






Languages
Pages
Legal


DEFENCE HEALTH LEADERSHIP INSTITUTE (DHLI)
Panel Discussions
HMAS PENGUIN -
24 November 2010
Professor Jim Bishop AOChief Medical Officer
Australian Government Department of Health and Ageing

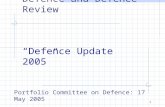
Health Expenditure per capita, public and private expenditure, OECD countries, 2008 ($US PPP)
7538
5004
4627
42104079 4063 3970
3793 3737 3696 36773540 3470
3359 33533129 3060 3008 2902 2870
2729 2687 2683
2151
1801 1781 1737
14371213
999852 767
0
1,000
2,000
3,000
4,000
5,000
6,000
7,000
8,000
1. Refers to insured population rather than resident population. 2. Current expenditure. 3. 2006. 4. 2007. Source: OECD, OECD Health Data, June 2010
Public expenditure on health Private expenditure on health
OECD HEALTH DATA 2010How Does AUSTRALIA Compare

AUSTRALIA’S RANKING AMONGOECD COUNTRIES 1987-2006
Source: AIHW Australia’s Health 2010

Projected Burden of Major Disease Groups, 2010
Source: AIHW Australia’s Health 2010

BROAD CAUSE MORTALITY TRENDS IN AUSTRALIA
Source: AIHW

CANCERS WITH REDUCING DEATH RATES 1997 to 2006 –
ALL AGES
Lung, -18.5Colon, -19.6 Prostate, -19.7
Leukaemia, -23.7
Stomach, -29.4
Head and Neck, -23.7
Bladder, -18.5
Testicular, -42.2
Breast, -13.8
Cervix, -38.3
NHL, -25.1
Unknown, -24.8
Rectum, -19.9
Bowel, -19.7
All cancers, -13.8
, -24.3
-18.5
Kidney, -24.1
, -15.2
-31.9
, -21.1
-19.0-19.0
, -18.9
-7.9
-45
-40
-35
-30
-25
-20
-15
-10
-5
0
Male FemaleSource: Tracey et al, Cancer Institute NSW

Source: AIHW Australia’s Health 2010
AGED ADJUSTED DEATH RATESFrom CVD, 1907 -
2006

Source: AIHW Australia’s Health 2010
CHRONIC PULMONARY DISEASEMORTALITY 1980 to 2007

Source: AIHW Australia’s Health 2010
PREVALENCE OF CURRENT ASTHMA 2007-08

Source: AIHW Australia’s Health 2010
DEATH RATES FROMINFECTIOUS DISEASES, 1922-2007

NSW POPULATION AGE
DISTRIBUTIONS, MALE (1977 –
2036)
Source: Cancer Institute NSW

TOTAL CANCER CASES & DEATHS per year (1972 to 2036)
Source: Cancer Institute NSW

TRENDS IN LEADING CAUSESOF DISEASE BURDEN 2003-2023
Source: AIHW Australia’s Health 2010

Commonwealth Government Health& Hospital expenditure under the NHHN
Source: Commonwealth Budget Papers, DOHA and PMC Analysis

HEALTH REFORM
Increasing expenditure to $15 billion 2010/11
Additional $7.3 billion over 4 years
Local Hospital Networks (LHN) 60% Federal Funds (60% of research and teaching)
Medicare locals (100% Federal funds)
GP Super-clinics –
multi disciplinary teams (100% Federal Funds)

MEDICARE LOCALS
Identification and response to local health needs
Integrated and coordinated care for the patient
Support clinicians to improve care
Implement new primary care initiatives
Accountable for efficiency and quality
OBJECTIVES

BUDGET 2010-11
e-Health –
connecting patients, providers and information systems
The Government will establish a personally controlled electronic
health record system ($466.7m)
The system will:
Enable people –
and their chosen health provider -
to
access online their key health information when and where it is needed, for their care across the health system.
Allow people to register online to establish a personally controlled electronic health record from 2012-13
Rigorous governance
Privacy maintained

HEALTH REFORM
KEY NEW STRUCTURES
National Performance Authority
Independent Hospital Pricing Authority
Expanded Australian Commission of Safety and Quality in Health Care (ACSQHC)

SUPPORTS FOR CLINICAL DECISION MAKING
Evidence Base
Highest Impact
Range of best practice tools
Successful implementation methods
Monitor and report
CLINICAL GUIDELINES

CLINICAL GUIDELINESHighest Impact
Greatest Burden of disease
Greatest harm from poor practice
Greatest demonstrated need:-
New Standard of Care
-
Proven variation in practice
Greatest time spent/cost to health system

HEALTH WORKFORCE
Established Health Workforce Australia
$1.2 billion in training more GPs and specialists, nurses and allied health
1375 more GPs by 2013, 5500 by 2020
680 more specialists by 2020
4600 practice nurses by 2013, 7500 rural nurses by 2020

Increasing burden of chronic diseases especially cancer, dementia and diabetes
New reform structures offer opportunities to set new clinical guidelines and standards
Opportunities for more coordinated care through medicare
locals, local hospital networks and lead
clinician groups
Increased health workforce provides opportunities for greater depth in general practice and in specialist training
Increased need for greater evidence base as a framework for improved guidelines and decision tools
CONCLUSIONS
Top Related