Makalah Vertigo
24
VERTIGO CASE REPORT Presented by : dr. Desin Pambudi Sejahtera Moderator : Dr. dr. Cempaka Thursina Srie, Sp.S(K) Examiners : Prof. Dr. dr. Sri Sutarni Sudarmadji, Sp.S(K) dr. Atitya Khairani, M.Sc., Sp.S Thursday, June 11 th , 2015 At 12.30 – 13.30 pm IDENTITY Name : Mrs. K Age : 66 years old Sex : Female Religion : Moslem Occupation : Housewife Education : Senior High School Address : Paseban, Bayat, Klaten Marital status : Married Date of addmission : May 13 th 2015 MR No : 01.72.87.xx ANAMNESIS (May 15 th 2015) Obtained from the patient (autoanamnesis) and her husband (alloanamnesis) Chief complaint : Abnormal sensation of rotation/movement of patient’s environment The history of present illness : Two weeks before admission, patient suddenly felt the rotation sensation of her environment. The intensity was moderate to severe. There was nausea but no vomitus. Patient denied: worsening of the rotation sensation when she changed the position of the head, decreasing rotation sensation when she closed her eyes, previous head trauma, uncounciousness, seizure, fever, ringing sound sensation in the ear, ear infection, clogged ear, decrease in hearing, ear discharge, skewed lips, lisp speech, limb weakness, psychososial stressor. Patient consulted to emergency department in Soejarwadi District Hospital. She was 1
-
Upload
marissa-ayu-anindyta -
Category
Documents
-
view
284 -
download
1
Transcript of Makalah Vertigo

VERTIGO CASE REPORTPresented by : dr. Desin Pambudi SejahteraModerator : Dr. dr. Cempaka Thursina Srie, Sp.S(K)Examiners : Prof. Dr. dr. Sri Sutarni Sudarmadji, Sp.S(K)
dr. Atitya Khairani, M.Sc., Sp.SThursday, June 11th, 2015At 12.30 – 13.30 pm
IDENTITYName : Mrs. KAge : 66 years oldSex : FemaleReligion : MoslemOccupation : HousewifeEducation : Senior High SchoolAddress : Paseban, Bayat, KlatenMarital status : MarriedDate of addmission : May 13th 2015MR No : 01.72.87.xxANAMNESIS (May 15th 2015)Obtained from the patient (autoanamnesis) and her husband (alloanamnesis)Chief complaint : Abnormal sensation of rotation/movement of patient’s environmentThe history of present illness :
Two weeks before admission, patient suddenly felt the rotation sensation of her environment. The intensity was moderate to severe. There was nausea but no vomitus. Patient denied: worsening of the rotation sensation when she changed the position of the head, decreasing rotation sensation when she closed her eyes, previous head trauma, uncounciousness, seizure, fever, ringing sound sensation in the ear, ear infection, clogged ear, decrease in hearing, ear discharge, skewed lips, lisp speech, limb weakness, psychososial stressor. Patient consulted to emergency department in Soejarwadi District Hospital. She was admitted to the hospital ward, examined with Head CT Scan dan diagnosed with vertigo. Patient given some medications which the patient didn’t remember the name. The rotation sensation did not reduced. Five days after admitted in this hospital, patient went home but the rotational sensation was still present. The intensity of the sensation was mild to moderate
Day of admission, the rotational sensation was still present. There was nausea without vomitus. The intensity of the sensation was moderate to severe. Patient denied: worsening of the rotation sensation when she changed the position of her head, decreasing of the sensation when she closed her eyes, previous head trauma, uncounciousness, seizure, fever, ringing sound sensation in the ear, ear infection, clogged ear, decrease in hearing, ear discharge, throbbing headache, skewed lips, lisp speech, limb weakness, psychososial stressor. Patient went to Sardjito Hospital Emergency Department and entered the Neurology Ward.
1

The history of previous illnessess1. There were history of :
a. Hypertension, approximately 10 years, with average systolic blood pressure approximately 150 mmHg, uncontrolled to physician
b. Diabetes melitus since 20 years ago without appropriate medication.c. No history of :
Previous vertigo, Head trauma, Tumor, chemo and radiotherapyChronic cough, cough treatment for 6 months, night sweats, subfebrile fever, bloody cough, Ear, nose, and teeth infectionHypercholesterolemia, heart disease, stroke, smoking.
The history of family illnessessHistory of stroke in father. The Psychosocial aspect:She was a grandmother with 4 grandchild from 2 sons and a daughter. Living with her husband, and her family in good conditions. Economic level was middle and her insurance with BPJS Non PBISystemic evaluation
Cerebrospinal system : sudden rotational sensation, lasting for two weeks, accompanied with nausea. The sensation did not reduced with eye closed and did not get worse with head position changing.
Cardiovascular system : uncontrolled hypertension Respiratory system : normal Gastrointestinal system : nausea Urogenital system : normal Musculoskeletal system : normal Integumental system : normal Endocrine system : uncontrolled diabetic
Summary of anamnesisFemale patient, 66 years old, came to Sardjito Hospital Emergency Department with the
chief complaint of rotational sensation with nausea which lasting for two weeks. The rotational sensation was decreased after patient took medication from previous hospital but it has no got better. The intensity was moderate to severe. The sensation did not get better with eye closing and did not get worse with head position changing. There is a history of uncontrolled hypertension and diabetic.
FIRST DISCUSSIONDizziness and vertigo are among the most common symptoms causing patients to visit a
physician (as common as back pain and headaches). The overall incidence of dizziness, vertigo, and imbalance is 5-10%, and it reaches 40% in patients older than 40 years. The incidence of falling is 25% in subjects older than 65 years. Falling can be a direct consequence of dizziness in this population, and the risk is compounded in those with other neurologic deficits. A report reviewing presentation to US emergency departments from 1995-2004 indicated that vertigo and dizziness accounted for 2.5% of presentations (Kerber et al., 2008)
2
Mild hearing loss is the most common disability in the United States and worldwide. The incidence of hearing loss is 25% in people younger than 25 years, and it reaches 40% in persons older than 40 years. About 25% of the population report tinnitus. Vertigo, dizziness, tinnitus, and hearing loss are typically associated with inner-ear diseases as opposed to CNS diseases. Migraine is more prevalent (10%) than Ménière disease (< 1%). About 40% of patients with migraine have vertigo, motion sickness, and mild hearing loss. Therefore, differentiating migraine from primary inner-ear disorders is sometimes difficult.
The role of the primary care physician and the neurologist in treating patients with dizziness or vertigo has increased over the last decade. Emphasis is on differentiating peripheral from central dizziness.
The patient's history is critical in the evaluation of the patient with dizziness. Ask the patient to describe their symptoms by using words other than "dizzy." The rationale for using other words is that patients may use dizzy nonspecifically to describe vertigo, unsteadiness, generalized weakness, syncope, presyncope, or falling.
Dizziness includes light-headedness, unsteadiness, motion intolerance, imbalance, floating, or a tilting sensation. A critical distinction is differentiating vertigo, which is a subtype of dizziness, defined as an illusion of movement caused by asymmetric input of the vestibular system, from other types of dizziness. This dichotomy is helpful because true vertigo is often due to inner-ear disease, whereas other symptoms of dizziness may be due to CNS, cardiovascular, or systemic diseases.
Sudden onset and vivid memory of vertiginous episodes are often due to inner-ear disease, especially if hearing loss, ear pressure, or tinnitus is also present. Gradual and ill-defined symptoms are common in CNS, cardiac, and systemic diseases. The time course of vertigo is also important. Episodic true vertigo that lasts for seconds and is associated with head or body position changes is probably due to benign paroxysmal positional vertigo (BPPV). Vertigo that lasts for hours or days is probably caused by Ménière disease (if associated with hydropic ear symptoms) or vestibular neuronitis (if hydropic ear symptoms are absent). Vertigo of sudden onset that lasts for minutes can be due to brain or vascular disease, especially if cerebrovascular risk factors are present.
Central vertigo secondary to brainstem or cerebellar ischemia usually lasts for 20 min to 24 h and is often associated with other brainstem characteristics, including diplopia, autonomic symptoms, nausea, dysarthria, dysphagia, or focal weakness. Patients with cerebellar disease are frequently unable to ambulate during acute episodes of vertigo. Patients with peripheral vertigo can usually ambulate during episodes and are consciously aware of their environment. A history of headaches, especially migraine headaches, can be associated with migraine-related dizziness. Previous viral illness, cold sores, or sensory changes in the cervical C2-C3 or trigeminal distributions usually indicate vestibular neuronitis or recurrent episodes of Ménière disease.
Dysdiadochokinesis and gait ataxia during episodes are more likely due to cerebellar diseases, especially in the elderly and in subjects with evident cardiovascular risk factors. Sensory and motor symptoms and signs are usually associated with CNS diseases. The history should include a review of systems (especially head trauma and ear diseases, trauma, or surgery). The impact of dizziness on activities of daily living at work and home should be addressed. Screening
3

for primary or reactive anxiety and depression is important. History of prescription medicines, over-the-counter medications, herbal medicines, and recreational drugs (including smoking and alcohol) can help to identify pharmacologically induced syndromes. Accurate diagnosis of dizziness or unsteadiness in the elderly may be more difficult mostly because of atypical presentation of underlying disorders. Although dizziness in the elderly can be attributed to weakness and fatigue at times, it may be more serious than in younger patients and should be carefully investigated. To diagnose dizziness, physicians must use the essential tools of history, clinical examination, and follow-up (Katsarkas , 2008).
Temporary diagnosis :Clinical diagnosis : Acute rotational sensation, nauseaTopical diagnosis : Organon vestibular central dd periferEtiological diagnosis :
1. Central : Vascular (Susp. Vertebrobasilar stroke dd vertebrobasilar artery insufficiency)2. Perifer 3. Mixed type
PHYSICAL EXAMINATION General status
General ConditionConsciousnessBMIVAS/ NPSBlood pressurePulseRespiratory rateTemperature
HeadNeck
ChestHeart
LungAbdomenExtremities
: Moderate: Compos mentis (GCS :E4,V5,M6): 26,66 (BB: 60Kg; TB: 150cm): 2/ 0: 150/90 mm Hg: 84 x/minute, regular: 16 x/minute, regular: 36,7 oC: Anemic conjunctival (-), icteric of sclerae (-): Jugular Vein pressure normal, no carotid bruit: No sign of inflammation or enlargement of thyroid gland within normal limit, mass (-)
: normal cor configuration, S1 and S2 regular, murmur (-), gallop (-)
: sonor, vesicular, ronchi (-): unpalpable liver and spleen, no tenderness, normal peristaltic: no edema
Neurobehavioural status: Alertness : alertBehavioural observations
1. History of behavioural changes : none2. Mental status
General behaviour : good Fluency : fluent
4

Mood and emotional change : none
Mind state : realistic Intelectual capasity : good enough Sensorium
a. Consciousness : compos mentisb. Attention : good enoughc. Orientation : good enoughd. Short term memory : good enoughe. Long-term memory : good enough
Calculation : good enough Visuospatial function : good enough Denial or neglect : (-) Apraxia : (-) MMSE : 29/30
Neurological ExaminationsConsciousnessHead & eye
Neck
: fully allert, GCS E4V5M6: mesocephal isochoric pupil, Ø 3mm/3mm light reflex +/+, corneal reflex +/+,
nistagmus horizontal : +/+, vertical +/+,pendular +/+, rotatoar +/+ slurred speech (+)
: meningeal sign (-)
Description of cranial nervesRight Left
N.I Smelling Wnl Wnl
N.II
Visual Function >3/60 >3/60
Visual Field Wnl Wnl
Colour Vision Wnl Wnl
N.III
Ptosis (-) (-)
Eye’s motion to medial Wnl Limited
Eye’s motion to below Wnl Limited
Eye’s motion to above Wnl Limited
Pupil 3 mm 3 mm
Kind of pupil Round Round
Direct of light reflex (+) (+)
Indirect of light reflex (+) (+)
Accomodation reflex (+) (+)
N.IV
Strabismus divergen (-) (-)
Eye’s motion to medial below (+) (+)
Strabismus konvergen (-) (-)
N.V Biting Wnl Wnl
Open mouth Wnl Wnl
Sensibility of face Wnl Wnl
Corneal reflex Wnl Wnl
5

Trismus (-) (-)
N.VI
Eye’s motion to lateral (+) (+)
Strabismus konvergen (-) (-)
Diplopia (-)
N.VII
Blinking (+) (+)
Nasolabial Fold Symmetrical
The angle of the mouth Symmetrical
Wrinkling of the forehead Symmetrical
Eye closure Wnl Wnl
Puffing cheek Symmetrical
Whistle (-) (-)
Taste on the 2/3 anterior of the tongue
Wnl Wnl
N.VIII
Hearing of the whispered voice, watch ticking
Normal Normal
Rinne (+) (+)
Weber No lateralization
Schwabah Normal Normal
Nystagmus (-) (-)
N.IX
Arcus pharyngeal Wnl Wnl
Taste on the 1/3 posterior of the tongue
Wnl Wnl
Vomiting Reflex (+)
Pronouncing the lingual (+)
Retching (+)
N.X
Pulse per minute 84x/mnt 84x/mnt
Arcus pharyngeal Wnl Wnl
Swallowing Wnl
NXI
Head Turning Wnl Wnl
Shoulder position Wnl Wnl
Shoulder elevation (+) (+)
Trophy of shoulder muscles Eutrophy Eutrophy
N.XII
Tongue position Wnl
Tremor of tounge (-) (-)
Tounge protraction Wnl
Trophy of tounge’s muscle Eutrophy Eutrophy
Fasiculation of tounge (-) (-)
Extremity
Movement Free Free Streng 5/5/5 5/5/5 RF 2+ 2+
Free Free 5/5/5 5/5/5 2+ 2+
RP - - Tn N N Tr E E Cl -/ -
- - N N E E Sensibility
6

Protophatic pain wnl temperature wnlPropioceptive pressure wnl
vibration wnl position wnl
discrimination wnl
Nistagmus horizontal : +/+Nistagmus vertical : +/+Nistagmus rotatoar : +/+Dismetri :(+)Disdiadokokinesis :(+)Rebound phenomenon : (+)Slurred speech : (+)Romberg test (opened) : (+)Tandem gait : (+)Fukuda : (+)Ataxia : (+)Fungsi Vegetatif : micturition, defecation wnl
Supporting examination:Laboratory findings
13-05-2015 14-05-2015 18-05-2015Hb (g/dL) 14,5 13,3Hct (%) 44,2 45,2RBC (106/mm3) 5,10 5,90WBC(103/mm3) 9,46 11,6PLT (103/mm3) 366 286Neut (%)LymphMonoEosBaso
82,613,21,81,00,3
72,623,21,51,00,6
KED (mm/jam) 8 (0-15)Na (mmol/L) 137 136K (mmol/L) 3,4 3,2Cl (mmol/L) 98 103GDN (mg/dL) 227 259
GD2JPP (mg/dL) 312HbA1C (%) 6,4Chol total (mg/dl) 189HDL (mg/dL) 35LDL (mg/dL) 45
7

TG (mg/dL) 125BUN (mg/dL) 16Cre (mg/dL) 0,9Uric (mg/dL)SGOT 50SGPT 21UrinalisisGlu -Pro -Bil -Uro NormalpH 6,0SG >1.030Bld -Ket -Nit -Leu -Color Light yellowSedimentLP 0LG 0Eritrosit 0Epitel 0
Electrocardiography Result : normal sinus rythm, HR 90 x/minuteRadiologic findings Chest X ray : NormalHead CT Scan
8

9

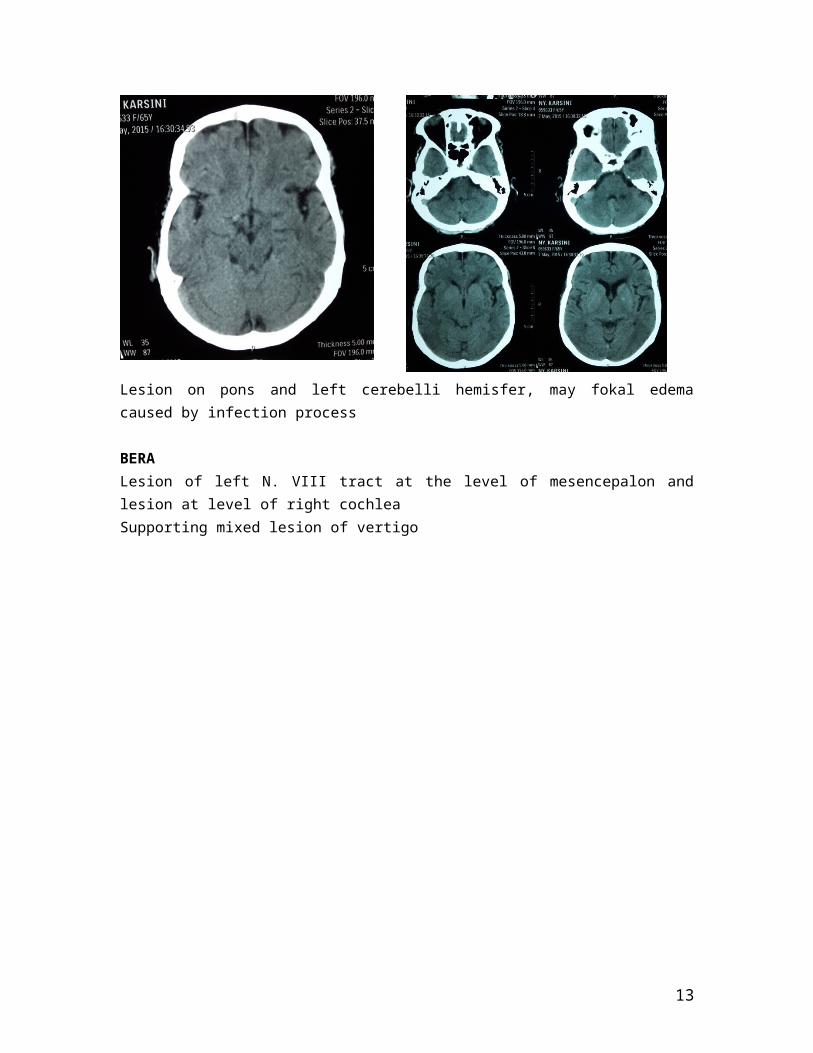
Lesion on pons and left cerebelli hemisfer, may fokal edema caused by infection process
BERALesion of left N. VIII tract at the level of mesencepalon and lesion at level of right cochleaSupporting mixed lesion of vertigo
10

Consult to others department:Internal Department:Diagnose:
- DM2O- Hipertension- Observasi vertigo
Therapy:- Novorapid 8-8-8- Amlodipin 10mg/ 24jam- Valsartan 80mg/ 24 jam
NeuroImaging:Hypodence lesion at border of mesencephalon and left pons.Hypodence lesion on left cerebellum.Suspecsious of infarction on both area.
11

RESUME OF EXAMINATION General status : moderate,compos mentis Vital sign : blood pressure 150/90 mmHg, pulse : 84x/minute, respiratory rate 16
x/minute, temperature 36,7 C VAS : 2, NPS: 0 Neurobehavior status is within normal limit Neurological status :
Cranial nerve examination parese of left 3rd Cranial Nerve Nistagmus horizontal : +/+ Nistagmus vertical : +/+ Nistagmus rotatoar : +/+ Dismetri : (+) Disdiadokokinesis : (+) Rebound phenomenon : (+) Slurred speech : (+) Romberg test : (+) Tandem gait : (+) Fukuda : (+) Ataxia : (+)
Head CT Scan : Hypodence lesion at border of mesencephalon and left pons. Hypodence lesion on left cerebellum. Susp of infarction on both area.
Chest X ray : Normal ECG : normal sinus rythm, HR 90 bpm. BERA: Lesion of left N. VIII tract at the level of mesncepalon and lesion at level of right
cochlea. Supporting mixed lesion of vertigo
SECOND DISCUSSIONIn patients with dizziness, general examination should emphasize vital signs, supine and
standing blood-pressure measurement, and evaluation of the cardiovascular and neurologic systems. Examine the ears for visible infection or inflammation of the external or middle ear. Test hearing and discrimination by using a tuning fork and by whispering and asking the patient to repeat heard words. Examine the neck for range of motion and flexibility. Focused neurologic examination of the cranial nerves, motor and sensory modalities, gait, and stance is important in initial visit. Cerebellar tests, especially failure of fixation suppression of vestibular eye movements, are important for checking the vestibulocerebellum. Failure of fixation suppression can be tested by asking the patient to stretch his arms and look at his thumb while being passively rotated (manual rotation of examination chair). A visible nystagmus (right or left) indicates failure of fixation suppression that is always central in origin.
Central vertigo is vertigo due to a disease originating from the central nervous system (CNS). In clinical practice, it often includes lesions of cranial nerve VIII as well. Individuals with vertigo experience hallucinations of motion of their surroundings. Central vertigo may be caused by hemorrhagic or ischemic insults to the cerebellum, the vestibular nuclei, and their connections within the brain stem. Other causes include CNS tumors, infection, trauma, and multiple sclerosis. Vertigo due to acoustic neuroma is also included in the broader category of central
12
vertigo. An acoustic neuroma develops within the eighth cranial nerve, usually within the course of the internal auditory canal, yet it often expands into the posterior fossa with secondary effects on other cranial nerves and the brain stem.
Pathophysiology
The brainstem, cerebellum, and peripheral labyrinths are all supplied by the vertebrobasilar arterial system. Thus, the central and peripheral ischemic vertigo syndromes overlap.
Vertebrobasilar arterial system
The basilar artery is formed from the 2 vertebral arteries within the cranium at the level of the medulla. The artery has 3 branches on each side that supply the cerebellum. The posterior inferior cerebellar artery branches from the vertebral artery, while the anterior inferior cerebellar artery and the superior cerebellar artery branch from the basilar artery. All 3 of the cerebellar arteries may have branches that supply brainstem tissue. A labyrinthine artery on each side branches from the basilar artery and supplies the labyrinth and associated structures via the internal auditory canal. In approximately two thirds of people, the basilar artery ends by bifurcating into the posterior cerebral arteries, with small posterior communicating arteries connecting to the internal carotid system in the circle of Willis.
Arterial occlusion and ischemic infarction
Arterial occlusion and ischemic infarction can result from cardioembolism, embolism of plaque from a vertebral artery, or local arterial thrombosis. One or both vertebral arteries, the basilar artery, or any of the smaller branches may be occluded. Even complete occlusion of a large artery may not result in death because of anastomotic retrograde flow via the circle of Willis and posterior communicating arteries. Temporary vertebrobasilar ischemia may present as migraine syndrome or transient ischemic attacks (TIAs). While less common than cerebellar infarction, spontaneous cerebellar hemorrhage is an important life-threatening cause of vertigo associated with hypertensive vascular disease and anticoagulation (St. Louis et al., 1998)
Laboratory Studies
Laboratory studies may be useful for patients who do not complain strictly of vertigo. Rule out anemia, pregnancy, and derangement of serum glucose, if relevant, in patients
who complain of lightheadedness or disequilibrium.
Imaging Studies
Imaging of the posterior fossa is necessary if the clinician suspects a central lesion. o Magnetic resonance imaging (MRI) is the preferred modality to detect infarction
(Simmons et al., 1986) , hemorrhage, tumor, and the white matter lesions of multiple sclerosis.
13

o If MRI is unavailable, computed tomography (CT) scan with fine cuts through the posterior fossa may be used. Unfortunately, CT scan is limited by poorer resolution than MRI and bony artifact.
o Intra-arterial angiography is used traditionally to diagnose occlusions in the vertebrobasilar system. CT angiography (CTA), noninvasive magnetic resonance angiography (MRA), and Doppler ultrasonography are steadily supplanting it. This may be particularly important as early thrombolysis becomes more established as a therapy.
Other Tests
Electrocardiography (ECG) is necessary to assess for atrial fibrillation, other dysrhythmias, or evidence of acute myocardial infarction (AMI).
AMI, particularly involving the anterior wall of the left ventricle, can lead to a stiffened ventricle with poor wall movement and secondary stasis. This may serve as a cardioembolic source for cerebral thromboembolism.
The consulting neurologist may perform caloric testing and electronystagmography (ENG) to help localize the lesion in the vestibular apparatus or vestibular nerve nuclei; audiometry and brainstem auditory evoked potentials (BAER) also may be performed.
FINAL DIAGNOSIS Clinical diagnosis : Acute rotational sensation, nausea, parese of left 3rd Cranial NerveTopical diagnosis : Organon vestibular central (pons and cerebellum) and perifer (cochlea)Etiological diagnosis : Central: Vascular (Brainstem and Cerebellum infarction)Other diagnosis : HT stage II, diabetic
ManagementEmergency Department CareFirst, distinguish true vertigo from disequilibrium and other forms of dizziness. Ascertaining this history from patients sometimes requires patience and persistence. Once the presence of vertigo or disequilibrium has been confirmed, consider a central cause. Evaluate on the basis of a careful history and physical examination and liberal use of imaging studies of the posterior fossa.
Therapy usually targets the etiology of the symptoms. However, a variety of medications may be used to reduce symptoms of central vertigo, including antihistamines and benzodiazepines.
Regardless of the vertigo's etiology, attempt to alleviate the patient's suffering. o Place intravenous lines to rehydrate patients.o Allow patients to lie still in bed as desired.o Administer parenteral medicines for symptomatic relief.
If clinical and radiologic evaluation suggest an acute ischemic stroke, consider thrombolytic therapy after thorough evaluation and consultation.
14

o Thrombolytic therapy is administered with an intra-arterial catheter close to the clot , or intravenously, if within 3 hours of the onset of symptoms and no other contraindications exist (The National Institute of Neurological Disorders, 1995).
o Prior to using thrombolytic therapy, consider several issues, especially the risk of intracerebral bleeding. Emergency physicians should be familiar with contraindications such as major surgery within the previous 10 days, severe hypertension, evidence of acute bleed or edema on CT scan, and rapidly improving symptoms.
o The decision to administer thrombolytic therapy preferably is made with direct neurologic consultation and only after the patient has received a thorough explanation of the procedure and given informed consent. This therapy is discussed further in other articles (see Stroke, Ischemic and Thrombolytic Therapy).
Lethargic patients or those with altered level of consciousness require vigilance and close supervision, including direct visual, ECG, and pulse oximetry monitoring.
Do not administer anticoagulant medicine, including aspirin, until intracranial hemorrhage has been ruled out by imaging.
Imaging studies should be performed expeditiously, and the patient never should be left unattended by clinical personnel in the imaging suite.
Patients with altered consciousness and a deteriorating course in the ED may require emergent interventions to minimize edema and brainstem compression.
o As the posterior fossa is a relatively small and nonexpandable space, hemorrhage or edema can lead to rapid compression and compromise of vital medullary functions, obstructive hydrocephalus, or herniation of the medullary tonsils.
o Invasive actions may include endotracheal intubation to protect the airway, control breathing, and allow therapeutic hyperventilation.
o Consider elevating the head of the bed, performing diuresis with mannitol or furosemide, and administering dexamethasone.
Preliminary evidence suggests that recombinant activated factor VII may be useful for acute hemorrhagic stroke when administered within 4 hours of symptom onset (Mayer et al., 2005). The data supporting the use of this therapy for hemorrhagic cerebellar stroke is too limited thus far to make a therapeutic recommendation, but further results are expected to clarify its utility and adverse effect profile.
Medical Treatment Overview
Acute dizziness and vertigo is usually managed with vestibular suppressants, antiviral medication, and antiemetic medications. Steroids are useful in selected patients. Vestibular suppressants should be used for a few days at most because they delay the brain's natural compensatory mechanism for peripheral vertigo. Vestibular rehabilitation is very useful in boosting central vestibular compensation.
Central Dizziness
Migraine
15
Migraine is a common disorder, affecting 10% of men and 30% of women. About 25% of migraineurs have motion intolerance/sickness as opposed to true vertigo. The pathophysiology of migraine-associated vestibulopathy is not completely understood.[4] Vestibular symptoms usually are dissociated from headaches but sometimes can occur as an aura or as part of a headache.
Treatment of migraine-associated vestibulopathy is the same as the treatment of migraine. Trigger factors should be eliminated and patients are encouraged to follow common sense diet and lifestyle.[4] Prophylactic and abortive medications commonly used in treating migraine should be tailored to patients with vestibular migraine.[3] In the authors’ experience, topiramate (Topamax) and rizatriptan benzoate (Maxalt) are associated with excellent control of vestibular migraine.
Transient ischemic attacks (TIAs)
TIAs are episodes of focal neurological symptoms of isolated or combined brainstem symptoms such as dizziness, diplopia, or weakness. These attacks are of sudden onset and resolve within 24 hours without residual subjective symptoms or objective signs (on examination). TIAs are usually due to either reduced blood flow (hemodynamic theory; eg, cardiac dysrhythmia) or blood flow obstruction (embolic theory; eg, plaques from the heart).
TIAs are commonly (75% of cases) due to posterior circulation (vertebrobasilar territory). The differential diagnosis of TIAs includes migraine, partial seizures, hypoglycemia, syncope, and hyperventilation.
Cerebrovascular disease
Stroke is the third most common cause of death or disability in adults. The vertebrobasilar circulation supplies the brainstem, cerebellum, and the inner-ear auditory and vestibular structures. Infarction of the cerebellar midline can cause acute vertigo without auditory or other neurologic features (eg, isolated vertigo). This potentially life-threatening occurrence must be differentiated from vestibular neuronitis. A key difference between these 2 entities is the inability to ambulate without support during the acute vertigo phase with cerebellar strokes. About one half of patients have other features of bulbar or long tract involvement, which make the diagnosis of stroke clear.
Evaluation of the patient with stroke is directed at identifying correctable vascular risk factors (hypertension, diabetes, hyperlipidemia, and smoking) and at determining the mechanism of stroke (small vessel, large vessel, cardioembolic, dissection, hypercoagulability, vacuities). Secondary prophylactic therapy and rehabilitation are individualized. Both hearing loss and vertigo can occur in the setting of stroke due to either central and/or peripheral injury.
The patient had given therapies:Non pharmacologic :
- Head up 30 degree- Education
16

- Diet of diabetic - Rehabilitation
Pharmacologic : - O2 3 lpm- IVFD NaCl 0,9% 16 dpm- Inj. Citicholin 500 mg/12 h- Clopidogrel 1 x 75 mg- Flunarizin 2 x 5 mg- Betahistine 6mg/ 8hour- Amlodipin 10mg/ 24h- Valsartan 80 mg/ 24h- Novorapid injection s.c. 8-8-8 after meal
Planning : - TCD- DSA
Prognosis
Prognosis for patients with central vertigo depends on the underlying disease and is highly variable.
Neurosurgical advancements have improved the prognosis for many serious conditions. This magnifies the importance of identifying these patients in the emergency setting.
The prognosis of infarction of the basilar or vertebral arteries is poor. In one series, 45% of patients presented in coma. Importantly, half of the patients in this series had prodromal symptoms, including vertigo, which cleared completely in the 6 months prior to the stroke (Ferbert et al., 1990)
The prognosis for this patient are: Death : dubia ad malamDisease : dubia ad malamDiscomfort : dubia ad malamDisability : dubia ad malamDissatisfaction : dubia ad malamDestitution : dubia ad malam
REFERENCES
17

Ferbert A, Bruckmann H, Drummen R. Clinical features of proven basilar artery occlusion. Stroke. Aug 1990;21(8):1135-42.
Kerber KA, Meurer WJ, West BT, Fendrick AM. Dizziness presentations in U.S. emergency departments, 1995-2004. Acad Emerg Med. Aug 2008;15(8):744-50.
Katsarkas A. Dizziness in aging: the clinical experience. Geriatrics. Nov 2008;63(11):18-20.
Mayer SA, Brun NC, Begtrup K, Broderick J, Davis S, Diringer MN, et al. Recombinant activated factor VII for acute intracerebral hemorrhage. N Engl J Med. Feb 2005;352:777-85.
Pokdi Vertigo, 2014. Pedoman Tata Laksana Vertigo. PERDOSSI
Simmons Z, Biller J, Adams HP Jr, Dunn V, Jacoby CG. Cerebellar infarction: comparison of computed tomography and magnetic resonance imaging. Ann Neurol. Mar 1986;19(3):291-3
St. Louis EK, Wijdicks EF, Li H. Predicting neurologic deterioration in patients with cerebellar hematomas. Neurology. Nov 1998;51(5):1364-9.
The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study. Tissue plasminogen activator for acute ischemic stroke. N Engl J Med. Dec 14 1995;333(24):1581-7
Walker MF. Treatment of vestibular neuritis. Curr Treat Options Neurol. Jan 2009;11(1):41-5.
18