





Languages
Pages
Legal


Editors: Gabrielli, Andrea; Layon, A. Joseph; Yu, Mihae
Title: Civetta, Taylor, & Kirby's: Critical Care, 4th Edition
Copyright ©2009 Lippincott Williams & Wilkins
> Table of Contents > Section VI - Shock States > Chapter 58 - Hemorrhagic Shock
Chapter 58
Hemorrhagic Shock
Marianne E. Cinat
David B. Hoyt
The definition of shock describes the final common pathway of many disease states:
ineffective tissue perfusion, resulting in severe dysfunction of organs vital to survival. The
most commonly used classification system for shock includes four categories based on
hemodynamic characteristics (1):
1. Hypovolemic shock resulting from a decreased circulating blood volume in relation to the
total vascular capacity and characterized by a reduction of diastolic filling pressures and
volumes
2. Cardiogenic shock related to cardiac pump failure caused by loss of myocardial
contractility/functional myocardium or structural/mechanical failure of the cardiac
anatomy characterized by elevations of diastolic filling pressures and volumes
3. Extracardiac obstructive shock involving obstruction to flow in the cardiovascular circuit
and characterized by either impairment of diastolic filling or excessive afterload
4. Distributive shock caused by loss of vasomotor control, resulting in arteriolar and
venular dilation and characterized by increased cardiac output and decreased systemic
vascular resistance after fluid resuscitation.
Although the hemodynamic characteristics of the various forms of shock may vary, the final
common pathway—inadequate cellular perfusion—must be addressed early to prevent long-
term sequelae and death (Fig. 58.1).
Hemorrhagic shock is a form of hypovolemic shock. It is a common, yet complicated,
clinical condition that physicians are frequently called upon to evaluate and treat.
Etiologies include trauma, postoperative bleeding, medical conditions, and iatrogenic
causes. Diagnosis must be accurate and expedient. Therapy must be direct, efficient, and
multifactorial in order to avoid the potential multisystem sequelae.
The purpose of this chapter is to address the immediate concerns for patients with
hemorrhagic shock, as well as the etiology and epidemiology of this clinical condition, and
Page 1 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

to describe the pathophysiology, clinical features, and diagnostic and therapeutic approach
to hemorrhagic shock. New and experimental therapies will also be introduced.
Immediate Concerns The key steps in the approach to patients with hemorrhagic shock are listed in Table 58.1.
1. Early recognition. Early recognition requires astute clinical acumen to identify early
systemic signs of hemorrhage and hypovolemic shock. Signs and symptoms include
restlessness, anxiety, altered level of consciousness, shortness of breath, tachypnea,
pallor, tachycardia, and oliguria. A decreased pulse pressure may also be observed along
with decreased capillary refill due to peripheral vasoconstriction. Hypotension indicates
significant volume depletion and may be a late clinical manifestation.
2. Important aspects in the patient history. An accurate history should be obtained
expediently. For patients with traumatic injury, a thorough understanding of the
mechanism of injury should be obtained, including the magnitude of blunt force trauma
and/or the trajectory of the missile or object in penetrating trauma. In postoperative or
postprocedural patients, the exact nature of the surgical procedure should be defined
and potential sites of hemorrhage identified. In patients without recent surgery, risk
factors for nonpostoperative, nontraumatic etiologies should also be sought (gastritis,
peptic ulcer disease, atherosclerosis with aneurysmal disease). Significant comorbidities
should also be delineated including coagulation disorders (von Willebrand, hemophilia),
medical conditions associated with altered coagulation (cirrhosis, renal failure,
iatrogenic vitamin K deficiency from parenteral nutrition or antimicrobials), or use of
medications such as antiplatelet therapy and anticoagulants (Coumadin, heparin, low-
molecular-weight heparin, or antimicrobials).
3. Initial action and intervention. The initial action taken in each case of hemorrhagic
shock, regardless of etiology, should be directed at restoring circulating volume to
ensure adequate tissue perfusion. Once the airway is secured and adequate ventilation is
ensured, two peripheral large-bore intravenous catheters should be placed and fluid
resuscitation begun. A blood sample should also be sent immediately for type and cross-
match per institutional protocol. Initial resuscitation can include crystalloid, but should
quickly be changed to blood products if signs of hypovolemia and ongoing hemorrhage
persist. If a patient is in extremis and cross-matched blood products are not immediately
available, type O blood (universal donor) should be immediately requested and
transfused. For massive hemorrhage, clotting factors such as fresh frozen plasma,
platelets, and cryoprecipitate should be prepared. The value of massive transfusion
protocols to include predetermined ratios of clotting factors will be discussed later in
this chapter.
4. Directed physical examination. Physical examination should be directed at obvious
sources of external bleeding such as lacerations, extremity fractures, or surgical
Page 2 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

incisions. If identified, these should be immediately controlled. Physical signs of
underlying liver disease should also be identified such as petechia, jaundice, ascites,
angiomas, or testicular atrophy. Previous cardiac or carotid surgical incisions may hint
toward concurrent antiplatelet or anticoagulant therapy. Evidence of retroperitoneal
bleeding in patients with pancreatitis is marked by flank or periumbilical contusions.
5. Identify occult source of hemorrhage. If no obvious source of external bleeding is
identified, a rapid evaluation should be performed to identify likely occult sources of
bleeding. In the trauma patient, significant internal hemorrhage can occur in four
defined regions: the thoracic cavity, the peritoneal cavity, the retroperitoneum, and
extremity fractures. These areas can be rapidly assessed by chest radiograph, pelvic
radiograph, a focused abdominal sonographic examination for trauma (FAST), and
physical examination of extremities along with appropriate radiographs. In nontrauma
patients without clear evidence of bleeding, the gastrointestinal tract should be rapidly
evaluated via nasogastric tube, rectal examination, and endoscopy where appropriate.
Additional diagnostic tests can be obtained based on clinical history, patient
background, and condition. Abdominal aortic aneurysms can be identified on physical
examination, by ultrasound, or by calcifications on abdominal radiograph. In rare
selected instances, angiography may be used to identify and treat sources of hemorrhage
not otherwise apparent (pelvic fractures, pancreatitis, lower gastrointestinal bleeding).
This should only be instituted when a specific source of hemorrhage is highly likely and
therapeutic intervention is sought. Computed tomography should never be sought in
hemodynamically unstable patients with hemorrhage.
P.894
Page 3 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

6. Expedite treatment. Once a source of bleeding is identified, a swift and directed
treatment plan should be formulated and implemented without delay. Prolonged
untreated hemorrhagic shock can lead to rapid decompensation and death if not
appropriately identified and treated. Rapid intervention with surgical, angiographic, or
endoscopic control of the hemorrhage is indicated, along with rapid correction of the
underlying coagulopathy.
Epidemiology and Etiology Hypovolemic shock can be due to hemorrhagic and nonhemorrhagic sources. Hemorrhage is
the most frequent cause of hypovolemic shock and is most commonly due to blood loss after
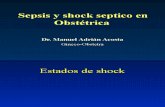
Figure 58.1. Final common pathway of shock. Hemorrhagic shock results in acute
changes in circulating blood volume that culminates in a final common pathway
shared by all classifications of shock.
Page 4 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

trauma or major surgery (Table 58.2). Following trauma, obvious external signs of injury
and hemorrhage should be rapidly identified and controlled. As described above, the
thoracic cavity, peritoneal cavity, and retroperitoneum should all be evaluated for occult
hemorrhage.
Table 58.1 Key steps in the approach to a patient with hemorrhagic shock
1. Early recognition
a. Signs and symptoms may be subtle.
b. Astute clinical acumen is necessary to identify hemorrhage prior to
hemodynamic collapse.
2. Obtain an accurate patient history
a. Trauma
b. Recent surgical procedures
c. Medical history
i. Gastrointestinal disease (peptic ulcer disease, varices, etc.)
ii. Atherosclerosis (aneurysmal disease)
iii. Coagulation disorders
d. Medication use
i. Antiplatelet therapy
ii. Anticoagulants
3. Initiate intervention
a. “ABCs”—airway, breathing, circulation
b. Initiate resuscitation
i. Crystalloid
ii. Blood products
1. Type O uncross-matched blood if in extremis
2. Cross-matched blood when available
3. Clotting factors
4. Directed physical examination
a. External sources of bleeding
b. Internal sources of bleeding
5. Expedite definitive treatment
a. Surgical control
b. Endoscopic control
c. Angiographic control
Page 5 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

6. Correct coagulopathy
Table 58.2 Major etiologies of hemorrhagic shock
I. Trauma (blunt or penetrating)
Intrathoracic
Intraperitoneal
Retroperitoneal
Soft tissue or fractures
II. Gastrointestinal
Upper gastrointestinal tract
Peptic ulcer disease, reflux esophagitis, variceal bleeding, erosive
gastritis, aortoduodenal fistula
Lower gastrointestinal tract
Hemorrhoids, tumor, arteriovenous malformation, diverticulitis,
ulcerative colitis, Crohn disease, ischemia
Hemobilia
Biliary tumor, iatrogenic injury or manipulation, penetrating trauma
Pancreatic
Pancreatitis, iatrogenic injury or manipulation
III. Retroperitoneal (nontrauma)
Abdominal aortic aneurysm
Page 6 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

Causes of hemorrhagic shock not due to trauma include a ruptured abdominal aortic
aneurysm and gastrointestinal bleeding. Gastrointestinal bleeding can be caused by peptic
ulcer disease, reflux esophagitis, variceal bleeding, erosive gastritis (stress ulcers), or an
aortoduodenal fistula after vascular surgery. Prior manipulation by endoscopy or
sphincterotomy can also lead to upper gastrointestinal bleeding. Lower gastrointestinal
bleeding can result from diverticular disease, carcinoma, polyps, arteriovenous
malformations, ischemia, or colitis. Pulmonary sources of hemorrhage can occur from
tumor, tuberculosis, fungal infection, bronchiectasis, or tracheoinnominate fistula following
tracheostomy. Hematuria from a tumor, trauma, or polycystic kidney disease is rare but can
lead to hemorrhagic shock.
Nonhemorrhagic sources of hypovolemic shock can also occur. Although not the focus of this
chapter, these are due to external fluid losses such as dehydration, vomiting, diarrhea,
polyuria, uncontrolled diabetes mellitus leading to osmotic diuresis, and acute
adrenocortical insufficiency. Disorders that lead to interstitial fluid redistribution such as
thermal injury, trauma, and anaphylaxis can also lead to hypovolemic shock. Finally,
disorders that cause increased vascular capacitance (venodilation) can lead to a relative
hypovolemia and include sepsis, anaphylaxis, and the release of toxins/drugs leading to
vasodilation.
Classification of Hemorrhagic Shock Early diagnosis of hemorrhagic shock is imperative to avoid delay in treatment. However,
clinical signs are relatively insensitive for small amounts of blood loss (2). There is a
progressive hemodynamic deterioration with ongoing blood loss. This classic progression is
delineated in Table 58.3. Total blood volume is estimated at approximately 70 mL/kg in the
average adult, or nearly 5 L for a 70-kg person.
Class I Class I hemorrhage is marked by a less than 750 mL estimated blood loss, or less than 15% of
total circulating blood volume. There are minimal physical signs associated with this volume
of blood loss. The patient may not have tachycardia, with a heart rate remaining less than
100 beats per minute; the systolic blood pressure and pulse pressure remain normal; the
respiratory rate remains at 14 to 20 breaths per minute; and urine output remains adequate
(>30 mL/hour). Only subtle physical signs such as delayed capillary refill and slight anxiety
may exist.
Class II Class II hemorrhage is marked by an estimated blood loss of 750 to 1,500 mL (or 15% to 30%
of the total circulating blood volume). Physical signs begin to manifest during this stage of
hemorrhage. Although the systolic blood pressure may be maintained, the patient usually
becomes tachycardic (heart rate greater than 100 beats per minute), the pulse pressure
P.895
Page 7 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

begins to decrease, and capillary refill is delayed. The respiratory rate begins to increase
(20–30 breaths per minute), urine output becomes diminished (20–30 mL/hour), and the patient becomes very anxious. P.896
Table 58.3 Clinical classes of hemorrhagic shock
Class I Class II Class III Class IV
Blood loss <750 mL 750–1,500
mL
>1,500–
2,000 mL
>2,000 mL
<15% 15%–30% >30%–40% >40%
Heart rate
(beats per
minute)
<100 >100 >120 >140
Systolic blood
pressure
Normal Normal Decreased Decreased
Pulse pressure Normal Decreased Decreased Decreased
Capillary refill Delayed Delayed Delayed Delayed
Respiratory rate
(breaths per
minute)
14–20 20–30 30–40 >35
Urine output
(mL/h)
>30 20–30 5–15 Minimal
Mental status Slightly
anxious
Anxious Confused Confused
and
lethargic
Page 8 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

Class III Class III hemorrhage is marked by an estimated blood loss of >1,500 to 2,000 mL (or >30%–
40% of total circulating blood volume). During this phase, significant hemodynamic
compromise becomes apparent. Heart rate increases to >120 beats per minute, systolic
blood pressure decreases, pulse pressure decreases, capillary refill decreases, tachypnea
worsens with a respiratory rate of 30 to 40 breaths per minute, urine output drops to 5 to
15 mL/hour, and the patient becomes confused, showing further evidence of decreased
perfusion of the central nervous system.
Class IV Class IV hemorrhage is marked by an estimated blood loss of >2,000 mL (or >40% of total
circulating blood volume). During this phase, most compensatory cardiovascular mechanisms
have been maximized and total hemodynamic collapse is imminent. Signs of class IV
hemorrhage include severe tachycardia with a heart rate >140 beats per minute, a
decreased systolic blood pressure, a decreased pulse pressure, delayed capillary refill,
significant tachypnea with a respiratory rate of >35 breaths per minute, minimal to no urine
output, and severely altered mental status as marked by confusion and/or lethargy.
Potential Pitfalls Despite these guidelines, several potential pitfalls exist that can make the diagnosis more
difficult. Concurrent medication, such as β-blockers, may attenuate the physiologic
response to hemorrhage. In the presence of β-blockade, tachycardia may be blunted or may
not occur at all. Prior hydration status and use of diuretics can also alter the rate at which
these signs present. Pregnant patients have a significantly increased total blood volume,
and thus can lose up to 1,000 mL of blood before presenting with any clinical signs of
hemorrhage. Blood is diverted from the placenta via vasoconstriction; the mother's total
blood circulation is maintained at the expense of the fetus. Elderly patients may have atrial
arrhythmias leading to a high ventricular response, making tachycardia less sensitive in this
patient population. Concurrent use of antiplatelet or anticoagulant medication can cause
relatively small injuries to bleed excessively, and identification and intervention may be
delayed. Although unloading of the baroreceptors and activation of the sympathetic nervous
system usually lead to tachycardia, some patients may respond to traumatic hemorrhage
with bradycardia as a result of a vagal nerve–mediated transient sympathoinhibition due to
acute and sudden blood loss (3,4,5,6,7,8,9). Finally, a significant reduction in skin blood
flow (i.e., cool, clammy skin) is an early ominous sign of shock in view of selective
cutaneous vasoconstriction (10). Intervention and resuscitation must be imminent upon
presentation of these signs and symptoms.
Pathophysiology
Page 9 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

Circulatory Changes Hemorrhage results in a predictable pattern of events that begins with acute changes in
circulating blood volume and culminates in a final common pathway shared by all
classifications of shock (Fig. 58.1). Hemodynamically, hypovolemic shock is characterized by
a fall in ventricular preload, resulting in decreased ventricular diastolic filling pressures and
volumes. This in turn leads to a decrease in cardiac output and stroke volume
(3,4,5,11,12,13,14,15). Following unloading of the cardiac baroreceptors and activation of
the sympathetic nervous system, tachycardia ensues in an attempt to compensate for the
decrease in cardiac output and stroke volume (12). The sympathetic output also results in
vasoconstriction, leading to a decrease in pulse pressure. Greater variations in blood
pressure will occur with the respiratory cycle due to an increased sensitivity of the
underfilled heart to changes in venous return with varying intrathoracic pressure (16,17,18).
The increased sympathetic tone may prevent a severe drop in arterial blood pressure
initially. However, continued blood loss will ultimately result in hypotension and shock (3).
Due to compensatory vasoconstriction, systemic vascular resistance rises early after the
development of hypovolemic shock, but may fall in later stages, potentially heralding
irreversibility and death (3,19,20).
The response to blood loss is a dynamic process that involves competing adaptive
(compensatory) and maladaptive responses at each stage of development. Although intravascular volume replacement is
always a necessary component of resuscitation in hypovolemic shock, the complex biologic
response to the insult may progress to a point at which such resuscitation is insufficient to
reverse the progression of the shock syndrome. For instance, patients who have sustained
greater than a 40% loss of blood volume for 2 hours or more may not be able to be
effectively resuscitated. Severe hemorrhage leads to a series of inflammatory mediator,
cardiovascular, and organ responses that supersede the injury itself and ultimately drive
recovery or death (3,19,20,21,22,23,24,25).
Oxygen Balance Shock is characterized by an oxygen deficit in tissues and cells. The significance of the
deficit and the extent of cellular injury can be quantified as a function of both the severity
and the duration of the deficit—the greater the severity, the longer the duration, the worse
the outcome of shock.
Oxygen delivery to tissues is determined by cardiac output and the oxygen content in
arterial blood. Oxygen content refers to the number of milliliters of oxygen contained in 100
mL of blood (mL/dL) and is a function of the hemoglobin concentration, the oxygen
saturation of hemoglobin, and the amount of oxygen dissolved in plasma (the calculation is [Hgb × 1.34 × O2 saturation] + [PaO2 × 0.0003]). During hemorrhage, as the cardiac output
falls, oxygen delivery to the tissues also falls. Initially, the body will maintain sufficient
uptake of oxygen by extracting more from the arterial blood. This will result in a fall in the
P.897
Page 10 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

mixed venous oxygen saturation (SvO2) with an increase in the arteriovenous oxygen content
gradient (CaO2 – CvO2). Eventually, this compensatory mechanism also fails, and tissue
hypoxia with lactic acidosis ensues. Cerebral and cardiac functions are maintained by
diversion of blood flow from other organs (skin, muscle, and kidneys) (26). However, when
these compensatory mechanisms are maximized, cardiac function and tissue oxygen
delivery deteriorates further, and irreversible shock may develop (27).
Critical oxygen delivery is a function of cellular needs for oxygen and the ability of cells to
extract oxygen from the arterial blood. Many factors contribute to this equation. During
hemorrhage, tissue oxygen needs may increase due to increased respiratory muscle activity
and increased catecholamine circulation (28). However, some evidence suggests that
catecholamines down-regulate the metabolic needs of cells during hypovolemic shock
(4,5,28,29,30). Regional blood flow is modified during hypovolemic shock in an attempt to
maintain oxygen delivery to critical tissues (26,31). In addition, the individual needs of
various tissues may vary during hemorrhagic shock. For instance, the oxygen needs of the
kidney may decline during hemorrhage because a fall in renal perfusion leads to a fall in
glomerular filtration and a decrease in energy-consuming tubular absorption (26). In
contrast, the gut may experience an increased oxygen debt early due to the high oxygen
need of the mucosa, along with redistribution of blood away from the gut to more critical
tissues. This is the physiologic basis for gastric tonometry as a means of measuring the
adequacy of resuscitation early following hemorrhage (32,33).
Oxygen extraction in tissues is influenced by the position of the oxyhemoglobin dissociation
curve (34,35,36,37). Factors that improve the ability of tissues to extract oxygen from
hemoglobin (i.e., shift the curve to the right) include acidosis, hypercarbia, hyperthermia,
and decreased blood viscosity. However, in any extreme, each of these factors can be
overcome by inadequate oxygen delivery and cardiovascular collapse. Interestingly, the
oxyhemoglobin curve has been shown to shift to the left in critically ill patients (38). The
presence of 2,3-diphosphoglycerate (DPG) in transfused blood has also been associated with
a left shift of the oxyhemoglobin dissociation curve (39). Thus, although transfusions may
increase the hemoglobin level, theoretically improving oxygen delivery, they may negatively
affect the ability of tissues to extract oxygen from the hemoglobin.
The severity of oxygen debt during hypovolemic shock has been shown to be a major
determinant of survival in animals and in patients following trauma, hemorrhage, and major
surgery (20,27,40,41). A large oxygen debt has been associated with the development of
acute respiratory distress syndrome (ARDS) and multiple organ dysfunction syndrome (MODS)
(33,40,41,42,43,44). Conversely, a high oxygen delivery and uptake during resuscitation has
been associated with improved survival (27,41,42,43,44,45,46). Whether increasing oxygen
delivery to supranormal levels ultimately improves survival during resuscitation in critical
illness remains controversial, and the medical literature has produced mixed results
(27,33,43,44,47,48,49,50).
Page 11 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

Cellular Response During hypovolemic shock, the oxygen deficit in the tissues causes a fall in the
mitochondrial production and concentration of high-energy phosphates because of greater
breakdown than production (51,52,53,54,55,56,57). This led many researchers to evaluate
the utility of adenosine triphosphate (ATP) in the resuscitation of hemorrhagic shock
(58,59). In the presence of sufficient oxygen, aerobic combustion of 1 mol of glucose yields
38 mol of energy-rich ATP. However, in the absence of sufficient oxygen, glucose taken up
by the cells cannot be combusted because of insufficient uptake of pyruvate into the
mitochondrial tricarboxylic acid cycle. Pyruvate is then converted to lactate within the
cytoplasm. Anaerobic glycolysis yields only 2 mol of ATP, which is then hydrolyzed into
hydrogen ion, ultimately leading to intracellular and extracellular metabolic acidosis
(51,52,60,61,62) (Fig. 58.2). This process is ultimately a function of the severity and
duration of regional hypoperfusion relative to oxygen demand and is more pronounced in
some tissues (diaphragm, liver, kidney, gut) than in others (heart, skeletal muscle).
Ultimately, a significant fall in the high-energy phosphates for a prolonged duration will
lead to irreversible cellular injury and death.
The sequelae of low ATP production are profound. About 60% of the energy produced by
respiring cellular mitochondria is needed to fuel the sodium-potassium (Na+-K+) pump of the
cell. This pump controls the gradient in electrolyte concentrations and electric potential
over the cell membrane. In the absence of sufficient ATP, the Na+-K+ pump is inhibited,
resulting in an influx of sodium into the cell and efflux of potassium out of the cell. This in
turn leads to cellular fluid uptake (51,53,63,64,65,66). Hyperkalemia may result due to
potassium exchange between cells, the interstitial fluid, and vascular space.
Independent of the Na+-K+ pump, there may be a selective increase in cell membrane
permeability for ions during hemorrhagic shock. Hypovolemic shock has been shown to lead
to a rapid decrease in the transmembrane potential (with a less negative inner membrane
potential), resulting in rapid electrolyte and fluid shifts across the membrane. Circulating
heat shock proteins may also contribute to these changes independent of energy deficit
(66,67,68,69,70,71).
P.898
Page 12 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

Finally, calcium (Ca2+) influx into cells and their mitochondria inhibits cellular respiration
and ultimately contributes to cellular damage and swelling. Plasma levels of free Ca2+ may
also fall. This may have profound consequences on the function of several organs during
shock including the liver, kidney, heart, and vascular smooth muscle
(64,65,72,73,74,75,76,77,78,79,80,81,82). Intracellular lysosomes lose their integrity, and
proteolytic enzymes are released and contribute to cellular dysfunction and cell death.
The sum of the intracellular changes and alterations in signaling transduction pathways
described above ultimately leads to the development of cellular dysfunction and multiple
organ dysfunction syndrome, which may be irreversible (82). Laboratory investigations are
aimed at novel resuscitation techniques involving substances that attenuate abnormalities
of cellular signaling following hemorrhagic shock (58,59,77,78,79,80,81,82).
Neurohumoral Response In response to hemorrhage and hypovolemia, a complex neurohumoral response is initiated
in an attempt to maintain blood pressure and retain fluid. Decreased intravascular volume
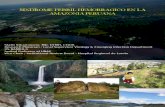
Figure 58.2. Cellular mechanisms during anaerobic and aerobic glycolysis. In
anaerobic conditions, pyruvic acid cannot enter the citric acid cycle within the
mitochondria and is instead shunted to the production of lactate. This process
produces only two molecules of adenosine triphosphate (ATP), as opposed to the 36
molecules of ATP produced from glucose in the mitochondria during aerobic glycolysis.
Hydrolysis of ATP molecules in anaerobic conditions results in the production of
hydrogen ions that cannot be cleared, leading to intracellular acidosis. (Adapted from
Mizock BA, Falk JL. Lactic acidosis in critical illness. Crit Care Med. 1992;20[1]:80.)
Page 13 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

stimulates baroreceptors in the carotid body and aortic arch, along with mechanoreceptors
in the right atrium. This stimulation leads to several neurohumoral responses (Fig. 58.3).
Circulating catecholamines are liberated by activation of the sympathetic nervous system
and the adrenal medulla. Direct sympathetic stimulation of the vessel wall leads to
vasoconstriction. Angiotensin II is liberated via the renin–angiotensin–aldosterone system.
Vasopressin (antidiuretic hormone [ADH]) is released by the pituitary in hypovolemic shock
and leads to vasoconstriction. Finally, decreased cardiac filling pressures reduce cardiac
secretion of α-atrial natriuretic peptide (ANP), thereby reducing the vasodilatory and
diuretic effects of ANP.
Macrocirculation During loss of circulating blood volume, mechanisms are initiated to counteract the fall in
cardiac output and oxygen delivery by facilitating a redistribution of peripheral blood flow
(26). Regional autoregulation takes place via a delicate balance of endogenous vasodilators
and vasoconstrictors. Endothelial cells produce potent vasodilators such as endothelium-
derived relaxing factor (nitric oxide [NO]), heme oxygenation–derived carbon monoxide (CO), and metabolic byproducts in tissues, including carbon dioxide (CO2), potassium, and
adenosine (25,83,84,85,86,87,88,89). Some authors describe that inhibition of NO early
following hemorrhage ameliorates early hypotension and improves mortality
(90,91,92,93,94). Conversely, other authors describe endothelial dysfunction in organs with
diminished NO production (95,96). Endothelin is a potent endothelial cell–derived
vasoconstrictor that is released upon catecholamine stimulation or hypoxia (97). The overall
increase in systemic peripheral vascular resistance is distributed differently among various
organs in the body (31). Vasoconstriction also occurs in the venous vasculature, increasing
return of available blood to the heart (14,98). The complex interplay of these mechanisms
for vasodilation and vasoconstriction ultimately determines the regional redistribution of
blood flow to organs following hemorrhagic shock. The redistribution of blood flow results in
a greater share of oxygen delivery to organs with high obligatory metabolic demands (heart
and brain), and a lesser share to those with fewer demands including the skin, skeletal
muscle, kidney, intestine, and pancreas (5,31,86,99,100,101).
Microcirculation One of the most important determinants of tissue perfusion during shock is the response and
function of the microvasculature, which is defined as vessels less than 100 to 150 µm in
diameter. Although arteries and medium-sized arterioles constrict in response to the
extrinsic control mechanisms described above, terminal arterioles, venules, and capillaries
remain unaffected and are more controlled by local metabolic factors.
Page 14 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

Alterations in microvascular function and flow are effected through precapillary and
postcapillary sphincters, which are sensitive to both extrinsic and intrinsic control
mechanisms. Exchange of metabolites and compartmental regulation of fluids occurs at the
capillary level. Therefore, alteration of tone of the pre- and postcapillary sphincters can
have significant effects on microcirculatory function (102,103,104). Failure to dilate
sphincters supplying metabolically active tissues may result in ischemia and anaerobic
metabolism with lactate production. Increased precapillary tone, as seen with sympathetic
stimulation, results in increased blood pressure systemically and decreased hydrostatic
pressure locally. In fact, the microvascular arterioles may even dilate in response to the
Figure 58.3. Neurohormonal response to hemorrhage. Hemorrhage results in a
decrease in the circulating intravascular volume, which initiates a complex cascade of
compensatory events. CNS, central nervous system; ACTH, adrenocorticotropic
hormone; ADH, antidiuretic hormone.
P.899
Page 15 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

above vasoconstriction due to release of metabolic byproducts of underperfusion (carbon
dioxide, hydrogen ion, etc.). The decrease in hydrostatic pressure locally then leads to
redistribution of fluid from the interstitium to the circulation. Conversely, increased
postcapillary tone (relative to precapillary tone) results in vascular pooling of blood and loss
of fluid to the interstitium (as a result of increased hydrostatic pressure). This increased
hydrostatic pressure may become accentuated in response to crystalloid resuscitation,
leading to interstitial edema (104). Finally, hemorrhage and shock have also been shown to
induce increased permeability of capillaries, leading to interstitial fluid leak during
resuscitation (105,106).
Hypovolemic shock and hemorrhage also induce the expression of endothelial adhesion
molecules on neutrophils and endothelium (63,107). This results in neutrophil adherence
and “rolling” of cells within the capillary bed (108,109,110,111,112,113). Capillary flow
then diminishes and may also impair red blood cell flow. While this decrease in transit time
may augment the ability of tissue to extract oxygen, it may also lead to microvascular
thrombosis and further tissue ischemia (114,115).
Metabolic and Hormonal Response The early hyperglycemic response to trauma/hemorrhage is the combined result of
enhanced glycogenolysis, caused by the hormonal response to stress including elevated
epinephrine, cortisol, and glucagon levels; increased gluconeogenesis in the liver, partly
mediated by glucagon; and peripheral resistance to the action of insulin (51,116). Increased
gluconeogenesis in the liver, and to a lesser extent in the kidneys, follows increased efflux
of amino acids, such as alanine and glutamine from the muscle to the liver, due to a
breakdown of muscle protein. The latter is evidenced by increased urinary losses of nitrogen and a negative nitrogen balance.
Lactate produced in muscle can also be converted to glucose in the liver (117). Increased
epinephrine also results in skeletal muscle insulin resistance, sparing glucose for use by
glucose-dependent organs such as the heart and brain. Later in shock, hypoglycemia may
ensue, possibly because of glycogen depletion or hepatic ischemia (51,117,118). Fatty acids
are increased early in shock, but later levels fall (116). Without energy for glycolysis, the
cell depends on lipolysis and the autodigestion of intracellular protein for energy. Initially,
ketone bodies and the branched-chain amino acids are used as alternative fuel sources.
Without oxygen, these sources become inefficient, leading to hypertriglyceridemia,
increased β-hydroxybutyric acid and acetoacetate levels, and changes in the amino acid
concentration pattern. As these metabolic changes occur, set in motion by cellular hypoxia
and promoted by systemic hormonal changes, structural changes occur within individual
cells (119).
Organ Perfusion and Function during Hemorrhage
Heart
P.900
Page 16 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

The heart is a critical organ in the pathophysiology of shock. At baseline, myocardial oxygen
extraction is almost maximal; therefore, increased cardiac work must be met by increased
coronary blood flow. When coronary perfusion is compromised, as it is during systemic
hypotension, cardiac function suffers. In the presence of sympathetic stimulation, blood
flow from the endocardium is redistributed toward the epicardium, impairing cardiac
performance (120). Underlying coronary artery disease, arrhythmias, hypoxemia, and
acidosis can add to cardiac dysfunction. In the absence of coronary stenosis, myocardial
necrosis/infarction is unusual in hypovolemic shock. Rather, the heart plays a participatory
role in which it is unable to compensate fully for arterial hypotension caused by
hypovolemia, vasodilation, and other factors.
Under basal aerobic conditions, 60% of energy comes from fat (free fatty acids and
triacylglycerides), 35% from carbohydrates, and 5% from amino acids and ketone bodies.
However, during anaerobic conditions imposed by hypoxemia or ischemia, the myocardium
shifts to glycolysis. Anaerobic glycolysis, however, is insufficient to meet cardiac work
demands for any length of time because the myocardial glycogen stores, as an alternative
fuel source, are minimal and rapidly depleted.
Brain Like the heart, the brain almost exclusively depends on perfusion, rather than changes in
extraction, to meet its oxidative metabolic needs. Protective mechanisms, collectively
referred to as autoregulation, have evolved to guard perfusion. Pressure autoregulation
refers to the ability of the brain to maintain total and regional cerebral blood flow (CBF)
nearly constant despite large changes in systemic arterial blood pressure (Fig. 58.4) (121).
Cerebral function seems to be maintained until the mean arterial pressure drops below 50
to 60 mm Hg (122). The factors that control cerebral autoregulation are not completely
understood, but seem to include local carbon dioxide and oxygen tension, and the so-called
Bayliss effect (i.e., contraction or dilation of arteriolar smooth muscle in the presence of
increased or decreased intravascular pressure).
Page 17 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

In the presence of neurotrauma, autoregulation is impaired and the brain is exquisitely
sensitive to secondary insults, such as hypoxia and hypotension. Hemorrhagic shock and
resuscitation may also impair autoregulation because of endothelial cell dysfunction and
diminished NO-dependent vasodilator reactivity, so that the brain may experience an
oxygen deficit along with metabolic and functional deterioration (52,87). However, the
vulnerability of the brain to anoxic injury is uncertain and appears variable. The adequacy
and the method of resuscitation can critically influence postischemic recovery. These
observations have motivated investigation of specific brain resuscitation regimens
(123,124,125,126). However, there are no conclusive data that one modality provides
improved outcomes.
Lungs Hypovolemic shock is associated with a rise in minute ventilation marked by tachypnea, hyperventilation, and a fall in arterial PCO2 (28,30,127,128,129,130). These changes are
usually due to a decrease in pulmonary perfusion, leading to an increase in dead space ventilation. Thus, a higher minute ventilation is necessary for a given CO2 production
(28,30,127). In addition, minute ventilation may need to increase further in order to
compensate for a metabolic acidosis following accumulation of lactic acid in the blood. The
imbalance between the increased demands of the diaphragm and reduced blood flow in
shock may finally lead to respiratory muscle fatigue and respiratory failure, requiring
intubation (28). Therefore, early airway control is imperative in patients with severe
hemorrhagic shock.
Hemorrhagic shock requiring massive transfusion also increases the risk of acute respiratory
distress syndrome (129,130,131,132). Contributing factors include release of proinflammatory mediators; activation of neutrophils in the lungs and other organs after
reperfusion; contusion and/or ischemia-reperfusion of the lung; pulmonary microemboli of
neutrophils, platelets, and fat particles from long bone fractures; and induction of
transfusion-related acute lung injury (TRALI), which is discussed later in this chapter.
Kidney Oliguria, as defined by a urinary output of less than 0.5 mL/kg/hour, is a cardinal
Figure 58.4. Autoregulation. Cerebral pressure autoregulation refers to the ability of
the brain to maintain total cerebral blood flow (CBF) nearly constant between a broad
range of mean arterial pressures (MAPs). Cerebral function seems to be maintained
until the mean arterial pressure drops below 50 mm Hg. However, in the presence of
traumatic brain injury, autoregulation may become impaired, and the brain may be
more susceptible to changes in mean arterial pressure.
P.901
Page 18 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

manifestation of shock. However, the pathogenesis of shock-related oliguria is more
complex than mere renal hypoperfusion (133,134,135). Blood flow to the kidney is rarely
reduced below 40% to 50% of normal levels, even in the face of more severe reductions in
overall cardiac output. Thus, the decreased glomerular filtration rate results from
additional mechanisms. Sympathetic stimulation, circulating catecholamines, angiotensin,
and locally produced prostaglandins contribute to afferent arteriolar vasoconstriction.
These compounds promote the redistribution of blood flow away from cortical glomeruli
toward the renal medulla (65). Vasodilation of the efferent arteriole may amplify these
changes. The net effect is a decreased glomerular filtration rate and a decrease in the
energy needs of the kidney. Additional fluid (and salt) conservation is promoted by the
effects of aldosterone and antidiuretic hormone.
If renal hypoperfusion persists, the cortical kidney will become ischemic. Three pathologic
changes are observed: (a) tubular necrosis with back-diffusion of glomerular infiltrate, (b)
tubular obstruction by casts or other cellular debris, and (c) tubular epithelial damage with
consequent interstitial edema and tubular collapse. Following hypovolemia and renal
ischemia, these pathologic changes may be secondary events (i.e., reperfusion injury) that
can amplify but rarely initiate acute renal failure. The presence of these pathologic changes
partially explains why restoration of normal hemodynamic function does not often lead to
an immediate improvement in renal function. Although irreversible renal failure from shock
alone is rare, fluid and electrolyte balance are often supported by dialysis although normal
perfusion has been restored.
Intestine During hypovolemic shock, blood flow from intestine is redistributed to other organs. The
decrease in blood flow to the gut is relatively greater than the decrease in cardiac output
due to the local vasoconstriction caused by catecholamines, vasopressin, and angiotensin II
(4,5,26,136,137,138,139). Ischemic injury to the gut is manifested primarily by interstitial
fluid sequestration and hemorrhage or necrosis of the mucosal lining, and is most prominent
in the stomach (139). Ulcer formation (140) with exsanguinating hemorrhage can occur
several days after normal hemodynamic function has been restored (141). Breakdown of the
gut epithelium creates a port of entry for translocation of bacteria or deleterious bacterial
products (endotoxin) (142,143). These factors may be important in the pathogenesis of
irreversible shock (144) by releasing mediators to the systemic circulation. The
determination of mucosal pH via tonometry has been described as a potential indicator of
the therapeutic response and a marker of MODS (145,146).
Liver Hepatic perfusion declines during hypovolemic shock because of diminished portal and
hepatic arterial blood flow, roughly in proportion to the fall in cardiac output
(57,61,109,147,148,149,150). Clinical manifestations of ischemic liver injury are not usually
apparent in the early stages of hemorrhagic shock, as the organ participates in the release
Page 19 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

of acute-phase reactants. As hepatic cells die, they release characteristic enzymes (i.e.,
aspartate aminotransferase, alanine aminotransferase) (151). Occasionally, an obstructive
picture with elevated bilirubin and alkaline phosphatase predominates. Later, the synthesis
of coagulation factors, albumin, and prealbumin may deteriorate (152,153). Less clinically
obvious is the impairment in the reticuloendothelial system function. Impaired hepatic
clearance functions and reticuloendothelial system failure contribute to continued
circulation of vasoactive substances that can perpetuate shock. Hepatic ischemia may result
in a diminished capacity for metabolism of drugs and for gluconeogenesis from lactate and
amino acids, contributing to hypoglycemia in the late stages of hypovolemic shock. The
capacity to clear gut-derived endotoxin and lactate may also decrease, and the ischemic
liver produces lactate (154). The appearance of “shock liver” with massive hepatocellular
necrosis is unusual and presents mainly in patients with pre-existing liver conditions (155).
Spleen The spleen contracts during hypovolemic shock, probably due to an increased sympathetic
tone, which results in the release of red blood cells into the circulation (5,26). Changes in
hematocrit during the early phase of bleeding probably underestimate the severity of
plasma losses. The spleen also releases stored platelets.
Pancreas The importance of the pancreas in the clinical picture in hemorrhagic shock has not been
fully established. Older studies have demonstrated that the pancreas becomes severely
ischemic during hypovolemic shock (156). Recently, much work has been done to better
elucidate the role of the pancreas following hemorrhage and reperfusion. Preliminary data
suggest that following hemorrhage, the mucosal barrier of the intestine becomes ischemic
and therefore has increased permeability to pancreatic enzymes. These digestive enzymes
then gain access to the wall of the intestine, initiating self-digestion of submucosal
extracellular matrix proteins and interstitial cells. This initiates the generation and release
of a host of strong inflammatory mediators, which may contribute to the multiorgan
dysfunction syndrome. Recent investigations are focusing on protease inhibition in the
intestinal lumen as a means of attenuating the inflammatory response following hemorrhage
(157,158,159,160,161,162,163).
Inflammatory Response and Tissue Injury A detailed discussion of the inflammatory and immune response to trauma and hemorrhage
is beyond the scope of this chapter. However, several general concepts can be introduced. Following hemorrhage and
resuscitation, macrophages, including lung macrophages and Kupffer cells in the liver, may
release proinflammatory cytokines including tumor necrosis factor (TNF)-α and interleukin
(IL)-1, -6, and -8. During reperfusion, cytokines may induce and amplify the inflammatory
response to ischemia and may further induce local and remote organ damage
P.902
Page 20 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

(148,164,165,166,167,168,169,170,171,172,173,174). The reperfused gut, for example,
may, together with the liver, be a source of systemically circulating cytokines, and possibly
endotoxin. Release of mediators into the mesenteric lymph, portal, or systemic circulations
during reperfusion may have deleterious effects on remote organs, such as the lungs, due to
neutrophil activation and adherence, leading to pulmonary vascular injury with increased
permeability (165,168,169). Circulating levels of proinflammatory cytokines may thus be of
predictive value for remote organ damage, including ARDS, after trauma and hemorrhage in
patients (167,170).
Arachidonic acid makes up 20% of cell membranes and is released from these membranes in response to a multitude of stimuli that activate phospholipase A2 and C, and is then
metabolized via one of two major enzyme systems. The cyclo-oxygenase pathway results in
the production of thromboxanes and prostaglandins, while the lipoxygenase pathway
produces leukotrienes. Thromboxane has potent vasoconstricting properties on both the
pulmonary and splanchnic circulation, promotes aggregation of thrombocytes and
neutrophils, causes bronchoconstriction, and can lead to increased vascular permeability. The prostaglandins have varied effects. Prostacyclin (prostaglandin I2 [PGI2]) has potent
vasodilating properties and inhibits thrombocyte and neutrophil aggregation (175). PGE2 and
PGD2 also have vasodilating properties, while other prostaglandins (PGF2α) are potent
vasoconstrictors. Leukotrienes, which are produced by the lipoxygenase pathway, cause
vasoconstriction and increased capillary permeability and attract neutrophils (175).
Thromboxane, prostaglandins, and leukotrienes interact with other mediators in a complex
fashion (175,176,177,178,179). Vasoconstricting prostaglandins may be involved in the
tissue damage during ischemia/reperfusion. Vasodilating prostaglandins may be involved in
the vasodilated state of terminal hypovolemic shock (3,175,176,177,178,179).
Platelet-activating factor (PAF) is a nonprotein phospholipid, which is secreted by many
cells including platelets, endothelial cells, and inflammatory cells. It is a major mediator of
the pulmonary and hemodynamic effects of endotoxin. The major systemic effects of PAF
are vasodilatation, cardiac depression, and enhancement of capillary leak. Its complex
interactions with other mediators are still poorly understood (180).
Antigen–antibody complexes activate the complement cascade, and complement fragments
thus generated can interact with other cytokines to promulgate the inflammatory response.
Complement activation can yield potent vasodilating and leukoattractant substances
(175,177,181,182).
Oxygen radicals, such as hydrogen peroxide and superoxide anion, are released by activated
neutrophils in response to a variety of stimuli. They are also released when xanthine
oxidase is activated after reperfusion in ischemia-reperfusion models. These highly reactive
products lead to cell membrane dysfunction, increased vascular permeability, and release
of eicosanoids (183,184,185,186).
This inflammatory process results in the local accumulation of activated inflammatory cells,
which release various local toxins such as oxygen radicals, proteases, eicosanoids, platelet-
Page 21 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

activating factor, and other substances. When unregulated, such accumulations can cause
tissue injury. The initial attachment of neutrophils to the vascular endothelium at an
inflammatory site is facilitated by the interaction of adherence molecules on the neutrophil
and endothelial cell surfaces (108,187,188,189,190,191,192).
Immune Function following Hemorrhage and Resuscitation Despite the initiation of the inflammatory cascade, hypovolemic shock and resuscitation
depress the immune system by suppressing the function of lymphocytes, macrophages, and
neutrophils, depressing both humoral and cellular immune responses, decreasing antigen
presentation and delayed hypersensitivity to skin-test antigens, and increasing susceptibility
to sepsis (63,166,193,194,195,196,197,198). The immune consequences of hemorrhage and
resuscitation differ among cell populations, however, with some cells expressing enhanced
(199,200,201) and others diminished inflammatory responses (202,203). Hormone may also
influence immune response (204,205). The immunosuppression after hypovolemic shock may
also be potentiated by the release of anti-inflammatory cytokines (IL-10) (206,207,208) and
soluble cytokine receptors (receptor antagonists) for the proinflammatory cytokines
(203,209,210).
Management of Hemorrhagic Shock Trauma is by far the most common etiology for hemorrhagic shock. While other causes do
exist, management priorities are similar regardless of the source of bleeding. Diagnosis,
evaluation, and management must often occur simultaneously. A methodical approach is
necessary to optimize outcome. Unique to hemorrhagic shock, as opposed to other forms of
shock, is that definitive management frequently requires surgical or procedural intervention
to cease bleeding. The diagnostic pathway and interventions pursued become part of the
resuscitation pathway. What follows is a summary of the interventions, diagnostic studies,
monitoring strategies, and resuscitation techniques for hemorrhagic shock.
Immediate Management
Airway and Breathing When approaching any patient in shock, the sequence of events should be to address the
issues of airway, breathing, and circulation—also known as the “ABCs” (211). Most patients
with fully developed shock require tracheal intubation and mechanical ventilation, even if
acute respiratory failure has not yet developed. Studies have shown that during shock, the
respiratory muscles require a disproportionate percent of the cardiac output (28). Failure to
mount a hyperventilatory response to a metabolic acidosis is a significant predictor of the
need for subsequent intubation in trauma patients (212). Mechanical ventilation allows flow to be
redistributed, lessens the work of breathing, may help reverse lactic acidosis, and supports
the patient's airway until other therapeutic measures can be effective. Tracheal intubation
P.903
Page 22 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

is also required if there is evidence of mental status changes, such that airway protection is
questionable. Evidence of hypoxemia and/or hypoventilation is also an absolute
requirement for early intubation.
Perhaps most complex is the patient with evidence of compensated hemorrhagic shock
whose mental status is still intact. In this type of patient, clinical acumen is imperative. If
the initial response to resuscitation is sustained (i.e., “a responder”—see below), then close
observation of the airway may be appropriate while additional workup and treatment are
pursued. However, in a patient who is not responsive or has a transient response (see
below) to fluid resuscitation, control of the airway early is necessary prior to respiratory
collapse (212). In addition, if diagnostic and therapeutic interventions, such as angiography
and embolization, are required during resuscitation to control hemorrhage, early airway
control should be obtained.
Once the airway is secured, it is important to closely monitor techniques of ventilation.
Studies have shown that there is a tendency of rescue and medical personnel to
hyperventilate patients during resuscitation (213,214). Hyperventilated patients have been
shown to have an increased mortality when compared to nonhyperventilated patients in the
setting of severe traumatic brain injury (214). Animal studies have supported this
information, showing that cardiac output increases with hypoventilation and decreases with
hyperventilation and positive end-expiratory pressure (PEEP) (215,216). Thus, adequate
appropriate ventilator strategies are imperative early in hemorrhagic shock to optimize
tissue perfusion and outcome.
Circulation The management steps to restore adequate circulation are threefold:
1. Secure access to the bloodstream in order to initiate infusion of fluids and blood
products
2. Control obvious sources of hemorrhage and prevent ongoing hemorrhage
3. Assess extent of shock and hemorrhage
Intravenous Access Access to the bloodstream should be obtained expediently. Two peripheral large-bore
intravenous catheters (18 gauge or larger) are necessary. If cannulation of a peripheral vein
is difficult due to collapse, then central venous access should be secured. In the presence of
trauma to the torso, venous access above and below the diaphragm is preferable. When
obtaining intravenous access, it is important to note that the maximal rate of infusion via a
catheter is directly proportional to the diameter of the catheter and indirectly proportional
to the length. Therefore, a 9 French percutaneous introducer sheath will infuse fluids more
rapidly than a 7 French triple-lumen catheter. A large-bore peripheral intravenous catheter
Page 23 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

will also infuse fluids more rapidly than a 7 French triple lumen catheter due to a shorter
length and less resistance. In pediatric patients, an intraosseous access may be necessary.
This is only recommended for children under the age of 6 and should only be used until an
alternative source of venous access is obtained.
Control Obvious Hemorrhage Immediately Resuscitation of the bleeding patient requires early identification of potential bleeding
sources followed by prompt action to minimize blood loss, restore tissue perfusion, and
achieve hemodynamic stability. This is particularly important in the trauma patient where
multiple sources may be involved. Wound compression is the initial maneuver to control an
exsanguinating wound. For massive soft tissue injuries, placing a tourniquet proximally may
decrease hemorrhage and allow resuscitation prior to definitive control. Fractures should be
splinted or placed in traction. Evidence of pelvic instability or hemorrhage may be
temporized by a sheet, a pelvic binder, an external fixator, or a pelvic C-clamp
(217,218,219,220). In the presence of massive trauma, patients may present with
coagulopathy in the emergency department and this should be preemptively addressed. The
same principles should be applied to nontraumatic hemorrhagic shock, such as
gastrointestinal bleeding and ruptured aortic aneurysms: rapidly identify and attenuate the
obvious sources of hemorrhage.
Initiate Resuscitation and Assess Extent of Bleeding: Responders and Nonresponders The traditional classification of hemorrhagic shock was discussed earlier (Table 58.3). While
this is a useful guideline for determining the extent of blood loss for a given patient,
perhaps more important in determining an appropriate treatment algorithm is the patient's
response to resuscitation. Following hemorrhage, resuscitation should be initiated with 2 L
of lactated Ringer solution or isotonic crystalloid solution. The response to this initial fluid
bolus will provide critical insight as to the presence of ongoing hemorrhage and need for
surgical intervention (Table 58.4) (221).
Rapid responders become hemodynamically normal and remain this way following the initial
fluid bolus. This group of patients has likely lost <20% of their total circulating blood
volume, and ongoing aggressive resuscitation is not necessary. Intravenous fluids can be
lowered to maintenance rates while additional workup proceeds. Blood should still be sent
for type and cross-match and should be made available. Retrospective studies have shown
that patients with field hypotension who become normotensive on arrival to the emergency
department have increased morbidity, mortality, need for operation, and admission rate to
the intensive care unit (ICU) (222,223,224). Approximately 15% of these patients will need
transfusion, with 37% requiring therapeutic surgery (224). Hence, even a brief episode of
hypotension can be a marker for significant underlying injury.
Transient responders represent a group of patients who initially respond to a 2-L bolus of
Page 24 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

crystalloid, but then begin to show signs of deterioration when intravenous fluid infusion is
lowered to maintenance levels. These patients have likely lost 20% to 40% of their
circulating blood volume, and either have ongoing blood loss or inadequate resuscitation.
Continued fluid resuscitation and initiation of blood transfusion are indicated. A transient
response to blood infusion indicates ongoing hemorrhage. Rapid surgical intervention or
angioembolization (225,226,227,228) to control hemorrhage is immediately indicated.
Nonresponders represent patients who fail to respond to crystalloid and blood
administration in the emergency department. These patients have likely lost >40% of their
circulation blood volume and have ongoing hemorrhage. Immediate control of hemorrhage is
necessary via surgical intervention or angioembolization in the face of significant pelvic fractures (225,226,227,228). On rare
occasions, failure to respond to fluid administration may be due to pump failure as a result
of blunt cardiac injury, cardiac tamponade, tension pneumothorax, or myocardial
infarction. Central venous pressure monitoring and cardiac ultrasonography may help
differentiate between various etiologies in this setting.
P.904
Table 58.4 Response to initial fluid resuscitation and patient management
Rapid response Transient response No response
Vital signs Return to
normal
Transient response,
recurrent
hypotension, and/or
tachycardia
Remains
abnormal
Estimated
blood loss
Minimal
(10%–20%)
Moderate (20%–40%) Severe (>40%)
Additional
crystalloid
Unlikely Yes Yes
Need for blood
transfusion
Unlikely Moderate to high Immediate
Blood
preparation
Type and
cross-match
Type-specific (10–20
min)
Emergency
blood release
Page 25 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

Emergency Department Resuscitative Thoracotomy Resuscitative thoracotomy is occasionally indicated for exsanguinating hemorrhage. In
trauma, indications for resuscitative thoracotomy include (a) patients with penetrating
thoracic injuries who arrive pulseless, but with myocardial electrical activity, and (b) blunt
trauma patients who have vital signs on arrival but then sustain a witnessed arrest or onset
of pulseless electrical activity. Specific recommendations are listed in Table 58.5.
Therapeutic maneuvers that can be attained with a resuscitative thoracotomy include (a)
evacuation of pericardial blood causing tamponade, (b) direct control of exsanguinating
thoracic or cardiac hemorrhage, (c) open cardiac massage, and (d) cross-clamping of the
descending aorta to slow blood loss below the diaphragm and improve perfusion to the
heart and brain.
Depending on the cause of injury, the overall mortality rate in these situations is extremely
high (229,230,231). The highest survival rates are found in patients with isolated cardiac
injury without loss of vital signs (approximately 35%). Some reports of thoracic aortic cross-
clamping for exsanguinating intra-abdominal hemorrhage have reported survival rates of
nearly one third (231,232), but this is mainly in the setting of penetrating abdominal
trauma. Survival rates following resuscitative thoracotomy in blunt trauma are dismal,
ranging from 0% to 5%. Aortic cross-clamping should be viewed as an adjunct to other initial
hemorrhage control measures. It has not been established whether thoracic aortic clamping
should be performed before or after the abdominal incision, or whether thoracic or intra-
abdominal aortic cross-clamping is more effective (233). However, when aortic cross-
clamping is deemed necessary for continuous bleeding or low blood pressure, the prognosis
(30–60 min) (immediate
type O Rh-
negative blood)
Operative
intervention
Possible Likely Highly likely
Early presence
of surgeon
Yes Yes Yes
Adapted from American College of Surgeons Committee on Trauma. Shock. In:
Advanced Trauma Life Support. 7th ed. American College of Surgeons Chicago,
IL; 2004:79.
Page 26 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

is generally poor (234). No clinical data exist for the use of emergency room thoracotomy in
nontrauma infradiaphragmatic bleeding.
Adjunctive Measures Historical teachings have been that tilting a patient into head-down position (i.e.,
Trendelenburg) diverts blood volume into the central circulation and improves venous
return, thereby improving stroke volume and cardiac output in hypovolemic shock.
However, recent studies do not show any significant redistribution of blood volume centrally
(235). In fact, the head-down position can worsen gas exchange and cardiac function.
Therefore, the Trendelenburg position is no longer recommended as a resuscitative
technique. If this type of measure is deemed desirable, raising the legs above the level of
the heart should be adequate (13).
Table 58.5 Indications and contraindications for emergency department resuscitative thoracotomy
INDICATIONS
Salvageable postinjury cardiac arrest
Patients sustaining witnessed penetrating trauma with <15 min of prehospital
cardiopulmonary resuscitation (CPR)
Patients sustaining witnessed blunt trauma with <5 min of prehospital CPR
Persistent severe postinjury hypotension (systolic blood pressure ≤60 mm Hg)
due to:
Cardiac tamponade
Hemorrhage—intrathoracic, intra-abdominal, extremity, cervical
Air embolism
CONTRAINDICATIONS
•Penetrating trauma: CPR >15 min, anda
•Blunt trauma: CPR >5 min, and No signs of lifea or asystole
aNo signs of life = no pupillary response, respiratory effort, or motor activity.
Page 27 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

The use of pneumatic antishock garments (PASGs, previously military antishock trousers
[MAST]) currently has a limited role in the management of hypotensive trauma patients.
Although their use was almost universal for hemorrhage control in the late 1970s and 1980s,
recent studies have demonstrated that they have no effect on patients with thoracic injury.
In fact, some evidence suggests that mortality is higher when PASGs are applied (236,237).
No survival advantage has been demonstrated in the pediatric population, although there
may be a small survival benefit in children with a systolic blood pressure of less than 50 mm
Hg (238). The main utility of PASGs currently is as a temporizing agent to stabilize pelvic
fractures.
Fluid Resuscitation Careful attention to fluid resuscitation is necessary during management of hemorrhagic
shock to optimize outcome. It is still unclear which type of fluid should be employed in the
initial treatment of the bleeding patient.
Colloids versus Crystalloids Several meta-analyses have shown an increased risk of death in patients resuscitated with
colloids as compared with crystalloids (239,240,241,242,243) during hemorrhagic shock.
While three of these studies suggested that the effect was particularly significant in the
trauma population (239,242,243), the results of a recent meta-analysis showed no
significant difference (244). A recent trial evaluating 4% albumin versus 0.9% normal saline
in nearly 7,000 ICU patients showed that albumin administration was not associated with
worse outcome. There was a trend, however, toward higher mortality in the trauma
subgroup that received albumin (p = 0.06) (245). The difficulty with interpreting these
meta-analyses and the individual studies is that they are very heterogenous. Each evaluates
different patient populations and resuscitation strategies, and mortality may not always be
Adapted from Cothren CC, Moore EE. Emergency department thoracotomy for the
critically injured patient: objectives, indications, and outcomes. World J Emerg
Surg. 2006;1:4.
P.905
Page 28 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

a primary end point. However, given these results, crystalloid resuscitation is currently the
accepted standard as initial therapy for hemorrhagic shock.
Many synthetic colloid solutions such as hetastarch and dextran have also been associated
with coagulopathy. Recent research suggests that hetastarch solutions with a high mean
molecular weight and a high C2/C6 ratio suppress coagulation more than solutions with
rapidly degradable low-molecular-weight colloids (246,247,248). This coagulopathy may be
produced by one of several potential mechanisms including a reduction in von Willebrand
factor, platelet dysfunction, reduced factor VII levels, and an interaction with fibrinogen
(249,250).
Crystalloid solutions are not without side effects. Resuscitation with fluids that contain
supraphysiologic concentrations of chloride can lead to hyperchloremic acidosis. This can be
significant in patients where lactic acidosis may already be present. Lactated Ringer
solution contains a more physiologic concentration of chloride (109 mEq/L) than normal
saline (NS 154 mEq/L), and therefore may be the preferred choice. Animal studies have also
shown that resuscitation with normal saline can lead to more coagulopathy and increased
blood loss than resuscitation with lactated Ringer solution (251).
Massive resuscitation with crystalloid fluids alone can lead to several significant
complications including cardiac and pulmonary complications, gastrointestinal dysmotility,
coagulation abnormalities, and immunologic dysfunction (252). Reports of lactated Ringer
solution and normal saline increasing reperfusion injury and leukocyte adhesion suggest that
crystalloid resuscitation may worsen acidosis and coagulopathy in severely injured patients
and possibly increases the risk of ARDS, systemic inflammatory response syndrome (SIRS),
and multiorgan failure (MOF) (252,253,254,255,256). Abdominal compartment syndrome has
been clearly associated with excessive use of crystalloid resuscitation
(50,257,258,259,260,261). Recently, there has been increased focus on early use of blood
products in order to minimize crystalloid use in the resuscitation of hemorrhagic shock
(262). Finally, resuscitation strategies that focus on early aggressive fluid resuscitation to
normalize blood pressure before bleeding is controlled may result in increased hemorrhage
and increased mortality. This has led some authors to suggest that “hypotensive
resuscitation” should be the goal until the source of hemorrhage is controlled
(263,264,265). However, the exact goals for mean arterial pressure and trigger points for
bleeding have not been established. The potential adverse sequelae when used in patients
with associated injuries or comorbidities (i.e., severe closed head injury) have not been
clearly established (266).
In light of these potential sequelae of resuscitation, future research should focus on
improvement in fluid composition and adjuncts to the administration of large volumes of
fluid (266). Current strategies should focus on the type of fluid delivered, the rate of
delivery, the timing of delivery, and the prevention of sequelae from large-volume
resuscitation.
Page 29 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

Preventing Hypothermia All fluids during resuscitation from hemorrhagic shock should be warmed to prevent
hypothermia. Equipment is now available that allows the rapid infusion of blood and/or
crystalloids at warmed temperatures (i.e., up to 750 mL fluid per minute warmed to over
37°C). This newer equipment is more effective and efficient and results in fewer
complications associated with earlier models (such as air embolism and bacterial
contamination) (267). Other techniques during resuscitation that can be used to prevent
hypothermia in the acutely hemorrhaging patient include warming the circuit on the
ventilator in ventilated patients, ensuring the patient is covered with warm blankets at all
times following exposure and thorough examination, warming the resuscitation and
operating rooms, using external warming blankets such as the Baer hugger during
resuscitation and in the operating room, and using warm water blankets on the operating
room table during exploratory operations. Hypothermia is clearly associated with increased
mortality following resuscitation from hemorrhagic shock (268), and every attempt to
prevent or minimize its occurrence and severity should be employed.
Diagnostic Approach If no obvious source of external bleeding is identified, a rapid evaluation should be
performed to identify likely occult sources of bleeding. In the trauma patient, significant
internal hemorrhage can occur in four defined regions: the thoracic cavity, the peritoneal
cavity, the retroperitoneum, and extremity fractures. These areas can be rapidly assessed
via chest radiograph, a pelvic radiograph, FAST, and physical examination of extremities
along with appropriate radiographs. In-depth coverage of the diagnosis of abdominal trauma
is provided in a later chapter of this book. In nontrauma patients without clear evidence of bleeding, the
gastrointestinal tract should be rapidly evaluated via nasogastric tube, rectal examination,
and endoscopy where appropriate. Additional diagnostic tests can be obtained based on
clinical history, patient background, and condition. Abdominal aortic aneurysms can be
identified on physical examination, by ultrasound, or by calcifications on abdominal
radiograph. In selected instances, angiography may be used to identify and treat sources of
hemorrhage not otherwise apparent (pelvic fractures, pancreatitis, lower gastrointestinal
bleeding) (225,226,227,228,269,270,271,272,273,274,275,276,277). This should only be
instituted when a specific source of hemorrhage is highly likely and therapeutic intervention
is sought. Computed tomography should never be sought in hemodynamically unstable
patients with hemorrhage.
Laboratory Testing and Monitoring of Resuscitation
Measurement of Bleeding
P.906
Page 30 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

Hematocrit/Hemoglobin Hemoglobin and hematocrit measurements have long been part of the basic diagnostic
workup of patients with hemorrhage and/or trauma. However, in patients with rapid
bleeding, a single hematocrit measurement on presentation to the emergency department
may not reflect the degree of hemorrhage. In a short transport or presentation time, prior
to initiation of resuscitation, the body's compensatory mechanisms for fluid retention and
resorption into the vascular space have not taken place, and initial hematocrit levels may
remain stable despite significant blood loss. A retrospective study of 524 trauma patients
(278) determined that the initial hematocrit had a sensitivity of only 0.50 for detecting
patients with an extent of traumatic hemorrhage requiring surgery. The diagnostic value is
further confounded by the administration of intravenous fluids and red cell concentrates
during resuscitation (278,279,280,281).
Two prospective observational studies determined the sensitivity of serial hematocrit
measurements for detecting patients with severe injury (282,283). In the first study (282),
the authors compared values of hematocrit at admission and 15 minutes and 30 minutes
following arrival to the emergency department. A normal hematocrit on admission did not
preclude significant injury. The mean change in hematocrit levels between arrival and 15
minutes, and 15 minutes and 30 minutes was not significantly different in patients with or
without serious injuries. However, a decrease of hematocrit by >6.5% at 15 and 30 minutes
had a high specificity for injury (0.93–1.0), but a low sensitivity (0.13–0.16).
Another prospective observational study examined the utility of serial hematocrit
measurements during the initial 4 hours following admission (283). A significant limitation
to this study is that they removed patients who required a blood transfusion in order to
eliminate confounding variables. In the remaining 494 patients, a decrease in hematocrit of
more than 10% between admission and 4 hours was highly specific for severe injury (0.92–
0.96), but again, it was not sensitive (0.09–0.27).
Overall, decreasing hematocrit levels over time may reflect continued bleeding. However,
patients with significant bleeding may maintain their hematocrit level, especially in the
absence of resuscitation. Conversely, hematocrit levels may also be confounded by
aggressive fluid resuscitation early during resuscitation (278,279,280,281). An initial
hematocrit level will help to identify patients who present with pre-existing anemia who
may have a lower threshold for hemorrhage. The hematocrit level should be used in
conjunction with other measures of perfusion in order to determine the presence of occult
hemorrhage.
Measurements of Perfusion
Lactate Lactate was initially suggested as a diagnostic parameter and prognostic indicator of
Page 31 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

hemorrhagic shock in the 1960s (284). Substantial data exist that lactate levels as a marker
of tissue oxygen debt can predict outcome in various forms of shock (60,285,286,287,288).
In 1983, Vincent et al. performed a prospective study on 27 patients with circulatory shock
and concluded that changes in lactate concentrations provided an early and objective
evaluation of a patient's response to therapy (289). However, its overall utility has been
questioned by some because it is felt to be a late marker of tissue hypoperfusion, can be
affected by hepatic function, and can be influenced by glycolysis and alkalosis
(290,291,292,293).
Despite these concerns, data do exist showing that the amount of lactate produced by
anaerobic glycolysis is an accurate indirect marker of oxygen debt, tissue hypoperfusion,
and the severity of hemorrhagic shock (294,295,296,297,298,299,300,301,302,303,304,305).
In many forms of shock, arterial lactate levels above 2 mEq/L have been associated with
increased mortality (286,287,300,305). However, during hemorrhage, not only is the initial
lactate level important, but also the rate of clearance (298,299). Two prospective studies
confirm this. In one prospective observational study (298), 76 patients with multiple trauma
were analyzed with respect to clearance of lactate between survivors and nonsurvivors over
48 hours. If lactate normalized within 24 hours, survival was 100%. Survival decreased to
77.8% if normalization occurred within 48 hours, and to 13.6% in those in whom lactate
levels remained elevated above 2 mEq/L for more than 48 hours. This was confirmed in
another prospective study of 129 trauma patients (299) in which initial lactate levels were
higher in nonsurvivors. A prolonged time to normalization (>24 hours) was associated with
the development of posttraumatic organ failure. Finally, venous lactate has been shown to
be an excellent approximation for arterial lactate in acute trauma patients and is a useful
marker for significant injury (306).
Taken together, these studies suggest that both the initial lactate level and the rate of
clearance are reliable indicators of morbidity and mortality following trauma. However,
whether lactate should be used as an end point of resuscitation or is merely a marker of
tissue ischemia has not been clearly established.
Base Deficit Base deficit values derived from arterial blood gas analysis have also been shown to provide
an indirect estimation of tissue acidosis due to impaired perfusion
(294,296,297,300,301,302,303). However, base deficit can be affected by resuscitation
fluids (hyperchloremic metabolic acidosis) and exogenous administration of sodium
bicarbonate. Despite these potential drawbacks, initial base deficit has been shown in
several retrospective studies to correlate with transfusion requirements, organ dysfunction,
morbidity, and mortality following trauma (307,308,309,310,311,312,313). The magnitude
and severity of the base deficit also correlates to outcome, and is useful in both pediatric
and elderly patients (307,310,311,312). Base deficit has been shown to be a better predictor of outcome than pH alone following traumatic injury (309). Recently,
serum bicarbonate levels have been shown to be an appropriate surrogate for arterial base
P.907
Page 32 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

deficit in the ICU (314,315).
Lactate versus Base Deficit Although many studies have shown that both base deficit and serum lactate levels correlate
with outcome following trauma and hemorrhage, these two parameters do not always
correlate with each other (304,316). In fact, lactate has been found to be a superior
predictor of mortality as compared to base deficit in a recent study of patients in the
intensive care unit following trauma (304). Both base deficit and lactate have been shown
to correlate to outcome in nontraumatic etiologies of hemorrhagic shock (268,317). Given
that there are confounding variables following trauma that can affect measured levels of
both lactate and base deficit, independent assessment of both parameters along with the
patient's clinical condition is recommended for the evaluation of shock in trauma patients.
Measurement of Coagulopathy
Standard Coagulation Studies Coagulopathy associated with hemorrhagic shock may be due to one of several etiologies:
(a) iatrogenic, in which a dilutional coagulopathy develops due to inadequate resuscitation
with clotting factors and blood products; (b) premorbid, in which some patients may have a
pre-existing coagulopathy due to underlying disease (such as cirrhosis, hemophilia, von
Willebrand, renal failure, etc.); and (c) acute traumatic coagulopathy, in which
coagulopathy after trauma is common. Traditional teachings have been that this
coagulopathy is not inherent, but rather iatrogenic, due to dilution from intravenous fluid
therapy, massive blood transfusions, progressive hypothermia, and acidosis. Recent
literature has now determined that an inherent acute traumatic coagulopathy is present in
up to 30% of patients who present to the emergency department immediately following
trauma and is an independent predictor of morbidity and mortality (318,319,320,321).
Therefore, acute measurement of coagulation parameters during resuscitation from
hemorrhagic shock is indicated.
Table 58.6 Transfusion guidelines for patients with coagulopathy and hemorrhage or traumatic injury
GOALS RECOMMENDED THERAPY
Hematologic/coagulation parameters Blood products
Hemoglobin/hematocrit
Hgb >7.0 g/dL
Packed red blood cells
Page 33 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

Traditional studies of coagulation include prothrombin time (PT), activated partial
thromboplastin time (aPTT), fibrinogen level, and platelet count. Although no tightly
controlled trials have been performed, current recommendations for therapeutic end points
in hemorrhagic shock include maintaining PT and aPTT at less than 1.5 times the normal
value, maintaining a platelet count of >100 in patients with active bleeding or traumatic
brain injury, and maintaining a fibrinogen level of >1 g/L (229,322,323) (Table 58.6).
While these laboratory studies are standard, they do present several drawbacks. To begin,
in vivo coagulation depends on the interaction between platelets and coagulation factor
enzymes. Laboratory values of PT and aPTT are performed on platelet-poor plasma and fail
to evaluate the cellular interactions of clotting. PT and aPTT measurements also do not
take into account hypothermia-induced coagulopathy because samples are warmed prior to
measurement. Platelet and fibrinogen assays give numerical values, but fail to assess
function. Finally, each of these tests takes time, up to 30 to 45 minutes. This lag time
makes these studies clinically inefficient because when the results become available, they
may not truly reflect the patient's clinical condition. During resuscitation, actively bleeding
patients are in a constant state of flux. Alternative point-of-care testing such as the iSTAT
handheld analyzer can provide rapid bedside results, but is currently limited to activated
clotting time (ACT) and PT/international normalized ratio (INR) (250). The clinical
implications of acute trauma coagulopathy and clinical testing are discussed further later in
this chapter.
Hemodynamic stability
Prothrombin time <1.5 times normal Fresh frozen plasma
Prothrombin complex
concentrate
Activated partial prothrombin time <1.5 times
normal
Fresh frozen plasma
Fibrinogen >100 g/dL Cryoprecipitate
Platelets >50 × 109 per liter (stable,
nonbleeding patient)
Platelets >100 × 109 per liter (acute, bleeding
patient)
Platelet transfusion
Page 34 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

Thromboelastograph Analyzer The thromboelastograph (TEG) analyzer is a bedside machine that provides a functional
evaluation of overall coagulation on whole blood at the same temperature as the patient.
The TEG has been shown to be a more sensitive measure of coagulation disorders than
standard coagulation measures (324). The thromboelastograph assay provides a tracing that
measures clotting (R value), clot formation (α angle), clot strength (maximum amplitude
[MA]), and clot lysis (LY 30) (Fig. 58.5). Elongation of the R value represents a deficiency in
coagulation factors. The α angle represents the rate of fibrin accumulation and cross-linking, which can be affected by
fibrinogen function and, to a lesser degree, platelet function. The MA is a measure of clot
strength and is affected primarily by platelets and, to a lesser degree, fibrinogen. A study
investigating the utility of the TEG in trauma patients found that 65% of patients were
hypercoagulable and 10% were hypocoagulable. Of the seven hypocoagulable patients, only
one had an elevated PT and PTT, but six of seven required blood transfusion (325). Only the
Injury Severity Score (ISS) and TEG were predictive of early transfusion.
A large volume of literature exists describing the use of the TEG in various settings including
trauma, transplant, and cardiac surgery (250,325,326,327,328,329,330). However, despite
P.908
Figure 58.5. Thromboelastogram. The thromboelastograph (TEG) analyzer is a
bedside machine that provides a functional evaluation of overall coagulation on whole
blood at the same temperature as the patient. The thromboelastograph assay provides
a tracing that measures time to clot formation (R value), speed to a certain clot
strength (K value), rate of clot formation (α angle), overall clot strength (maximum
amplitude [MA]) and clot lysis (LY 30).
Page 35 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

its many advantages, the TEG has not become the standard of care for measurement of
coagulopathy. Using the TEG, whole blood samples must be run within 3 to 4 minutes of
collection, necessitating the presence of multiple machines in critical areas of the hospital.
Quality control of each of these machines is work intensive. Differences due to age, gender,
blood collection sites, and sample stability have been raised (331,332,333,334,335,336).
Finally, accurate readings require appropriate processing, and intensive ongoing education
of hospital staff would be necessary to ensure accurate results. Although the real-time
functional results of routine TEG analysis would be clinically useful, the current processing
and maintenance requirements make it impractical for routine use.
Rapid Definitive Control of Bleeding Multiple studies have confirmed that patients in need of emergency surgery for ongoing
hemorrhage have a better survival if the elapsed time to definitive care is minimized
(337,338,339,340,341,342,343,344,345,346,347). Those patients with unnecessary delays in
diagnosis and definitive treatment will have increased morbidity and mortality (344).
Although there are no prospective randomized trials confirming this, multiple retrospective
studies provide ample data to confirm the validity of this strategy. In trauma, early surgical
control of hemorrhage has been associated with improved survival in penetrating vascular
injuries (337), duodenal injuries (338), and polytrauma patients in extremis (339). A
multicenter retrospective review of over 500 deaths in the operating room concluded that
delayed transfer to the operating room was a cause of death that could be avoided by
shortening the time to diagnosis and resuscitation (348). Similar results have been
documented in the treatment of patients with ruptured abdominal aortic aneurysms who
are hemodynamically unstable (345,346,347). The benefit for rapid transport time to the
operating room is not as dramatic for patients who are hemodynamically stable following
ruptured abdominal aortic aneurysm (AAA), implying that ongoing hemorrhage has been
arrested in this group of patients.
The development of trauma systems has significantly contributed to improved trauma
outcomes by triaging more severely injured patients to hospitals that have systems in place
to rapidly diagnose, resuscitate, and definitively treat patients with hemorrhagic shock
(340,341,342,343). The implementation of trauma systems has resulted in improved
outcomes in severely injured patients, decreased time to operating room in hypotensive
patients, decreased complications, decreased hospital length of stay, and decreased
mortality, especially in patients with severe injury as measured by an ISS of >15 (343).
Definitive prompt care is critical to optimize outcomes in patients with trauma and
hemorrhage.
Lethal Triad of Resuscitation: Hypothermia, Acidosis, and Coagulopathy Patients with severe hemorrhagic shock requiring massive resuscitation are at risk for
exhaustion of their physiologic reserves, leading to irreversible shock and the inability to
Page 36 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

recover despite ongoing resuscitation. The common denominator in these patients is the
development of the “lethal triad,” “bloody vicious cycle,” or “spiral of death”—terms used
to describe the combination of profound acidosis, hypothermia, and coagulopathy (Fig.
58.6). Each of these factors has been independently associated with increased risk of death (268,303,319,349,350,351,352,353,354). There also seems to be a cumulative synergistic
effect for each of these risk factors in patients with hemorrhagic shock. In one
retrospective study of 39 patients with abdominal packing for surgically uncontrollable
bleeding (351), five risk factors for death were identified: pH <7.18, temperature ≤33°C, PT
≥16, PTT ≥50, and transfusion greater than 10 units of blood. Patients with zero to one risk
factor had an 18% mortality, two to three risk factors 83% mortality, and four to five risk
factors 100% mortality. Similar findings were reported by Cosgriff et al., who identified risk
factors for the development of life-threatening coagulopathy (352). Patients with an ISS of
>25, pH <7.1, temperature less than 34°C, and systolic blood pressure ≤70 mm Hg had a 98%
chance of developing life-threatening coagulopathy, whereas patients with none of these
risk factors had a 1% chance of developing coagulopathy.
The development of profound acidosis, hypothermia, and coagulopathy is a lethal
combination in patients during the resuscitation from hemorrhagic shock. Resuscitation
strategies should be designed at limiting the development of these complications.
P.909
Figure 58.6. Lethal triad of hemorrhagic shock. The development of acidosis,
hypothermia, and coagulopathy during resuscitation from hemorrhagic shock is
described as the “lethal triad,” “bloody vicious cycle,” or “spiral of death.” Each of
these factors has been independently associated with mortality. There is a cumulative
synergistic effect for each of these variables, such that irreversible shock may develop
if all factors are present.
Page 37 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

Damage Control Laparotomy Damage control laparotomy (355) is a concept that was initially introduced by Pringle in
1908 when he described the use of hepatic sutures over packs to control bleeding. In 1913,
Halsted detailed the procedure and modified its techniques. During World War II, damage
control laparotomy fell out of favor and was not reintroduced until 1955 when Madding et
al. reported the use of packs to temporize intraoperative bleeding, but felt that they
needed to be removed prior to abdominal closure. In the 1970s, Ledgerwood had successful
case reports using abdominal packing to control bleeding following trauma. However, the
modern era of damage control laparotomy is attributed to Stone et al. who, in 1983,
described the techniques of abbreviated laparotomy, packing to control hemorrhage, and
deferred definitive surgical repair of injuries until coagulation had been established (356).
Since then, a number of authors have described the beneficial effects of damage control
laparotomy (357,358,359,360,361,362,363,364,365,366). Although retrospective, studies
have documented a nearly 50% decrease in operative times for the most severely injured
patients treated by this approach and salvage rates of 20% to 60% in patients who would
have formerly died in the operating room (351,353,358,367).
The principle of damage control surgery is to obtain rapid control of hemorrhage and
contamination, with early completion of the operation, with a goal to restore normal
physiology as opposed to normal anatomy (Table 58.7). The ultimate goal is to prevent
patients from exhausting their physiologic reserves by developing the “lethal triad of
death,” or profound hypothermia, acidosis, and coagulopathy. Damage control surgery has
three basic components. First, an abbreviated laparotomy for control of bleeding, control of
contamination, and restitution of blood flow are necessary. The goal is to achieve these end
points as quickly as possible without spending unnecessary time on traditional organ repairs
that can be performed at a later time. The abdomen is packed and a temporary abdominal
closure is performed (Fig. 58.7). The second component involves treatment in the intensive
care unit that is focused on core rewarming, correction of acidosis, and reversal of
coagulopathy, as well as optimizing ventilation and hemodynamic status. This phase will typically last for 24 to 48 hours. The third component
is definitive surgical repair that is performed only when target parameters have been
achieved. This sequence may require several operative interventions to attain definitive
repair, each with a goal of preserving the physiologic reserve of the patient.
P.910
Table 58.7 Damage control laparotomy and damage control resuscitation
DAMAGE CONTROL LAPAROTOMY
Page 38 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

1. Abbreviated laparotomy (initial procedure)
Control of bleeding
Control of contamination
Restitution of blood flow
2. Resuscitation in the intensive care unit (24–48 h)
Core rewarming
Correction of acidosis
Reversal of coagulopathy
Optimization of ventilation and hemodynamics
3. Definitive surgical repair (days to weeks)
Restoration of continuity
Completion of resection
Removal of packs
Closure of abdomen
DAMAGE CONTROL RESUSCITATION
Hypotensive resuscitationa
Hemostatic resuscitation
aHypotensive resuscitation is still considered experimental and requires
experienced physician oversight and careful patient selection.
Page 39 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

Damage Control Resuscitation Damage control resuscitation (DCR) is a term that has recently been coined to describe a
specific strategy during the resuscitation phase of trauma care (250,368,369). It should be
initiated within minutes of presentation and is meant to preemptively address issues
associated with resuscitating critically injured patients: prevention of hypothermia,
acidosis, and coagulopathy. Damage control resuscitation involves two components:
hypotensive resuscitation and hemostatic resuscitation (Table 58.7).
Hypotensive Resuscitation Hypotensive resuscitation refers to the concept that fluid should be administered at a rate
that returns the systolic blood pressure to a safe but lower than normal pressure until
Figure 58.7. Open abdomen with temporary abdominal closure. A key component to
damage control laparotomy is to perform an abbreviated laparotomy for control of
bleeding, control of contamination, and restitution of blood flow. The goal is to
achieve these end points as quickly as possible to avoid the development of
irreversible shock and the lethal triad of acidosis, hypothermia, and coagulopathy.
Frequently, the abdomen is temporarily closed and the fascia left open to prevent the
development of abdominal compartment syndrome during resuscitation. Re-
exploration usually takes place 24 to 48 hours later, and every few days thereafter
until the fascia is closed. Occasionally, the fascia cannot be reapproximated due to
loss of domain. In this circumstance, a ventral hernia remains, which can be repaired
at a later date (usually 6–12 months postinjury).
Page 40 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

operative control of bleeding can be established. The traditional treatment of hemorrhaging
patients has used early and aggressive fluid administration to restore blood volume.
However, this approach may increase hydrostatic pressure on the wound or injured vessel,
leading to dislodgement of blood clots, a dilution of coagulation factors, and undesirable
cooling of the patient. Low-volume fluid resuscitation, or “permissive hypotension,” may
avoid the adverse effects of early aggressive resuscitation while maintaining a level of
tissue perfusion adequate for short periods. This strategy has been suggested historically for
the management of ruptured abdominal aortic aneurysm patients (370), and has recently
regained attention in the trauma population (263,264,265,266,371,372,373,374,375). It has
shown promise in animal and human trials (263,265), but has yet to be confirmed in large-
scale prospective randomized human clinical trials. Overall, data have been mixed (264). A
recent animal trial suggests that increases in blood pressure are well tolerated without
exacerbating hemorrhage when they are achieved gradually and with a significant delay
following the injury (376). Finally, a recent Cochrane Database review found that there was
not conclusive evidence from randomized controlled trials for or against early or larger
volumes of intravenous fluid resuscitation in uncontrolled hemorrhage (377).
Although the concept of permissive hypotension seems promising in some circumstances,
further work needs to be done. In addition, it requires extraordinarily tight control by an
experienced physician who is guiding fluid resuscitation moment to moment. Hypotensive
resuscitation should not be considered in patients with traumatic brain injury and spinal
cord injury where adequate cerebral perfusion pressure is crucial to ensure tissue
oxygenation (229,375). It should also be carefully considered in elderly patients and may be
contraindicated in patients with a history of chronic hypertension (229). At the present
time, it is considered experimental, and should be employed only in specific circumstances
with experienced physicians.
Hemostatic Resuscitation Conventional resuscitation practice for damage control has focused on rapid reversal of
acidosis and prevention of hypothermia. Surgical techniques are aimed at controlling
hemorrhage and contamination rapidly, with definitive repair occurring following
hemodynamic stabilization. However, direct treatment of coagulopathy early has been
relatively neglected, and has been viewed as a byproduct of resuscitation, hemodilution,
and hypothermia. Delay in availability of blood products due to current blood banking
techniques has also hindered the ability to employ immediate resuscitation with clotting
factors.
It has now been demonstrated that acute traumatic coagulopathy is present in 25% to 30%
of critically injured patients on arrival to the emergency department (318,319,320,321).
The presence of coagulopathy may be even higher in patients with severe closed head
injury, with an incidence of 21% to 79% when stratified by ISS (378). It has also been shown
that the presence of early coagulopathy is an independent predictor of mortality following
trauma (319). Early acute traumatic coagulopathy appears to be due to alterations in the
Page 41 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

thrombomodulin–protein C pathway rather than consumption of coagulation factors (321);
however, additional work needs to be done to clarify these mechanisms.
Hemostatic resuscitation employs blood components early in the resuscitation process to
restore both perfusion and normal coagulation function while minimizing crystalloid use.
Lactated Ringer solution and normal saline resuscitation have been shown to increase
reperfusion injury and leukocyte adhesion (252,253,254,255,256,379). As such, standard
crystalloid resuscitation may worsen, presenting acidosis and coagulopathy in severely
injured patients. Several retrospective studies in trauma have shown that survival is
associated with an increased use of clotting factors (352,367). Many other studies have
recommended more aggressive use of clotting factors to treat and correct underlying
coagulopathy (380,381,382,383,384,385,386,387,388).
Although additional prospective studies need to be completed, there seems to be increased
literature supporting early aggressive resuscitation with clotting factors while minimizing
crystalloid use during massive resuscitation. Current military experience has moved to using
thawed plasma as the primary resuscitation fluid in at least a 1:1 or 1:2 ratio with packed
red blood cells (368,387,388,389). Continued resuscitation occurs with a massive transfusion
protocol at a ratio of 6 units of plasma, 6 units of packed red blood cells, 6 units of
platelets, and 10 units of cryoprecipitate. Recombinant factor VIIa is occasionally used
along with early red cell transfusion to promote early hemostasis (368,389).
Massive Transfusion
Definition In the 1970s, massive transfusion was defined as greater than 10 units of blood transfused
in a 24-hour period of time, and survival rates were dismal (6.6%) (390). Over the last two
decades, however, survival rates have improved, and the criteria to define massive
transfusion have evolved (367,383,384,391,392,393,394,395,396). Recent reports use
variable end points, increasing the number of transfusions to greater than 20 units in 24
hours (383) or defining transfusions during the entire hospital stay (392). Most recently, investigators have reported outcomes on patients receiving over 50
units of blood in 48 hours (367).
P.911
Table 58.8 Survival following massive transfusion
No. of Transfusion volume Overall
Study/year patients (avg. units) survival (%)
Page 42 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

Survival As technology and blood banking procedures have improved, patient outcomes following
massive transfusion have also improved (397). Although early survival rates were dismal,
recent reviews report survival rates as high as 60% in patients requiring over 50 units of
blood in the early resuscitation period (Table 58.8). Moreover, many of these patients can
ultimately return to work (75% of survivors), and survival in elderly patients has also been
reported in several studies (367,392,394,395). This dramatic improvement in survival over
the past several decades can be attributed to many factors including an improved
understanding of the consequences of massive resuscitation (268,349,352), improved
technology for massive resuscitation (i.e., rapid transfusion with warmed fluids) (267),
increased use of damage control techniques (353,367), improved trauma systems (343),
improved transfusion practices during resuscitation (367), and improved blood banking
techniques (367). Based on these results, massive transfusion in trauma patients receiving
Wilson et al., 1971 (390) 45 >25 7
Phillips et al., 1987 (383) 56 35 39
Kivioja et al., 1991 (391) 29 56 38
Wudel et al., 1991 (392) 92 33 52
Harvey et al., 1995 (384) 43 19 60
Velmahos et al., 1998 (393) 141 31 31
Cinat et al., 1999 (367) 46 63 45
Hakala et al., 1999 (394) 23 79 69
Vaslef et al., 2002 (395) 44 75 43
Huber-Wagner et al., 2007 (396) 148 41 40
Page 43 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

over 50 units of blood in the acute period following injury is justified, with acceptable
survival and functional capacity following discharge
(367,383,384,391,392,393,394,395,396,397).
Transfusion Protocols Historically, massive transfusion protocols have been developed to assist clinicians in the
resuscitation of hemorrhaging patients. However, a recent review of massive transfusion
protocols globally revealed wide variation in practice (389). Most protocols recommend
empiric strategies of 1 unit of fresh frozen plasma (FFP) for every 4 to 10 units of packed
red blood cells (PRBCs) and 1 plateletpheresis for every 10 to 20 units of PRBCs (380).
Organizational guidelines recommended transfusing to laboratory end points (322).
However, recent literature suggests that a more aggressive approach is warranted
(368,380,387,388). During ongoing hemorrhage, the clinical situation of the patient changes
too rapidly to depend on laboratory values sent 20 to 45 minutes prior. Thus, empiric
strategies to correct or avoid coagulopathy need to be employed. These strategies need to
be modified for two clinical conditions: (a) ongoing hemorrhage and (b) coagulopathy
following hemorrhage control.
Resuscitation during Ongoing Hemorrhage Recent data have established that a significant number of patients have an acute traumatic
coagulopathy on presentation to the emergency department immediately following injury.
Moreover, it appears that traditional strategies for resuscitation have been inadequate and
unable to reverse this coagulopathy early following trauma (387). Several retrospective
clinical studies suggest that aggressive early transfusion of clotting factors (fresh frozen
plasma, platelets, and cryoprecipitate) is associated with increased survival
(352,367,380,385,388).
Randomized prospective controlled trials evaluating therapy for massive hemorrhage are
challenging. However, recently two studies utilizing computer modeling have suggested that
more aggressive resuscitation is necessary to correct coagulopathy. In the first study, the
optimal replacement ratios were 2:3 of FFP to PRBCs and 8:10 of platelets to PRBCs (398).
Interestingly, a second computer model found similar results, suggesting a transfusion rate
of 1:1 for FFP per unit of blood transfused if there is no pre-existing coagulopathy, and a
ratio of 1.5 units of FFP per unit of PRBCs if coagulopathy exists on presentation (399).
Moreover, both of these mathematical models underestimate the potential need for clotting
factor replacement because only dilutional coagulopathy is taken into account; there is no
assessment for the relative contributions of consumption, acidosis, and hypothermia, which
are frequently seen in the acute trauma patient.
Based on these data, old transfusion strategies appear to be fundamentally flawed in the
acutely hemorrhaging patient. Current recommendations suggest that, in patients with
ongoing hemorrhage, empiric transfusion should occur in the ratio of 1:1:1 (1 unit of fresh
Page 44 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

frozen plasma to 1 unit of packed red blood cells to 1 unit of platelets) (Table 58.9)
(368,380,387,388). Since platelets are usually supplied pooled as 6 to 10 units or as a
plateletpheresis, which is equivalent to 6 to 10 units, patients should receive a platelet
transfusion for every 6 to 10 units of PRBCs. When blood products are available, crystalloids
should be avoided in the acutely hemorrhaging patients as they can worsen coagulopathy.
It is important to note that while this is the recommended transfusion protocol for patients
with traumatic injury and hemorrhage, it is unclear if the same blood products and clotting
factors are necessary in nontrauma patients with acute hemorrhage (i.e., intra-operative,
gastrointestinal, ruptured aneurysm) (322,400,401,402,403). In blood loss during elective surgery, the situation is more controlled and resuscitation can be initiated immediately. A
premorbid coagulopathy may or may not exist. Goals in resuscitation in this circumstance
are similar: maintain adequate tissue perfusion to avoid acidosis, correct coagulopathy, and
prevent hypothermia.
Resuscitation Once Hemorrhage Is Controlled Once hemorrhage is controlled, goal-directed transfusion can be pursued based on
laboratory data and clinical variables. Many clinicians will work to achieve normal
coagulation parameters for 24 hours post injury and control of hemorrhage (PT INR <1.5,
platelet count >100 × 109 per liter) (387). In a patient who no longer shows evidence of
medical or surgical bleeding, traditional guidelines for transfusion therapy can be employed
(322). These include using red blood cell transfusion for symptomatic anemia or a
P.912
Table 58.9 Recommended empiric massive transfusion protocol for acute ongoing hemorrhage
CURRENT SUGGESTED PROTOCOL FOR TRAUMATIC HEMORRHAGE
6 units packed red blood cells
6 units of fresh frozen plasma
1 plateletpheresis (or 6–10 units of platelets)
Cryoprecipitate as indicated
TRADITIONAL PROTOCOL–INADEQUATE FOR TRAUMA
10–20 units packed red blood cells
1–4 units fresh frozen plasma
1 plateletpheresis
Cryoprecipitate as indicated
Page 45 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

hemoglobin concentration of less than 7 g/dL; FFP or prothrombin complex concentrate for
a prothrombin time >1.5 times normal; fresh frozen plasma for an activated partial
thromboplastin time >1.5 times normal; cryoprecipitate for a fibrinogen level <80 to 100
mg/dL; and platelet transfusion for a platelet count <50 × 109 per liter (Table 58.6).
Complications of Massive Transfusion Despite acceptable survival rates, there are several known complications to massive
transfusion (Tables 58.10 and 58.11) (397,404,405,406,407,408,409). Physicians caring for
patients who require massive transfusion must anticipate, identify, and rapidly treat these
potential complications in order to optimize outcome.
Disordered hemostasis following massive transfusion is a known complication of massive
blood transfusion (397,400,401). Stored blood is lacking in factors V and VIII. These factors
degrade over time in stored blood, and thus become deficient in the massively transfused
patient. This can contribute to the coagulopathy seen following massive transfusion.
Dilutional thrombocytopenia also occurs during massive transfusion, and is more common
after 1.5 times the normal blood volume is transfused. However, thrombocytopenia can
occur earlier, especially if there is disseminated intravascular coagulation, pre-existing
thrombocytopenia, or a consumptive coagulopathy. As discussed previously, resuscitation of
hemorrhagic shock must include clotting factors and platelets to avoid ongoing
coagulopathy.
Page 46 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

Oxygen delivery to tissues is also affected by blood transfusion. Transfused blood tends to
have a higher affinity for oxygen, thus leading to decreased oxygen delivery to tissues.
Longer storage periods for blood lead to a reduction in red cell deformability, altered red
cell adhesiveness, and other red cell storage lesions. These changes reduce red blood cell
viability after transfusion, reduce tissue oxygen availability, and promote the inflammatory
response, specifically neutrophil priming and pulmonary endothelial cell activation.
Systemic inflammation and potential tissue injury may also be induced by the transfusion of
aged blood. Transfusion of aged blood (>14 days of storage) in the first 6 hours of
resuscitation has been shown to be an independent risk factor for postinjury multiorgan
failure (410) and is associated with delayed apoptosis of neutrophils (411), increased infection rates (412), and a longer ICU
stay (413). This may be particularly significant in large trauma centers and transplantation
centers where older blood is preferentially distributed because of their high-volume use.
Table 58.10 Noninfectious transfusion-associated complications
ACUTE (WITHIN 24 H OF TRANSFUSION)
Hemolytic reactions
Febrile nonhemolytic reactions
Allergic reactions
Transfusion-related acute lung injury (TRALI)
Hypothermia
Hypocalcemia
Hypo- or hyperkalemia
Acid-base derangements
DELAYED (MORE THAN 24 H AFTER TRANSFUSION)
Alloimmunization
Immunosuppression
Posttransfusion purpura
Graft vs. host disease
Multiple organ dysfunction syndrome
P.913
Table 58.11 Infectious transfusion-associated complications
Type of infectious Incidence per all
Page 47 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

Alloimmunization can occur when an immunocompetent host develops an immune response
to donor antigens. The antigens most often involved include the human leukocyte antigen
(HLA) class I and II on platelets and leukocytes, granulocyte-specific antigens, platelet-
specific antigens, and red blood cell–specific antigens. Consequences of alloimmunization
include a refractory response to platelet transfusion, posttransfusion purpura, neonatal
alloimmune thrombocytopenia, acute intravascular hemolytic transfusion reaction,
hemolytic disease in newborns, and febrile nonhemolytic reactions against granulocytes.
Clinical manifestations can be minor, such as fever, leading to active bleeding and
hemolysis, which can be fatal. Workup and treatment vary, depending on the severity of the
reaction (414,415).
Metabolic and electrolyte disturbances can also occur following massive transfusion (397).
complication transfused components
Bacterial contamination (PRBCs + platelets) 1 per 2,000
Hepatitis B transmission 1 per 205,000
PRBC-related bacterial sepsis 1 per 500,000–786,000
Hepatitis A transmission 1 per 1,000,000
Hepatitis C transmission 1 per 1,600,000
HIV transmission 1 per 2,135,000
PRBC, packed red blood cell; HIV, human immunodeficiency virus. Adapted with
data from Silliman CC, Moore EE, Johnson JL, et al. Transfusion of the injured
patient: proceed with caution. Shock. 2004;21(4):291; McIntyre LA, Hebert PC.
Can we safely restrict transfusion in trauma patients? Curr Opin Crit Care.
2006;12:575; Dodd RY, Notari EP, Stramer SL. Current prevalence and incidence
of infectious disease markers and estimated window-period risk in the American
Red Cross donor population. Transfusion. 2002;42:975; and Kleinman S, Chan P,
Robillard P. Risks associated with transfusion of cellular blood components in
Canada. Transfus Med Rev. 2003;17:120.
Page 48 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

Citrate toxicity can occur in patients with abnormal liver function or in whom the
administration of blood is very rapid. The healthy adult liver will metabolize 3 g of citrate
every 5 minutes. Each unit of blood contains approximately 3 g of citrate. Therefore,
transfusion rates higher than 1 unit every 5 minutes can exceed the liver's capacity to
handle this overload. Citrate then binds to calcium and can lead to clinical hypocalcemia.
Patients may exhibit temporary tetany and hypotension. Calcium replacement should occur
concurrently during massive transfusion.
Electrolyte disturbances such as hyperkalemia or hypokalemia can occur with massive
transfusion. The longer the shelf life, the higher the potassium concentration; sometimes
concentrations may even exceed 30 mmol/L. Unless very large amounts of blood are
transfused, hyperkalemia is generally not a problem. On the other hand, as red cells begin
active metabolism, intracellular uptake of potassium begins, and hypokalemia may result.
Acid-base disturbances can also occur with massive blood transfusions. Stored blood
contains lactate at levels up to 30 to 40 mmol/L. In addition, citric acid is present and may
be metabolized to bicarbonate, resulting in severe metabolic alkalosis. Conversely, the
patient's overall condition and tissue hypoperfusion may actually lead to metabolic acidosis.
Although rare, blood transfusion can also result in the induction of acquired inhibitors of
coagulation. The most common antibodies are directed against coagulation factor VIII. This
can result in massive bleeding, which is difficult and costly to treat. The main goals of
treatment are to stop hemorrhage and remove the inhibitor. Factor VIII concentrate is used
only for life-threatening circumstances. Successful elimination of the anti-VIII antibody has
been accomplished with the use of oral immunosuppressants such as cyclophosphamide and
prednisone (416).
Transfusion-related acute lung injury TRALI is a devastating complication of transfusion that consists of a syndrome that includes
dyspnea, hypotension, bilateral pulmonary edema, and fever. Its incidence is reported to be
between 0.04% and 0.06% (or approximately 1 in 2,000). Clinically, it resembles acute
respiratory distress syndrome. Criteria for the diagnosis of TRALI include:
Acute lung injury (ALI) as defined by acute onset, hypoxemia (PaO2: FiO2 ratio ≤300),
bilateral infiltrates on frontal chest radiograph, and no evidence of left atrial
hypertension or circulatory overload
No pre-existing ALI before transfusion
Occurs during or within 6 hours of transfusion
No temporal relationship to an alternative risk factor for ALI (i.e., burns, aspiration,
multiple trauma, cardiopulmonary bypass, sepsis, etc.)
If an additional risk factor exists, then possible TRALI is diagnosed (Table 58.12)
Page 49 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

(417,418,419,420).
The pathogenesis can be either immune (antibody) mediated or nonimmune mediated
(Table 58.13) (418,419,420,421,422). Immune-mediated TRALI is most common and is due
to the presence of leukocyte antibodies in the donor transfusion (421,422). These antibodies
form immune complexes that are deposited in the pulmonary vascular bed, leading to
release of vasoactive substances, leakage of fluid into alveolar spaces, activation of
complement, leukostasis, and activation of polymorphonuclear neutrophils. Immune-
mediated TRALI occurs more commonly with fresh frozen plasma than with platelet
concentrates, is associated with multiparous female donors (423), can occur in healthy
recipients, and is usually severe, requiring mechanical ventilation in 70% of individuals.
Non–immune-mediated TRALI is thought to be due to the presence of biologically active
lipids in the donor transfusion (418,419,420). It occurs with stored platelet concentrates
more commonly than stored red cells, occurs predominantly in critically ill patients with a
primed immune system, and is usually mild and transient, requiring only supplemental
oxygen support. Treatment of TRALI is generally supportive and includes ventilatory and
hemodynamic assistance. There are no data to support the use of corticosteroids, and
additional blood component therapy should be given only if transfusion needs exist. The
diagnosis of TRALI in the patients requiring massive transfusion is difficult because of the many other etiologies also present that can lead to acute lung
injury (424,425).
P.914
Table 58.12 Criteria for transfusion-related acute lung injury (TRALI)
CRITERIA FOR TRALI
Acute lung injury (ALI)
Acute onset
Hypoxemia
PaO2: FiO2 ratio ≤300
SpO2 <90% on room air
No pre-existing ALI before transfusion
Occurs during or within 6 h of transfusion
No temporal relationship to an alternative risk factor for ALI
CRITERIA FOR POSSIBLE TRALI
ALI
No pre-existing ALI before transfusion
Occurs during or within 6 h of transfusion
Page 50 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

Recombinant Factor VIIA in Massive Transfusion and
A clear temporal relationship to an alternative risk factor for ALI
Adapted from Kleinman S, Caulfield T, Chan P, et al. Toward an understanding of
transfusion-related acute lung injury: statement of a consensus panel.
Transfusion. 2004;44:1774.
Table 58.13 Characteristics of immune and nonimmune transfusion-related acute lung injury (TRALI)
Immune TRALI Nonimmune TRALI
Trigger Leukocyte antibodies Biologically active lipids
Blood components
implicated
Fresh frozen plasma >
platelet concentrates
Stored platelet concentrates
> stored red blood cells
Host Healthy or critically ill Predominantly in critically
ill
Clinical course Severe, often life
threatening
Mechanical ventilation
Mild, self-limiting
Supplemental oxygen
Adapted from Bux J. Transfusion-related acute lung injury (TRALI): a serious
adverse event of blood transfusion. Vox Sang. 2005;89:1.
Page 51 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

Hemorrhage New developments in transfusion therapy include the discovery and use of recombinant
coagulation factor VIIa (rFVIIa). Recombinant factor VIIa is a synthesized analog of human
factor VII that has been used effectively in the treatment of patients with hemophilia as
well as other congenital and acquired coagulopathies. Recently, there have been reports of
the successful use of rFVIIa in treating coagulopathic trauma patients (426). In this study,
patients with active hemorrhage and clinical coagulopathy from diverse causes such as
traumatic hemorrhage, traumatic brain injury, warfarin use, congenital factor VII
deficiency, and other acquired hematologic defects were administered rFVIIa as a last
resort. Coagulopathy was reversed in 75% of patients, with an associated decrease in
prothrombin time. Forty-two percent of patients survived to discharge.
Recently, two randomized, prospective, placebo-controlled, double-blind clinical trials
were conducted simultaneously to evaluate the efficacy and safety of recombinant factor
VIIa as adjunctive therapy for the control of bleeding in patients with severe blunt (N = 143)
or penetrating (N = 134) trauma (427). In blunt trauma, the red blood cell transfusion
requirement was significantly reduced by 2.6 units (p = 0.02) and the need for massive
transfusion (>20 units of packed red blood cells) was reduced (14% vs. 33%, p = 0.03). In
patients with penetrating trauma, the trends were similar, but not significant (reduction in
red cell transfusion 1.0 unit, p = 0.10; massive transfusion 7% vs. 19%, p = 0.08). Trends
toward reduction in mortality and critical complications were also observed. A subgroup
analysis from this trial found particular benefit in those patients who were coagulopathic on
presentation to the emergency department, with a significant decrease in transfusion of
packed red blood cells, fresh frozen plasma, platelets, and need for massive transfusion. In
addition, treatment with rFVIIa was also associated with a significant reduction in
multiorgan failure and/or acute respiratory distress syndrome (3% vs. 20%, p = 0.004),
without an increase in thromboembolic events (428).
Recombinant factor VIIa, however, must be used responsibly. Recent studies have shown
that early administration following trauma is more effective than late administration
(429,430). Furthermore, the presence of profound acidosis, coagulopathy, and signs of
irreversible hemorrhagic shock predict failure of rFVIIa therapy (431). Current
recommendations suggest that optimal preconditions should be present prior to
administration of rFVIIa, which include a fibrinogen concentration of >50 mg/dL, a platelet
count of >50 × 109 per liter, and a pH ≥7.2 (432,433). Although early results in traumatic
hemorrhage appear promising, rFVIIa should still be considered experimental and further
investigation is warranted. Recombinant factor VIIa has shown promise for perioperative
bleeding during liver transplantation (434) and in patients undergoing cardiac surgery
(435,436). Investigations for its utility in perioperative bleeding for other surgical
procedures have been mixed (437,438,439,440,441,442).
A prospective randomized trial investigating the use of rFVIIa in patients with cirrhosis and
upper gastrointestinal bleeding who were treated with standard endoscopic therapy and
Page 52 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

pharmacologic interventions showed that the administration of rFVIIa was not more
effective than placebo with respect to the primary end point of failure to control bleeding
within 24 hours and failure to prevent rebleeding or death within 5 days (443). However,
subgroup analysis of patients with more severe cirrhosis showed that rFVIIa showed a
reduction in the composite primary end point (8% vs. 23%, p = 0.03). None of the rFVIIa
patients had rebleeding within the first 24 hours, whereas rebleeding occurred in 11% of the
placebo group (p = 0.01) (443).
As with any hemostatic agent, there are concerns over the potential thrombogenicity of
rFVIIa (444). Although preliminary evidence shows a favorable safety profile (445,446),
thrombogenic effects are being followed closely in ongoing clinical trials.
Prevention of Hemorrhagic Shock
Antifibrinolytic Therapy Antifibrinolytic therapy has been shown to significantly reduce the risk of bleeding following
cardiac surgery in several randomized controlled trials. Aprotinin has been studied most extensively
(447,448,449,450,451), followed by tranexamic acid, then aminocaproic acid. However,
recent information raises concern for the risk of renal failure following use of aprotinin with
cardiac surgery (448,449) and a potential for increased mortality at 5 years following use of
aprotinin (450). Although clearly the risk of postoperative bleeding following cardiac surgery
is reduced, further investigation into these potential side effects is warranted.
A recent systematic review of randomized controlled trials of antifibrinolytic agents (mainly
aprotinin or tranexamic acid) in elective surgical procedures identified 89 trials including
8,580 randomized patients (74 cardiac, eight orthopedic, four liver, three vascular). Results
demonstrated that these treatments reduced the number of patients needing transfusion by
one third, reduced the volume needed per patient by 1 unit, and halved the need for
further surgery to control bleeding. These differences were all statistically significant.
There was also a trend toward a reduction in the risk of death (risk ratio = 0.85; 95%
confidence interval, 0.63–1.14), although this was not statistically significant (452).
To date, there are limited data on the use of antifibrinolytic agents in other clinical
scenarios (453). However, at this time, the CRASH-2 trial (Clinical Randomization of an Anti-
fibrinolytic in Significant Hemorrhage) is ongoing in Europe and is designed to evaluate the
utility of antifibrinolytic agents in the management of acute traumatic injury (454).
Experimental Therapy
Red Cell Substitutes Although the blood supply in the United States is safe and currently has sufficient capacity
to meet most patient needs, there is room for considerable improvement. The current
P.915
Page 53 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

system is dependent on blood donors on a regular basis, and the blood supply is subject to
seasonal shortages due to holidays and convenience. The gap between the donor pool and
the increasing transfusion requirements of an aging population is narrowing, and shortages
are becoming more frequent. The risk of transmission of known infectious diseases still
exists (Table 58.11), while the threat of new and emerging infections such as West Nile
virus and Creutzfeldt-Jakob disease underscore the risk of a tainted blood supply (455).
The ideal red cell substitute should have several characteristics including an ability to
deliver (and potentially enhance) oxygen delivery, no risk of disease transmission, no
immunosuppressive effects, available in abundant supply, universally compatible, prolonged
shelf life, similar in vivo half-life to the red blood cell, available at a reasonable cost, easy
to administer, able to access all areas of the human body (including ischemic tissues), and
effective at room air or ambient conditions (455,456,457). There have been many attempts
to develop red cell substitutes since 1934 when Amberson first reported the successful use
of a bovine hemolysate for exchange transfusions in cats and dogs (455). However, this work
could not be replicated.
The two main types of oxygen carriers that are used as red blood cell substitutes are
hemoglobin-based oxygen carriers (HBOCs) and perfluorocarbons (PFCs). Based on previous
clinical trials, many obstacles still need to be overcome. Adverse effects associated with
HBOCs include (a) severe vasoconstriction due to binding of nitric oxide and dysregulation of
endothelin; (b) nephrotoxicity; (c) interference of macrophage function; (d) antigenicity;
(e) oxidation on storage; (f) activation of complement, kinin, and coagulation; (g) iron
deposition with concerns of hemochromatosis and iron overload; (h) gastrointestinal
distress; (i) neurotoxicity; (j) free radical generation; and (k) interference with diagnosis of
transfusion reaction. Adverse effects of PFCs include (a) limited shelf life, (b) flulike
symptoms during infusion, (d) complement and phagocytic activation, and (d) short
circulation time (456).
Despite much research, no product to date has been able to fulfill all of the previously
mentioned criteria or meet the U.S. Food and Drug Administration's requirements of purity,
potency, and safety. At the time of this publication, three HBOC products continue in
advanced clinical trials (455).
Hypertonic Saline Hypertonic saline (7.5% saline ± 6% dextan-70) has been investigated as an alternative
resuscitation strategy in critically injured patients (458,459,460,461,462,463,464).
Hypertonic resuscitation evokes an increase in serum osmolarity, which results in the
redistribution of fluid from the interstitial and intracellular space to the intravascular
space. This leads to a rapid restoration of circulating intravascular volume with a small
amount resuscitation fluid. Hypertonic saline has also been shown to decrease intracranial
pressure via its osmotic effects (125,126). This is particularly beneficial in patients with
hypovolemic shock and closed head injury due to the ability of hypertonic saline
Page 54 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

resuscitation to concurrently restore circulating blood volume, improve tissue (including
cerebral) perfusion, and lower intracranial pressure (126,465,466).
Hypertonic saline resuscitation has also been shown to have significant immunomodulatory
effects that could mitigate the dysfunctional inflammatory response seen after traumatic
injury (108,109,111,150,253,467,468,469,470,471,472). The hypertonicity associated with
hypertonic saline resuscitation is associated with significant effects on the innate and
adaptive immune systems. There is suppression of the neutrophil oxidative burst,
potentially leading to an attenuation of inflammatory organ injury (150,473).
Several clinical trials and meta-analyses have suggested improved outcome in patients
resuscitated with hypertonic saline (474,475,476,477). Despite these results, hypertonic
saline resuscitation has not gained widespread acceptance in North America. However, in
1999, the U.S. Navy, through the Office of Naval Research, requested that the Institute of
Medicine (IOM) recommend that hypertonic saline be used as the initial resuscitation fluid
for combat casualty (256,478). The rapid restoration of intravascular volume and possible
immunomodulatory effects associated with hypertonic saline resuscitation make it an
attractive alternative for the resuscitation of severe hemorrhagic shock. However, it is still
considered experimental and prospective randomized trials are needed to confirm its
utility.
Summary Hemorrhagic shock is a common, yet complicated, clinical condition that physicians are
frequently called upon to evaluate and treat. Diagnosis must be accurate and expedient.
Therapy must be direct, efficient, and multifactorial in order to avoid the potential multisystem sequelae. Metabolism and function of all organs are altered
during hemorrhagic shock. A better understanding of the pathophysiology of hemorrhagic
shock has led to improved resuscitation techniques and improved survival over recent years.
Damage control laparotomy and damage control resuscitation have changed the approach to
management in patients with multisystem trauma and hemorrhagic shock. Staged
resuscitation and operative intervention to avoid irreversible shock are now the mainstays
of care. Recognition of acute traumatic coagulopathy has improved the composition of
massive transfusion protocols to include increased use of clotting factors early during
resuscitation. New experimental therapies for resuscitation are being evaluated and appear
promising. Overall, survival following hemorrhagic shock has improved. Early diagnosis,
definitive cessation of bleeding, and comprehensive hemostatic resuscitation are the key
elements to successful outcome.
References
1. Weil MH, Shubin H. Proposed reclassification of shock states with special reference
to distributive effects. In: Hinshaw LB, Cox BG, eds. The Fundamental Mechanisms of
P.916
Page 55 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

Shock. New York: Plenum Press; 1972:13.
2. Hamilton-Davies C, Mythen MG, Salmon JB, et al. Comparison of commonly used
clinical indicators of hypovolaemia with gastrointestinal tonometry. Intens Care Med.
1997;23(3):276.
3. Bond RF, Johnson G III. Vascular adrenergic interactions during hemorrhagic shock.
Fed Proc. 1985;44:281.
4. Schadt JC, Ludbrook J. Hemodynamic and neurohumoral responses to acute
hypovolemia in conscious mammals. Am J Physiol. 1991;260:H305.
5. Koyama S, Sawano F, Matsuda Y, et al. Spatial and temporal differing control of
sympathetic activities during hemorrhage. Am J Physiol. 1992;262:R579.
6. Wisbach G, Tobias S, Woodman R, et al. Preserving cardiac output with beta-
adrenergic receptor blockade and inhibiting the Bezold-Jarisch reflex during
resuscitation from hemorrhage. J Trauma. 2007;63(1):26.
7. Victorino GP, Battistella FD, Wisner DH. Does tachycardia correlate with hypotension
after trauma? J Am Coll Surg. 2003;196(5):679.
8. Demetriades D, Chan LS, Bhasin P, et al. Relative bradycardia in patients with
traumatic hypotension. J Trauma. 1998;45:534.
9. Sander-Jensen K, Secher NH, Bie P, et al. Vagal slowing of the heart during
hemorrhage: observations from 20 consecutive hypotensive patients. Br J Med.
1986;292:364.
10. Vincent JL, Moraine JJ, Van der Linden P. Toe temperature versus transcutaneous
oxygen tension monitoring during acute circulatory failure. Intensive Care Med.
1988;14:64.
11. Van Leeuwen AF, Evans RG, Ludbrook J. Haemodynamic responses to acute blood
loss: new roles for the heart, brain, and endogenous opioids. Anaesth Intensive Care.
1989;17(3):312.
Page 56 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

12. Ludbrook J, Ventura S. Roles of carotid baroreceptor and cardiac afferents in
hemodynamic responses to acute central hypovolemia. Am J Physiol. 1996;270(5 Part
2):H1538.
13. Wong DH, O'Connor D, Tremper KK, et al. Changes in cardiac output after acute
blood loss and position change in man. Crit Care Med. 1989;17(10):979.
14. Bressack MA, Raffin TA. Importance of venous return, venous resistance, and mean
circulatory pressure in the physiology and management of shock. Chest. 1987;92:906.
15. Shen YT, Knight DR, Thomas JX Jr, et al. Relative roles of cardiac receptors and
arterial baroreceptors during hemorrhage in conscious dogs. Circ Res. 1990;66(2):397.
16. Westphal G, Garrido Adel P, de Almeida DP, et al. Pulse pressure respiratory
variation as an early marker of cardiac output fall in experimental hemorrhagic shock.
Artif Organs. 2007;31(4):284.
17. Magder S, Lagonidis D, Erice F. The use of respiratory variations in right atrial
pressure to predict the cardiac output response to PEEP. J Crit Care. 2001;16(3):108–
114.
18. Rooke GA, Schwid HA, Shapira Y. The effect of graded hemorrhage and
intravascular volume replacement on systolic pressure variation in humans during
mechanical and spontaneous ventilation. Anesth Analg. 1995;80(5):925.
19. Zweifach BW, Fronek A. The interplay of central and peripheral factors in
irreversible hemorrhagic shock. Prog Cardiovasc Dis. 1975;18(2):147.
20. Schwartz S, Frantz RA, Shoemaker WC. Sequential hemodynamic and oxygen
transport responses in hypovolemia, anemia, and hypoxia. Am J Physiol. 1981;241
(6):H864.
21. Alyono D, Ring WS, Chao RY, et al. Characteristics of ventricular function in severe
hemorrhagic shock. Surgery. 1983;94(2):250.
22. Sarnoff SJ, Case RB, Waithe PE, et al. Insufficient coronary flow and myocardial
Page 57 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

failure as a complication factor in late hemorrhagic shock. Am J Physiol. 1954;176
(3):439.
23. Rush BF Jr. Irreversibility in the post-transfusion phase of hemorrhagic shock. Adv
Exp Med Biol. 1971;23:215.
24. Secher NH, Sander-Jensen K, Werner C, et al. Bradycardia during severe but
reversible hypovolemic shock in man. Circ Shock. 1984;14:267.
25. Thiemermann C, Szabo C, Mitchell JA, et al. Vascular hyporeactivity to
vasoconstrictor agents and hemodynamic decompensation in hemorrhagic shock is
medicated by nitric oxide. Proc Natl Acad Sci. 1993;90:267.
26. Vatner SF. Effects of hemorrhage on regional blood flow distribution in dogs and
primates. J Clin Invest. 1974;54:225.
27. Shoemaker WC. Relation of oxygen transport patterns to the pathophysiology and
therapy of shock states. Intensive Care Med. 1987;13(4):230.
28. Aubier M, Viires N, Syllie G, et al. Respiratory muscle contribution to lactic acidosis
in low cardiac output. Am Rev Respir Dis. 1982;126(4):648.
29. Revelly JP, Gardaz JP, Nussberger J, et al. Effect of epinephrine on oxygen
consumption and delivery during progressive hemorrhage. Crit Care Med. 1995;23
(7):1272.
30. Hannon JP, Wade CE, Bossone CA, et al. Oxygen delivery and demand in conscious
pigs subjected to fixed-volume hemorrhage and resuscitated with 7.5% NaCl in 6%
Dextran. Circ Shock. 1989;29(3):205.
31. Edouard AR, Degremont AC, Duranteau J, et al. Heterogeneous regional vascular
responses to simulated transient hypovolemia in man. Intensive Care Med. 1994;20
(6):414.
32. Groeneveld AB, Kolkman JJ. Splanchnic tonometry: a review of physiology,
methodology, and clinical implications. J Crit Care. 1994;9(3):198.
Page 58 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

33. Kirton OC, Windsor J, Wedderburn R, et al. Failure of splanchnic resuscitation in
the acutely injury trauma patient correlates with multiple organ failure and length of
stay in the ICU. Chest. 1998;113:1064.
34. Riggs TE, Shafer AW, Guenter CA. Acute changes in oxyhemoglobin affinity: effects
on oxygen transport and utilization. J Clin Invest. 1973;52:2660.
35. Malmberg PO, Hlastala MP, Woodson RD. Effect of increased blood-oxygen affinity
on oxygen transport in hemorrhagic shock. J Appl Physiol. 1979;47(4):889.
36. Woodson RD. Physiologic significance of oxygen dissociation curve shifts. Crit Care
Med. 1979;7(9):368.
37. Woodson RD. Functional consequences of altered blood oxygen affinity. Acta Biol
Med Ger. 1981;40:733.
38. Myburgh JA, Webb RK, Worthley LI. The P50 is reduced in critically ill patients.
Intensive Care Med. 1991;17(6):355.
39. Herman CM, Rodkey FL, Valeri CR, et al. Changes in the oxyhemoglobin dissociation
curve and peripheral blood after acute red cell mass depletion and subsequent red cell
mass restoration in baboons. Ann Surg. 1971;174:734.
40. Sauaia A, Moore FA, Moore EE, et al. Early predictors of postinjury multiple organ
failure. Arch Surg. 1994;129(1):39.
41. Shoemaker WC, Appel PL, Kram HB. Role of oxygen debt in the development of
organ failure sepsis, and death in high-risk surgical patients. Chest. 1992;102(1):208.
42. Abou-Khalil B, Scalea TM, Trooskin SZ, et al. Hemodynamic responses to shock in
young trauma patients: need for invasive monitoring. Crit Care Med. 1994;22(4):633.
43. Shoemaker WC, Appel PL, Kram HB, et al. Prospective trial of supranormal values
of survivors as the therapeutic goals in high-risk surgical patients. Chest. 1988;94:1176–
1186.
Page 59 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

44. Bishop MH, Shoemaker WC, Appel PL, et al. Prospective randomized trial of
survivor values of cardiac index, oxygen delivery, and oxygen consumption as
resuscitation endpoints in severe trauma. J Trauma. 1995;38(5):780.
45. Shoemaker WC, Appel PL, Kram HB. Measurement of tissue perfusion by oxygen
transport patterns in experimental shock and in high-risk surgical patients. Intensive
Care Med. 1990;16(Suppl 2):S135.
46. Chang MC, Mondy JS, Meredith JW, et al. Redefining cardiovascular performance
during resuscitation: ventricular stroke work, power, and the pressure-volume diagram.
J Trauma. 1998;45(3):470.
47. Velmahos GC, Demetriades D, Shoemaker WC, et al. Endpoints of resuscitation of
critically injured patients: normal or supranormal? A prospective randomized trial. Ann
Surg. 2000;232(3):409.
48. Kern JW, Shoemaker WC. Meta-analysis of hemodynamic optimization in high-risk
patients. Crit Care Med. 2002;30(8):1686.
49. Yu M, Levy MM, Smith P, et al. Effect of maximizing oxygen delivery on morbidity
and mortality rates in critically ill patients: a prospective, randomized, controlled
study. Crit Care Med. 1993;21(6):830.
50. Balogh Z, McKinley BA, Cocanour CS, et al. Supranormal trauma resuscitation
causes more cases of abdominal compartment syndrome. Arch Surg. 2003;138:637.
51. Chaudry IH. Cellular mechanisms in shock and ischemia and their correction. Am J
Physiol. 1983;245(2):R117.
52. Mongan PD, Fontana JL, Chen R, et al. Intravenous pyruvate prolongs survival
during hemorrhagic shock in swine. Am J Physiol. 1999;277(6 Part 2):H2253.
53. Amundson B, Jennische E, Haljamae H. Correlative analysis of microcirculatory and
cellular metabolic events in skeletal muscle during hemorrhagic shock. Acta Physiol
Scand. 1980;108(2):147.
P.917
Page 60 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

54. Ratcliffe PJ, Moonen CT. Holloway PA, et al. Acute renal failure in hemorrhagic
hypotension: cellular energetics and renal function. Kidney Int. 1986;30(3):355.
55. Zager RA. Adenine nucleotide changes in kidney, liver, and small intestine during
different forms of ischemic injury. Circ Res. 1991;68(1):185.
56. Pellicane JV, DeMaria EJ, Abd-Elfattah A, et al. Interleukin-1 receptor antagonist
improves survival and preserves organ adenosine-5-triphosphate after hemorrhagic
shock. Surgery. 1993;114(2):278.
57. Salzman AL, Vromen A, Denenberg A, et al. K(ATP)-channel inhibition improves
hemodynamics and cellular energetics in hemorrhagic shock. Am J Physiol. 1997;272(2
Part 2):H688.
58. Robinson DA, Wang P, Chaudry IH. Administration of ATP-MgCl2 after trauma-
hemorrhage and resuscitation restores the depressed cardiac performance. J Surg Res.
1997;69(1):159.
59. Kline JA, Maiorano PC, Schroeder JD, et al. Activation of pyruvate dehydrogenase
improves heart function and metabolism after hemorrhagic shock. J Mol Cell Cardiol.
1997;29(9):2465.
60. Mizock BA, Falk JL. Lactic acidosis in critical illness. Crit Care Med. 1992;20(1):80.
61. Nakatani T, Sakamoto Y, Ando H, et al. Bile and bilirubin excretion in relation to
hepatic energy status during hemorrhagic shock and hypoxemia in rabbits. J Trauma.
1995;39(4):665.
62. Sjoberg F, Gustafsson U, Lewis DH. Extracellular muscle surface pO2 and pH
heterogeneity during hypovolemia and after reperfusion. Circ Shock. 1991;34(3):319.
63. Davis JM, Stevens JM, Peitzman A, et al. Neutrophil migratory activity in severe
hemorrhagic shock. Circ Shock. 1983;10(3):199.
64. Sayeed MM. Ion transport in circulatory and/or septic shock. Am J Physiol. 1987;252
(5 Part 2):R809.
Page 61 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

65. Horton JW. Calcium-channel blockade in canine hemorrhagic shock. Am J Physiol.
1989;257(5 Part 2):R1012.
66. Eastridge BJ, Darlington DN, Evans JA, et al. A circulating shock protein depolarizes
cells in hemorrhage and sepsis. Ann Surg. 1994;219(3):298.
67. Kiang JG. Inducible heat shock protein 70kD and inducible nitric oxide synthase in
hemorrhage/resuscitation-induced injury. Cell Res. 2004;14(6):450.
68. Menezes JM, Hierholzer C, Watkins SC, et al. The modulation of hepatic injury and
heat shock expression by inhibition of inducible nitric oxide synthase after hemorrhagic
shock. Shock. 2002;17(1):13.
69. DeMaio A. Heat shock proteins: facts, thoughts, and dreams. Shock. 1999;11(1):1.
70. Kregel KC. Heat shock proteins: modifying factors in physiological stress responses
and acquired thermotolerance. J Appl Physiol. 2002;92:2177.
71. DeMaio A. The heat-shock response. New Horizons. 1995;3(2):198.
72. Zhao Q, Zhao KS. Inhibition of L-type calcium channels in arteriolar smooth muscle
cells is involved in the pathogenesis of vascular hyporeactivity in severe shock. Shock.
2007; accepted for print.
73. Carlson DE, Nguyen PX, Soane L, et al. Hypotensive hemorrhage increases calcium
uptake capacity and Bcl-XL content of liver mitochondria. Shock. 2007;27(2):192.
74. Zhao K, Liu J, Jin C. The role of membrane potential and calcium kinetic changes in
the pathogenesis of vascular hyporeactivity during severe shock. Chin Med J.
2000;113:59.
75. Maitra SR, Geller ER, Pan W, et al. Altered cellular calcium regulation and hepatic
glucose production during hemorrhagic shock. Circ Shock. 1992;38(1):14.
76. Xu J, Liu L. The role of calcium desensitization in vascular hyporeactivity and its
Page 62 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

regulation after hemorrhagic shock in the rat. Shock. 2005;23(6):576.
77. Yang G, Liu L, Xu J, et al. Effect of arginine vasopressin on vascular reactivity and
calcium sensitivity after hemorrhagic shock in rats and its relationship to Rho-kinase. J
Trauma. 2006;61(6):1336.
78. Silomon M, Rose S. Effect of sodium bicarbonate infusion on hepatocyte Ca2+
overload during resuscitation from hemorrhagic shock. Resuscitation. 1998;37(1):27.
79. Silomon M, Pizanis A, Larsen R, et al. Pentoxyfilline prevention of altered
hepatocyte calcium regulation during hemorrhagic shock/resuscitation. Crit Care Med.
1998;26(3):494.
80. Zhong Z, Enomoto N, Connor HD, et al. Glycine improves survival after hemorrhagic
shock. Shock. 1999;12(1):54.
81. Wang G, Zhao M, Wang EH. Effects of glycine and methylprednisolone on
hemorrhagic shock in rats. Chin Med J. 2004;117(9):1334.
82. Jarrar D, Chaudry IH, Wang P. Organ dysfunction following hemorrhage and sepsis:
mechanisms and therapeutic approaches (review). Int J Mol Med. 1999;4(6):575.
83. Lieberthal W, McGarry AE, Sheils J, et al. Nitric oxide inhibition in rats improves
blood pressure and renal function in hypovolemic shock. Am J Physiol. 1991;261(5 Part
2):F868.
84. Szabo C, Farago M, Horvath I, et al. Hemorrhagic hypotension impairs endothelium-
dependent relaxations in the renal artery of the cat. Circ Shock. 1992;36(3):238.
85. Dignan RJ, Wechsler AS, DeMaria EJ. Coronary vasomotor dysfunction following
hemorrhagic shock. J Surg Res. 1992;52(4):382.
86. Bitterman H, Brod V, Weisz G, et al. Effects of oxygen on regional hemodynamics in
hemorrhagic shock. Am J Physiol. 1996;271(1 Part 2):H203.
87. Szabo C, Csaki C, Benyo Z, et al. Role of L-arginine-nitric oxide pathway in the
changes in cerebrovascular reactivity following hemorrhagic hypotension and
Page 63 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

retransfusion. Circ Shock. 1992;37(4):307.
88. Guarini S, Bini A, Bazzani C, et al. Adrenocorticotropin normalizes the blood levels
of nitric oxide in hemorrhage-shocked rats. Eur J Pharmacol. 1997;336(1):15.
89. Pannen BH, Kohler N, Hole B, et al. Protective role of endogenous carbon monoxide
in hepatic microcirculatory dysfunction after hemorrhagic shock in rats. J Clin Invest.
1998;102(6):1220.
90. Szabo C, Billiar TR. Novel roles of nitric oxide in hemorrhagic shock. Shock. 1999;12
(1):1.
91. Kiang JG, Bowman PD, Lu X, et al. Geldanamycin inhibits hemorrhage-induced
increases in caspase-3 activity: role of inducible nitric oxide synthase. J Appl Physiol.
2007;103:1045.
92. Ng KC, Moochhala SM, Md S, et al. Preservation of neurological functions by nitric
oxide synthase inhibitors following hemorrhagic shock. Neuropharmacology. 2003;44
(2):244.
93. Hierbolzer C, Billiar TR, Tweardy DJ, et al. Reduced hepatic transcription factor
activation and expression of IL-6 and ICAM-1 after hemorrhage by NO scavenging. Arch
Orthop Trauma Surg. 2003;123(2–3):55.
94. Hierbolzer C, Menezes JM, Ungeheuer A, et al. A nitric oxide scavenger against
pulmonary inflammation following hemorrhagic shock. Shock. 2002;17(2):98.
95. Kobara M, Tatsumi T, Takeda M, et al. The dual effects of nitric oxide synthase
inhibitors on ischemia-reperfusion injury in rat hearts. Basic Res Cardiol. 2003;98
(5):319.
96. Adachi T, Hori S, Miyazaki K, et al. Inhibition of nitric oxide synthesis aggravates
myocardial ischemia in hemorrhagic shock in constant pressure model. Shock. 1998;9
(3):204.
97. Thompson A, Valeri CR, Lieberthal W. Endothelin receptor A blockade alters
hemodynamic response to nitric oxide inhibition in rats. Am J Physiol. 1995;269(2 Part
Page 64 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

2):H743.
98. Rothe CF, Drees JA. Vascular capacitance and fluid shifts in dogs during prolonged
hemorrhagic hypotension. Circ Res. 1976;38(5):347.
99. Schlichtig R, Kramer DJ, Pinsky MR. Flow redistribution during progressive hemorrhage is a determinant of critical O2 delivery. J Appl Physiol. 1991;70(1):169.
100. Chien S. Role of the sympathetic nervous system in hemorrhage. Physiol Rev.
1967;47(2):214.
101. Forsyth RP, Hoffbrand BI, Melmon KL. Redistribution of cardiac output during
hemorrhage in the unanesthetized monkey. Circ Res. 1970;27(3):311.
102. Rothe CF, Drees JA. Vascular capacitance and fluid shifts in dogs during prolonged
hemorrhagic hypotension. Circ Res. 1976;38(5):347.
103. Zweifach BW. Mechanisms of blood flow and fluid exchange in microvessels:
hemorrhagic hypotension model. Anesthesiology. 1974;41(2):157.
104. Prist R, Rocha-e-Silva M, Scalabrini A, et al. A quantitative analysis of
transcapillary refill in severe hemorrhagic hypotension in dogs. Shock. 1994;1(3):188.
105. Childs EW, Udobi KF, Hunter FA, et al. Evidence of transcellular albumin transport
after hemorrhagic shock. Shock. 2005;23(6):565.
106. Schumacher J, Binkowski K, Dendorfer A, et al. Organ-specific extravasation of
albumin-bound Evans blue during non-resuscitated hemorrhagic shock in rats. Shock.
2003;20(6):565.
107. Boyd AJ, Rubin BB, Walker PM, et al. A CD18 monoclonal antibody reduces
multiple organ injury in a model of ruptured abdominal aortic aneurysm. Am J Physiol.
1999;277(1 Part 2):H172.
108. Pascual JL, Ferri LE, Seely AJ, et al. Hypertonic saline resuscitation of
hemorrhagic shock diminishes neutrophil rolling and adherence to endothelium and
Page 65 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

reduces in vivo vascular leakage. Ann Surg. 2002;236(5):634.
109. Corso CO, Okamoto S, Ruttinger D, et al. Hypertonic saline dextran attenuates
leukocyte accumulation in the liver after hemorrhagic shock and resuscitation. J
Trauma. 1999;46(3):417.
110. Childs EW, Udobi KF, Wood JG, et al. In vivo visualization of reactive oxidants and
leukocyte-endothelial adherence following hemorrhagic shock. Shock. 2002;18(5):423.
111. Yada-Langui MM, Anjos-Valotta EA, Sannomiya P, et al. Resuscitation affects
microcirculatory polymorphonuclear leukocyte behavior after hemorrhagic shock: role
of hypertonic saline and pentoxyfilline. Exp Biol Med (Maywood). 2004;229(7):684.
112. Childs EW, Udobi KF, Wood JG, et al. In vivo visualization of reactive oxidants and
leukocyte-endothelial adherence following hemorrhagic shock. Shock. 2002;18(5):423.
113. Botha AJ, Moore FA, Moore EE, et al. Early neutrophil sequestration after injury: a
pathogenic mechanism for multiple organ failure. J Trauma. 1995;39(3):411.
114. Barroso-Aranda J, Schmid-Schonbein GW, Zweifach BW, et al. Granulocytes and
no-reflow phenomenon in irreversible hemorrhagic shock. Circ Res. 1988;63(2):437.
115. Connolly HV, Maginniss LA, Schumacker PT. Transit time heterogeneity in canine
small intestine: significance for oxygen transport. J Clin Invest. 1997;99(2):228.
116. Douglas RG, Shaw JHF. Metabolic response to sepsis and trauma. Br J Surg.
1989;76:115.
117. Pearce FJ, Connett RJ, Drucker WR. Extracellular-intracellular lactate gradients in
skeletal muscle during hemorrhagic shock in the rat. Surgery. 1985;98:625.
118. Alibegovic A, Ljungqvist O. Pretreatment with glucose infusion prevents fatal
outcome after hemorrhage in food-deprived rats. Circ Shock. 1993;39:1.
119. Barton R, Cerra FB. The hypermetabolism of multiple organ failure syndrome.
Chest. 1989;96:1153.
P.918
Page 66 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

120. Miyazaki K, Hori S, Inoue S, et al. Characterization of energy metabolism and
blood flow distribution in myocardial ischemia in hemorrhagic shock. Am J Physiol.
1997;273(2 Pt 2):H600.
121. Paulson OB, Strandgaard S, Edvinsson L. Cerebral autoregulation. Cerebrovasc
Brain Metab Rev. 1990;2:161.
122. Harper AM. Autoregulation of cerebral blood flow: influence of the arterial blood
pressure on the blood flow through the cerebral cortex. J Neurol Neurosurg Psychiatry.
1966;29:398.
123. Meybohm P, Cavus E, Bein B, et al. Cerebral metabolism assessed with
microdialysis in uncontrolled hemorrhagic shock after penetrating liver trauma. Anesth
Analg. 2006;103(4):948.
124. Meybohm P, Renner J, Boening A, et al. Impact of norepinephrine and fluid on
cerebral oxygenation in experimental hemorrhagic shock. Pediatr Res. 2007;62(4):1.
125. Filho JA, Machado MA, Nani RS, et al. Hypertonic saline solution increases cerebral
perfusion pressure during clinical orthotopic liver transplantation for fulminant hepatic
failure: preliminary results. Clinics. 2006;61(3):231.
126. Pinto FC, Capone-Neto A, Prist R, et al. Volume replacement with lactated
Ringer's or 3% hypertonic saline solution during combined experimental hemorrhagic
shock and traumatic brain injury. J Trauma. 2006;60(4):758.
127. Steenblock U, Mannhart H, Wolff G. Effect of hemorrhagic shock on
intrapulmonary right-to-left shunt (QS/QT) and dead space (VD/VT). Respiration.
1976;33(2):133.
128. Adrogue HJ, Rashad MN, Gorin AB, et al. Arteriovenous acid-base disparity in
circulatory failure: studies on mechanism. Am J Physiol. 1989;257(6 Pt 2):F1087.
129. Pretorius JP, Schlag G, Redl H, et al. The “lung in shock” as a result of
hypovolemic-traumatic shock in baboons. J Trauma. 1987;27(12):1344.
Page 67 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

130. Garber BG, Hebert PC, Yelle JD, et al. Adult respiratory distress syndrome: a
systemic overview of incidence and risk factors. Crit Care Med. 1996;24(4):687.
131. Pallister I, Dent C, Topley N. Increased neutrophil migratory activity after major
trauma: a factor in the etiology of acute respiratory distress syndrome? Crit Care Med.
2002;30(8):1717.
132. Pallister I, Gosling P, Alpar K, et al. Prediction of post-traumatic adult respiratory
distress syndrome by albumin excretion rate eight hours after admission. J Trauma.
1997;42(6):1056.
133. Wardle EN. Acute renal failure and multiorgan failure. Nephron. 1994;66(4):380.
134. Myers BD, Moran SM. Hemodynamically mediated acute renal failure. N Engl J
Med. 1986;314(2):97.
135. Brenner BM. Hemodynamically mediated glomerular injury and the progressive
nature of kidney disease. Kidney Int. 1983;23(4):647.
136. Toung T, Reilly PM, Fuh KC, et al. Mesenteric vasoconstriction in response to
hemorrhagic shock. Shock. 2000;13(4):267.
137. Reilly PM, Bulkly GB. Vasoactive mediators and splanchnic perfusion. Crit Care
Med. 1993;21(2 Suppl):S55.
138. Yilmaz EN, Vahl AC, van Rij GL, et al. The renin-angiotensin system in swine
during hypovolaemic shock combined with low-flow ischaemia of the sigmoid colon.
Cardiovasc Surg. 1999;7(5):539.
139. Reilly PM, Wilkins KB, Fuh KC, et al. The mesenteric hemodynamic response to
circulatory shock: an overview. Shock. 2001;15(5):329.
140. Fusamoto H, Hagiwara H, Meren H, et al. A clinical study of acute gastrointestinal
hemorrhage associated with various shock states. Am J Gastroenterol. 1991;86(4):429.
141. Schuster DP, Rowley H, Feinstein S, et al. Prospective evaluation of the risk of
Page 68 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

upper gastrointestinal bleeding after admission to a medical intensive care unit. Am J
Med. 1984;76(4):623.
142. Van Leeuwen PAM, Boermeester MA, Houdijk APJ, et al. Clinical significance of
translocation. Gut. 1994;35 (Suppl 1):S28.
143. Berg RD. Bacterial translocation from the gastrointestinal tract. Adv Exp Med Biol.
1999;473:11.
144. Haglund U. Systemic mediators released from the gut in critical illness. Crit Care
Med. 1993;21(Suppl 2):S15.
145. Fiddian-Green RG. Associations between intramucosal acidosis in the gut and
organ failure. Crit Care Med. 1993;21(Suppl 2):S103.
146. Hameed SM, Cohn SM. Gastric tonometry: the role of mucosal pH measurement in
the management of trauma. Chest. 2003;123:475S.
147. Wang P, Ba ZF, Burkhardt J, et al. Measurement of hepatic blood flow after severe
hemorrhage: lack of restoration despite adequate resuscitation. Am J Physiol. 1992;262
(1 Part 1):G92.
148. Nordin A, Mildh L, Makisalo H, et al. Hepatosplanchnic and peripheral tissue
oxygenation during treatment of hemorrhagic shock: the effects of pentoxifylline
administration. Ann Surg. 1998;228(6):741.
149. Tadros T, Traber DL, Herndon DN. Trauma- and sepsis-induced hepatic ischemia
and reperfusion injury: role of angiotensin II. Arch Surg. 2000;135:766.
150. Hoppen RA, Corso CO, Grezzana TJ, et al. Hypertonic saline and hemorrhagic
shock: hepatocellular function and integrity after six hours of treatment. Acta Cir Bras.
2005;20(6):414.
151. Kitai T, Tanaka A, Tokuka A, et al. Changes in the hepatic oxygenation state
during hemorrhage and following epinephrine or dextran infusion as assessed by near-
infrared spectroscopy. Circ Shock. 1993;41(3):197.
Page 69 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

152. Bor NM, Alvur M, Ercan MT, et al. Liver blood flow rate and glucose metabolism in
hemorrhagic hypotension and shock. J Trauma. 1982;22(9):753.
153. Hawker F. Liver dysfunction in critical illness. Anaesth Intensive Care. 1991;19
(2):165.
154. Tashkin DP, Goldstein PJ, Simmons DH. Hepatic lactate uptake during decreased
liver perfusion and hypoxemia. Am J Physiol. 1972;223(4):968.
155. Champion HR, Jones RT, Trump BF, et al. A clinicopathologic study of hepatic
dysfunction following shock. Surg Gynecol Obstet. 1976;142(5):657.
156. Lefer AM, Spath JA. Pancreatic hypoperfusion and the production of a myocardial
depressant factor in hemorrhagic shock. Ann Surg. 1974;179(6):868.
157. Schmid-Schonbein GW, Hugli TE, Kistler EB, et al. Pancreatic enzymes and
microvascular cell activation in multiorgan failure. Microcirculation. 2001;8(1):5.
158. Mitsuoka H, Kistler EB, Schmid-Schonbein GW. Protease inhibition in the intestinal
lumen: attenuation of systemic inflammation and early indicators of multiple organ
failure in shock. Shock. 2002;17(3):205.
159. Waldo SW, Rosario HS, Penn AH, et al. Pancreatic digestive enzymes are potent
generators of mediators for leukocyte activation and mortality. Shock. 2003;20(2):138.
160. Fitzal F, DeLano FA, Young C, et al. Improvement in early symptoms of shock by
delayed intestinal protease inhibition. Arch Surg. 2004;139:1008.
161. Ishimaru K, Mitsuoka H, Unno N, et al. Pancreatic proteases and inflammatory
mediators in peritoneal fluid during splanchnic arterial occlusion and reperfusion.
Shock. 2004;22(5):467.
162. Schmid-Schonbein GW, Hugli TE. A new hypothesis for microvascular inflammation
in shock and multiorgan failure: self-digestion by pancreatic enzymes.
Microcirculation. 2005;12:71.
Page 70 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

163. Penn AH, Hugli TE, Schmid-Schonbein GW. Pancreatic enzymes generate cytotoxic
mediators in the intestine. Shock. 2007;27(3):296.
164. Ramos-Kelly JR, Toledo-Pereyra LH, Jordan JA, et al. Upregulation of lung
chemokines associated with hemorrhage is reversed with a small molecule multiple
selectin inhibitor. J Am Coll Surg. 1999;189(6):546.
165. Upperman JS, Deitch EA, Guo W, et al. Post-hemorrhagic shock mesenteric lymph
is cytotoxic to endothelial cells and activates neutrophils. Shock. 1998;10(6):407.
166. Chaudry IH, Ayala A, Ertel W, et al. Hemorrhage and resuscitation: immunological
aspects. Am J Physiol. 1990;259(4 Part 2):R663.
167. Nast-Kolb D, Waydhas C, Gippner-Steppert C, et al. Indicators of the
posttraumatic inflammatory response correlate with organ failure in patients with
multiple injuries. J Trauma. 1997;42(3):446.
168. Hierholzer C, Kalff JC, Omert L, et al. Interleukin-6 production in hemorrhagic
shock is accompanied by neutrophil recruitment and lung injury. Am J Physiol.
1998;275(3 Part 1):L611.
169. Hierholzer C, Kalff JC, Chakraborty A, et al. Impaired gut contractility following
hemorrhagic shock is accompanied by IL-6 and G-CSF production and neutrophil
infiltration. Dig Dis Sci. 2001;46(2):230.
170. Roumen RMH, Hendriks T, van der Ven-Jongekrijg J, et al. Cytokine patterns in
patients after major vascular surgery, hemorrhagic shock and severe blunt trauma:
relation with subsequent adult respiratory distress syndrome and multiple organ
failure. Ann Surg. 1993:218(6):769.
171. Meng X, Ao L, Song Y, et al. Signaling for myocardial depression in hemorrhagic
shock: roles of toll-like receptor 4 and p55 TNF-alpha receptor. Am J Physiol Regul
Integr Comp Physiol. 2005;288(3):R600.
172. Prince JM, Levy RM, Yang R, et al. Toll-like receptor-4 signaling mediates hepatic
injury and systemic inflammation in hemorrhagic shock. J Am Coll Surg. 2006;202
Page 71 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

(3):407.
173. Watters JM, Tieu BH, Todd SR, et al. Fluid resuscitation increases inflammatory
gene transcription after traumatic injury. J Trauma. 2006;61(2):300.
174. Lee CC, Chang IJ, Yen ZS, et al. Delayed fluid resuscitation in hemorrhagic shock
induces proinflammatory cytokine response. Ann Emerg Med. 2007;49(1):37.
175. Turnage RH, Kadesky KM, Rogers T, et al. Neutrophil regulation of splanchnic
blood flow after hemorrhagic shock. Ann Surg. 1995;222(1):66.
176. Gonzalez RJ, Moore EE, Ciesla DJ, et al. Phospholipase A(2)-derived neutral lipids
from post-hemorrhagic shock mesenteric lymph prime the neutrophil oxidative burst.
Surgery. 2001;130(2):198.
177. Patel JP, Beck LD, Briglia FA, et al. Beneficial effects of combined thromboxane
and leukotriene receptor antagonism in hemorrhagic shock. Crit Care Med. 1995;23
(2):231.
178. Yokoyama Y, Nimura Y, Nagino M, et al. Role of thromboxane in producing hepatic
injury during hepatic stress. Arch Surg. 2005;140:801.
179. Vanlersberghe C, Lauwers MH, Camu F. Prostaglandin synthetase inhibitor
treatment and the regulatory role of prostaglandins on organ perfusion. Acta
Anaesthesiol Belg. 1992;43(4):211.
180. Yamakawa Y, Takano M, Patel M, et al. Interaction of platelet-activating factor,
reactive oxygen species generated by xanthine oxidase, and leukocytes in the
generation of hepatic injury after shock/resuscitation. Ann Surg. 2000;231(3):387.
181. Fruchterman TM, Spain DA, Wilson MA, et al. Complement inhibition prevents gut
ischemia and endothelial cell dysfunction after hemorrhage/resuscitation. Surgery.
1998;124(4):782.
182. Spain DA, Fruchterman TM, Matheson PJ, et al. Complement activation mediates
intestinal injury after resuscitation from hemorrhagic shock. J Trauma. 1999;46(2):224.
P.919
Page 72 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

183. Childs EW, Udobi KF, Hunter FA. Hypothermia reduces microvascular permeability
and reactive oxygen species expression after hemorrhagic shock. J Trauma. 2005;58
(2):271.
184. Szabo C. The pathophysiological role of peroxynitrite in shock, inflammation, and
ischemia-reperfusion injury. Shock. 1996;6(2):79.
185. Kapoor R, Prasad K. Role of oxyradicals in cardiovascular depression and cellular
injury in hemorrhagic shock and reinfusion: effect of SOD and catalase. Circ Shock.
1994;43(2):79.
186. Prasad K, Kalra J, Buchko G. Acute hemorrhage and oxygen free radicals.
Angiology. 1988;39(12):1005.
187. Ahmed N, Christou N. Systemic inflammatory response syndrome: interactions
between immune cells and the endothelium. Shock. 1996;6(Suppl 1):S39.
188. van Meurs M, Wulfert FM, Knol AJ, et al. Early organ-specific endothelial
activation during hemorrhagic shock and resuscitation. Shock. 2008;29:291.
189. Martinez-Mier G, Toledo-Pereyra LH, Ward PA. Adhesion molecules and
hemorrhagic shock. J Trauma. 2001;51(2):408.
190. Horgan MJ, Ge M, Gu J, et al. Role of ICAM-1 in neutrophil-mediated lung vascular
injury after occlusion and reperfusion. Am J Physiol. 1991;261(5 Part 2):H1578.
191. Adams CA, Sambol JT, Xu DZ, et al. Hemorrhagic shock induced up-regulation of
P-selectin expression is mediated by factors in mesenteric lymph and blunted by
mesenteric lymph duct interruption. J Trauma. 2001;51(4):625.
192. Xu DZ, Lu Q, Adams CA, et al. Trauma-hemorrhagic shock-induced upregulation of
endothelial cell adhesion molecules is blunted by mesenteric lymph duct ligation. Crit
Care Med. 2004;32(3):760.
193. Jarrar D, Chaudry IH, Wang P. Organ dysfunction following hemorrhage and sepsis:
mechanisms and therapeutic approaches. Int J Mol Med. 1999;4(6):575.
Page 73 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

194. Guillou PJ. Biological variation in the development of sepsis after surgery or
trauma. Lancet. 1993;342(8865):217.
195. O'Mahony JB, Palder SB, Wood JJ, et al. Depression of cellular immunity after
multiple trauma in the absence of sepsis. J Trauma. 1984;24(10):869.
196. Stephan RN, Kupper TS, Geha AS, et al. Hemorrhage without tissue produces
immunosuppression and enhances susceptibility to sepsis. Arch Surg. 1987;122(1):62.
197. Walz CR, Zedler S, Schneider CP, et al. Depressed T cell-derived IFN-gamma
following trauma-hemorrhage: a potential mechanism for diminished APC responses.
Langenbecks Arch Surg. 2007;392(3):339.
198. Ertel W, Morrison MH, Ayala A, et al. Insights into the mechanisms of defective
antigen presentation after hemorrhage. Surgery. 1991;110(2):440.
199. Fan J, Li Y, Levy RM, et al. Hemorrhagic shock induces NAD(P)H oxidase activation
in neutrophils: role of HMGB1-TLR4 signaling. J Immunol. 2007;178(10):6573.
200. Lomas-Neira J, Chung CS, Perl M, et al. Role of alveolar macrophage and migrating
neutrophils in hemorrhage-induced priming for ALI subsequent to septic challenge. Am
J Physiol Lung Cell Mol Physiol. 2006;290(1):L51.
201. Fan J, Li Y, Vodovotz Y, et al. Hemorrhagic shock-activated neutrophils augment
TLR4 signaling-induced TLR2 upregulation in alveolar macrophages: role in hemorrhage-
primed lung inflammation. Am J Physiol Lung Cell Mol Physiol. 2006;290(4):L738.
202. Schneider CP, Schwacha MG, Chaudry IH. Influence of gender and age on T-cell
responses in a murine model of trauma-hemorrhage: differences between circulating
and tissue-fixed cells. J Appl Physiol. 2006;100(3):826.
203. Faist E, Schinkel C, Zimmer S. Update on the mechanisms of immune suppression
of injury and immune modulation. World J Surg. 1996;20(4):454.
204. Angele MK, Chaudry IH. Surgical trauma and immunosuppression: pathophysiology
and potential immunomodulatory approaches. Langenbeck Arch Surg. 2005;390(4):333.
Page 74 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

205. Knoferl MW, Angele MK, Diodato MD, et al. Female sex hormones regulate function
after trauma-hemorrhage and prevent increased cell death rate from subsequent
sepsis. Ann Surg. 2002;235(1):105.
206. Schneider CP, Schwacha MG, Chaudry IH. The role of interleukin-10 in the
regulation of the systemic inflammatory response following trauma-hemorrhage.
Biochim Biophys Acta. 2004;1689(1):22.
207. Yokoyama Y, Kitchens WC, Toth B, et al. Role of IL-10 in regulating
proinflammatory cytokine release by Kupffer cells following trauma-hemorrhage. Am J
Physiol Gastrointest Liver Physiol. 2004;286(6):G942.
208. Lyons A, Kelly JL, Rodrick ML, et al. Major injury induces increased production of
interleukin-10 by cells of the immune system with a negative impact on resistance to
infection. Ann Surg. 1997;226(4):450.
209. Cinat ME, Waxman K, Granger GA, et al. Trauma causes sustained elevation of
soluble tumor necrosis factor receptors. J Am Coll Surg. 1994;179(5):529.
210. Cinat M, Waxman K, Vaziri ND, et al. Soluble cytokine receptors and receptor
antagonists are sequentially released after trauma. J Trauma. 1995;39(1):112.
211. American College of Surgeons Committee on Trauma. Initial assessment and
management. In: Advanced Trauma Life Support. 7th ed. American College of
Surgeons, Chicago, IL; 2004:11.
212. Daniel SR, Morita SY, Yu M, et al. Uncompensated metabolic acidosis: an
underrecognized risk factor for subsequent intubation requirement. J Trauma.
2004;57:993.
213. Aufderheide TP, Sigurdsson G, Pirrallo RG, et al. Hyperventilation-induced
hypotension during cardiopulmonary resuscitation. Circulation. 2004;109:1960.
214. Davis DP, Hoyt DB, Ochs M, et al. The effect of paramedic rapid sequence
intubation on outcome in patients with severe traumatic brain injury. J Trauma.
2003;54:444.
Page 75 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

215. Pepe PE, Lurie KG, Wigginton JG, et al. Detrimental hemodynamic effects of
assisted ventilation in hemorrhagic states. Crit Care Med. 2004;32:S414.
216. Krismer AC, Wenzel V, Lindner KH, et al. Influence of negative expiratory pressure
ventilation on hemodynamic variables during severe hemorrhagic shock. Crit Care Med.
2006;34:2175.
217. Miller PR, Moore PS, Mansell E, et al. External fixation or arteriogram in bleeding
pelvic fracture: initial therapy guided by markers of arterial hemorrhage. J Trauma.
2003;54:437.
218. Heetveld MJ, Harris I, Schlaphoff G, et al. Guidelines for the management of
haemodynamically unstable pelvic fracture patients. ANZ J Surg. 2004;74:520.
219. Ertel W, Keel M, Eid K, et al. Control of severe hemorrhage using C-clamp and
pelvic packing in multiply injured patients with pelvic ring disruption. J Orthop
Trauma. 2001;15:468.
220. Giannoudis PV, Pape HC. Damage control orthopaedics in unstable pelvic ring
fractures. Injury. 2004;35:671.
221. American College of Surgeons Committee on Trauma. Shock. In: Advanced Trauma
Life Support. 7th ed. American College of Surgeons, Chicago, IL; 2004:69.
222. Codner P, Obaid A, Porral D, et al. Is field hypotension a reliable indicator of
significant injury in trauma patients who are normotensive on arrival to the emergency
department? Am Surg. 2005;71(9):768.
223. Chan L, Bartfield JM, Reilly KM. The significance of out-of-hospital hypotension in
blunt trauma patients. Acad Emerg Med. 1997;4:785.
224. Lipsky AM, Gausche-Hill M, Henneman PL, et al. Prehospital hypotension is a
predictor of the need for an emergent, therapeutic operation in trauma patients with
normal systolic blood pressure in the emergency department. J Trauma. 2006;61:1228.
225. Hagiwara A, Minakawa K, Fukushima H, et al. Predictors of death in patients with
Page 76 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

life-threatening pelvic hemorrhage after successful transcatheter arterial
embolization. J Trauma. 2003;55:696.
226. Hoffer EK, Borsa JJ, Bloch RD, et al. Endovascular techniques in the damage
control setting. Radiographics. 1999;19:1340.
227. Shapiro M, McDonald AA, Knight D, et al. The role of repeat angiography in the
management of pelvic fractures. J Trauma. 2005;58:227.
228. Panetta T, Sclafani SJ, Goldstein AS, et al. Percutaneous transcatheter
embolization for massive bleeding from pelvic fractures. J Trauma. 1985;25:1021.
229. Spahn DR, Cerny V, Coats TJ, et al. Management of bleeding following major
trauma: a European guideline. Crit Care. 2007;11:R17.
230. Hunt PA, Greaves I, Owens WA. Emergency thoracotomy in thoracic trauma—a
review. Injury. 2006;37:1.
231. Cothren CC, Moore EE. Emergency department thoracotomy for the critically
injured: objectives, indications, and outcomes. World J Emerg Surg. 2006;1:4.
232. Millikan JS, Moore EE. Outcome of resuscitative thoracotomy and descending
aortic occlusion performed in the operating room. J Trauma. 1984;24:387.
233. Richardson JD, Bergamini TM, Spain DA, et al. Operative strategies for
management of abdominal aortic gunshot wounds. Surgery. 1996;120:667.
234. Nicholas JM, Rix EP, Easley KA, et al. Changing patterns in the management of
penetrating abdominal trauma: the more things change, the more they stay the same.
J Trauma. 2003;55:1095.
235. Reich DL, Konstadt SN, Raissi S, et al. Trendelenburg position and passive leg
raising do not significantly improve cardiopulmonary performance in the anesthetized
patient with coronary artery disease. Crit Care Med. 1989;17:313.
236. Mattox KL, Bickell W, Pepe PE, et al. Prospective MAST study in 911 patients. J
Page 77 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

Trauma. 1989;29(8):1104.
237. Mattox KL, Bickell WH, Pepe PE, et al. Prospective randomized evaluation of
antishock MAST in post-traumatic hypotension. J Trauma. 1986;26(9):779.
238. Cayten CG, Berendt BM, Byrne DW, et al. A study of pneumatic antishock
garments in severely hypotensive trauma patients. J Trauma. 1993;34(5):728.
239. Velanovich V. Crystalloid versus colloid fluid resuscitation: a meta-analysis of
mortality. Surgery. 1989;105:65.
240. Bisonni RS, Holtgrave DR, Lawler F, et al. Colloids versus crystalloids in fluid
resuscitation: an analysis of randomized controlled trials. J Fam Pract. 1991;32:387.
241. Schierhout G, Roberts I. Fluid resuscitation with colloid or crystalloid solutions in
critically ill patients: a systematic review of randomized trials. BMJ. 1998;316:961.
242. Human albumin administration in critically ill patients: systematic review of
randomized controlled trials. Cochrane Injuries Group Albumin Reviewers. BMJ.
1998;317:235.
243. Choi PT, Yip G, Quinonez LG, et al. Crystalloids vs. colloids in fluid resuscitation:
a systematic review. Crit Care Med. 1999;27:200.
244. Roberts I, Alderson P, Bunn F, et al. Colloids vs crystalloids for fluid resuscitation
in critically ill patients. Cochrane Database Syst Rev. 2004;CD000567.
245. Finfer S, Bellomo R, Boyce N, et al. A comparison of albumin and saline for fluid
resuscitation in the intensive care unit. N Engl J Med. 2004;350:2247.
246. Entholzner EK, Mielke LL, Calatzis AN, et al. Coagulation effects of a recently
developed hydroxyethyl starch (HES 130/0.4) compared to hydroxyethyl starches with
higher molecular weight. Acta Anesth Scand. 2000;44:1116.
247. Jamnicki M, Zollinger A, Seifert B, et al. Compromised blood coagulation: an in
vitro comparison of hydroxyethyl starch 130/0.4 and hydroxyethyl starch 200/0.5 using
P.920
Page 78 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

thromboelastography. Anesth Analg. 1998;87:989.
248. Langeron O, Doelberg M, Ang ET, et al. Voluven, a lower substituted novel
hydroxyethyl starch (HES 130/0.4) causes fewer effects on coagulation in major
orthopedic surgery than HES 200/0.5. Anesth Analg. 2001;92:855.
249. Fenger-Eriksen C, Anker-Moller E, Heslop J, et al. Thromboelastographic whole
blood clot formation after ex vivo addition of plasma substitutes: improvements of the
induced coagulopathy with fibrinogen concentrate. Br J Anaesth. 2005;94:324.
250. Tieu BH, Holcomb JB, Schreiber MA, et al. Coagulopathy: its pathophysiology and
treatment in the injured patient. World J Surg. 2007;31:1055.
251. Kiraly LN, Differding JA, Enomoto TM, et al. Resuscitation with normal saline
versus lactated ringers modulates hypercoagulability and leads to increased blood loss
in an uncontrolled hemorrhagic shock swine model. J Trauma. 2006;61:57.
252. Cotton BA, Guy JS, Morris JA, et al. The cellular, metabolic, and systemic
consequences of aggressive fluid resuscitation strategies. Shock. 2006;26:115.
253. Coimbra R, Hoyt DB, Junger WG, et al. Hypertonic saline resuscitation decreases
susceptibility to sepsis after hemorrhagic shock. J Trauma. 1997;42:602.
254. Rhee P, Wand D, Ruff P, et al. Human neutrophil activation and increased
adhesion by various resuscitation fluids. Crit Care Med. 2000;28:74.
255. Ayuste EC, Chen H, Koustova E, et al. Hepatic and pulmonary apoptosis after
hemorrhagic shock in swine can be reduced through modifications of conventional
Ringers solution. J Trauma. 2006;60:52.
256. Rhee P, Koustova E, Alam HB. Searching for the optimal resuscitation method:
recommendations for the initial fluid resuscitation of combat casualties. J Trauma.
2003;54(Suppl.):S52.
257. Raeburn CD, Moore EE, Biffl WL, et al. The abdominal compartment syndrome is a
morbid complication of post injury damage control surgery. Am J Surg. 2001;182:542.
Page 79 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

258. Biffl WL, Moore EE, Burch JM, et al. Secondary abdominal compartment syndrome
is a highly lethal event. Am J Surg. 2001;182:645.
259. Maxwell RA, Fabian TC, Croce MA, et al. Secondary abdominal compartment
syndrome: an underappreciated manifestation of severe hemorrhagic shock. J Trauma.
1999;47:995.
260. Miller RS, Morris JA, Diaz JJ, et al. Complications after 344 damage control open
celiotomies. J Trauma. 2004;57:436.
261. Gracias VH, Braslow B, Johnson J, et al. Abdominal compartment syndrome in the
open abdomen. Arch Surg. 2002;137:1298.
262. Kauvar DS, Holcomb JB, Norris GC, et al. Fresh whole blood transfusion: a
controversial military practice. J Trauma. 2006;61:181.
263. Owens TM, Watson WC, Prough DS, et al. Limiting initial resuscitation of
uncontrolled hemorrhage reduces internal bleeding and subsequent volume
requirements. J Trauma. 1995;39:200.
264. Dutton RP, Mackenzie CF, Scalea TM. Hypotensive resuscitation during active
hemorrhage: impact on in-hospital mortality. J Trauma. 2002;52:1141.
265. Bickell WH, Wall MJ, Pepe PE, et al. Immediate versus delayed fluid resuscitation
for hypotensive patients with penetrating torso trauma. N Engl J Med. 1994;331:1105.
266. Hirschberg A, Hoyt DB, Mattox KL. From “leaky buckets” to vascular injuries:
understanding models of uncontrolled hemorrhage. J Am Coll Surg. 2007;204:665.
267. Iserson KV, Huestis DW. Blood warming: current applications and techniques.
Transfusion. 1991;31:558.
268. Janczyk RJ, Howells GA, Bair HA, et al. Hypothermia is an independent predictor
of mortality in ruptured abdominal aortic aneurysms. Vasc Endovascular Surg.
2004;38:37.
Page 80 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

269. Strate LL, Syngal S. Predictors of utilization of early colonoscopy versus
radiography for severe lower intestinal bleeding. Gastrointest Endosc. 2005;61:46.
270. Gady JS, Reynolds H, Blum A. Selective arterial embolization for control of lower
gastrointestinal bleeding: recommendations for a clinical management pathway. Curr
Surg. 2003;60(3):344.
271. Kuo WT, Lee DE, Saad WE, et al. Superselective microcoil embolization for the
treatment of lower gastrointestinal hemorrhage. J Vasc Intern Radial. 2003;14
(12):1503.
272. DeBarros J, Rosas L, Cohen J, et al. The changing paradigm for the treatment of
colonic hemorrhage: superselective angiographic embolization. Dis Colon Rectum.
2002;45(6):802.
273. Johnston C, Tuite D, Pritchard R, et al. Use of provocative angiography to localize
site in recurrent gastrointestinal bleeding. Cardiovasc Intervent Radiol. 2007;30:1042.
274. Lin S, Rockey DC. Obscure gastrointestinal bleeding. Gastroenterol Clin North Am.
2005;34(4):679.
275. Hyare H, Desigan S, Brookes JA, et al. Endovascular management of major arterial
hemorrhage as a complication of inflammatory pancreatic disease. J Vasc Interv
Radiol. 2007;18(5):591.
276. Zyromski NJ, Vieira C, Stecker M, et al. Improved outcomes in postoperative and
pancreatitis-related visceral pseudoaneurysms. J Gastrointest Surg. 2007;11(1):50.
277. Nicholson AA, Patel J, McPherson S, et al. Endovascular treatment of visceral
aneurysms associated with pancreatitis and a suggested classification with therapeutic
implications. J Vasc Interv Radiol. 2006;17(8):1279.
278. Snyder HS. Significance of the initial spun hematocrit in trauma patients. Am J
Emerg Med. 1998;16:150.
279. Greenfield RH, Bessen HA, Henneman PL. Effect of crystalloid infusion on
Page 81 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

hematocrit and intravascular volume in healthy nonbleeding subjects. Ann Emerg Med.
1989;18:51.
280. Kass LE, Tien IY, Ushkow BS, et al. Prospective crossover study of the effect of
phlebotomy and intravenous crystalloid on hematocrit. Acad Emerg Med. 1997;4:198.
281. Stamler KD. Effect of crystalloid infusion on hematocrit in non-bleeding patients
with application to clinical traumatology. Ann Emerg Med. 1989;18:747.
282. Paradis NA, Balter S, Davison CM, et al. Hematocrit as a predictor of significant
injury after penetrating trauma. Am J Emerg Med. 1997;15:224.
283. Zehtabchi S, Sinert R, Goldman M, et al. Diagnostic performance of serial
hematocrit measurements in identifying major injury in adult trauma patients. Injury.
2006;37:46.
284. Broder G, Weil MH. Excess lactate: an index of reversibility of shock in human
patients. Science. 1964;143:1457.
285. Bakker J, Coffemils M, Leon M, et al. Blood lactate levels are superior to oxygen-
derived variables in predicting outcome in human septic shock. Chest. 1992;99:956.
286. Weil MH, Atiti AA. Experimental and clinical studies on lactate and pyruvate as
indicators of the severity of acute circulatory failure (shock). Circulation. 1970;41:989.
287. Hemming RJ, Weil MH, Weiner F. Blood lactate as a prognostic indicator of
survival in patients with acute myocardial infarction. Circ Shock. 1982;9:307.
288. Vincent JL, Roman A, Kahn RJ. Dobutamine administration in septic shock:
addition to a standard protocol. Crit Care Med. 1990;18:689.
289. Vincent JL, Dufaye P, Berre J, et al. Serial lactate determinations during
circulatory shock. Crit Care Med. 1983;11:449.
290. Levy B. Lactate and shock state: the metabolic review. Curr Opin Crit Care.
2006;12:315.
Page 82 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

291. Fall PJ, Szerlip HM. Lactic acidosis: from sour milk to septic shock. J Intens Care
Med. 2005;20(5):255.
292. Madias NE. Lactic acidosis. Kidney Int. 1986;29:752.
293. Eldridge F, Sulzer J. Effect of respiratory alkalosis on blood lactate and pyruvate
in humans. J Appl Physiol. 1967;22:461.
294. Wilson M, Davis DP, Coimbra R. Diagnosis and monitoring of hemorrhagic shock
during the initial resuscitation of multiple trauma patients: a review. J Emerg Med.
2003;24:413.
295. Baron BJ, Scalea TM. Acute blood loss. Emerg Med Clin North Am. 1996;14:35.
296. Porter JM, Ivatury RR. In search of the optimal endpoints of resuscitation in
trauma patients: a review. J Trauma. 1998;44:908.
297. Bilkovski RN, Rivers EP, Horst HM. Targeted resuscitation strategies after injury.
Curr Opin Crit Care. 2004;10:529.
298. Abramson D, Scalea TM, Hitchcock R, et al. Lactate clearance and survival
following injury. J Trauma. 1993;35:584.
299. Manikis P, Jankowski S, Zhang H, et al. Correlation of serial blood lactate levels to
organ failure and mortality after trauma. Am J Emerg Med. 1995;13:619.
300. Rixen D, Siegel JH. Bench-to-bedside review: oxygen debt and its metabolic
correlates as quantifiers of the severity of hemorrhagic and post-traumatic shock. Crit
Care. 2005;9:441.
301. Aslar AK, Kuzu MA, Elhan AH, et al. Admission lactate level and the APACHE II
score are the most useful predictors of prognosis following torso trauma. Injury.
2004;35:746.
302. Dunne JR, Tracy K, Scalea TM, et al. Lactate and base deficit in trauma: does
Page 83 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

alcohol or drug use impair their predictive accuracy? J Trauma. 2005;58:959.
303. Kaplan LJ, Kellum JA. Initial pH, base deficit, lactate, anion gap, strong ion
difference, and strong ion gap predict outcome from major vascular injury. Crit Care
Med. 2004;32:1120.
304. Martin MJ, FitzSullivan E, Salim A, et al. Discordance between lactate and base
deficit in the surgical intensive care unit: which one do you trust? Am J Surg.
2006;191:625.
305. Waxman K, Nolan LS, Shoemaker WC. Sequential perioperative lactate
determination. Physiological and clinical implications. Crit Care Med. 1982;10:96.
306. Lavery RF, Livingston DH, Tortella BJ, et al. The utility of venous lactate to triage
injured patients in the trauma center. J Am Coll Surg. 2000;190(6):656.
307. Rutherford EJ, Morris JA, Reed GW, et al. Base deficit is stratifies mortality and
determines therapy. J Trauma. 1992;33:417.
308. Davis JW, Parks SN, Kaups KL, et al. Admission base deficit predicts transfusion
requirements and risk of complications. J Trauma. 1996;41:769.
309. Davis JW, Kaups KL, Parks SN. Base deficit is superior to pH in evaluating
clearance of acidosis after traumatic shock. J Trauma. 1998;44:114.
310. Davis JW, Kaups KL. Base deficit in the elderly: a marker of severe injury and
death. J Trauma. 1998;45:873.
311. Randolph LC, Takacs M, Davis KA. Resuscitation in the pediatric trauma
population: admission base deficit remains an important prognostic indicator. J
Trauma. 2002;53:838.
312. Peterson DL, Schinco MA, Kerwin AJ, et al. Evaluation of initial base deficit as a
prognosticator of outcome in the pediatric trauma population. Am Surg. 2004;70
(4):326.
313. Sauaia A, Moore FA, Moore EE, et al. Early risk factors for post-injury multiple
P.921
Page 84 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

organ failure. World J Surg. 1996;20:392.
314. Martin MJ, FitzSullivan E, Salim A, et al. Use of serum bicarbonate measurement
in place of arterial base deficit in the surgical intensive care unit. Arch Surg.
2005;140:745.
315. FitzSullivan E, Salim A, Demetriades D, et al. Serum bicarbonate may replace the
arterial base deficit in the trauma intensive care unit. Am J Surg. 2005;190:961.
316. Mikulaschek A, Henry SM, Donovan R, et al. Serum lactate is not predicted by
anion gap or base excess after trauma resuscitation. J Trauma. 1996;40:218.
317. Singhal R, Coghill JE, Guy A, et al. Serum lactate and base deficit as predictors of
mortality after ruptured abdominal aortic aneurysm repair. Eur J Vasc Endovasc Surg.
2005;30(3):263.
318. Brohi K, Singh J, Heron M, et al. Acute traumatic coagulopathy. J Trauma.
2003;54:1127.
319. MacLeod JBA, Lynn M, McKenney MG, et al. Early coagulopathy predicts mortality
in trauma. J Trauma. 2003;55:39.
320. Hess JR, Lawson JH. The coagulopathy of trauma versus disseminated
intravascular coagulation. J Trauma. 2006;60:S12.
321. Brohi K, Cohen MJ, Ganter MT, et al. Acute traumatic coagulopathy: initiated by
hypoperfusion. Modulated through the protein C pathway? Ann Surg. 2007;245:812.
322. Practice guidelines for perioperative blood transfusion and adjuvant therapies: an
updated report by the American Society of Anesthesiologists Task Force on
Perioperative Blood Transfusion and Adjuvant Therapies. Anesthesiology.
2006;105:198.
323. Roissant R, Cerny V, Coats TJ, et al. Key issues in advanced bleeding care in
trauma. Shock. 2006;26(4):322.
324. Zuckerman L, Cohen E, Vagher JP, et al. Comparison of thromboelastography with
Page 85 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

common coagulation tests. Thromb Haemost. 1981;46:752.
325. Kaufmann CR, Dwyer KM, Crews JD, et al. Usefulness of thromboelastography in
assessment of trauma patient coagulation. J Trauma. 1997;42:716.
326. Rugeri L, Levrat A, David JS, et al. Diagnosis of early coagulation abnormalities in
trauma patients by rotation thrombelastography. J Thromb Haemost. 2007;5(2):289.
327. Coakley M, Reddy K, Mackie I, et al. Transfusion triggers in orthotopic liver
transplantation: a comparison of the thromboelastometry analyzer, the
thromboelastogram, and conventional coagulation tests. J Cardiothorac Vasc Anesth.
2006;20(4):548.
328. Ronald A, Dunning J. Can the use of thromboelastography predict and decrease
bleeding and blood and blood product requirements in adult patients undergoing
cardiac surgery? Interact Cardiovasc Thorac Surg. 2005;4(5):456.
329. Spalding GJ, Hartrumpg M, Sierig T, et al. Cost reduction of perioperative
coagulation management in cardiac surgery: value of “bedside” thromboelastography
(ROTEM). Eur J Cardiothorac Surg. 2007;31(6):1052.
330. Hobson AR, Agarwala RA, Swallow RA, et al. Thromboelastography: current clinical
applications and its potential role in interventional cardiology. Platelets. 2006;17
(8):509.
331. Zambruni A, Thalheimer U, Leandro G, et al. Thromboelastography with citrated
blood: comparability with native blood, stability of citrate storage, and effect of
repeated sampling. Blood Coagul Fibrinolysis 2004;15:103.
332. Pivalizza EG, Pivalizza PJ, Gottschalk LI, et al. Celite-activated
thromboelastography in children. J Clin Anesth. 2001;13:20.
333. Gorton HJ, Warren ER, Simpson NS, et al. Thromboelastography identifies sex-
related differences in coagulation. Anesth Analg. 2000;91:1279.
334. Camenzind V, Bombeli T, Seifert B, et al. Citrate storage affects
Page 86 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

thromboelastograph analysis. Anesthesiology. 2000;92:1242.
335. Vig S, Chitolie A, Bevan DH, et al. Thromboelastography: a reliable test? Blood
Coagul Fibrinolysis. 2001;12:555.
336. Rajwal S, Richards M, O'Meara M. The use of recalcified citrated whole blood—a
pragmatic approach for thromboelastography in children. Paediatr Anaesth.
2004;14:656.
337. Jackson MR, Olson DW, Beckett WC Jr, et al. Abdominal vascular trauma: a review
of 106 injuries. Am Surg. 1992;58:622.
338. Blocksom JM, Tyburski JG, Sohn RL, et al. Prognostic determinants in duodenal
injuries. Am Surg. 2004;70:248.
339. Ertel W, Eid K, Keel M, et al. Therapeutic strategies and outcome of
polytraumatized patients with pelvic injuries: a six year experience. Eur J Trauma.
2000;26:278.
340. Hill DA, West RH, Roncal S. Outcome of patients with haemorrhagic shock: an
indicator of performance in a trauma centre. J R Coll Surg Edinb. 1995;40:221.
341. Thoburn E, Norris P, Flores R, et al. System care improves trauma outcome:
patient care errors dominate reduced preventable death rate. J Emerg Med.
1993;11:135.
342. Alberts KA, Brismar B, Nygren A. Major differences in trauma care between
hospitals in Sweden: a preliminary report. Qual Assur Health Care. 1993;5:13.
343. Peitzman AB, Courcoulas AP, Stinson C, et al. Trauma center maturation:
quantification of process and outcome. Ann Surg. 1999;230(1):87.
344. Harrington DT, Connolly M, Biffl WL, et al. Transfer times to definitive care
facilities are too long: a consequence of an immature trauma system. Ann Surg.
2005;241(6):961.
345. Moore R, Nutley M, Cina CS, et al. Improved survival after introduction of an
Page 87 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

emergency endovascular therapy protocol for ruptured abdominal aortic aneurysms. J
Vasc Surg. 2007;45:443.
346. Bounoua F, Schuster R, Grewal P, et al. Ruptured abdominal aortic aneurysm:
does trauma center designation affect outcome? Ann Vasc Surg. 2007;21(2):133.
347. Salhab M, Farmer J, Osman I. Impact of delay on survival in patients with ruptured
abdominal aortic aneurysm. Vascular. 2006;14(1):38.
348. Hoyt DB, Bulger EM, Knudson MM, et al. Death in the operating room: an analysis
of a multicenter experience. J Trauma. 1994;37:426.
349. Jurkovich GJ, Greiser WB, Luterman A, et al. Hypothermia in trauma victims: an
ominous predictor of survival. J Trauma. 1987;27(9):1019.
350. Garrison JR, Richardson JD, Hilakos AS, et al. Predicting the need to pack early for
severe intra-abdominal hemorrhage. J Trauma. 1996;40(6):923.
351. Sharp KW, Locicero RJ. Abdominal packing for surgically uncontrollable
hemorrhage. Ann Surg. 1992;215(5):467.
352. Cosgriff N, Moore EE, Sauaia A, et al. Predicting life-threatening coagulopathy in
the massively transfused trauma patient: hypothermia and acidosis revisited. J
Trauma. 1997;42(5):857.
353. Gentilello LM, Pierson DJ. Trauma critical care. Am J Respir Crit Care Med.
2001;604.
354. Lee JC, Peitzman AB. Damage control laparotomy. Curr Opin Crit Care.
2006;12:346.
355. Morris JA, Eddy VA, Rutherford EJ. The trauma celiotomy: the evolving concepts
of damage control. Curr Probl Surg. 1996;33:611.
356. Stone HH, Strom PR, Mullins RJ, et al. Management of the major coagulopathy
with onset during laparotomy. Ann Surg. 1983;197:532.
Page 88 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

357. Burch JM, Ortiz VB, Richardson RJ, et al. Abbreviated laparotomy and planned
reoperation for critically injured patients. Ann Surg. 1992;215:476.
358. Morris JA, Eddy VA, Blinman TA, et al. The staged celiotomy for trauma: issues in
packing and reconstruction. Ann Surg. 1993;217:576.
359. Moore EE, Burch JM, Franciose RJ, et al. Staged physiologic restoration and
damage control surgery. World J Surg. 1998;22:1184.
360. Johnson JW, Gracias VH, Schwab CW, et al. Evolution in damage control for
exsanguinating penetrating abdominal injury. J Trauma. 2001;51:261.
361. Grotz MR, Gummerson NW, Gansslen A, et al. Staged management and outcome of
combined pelvic and liver trauma: an international experience of the deadly duo.
Injury. 2006;37:642.
362. Rotondo MF, Schwab CW, McGonigal MD, et al. “Damage control”: an approach for
improved survival in exsanguinating penetrating abdominal injury. J Trauma.
1993;35:375.
363. Carrillo EH, Spain DA, Wilson MA, et al. Alternatives in the management of
penetrating injuries to the iliac vessels. J Trauma. 1998;44:1024.
364. Moore EE. Thomas G. Orr Memorial Lecture. Staged laparotomy for the
hypothermia, acidosis, and coagulopathy syndrome. Am J Surg. 1996;172:405.
365. Rotondo MF, Zonies DH. The damage control sequence and underlying logic. Surg
Clin North Am. 1997;77:761.
366. Shapiro MB, Jenkins DH, Schwab CW, et al. Damage control: collective review. J
Trauma. 2000;49:969.
367. Cinat ME, Wallace WC, Nastanski F, et al. Improved survival following massive
transfusion in patients who have undergone trauma. Arch Surg. 1999;134:964.
368. Holcomb JB, Jenkins D, Rhee P, et al. Damage control resuscitation: directly
Page 89 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

addressing the early coagulopathy of trauma. J Trauma. 2007;62:307.
369. Holcomb JB, Hoyt DB. Damage control resuscitation: the need for specific blood
products to treat the coagulopathy of trauma. Transfusion. 2006;46:685.
370. Roberts K, Revell M, Youssef H, et al. Hypotensive resuscitation in patients with
ruptured abdominal aortic aneurysm. Eur J Vasc Endovasc Surg. 2006;31(4):339.
371. Stern SA. Low-volume fluid resuscitation for presumed hemorrhagic shock: helpful
or harmful? Curr Opin Crit Care. 2001;7(6):422.
372. Kauvar DS, Wade CE. The epidemiology and modern management of traumatic
hemorrhage: US and international perspectives. Crit Care. 2005;9(Suppl 5):S1.
373. Sondeen JL, Coppes VG, Holcomb JB. Blood pressure at which rebleeding occurs
after resuscitation in swine with aortic injury. J Trauma. 2003;54(Suppl):S110.
374. Wade CE, Holcomb JB. Endpoints in clinical trials of fluid resuscitation of patients
with traumatic injuries. Transfusion. 2005;45:4S.
375. Deitch EA, Dayal SD. Intensive care unit management of the trauma patient. Crit
Care Med. 2006;34:2294.
376. Burris D, Rhee P, Kaufmann C, et al. Controlled resuscitation for uncontrolled
hemorrhagic shock. J Trauma. 1999;46(2):216.
377. Kwan I, Bunn F, Roberts I. Timing and volume of fluid administration for patients
with bleeding. Cochrane Database Syst Rev. 2003;CD002245.
378. May AK, Young JS, Butler K, et al. Coagulopathy in severe closed head injury: is
empiric therapy warranted? Am Surg. 1997;63:233.
379. Alam HB, Stanton K, Koustova E, et al. Effect of different strategies on neutrophil
activation in a swine model of hemorrhagic shock. Resuscitation. 2004;60(1):91.
380. Ho AM, Karmakar MK, Dion PW. Are we giving enough coagulation factors during
P.922
Page 90 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

trauma resuscitation? Am J Surg. 2005;190:479.
381. Faringer PD, Mullins RJ, Johnson RL, et al. Blood component supplementation
during massive transfusion of AS-1 red cells in trauma patients. J Trauma. 1993;34:481.
382. Hewson JR, Neame PB, Kumar N, et al. Coagulopathy related to dilution and
hypotension during massive transfusion. Crit Care Med. 1985;13:387.
383. Phillips TF, Soulier G, Wilson RF. Outcome of massive transfusion exceeding two
blood volumes in trauma and emergency surgery. J Trauma. 1987;27:903.
384. Harvey MP, Greenfield TP, Sugrue ME, et al. Massive blood transfusion in a tertiary
referral hospital: clinical outcomes and haemostatic complications. Med J Aust.
1995;163:356.
385. Mitchell KJ, Moncure KE, Onyeije C, et al. Evaluation of massive volume
replacement in the penetrating trauma patient. J Natl Med Assoc. 1994;86:926.
386. Spahn DR, Rossaint R. Coagulopathy and blood component transfusion in trauma.
Br J Anaesth. 2005;95:130.
387. Gonzalez EA, Moore FA, Holcomb JB, et al. Fresh frozen plasma should be given
earlier to patients requiring massive transfusion. J Trauma. 2007;62:112.
388. Ketchum L, Hess JR, Hiippala S. Indications for early fresh frozen plasma,
cryoprecipitate, and platelet transfusion in trauma. J Trauma. 2006;60(6):S51.
389. Malone L, Hess JR, Fingerhut A. Massive transfusion practices around the globe
and a suggestion for a common massive transfusion protocol. J Trauma. 2006;60
(6):S91.
390. Wilson RF, Mammen E, Walt AJ. Eight years experience with massive blood
transfusion. J Trauma. 1971;11(4):275.
391. Kivioja A, Myllynen P, Rokkanen P. Survival after massive transfusion exceeding
four blood volumes in patients with blunt injuries. Am Surg. 1991;57(6):398.
Page 91 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

392. Wudel JH, Morris JA, Yates K, et al. Massive transfusion: outcome in blunt trauma
patients. J Trauma. 1991;31(1):1.
393. Velmahos GC, Chan L, Chan M, et al. Is there a limit to massive blood transfusion
after severe trauma? Arch Surg. 1998;133:947.
394. Hakala P, Hiippala S, Syrjala M, et al. Massive blood transfusion exceeding 50 units
of plasma poor red cells or whole blood: the survival rate and the occurrence of
leucopenia and acidosis. Injury. 1999;30:619.
395. Vaslef SN, Knudsen NW, Neligan PJ, et al. Massive transfusion exceeding 50 units
of blood products in trauma patients. J Trauma. 2002;53(2):291.
396. Huber-Wagner S, Qvick M, Mussack T, et al. Massive blood transfusion and
outcome in 1062 polytrauma patients: a prospective study based on the trauma registry
of the German Trauma Society. Vox Sang. 2007;92:69.
397. Codner P, Cinat ME. Massive transfusion for trauma is appropriate. Trauma Care,
The Official Publication of ITACCS. 2005;15(3):148.
398. Hirschberg A, Dugas M, Banez EI, et al. Minimizing dilutional coagulopathy in
exsanguinating hemorrhage: a computer simulation. J Trauma. 2003;54:454.
399. Ho AM, Dion PW, Cheng CAY, et al. A mathematical model for fresh frozen plasma
transfusion strategies during major trauma resuscitation with ongoing hemorrhage. Can
J Surg. 2005;48(6):470.
400. Hardy JF, de Moerloose P, Samama CM. The coagulopathy of massive transfusion.
Vox Sang. 2005;89:123.
401. Hardy JF, Moerloose P, Samama CM, et al. Massive transfusion and coagulopathy:
pathophysiology and implications for clinical management. Can J Anesth. 2006;53
(6):S40.
402. Erber WN. Massive blood transfusion in the elective surgical setting. Transfus
Apheresis Sci. 2002;27:83.
Page 92 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

403. Kozek-Langenecker S. Management of massive operative blood loss. Minerva
Anesthesiol. 2007;73:1–15.
404. Silliman CC, Moore EE, Johnson JL, et al. Transfusion of the injured patient:
proceed with caution. Shock. 2004;21(4):291.
405. McIntyre LA, Hebert PC. Can we safely restrict transfusion in trauma patients?
Curr Opin Crit Care. 2006;12:575.
406. Dodd RY, Notari EP, Stramer SL. Current prevalence and incidence of infectious
disease markers and estimated window-period risk in the American Red Cross donor
population. Transfusion. 2002;42:975.
407. Kleinman S, Chan P, Robillard P. Risks associated with transfusion of cellular blood
components in Canada. Transfus Med Rev. 2003;17:120.
408. Blajchmann MA. Incidence and significance of the bacterial contamination of
blood components. Dev Biol (Basel). 2002;108:59.
409. Schreiber GB, Busch MP, Kleinman SH, et al. The risk of transfusion-transmitted
viral infections: the retrovirus epidemiology donor study. N Engl J Med. 1996;334:1685.
410. Zallen G, Offner PJ, Moore EE, et al. Age of transfused blood is an independent
risk factor for postinjury multiple organ failure. Am J Surg. 1999;178:570.
411. Biffl WL, Moore EE, Offner PJ, et al. Plasma from aged stored red blood cells
delays neutrophil apoptosis and primes for cytotoxicity: abrogation by poststorage
washing by not prestorage leukoreduction. J Trauma. 2001;50:426.
412. Offner PJ, Moore EE, Biffl WL, et al. Increased rate of infection associated with
transfusion of old blood after severe injury. Arch Surg. 2002;137:711.
413. Murrell Z, Haukoos JS, Putnam B, et al. The effect of older blood on mortality,
need for ICU care, and the length of stay after major trauma. Am Surg. 2005;71:781.
414. Heddle NM, Soutar RI, Ohoski PL, et al. A prospective study to determine the
Page 93 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

frequency and clinical significance of alloimmunization post-transfusion. Br J
Haematol. 1995;91:1000.
415. Dutton RP, Shih D, Edelman BB, et al. Safety of uncrossmatched Type-O red cells
for resuscitation from hemorrhagic shock. J Trauma. 2005;59:1445.
416. Shaffer LG, Phillips MD. Successful treatment of acquired hemophilia with oral
immunosuppressive therapy. Ann Intern Med. 1997;127:206.
417. Kleinman S, Caulfield T, Chan P, et al. Toward an understanding of transfusion-
related acute lung injury: statement of a consensus panel. Transfusion. 2004;44:1774.
418. Bux J, Sachs UJH. The pathogenesis of transfusion-related acute lung injury. Br J
Haematol. 2007;136:788.
419. Bux J. Transfusion-related acute lung injury (TRALI): a serious adverse event of
blood transfusion. Vox Sang. 2005;89:1.
420. Triulzi DJ. Transfusion-related acute lung injury: an update. Hematol Am Soc
Hematol Educ Program. 2006;497.
421. Curtis BR, McFarland JG. Mechanisms of transfusion-related acute lung injury
(TRALI): anti-leukocyte antibodies. Crit Care Med. 2006;34(Suppl):5118.
422. Zupanska B, Uhrynowska M, Michur H, et al. Transfusion-related acute lung injury
and leucocyte-reacting antibodies. Vox Sang. 2007;93:70.
423. Eder AF, Herron R, Strupp A, et al. Transfusion-related acute lung injury
surveillance (2003-2005) and the potential impact of the selective use of plasma from
male donors in the American Red Cross. Transfusion. 2007;47:599.
424. Gajic O, Gropper MA, Hubmayr RD. Pulmonary edema after transfusion: how to
differentiate transfusion-associated circulatory overload from transfusion-related acute
lung injury. Crit Care Med. 2006;34(Suppl):S109.
425. Swanson K, Dwyre DM, Krochmal J, et al. Transfusion-related acute lung injury
Page 94 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

(TRALI): current clinical and pathophysiologic considerations. Lung. 2006;184:177.
426. Dutton RP, McCunn M, Hyder M, et al. Factor VIIa for correction of traumatic
coagulopathy. J Trauma. 2004;57(4):709.
427. Boffard KD, Riou B, Warren B, et al. Recombinant factor VIIa as adjunctive
therapy for bleeding control in severely injured trauma patients: two parallel
randomized, placebo-controlled, double-blind clinical trials. J Trauma. 2005;59:8.
428. Rizoli SB, Boffard KD, Riou B, et al. Recombinant activated factor VII as an
adjunctive therapy for bleeding control in severe trauma patients with coagulopathy:
subgroup analysis from two randomized trials. Crit Care. 2006;10:R178.
429. Perkins JG, Schreiber MA, Wade CE, et al. Early versus late recombinant factor
VIIa in combat trauma patients requiring massive transfusion. J Trauma. 2007;62:1095.
430. Harrison TD, Laskosky J, Jazaeri O, et al. “Low dose” recombinant activated
factor VII results in less blood and blood product use in traumatic hemorrhage. J
Trauma. 2005;59:150.
431. Stein DM, Dutton RP, O'Connor J, et al. Determinants of futility of administration
of recombinant factor VIIa in trauma. J Trauma. 2005;59:609.
432. Martinowitz U, Michaelson M. Guidelines for the use of recombinant activated
factor VII (rFVIIa) in uncontrolled bleeding: a report by the Israeli Multidisciplinary
rFVIIa Task Force. J Thromb Haemost. 2005;3:640.
433. Rizoli SB, Nascimento B, Osman F, et al. Recombinant activated coagulation factor
VII and bleeding trauma patients. J Trauma. 2006;61:1419.
434. Lodge JPA, Jonas S, Jones RM, et al. Efficacy and safety of repeated perioperative
doses of recombinant factor VIIa in liver transplantation. Liver Transpl. 2005;11:973.
435. Filsoufi F, Castillo JG, Rahmanian PB, et al. Effective management of refractory
postcardiotomy bleeding with the use of recombinant activated factor VII. Ann Thorac
Surg. 2006;82:1779.
Page 95 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

436. Diprose P, Herbertson MJ, O'Shaughnessy D, et al. Activated recombinant factor
VII after cardiopulmonary bypass reduces allogeneic transfusion in complex non-
coronary cardiac surgery: randomized double-blind placebo controlled pilot study. Br J
Anaesth. 2005;95(5):596.
437. Grounds RM, Seebach C, Knothe C, et al. Use of recombinant factor VII
(Novoseven) in trauma and surgery: analysis of outcomes reported to an international
society. J Intensive Care Med. 2006;21:27.
438. Vincent JL, Rossaint R, Riou B, et al. Recommendations on the use of recombinant
activated factor VII as an adjunctive treatment for massive bleeding—a European
perspective. Crit Care. 2006;10:R120.
439. Scarpelini S, Rizoli S. Recombinant factor VIIa and the surgical patient. Curr Opin
Crit Care. 2006;12:351.
440. Kaw LL, Coimbra R, Potenza BM, et al. The use of recombinant factor VIIa for
severe intractable bleeding during spine surgery. Spine. 2004;29:1384.
441. Shao YF, Yang JM, Chau GY, et al. Safety and hemostatic effect of recombinant
activated factor VII in cirrhotic patients undergoing partial hepatectomy: a
multicenter, randomized, double-blind, placebo-controlled trial. Am J Surg.
2006;191:245.
442. Friederich PW, Henry CP, Messelink EJ, et al. Effect of recombinant activated
factor VII on perioperative blood loss in patients undergoing retropubic prostatectomy:
a double-blind placebo-controlled randomized trial. Lancet. 2003;361:201.
443. Bosch J, Thabut D, Bendtsen F, et al. Recombinant factor VIIa for upper
gastrointestinal bleeding in patients with cirrhosis: a randomized, double-blind, trial.
Gastroenterology. 2004;127:1123.
444. Aledort LM. Comparative thrombotic event incidence after infusion of
recombinant factor VIIa versus factor VIII inhibitor bypass activity. J Thromb Haemost.
2004;2:1700.
445. Roberts HR, Monroe DM III, Hoffman M. Safety profile of recombinant factor VIIa.
P.923
Page 96 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

Semin Hematol. 2004;41(1 Suppl 1):101.
446. Levi M, Peters M, Buller HR. Efficacy and safety of recombinant factor VIIa for
treatment of severe bleeding: a systematic review. Crit Care Med. 2005;33:883.
447. Mannucci PM, Levi M. Prevention and treatment of major blood loss. N Engl J Med.
2007;356:2301.
448. Brown JR, Birkmeyer NJO, O'Connor GT. Meta-analysis comparing the
effectiveness and adverse outcomes of antifibrinolytic agents in cardiac surgery.
Circulation. 2007;115:2801.
449. Mangano DT, Tudor JC, Dietzel C, et al. The risk associated with aprotinin in
cardiac surgery. N Engl J Med. 2006;354:353.
450. Mangano DT, Miao Y, Vuylsteke A, et al. Mortality associated with aprotinin during
5 years following coronary artery bypass graft surgery. JAMA. 2007;297(5):471.
451. Bridges CR. Valid comparisons of antifibrinolytic agents used in cardiac surgery.
Circulation. 2007;115:2790.
452. Henry DA, Moxey AJ, Carless PA, et al. Anti-fibrinolytic use for minimizing
perioperative allogeneic blood transfusion. Cochrane Database Syst Rev.
2001;1:CD001886.
453. Coats T, Roberts I, Shakur H. Antifibrinolytic drugs for acute traumatic injury
(review). Cochrane Database Syst Rev. 2004;4:CD004896.
454. Coats T, Hunt B, Roberts I, et al. Antifibrinolytic agents in traumatic hemorrhage:
a large-scale randomized controlled trial is needed. PLoS Med. 2005;2(3):e64.
455. Ness PM, Cushing MM. Oxygen therapeutics: pursuit of an alternative to the donor
red blood cell. Arch Pathol Lab Med. 2007;131:734.
456. Jahr JS, Walker V, Manoochehri K. Blood substitutes as pharmacotherapies in
clinical practice. Curr Opin Anaesthesiol. 2007;20:235.
Page 97 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

457. Moore EE, Johnson JL, Cheng AM, et al. Insights from studies of blood substitutes
in trauma. Shock. 2005;24(3):197.
458. Bulger EM, Cuschieri J, Warner K, et al. Hypertonic resuscitation modulates the
inflammatory response in patients with traumatic hemorrhagic shock. Ann Surg.
2007;245(4):635.
459. Holcroft JW, Vassar MJ, Perry CA. Use of 7.5% NaCl/6% Dextran 70 solution in the
resuscitation of injured patients in the emergency room. Prog Clin Biol Res.
1989;299:331.
460. Mattox KL, Maningas PA, Moore EE, et al. Prehospital hypertonic saline/dextran
infusion for post-traumatic hypotension: the USA multicenter trial. Ann Surg.
1991;213:482.
461. Vassar MJ, Perry CA, Gannaway WL, et al. 7.5% sodium chloride/dextran for
resuscitation of trauma patients undergoing helicopter transport. Arch Surg.
1991;126:1065.
462. Younes RN, Aun F, Accioly CQ, et al. Hypertonic solutions in the treatment of
hypovolemic shock: a prospective randomized study in patients admitted to the
emergency room. Surgery. 1992;111:380.
463. Vassar MJ, Fischer RP, O'Brien PE, et al. A multicenter trial for resuscitation of
injured patients with 7.5% sodium chloride: the effect of added dextran 70. The
Multicenter Group for the Study of Hypertonic Saline in Trauma Patients. Arch Surg.
1993;128:1003.
464. Cooper DJ, Myles PS, McDermott FT, et al. Prehospital hypertonic saline
resuscitation of patients with hypotension and severe traumatic brain injury: a
randomized controlled trial. JAMA. 2004;291:1350.
465. Tyagi R, Donaldson K, Loftus CM. Hypertonic saline: a clinical review. Neurosurg
Rev. 2007;30:277.
466. Tseng MY, Al-Rawi PG, Czosnyka M, et al. Enhancement of cerebral blood flow
using systemic hypertonic saline therapy improves outcome in patient with poor-grade
Page 98 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

spontaneous subarachnoid hemorrhage. J Neurosurg. 2007;107(2):274.
467. Kolsen-Petersen JA. Immune effect of hypertonic saline: fact or fiction? Acta
Anaesthesiol Scand. 2004;48:667.
468. Junger WG, Coimbra R, Liu FC, et al. Hypertonic saline resuscitation: a tool to
modulate immune function in trauma patients? Shock. 1997;8:235.
469. Homma H, Deitch EA, Feketeova E, et al. Small volume resuscitation with
hypertonic saline is more effective in ameliorating trauma-hemorrhagic shock-induced
lung injury, neutrophil-activation, and red blood cell dysfunction than pancreatic
protease inhibition. J Trauma. 2005;59:266.
470. Coimbra R, Loomis W, Melbostad H, et al. Role of hypertonic saline and
pentoxifylline on neutrophil activation and tumor necrosis factor-alpha synthesis: a
novel resuscitation strategy. J Trauma. 2005;59(2):257.
471. Rotstein O. Novel strategies for immunomodulation after trauma: revisiting
hypertonic saline as a resuscitation strategy for hemorrhagic shock. J Trauma.
2000;49:580.
472. Deree J, Martins JO, Leedom A, et al. Hypertonic saline and pentoxifylline reduces
hemorrhagic shock resuscitation-induced pulmonary inflammation through attenuation
of neutrophil degranulation and proinflammatory mediator synthesis. J Trauma.
2007;62(1):104.
473. Cryer HM, Gosche J, Harbrecht J, et al. The effect of hypertonic saline
resuscitation on responses to severe hemorrhagic shock by the skeletal muscle,
intestinal, and renal microcirculation systems: seeing is believing. Am J Surg.
2005;190:305.
474. Wade C, Grady J, Kramer G. Efficacy of hypertonic saline dextran (HSD) in
patients with traumatic hypotension: meta-analysis of individual patient data. Acta
Anaesthesiol Scand Suppl. 1997;110:77.
475. Wade CE, Grady JJ, Kramer GC. Efficacy of hypertonic saline dextran fluid
resuscitation for patient with hypotension and penetrating trauma. J Trauma. 2004;54
Page 99 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...

(Suppl 5):144.
476. Wade CE, Grady JJ, Kramer GC. Individual patient cohort analysis of the efficacy
of hypertonic saline/dextran in patients with traumatic brain injury. J Trauma. 1997;42
(Suppl 5):61.
477. Wade CE, Kramer GC, Grady JJ, et al. Efficacy of hypertonic 7.5% saline and 6%
dextran-70 in treating trauma: a meta-analysis of controlled clinical studies. Surgery.
1997;122:609.
478. Alam HB, Koustova E, Rhee P. Combat casualty care research: from bench to the
battlefield. World J Surg. 2005;29:S7.
P.924
Page 100 of 100Ovid: Civetta, Taylor, & Kirby's: Critical Care
27/09/2010mk:@MSITStore:C:\Documents%20and%20Settings\GERARDO%20AVI...