







Languages
Pages
Legal


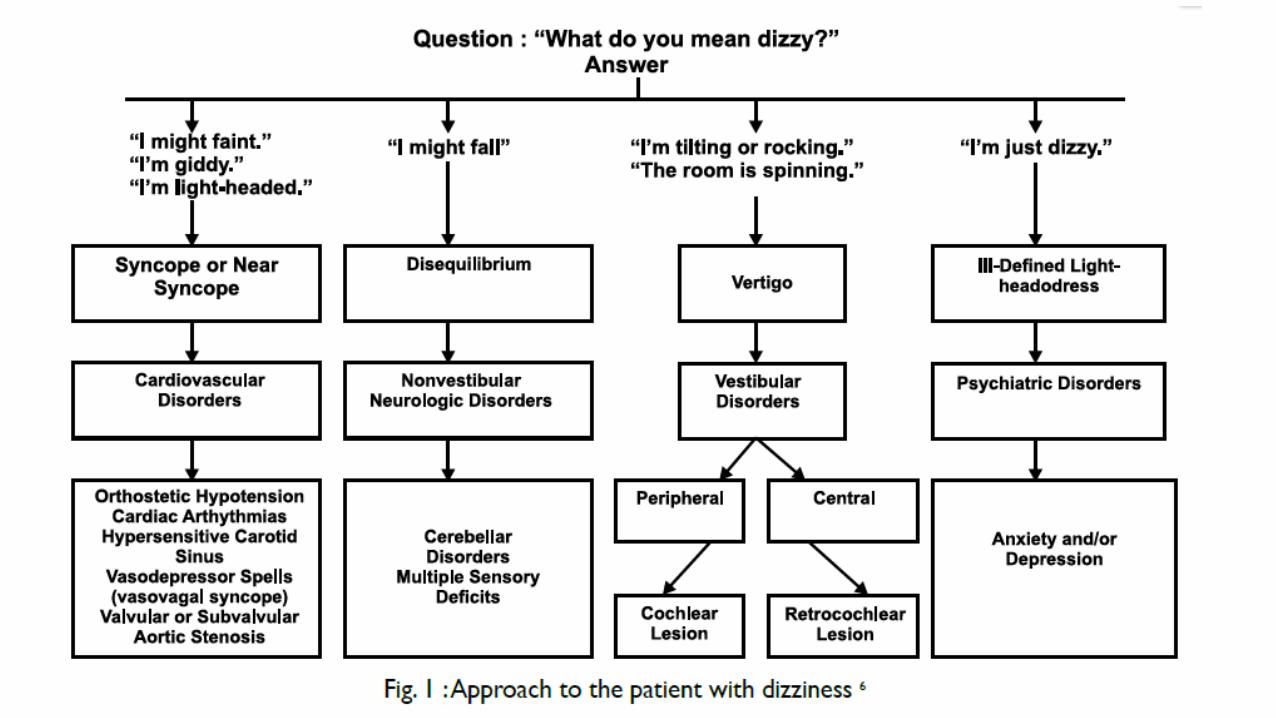
CENTRAL VERTIGO

Central vertigo
• caused by dysfunction of central structures that process sensory input
from the inner ear.

CASE SCENARIO
A 60 yr old gentleman was brought to the casualty with complaints of
• sudden onset of dizziness with him feeling the perception of the
surroundings revolving about him of two hours duration
• nausea and vomiting at the time of onset
• had difficulty in sitting up in the bed and had to be given support to
go to the bathroom
• He is a known hypertensive and diabetic

• On examination he had :-
• Nystagmus
• Motor ataxia – Towards the right side
• Right palate, pharynx and laryngeal paresis
• loss of pain and temperature on right half of the face and left half
of the body


8
Wallenberg Syndrome
• Occlusion of posterior inferior cerebellar artery
• Relatively common cause of central vertigo
• Associated Symptoms:
• nausea
• Vomiting
• Nystagmus
• ataxia
• Horner syndrome
• palate, pharynx and laryngeal paresis
• loss of pain and temperature on ipsilateral face and contralateral body

9



• The brainstem, cerebellum, and peripheral labyrinths - all supplied by
the vertebrobasilar arterial system.
• Central and peripheral ischemic vertigo syndromes may
overlap






Brainstem/cerebellar infarct
• Abrupt onset
>24hrs vs minutes
Brainstem ischemia
• accompanied by other neurological signs and symptoms
• motor and sensory pathways are in close proximity to vestibular
pathways.

Cerebellar Ischemia
• vertigo as the most prominent or only symptom
• Acute-onset vertigo - MRI study to rule out cerebellar infarction.
• Oculomotor testing can show:
1- Pure unidirectional nystagmus
2- Direction-changing gaze evoked nystagmus
3- Impaired smooth pursuit
4- Overshooting saccades



ManagementThrombolysis
Antiplatelets
Physiotherapy
Occupational therapy

24
Cerebellar Hemorrhage
• Neurosurgical emergency
• Suspected in any patient with sudden onset headache, vertigo, vomiting and
ataxia
• May have gaze preference
• Motor-sensory exam usually normal
• Gait disturbance often not recognized because patient appears too ill to
move


Patients who are at risk for deterioration
• Admission systolic blood pressure greater than 200 mm Hg
• Pinpoint pupils and abnormal corneal and oculocephalic reflexes
• Hemorrhage extending into the cerebellar vermis
• Hematoma diameter greater than 30 mm
• Brainstem distortion
• Intraventricular hemorrhage
• Acute hydrocephalus
• Emergency management
• Oxygen support – Endotracheal intubation if necessary
• Atropine – bradycardia 2° to Cushing’s Reflex
• Surgical management

28
Sub-clavian Steal Syndrome
• Rare, but treatable
• Arm exercise on side of stenotic subclavian artery usually causes symptoms of
intermittent claudication
• Blood is shunted into the ipsilateral upper limb by the vertebral artery into the
subclavian artery from the opposite vertebral artery and basilar artery.
• Hence the brainstem suffers from ischaemia
Multiple Sclerosis• Subacute onset• Duration - Minutes-wks
• 5% of patients with MS report vertigo as an initial symptom.
• Vertigo may be rotatory with a positional component
• Diplopia, facial paraesthesia and weakness may co-exist
• 0ccasionally patients show typical peripheral vestibular nystagmus -
The lesion affects the root entry zone of the vestibular nerve.

Eye signs in MS patients with vertigo :-
• Nystagmus
• Internuclear ophthalmoplegia is characteristic
• Abnormal saccades
• Impaired pursuit
• Impaired convergence



Treatment
Chronic Disease:-• Interferon β-1α• Glatrimer Acetate• Mitoxantrone• Fingolamide
Acute attacks :-• High dose
corticosteroids – Methyl prednisolone
• Plasmapharesis

Cranio Vertebral Junction Anomalies
I. Bony AnomaliesA. Major Anomalies
1. Platybasia2. Occipitalization3. Basilar Invagination4. Dens Dysplasia5. Atlanto- axial dis.
B. Minor Anomalies1. Dysplasia of Atlas2. Dysplasia of
occipital condyles, clivus, etc.
II. Soft Tissue anomalies1. Arnold-Chiari Malformation2. Syringomyelia/ Syringobulbia

Chiari malformation
• The brainstem and cerebellum are elongated downward into the
cervical canal - pressure on both the caudal midline cerebellum and
the cervicomedullary junction.
• Spontaneous or positional downbeat nystagmus
• central nystagmus can also occur.

• Dysphagia, hoarseness, and dysarthria - stretching of the lower cranial
nerves
• obstructive hydrocephalus - occlusion of the basilar cisterns.

• Sagittal and coronal MRI images of Chiari type I malformation.
• descent of cerebellar tonsils (T) below the level of foramen magnum (white line) down to the level of C1 posterior arch (asterisk).

Management
Duraplasty with pericranial graft• The duraplasty - additional room for
cerebellar tonsils at the craniocervical junction, while achieving closure of dura and prevention of cerebrospinal fluid leak.


Central Nervous System Tumors
• The most common -gliomas in adults and medulloblastoma in
children.
• Ocular motor dysfunction (impaired smooth pursuit, overshooting
saccades), impaired coordination, and other central nervous system
• An early finding - central positional nystagmus.

41
Acoustic Neuroma
• Peripheral Vertigo With Central Manifestations
• Tumor Of The Schwann Cells Around The 8th Cn
• Vertigo With Hearing Loss And Tinnitus
• Earliest Sign Is Decreased Corneal Reflex
• Later Truncal Ataxia

Neurodegenerative disorder
• Onset - Spontaneous or positionally triggered
• Parkinsonism
• Progressive supranuclear palsy
• Multi-system atrophy
• spinocerebellar ataxia involving cerebellum and brainstem.

Epilepsy
• Vestibular symptoms are common with focal seizures, particularly
those originating from the temporal and parietal lobes.
• The key to differentiate vertigo with seizures from other causes of
vertigo - association of seizures with an altered level of consciousness.
• Episodic vertigo as an isolated manifestation of a focal seizure is a
rarity, if it occurs at all.

Familial ataxia syndromes
• Onset - Acute-subacute, episodic type with stress, exercise
• Duration - hours
• Vestibular symptoms and signs –
• spinocerebellar ataxia types 1, 2, 3, 6, and 7
• Friedreich's ataxia
• Refsum's disease
• episodic ataxia (EA) types 2, 3, 4, and 5

• The positional vertigo and nystagmus can be the initial symptom
• the symptoms are slowly progressive, with the cerebellar ataxia and
incoordination later overshadowing the vestibular symptoms.
• Attacks of vertigo may occur in up to half of patients with SCA6 many
of which are positionally triggered
• Persistent down-beating nystagmus often is seen in patients placed in
the head-hanging position


Management
• no known cure for spinocerebellar ataxia• directed towards alleviating symptoms• Physical therapy

Basilar Migraine
• heterogeneous genetic disorder characterized by headaches in addition to many other
neurological symptoms
• Benign recurrent vertigo may be considered as a migraine equivalent
• Onset - With typical migraine triggers
• Duration from hours to days
• + family history
• Normal neurological exam
• No progressive hearing loss
• Some patients - auditory symptoms similar to Meniere's disease, and
a mild hearing loss also may be evident on the audiogram
• The key factor distinguishing between migraine and Meniere's disease
is the lack of progressive unilateral hearing loss
• Positional vertigo also may occur in patients with migraine
• diagnosis of migraine-associated dizziness remains one of exclusion

References
1. Bradley: Neurology in Clinical Practice, 5th ed.
2. Adams and Victors Priniciples of Neurology , 9th ed.
3. Harrison's Principles of Internal Medicine, 18th ed.
4. Practical Neurology, 3rd Edition
Top Related