
Xchanging Forum Health Benefits Of Work (HBOW) · Xchanging Forum . Health Benefits Of Work (HBOW)...
78
Xchanging Forum Health Benefits Of Work (HBOW) Sydney, 7 May 2014 Dame Carol Black Expert Adviser on Health and Work Department of Health, England Principal, Newnham College Cambridge Making it Happen : International Reflections
Transcript of Xchanging Forum Health Benefits Of Work (HBOW) · Xchanging Forum . Health Benefits Of Work (HBOW)...

Xchanging Forum Health Benefits Of Work (HBOW) Sydney, 7 May 2014
Dame Carol Black
Expert Adviser on Health and Work Department of Health, England
Principal, Newnham College Cambridge
Making it Happen : International Reflections

Consensus Statements on Health Benefits of Work
Australasia 30 March 2011 (abbreviated) “ We acknowledge the following fundamental principles… of the relation of health and work : • Work is generally good for health …. • Long term absence… have negative impact • Work must be safe so far as ..practicable • Work is effective in reducing poverty including that of indigenous populations • With appropriate support, many … who are
disadvantaged can access benefits of work. • Work practices, culture, etc … are key determinates of individual health, wellbeing and productivity. • Good outcomes are more likely when people understand HBOW, and take responsibility for their own situation. • Health professionals exert significant influence on work absence and work disability ….
UK 5 March 2008: launched RCGP “ We will work with government, other healthcare workers, the voluntary sector, employers and trades unions, to promote and develop ways of supporting individuals to achieve the socio-economic and health benefits of work. This pledge includes a commitment to continue to educate the healthcare community, employers and people of working age about the benefits that work can provide; and, as appropriate, to do all we can to help people enter, stay in or return to work. ”

Source: OECD (2014), Mental Health and Work: United Kingdom, Paris: OECD Publishing. Courtesy Shruti Singh
New UK disability claims are among the highest in the OECD New claims per 1,000 of the working-age population (inflow rates), latest year available
0
2
4
6
8
10
12
OECD
average
Lack of early intervention ? – on journey to benefit claim
Earlier intervention could improve this

Work Sickness absence
Claim to Employment
Support Allowance
(ESA)
Work Capability
Assessment
ESA benefit and support
JSA
benefit and support
Work
Inactivity
28 weeks 39 weeks
The journey from work and wellbeing in the UK
Claim to Employment
Support Allowance
(ESA)
Work Capability
Assessment (WCA)
LEAVE WORK Wait for WCA completion can be nine months – many appeal decision
Too few drivers in the journey keeping people in work.
Too little help here to maintain people in work. Poor and ineffective early intervention or prevention. SSP = Statutory Sick Pay OSP = Occupational Sick Pay
SSP/OSP
Active support here BUT too late
Family doctors the gateway to benefits
WCA = Work Capability Assessment

The UK journey started in 2005 ..
The position : • sickness absence a persistent problem • too many people leaving the labour market permanently with a health condition, with mental ill-health a major problem • substantial ‘presenteeism’ . Resulting in: • rising bill for welfare benefits, increasing healthcare costs • reduced productivity and competitiveness for UK plc
Also : - an ageing population - an epidemic of obesity - increase in chronic diseases (often with mental co-morbidity) Action : cross-government (DH, DWP, HSE, Wales Scotland) Health, Wellbeing and Work strategy, and appointment of National Director for Health and Work.

Reviews 2006 – 2014 in the UK on Health, Work, Safety, Well-being, Engagement
Reclaiming Health and Safety for All”: an independent review of Health and Safety Legislation - Lofstedt
Also, political think tanks produced documents
Rich evidence in this area – but delivery and evaluation remain the challenges

Effect Internationally
The two reports, Black 2008 and Black and Frost 2011, have affected thinking, policy and practice. Their ideas have been adapted and used in :
• Singapore • Hong Kong • South Korea • Australia • New Zealand • USA • Countries in the European Union • Russia (early signs)

UK Progress to date : Government
• Fit Note, new 2010, paper .... a well-designed instrument
• Electronic Fit Note formulation – gradually covering the country
• Fit for Work pilots – to show value of early VR and case management
• SEQOHS - raising standards in Occupational Medicine
• Health for Work Adviceline ….. 3 channels, useful to SMEs
• Council for Health and Work …. collaborative, making a difference
• Regional Co-ordinators …. showed the value of local action.
• Public Health Responsibility Deal ..Health at Work Network, 10 pledges
• Public Health England ….. committed, with work in progress.

Caveat re government
• The UK Government may be good at thinking and policy …
• ..... but does it deliver and implement as intended ?
• Note: OECD Report on UK Mental Health and Work 2013 “ Policy – rhetoric, thinking and documents – are more advanced than is actual practice. There are still a number of problems that the UK will have to address … to ensure that ongoing structural reforms are successful. ”
UK Progress to date : Other bodies
• Employers, large medium and small, making changes, writing business cases, improving engagement and productivity.
• Local Actions …. many, e.g. Liverpool’s Workplace Wellbeing Charter • Progress in Occupational Health community …. co-ordination,
training, relevance to Government, standard-setting
• RCP/FOM Auditing .... of implementation by NHS Trusts of NICE Workplace Guidance, collaborations
• Trade Unions increasingly on board …. engaged and represented, NE a good example
• NGOs showing great interest and support … for example BHF, Diabetes UK, Macmillan Cancer, etc.

Ensuring better medical certification: the ‘Fit Note’ – a journey
Family doctors (GPs) are the gatekeepers. When the new Fit Note is used as intended, results are good, and employers satisfied. GP education/training material is of high quality, face-to-face and on-line Evaluation is ongoing : - 77% of GPs have felt obliged to give a Note for non-medical reasons - 38% said Fit Note had not changed their practice - only 23% had good knowledge of benefit system.
Brought in April 2010, by law
A further independent Sickness Absence Review was commissioned in 2011.

Fit for Purpose CBI and Pfizer 2013 Fit note scheme needs a tonic
• Launch of the fit note was welcomed by employers, who had high expectations of its impact as a guide for health interventions.
• Practical experience has not lived up to expectations. Only a fifth of employers report that the fit note has helped their rehabilitation policies or contains constructive advice.
• Only one employer in ten is confident that doctors are sufficiently trained to use the fit note properly. Only 5% are sure that doctors have sufficient workplace understanding.
• Only 17% believe the new fit note has changed culture around rehabilitation and return to work.
• The recently-relaunched guidance – plus the new electronic fit note – provide a clear opportunity to revamp the scheme.

Early intervention : pilots of ‘Fit for Work’ Service to support Fit Note
Musculo-skeletal 24% Mental Ill Health (moderate to severe)
8%
Mediation/Negotiation 18%
Personal Support 41%
Help with new employment
9%
i.e. 68% non-medical
Aim - To provide employees in early stages of sickness absence with case-managed multidisciplinary support to enable return to work How : • Service for people off work sick after 4 to 6 weeks (via GPs, voluntary). • Access to co-ordinated health treatment and employment support, including debt, housing, learning and skills, employer liaison, conciliation • Case-management a key component
In the first year 6,700 people sought help from FfWS across the nation. Need to develop a sustainable model.
Most Helpful Intervention: (Leicester FFWS pilot)
During the Leicester pilot, 94% of local GPs referred to the Service, which issued 2,580 Fit Notes, 47% saying fit for some work.

Determinants of Employment
• Employment is not determined solely by the measurable pathological effects of the disease, but also by the influence of the job and various psycho-social factors.
Examples : • Research by David Coggon suggests that much musculo-skeletal
disability attributed to occupational injury is the consequence, not of disease, but of a psychologically-mediated response to an external trigger, conditioned by individual characteristics and cultural values, beliefs and expectations.
• Christensen et al explored longitudinally a set of psychological/social and mechanical work factors as predictors of back pain severity (defined as the product of pain intensity and duration)….
…. and found that leadership factors best predicted back pain severity.

Predictors of back pain are not always ‘medical’
After adjustment for age, sex, skill level, back pain severity and other potential confounders, the most consistent predictors of back pain were:
• decision control at work
(lowest OR 0.68; 99% confidence interval (CI): 0.49 -0.95),
• empowering leadership at work
(lowest OR 0.59; 99% CI: 0.38-0.91) • fair leadership at work (lowest OR 0.54; 99% CI: 0.34-0.87) Christensen JO, Knardahl S. 2012 Do not forget leadership and other psycho-social factors

The pace of change was not enough... ... hence an Independent Review of
Sickness Absence was announced by the Prime Minister on 17 Feb 2011
Co-chairs: Carol Black, then National Director for Health and Work David Frost, former Director-General British Chambers of Commerce.
“ We simply have to get to grips with the sick-note culture that means a short spell of sickness absence can far too easily become a gradual slide to a life of long-term benefit dependency.”

SA Review: Conclusions of research and evidence-gathering
• Current system lacks coherence, wastes human/material resources
• Advocacy by GPs often inappropriate for employees’ long term health
• Lack of appropriate interventions at critical stage, at 4 to 6 weeks of absence. Lower skilled, lower paid employees particularly vulnerable.
• Some employers lack confidence in the medical certificate (‘fit note’) and
lack knowledge of legal rights and duties.
• Some people need to change employment to return to work. Late recognition of the ‘never going back’ syndrome
• State too slow to get the right support to individuals at the right time. • Significant differences between public and private sectors. 2011

Recommendations
Sickness Absence reduction
Independent Assessment
Service
Tax relief on Vocational
Rehabilitation
Abolition of Payment
Threshold Scheme in
SSP
Public Sector – Review of
Sick Pay
Job Brokering
Service
Changes to Employment and Support Allowance
Six major ones …
… plus six of lesser importance.

Work related/ workplace adjustments
Assessment
Telephone/face-to-face assessment
Identification of issues and recommendations
Health-related Non-work/non-health related
Intervention
Case management
Improvement/ resolution
GP referral At 4 weeks
Health and Work Service
Return to Work
Employers to have option to refer
The Future ?
Black and Frost, authors of the 2011 Review of sickness absence, said:
• Essentially, the service must be early, and must solve the employee’s problems – medical, work- related and/or non-work-related. • It has to have obligation or mandation
• It must be supported by a fully-functioning electronic Fit Note.
Will the Government deliver and bring about the
necessary change?

Public sector : National Health Service
The NHS employs 1.6 m people and is made up of lots of workplaces. Their goal is patient care of high quality, with efficiency.
The Boorman Review 2009 : Current staff health and wellbeing: If absence reduced by a third:
10.3 million working days lost per year
Equivalent to 45,000 FTEs
Costing £1.7 billion per year.
3.4 million days gained
14,900 additional care FTEs
Annual savings of £555m

Public Sector : Health and Wellbeing Improvement Framework (DH for NHS)
With strong visible
leadership
Supported by improved
management capability
With all staff encouraged and enabled to take more
personal responsibility
Better, local high-quality accredited
Occupational Health services
Developing local
evidence- based
improvement plans
• The Department of Health published a Health and Well-being Improvement Framework which highlights the evidence and detail behind the 5 high impact change pathway: uptake is supported by NHS Employers. http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsP
olicyAndGuidance/DH_128691
…. sets out five high-impact changes that NHS organisations can follow to improve staff health and well being and reduce sickness absence:

HWIF 2 : Strong visible leadership
• Board level involvement will make the difference
• Where NHS Boards live the values they want to achieve, staff will take those values seriously.
• A named board member responsible for H&WB and reviewing progress every 6 months will drive this agenda forward.
Example: York Teaching Hospitals NHS FT • Used board engagement to drive progress across the Trust
• Board visibly involved in events to promote better health and well-
being, and communicated this to staff.
• Delivered sickness absence savings of £2.7m yearly, and 72% reduction in long-term absence.

Supported by Improved Management Capability
• The best providers enable
and support managers to follow good practice in building resilience, holding return-to-work interviews, recognising and supporting signs of stress, and addressing health in appraisals.
South West Yorkshire Hospitals • Showed that health and well-being of
staff is helped by better management
• Managers undertake a learning programme to help build their teams’ resilience and increase productivity.
• Achieved big reductions for all staff in : - working long hours, - harassment and bullying, - disengagement with increase in - engagement and - take-up of development opportunities.

Occupational Health : National Standards and Accreditation
1. Defining standards of practice to which services should aspire
2. Credit good work by OH services, with independent validation of satisfying standards
3. Raise standards where needed 4. Help purchasers differentiate OH services that
attain the desired standards from those that don’t. Standards published Jan 2010
www.seqohs.org
Produced by Faculty of Occupational Medicine
Accreditation scheme launched 2011 Overall 328 organisations registered (October 2013), 106 fully accredited. NHS in England has 150 in-house OH services: 132 are registered with SEQOHS, and 61 are fully accredited. NHS Occupational Health accounts for 40% of registrations, and 58% of fully accredited units.

Engaging the NHS
• Some hospitals have been slow to respond to letters, emails etc.
• However, visits to individual hospitals, plus follow-up letters, have been successful
• Participation by the hospital in the RCP/FOM NICE audit improved engagement, as did the need to comply with national OH standards.
• Hospitals tended to think this important but to say they had no time to make the business case – and where was the ‘road map’ ?
• The top NHS leadership must be engaged and supportive for this to work.
• NHS Employers have provided a road map.
NHS Staff Health and Wellbeing Engaging the leaders At the NHS Health and Wellbeing Summit in London on 23 April 2013 the five pledges that organisations committed themselves to were: • foster a culture that promotes better physical and mental health and wellbeing for staff in all workplaces used by the organisation
• work to strengthen staff engagement in and through these endeavours
• include measures of employee health and wellbeing within KPIs and other performance-monitoring systems
• sign up to the Public Health Responsibility Deal
• exploit relationships with other NHS organisations, and share expertise to safeguard and improve staff health and wellbeing.

Leadership Engagement : signing NHS staff health pledge
23 April 2013

NICE Guidance : Audit in NHS Collaboration RCP, NHS Employers and FOM
73% of NHS hospitals in England participated
Audit of implementation in hospitals of NICE Guidance on public health for the workplace
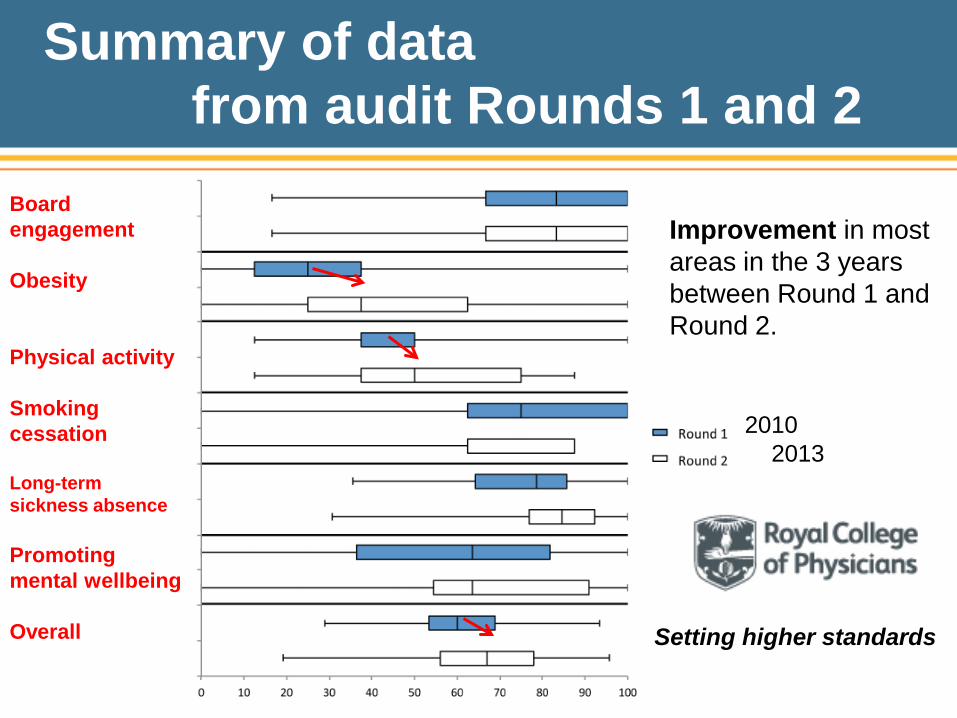
Summary of data from audit Rounds 1 and 2
Setting higher standards
Improvement in most areas in the 3 years between Round 1 and Round 2.
2010 2013
Board engagement Obesity Physical activity Smoking cessation Long-term sickness absence Promoting mental wellbeing Overall
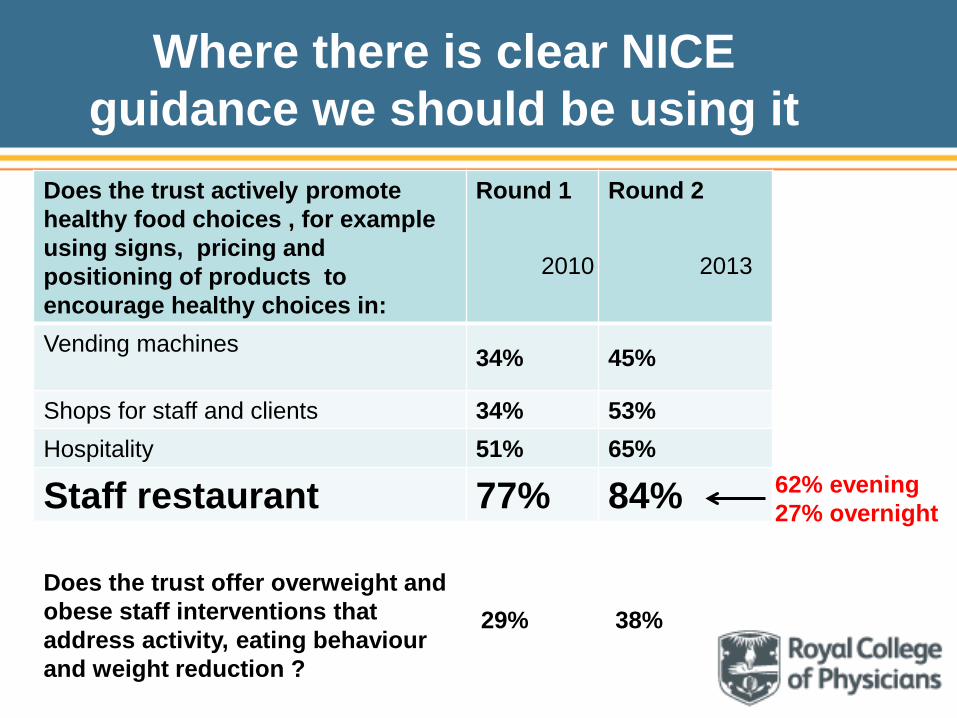
Where there is clear NICE guidance we should be using it
Does the trust actively promote healthy food choices , for example using signs, pricing and positioning of products to encourage healthy choices in:
Round 1 Round 2
Vending machines 34% 45%
Shops for staff and clients 34% 53% Hospitality 51% 65%
Staff restaurant 77% 84%
2010 2013
62% evening 27% overnight
Does the trust offer overweight and obese staff interventions that address activity, eating behaviour and weight reduction ?
29% 38%
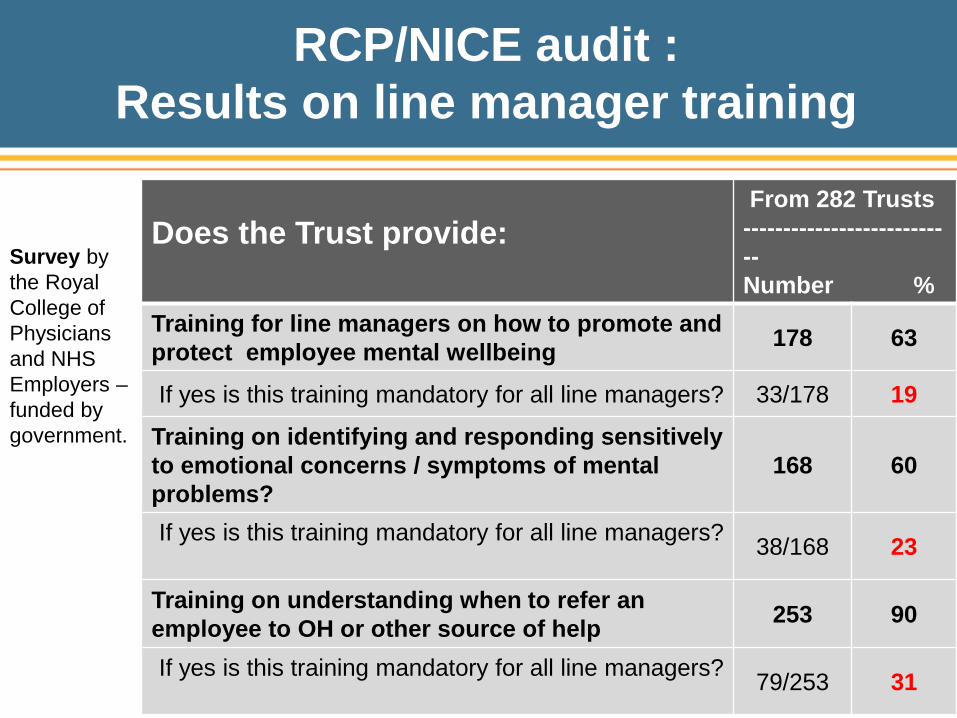
RCP/NICE audit : Results on line manager training
Does the Trust provide:
From 282 Trusts --------------------------- Number %
Training for line managers on how to promote and protect employee mental wellbeing 178 63
If yes is this training mandatory for all line managers? 33/178 19
Training on identifying and responding sensitively to emotional concerns / symptoms of mental problems?
168 60
If yes is this training mandatory for all line managers? 38/168 23
Training on understanding when to refer an employee to OH or other source of help 253 90
If yes is this training mandatory for all line managers? 79/253 31
Survey by the Royal College of Physicians and NHS Employers – funded by government.

Managers and Health and Wellbeing
• Good line management is key to good workplace mental health but managers do not need to be experts or counsellors.
• Managers should focus on: – effective communication with the
employee and other members of staff – awareness of the issues and the
ability to empathise – developing open culture with employees feeling
able to discuss their problems. • Learning about mental health enables managers to judge when
they need to refer employees to outside help. • There are many sources of advice and good training courses.

Results 2010: Actions in high-performing Trusts Actions that have been taken by organisations that are progressing well with the NICE guidance include: • assigning responsibility for staff H&WB to a committed and influential board lead who establishes a H&WB Group to interpret data, develop a strategy, and drive forward an action plan
• establishing and communicating the clear link between staff health (including respecting and engaging staff) and the quality of patient care delivered
• engaging staff and managers through frequent assessment of staff health and well-being needs, and including H&WB in staff recruitment, managers’ objectives, training, supervision guidance, and appraisals.
2013 Audit now in progress RCP Health and Work Development Unit

Healthy Engaged Workforces are Safer
• NHS hospitals with high staff engagement have standardised
patient mortality rates lower (by 5%) than hospitals with medium engagement.
• Organisations with engagement in the
bottom quartile average 62% more accidents than those in the top quartile.
• The Olympic construction had an Accident
Frequency Rate of 0.17 per 100,000 hours worked, less than half the average for the construction industry – this was attributed to strategies known to improve employee engagement.
• Engagement comes with Health and Wellbeing
90
92
94
96
98
100
102
104
Low Medium HighEngagement
Mortality mean 100

Costs of disengagement
Lack of motivation and sub-optimal health cause UK workers to work below peak productivity, holding back potential growth. Study of 5000 workers • About half of people do not go above and beyond at work because they
think it won’t be acknowledged or rewarded.
• One in four staff admit they don’t want to win new business, as it will only mean more work for them.
• Over a third of teams are experiencing extra stress and pressure due to staff ill-health and absences.
• Failure to unlock employees’ ‘discretionary effort’ costs businesses dearly, cutting a potential £6 billion – equivalent to 0.4% of GDP – from the UK economy in 2012.
BUPA/Centre for Economics and Business Research, December 2013

Source: OECD (2014), Mental Health and Work: United Kingdom,
Paris: OECD Publishing. Courtesy Shruti Singh
Mental ill-health costs the UK economy ₤ 70 billion every year - loss in employment & productivity: 53% - health care costs: 47% People with mental illness fare badly in the labour market - large employment gap - high unemployment rates Poverty risks are almost double the overall risk and the highest
in a comparison of ten OECD countries. Key factor for labour market exclusion - 40% of disability caseload has mental ill-health
Mental Ill-health and work in the UK

UK Government Activities supporting Mental Health (e.g. in the Workplace)
• Mandate, Government to NHS Commissioning Board, Nov 2012 to show progress in helping people with mental ill-health to remain in or return to work
• Health and Social Care Act 2012 section 1 Mental Health problems to have same attention as physical ones. • Government’s cross-dept Strategy “No health without mental health”
includes improving population mental health and reducing stigma, IAPT services. • Support for National Anti-Stigma Campaign “Time to change”
(£16 million over 4 years) partners: Mind, Comic Relief and Rethink Mental Health. Employers can pledge to support campaign.
• Public Health Responsibility Deal (Department of Health) Health at Work Network, Mental Health pledge • Engage for Success (Dept of Business Innovation and Skills) Engaged staff have greater well-being

Mental Health and Work in UK: OECD 2014 Recommendations
1. Acting Early when people still have a job • Rigorous implementation of the new H&W Service, with strengthened employer incentives • Make DWP’s Access to Work more available • Make better use of tools and guidelines • Make H&WS available to those struggling at work
2. Better and Tailored Employment Support • Strengthen early welfare intervention • Get incentives right e.g. for government programmes • Provide integrated MH and employment services.
3. Mental Health Risks in the Workplace • Improve access to therapies e.g. IAPT • Empower and educate GPs
Still a long way to go

Lessons learnt
• The importance of leadership
• Empowering well-trained managers is crucial
• Measurement and audit
• Standards plus incentives
• Staff engagement: Engage for Success
• Mental Health - still much to do

Private Sector : Health in Construction and Civil Engineering 1.2 million people work in Construction, 6% of the entire UK workforce. • High mortality rate, independent of social class.
• Itinerant, male-dominated, workers hard to reach.
• Employers can impact workers’ health and wellbeing,
in their own organisations and through supply chains.
• For employees, keeping well and in work protects against financial hardship, and promotes better quality of life.
• Employees are likely to take more responsibility for their own health and
wellbeing if there is leadership from the top. • Pro-active management of employees’ health brings important
business benefits

PHRD Pledge for Construction and Civil Engineering Industries
A special pledge for construction within the Public Health Responsibility Deal “As organisations working in the construction or civil engineering industries, we will take action to manage the causes of occupational disease and to improve the health and well-being of people working across offices and sites, large and small. We recognise that prevention and early intervention are the keys to success, and will take continuing action on the following: (1) Annual reporting of the health and well-being of employees (2) Provision of clinical Occupational Health Services (OHS) that work in accordance with the relevant standards e.g. SEQOHS (3) Arrangements to develop a programme to actively promote health and well-being and the effective management of health. We also pledge to encourage our subcontractors and our supply chains to endorse at least one of the actions above to implement good health and well-being activities.”

• Walk-in treatment service for minor injuries and illness • Physiotherapy • Health Surveillance • Emergency response
• Lifestyle medicals • Non Work Related • National campaigns • Linkage to other organisations
• Health Promotion - food, exercise - smoking, alcohol - sexual health
On –site Health, Safety and Well-being Services
Courtesy Dr Dyer, Park Health
All services provided close to the workers.
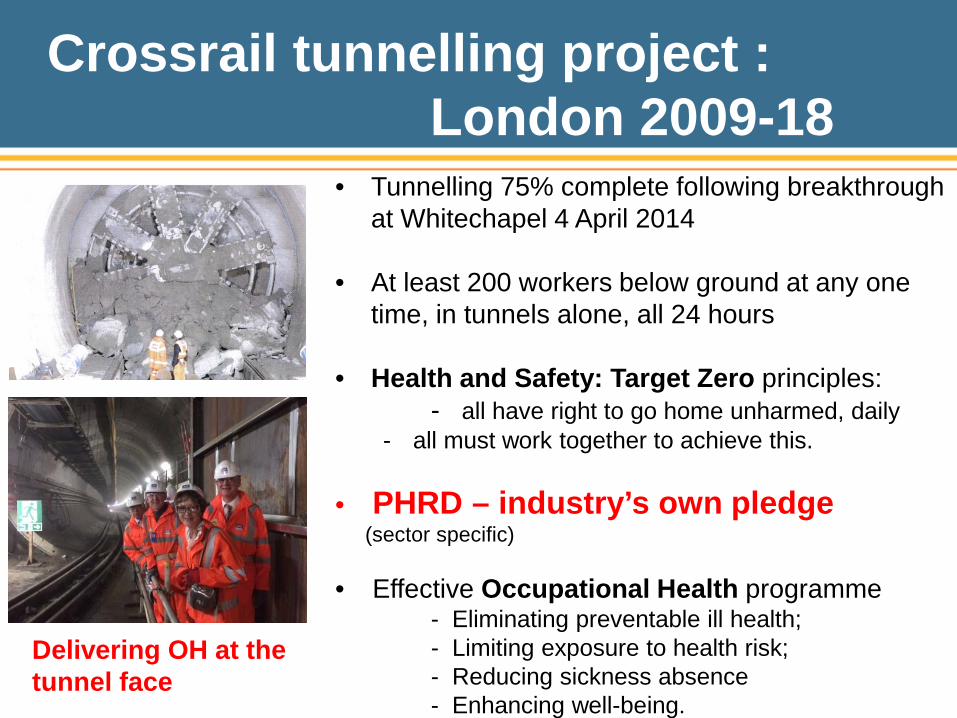
Crossrail tunnelling project : London 2009-18
• Tunnelling 75% complete following breakthrough at Whitechapel 4 April 2014
• At least 200 workers below ground at any one time, in tunnels alone, all 24 hours
• Health and Safety: Target Zero principles: - all have right to go home unharmed, daily
- all must work together to achieve this.
• PHRD – industry’s own pledge (sector specific)
• Effective Occupational Health programme - Eliminating preventable ill health; - Limiting exposure to health risk; - Reducing sickness absence - Enhancing well-being.
Delivering OH at the tunnel face
Coalition Government : Collaboration Public Health Responsibility Deal
“ The Responsibility Deal is a Coalition response to challenges which we know cannot be solved by regulation and legislation alone .. ..
. a partnership between Government, business and other organisations that balances proportionate regulation with corporate responsibility.”
Established 2010 The partners are working together to:
• recognise their vital role in improving people’s health
• actively support our workforce to lead healthier lives
• encourage and enable people to :
- be healthy and in work
- adopt a healthier diet
- be more physically active
- drink responsibly.
The Responsibility Deal is delivered through five networks :
• Food • Alcohol • Physical activity • Behaviour change • Health at work

Health at Work pledges Nine collective pledges, with tools : - H1. Chronic conditions guide - H2. Occupational health standards - H3. Board Reporting on health and well-being - H4. Healthier staff restaurants - H5. Smoking cessation/Respiratory health - H6. Staff Healthchecks - H7. Mental Health in the workplace - H8. Young persons’ health at work - H9. Domestic violence - H10 Industry-specific pledge for Construction and Civil Engineering

SMEs : A road map Workplace Wellbeing Charter
• Eight workplace standards to promote good, safe and healthy work, evidence-based, SME focussed, locally derived in Liverpool. • Standards are set for Leadership, Attendance Management, Health and Safety Requirements, Mental Health and Wellbeing, Smoking and Tobacco-related ill-health, Physical Activity, Healthy Eating and Alcohol and Substance Misuse.
• An Award is given to organisations that achieve the Charter standards. • All completely voluntary. Employers can use the Charter to assess their approach to workplace wellbeing in whichever way suits their business best - only obliged to share self-assessments if going for an Award.

Collaboration : Workplace Wellbeing Charter
Developed by Liverpool PCT, spread round country, very user-friendly. To improve it: • Public Health England have commissioned Liverpool City Council and Health at Work Centre jointly to refresh the national standards for the Charter ….. • …. and to provide detailed toolkits to support local government and businesses to engage with the scheme.
• The Charter will be supported by topic guides aligned with the Public Health Responsibility Deal showing links between the two.
• An Award is given to organisations that achieve the Charter standards.
Self-assessment Charter much liked by SMEs.

Lessons learnt
• Engage by industry sectors
• Allow sectors to develop their own plans and drivers.
• Form collaborations or coalitions e.g. PHRD, Engage for Success
• Learn from others
e.g. Liverpool Wellbeing Charter
Looking forward : Challenges and Opportunities
• Doctors, especially GPs, still not fully captured • Health at Work Service …. policy into practice?
• Effective intervention at right time …. GPs and employers vital • Mental Health …. problem known, but solutions? (RAND, OECD) • Workplace leadership and management …. crucial, much to do
• Engagement …. and disengagement …. evidence base strong
• Integration of Safety, Health and Wellbeing …. needed for sustainability • Ageing population, obesity, chronic disease …. extending working lives
• Skills deficit. The life span and capability for work.

Final thought
“ In order to act wisely it is not enough to be wise. ”
Dostoevsky

Personal Observations
Major challenges :
• Doctors, especially GPs . Engagement still not fully captured - we have understanding but not adequate action.
• Early co-ordinated interventions
• Government : policy good, but delivery ?
• Business – making the case.
• Each industry sector must own the change, and tailor it to their own needs.

Work Sickness absence
The crucial stage
SSP/OSP
GPs ? Leave Work towards benefits
Transfer into this space is full of danger, unless absolutely necessary
The ‘Holy Grail’ must be early effective intervention and support, by Employers, Health Professionals, Third Sector and Trade Unions. Government is crucial to a satisfactory outcome.

Progress in OH Community
Single organisation : • joined-up multidisciplinary approach, clear roles and competencies • single voice, improved influence, enhanced communication • excellent training, consistent standard setting, CPD • national school, with core training for all OH professionals.
OH Workforce Project :
• vision for future OH practice, service delivery models, planning • knowledge, skills, roles, competencies needed • national audits, national online benchmarking tool.
OH National Standards and Accreditation (SEQOHS) : good progress Recognise the need for :
• links with Public Health, workplace key for health promotion • integrated care to include consideration of work and workplace • to deploy OH skills to support those out of work.

Results 2010: Actions in high-performing Trusts Actions that have been taken by organisations that are progressing well with the NICE guidance include: • assigning responsibility for staff H&WB to a committed and influential board lead who establishes a H&WB Group to interpret data, develop a strategy, and drive forward an action plan
• establishing and communicating the clear link between staff health (including respecting and engaging staff) and the quality of patient care delivered
• engaging staff and managers through frequent assessment of staff health and well-being needs, and including H&WB in staff recruitment, managers’ objectives, training, supervision guidance, and appraisals.
2013 Audit now in progress RCP Health and Work Development Unit

Summary of data from audit Rounds 1 and 2
Setting higher standards
Improvement in most areas in the 3 years between Round 1 and Round 2.
2010 2013

Board engagement – room for more
48%
72%
99%
99% Board member
Absence data
H&WB data
Absence data + H&WB data

Where there is clear NICE guidance we should be using it
Does the trust actively promote healthy food choices , for example using signs, pricing and positioning of products to encourage healthy choices in:
Round 1 Round 2
Vending machines 34% 45%
Shops for staff and clients 34% 53% Hospitality 51% 65%
Staff restaurant 77% 84%
2010 2013
62% evening 27% overnight
Does the trust offer overweight and obese staff interventions that address activity, eating behaviour and weight reduction ?
29% 38%

Mental Health Care Systems
Mental Health Care Systems in most countries often: • do not help with employment issues and do not partner with employers/companies
• leave health care and employment services separate
• do not include employment among care quality indicators
• neglect CMDs and provide few services for them
• leave healthcare professionals believing that work is neither a realistic aim nor beneficial for people with mental ill-health
• provide sparse evidence on Mental Health and connection with work

Occupational Health : National Standards and Accreditation
1. Defining standards of practice to which services should aspire
2. Credit good work by OH services, with independent validation of satisfying standards
3. Raise standards where needed 4. Help purchasers differentiate OH services that
attain the desired standards from those that don’t. Standards published Jan 2010
www.seqohs.org
Produced by Faculty of Occupational Medicine
Accreditation scheme launched 2011 Overall 328 organisations registered (October 2013), 127 fully accredited. Of 150 NHS in-house OH services in England, 132 registered 61 accredited. Review of SEQOHS due 2015.
Multi-channelled (web; Ask-A-Question; Live Chat; phone). Telephone calls averaging 250 monthly – up 18% year-on-year Web traffic rising strongly, visits in excess of 15,000 per month Social media (blogs; tweets) driving 40% of total web traffic 26,045 registrations at end December 2013 within first 2 years 65% of users found the Service via on-line activity Approx 40% of all guides viewed relate to mental health issues 91% of service users are satisfied with on-line knowledge-base and
95% with the specialist OH telephone advice. Only 2% (126) of enquiries are from GPs (35 as employers, 91 as
doctors) but 55% from employers and 26% from employees. Service now in closing phases.
Health for Work Adviceline for GPs Employers and Employees

CrossRail : In the Tunnel
Taking Health and Wellbeing to the tunnel machine face, where the miners work

Innovation by Companies : Unilever Heart Age : Contrasting Data
Marketing Site : Factory Site :
Proportion of people in sample with heart ages in different ranges above their actual age – very different distributions at the two sites.
0 Heart Age above actual 0 +
A simple online tool to find out your estimated Heart Age based on input of personal information on risk factors.
Inequalities of health !

Characteristics of sickness absence in UK
Higher sickness absence is associated in general with the factors and characteristics below. Caution is needed in drawing conclusions as several are inter-related, potentially contradictory, or picking up similar effects.
– Older workers – Women – The public sector – Larger firms – Public administration and health/social work sectors – A trades union at the workplace – Part-time workers – Low paid workers – Those paid at normal rate for the first 7 days of absence – Those in elementary or unskilled occupations – Those with a long-term health condition
Black and Frost, Health at Work, 2011

Sickness Absence in the UK Labour Market Office for National Statistics, February 2014 Key points : • 131 million days lost in 2013, down from 178 m twenty years before • Absence has fallen for all ages since 1993, but least for those 65+ • Sickness absence increases with age but falls after state pension age
• Minor illnesses the most common reason for absence, but more days
lost due to musculo-skeletal problems • Men consistently have lower absence rates than women
• Private sector rates lower, but gap with public sect. less since 1993 • Workers in public sector absent sick 24% more than private sector • Sickness rates highest for public-sector health workers. • Absence lowest for managers, directors, senior officials – and in London • Self-employed less likely than employees to have a spell of sickness. • Largest workforces report highest sickness levels

Work Sickness absence
The crucial stage
SSP/OSP
GPs ? Leave Work towards benefits
Transfer into this space is full of danger, unless absolutely necessary
The ‘Holy Grail’ must be early effective intervention and support, by Employers, Health Professionals, Third Sector and Trade Unions. Government is crucial to a satisfactory outcome.

Keeping people in work Recommendations Black and Frost 2011
Sickness Absence reduction
Independent Assessment
Service
Tax relief on Vocational
Rehabilitation
Abolition of Payment
Threshold Scheme in
SSP
Public Sector –
Review of Sick Pay
Job Brokering
Service
Changes to Employment and Support Allowance
Six major ones ...
... plus six of lesser importance.

Psychological Wellbeing and Work : RAND Europe 2013
Lessons learnt :
• Early access to support is important to prevent people from falling out of work
• Integration of health and employment services critical to shorten client journey
• New and innovative pilots could build better evidence
DWP/DH accepted recommendations, and will pilot
Pilots: 1. Individual Placement and support for those with Common MH problems
2. Group-work based on Jobs 11, successful in USA
3. On-line Assessment and support, with computerised CBT focussed on
employment, leading to 4. Early specialist advice.

Staff Engagement
Archie Norman, writing in the Daily Telegraph, March 2013 : “Our productivity gap is matched by an ‘engagement gap’ … UK output per hour is 15% less than the G7 average. Britain ranks about ninth among the world’s top economies for engagement. Yet MacLeod and Clarke’s work has shown that engaged UK organisations outperform on productivity and on shareholder return. Roots of engagement lie in the culture and values of the business, attitude of management, who you recruit, and how you communicate with them. ” NHS hospitals with high staff engagement have patient mortality rates lower (by 2.5%) than hospitals with medium engagement. Organisations with bottom-quartile engagement average 62% more accidents than those in top quartile on engagement score.

Costs of disengagement
Lack of motivation and sub-optimal health cause UK workers to work below peak productivity, holding back potential growth. Study of 5000 workers • About half of people do not go above and beyond at work because they
think it won’t be acknowledged or rewarded.
• One in four staff admit they don’t want to win new business as it will only mean more work for them.
• Over a third of teams are experiencing extra stress and pressure due to staff ill health and absences.
• Failure to unlock employees’ ‘discretionary effort’ costs businesses dearly, cutting a potential £6 billion – equivalent to 0.4 per cent of GDP – from the UK economy in 2012.
BUPA/Centre for Economics and Business Research, December 2013

NHS Staff Survey 2013 : Results
• Only 41% satisfied with extent they felt their Trust values their work (lowest for ambulance staff at 21%, highest for Clinical Commissioning Groups at 65%)
• Proportion who would recommend their organisation as a place to work up, to 58% from 55% in 2012.
• Only 36% said communication between senior managers and staff is effective; only 28% that managers act on feedback from staff – but 74% said that they can make suggestions to improve work of team or Dept.
• Improvement n proportion of staff receiving appraisals, up to 84% from 82% in 2012. But only 38% said appraisals were well structured.
• Overall Engagement Score up to 3.71 in 2013 from 3.68 in 2012.

Further into the Future ?
• Work is meaningful - and work and life are blurred. • We are paid for output not input - and do shorter formal working hours.
• We are 50% core and 50% contingent workers • We are 50/50 male and female at every level in an organisation • Doing community work one day per work is normal
• Models for success have shifted from senior execs and celebrity • The business world is no longer dominated by uniformity and
standardisation but built on the belief that different people create value • 20-30 year olds love working in corporations and stay more than 2 years
• The traditional concept of retirement is unrecognisable • Our working lives are extended and therefore transformed • Older workers are valued and work part-time extensively • Diversity is celebrated and normal
courtesy Penny de Valk CEO Cedar

Final thoughts
“ Change is the law of life. And those who look only to the past or present are certain to miss the future. ” John F. Kennedy “ Out of intense complexities intense simplicities emerge.” Winston Churchill, The World Crisis, 1931 At the heart of this new vision for the health of the working-age population are three principal objectives :
• prevention of illness and promotion of health and wellbeing
• early intervention for those who develop a health condition, and
• improvement in the health of those out of work – so that everyone with the potential to work has the support they need to do so.
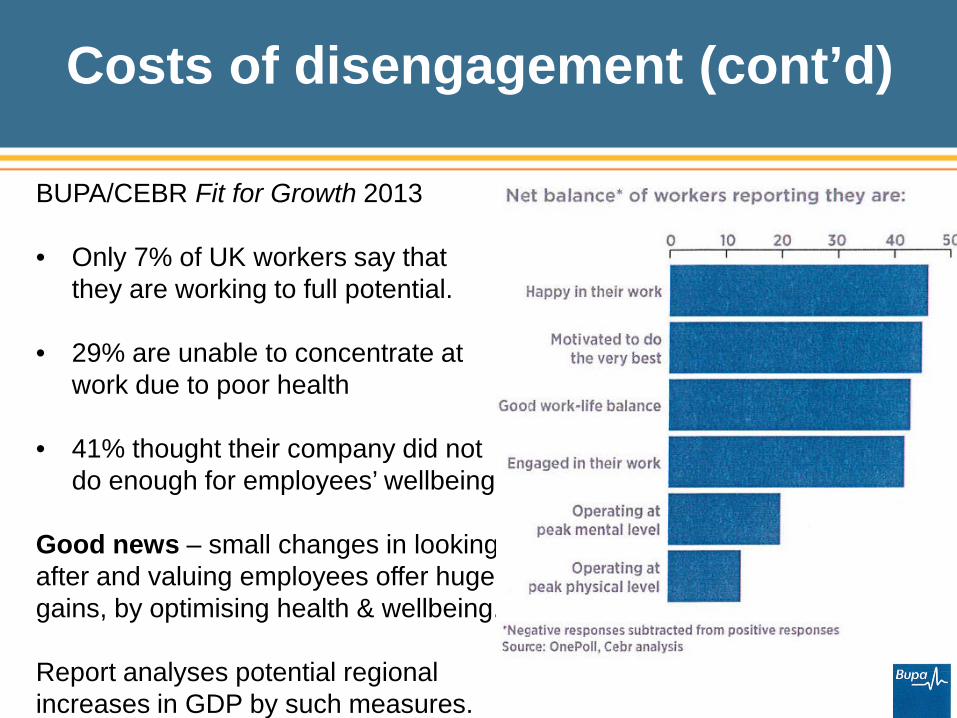
Costs of disengagement (cont’d)
BUPA/CEBR Fit for Growth 2013 • Only 7% of UK workers say that
they are working to full potential.
• 29% are unable to concentrate at work due to poor health
• 41% thought their company did not do enough for employees’ wellbeing
Good news – small changes in looking after and valuing employees offer huge gains, by optimising health & wellbeing. Report analyses potential regional increases in GDP by such measures.

NHS Staff Survey 2013: Results : Key Finding Scores
2013 2012 Satisfied with quality of work/care they deliver 77.8 77.6 % Agree their role makes difference to patients 90.2 89.5 % Work pressure felt by staff score 3.06 3.06 Felt team environment well structured score 3.74 3.73 Working extra hours 70.5 69.7 % Received job-relevant training etc in past year 80.8 80.8 % Appraised in last 12 months 84.3 83.2 % Support from immediate managers score 3.66 3.63 Overall engagement score 3.71 3.68

Future Demographics
• Female employment is projected to continue increasing, reaching 47.5 %
of the total in 2020. • Skills shortages are not all about the economy, mismatch is an issue. • More than one in five Britons will be of an ethnic minority by 2051 • BRIC countries represented 6% of the global economy in 1994, today its
20% and the fastest growing
• By 2035 the number of over-65s is expected to almost double, Europe the most rapidly aging area. By 2040, 1/4 of Europeans will be over 65.
• 56% of people aged 50-65 plan to work beyond state pension age
• Globalisation of labour markets has reshaped
the workforce.


















