Why Do the Pleural Pressure Go Negative

of 5
Transcript of Why Do the Pleural Pressure Go Negative
-
8/14/2019 Why Do the Pleural Pressure Go Negative
1/5
Coop 2010Physiology - lecture 53March 12, 2007 9-10amLecturer: Dr. Forster Writer: Jena Kern
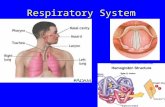
Respiratory Structures
Dr. Forster started the lecture with a brief review of the anatomical structures involved inrespiration. He mentioned that the muscles of inspiration are the diaphragm and theexternal intercostals, and the muscles of expiration are the internal intercostals andabdominal muscles. These muscles function as a respiratory pump, which creates achange in pressure and allows air to flow. He also mentioned that CNS apnea is whereyou wont breath and obstructive apnea is where you cant breath. 15-20% of Americanshave sleep disordered breathing.
Respiratory Mechanics
1. How do you define respiratory mechanics?It is a relationship between volume, pressure and flow.3 main pressures that deal with mechanics: these are important
1. Pleural pressurepressure between chest wall and lungs (virtual space)2. Alveolar pressurepressure within alveoli, is pressure that causes flow(less than atmospheric during inspiration, greater than atmospheric duringexpiration)3. Transpulmonary pressure (aka recoil pressure) difference betweenalveolar and pleural pressures. P TP =P A-P pl. Reflects pressure required toovercome lung elasticity since the lungs want to totally collapse. Cantuse pleural and transpulmonary pressures interchangeably, they are
different as we will see later.2. What causes air to flow between atmosphere and alveoli?
Keep it simple. Air only flows if theres a pressure difference. If alveolar pressure is less than atmospheric pressure air will flow in. If it is greater thanatmospheric pressure air will flow out.
3. What causes alveolar pressure to change during inspiration?It changes because pleural pressure changes. Part of the change in pleural
pressure is transferred to alveoli to give subatmospheric pressure. During eupnea pleural pressure is always slightly negative. Then during inspiration it becomes even morenegative, causing alveolar pressure to become negative.
4. What causes pleural pressure to change during inspiration?Due to action of inspiratory pump muscles. The diaphragm and intercostals
contract to expand the chest (space increases so pressure decreases).
5. Why during inspiration and expiration does alveolar pressure change less than thechange in pleural pressure? (figure is in Guyton, p. 472)
-
8/14/2019 Why Do the Pleural Pressure Go Negative
2/5
Lung volume increases and air goes in during inspiration (tidal volume) Pleural pressure goes down during inspiration Alveolar pressure goes down during inspiration (becomes subatmospheric). It
does not change as much as pleural pressure because a portion of the changein pleural pressure is needed to overcome elasticity of lungs. The lungs wantto totally collapse.
Transpulmonary pressure increases during inspiration.
6. What causes alveolar and pleural pressure to change during expiration?The change is passive while resting, no energy is required. The recoil of lungs
creates positive alveolar pressure, which causes air to move out. Also, when youexercise, the expiratory muscles contract since need for ventilation is so great and youget a more rapid flow.
7. What is the relationship between pleural pressure and lung volume during inspirationand expiration? (see figure on p. 585)Dr. Forster spent a lot of time on this figure and stated it was very important. Hesaid he would go over it a couple more times throughout his lectures.
Pleural pressure goes negative during inspiration, while lung volume increases.So you are basically following the bottom of the oval as you inspire. At end of inspiration, you relax and then air flows out, which is the top part of the oval. Dr. Forster then gave an example of a breath half as large as the breath in the figure and the oval wasabout half as large (the end of the oval was about half way down the original oval). If you double the tidal volume (volume of each breath), it will get larger. At each reversal
point, there is a few milliseconds where there is no air flow so alveolar pressure is zero.This pressure at that point is needed only to overcome the elastic recoil.
The slope of the line connecting the beginning of the breath and the reversal pointreflects the force necessary to prevent recoil or overcome the elasticity. This is thecompliance given by the following equation:
C=V/P TP (he stated the key thing is the transpulmonary pressure)At each reversal point, transpulmonary pressure equals the pleural pressure since flow iszero and alveolar pressure is zero. He said you can get a feel for the recoil if you take alarger than normal inspiration and then at the end of the inspiration, hold your breath,
pinch your nose and relax. Your cheeks puff out because the lungs have recoiled andcreated a positive pressure which normally results in expiration. He then stated thatrecoil pressure is the same as transpulmonary pressure.
Back to the figure. Everything to the left of the diagonal line is the pleural pressure change needed to overcome elasticity. The area to the right of the diagonal is
alveolar pressure (pressure needed to overcome the loss of energy due to air molecules bumping against each other and the airway). We can calculate resistance by thefollowing equation:
R=P A/f (pressure is alveolar pressure, f is flow)(He didnt say this this year, but its probably good to know)He said that on the test, hecould give us a flow and then we would need to obtain the alveolar pressure from the
figure by drawing a horizontal line from the diagonal line straight across to thecorresponding point where the shaded oval ends. This number or pressure difference is
-
8/14/2019 Why Do the Pleural Pressure Go Negative
3/5
the P A. We could then calculate airway resistance from these numbers. Dr. Forster said we need to know how to use this graph to obtain transpulmonary pressure tocalculate compliance and alveolar pressure to calculate resistance.
His main point was that we have to extract alveolar pressure and transpulmonary pressure from pleural pressure as described above.
8. What is the relationship between transpulmonary pressure and lung volume?(The figure on pg 586 is lung at three different volumes, x-axis is transpulmonary
pressure or how much lungs want to recoil)RV (residual volume)--lowest volume we can reach in lungs (about 20% of lung
capacity). We will still have air in lungs even after we forcefully expire and lungs willwant to recoil. VC (vital capacity) is maximal amount of air we can inhale. As you moveup the curve, there is a greater tendency for lungs to want to recoil. So there is a greater
pressure required to maintain a larger volume. This is the compliance curve, so there is adirect relationship between P TP and VC that is not linear since it levels off at higher lungvolumes.
What is lung compliance? Lung compliance is the relationship between change involume and change in transpulmonary pressure reflecting the elasticity of lung.What is difference between static and dynamic lung compliance? The difference
is only in how compliance is measured. Dynamic compliance is measured during normal breathing and the two endpoints are taken to measure P TP. Static is measured by holding breath (a purposefully stop) at each reversal point. They both give the same value innormal individuals, but in disease states, static compliance is more useful.
9. How does relationship between volume and pressure differ between an air filled and asaline filled lung?
We will create these graphs in lab.The major difference in curves is it takes more pressure to fill a lung with air than
it does with saline. With saline, the entire elastic force is due to tissue itself. With air filled, there is an added contribution of surface tension. Surface tension is due to theliquid molecules attracting each other on an air-liquid interface, which acts as an elasticcomponent. Here is the equation for surface tension:
P=2T/r (T is surface tension of a specific liquid and r is radius of airway)This is reduced in alveoli due to surfactant production from type II pneumocytes. Fromthe equation, one can see that the collapsing pressure created would be greater for a smallalveoli than for a large alveoli. The concentration of surfactant is higher at low lungvolumes than at high lung volumes so because of this, as lung volume increases, surfacetension actually increases thereby minimizing small alveoli emptying into large alveoli(figure at bottom of page sort of helps to explain this). Another way to describe thisrelationship is as lung volume increases surface tension increases because the density of surfactant molecules on the surface becomes less. If we didnt have surfactant we wouldneed to work harder to overcome elasticity.
The next page (p. 588) shows compliance curves for normal and diseasedindividuals. Emphysema patients have a very high compliance because they have lostelasticity. They have had a destruction of elastic tissue and its easier to fill the airways.The fibrosis curve shows low compliance because the lung is stiff due to environmental
-
8/14/2019 Why Do the Pleural Pressure Go Negative
4/5
pollutants or in respiratory distress syndrome. The lung becomes less distensible andcompliance and elasticity is increased.
10. What are the elastic characteristics of the chest wall?
The chest wall has elastic characteristics. The lungs want to go to zero (this istheir equilibrium position). The chest wall's equilibrium position is about 60% vitalcapacity. To go either below or above this, you need work or energy.
11. At the end of a normal expiration (FRC), the lungs remain partially filled. Why?(Graph is pressure vs. vital capacity)The lung and the chest wall act as a unit and this graph reflects their opposing
tendencies. The lines show the lung wanting to go to zero and the chest wall wanting togo to sixty. When you put the two together, the lungs want to suck the chest in, the chestwall wants to pull the lungs out. So in a completely relaxed position, you end upsomewhere in between, which is the functional residual capacity (FRC). This value is
about 40% total lung capacity in a normal individual. In emphysema, FRC increases dueto loss of lung recoil. In fibrosis, the opposite occurs. The answer to the question aboveis because it reflects the balance between the chest wall and lungs going toward their ownequilibrium position.
12. What factors determine airway resistance? Length of airway Diameter of airway --major determinant (and the one you can change) Density of gas molecules (helium gives a decrease in resistance)
13. What is the importance of lung elastic tissue on airway diameter?
Elastic tissue of the alveoli exerts attraction to help keep airway open. First graphis airway resistance vs. volume. This shows that resistance is much higher at lowvolumes than high volumes. At high volumes the elastic tissue acts as a tether, or tugsto hold airways open. This does not occur at low volumes. In emphysema, you have lesselasticity so less tethering action resulting in smaller airways and increased resistance.
The second graph is resistance vs. airway generation. The table on the next pagegoes along with this graph. Over the first four generations, the total cross sectional areadecreases resulting in an increase in resistance. Afterward, the total cross sectional areaincreases even though diameter of each individual airway will decrease. This is due to anincrease in the number of airways. So, overall resistance is lesser deep in the lungs thanit is in the upper airway. The greatest resistance to airflow occurs in the upper airway.
*From last years co-op Dr. Forster then mentioned four diseases of increased airway resistance due tonarrowing. They are:
-emphysemaincreased resistance due to reduced tethering -chronic bronchitis--due to increased mucus production-asthmadue to constriction of airway smooth muscle-loss of dilation in larynx and pharynx (obstructive sleep apnea and snoring)
-
8/14/2019 Why Do the Pleural Pressure Go Negative
5/5
14. What is the relationship between maximum expiratory flow and lung volume?The graph at the top of the page shows relationship between flow and lung
volume. Curve A shows a maximal effort. Flow decreases even though you are pushingas hard as you can throughout. Why does flow go down even though you are maintaining
same effort throughout? This happens for two reasons. The first is that the drivingalveolar pressure for flow will decrease as lungs reach lower volumes (recoil pressure becomes less so driving pressure is less while pleural pressure remains at its max). Thesecond reason is because the resistance will increase because the tethering action of theelastic tissue on the airways becomes less so airways become smaller.
Curves B and C shows exerting 50 and 25% max effort. The peak flow decreases because pleural pressure is less. At low volumes flow or expiration becomes independentof effort.
The reason you reach the same point on all three curves is depicted on the nextfigure. The drawing on the left shows airway and alveolar pressure before an inspiration,which are both the same (0) so there is no flow. Pleural pressure is slightly negative to
offset the tendency of alveoli to collapse, keeping the airway open. The top drawingshows the beginning of inspiration. The pleural and alveolar pressures become morenegative so air flows in. The difference between the inside and outside of the airway isnow +6 instead of +5 so that will have a dilating effect on the airway. The right drawingis at the end of inspiration. This is the reversal point so alveolar and airway pressure areequal and there is no flow. The pleural pressure is more negative to hold it at the higher volume, so the transpulmonary pressure has increased from -5 to +10 overall. The
pleural pressure has a huge dilating effect on airways. The bottom is the forcedexpiration. The muscles create a very positive pleural pressure which is transferred toalveoli and contributes to driving pressure for flow. In addition, there is a recoil pressureso alveolar pressure is greater than pleural pressure. As you go down airway, pressuredecreases due to air molecules bumping into each other and the wall. Eventually youreach a point where the pressure inside of the airway is less than outside of the airwayand the airway collapses. At this point, the increase in driving pressure is offset by thecollapsing pressure so you get the same flow irrespective of effort.
Dr. Forster stopped here for today.