
Osteoporosis Ahmed Shaman Department of Clinical Pharmacy [email protected].
Upload
alyson-curtisCategory
view
219download
0
Women’s Health
Ibrahim Sales, Pharm.D. Associate Professor of Clinical Pharmacy
King Saud University College of [email protected]

Lecture OutlinePregnancy & Lactation
DevelopmentalTeratogenicityVitamin supplementation
Gestational complicationsNausea, Vomiting; Constipation & Heartburn
Maternal HealthGestational diabetes, thyroidHypertension (pre-eclampsia), VTE
Contraception
Menopause

Pregnancy40 weeks (280 days or 9 months)
Gestational age First day of the last menstruation2 weeks prior to fertilization
Week 2-8 = Embryonic periodBody structures
Week 9-40 = Fetal periodGrowth and maturity
Congenital Anomalies Minor 10-25% Major 3%
DefinitionsTeratogen – Drug or environmental agent with
the potential to cause abnormal fetal growth and development (thalidomide)
Teratogenicity – Capability of producing congenital abnormalities, major or minor malformations

Causes of Birth Defects
Genetics64%
Medica-tions25%
Unknown11%
Cause of Defect

Influencing FactorsGenotypes of mother and fetus
Embryonic stage at exposure
Medication dose
Simultaneous exposure to other drugs that may increase or decrease

Influencing FactorsTiming of exposure
One month before conception: ≥ Folic acid 0.4mgPrevent neural tube defects
Around time of conception and implantationFirst 12-15 days postconception
If one cell is damaged another can assume its functionFirst 3 months
Physical malformationsThroughout pregnancy: Functional and behavioral
defectsBrain development occurs throughout pregnancy

Vitamin Supplementation
Folic acid 0.4 – 1 mg daily Neural tube defectsNeural tube closure occurs during the first month
of pregnancyMost common major congenital abnormalities
Cleft palate and lipCardiac anomalies
4 mg if on Carbamazepine, Valproic Acid etc
Iron27% anemic in 3rd trimester

Influencing FactorsFactors for placental transport
Molecular weight of drug less than 400–600 Daltons crosses placentaMost drugs weigh 250–400 Da
Degree of protein bindingPlasma albumin decreases in mother and increases in
fetus; higher concentrations of protein-bound drugs in the fetus
Maternal and fetal blood flow usually equivalent

Pregnancy Risk Categories
Risk Category
Definition
A Controlled studies in women fail to show risk
B Animal studies indicate no risk
C No available studies of women or animals
D Positive evidence of fetal risk
X Definite fetal risk in animals or women

Factors to ConsiderRisk-benefit ratio
Is the drug necessary?
Most effective with least risk
Lowest effective dose for shortest possible duration
Health of mother without drug

Gestational Complications

ConstipationPrevalence ranges from 25 to 40%
Nonpharmacologic therapy initially Light physical exercise Increased intake of dietary fiber and fluid
Pharmacologic therapy Osmotic laxatives (polyethylene glycol, lactulose,
sorbiol, and magnesium and sodium salts) Senna and bisacodyl Avoid castor oil and mineral oil
The irritating effects of mineral oil in the bowel also tend to irritate the uterus, which is in close proximity

Gastroesophageal Reflux Disease
Prevalence of up to 80%
Lifestyle and dietary modifications
Antacids (aluminum, calcium, or magnesium preparations) or sucralfate
H-2 receptor antagonists
Metoclopramide
Avoid sodium biocarbonate and magnesium trisilicate 1960 study found an increase in major and minor congenital
malformations in infants; but currently no such association
Reserve PPI for complicated or intractable GERD

Nausea and VomitingPrevalence of up to 90%
Begins around week 5 and continues through the first trimester
Dietary modificationsEating frequent, small, bland meals and avoiding
fatty foods

Nausea and VomitingPharmacologic
MultivitaminsPyridoxine (vitamin B6)AntihistaminesPhenothiazines
(Promethazine and prochlorperazine)MetoclopramideOndansetron Ginger

Gestational DiabetesPrevalance ranges from 1 to 14%
Glucose testing recommended at first prenatal visit if risk factors:ObesityHistory of diabetesGlycosuriaStrong family history
Repeat at weeks 24 and 28 if normal
Test women at weeks 24 and 28 with average risk

Gestational DiabetesLow risk patients are not in need of testing
Low risk patients must fulfill all of the following:Younger than 25 y/oNormal body weightNo known diabetes in first-degree relativesNo history of abnormal glucose toleranceNo history of adverse obstetric outcomesNot a member of an ethnic group with a high
prevalence of GDM (African Americans, Native Americans, Asian Americans, Hispanic Americans, Pacific Islanders)

Gestational DiabetesDietary modification is first-line therapy
Self-monitoring of blood glucose is required
Insulin therapy when on dietary therapy and:Preprandial glucose ≤ 105mg/dL (5.3mmol/L)One hour PPG ≤ 140mg/dL (7.8mmol/L)Two hour PPG ≤ 120mg/dL (6.7mmol/L)
Diabetes Care 2014; 37(1): S14-S80

Women With Pre-existing Diabetes
Optimal glycemic goals
Premeal, bedtime and overnight glucose: 60-99mg/dL (3.3-5.4mmoL/L)
Peak postprandial glucose: 100 – 129mg/dL (5.4-7.1mmol/L)
A1C < 6.0%
Diabetes Care 2014; 37(1): S14-S80

Gestational DiabetesPregnancy Category B Pregnancy Category C
DetemirNPHInsulin lisproInsulin aspart
GlargineInsulin glulisine
Gestational DiabetesOral agents for women who cannot or will not use insulin
GlyburideMetformin

Hypertension Prevalence of 10%
Four categories in pregnancy Chronic hypertension (preexisting) Gestational hypertension (w/o proteinuria) Preclampsia (w/ proteinuria) Preclampsia superimposed on chronic HTN
Mild-to-moderate hypertension Treatment of HTN (140-159/90-109) reduces the risk of severe
HTN by 50%, but doesn’t substantially affect fetal outcomes
Severe hypertension Can cause maternal complications, hospital admission and
potential premature delivery

HypertensionPharmacologic therapy
MethyldopaLabetalolNifedipine (extended-release)
No evidence supports selection of one agent as first-line-therapy
Avoid ACE inhibitors, ARBs, diuretics, magnesium sulfate, high-dose diazoxide, nimopidine, and chlorpromazine

PreeclampsiaWhen a pregnant woman develops high blood pressure
> 140/90 AND protein in the urine after the 20th week (late 2nd or 3rd trimester) of pregnancy
Severe if target organ damage
Treatment IV Labatolol Hydralazine - more hypotension Nifedipine PO 30 mg then 10-20 mg Q4-6 hrs NOT ACE-I, DON’T reduce too quickly
Eclamptic seizures Magnesium 6 g / 15 minute then 1-3 g / hr

Hypothyroidism Occurs in up to 2.5% of pregnancies
Second most common endocrine d/o after DM
50 to 85% will require a dosage adjustment
Treatment of choice: levothyroxine
Empiric treatment Increase levothyroxine dose as soon as a menstrual cycle is missed One method is to take two extra doses per week (i.e., increase
from seven doses to nine doses per week).
Preexisting history or untreated subclinical hypothyroidism TSH should be monitored every four weeks during the first 20
weeks of pregnancy (i.e., first half of pregnancy), and then at least once between 26 weeks and 32 weeks of gestation

Reference TSH RangesTrimester Range (mIU/L)
First 0.1 – 2.5
Second 0.2 – 3.0
Third 0.3 – 3.0
Nonpregnant 0.4 – 4.0

HyperthyroidIncrease in thyroxine binding globulin leads to
increased T3, T4
Propylthiouracil drug of choice

ThromboembolismOccurs in 0.06 to 0.13% of women
5 to 10-fold increase in risk over nonpregnant women
Preferred agent is a LMWH
Alternative is unfractionated heparin
Treatment durationThroughout pregnancy and for 6 weeks postpartum
for acute and prior VTELong-term vitamin K antagonist (VKA)
Adjusted dose or 75% of therapeutic dose of LMWH; restart VKA postpartum

Epilepsy No seizure frequency change in 54 to 80% of women
Risk of untreated epilepsy Drug withdrawal should be planned at least 6 months before
planning to conceive
Polytherapy associated with greater rate of malformation
Carbamazepine and lamotrigine Appear to be safest
Valproic acid 6.2 to 10.7% major malformations
Folic acid supplementation All women taking AEDs should receive FA suppl. 4 to 5 mg daily
before pregnancy and through at least the first trimester

Human ImmunodeficiencyVirus (HIV) Infection
Newly diagnosed women should receive HAART (Highly active antiretroviral therapy) 2 NRTIs (Nucleoside Reverse Transcriptase Inhibitors) plus either a
NNRTI (Non-Nucleoside Reverse Transcriptase Inhibitors) or a protease inhibitor
Women currently receiving therapy should continue
Delay prophylaxis until after the first trimester
Zidovudine and lamivudine Recommended for use during pregnancy, labor, delivery, and the
postpartum period
Nevirapine or lopinavir/ritonavir
Efavirenz Avoid during the 1st trimester and the entire pregnancy if possible

Mental Health Conditions
Nonpharmacologic therapies
Monotherapy is preferred
SSRIs
Benzodiazepines Use in 3rd trimester associated with infant sedation and
withdrawal symptoms
Mood stabilizers Refer to seizure medication section (lithium: cardiovascular
malformations)
Typical and Atypical antipsychotics Typical agents studied more than atypical although atypical are
first line in general population treatment

Medication Effects upon Lactation
Decrease Milk Supply Increase Milk Production
SympathomimeticsNicotineLevodopaBromocriptineErgot alkaloidsPyridoxineMonoamine oxidase inhibitors (MAOIs)EstrogenAndrogens
AntipsychoticsCimetidineMetoclopramideReserpineAmoxapineMethyldopa

Strategies to Minimize Effects
Short-term drug: Mother can pump and discard milk
Choose drugs with short half-lives
Administer drug immediately after a feeding or before a long sleep period
Consider whether the drug is given to neonates

Drugs Contraindicated in Breastfeeding
Contraindicated in Breastfeeding
Amphetamines Bromocriptine
Cocaine Ergotamine
Lithium Nicotine
Antineoplastics Drugs of abuse

Safe Agents During Lactation
Relatively Safe During Lactation
Alcohol (in moderation) Caffeine (in moderation [1 or 2 cups/day])
Analgesics Laxatives
Anticonvulsants Insulin
Antibiotics (penicillins, cephalosporins, erythromycins)


Percentage of FailureTypical Use Perfect Use
No Method 85% 85%
Sponge/Spermicide
16-32%, 29% 9-20%, 18%
Condom 15% 2%
Oral Contraceptives
8% 0.3%
IUD 0.8% 0.6%
Implant 0.05% 0.05%
Sterilization F 0.5%M 0.15%
F 0.5%M 0.5%

Oral ContraceptivesSuppress ovulation, change cervical mucus &
alter endometrium
Synthetic estrogens and progestinsEstrogens:
Ethinyl estradiol 20 – 50 mcg/day (35 mcg usually)Mestranol (prodrug)
Progestins: manyNorethindroneNorgestimate, Desogestrel, Gestodene, DrospirenoneLevonorgestrel (more androgenic – not good)

Female Reproductive System
Ovarian cycle and the menstrual cycleEndocrine system produces hormones that control
these cyclesAverage cycle lasts 28 days
Ovarian cycle Follicular phase and the luteal phase Follicular phase Day 1 to 14
FSH (follicle stimulating hormone)Follicle that contains the egg begins to matureOnce mature, egg is released from ovary into the
fallopian tube and begins the luteal phase

Female Reproductive System
Luteal phaseLH (lutenizing hormone) increasesAllows the corpus luteum to develop from the
follicleNeeded in pregnancy to provide progesterone until
the fourth monthThe ovum (egg) itself does not reach the uterus
until 72 to 96 hours after release

Female Reproductive System
Menstrual cycle
Occurs 14 days after ovulation in non-pregnant females
Four phases: Menstrual, Proliferative, Secretory, and Ischemic phases Menstrual
Days 1 to 6 Estrogen levels are low and the endometrium (inner layer of the uterus) is
shed Proliferative
Days 7 to 14 Endometrial glands in the uterus enlarge due to an increase in estrogen
levels Blood supply to the endometrium is increased and the thickness of the
endometrial layer increases 6 to 8 times Cervical mucus begins to thin to allow sperm easier passage

Female Reproductive System
Menstrual cycle continued… Secretory
Preparation for a fertilized ovum begins Vascularization increases, glycogen stores for nourishment
increase, endometrium continues to thicken Ischemic
Occurs in the absence of fertilization Estrogen and progesterone levels fall, small blood vessels rupture,
blood flow to the endometrium decreases
Fertilization Limited time period
Egg is only fertile for 12 to 24 hours after ovulation Sperm is fertile for only 48 to 72 hours after it enters the female
reproductive tract

Oral ContaceptivesOral formulations differ with regard to the dose, as well as
combination, of progestin and estrogen they contain
Newer formulations of oral contraceptives contain less estrogen and progestin compared to older preparations Reports of increased risk of ischemic stroke, myocardial
infarction, and pulmonary embolism with high-dose estrogen Contraceptive efficacy has not diminished with lower-dose
formulations
Ethinyl estradiol doses: 50 mcg (high-dose) to 20 mcg (ultra-low-dose) Average doses: 30 to 35 mcg
Mestranol: 50 mcg (~35 mcg of ethinyl estradiol)

Oral Contaceptives Current products more closely mimic a woman's natural
menstrual cycle Vary the dose of estrogen, progestin, or both throughout the cycle
Biphasic, triphasic, or quadriphasic Monophasic preparations contain a consistent amount of estrogen and
progestin
Yasmin (ethinyl estradiol/drospirenone) is a combination, monophasic oral contraceptive that is unique in that its progestin is structurally similar to spironolactone 30 mcg of ethinyl estradiol and 3 mg of drospirenone (~25 mg of
spironolactone) Weak potassium-sparing diuretic effect may be preferred by women
who experience water retention associated with their menstrual cycle
Patients should be monitored for hyperkalemia

Oral Contaceptives Progestin-only pill (POP) also known as the mini pill
Oral alternative for lactating women Progestins have not been shown to decrease milk production
Women with contraindications or intolerance to estrogen-containing contraceptives or who would like to become pregnant in the near future (progestin-only pills do not stop ovulation)
Strict adherence to timing of daily dosing is necessary with progestin-only pills Decreased effect of the progestin on the cervical mucosa 22 hours
after the dose is taken A dose that is three hours late is considered missed and should be
taken as soon as it is remembered Recommended to use an alternative means of contraception for two
days following late or missed doses

Oral ContaceptivesProgestin-only pill (POP) continued
Slightly less effective than combination oral contraceptives 99.5% vs. 99.9% for combination products
Associated with a greater degree of irregular bleeding 35% to 45% of women on POPs experience spotting and
breakthrough bleeding throughout the first three months of use; in comparison, 5% to 20% of women using combination oral contraceptives experience these adverse effects
Other common side effects include headache, breast tenderness, nausea, and dizziness

MonophasicContain the same amount of estrogen and progestin in
each active tablet Less likely to cause side effects that may stem from
fluctuating hormones
Classified by their estrogen level: Low dose tablets have the least amount of estrogen (20 mcg) Regular dose pills contain 30–35 mcg estrogen High dose pills have about 50 mcg of estrogen
Work as well as the phasic options
Low estrogen, monophasic pills may cause less bloating or breast tenderness, but may result in more spotting
Biphasic Alter the level of hormones once during the menstrual cycle
Deliver the same amount of estrogen each day, but the level of progestin is increased about halfway through the cycle
Although the estrogen level remains the same, during the first half of the cycle, the progestin/estrogen ratio is lower to allow the endometrium to thicken as it normally does
During the second half of the cycle, the progestin/estrogen ratio is higher to allow for the normal shedding of the lining of the uterus
The first 7 to 10 days are one strength (and usually one color), and the next 11 to 14 tablets are another strength (and another color). The last 7 tablets (if included) are placebo pills and contain no hormones

Triphasic Contain 3 different doses of hormones in the 3 weeks of active
tablets
The hormone combination changes approximately every 7 days throughout the tablet pack
The amount of estrogen may change as well as the amount of progestin May have a gradual estrogen increase and/or some pills may also
increase the dose of progestin 3 different strength combinations in each pack The first third of tablets consist of one strength (and one color) The next 5, 7 or 9 tablets are another strength (and another color) The final phase of tablets are a different color The last 7 tablets (if included) are placebo pills and contain no
hormones

QuadriphasicFor the first 2 days, the tablets consist of one
strength (the first phase)
The next 3 to 7 days, a second strength (the second phase)
Days 8 to 24, a third strength (the third phase)
For days 25 and 26, a fourth strength
Two days of inactive tablets

Other Hormonal Contraceptives
Injectable Q 3 months; 6-12 month infertilityMedroxyprogesterone (Depo-Provera)
Implant Q 3 yearsEtonogestrel
Intrauterine Device (IUD)Copper or levonorgestrel
Emergency Oral Contraceptionwithin 72 hours

Contraindication & Risks
Absolute Previous VTE or Stroke Estrogen-dependent tumor Active liver disease Pregnancy Undiagnosed abnormal
uterine bleeding Hypertriglycerides Age > 35 years and
smokes > 15 cigarettes/day
Relative Hypertension Anticonvulsants
Increased MI (smokers > 35 years Hypertension (RR = 1.8) VTE (RR = 4) Stroke if also htn Cervical CA (RR = 2-4)
Decreased Ovarian CA (50% less) Endometrial CA (40% less)
Benefits Regulate menses Reduce ectopic pregnancy,
benign breast disease. Improve hirsutism & acne

Pill Early Danger Signs (ACHES)
Signals Possible Problem
Abdominal pain (severe) Gall bladder disease, hepatic adenoma, blood clot, pancreatitis
Chest pain (severe), shortness of breath or coughing up blood
Blood clot in lungs or myocardial Infarction
Headache (severe) Stroke, hypertension or migraine headache
Eye problems: blurred vision, flashing lights or blindness
Stroke, hypertension or temporary vascular problem
Severe leg pain (calf or thigh)
Blood clot in legs

Practical Issues – Patient Education
Start taking pills by following manufacturers recommendations
Use back up method for first week at least when starting
Take at same time every day
If you miss one dose, take two pills the next day
If you miss more than one dose, follow package insert including using backup method for at least one week

Practical IssuesDrug Interactions leading to spotting,
breakthrough bleeding or pregnancyAny antibiotic via altering intestinal bacterial floraDrugs (including antibiotics) that alter
enterohepatic circulationEnzyme inducers (rifampin, phenytoin etc)
Unlikely, but safest to use alternative method
MenopauseLoss of ovarian follicular activity
Stop making estradiol, progeteroneStarts making androgens (testosterone)Not all at once, rather in phases
Symptoms 4 years before menses stopIrregular cycles, Vasomotor, Mood, Sexual
Hormonal clues10 – 15 x increase in FSH4-5 increase in LH90% decrease in estradiol

TreatmentWhy treat?
Short term for symptoms (70 – 80% reduction) Long term for osteoporosis prevention (HR 0.66)
20 – 50 % decreased risk of fracture
Risks of therapy? Endometrial CA if not given with progestin (HR 3-6) Women’s Health Initiative 16,608
Thrombosis (HR 2.13)Cardiovascular disease (HR 1.29)Stroke HR (1.41)Breast Cancer HR (1.26)Gall bladder disease (110% increase risk)

Estrogen for SymptomsSystemic
Oral EstrogensConjugated equine estrogens (Premarin 0.625 mg)Give with progestin if patient has uterus
Medroxyprogesterone acetate Protect against endometrial cancer
Otherwise (i.e after hysterectomy) estrogen aloneLess effective: Antidepressants, gabapentin,
clonidine, vitamin E phytoestrogens
Topical for local (genitourinary) symptoms

Estrogen for Osteoporosis
Safer alternatives now availableCalcium & vitamin DBisphosphonatesSelective Estrogen Receptor Modulators
Estrogen agonist on bone, antagonist at other tissues Tamoxifen Raloxifene

Women’s HealthIbrahim Sales, Pharm.D.
Associate Professor of Clinical PharmacyKing Saud University College of Pharmacy


Oral Estrogen Products

Vaginal Estrogen Products
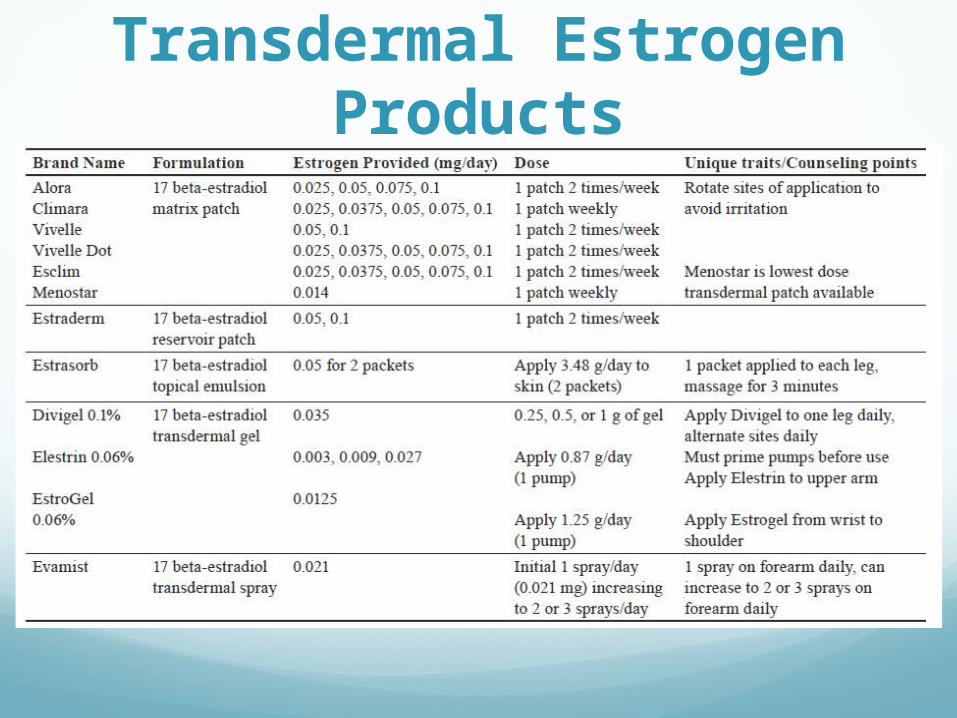
Transdermal Estrogen Products
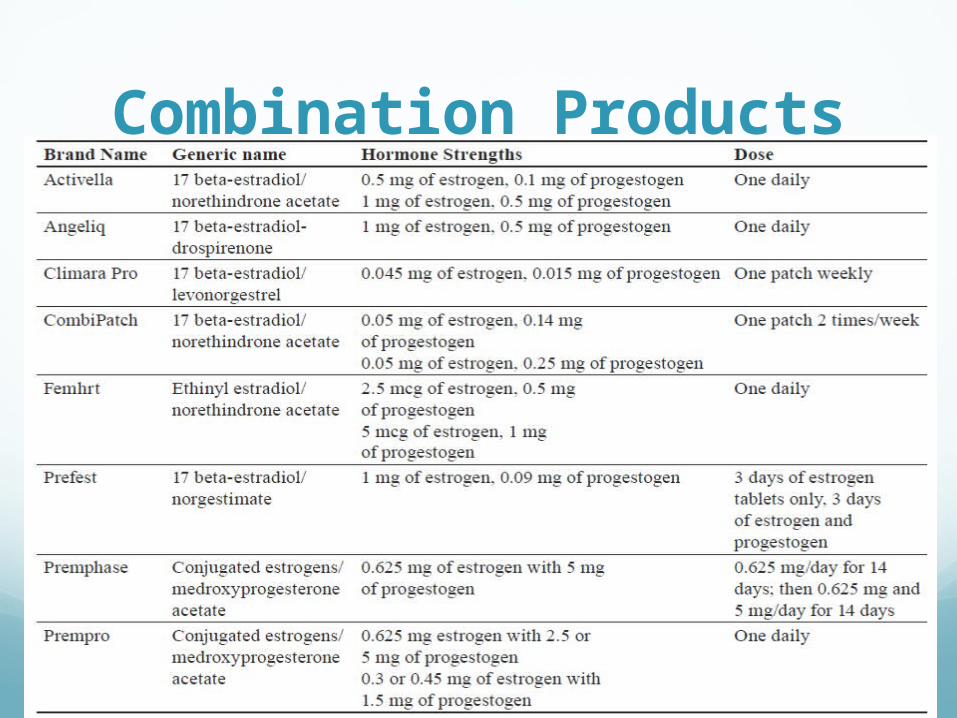
Combination Products

Progestogen Products

Category X Medications HMG CoA Reductase Inhibitors (Statins)
Cholesterol synthesis important in fetal development
Oral Contraceptives Controversial
Ergotamines Convulsions, vomiting, diarrhea, gangrene
Ethanol Fetal Alcohol Syndrome
Isotretinoin Abnormalities, spontaneous abortion
Methotrexate Immune system dysfunction
Raloxifene Spontaneous abortion

Category D MedicationsACE Inhibitors
2nd and 3rd trimester Renal defects
Benzodiazepines Neonatal withdrawal, respiratory problems
ASA Doses > 81mg/day Closure of the ductus arteriosus, inhibit labor
Atenolol Intrauterine growth retardation

Category D Medications Carbamazepine
Neural tube defect
Divalproex Neural tube defect, facial abnormalities
Doxycycline 2nd and 3rd trimester Tooth abnormalities
Angiotensin Receptor Blockers 2nd and 3rd trimester Renal abnormalities
Lithium Cardiovascular dysfunction

Category D Medications NSAIDS
Use near term may cause premature closure of the ductus arteriosus, inhibits labor
SSRIs Congenital malfromations, neonatal behavior syndrome,
persistent pulmonary hypertension
Phenobarbital Sedation, withdrawal, blood dyscrasias
Phenytoin Fetal Hydantoin Syndrome
Warfarin Facial abnormalities, fetal hemorrhage


















