
<5 Weeks
4–6 Weeks
No ResponseChemotherapy
(4–6 Cycles)
Reprinted from Slotman BJ, et al. (ASCO 2007, #4; N Engl J Med. 357:664-672, 2007).
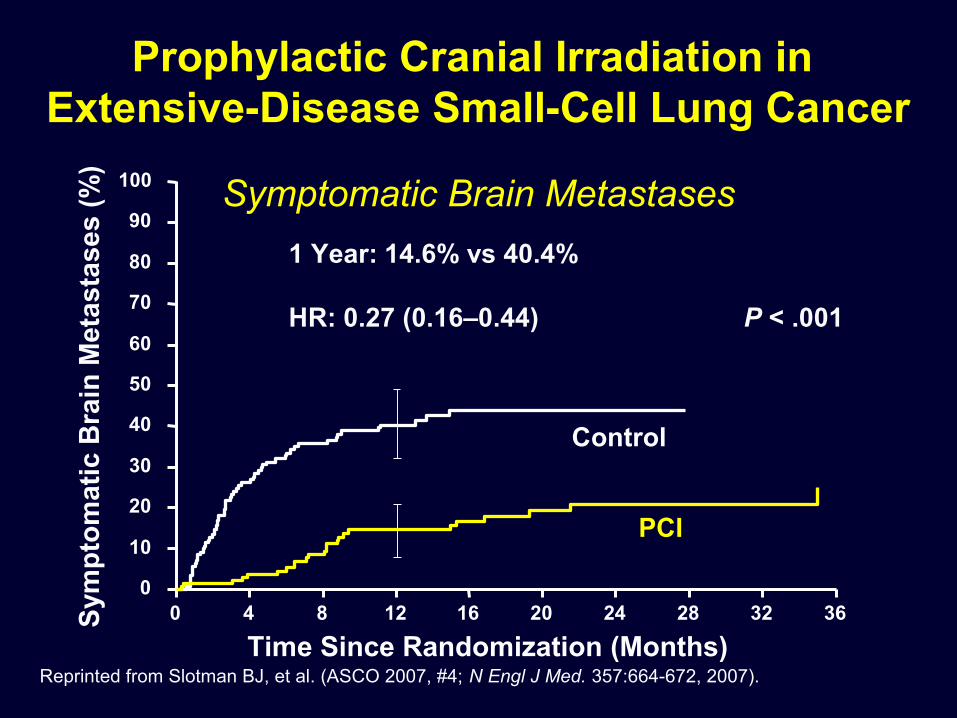
Prophylactic Cranial Irradiation in Prophylactic Cranial Irradiation in Extensive-Disease Small-Cell Lung CancerExtensive-Disease Small-Cell Lung Cancer
(EORTC 08993-22993)(EORTC 08993-22993)
0 4 8 12 16 20 24 28 32 360
10
20
30
40
50
60
70
80
90
100
PCI
Control
1 Year: 14.6% vs 40.4%
HR: 0.27 (0.16–0.44)
Sym
pto
mat
ic B
rain
Met
asta
ses
(%)
Prophylactic Cranial Irradiation in Extensive-Disease Small-Cell Lung Cancer
Symptomatic Brain Metastases
P < .001
Time Since Randomization (Months)Reprinted from Slotman BJ, et al. (ASCO 2007, #4; N Engl J Med. 357:664-672, 2007).
Time Since Randomization (Months)0 4 8 12 16 20 24 28 32 36
0
10
20
30
40
50
60
70
80
90
100
PCI
Control
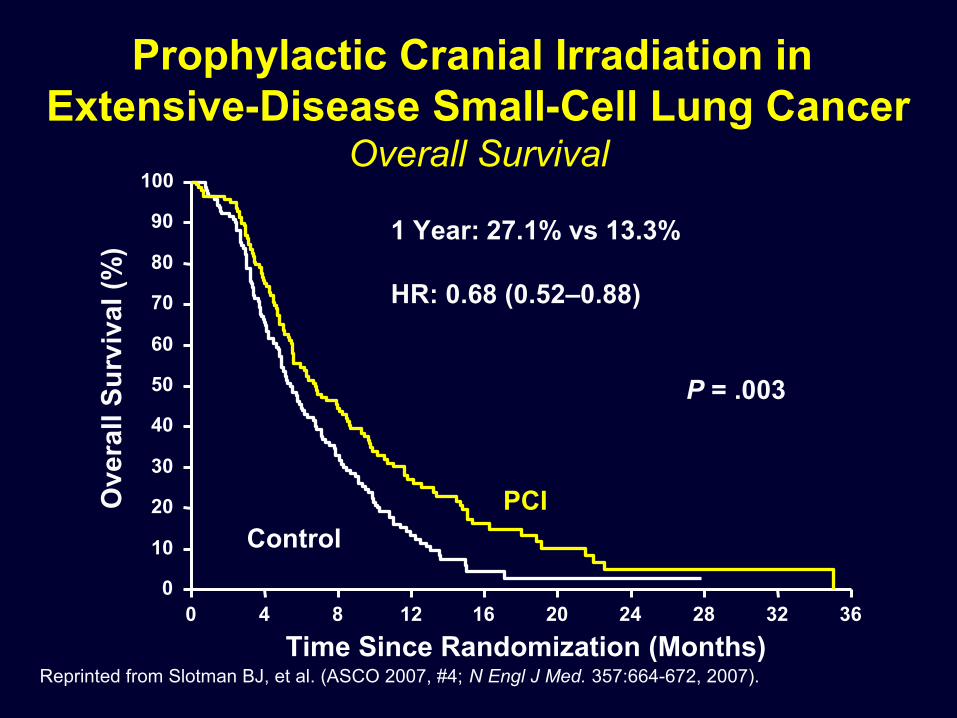
1 Year: 27.1% vs 13.3%
HR: 0.68 (0.52–0.88)
Ove
rall
Su
rviv
al (
%)
Prophylactic Cranial Irradiation in Extensive-Disease Small-Cell Lung Cancer
Overall Survival
P = .003
Reprinted from Slotman BJ, et al. (ASCO 2007, #4; N Engl J Med. 357:664-672, 2007).

STRATIFY
RANDOMIZE
RPA Class2
1 (<65 y and no extracranial cancer vs 2
(>65 y or extracranial metastases)
Number of Brain Metastases2
1 vs 2/3
Extent of Extracranial Disease2
Yes vs no
WBRT + SRS
WBRT + SRS + Temozolomide
WBRT + SRS + Erlotinib
Eligibility1
NSCLC 1–3 brain metastases
Max. lesion: 4 cm
No brainstem metastases
No actively progressing
extracranial cancerx 1 month
WBRT = whole brain radiation therapy; SRS = stereotactic radiosurgery; RPA = recursive partitioning analysis.
1. ClinicalTrials.gov Web site. http://www.clinicaltrials.gov/ct/show/NCT00096265?order=1. 2. Sperduto PW, et al. Slide 4. www.rtog.org/members/protocols/0320/0320Presentation.pdf.
Phase III Trial of WBRT and SRS Phase III Trial of WBRT and SRS with Temozolomide or Erlotinib with Temozolomide or Erlotinib
RTOG 0320RTOG 0320

On multivariate analysis, PET response was a more significant predictor (P = .006) than Karnofsky performance status (P = .09) and weight loss (P = .14).
N = 57
MacManus M, et al. 36th ASCO; May 20-23, 2000. Abstract 1888; Slide 22.
Response to Chemoradiotherapy on Response to Chemoradiotherapy on FDG-PET Correlates with SurvivalFDG-PET Correlates with Survival
100
80
60
40
20
00 3 9 15 48
Est
imat
ed S
urv
ival
(%
)
Months Following PET Scan
2118126
CRPRNR/PD
P = .0033
18%
53%
36%
84%84%

REGISTER
PPEET T
Concurrent chemotherapy/radiation therapy(+/- adjuvant chemotherapy per MD)
PET or PET-CT to be done 12–16 weeks following radiation therapy PET or PET-CT to be done 12–16 weeks following radiation therapy and at least 4 weeks after adjuvant chemotherapy (if given)and at least 4 weeks after adjuvant chemotherapy (if given)
N = 250
PPEET T
Machtay M, et al. 2004. ACR Web site. p 3. http://www.acrin.org/files/protocol_docs/A6668partial_summary.pdf.
Lung Cancer PET StudyLung Cancer PET Study ACRIN 6668/RTOG 0235 DesignACRIN 6668/RTOG 0235 Design
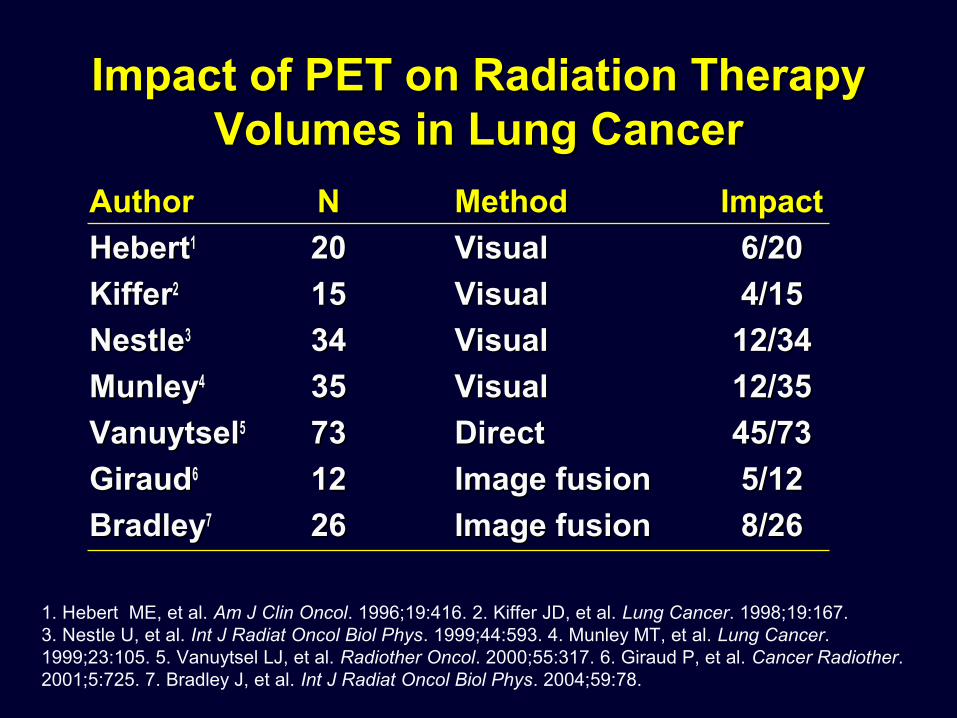
AuthorAuthor NN MethodMethod ImpactImpact
HebertHebert11 2020 VisualVisual 6/206/20
KifferKiffer22 1515 VisualVisual 4/154/15
NestleNestle33 3434 VisualVisual 12/3412/34
MunleyMunley44 3535 VisualVisual 12/3512/35
VanuytselVanuytsel55 7373 DirectDirect 45/7345/73
GiraudGiraud66 1212 Image fusionImage fusion 5/125/12
BradleyBradley77 2626 Image fusionImage fusion 8/268/26
1. Hebert ME, et al. Am J Clin Oncol. 1996;19:416. 2. Kiffer JD, et al. Lung Cancer. 1998;19:167. 3. Nestle U, et al. Int J Radiat Oncol Biol Phys. 1999;44:593. 4. Munley MT, et al. Lung Cancer. 1999;23:105. 5. Vanuytsel LJ, et al. Radiother Oncol. 2000;55:317. 6. Giraud P, et al. Cancer Radiother. 2001;5:725. 7. Bradley J, et al. Int J Radiat Oncol Biol Phys. 2004;59:78.
Impact of PET on Radiation Therapy Impact of PET on Radiation Therapy Volumes in Lung CancerVolumes in Lung Cancer