Xavier Chitnis & Michael Cooke: Marie Curie service impact
23
© Nuffield Trust The impact of the Marie Curie Nursing Service on place of death and hospital use at the end of life Xavier Chitnis, Michael Cooke Predictive Risk Conference 8 th July 2013
-
Upload
nuffield-trust -
Category
Health & Medicine
-
view
841 -
download
1
Transcript of Xavier Chitnis & Michael Cooke: Marie Curie service impact

© Nuffield Trust
The impact of the Marie Curie Nursing
Service on place of death and hospital
use at the end of life
Xavier Chitnis, Michael Cooke
Predictive Risk Conference
8th July 2013

© Nuffield Trust
Background: End of Life Care at home
• Spending time with loved ones, pain control, and being cared from in their preferred place are among the top priorities for people at the end of life (Engelberg et al. 2005)
• Surveys of the general public and dying people suggest the majority would prefer to die at home (Gomes et al. 2013)
• 51% of deaths in hospital in England in 2011, with only 22% of deaths at home
• The 2011 VOICES survey asked bereaved relatives whether the person who died had enough choice about where they died: Hospital 29% yes, care home 53%, hospice 70%, home 88%.

© Nuffield Trust
Evaluation: The Marie Curie Nursing Service (MCNS)
• Service model: home-based end-of-life nursing care delivered my registered nurses and healthcare assistants, most often 9 hour shifts of overnight care. 30,000 patients per year across UK.
• Longstanding belief: MCNS enables more people to die at home and reduces the amount of time they spend in hospital
• Evidence gaps:
• How many MCNS patients die at home? Service data has gaps.
• How much time do MCNS patients spend in hospital?
• What is a fair comparison? We know ≠ ‘general’ dying population
• Aim: To evaluate the impact of Marie Curie Nursing Service care on place of death, hospital use and costs at the end of life

© Nuffield Trust
Matched control studies – broad aim
>1M individuals - died Jan 2009 to Nov 2011, did not
receive service
(everyone else)
30,000 individuals - died Jan 2009 to Nov 2011 &
received Marie Curie nursing service before death

© Nuffield Trust
Matched control studies – broad aim
>1M individuals - died Jan 2009 to Nov 2011, did not
receive service
(everyone else)
Aim to find 30,000 individuals who match
almost exactly on a broad range of
characteristics
Use these people as study control group
30,000 individuals - died Jan 2009 to Nov 2011 &
received Marie Curie nursing service before death

© Nuffield Trust
Final datasets available for analysis
Nuffield trust
Identifiers:
HESID on all
ONS deaths Hospital inpatient, outpatient, AE MC data - desensitised
Use all this
info to carry
out matched
control
analysis

© Nuffield Trust
Measure Mean (sd)
Age (years) 75.2 (12.1)
Female 47.60%
History of cancer 76.90%
Number of different cancers (in preceding three years) 1.6 (1.3)
Number of chronic conditions 1.5 (1.5)
Median number of days from first MCNS visit to death 8
Characteristics of Marie Curie Cohort (n=31,107)

© Nuffield Trust
Stages in matching process
• Construct longitudinal histories for agreed time periods and estimate costs
• Match on selected variables eg time to death; age; gender; deprivation health conditions/diagnoses; cancer type and history, prior hospital use (IP, OP and A&E)
• Select cases with the best match
• Compare hospital activity and costs

© Nuffield Trust
Period of interest
23rd May 2010
9th March 2010
Date of death Time (days)
First Marie Curie Nursing
Service visit 9th May 2010
Index date 23rd
February 2010
Marie Curie case
Matched control
14 days
Figure 1 - Process for calculating the index date

© Nuffield Trust
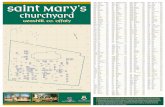
Control group – how well matched?
0%
5%
10%
15%
20%
25%
30%
35%
40%
19-44 45-54 55-64 65-74 75-84 85+
% o
f e
ach
gro
up
Age band
Age
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
% White % Black % Asian % Other
Ethnicity
Ethnicity
0%
2%
4%
6%
8%
10%
12%
14%
1 2 3 4 5 6 7 8 9 10
Decile of deprivation
Deprivation
0%
5%
10%
15%
20%
25%
30%
35%
40%
19-44 45-54 55-64 65-74 75-84 85+
% o
f e
ach
gro
up
Age band
Age
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
% White % Black % Asian % Other
Ethnicity
Ethnicity
0%
2%
4%
6%
8%
10%
12%
14%
1 2 3 4 5 6 7 8 9 10
Decile of deprivation
Deprivation
Marie Curie Controls

© Nuffield Trust
0%
10%
20%
30%
40%
50%
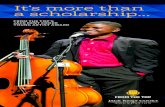
Comorbidities
0%
5%
10%
15%
20%
25%
30%
35%
Cancer diagnoses
Control group – how well matched? Diagnostic history
0%
10%
20%
30%
40%
50%
Comorbidities
0%
5%
10%
15%
20%
25%
30%
35%
Cancer diagnoses
Marie Curie Controls

© Nuffield Trust
Place of death for Marie Curie patients and matched
controls

© Nuffield Trust
Mean (sd) activity per person
Activity type Marie Curie
Matched
controls
Crude
difference IRR P value
Emergency
admissions 0.15 (0.48) 0.44 (0.73) -0.29 0.34 <.0001
Elective admissions 0.06 (0.78) 0.14 (1.16) -0.08 0.47 <.0001
Outpatient
attendances 0.25 (1.65) 0.52 (2.01) -0.27 0.46 <.0001
A&E attendances 0.10 (0.38) 0.34 (0.63) -0.24 0.28 <.0001
Emergency bed-days 1.32 (5.59) 3.60 (8.97) -2.28 0.37 <.0001
Elective bed-days 0.25 (2.38) 0.45 (3.35) -0.2 0.58 <.0001
Hospital activity for Marie Curie patients and matched controls

© Nuffield Trust
Number of emergency admissions per 1,000 people by
day over the last three months of life

© Nuffield Trust
Number of emergency admissions per 1,000 people by
day over the last three months of life (continued)

© Nuffield Trust
Post-index date average hospital costs for Marie Curie
patients and matched controls

© Nuffield Trust
Proportion of deaths at home for Marie Curie patients
and matched controls, by history of cancer

© Nuffield Trust
Difference in adjusted hospital costs per person between
Marie Curie patients and controls, by history of cancer

© Nuffield Trust
Conclusions
• Evaluation of large-scale, existing end-of-life care service using
well-matched controls
• Those who received home-based nursing care:
• Much more likely to die at home
• Lower use of hospital care
• Lower hospital costs
• Impact of MCNS care greater for those without cancer –
surprising finding, although literature limited
• Results confirm previous work on benefits of home-based
support but added significance from numbers studied and the
breadth of service provision

© Nuffield Trust
Conclusions (continued)
• Caveats:
• Other costs – reduction in hospital costs considered against
other costs (including MCNS care), and possible increased
used of other services (e.g. GPs, community services & social
care)
• Unobserved confounders – although groups well-matched,
there may have been unobserved factors not recorded in
routine data influencing suitability for home-based end-of-life
care, e.g. personal preferences, availability of family/carer
support etc.

© Nuffield Trust
Impact for Marie Curie
Understanding our patients
• Much richer understanding of demographic profile, clinical
characteristics and outcomes for MCNS patients
• Outcomes for patients with and without cancer of great interest
Commissioning
• Can demonstrate, for the first time, that service reduces hospital
costs and increases the number of home deaths
• Breakdowns by service type enable us to build much more
robust business cases for the potential impact of new services

© Nuffield Trust
Impact for Marie Curie
‘The report clearly shows that specialist nurses support patient choice, reduce unwanted hospital admission and also appear to realise significant savings.
Nurses see too many instances of patients at the end of their life having to come into hospital, often at night and against their best wishes. This obviously causes distress to individuals and families.
The NHS needs to sustain investment in this specialist, out of hours care, so that wherever and whenever a person dies, they can be given excellent pain-relief, dignity and care.’
Dr Peter Carter, RCN Chief Executive and General Secretary

© Nuffield Trust
www.nuffieldtrust.org.uk
Sign-up for our newsletter www.nuffieldtrust.org.uk/newsletter
Follow us on Twitter: Twitter.com/NuffieldTrust
© Nuffield Trust