Year 1 Mh linical Skills Session ardiovascular examination...Prior to any clinical examination a...
14
Year 1 MBChB Clinical Skills Session Cardiovascular examination Authors The Clinical Skills Lecturer Team Reviewed & rafied by: Dr David Roberts - Cardiovascular System Lead (Consultant Cardiologist) August 2020
Transcript of Year 1 Mh linical Skills Session ardiovascular examination...Prior to any clinical examination a...

Year 1 MBChB
Clinical Skills Session
Cardiovascular examination
Authors
The Clinical Skills Lecturer Team
Reviewed & ratified by:
Dr David Roberts - Cardiovascular System Lead (Consultant Cardiologist)
August 2020

2
Cardiovascular Examination
OBJECTIVES
To underpin anatomy and physiology of heart & sites of peripheral pulses.
To link anatomy and physiology to practical skill.
To be able to measure lower limb pulses, locate apex beat & listen to heart sounds.
The Cardio-Vascular System
The cardio-vascular system (CVS) is comprised of the heart and the blood vessels (arteries, arterioles, capillaries, venules and veins).
The Heart
The heart is a 4 chamber pump with the right atrium and right ventricle being on the venous side of the circulation and the left atrium and left ventricle being on the arterial side.
The right atrium receives deoxygenated blood from the Superior Vena Cava, in turn the right atrium pumps the blood into the right ventricle which pumps it through the pulmonary circulation (through the lungs) where it becomes oxygenated.
Pulmonary Circulation
By OpenStax College - Anatomy & Physiology, Connexions Web site. http://cnx.org/content/col11496/1.6/, Jun 19, 2013., CC BY 3.0, https://commons.wikimedia.org/w/index.php?curid=30148269

3
The left atrium receives the oxygenated blood from the pulmonary circulation in turn the left atrium pumps the blood into the left ventricle which pumps it through the systemic circulation (around the body).
The atria are separated from the ventricles by the Tricuspid valve on the right and the Mitral valve on the left. The right ventricle is separated from the pulmonary circulation by the Pulmonary valve and the left ventricle from the systemic circulation by the Aortic valve.

4
By ZooFari - Own workSupporting references↑ [1] (cache)↑ [2] (cache), CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=9841860
Heart valves open to allow the blood to flow around the heart, pulmonary circulation and the systemic circulation. When the valves shut to prevent retrograde (backwards) flow they produce sounds known as the heart sounds. When we will listen to these sounds the first sound (S1) is produced by closure of the Tricuspid and Mitral valves. The second sound (S2) is produced by the Pulmonary and Aortic valves. If you palpate the pulse whilst listening to the heart sounds you will note that S1 occurs just as the pulse is felt and S2 is heard immediately after the pulse.
The Function of the Cardio-Vascular system
The Cardio-Vascular system’s function is to circulate blood around the body carrying oxygen and nutrients to the cells and to carry carbon dioxide and the waste products away.
For this to be effective the heart needs to be able to pump in a coordinated manner with complete valve closure occurring at the correct time. The blood vessels need to be patent and offer an appropriate amount of resistance to flow (to maintain blood pressure) and there needs to be an adequate volume of blood to fill the system.

5
Why perform the cardiovascular examination
There are many indications for performing the cardiovascular examination. The decision as to which
examinations will be performed is made based upon the patient’s history.
• Acute chest pain
• Acute breathlessness
• Exacerbation of chronic cardiovascular conditions
• Poor peripheral perfusion
• Trauma
• Collapse? cause (syncope)
Equipment required to perform the examination
Hand wash
Stethoscope
Alcohol swabs to clean stethoscope
Starting the examination
Prior to any clinical examination a detailed history should be taken from the patient, this will enable you to tailor
the examination to the patients presenting complaint and additional symptoms the patient may elude to when
you elicit a full history. For guidance on history taking please click MBCHB students – Year 1 – History taking.

6
General Inspection
Look at the patient and their environment at the beginning of the examination.
In the environment there may be many indicators of possible cardiovascular conditions including:
• Medications related to CVS system including angina spray (GTN)
• Cigarette paraphernalia (smoking is associated with cardiovascular and respiratory disease)
• Oxygen therapy (can be required by patients with cardiovascular or respiratory disease)
• Electrocardiogram monitor (ECG monitor)
• Inotropic infusions (to keep blood pressure up)
The patient may show some signs of possible cardiovascular disease such as:
• Expression of pain in clutching facial grimace or clutching chest
• Central or peripheral cyanosis (blue colour of skin due to poor perfusion (due to hypoxia))
• Pallor (pale appearance)
• Sweating without exertion can be a sign of cardiovascular disease
• Breathlessness
• Trauma and blood loss (affecting volume of blood)
• Collapse (possible unresponsive patient – assess for cardiorespiratory arrest)
Palpation – upper limb pulses
The radial pulse The radial pulse is located on the lateral aspect of the lower forearm just proximal (towards the centre of the body) to the wrist joint. It is only possible to assess the rhythm (how regular the pulse is) and rate (how fast) of the pulse at the radial artery. Place your fingertips onto the anterior surface of the wrist in the midline just above the wrist joint. Move your fingers laterally (towards the outside) and the tips of your fingers will drop into a groove. Apply light pressure and slowly increase the amount of pressure until you feel the pulse. The pulses can be felt (palpable) when the artery is lightly compressed against the underlying radius (bone). See images below.

7
The brachial pulse The brachial pulse is located on the anterior surface of the arm at the level of the elbow joint. The artery is larger than the radial artery and in addition to the rhythm and rate you will be able to determine volume (how much blood passes through the artery each time the heart contracts), the character (how the pulse feels as it rises and falls) and begin to start to appreciate the health of the vessel wall (is it soft and pliant (healthy) or is it hardened (possibly due to arteriosclerosis)). Place your fingertips onto the anterior surface of the elbow in the midline at the level of the joint. Have the patient slightly bend their elbow and move your fingers medially (towards the inside) and the tips of your fingers will feel a large tendon. Move your fingers to the medial aspect of this tendon and ask the patient to straighten their arm. Apply light pressure and slowly increase the amount of pressure until you feel the pulse. The pulse can be felt (palpable) when the artery is lightly compressed against the underlying humerus and soft tissues. The brachial artery is deeper than the radial artery and requires a little more pressure to compress it. See images below.
Blood pressure measurement
• Blood pressure measurement is routinely done as part of a cardiovascular examination.
• A blood pressure should always be taken on both arms when first meeting a patient. The reasoning behind
this practice is that there are sometimes important differences between the two readings, and that the
lower blood pressure in one arm should be investigated as it may be a sign of an abnormality (coarctation,
stenosis, dissection). A difference of equal to or less than 10mmHg is acceptable and needs no further
investigation.
• Lying and standing BP’s should be taken on first meeting the patient, if symptoms indicate postural
hypotension (low blood pressure) or history of collapse (syncope)
• Blood pressure measurement was covered in a previous session.
Carotid Pulse
The carotid pulse is located on the anterior aspect of the neck just lateral (towards the outside of the body) to the larynx (voice box). Position yourself slightly to the side of the patient. Place your fingertips (some practitioners may use their thumb) onto the anterior surface of the neck in the midline with your index finger at the level of the Thyroid Cartilage (Adam’s apple). Move your fingers laterally (towards the outside) approximately 2.5 – 4 cm and the tips of your fingers will drop into a groove. Apply light pressure and slowly increase the amount of pressure until

8
you feel the pulse. The pulse can be felt (palpable) when the artery is lightly compressed against the underlying tissues. See picture below. The Carotid Arteries contain pressure receptors and you should take care not to press too hard. You MUST NOT palpate both arteries at the same time and you MUST NOT rub the Carotid Artery.
Inspection of chest wall Inspect the chest wall for the following
• Scars may indicate previous surgery or trauma (large midline incisions may be an indication of previous
sternotomy)
• Rashes may be painful (shingles) and be the cause of a patient’s “chest pain”
• Lesions or bruising may indicate underlying conditions or trauma
• Pulsation of chest wall (cardiac impulse) due to enlarged heart or pulsation of a swelling.
• Respiratory rate, depth and pattern may indicate problems with circulation or respiration.
• Distended veins may indicate a back pressure building within the venous system.
Palpation of the apex beat
The Apex beat is the point most laterally and inferiorly at which the heart beat can be felt.
The Patient should be at 45o (laying on back) or they may be asked to sit forward or to roll to the left slightly
Place the fingertips of the index, middle and ring fingers into the mid axillary line on the left lateral chest wall.
Place the fingers into intercostal spaces (dips between the ribs which should approximate to the 4th, 5th and 6th
intercostal spaces laterally)

9
Gradually bring tips of fingers medially until a beat is felt (may only be a faint tapping)
Describe position in relation to intercostal spaces and vertical landmarks of the chest (e.g. mid-clavicular line,
anterior axillary line, mid-axillary line)
Location of the apex beat
Apex beat is normally palpated within the 5th intercostal space at the mid-clavicular line.
A shift away from this position may indicate that the heart is larger than normal or being displaced by another
structure.
Once the apex beat has been located you should note its position or leave a finger in place and then;
Palpate down from the sternal notch to the raised sterno-manubrial joint (angle of Louis) situated
approximately 5cms below sternal notch
Move the finger from the sterno-manubrial joint to the left until your finger is either on a rib (2nd rib) or in a dip
(2nd intercostal space).
Carefully count down the ribs and intercostal spaces until in the 5th intercostal space.
Move your finger laterally towards the point where you felt the apex beat (or where your other finger is)

10
Is the point where you found the apex beat in the 5th intercostal space mid clavicular line or is it a rib space
above (4th) or below (6th) or is it medial (towards the midline) or lateral (towards the outside)?
Auscultation of the heart sounds
Auscultation is the listening (with a stethoscope) to the sounds of the heart, the sound of abnormal blood flow
in the blood vessels (bruits) (normal blood flow is silent), the movement of air during respiration or the gurgles
or rumblings of gas and fluid in the bowel.
Stethoscope
A stethoscope is a device which allows you to hear these sounds. You will have been introduced to the
stethoscope in previous sessions and will remember that the diaphragm is used to listen for higher pitched
sounds and the bell for lower.
When you offer the ear pieces up to your ears they should point slightly forward as this is the direction of the
ear canal.
Ensure the stethoscope is set to the side you wish to listen to.
The bell is used to listen to low pitched sounds.
The diaphragm is used to listen to higher pitched sounds.
The ear pieces should be angled forward as they are inserted into the ears.
The spring should hold the earpieces comfortably in the ears.
11
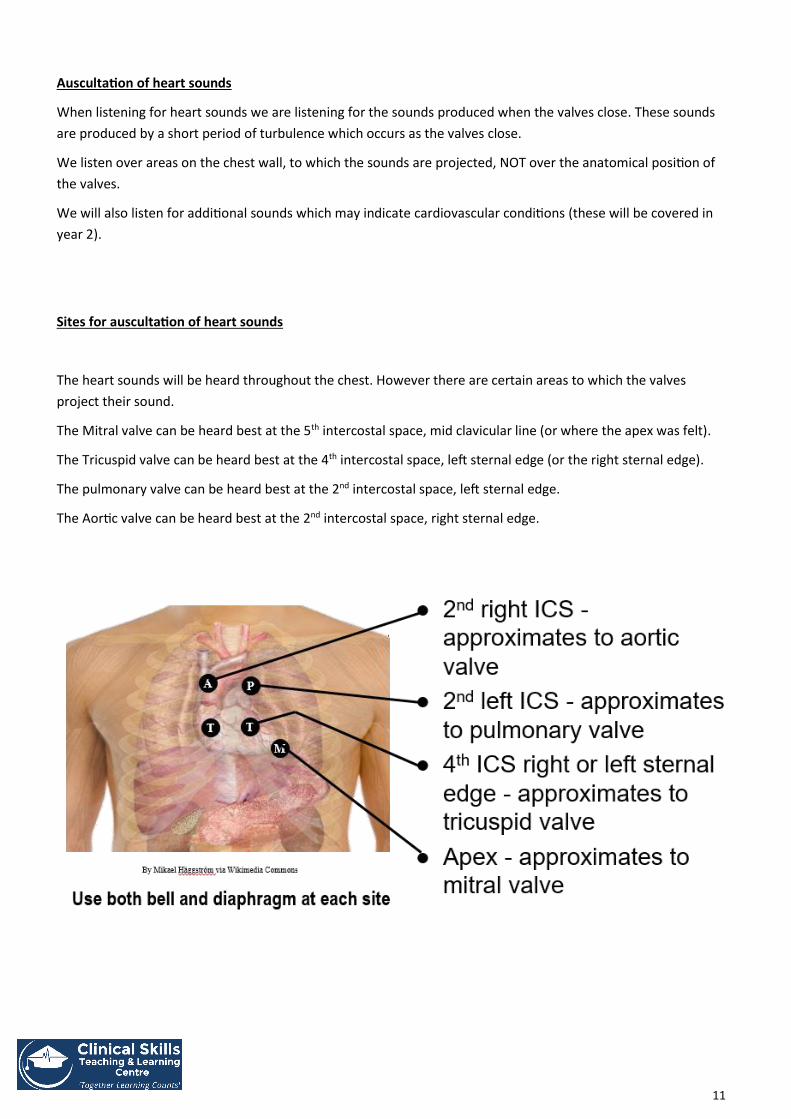
Auscultation of heart sounds
When listening for heart sounds we are listening for the sounds produced when the valves close. These sounds
are produced by a short period of turbulence which occurs as the valves close.
We listen over areas on the chest wall, to which the sounds are projected, NOT over the anatomical position of
the valves.
We will also listen for additional sounds which may indicate cardiovascular conditions (these will be covered in
year 2).
Sites for auscultation of heart sounds
The heart sounds will be heard throughout the chest. However there are certain areas to which the valves
project their sound.
The Mitral valve can be heard best at the 5th intercostal space, mid clavicular line (or where the apex was felt).
The Tricuspid valve can be heard best at the 4th intercostal space, left sternal edge (or the right sternal edge).
The pulmonary valve can be heard best at the 2nd intercostal space, left sternal edge.
The Aortic valve can be heard best at the 2nd intercostal space, right sternal edge.

12
S1 – 1st heart sounds (LUB) Heard loudest over the mitral area, the sound immediately precedes (comes before) systole (when the pulse
occurs) and generates the sound “LUB” (low pitched, longer in duration than S2). Therefore you can tell which
sound is which by taking the pulse whilst you listen. The 1st heart sound is produced by closure of the Mitral and
Tricuspid valves.
S2 – 2nd heart sounds (DUP)
Heard loudest over the pulmonary area, the sound immediately succeeds (comes after) systole (after the pulse
occurs) and generates the sound “DUP” (High pitched, shorter in duration than S1). Therefore you can tell which
sound is which by taking the pulse whilst you listen. The 2nd heart sound is produced by closure of the
Pulmonary and Aortic valves
During inspiration, delayed pulmonary valve closure may cause 2nd heart sound to split “dup-p”

13
Palpation – Lower limb pulses
Femoral artery
The femoral artery enters the upper leg by passing under the inguinal ligament. It enters the leg at the mid-inguinal point. The femoral artery is usually easily palpated and is an important point of access to the arterial system. The artery lies in-between the femoral nerve and femoral vein as it enters the leg. The term NAVY (From the outside (Nerve, Artery, Vein, Y fronts (genitals)) will remind you. Femoral Nerve Femoral Artery Femoral Vein
Genitalia
Popliteal artery The popliteal artery is palpable in the popliteal fossa which is at the back of the knee joint. The artery enters in the midline as it passes through the fossa the popliteal artery can be palpated in the midline of the fossa at the level of the femoral condyles.
With knee in slight flexion. Place the fingertips of both hands into the centre of the popliteal fossa and pull them
into the back of the knee. The artery is deep so start by applying light pressure and slowly increase the pressure
until the pulse is felt. If you cannot find the pulse relax your hands and move the fingertips apart slightly and try
again. This is a deep pulse and you may need to apply more pressure than you would expect (without causing
pain).

14
Tibialis posterior artery
The tibialis posterior artery is found on the medial aspect of the ankle.
It is palpable at a position midway between the prominence of the medial malleolus (ankle bone) and the
prominence of the calcaneus (heel bone). Again you should place your fingers over the area and apply light
pressure, increase the pressure until the artery and pulse are palpated.
Dorsalis pedis
Dorsalis pedis is a continuation of the tibialis anterior
Tibialis anterior is often palpable medial to the extensor hallucis longus tendon, you can ask your patient to lift
their big toe and the tendon will stand proud. The tendon crosses the artery laterally to medially. The dorsalis
pedis artery can be palpated, with clean hands, on the dorsum of the foot, lateral to the extensor hallucis longus
tendon.
This concludes the 1st year teaching of Cardiovascular Examination. Further components of the examination will be taught
in 2nd year.