
Constipation By: Dr. Shahram Ala (Pharm.D, BCPS) (Pharm.D, BCPS)
Upload
jade-georgeCategory
view
224download
2
Migraine Headache
Ibrahim Sales, Pharm.D.Associate Professor of Clinical Pharmacy
King Saud [email protected]

Epidemiology & Etiology
• Migraines – 10-15% of adults in the US, 34 million worldwide
• Tension-Type Headache– 30 – 90% of population per year• 5% have them chronically (> 15 attacks /month)
– Females > Males
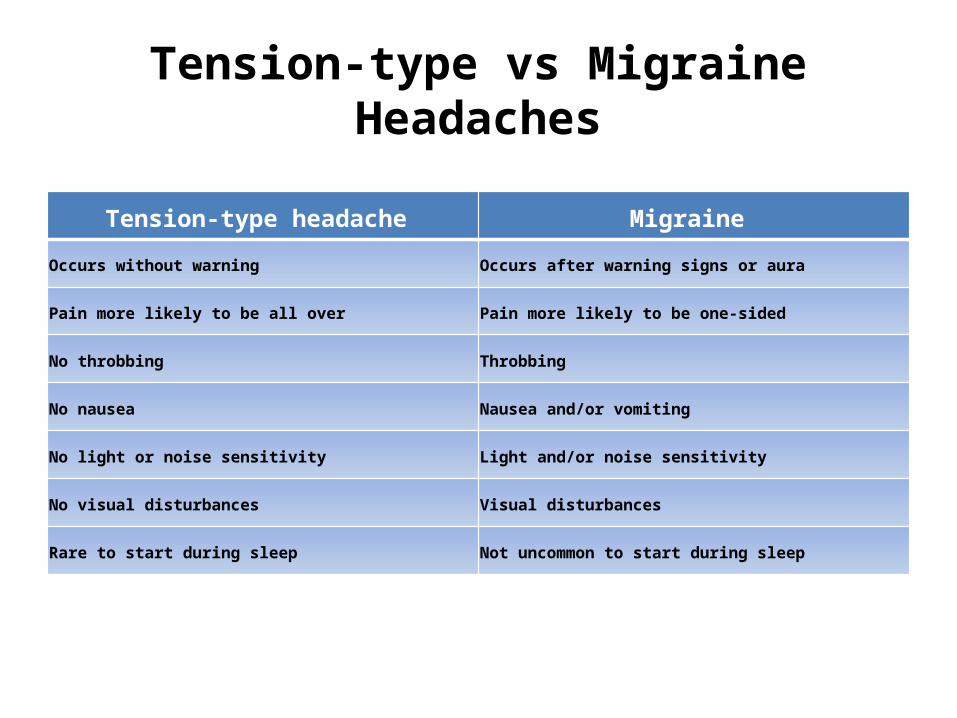
Tension-type vs Migraine Headaches
Tension-type headache Migraine
Occurs without warning Occurs after warning signs or aura
Pain more likely to be all over Pain more likely to be one-sided
No throbbing Throbbing
No nausea Nausea and/or vomiting
No light or noise sensitivity Light and/or noise sensitivity
No visual disturbances Visual disturbances
Rare to start during sleep Not uncommon to start during sleep

Clinical Presentation

International Headache Society Diagnostic Criteria
Migraine without aura Migraine with aura
Diagnostic criteria:Headache lasts 4-72 hours (untreated or unsuccessfully treated)
Headache has at least two of the following:• Aggravation by or causing avoidance of
routine physical activity (e.g. walking)• Moderate or severe pain intensity• Pulsating quality• Unilateral locationDuring headache, at least one of the following:• Nausea and/or vomiting• Photophobia and phonophobiaNot attributed to another disorderHistory of at least five attacks fulfilling above criteria
• Recurrent disorder manifesting in headaches of reversible focal neurologic symptoms that usually develop gradually over 5-20 minutes and last for less than 60 minutes
• Headache with the features of migraine without aura usually follows the aura symptoms
• Less commonly, headache lacks migrainous features or is completely absent
Diagnostic criteria:Aura consisting of at least one of the following, but no motor weakness:• Fully reversible dysphasic speech disturbance• Sensory symptoms that are fully reversible, including positive features
(pins and needles) and/or negative features (numbness)• Visual symptoms that are fully reversible, including positive features
(flickering lights, spots) and/or negative features (loss of vision)At least two of the following:Homogeneous visual symptoms and/or unilateral sensory symptomsAt least one aura symptom develops gradually over 5 minutes or different aura symptoms occur in succession over 5 minutesEach symptom lasts at least 5 minutes, but no longer than 60 minutesHeadache fulfilling criteria for migraine without aura begins during the aura or follows aura within 60 minutesNot attributed to another disorderHistory of at least two attacks fulfilling above criteria

Diagnosis
• POUND– Pulsatile quality of headache– One-day duration (four to 72 hours)– Unilateral location– Nausea or vomiting– Disabling intensity
• In a primary care setting, the probability of migraine is 92% in patients who report at least four of the five symptoms
• The probability decreases to 64% in patients with three of the symptoms and 17 % in patients with two or less symptoms

Treatment Evaluation
Migraine Disability Assessment Test (MIDAS)– Validated, seven-item questionnaire to determine
the severity of migraine headaches– Addresses limitations in activities at work and
home as well as social and leisure activities– The score is a sum of missed days of activities at
work/home and reduced productivity over 3 months
– Final two questions assess frequency and pain
MIDAS Questionnaire

Classification
MIDAS questionnaire cont.• Grade I (sum of 0 – 5): Minimal or infrequent
disability• Grade II (sum of 6 – 10): Mild or infrequent
disability• Grade III (sum of 11 – 20): Moderate disability• Grade IV (sum of 21 or greater): Severe
disability

Seek Urgent Medical Evaluation
• New onset of sudden and/or severe pain• Onset after 40 years of age• Usual pattern gets worse• Systemic signs (fever, weight loss)• Papilledema• Cough, exertion • Pregnancy or post partum• Cancer, HIV or other immunodeficiency/infection• Seizures

Treatment Goals
• Identify abortive and prophylactic treatments• Reduced migraine attack frequency• Reduced number of migraine days• Reduced attack severity• Relieve associated adverse effects• Enhance quality of life

Drug Therapy
• Treatment:– Analgesics• APAP, ASA, NSAIDs; Opiods; • Caffeine & Metoclopramide
– Serotonin (5-HT1) Receptor Agonists– Ergot Alkaloids
• Prevention– Beta-blockers, CCB– AED, TCA, et al.

Analgesics
• First-line for mild to moderate migraines– Aspirin– NSAIDs– Acetaminophen– OTC combinations
• acetaminophen, aspirin & caffeine (Excedrin Migraine)• acetaminophen, isometheptene & dichloralphenazone (Midrin)• aspirin, caffeine and butalbital* (Fiorinal)• acetaminophen, caffeine and butalbital* (Fioricet)

Aspirin
• MOA: Inhibits prostaglandin synthesis by inhibiting COX-1 and COX-2 enzymes thereby reducing sensitivity of pain receptors to the initiation of pain impulses at the source of inflammation
• Immediate-release, buffered, enteric coated, effervescent and chewable tablets
• 650 – 1000 mg every 4 – 6 hours up to 4000 mg• Adverse effects: GI bleeding, dyspepsia, epigastric
discomfort, nausea, and vomiting; Reye’s syndrome• Should be taken with food

NSAIDS
• MOA: Inhibition of prostaglandin synthesis through peripheral inhibition of COX enzymes
• Ibuprofen: Immediate release and chewable tablets; capsules– 200 – 400 mg every 4 – 6 hours up to 1200 mg
• Naproxen: Tablets– 220 mg every 8 – 12 hours up to 660 mg– Longer t1/2
• Adverse effects: GI bleeding, dyspepsia, heartburn, nausea, epigastric pain
• Should be taken with food

Acetaminophen
• MOA: Inhibition of prostaglandin synthesis by inhibiting COX enzymes in the CNS
• Immediate-release, extended-release, effervescent, chewable tablets, capsules, suppositories
• 325 mg – 1000 mg every 4 – 6 hours– Maximum previously was 4000 mg

Combination Products
• Acetaminophen, 250 mg/aspirin, 250 mg/caffeine, 65 mg (Excedrin Migraine)– 1 or 2 tablets (or capsules) every 6 hours, not to
exceed 8 tablets per day • Acetaminophen, 325 mg/dichloralphenazone, 100
mg/isometheptene, 65 mg (Midrin)– 1 to 2 capsules orally every 4 hours; not to exceed 8
capsules per day • Potential to cause medication-overuse headache
with frequent use

Analgesics• Opioids
– Studies have demonstrated effectiveness in pain relief– Guidelines for use:
• Infrequent use in the treatment of moderate-to-severe headaches not responsive to standard medications
• For acute headache when nonopioid medication has failed or is contraindicated, or in the presence of a coexistent disease or lack of diagnosis
• As rescue medication for severe, middle-of-the-night headache • In patients with no history of abuse • Limit use to 1 or 2 treatment days per week. Set strict limits and prescribe small amounts to
avoid overuse. Relax restrictions with menstrual migraine• Barbiturates
– Butalbital; butorphanol – Issues: overuse, drug-induced headache, and withdrawal– Withdrawal symptoms
• Minor (e.g., restlessness, anxiety, sleep disturbances, tremulousness, and gastric distress) • Major ≥400mg/day (e.g., agitation, delirium, psychosis, hypotension, hyperthermia, and
seizures)

Serotonin (5-HT1) Receptor Agonists“Triptans”
• First-line therapy in moderate to severe migraine or mild to moderate migraine unresponsive to analgesics
• 5-Hydroxytryptamine (5-HT): 5-HT1B, 5-HT1D Agonists– MOA: Block release of vasoactive peptides
• Take early in attack for best effect• Most patients prefer oral form (if no N/V)• 20-40% will have recurrence within 24 hours– Give second dose of same triptan up to maximal daily dose

Serotonin (5-HT1) Receptor Agonists“Triptans”
• Sumatriptan (SC, NS, PO)– SC & NS good if associated N/V– Relief at 2 hours depends on dosage form
• SC = 80%, NS = 60%, PO 50 – 60%
• Almotriptan (Axert), Eletriptan (Relpax), Rizatriptan (Maxalt), Zolmitriptan (Zomig), Frovatriptan (Frova)– All are similar in effectiveness and tolerability
Triptan Clinical Pearls• A 100mg dose of sumatriptan may be more effective than lower doses• It is sometimes necessary to increase the dose of an individual agent
before judging response• Nonresponders to one triptan may respond to another• Zolmitriptan tastes “better”• Rizatriptan has a quicker onset of action than sumatriptan• Frovatriptan, naratriptan, and eletriptan have longer t1/2 than
sumatriptan• Matching the pharmacokinetics to the temporal pattern of the
migraine– Rapid onset medication for short course migraine vs. long-acting medication
for slower onset, long lasting symptoms

Triptans• Almotriptan (Axert)
– 6.25 to 12.5 mg orally, can be repeated in 2 hours, not to exceed 25 mg per day • Eletriptan (Relpax)
– 20 to 40 mg orally, can be repeated in > 2 hours, not to exceed 80 mg per day • Frovatriptan (Frova)
– 2.5 mg orally, can be repeated in 2 hours, not to exceed 7.5 mg per day• Naratriptan (Amerge)
– 1 to 2.5 mg orally, can be repeated in 2 hours, not to exceed 5 mg per day • Rizatriptan (Maxalt)
– 5 to 10 mg orally, can be repeated in 2 hours, not to exceed 30 mg per day • Sumatriptan (Imitrex)
– Intranasal: 5 to 20 mg, can be repeated in 2 hours, not to exceed 40 mg per day – Oral: 25 to 100 mg, can be repeated in 2 hours, not to exceed 200 mg per day – Subcutaneous: 4 to 6 mg, may repeat in 1 hour, not to exceed 12 mg per day
• Zolmitriptan (Zomig, Zomig-ZMT) – Intranasal: 5 mg, may repeat in 2 hours, not to exceed 10 mg per day– Oral disintegrating tablets: 2.5 mg, can be repeated in 2 hours, not to exceed 10 mg per day– Oral: 1.25 to 2.5 mg, can be repeated in 2 hours, not to exceed 10 mg per day
• Sumatriptan, 85 mg/naproxen, 500 mg (Trexima) – 1 tablet at onset, may repeat in 2 hours, not to exceed 2 tablets per day

Triptan Adverse Effects
• Tingling, flushing, dizziness, drowsiness, fatigue & feeling of heaviness, tightness or pressure in chest with all– Uncomfortable but not life threatening…– Highest with Sumatriptan Injection*
* Also causes injection reaction
• Cardiovascular vasoconstriction– Rare: angina, MI, arrhythmia, stroke & death– Contraindications:
Coronary, CV or other arterial disease, uncontrolled HTN– Caution with other vascular disease

Triptan Drug Interactions & Issues
• Avoid giving within 24 h of Ergot, another triptan (additive vasoconstriction)
• Risk of Serotonin syndrome with SSRI, SNRI’s• Need 2 week washout from Monoamine
oxidase inhibitors (MAO-I) for some– Rizatriptan, sumatriptan, zolmitriptan
• CYP-3A4 with Almotriptan, Eletriptan• Pregnancy Category C

Ergot Alkaloids
• Serotonin agonist – vasoconstrictor• Less effective than triptans in general, may
work in triptan-refractory patients• Ergotamine tartrate– Combination with caffeine may have fewer
adverse effects than pure ergotamines • Dihydroergotamine mesylate– SC, IM, IV or sprayed intranasally– Relief in 2 hours for 50% of patients

Ergot Alkaloids
• Ergotamine tartrate + Caffeine– 2 tablets at onset of attack, then 1 tablet every ½ hour if
needed; max 6 tabs/attack, 10 tabs/week.• Dihydroergotamine (DHE; Migranal) – Intranasal: 1 spray in each nostril, repeat once after 15
minutes; not to exceed 4 sprays per attack, 6 sprays per day, 8 sprays per week
– IV: 0.5 to 1 mg repeated every 8 hours, or continuous IV infusion totaling 3 mg per 24 hours; not to exceed 3 mg per attack
– Subcutaneous: 1 mg every hour; not to exceed 3 mg per day

Ergot Adverse Effects
• Dihydroergotamine < Ergotamine• Nausea / vomiting common • Vascular occlusion (MI, gangrene) rare except in
overdose• Contraindicated in pregnancy• Potentiated by beta-blockers, nicotine, triptans– Don’t give triptans/ergot within 24 hrs of each other
• CYP-3A4 inhibitors– contraindicated with clarithromycin, itraconazole

Prevention
• Frequent or severe migraine, or those that can’t take / don’t respond to acute treatment
• Beta-blockers (usual ADE’s, contraindications)– Propranolol, Timolol FDA approved• Metoprolol, Nadolol, atenolol work
• Tricyclic antidepressants (sedation, dry mouth)– Amitriptyline has best data, others used too

Prevention
• Calcium Channel Blockers– Verapamil shown better than placebo– Interacts with ergots via CYP-3A4– Don’t use with beta blockers (heart block)
• Antiepileptic drugs– Valproate, topiramate = best data– Half of patients will have > 50% reduction in frequency of
migraines– VPA: Nausea, fatigue, tremor, weight gain & hair loss
• Liver failure, pancreatitis, hyper-ammonemia et al
• Others: ACE-I, NSAIDs…

Preventative Evidence
Summary
• Mild to moderate: non-opioid analgesic– Acetaminophen (esp. if pregnant), ASA, NSAID
• Moderate to severe: triptan– Sumatriptan SC is fastest, most effective– May try different one if inadequate response– Ergots are not as effective, more toxic
• Prevention– Beta-blockers, AEDs 1st line• VPA, topiramate work but ADE’s…


















