who.drug information.pdf

of 52
-
Upload
nauli-panjaitan -
Category
Documents
-
view
230 -
download
0
Transcript of who.drug information.pdf
-
8/13/2019 who.drug information.pdf
1/52
99
WHO Drug Information Vol. 25, No. 2, 2011
WHO Prequalification ofMedicines ProgrammeFacts and figures for 2010 101
Safety and Efficacy IssuesSafety trials for long acting beta-agonists104Rotavirus vaccination: risk of intus-
susception 104Tumour necrosis factor blockers: hepato-
splenic T-cell lymphoma 106Dipeptidyl peptidase-4 inhibitors:
possible glycaemic complications 106Lenalidomide: risk of new malignancies 106Pneumovax 23: injection site reactions 107Dabigatran etexilate mesylate capsules:
storage and handling 107Proton pump inhibitors: low magnesium
levels 108Seasonal influenza vaccines 108Ipilimumab: severe immune-mediated
reactions 108
Fluticasone propionate: risk ofosteonecrosis 109Varenicline: hyperglycaemia in patients
with diabetes 109Quinine sulfate: serious adverse
reactions 110Risk of oral clefts in children born to
mothers taking topiramate 110WHO training course on pharmaco-
vigilance 111
Quality Assurance Issues
WHO Certification Scheme: questionsand answers 113
Regulatory Action and NewsBuflomedil: marketing authorization
suspended 122Dolasetron mesylate intravenous
injection: withdrawal 122
Abiraterone acetate approved forlate-stage prostate cancer 122
Rituximab approved for Wegenergranulomatosis and microscopicpolyangiitis 122
Human normal immuno-globulin: liftingof suspension 123
Everolimus approved for pancreaticcancer 123
Boceprevir approved for hepatitis C 124
Linagliptin approved for type 2 diabetes 124Naproxcinod: withdrawal of marketing
authorization application 124Lumiracoxib: withdrawal of marketing
authorization application 125Erythropoietin: withdrawal of marketing
authorization application 125
ATC/DDD ClassificationATC/DDD Classification (temporary) 126ATC/DDD Classification (final) 128
Recent Publications,Information and EventsSelection and use of medicines 131Policy guidelines on controlled
substances 132List of medicines to save mothers and
children 133World medicines situation 133Artesunate instead of quinine saves lives134
Consultation Documents
The International PharmacopoeiaRevision of monograph on capsules 135Revision of monograph on tablets 139Paediatric retinol oral solution 147
Proposed InternationalNonproprietary Names List 105
WHO Drug Information
World Health Organization
Contents
151
-
8/13/2019 who.drug information.pdf
2/52
100
WHO Drug Information Vol. 25, No. 2, 2011World Health Organization
WHO Drug Information
Digital Library,
e-mail table of contents
and subscriptions
available at:
http://www.who.int/druginformation
-
8/13/2019 who.drug information.pdf
3/52
101
WHO Drug Information Vol. 25, No. 2, 2011
WHO Prequalification of
Medicines Programme
Facts and figures for 2010
Evaluation of medicines by the WHOPrequalification of Medicines Programme(PQP) includes assessment of data andinformation on safety, efficacy and quality.Inspections are performed to assesscompliance with good manufacturingpractices (GMP) and include manufactur-ers of selected active pharmaceuticalingredients (API) and clinical sites.
Clinical sites, including contract researchorganizations (CROs), are also inspectedto verify bio-equivalence with goodlaboratory practices and good clinicalpractices.
Thirty-six products were prequalified in2010, of which 30 were generics. At theend of 2010, the WHO list of prequalifiedmedicines totalled 252 products manufac-tured in 20 countries. WHO prequalifica-tion firsts included artesunate powder
for injection (which was the first prequali-fied sterile product made in China); thefirst combination tenofovir disoproxilfumarate/lamivudine and the first genericemtricitabine.
Six medicines quality control laboratories(QCLs) were also prequalified: one inBolivia, one in Canada, one in Peru, twoin Ukraine and one in Uruguay. At the endof 2010, a total of 17 QCLs had beenprequalified and a further 30 were work-
ing towards becoming prequalified.
Invitations to manufacturers to submit anexpression of interest (EOI) for productevaluation were issued for anti-TB medi-cines, HIV/AIDS-related care and treat-ment products, and reproductive healthproducts. The new invitations incorporateadditional products and/or take intoaccount revisions made to WHO treat-
ment guidelines. Additionally, the firstinvitation to manufacturers of activepharmaceutical ingredients (APIs) wasissued in October 2010, marking thelaunch of WHO prequalification of APIs.(A second, expanded invitation to APImanufacturers to submit an EOI wasissued in March 2011.) It is expected thattime taken to reach prequalification will beshorter for finished pharmaceuticalproducts (FPPs) that are manufactured
using WHO-prequalified APIs, than forFPPs that are manufactured using APIsthat have not previously been evaluatedby WHO PQP.
Assessment activitiesIn 2010, 51 dossiers were submitted and53 dossiers (two of which were receivedin late 2009) were accepted for evalua-tion. Nearly 1000 assessment reportswere produced. PQP also assessednearly 600 variations submitted by
manufacturers of prequalified products.
The assessment sessions held in Copen-hagen, Denmark, include a trainingcomponent which is enabling a growingnumber of developing country assessorsto acquire stringent regulatory expertise.The Copenhagen sessions also incorpo-rate technical consultations so thatapplicants can discuss technical issuesrelating to their dossiers with assessors.
The consultations benefit from the pres-ence of a range of assessors with consid-erable assessment experience.
A new collaborative procedure for facilitat-ing registration of prequalified medicinesin the East African Community (EAC) waspiloted. The overall aim was to identify aframework, for WHO-EAC, for jointevaluation and approval of dossiers and
-
8/13/2019 who.drug information.pdf
4/52
102
WHO Drug Information Vol. 25, No. 2, 2011WHO Prequalification of Medicines Programme
inspections of medicine manufacturingsites, and to ensure that these assess-ments are integrated into national regula-tory decision-making. Two assessorseach from three EAC countries (Kenya,Tanzania and Uganda) and six WHOassessors jointly assessed two productdossiers submitted by a single manufac-turer. The dossiers were submitted inparallel, and with identical content, toeach participating EAC country and toPQP. The products were both prequali-fied: HA488 (abacavir, dispersible tablets60 mg) in August 2010 and TB217(amikacin, injection 500 mg/2 ml) inJanuary 2011. For the manufacturer, theprincipal benefit of this joint assessment
was that once the products had beenjointly assessed and approved by WHO-EAC, they were granted immediateaccess to the markets of each of thecountries that had participated in the jointassessment. For the regulators involved,such joint assessment contributes toharmonization of regulatory requirementsat regional level. PQP is hoping to usethe same model for assessing selected,technically complex, high-priority prod-ucts. Several partners and stakeholderssee joint assessment as an effectivemeans of speeding up access to muchneeded products.
InspectionsPQP inspectors carried out 59 inspec-tions in 18 countries: 38 of finishedpharmaceutical product manufacturingsites; five of API manufacturing sites;seven of CROs and nine of pharmaceuti-cal QCLs. (Inspections were carried out
mostly in India and in China, but also inAlgeria, Belgium, Bolivia, Egypt, France,Iran, Kenya, Morocco, the Netherlands,Peru, Russia, South Africa, Tanzania,Uganda, Uruguay, the United States andZimbabwe.)
A new collaborative procedure for jointinspections was initiated at the beginningof 2010. A secure web site has beenestablished for the sharing of inspection
plans, arranging of joint inspections, andsharing of information and inspectionreports, with recognition by participatingEAC parties and PQP. This will be furtherexplored and possibly expanded. Jointinspections are planned for 2011 in anattempt to prevent duplication of inspec-tions. Inspection reports will be shared bythe parties following the inspection. It ishoped that the outcome of the inspectionwill be accepted by all participatinginspectorates. PQP continues to invitelocal medicines regulatory authority staffor observers to participate in inspections.
The risk assessment procedure foridentifying which API manufacturing sitesshould be inspected has been completedfor substances used to manufactureproducts for the treatment of malaria andTB. It is planned to expand this riskassessment to APIs used in products forthe treatment of HIV/AIDS.
Advice and assistancePQP continues to respond to manufactur-ers request for assistance concerningissues relating to, for example, bioequiva-lence study protocols and choice of
comparator products.
PQP continues to provide technicalassistance to manufacturers and nationalQCLs that aims at resolving specificpractical problems related to GMP, goodpractices for QCLs and/or meetingmedicines regulatory requirements.Assistance is given in the form of anaudit, advice on development of animprovement plan, and training in techni-cal or regulatory areas. Follow-up mis-sions are also organized to supportimplementation of improvement plans. In2010, PQP organized 22 technical assist-ance missions to pharmaceutical manu-facturers in four countries (Argentina,China, India and Indonesia) and 10technical assistance missions to nationalQCLs (in Argentina, Brazil, Burkina Faso,China, Egypt, Jamaica, Panama, Peruand Yemen).
-
8/13/2019 who.drug information.pdf
5/52
103
WHO Drug Information Vol. 25, No. 2, 2011 WHO Prequalification of Medicines Programme
Training and hands-on practice remaincrucial to capacity building. PQP organ-ized, co-organized or supported 23training courses. Training on general orspecific technical issues was given tomanufacturers, and to MRA and QCLstaff, as well as an introduction and/orupdate on PQP requirements and serv-ices. Training included group sessions aswell as discussion sessions with mem-bers of assessment or inspection teamsworking with PQP. In 2010, these work-shops involved more than 1200 partici-pants representing regulatory authorities,pharmaceutical manufacturers and QCLstaff.
Testing of medicines qualityWhen implementing sampling and testingprojects PQP evaluates specifically thequality of WHO-prequalified products. Ina study of the quality of antimalarials,concluded in 2010, the quality of WHO-prequalified products far exceeded that ofnon-WHO-prequalified products. (Lessthan 4% of WHO-prequalified artemether-lumefantrine and artesunate-amodiaquinesamples failed to comply with interna-tional quality standards, whereas thefailure rate reached 60% for non-WHO-prequalified samples of the same compo-sition.) Similarly, a survey of the quality ofanti-TB medicines conducted in 2009/2010 in Armenia, Azerbaijan, Belarus,Kazakhstan, Ukraine and Uzbekistanshowed that all prequalified productssampled and containing isoniazid/ri-fampicin complied with internationalquality standards.
Norms and standards underpinning orrelevant to WHO prequalificationactivitiesThe Forty-fifth meeting of the WHOExpert Committee on Specifications forPharmaceutical Preparations adoptedfive monographs for HIV and relatedconditions, four monographs for antima-larial medicines, six monographs for
antituberculosis medicines, two mono-graphs for influenza-specific antiviralmedicines and one for a reproductivehealth product. The Committee alsoadopted a number of new or revisedguidelines and procedures of directrelevance to PQPs activities.
Improving PQP servicesThe results of a survey of manufacturersprovided further information for develop-ing greater client focus. Based on thesurvey results, PQP staff worked onimprovements to the Programme, someof which have already been implemented.For example, raising awareness of theopportunity for manufacturers to meet
and consult with PQP assessors, clarify-ing procedure for resolving disagree-ments surrounding questions raisedduring the assessment of product dossi-ers and some of which (e.g., reducingthe time taken to review and reply toapplicants during the dossier assessmentprocess, providing the same assessorsthroughout the assessment process for aproduct dossier) depend upon completionof other activities (e.g., finalization ofPQPs new information managementsystem). Others for example, theperceived greater stringency of WHOGMP requirements will require furtherdiscussion with manufacturers.
Benefits to manufacturersIn 2010, PQP initiated a study to help itdescribe and quantify the potentialbenefits to manufacturers of having aproduct or products prequalified by WHO.PQP will use the results to develop a
business case for participation in WHOmedicines prequalification for presenta-tion to manufacturers.
Further information on the WHO Prequali-fication of Medicines Programme, includ-ing the full list of medicines prequalifiedby WHO can be found at: http://www.who.int/prequal.
-
8/13/2019 who.drug information.pdf
6/52
104
WHO Drug Information Vol. 25, No. 2, 2011
Safety and Efficacy Issues
Safety trials for long actingbeta-agonists
United States of America To furtherevaluate the safety of long acting beta-agonists (LABAs) when used in combina-tion with inhaled corticosteroids for thetreatment of asthma, the Food and DrugAdministration (FDA) is requiring manu-facturers to conduct five randomized,double-blind, controlled clinical trials
comparing the addition of LABAs toinhaled corticosteroids versus inhaledcorticosteroids alone.
Four clinical trials will be conducted inadult and adolescent patients 12 yearsof age and older to evaluate:
Budesonide and formoterol.
Fluticasone and salmeterol.
Mometasone and formoterol. Formoterol.
One clinical trial will be conducted inpaediatric patients aged 4 to 11 years andwill include 6200 patients. Patients in alltrials will be treated for six months, andthe primary endpoint will be a compositeof serious asthma outcomes: asthma-related death, intubation, or hospitaliza-tion. The paediatric trial will also assess
other relevant quality of life endpointssuch as days of school missed andemergency room visits because ofasthma related illness.
The clinical trials will begin in 2011 andFDA expects to receive results in 2017.
Reference: FDA Drug Safety Communication,15 April 2011 at http://www.fda.gov/Drugs/DrugSafety
Rotavirus vaccination: riskof intussusception
Australia The Therapeutic GoodsAdministration (TGA) has undertaken aninvestigation of a possible associationbetween the use of the rotavirus vaccinesRotarix and RotaTeq and the occur-rence of a rare form of bowel obstructionknown as intussusception (IS). This is acondition caused by the telescoping of
one segment of the bowel into another. Itis estimated to occur each year in around80 per 100 000 children under 12 monthsof age, which represents approximately200 cases per year in Australia. The peakincidence is in infants 510 months ofage, with 80% of cases occurring before24 months of age. It is much more com-mon in males than females.
IS was found to be a side effect of thefirst generation rotavirus vaccine,
RotaShield, that was available in theUnited States in 19981999 and wasestimated to cause IS in 1020 of every100 000 doses given to infants. It wasvoluntarily withdrawn from the US marketin October 1999 (1, 2).
RotaShield was not used outside theUSA, however, as the historical incidenceof IS is 2.5 to 3 times higher in infants inAustralia than in the US, this would have
translated to 2560 cases of IS for every100 000 doses of RotaShield.
Subsequently, two new rotavirus vac-cines, Rotarix and RotaTeq weredeveloped and both were tested in largestudies designed to explore whether therewas a risk of IS (3, 4). In Australia, twopost-marketing studies have been con-ducted to investigate whether the new
-
8/13/2019 who.drug information.pdf
7/52
105
WHO Drug Information Vol. 25, No. 2, 2011 Safety and Efficacy Issues
rotavirus vaccines are associated with anincreased risk of IS. The first study wasconducted using two surveillance sys-tems, the Paediatric Enhanced DiseaseSurveillance (PAEDS) and the AustralianPaediatric Surveillance Unit (APSU). Thisstudy found an apparent four-fold in-creased risk of IS in babies within oneweek of being given the first dose ofeither vaccine, compared with historicaldata on hospitalizations coded as IS, butno overall increase in overall rates of ISup to the age of nine months.
Following this, a large self-controlled caseseries (SCCS) study using data on allhospitalized cases coded as IS was
commissioned by the TGA. This studyfound a statistically significant four-foldincrease in the occurrence of IS in thefirst 17 days following the first dose ofeither Rotarix or RotaTeq comparedwith other time periods after vaccinereceipt. This increase in risk translates toapproximately two additional cases of ISoccurring in every 100 000 first doses ofvaccine administered, or six additionalcases each year in children under 12months of age in Australia.
The World Health Organization (WHO)and the Australian Technical AdvisoryGroup on Immunization (ATAGI) haverecommended the continued use ofrotavirus vaccine for infants.
References
1. Withdrawal of Rotavirus Vaccine Recom-mendation. MMWR 1999;48(3):1107.
2. Murphy T, Gargiullo P, Massoudi M, NelsonD et al. Intussusception among infants givenan oral rotavirus vaccine. New EnglandJournal of Medicine 2001; 344(8):56472
3. Ruiz-Palacios G, P rez-Schael I, VelazqueaF, H HA, Breuer T et al. Safety and efficacy ofan attenuated vaccine against severe rotavi-rus gastroenteritis. New England Journal ofMedicine 2006;354(1):1122.
4. Vesikari T, Matson D, Dennehy P, DammePV et al. Safety and efficacy of a pentavalenthuman-bovine (WC3) reassortant rotavirusvaccine. New England Journal of Medicine2006;354(1):2333.
5. Macartney KK, Porwal M, Dalton D, CrippsT et al. Decline in rotavirus hospitalisationsfollowing introduction of Australias nationalrotavirus immunisation programme. J PaediatrChild Health 2011; published online: 18 Jan2011 DOI: 10.1111/j.1440-1754.2010.01953.
6. Lambert SB, Faux CE, Hall L, Birrell FA etal. Early evidence for direct and indirect ef-fects of the infant rotavirus vaccine program inQueensland. Med J Aust 2009; 191: 157160.
7. Haber P, Patel M, Izurieta H, Baggs J et al.Postlicensure monitoring of intussusception
after RotaTeq vaccination in the UnitedStates, February 1, 2006, to September 25,2007. Pediatrics 2008;121(6):120612.
8. Velazquez FR, Colindres R, Grajales C,Hernandez MT, Mercadillo MG, Torres FJ,Yolanda M Apolinar C, DeAntonio-Suarez R,Ortega E, Blum M, Breuer T, Verstraeten T.Postmarketing surveillance of intussusceptionfollowing mass introduction of the humanrotavirus vaccine in Mexico: an interimanalysis. Excellence in Paediatrics, London,December 24, 2010
9. World Health Organization, Global AdvisoryCommittee on Vaccine Safety. Statement onRotarix and Rotateq vaccines and intus-susception. 22 September 2010.
10. Buttery JP, Danchin MH, Lee KJ, CarlinJB, McIntyre PB, Elliott EJ, Booy R, Bines JEfor the PAEDS/APSU Study Group. Intussus-ception following rotavirus vaccine administra-tion: post marketing surveillance in theNational Immunization Program in Australia.Vaccine, 2011. In Press.
11. Tapiainen T, Bonhoeffer J, Heininger U.Evaluation of the Brighton Collaboration casedefinition of acute intussusception during ac-tive surveillance. Vaccine 2006;24(9):14837.
12. Galati JC, Harsley S, Richmond P, CarlinJB. The burden of rotavirus-related illnessamong young children on the Australian healthcare system. ANZ Journal of Public Health2006;30:416-421.
-
8/13/2019 who.drug information.pdf
8/52
106
WHO Drug Information Vol. 25, No. 2, 2011Safety and Efficacy Issues
Tumour necrosis factorblockers: hepatosplenicT-cell lymphoma
United States of America The Food
and Drug Administration (FDA) continuesto receive reports of hepatosplenic T-Celllymphoma (HSTCL), primarily in adoles-cents and young adults being treated forCrohn disease and ulcerative colitis withmedicines known as tumour necrosisfactor (TNF) blockers, as well as withazathioprine, and/or mercaptopurine.Crohn disease and ulcerative colitiscause inflammation of the digestivesystem. Common symptoms are pain inthe abdomen, cramps, and diarrhoea.
Bleeding from the rectum, weight loss,joint pain, skin problems and fever alsomay occur. Children with the disease mayhave growth problems, develop intestinalblockage and experience malnutrition.
FDA believes the risks and benefits ofusing TNF blockers, azathioprine, and/ormercaptopurine should be carefullyweighed when prescribing these drugs tochildren and young adults, especially forthe treatment of Crohn disease andulcerative colitis.
The product labels for infliximab(Remicade) and adalimumab (Humira)have been updated and the productlabels for azathioprine and mercaptopu-rine are being updated to include warn-ings about HSTCL that have been re-ported in patients treated with theseproducts.
Reference: FDA Drug Safety Communication,14 April 2011 at http://www.fda.gov/Drugs/DrugSafety
Dipeptidyl peptidase-4inhibitors: possible glycaemiccomplications
Japan The Ministry of Health, Labourand Welfare (MHLW) has warned about
the risk of hypoglycaemia associatedwith concomitant use of dipeptidyl pepti-dase-4 (DPP-4) inhibitors and sulfony-lureas, and the risk of diabetic keto-acidosis and hyperglycaemia afterswitching from insulin to glucagon-likepeptide-1 (GLP-1) receptor agonists.
DPP-4 inhibitors and GLP-1 receptoragonists are antidiabetic drugs whichinactivate incretin. Incretin is a gastroin-testinal hormone which stimulatesinsulin secretion. DPP-4 inhibitors areused to treat type 2 diabetes mellitus byincreasing the endogenous active incretinlevel and thereby controlling bloodglucose. As of December 2010, sitagliptin
phosphate hydrate, vildagliptin, andalogliptin benzoate have been approvedin Japan.
GLP-1 receptor agonists are used to treattype 2 diabetes mellitus by binding to theGLP-1 receptor to promote insulin secre-tion in response to the increase in bloodglucose. As of December 2010, liraglutide(genetic recombination) and exenatidehave been approved.
Reference: Pharmaceuticals and MedicalDevices Safety Information, No.275. Decem-ber 2010 at http://www.pmda.go.jp/english
Lenalidomide: risk ofnew malignancies
United States of America The Foodand Drug Administration (FDA) hasprovided information on clinical trials thatfound that patients treated with lenalido-mide (Revlimid) may be at increasedrisk of developing new types of cancercompared to patients who did not take thedrug.
FDA is currently reviewing all availableinformation on this potential risk andrecommends that patients continuelenalidomide treatment as prescribed bytheir physician. The benefits and the risks
-
8/13/2019 who.drug information.pdf
9/52
107
WHO Drug Information Vol. 25, No. 2, 2011 Safety and Efficacy Issues
should be carefully weighed when pre-scribing this drug. Lenalidomide is usedto treat myelodysplastic syndrome and isused along with other drugs to treatpeople with multiple myeloma.
Preliminary data derived from evaluationof outcomes after longer-term exposureto lenalidomide and from controlledclinical trials conducted inside and out-side the Unites States shows an in-creased incidence of some secondprimary malignancies, particularly acutemyelogenous leukemia (AMaL) and B-celllymphoma malignancies when comparedto controls. Since lenalidomide is ananalogue of thalidomide, FDA is alsocurrently reviewing all available informa-tion on this potential risk for thalidomide.
Reference: FDA Drug Safety Communication,8 April 2011 at http://www.fda.gov/Drugs/DrugSafety
Pneumovax 23:injection site reactions
Australia The Therapeutic GoodsAdministration (TGA) is advising healthprofessionals not to administer a secondor subsequent dose of Pneumovax 23vaccine pending the outcome of a reviewof an apparent increased rate of injectionsite reactions following administration ofthe second dose.
Pneumovax 23 vaccination is used toprevent life threatening bacterial infec-tions for anyone who is at high risk ofpneumococcal infections.
Pneumovax 23 vaccine is known to be
associated with a high rate of localinjection site reactions which can includesevere injection site reactions such ascellulitis and abscess. There is varyingevidence from published trials as towhether injection site reactions are morecommon following revaccination.
The Australian Technical Advisory Groupon Immunization (ATAGI) is currently
reviewing the place of Pneumovax 23in the National Immunization Programme.This alert is not applicable to use of the7-valent pneumococcal conjugate vaccinePrevenar or the 10-valent pneumococ-cal conjugate vaccine, Synflorix, whichare given to babies.
Reference:Therapeutic Goods AdministrationSafety Alert. 18 April 2011. http://www.tga.gov.au/safety/alerts-medicine-pneumovax-110416.htm
Dabigatran etexilate mesylatecapsules: storage and handling
United States of America The Food
and Drug Administration (FDA) is alertingthe public to important storage andhandling requirements for dabigatranetexilate mesylate (Pradaxa) capsules.Due to the potential for product break-down from moisture and loss of potency,Pradaxa capsules should only bedispensed and stored in the original bottleor blister package. However, manyconsumers use pill boxes or pill organiz-ers to aid them in remembering to taketheir medications.
Although the current Pradaxa labelstates that the product should be dis-carded 30 days after the original bottle isopened, data currently under review bythe FDA indicate that the product main-tains its potency up to 60 days after bottleopening as long as it is stored in theoriginal bottle and the handling require-ments are met including that the cap isclosed tightly after use and the bottle is
kept away from excessive moisture, heatand cold. Pradaxa capsules will hydro-lyse over time when exposed to humidity,causing a breakdown of active ingredientand rendering the medication less effec-tive.
Reference: FDA Drug Safety Communication,29 March 2011 at http://www.fda.gov/Drugs/DrugSafety
-
8/13/2019 who.drug information.pdf
10/52
108
WHO Drug Information Vol. 25, No. 2, 2011Safety and Efficacy Issues
Proton pump inhibitors:low magnesium levels
United States of America The Foodand Drug Administration (FDA) is inform-ing the public that prescription protonpump inhibitor (PPI) drugs may causehypomagnesaemia if taken for prolongedperiods of time (in most cases, longerthan one year). In approximately one-quarter of the cases reviewed, magne-sium supplementation alone did notimprove low serum magnesium levelsand the PPI had to be discontinued.PPIs are used to treat gastroesophagealreflux disease (GERD), stomach andsmall intestine ulcers, and inflammation of
the esophagus.
Prescription PPIs include esomeprazolemagnesium, dexlansoprazole, ome-prazole, lansoprazole, pantoprazolesodium, and abeprazole sodium.
Reference: FDA Drug Safety Communication,2 March 2011 at http://www.fda.gov/Drugs/DrugSafety
Seasonal influenza vaccines
Australia During the 2010 influenzaseason, an excess number of cases offebrile reactions and febrile convulsionswere observed in paediatric populationsfollowing immunization with one of theregistered seasonal trivalent influenzavaccines. Consequently, the TherapeuticGoods Administration (TGA) has imposeda condition on the registration of all 2011seasonal influenza vaccines with apaediatric indication which were not
supplied in Australia in 2010. Sponsorsare required to undertake active surveil-lance of children from six months to nineyears of age to ensure effective monitor-ing of paediatric populations in Australiapreviously unexposed to these vaccines.Two sponsors were unable to meet thiscondition of registration. Although thesafety of Agrippal and Fluarix hasbeen demonstrated in the northern
hemisphere 2010/2011 influenza season,the TGA does not have any safety dataon the use of these vaccines in Australianchildren. Hence, the TGA recommendsthat these vaccines are not used in anychild under the age of nine years.
For children under the age of nine years itis recommended that they be vaccinatedwith either Influvac or Vaxigrip. Thesetwo vaccines were not associated withincreased rates of fever or febrile reac-tions in 2010.
Reference:Therapeutic Goods AdministrationSafety Advisory, 11 March 2011. http://www.tga.gov.au/safety
Ipilimumab: severe immune-mediated reactions
United States of America The Foodand Drug Administration (FDA) hasposted information from the manufacturerof Ipilimumab (Yervoy) about the riskevaluation and mitigation strategy(REMS) developed to ensure that thebenefits of ipilimumab outweigh the risksof severe and fatal immune-mediatedadverse reactions.
Ipilimumab was approved in March 2011with a boxed warning stating that use ofthe product can result in severe and fatalimmune-mediated adverse reactions dueto T-cell activation and proliferation.These immune-mediated reactions mayinvolve any organ system. However, themost common severe immune-mediatedadverse reactions are enterocolitis,hepatitis, dermatitis (including toxic
epidermal necrolysis), neuropathy, andendocrinopathy. The majority of theseimmune-mediated reactions initiallymanifested during treatment. However, aminority occurred weeks to months afterdiscontinuation.
Reference: FDA Medwatch Communication,Dear Healthcare Professional Letter, 6 April2011 at http://www.fda.gov/Drugs/DrugSafety
-
8/13/2019 who.drug information.pdf
11/52
109
WHO Drug Information Vol. 25, No. 2, 2011 Safety and Efficacy Issues
Fluticasone propionate:risk of osteonecrosis
Canada Health Canada has receivedfive reports of osteonecrosis suspected
of being associated with fluticasonepropionate.
The potential for osteonecrosis with highdoses of inhaled corticosteroids has beensuggested in the literature. Becausecorticosteroid-induced osteonecrosistends to occur in younger patients andtreatment options for advanced diseaseare limited, early identification is impor-tant.
Fluticasone propionate is a highly potentglucocorticoid anti-inflammatory steroid.In Canada, it is available as an aqueousnasal spray, an inhalation aerosol, apowder for inhalation and a topical cream(13). Steroid-induced osteonecrosis, oravascular necrosis, is characterized bybone cell death resulting from compro-mized blood supply. Corticosteroids,administered orally or parenterally, havebeen associated with osteonecrosis (4).Osteonecrosis related to inhaled or
topical use of steroids has also beenreported but the oral or parenteral use ofsteroids was a confounding factor (4).The potential for osteonecrosis with highdoses of inhaled corticosteroids, such asin the treatment of severe persistentasthma or eosinophilic oesophagitis, hasbeen suggested (4).
Systemic adverse reactions may occurwith intranasal and inhaled use of corti-costeroids (1, 2). The long-term effects offluticasone propionate are still unknown.The relative determinants of systemicadverse reactions to inhaled and intrana-sal corticosteroids have been assessedand fluticasone propionate was deter-mined to have a high systemic potency(5). Because corticosteroid-inducedosteonecrosis tends to occur in youngerpatients (the average age at onset is 33)and treatment options for advanced
disease are limited, early identification isimportant (4).
Extracted from the Canadian AdverseReaction Newsletter, Volume 21(2), April2011 at http://www.healthcanada.gc.ca
References
1. Flovent HFA, Flovent Diskus (fluticasonepropionate) [product monograph]. Mississauga(ON): GlaxoSmithKline Inc.; 2010.
2. Flonase (fluticasone propionate) [productmonograph]. Mississauga (ON):GlaxoSmithKline Inc.; 2004.
3. Advair Diskus (salmeterol xinafoate/
fluticasone propionate) [product monograph].Mississauga (ON): GlaxoSmithKline Inc.;2008.
4. Powell C, Chang C, Naguwa S, et al.Steroid induced osteonecrosis: an analysis ofsteroid dosing risk. Autoimmun Rev2010;9(11):72143.
5. Lipworth BJ, Jackson CM. Safety ofinhaled and intranasal corticosteroids. DrugSaf 2000;23(1):1133.
Varenicline: hyperglycaemiain patients with diabetes
Canada Health Canada has received18 reports of hyperglycaemia suspectedof being associated with varenicline(Champix) in patients with type 1 andtype 2 diabetes.
Varenicline is indicated for smoking-cessation treatment in adults in conjunc-
tion with smoking-cessation counselling.The current Canadian product mono-graph lists diabetes mellitus and hypogly-caemia under less common clinical trialadverse drug reactions and describesthese adverse reactions (ARs) as infre-quent and rare, respectively.
Diabetes mellitus is a chronic metabolicdisorder characterized by the presence ofhyperglycaemia and consequently is a
-
8/13/2019 who.drug information.pdf
12/52
110
WHO Drug Information Vol. 25, No. 2, 2011Safety and Efficacy Issues
confounder. Other confounders identifiedin some of the reports included infection,medications (e.g., insulin, oral antidiabeticagents, diuretics), alcohol consumptionand smoking cessation. In some in-
stances, the patient was still smokingwhile taking varenicline.
Extracted from the Canadian AdverseReaction Newsletter, Volume 21(2), April2011 at http://www.healthcanada.gc.ca
References
1. Champix (varenicline) [product mono-graph]. Kirkland (QC): Pfizer Canada Inc;2010.
2. Kristensen PL, Pedersen-Bjergaard U,Thorsteinsson B. Varenicline may triggersevere hypoglycaemia in type 1 diabetes.Diabet Med 2008;25(5):625-6.
Quinine sulfate: seriousadverse reactions
Canada Quinine sulfate, in combina-tion with a second antimalarial drug, isrecommended for the treatment of un-complicated Plasmodium falciparummalaria. Quinine sulfate is not indicated inCanada for the prevention or treatment ofnocturnal leg cramps. However, quininesulfate is used for the prevention andtreatment of leg cramps, at a dose of 200to 300 mg at bedtime. The use of quininesulfate to prevent leg cramps has been asubject of recent concern. Several inter-national regulators have taken action toeither withdraw this indication for use orhave added conditions for its use for leg
cramps.
Adverse reactions to quinine sulfateinclude life-threatening blood-relatedreactions, such as sudden, severethrombocytopenia.
Extracted from the Canadian AdverseReaction Newsletter, Volume 21(2), April2011 at http://www.healthcanada.gc.ca
References
1. CATMAT. Canadian recommendations forthe prevention and treatment of malariaamong international travellers 2009. CanCommun Dis Rep 2009;35(Suppl 1):182.
2. Quinine sulfate [Canadian PharmacistsAssociation monograph]. In: e-CPS. Ottawa(ON): Canadian Pharmacists Association;2010.
3. Adverse Drug Reactions Advisory Commit-tee (ADRAC) Quinine indications crampsdeleted. Aust Adv Drug Reactions Bull2004;23(5):20.
4. Medsafe. Quinine not for leg crampsanymore. Prescriber Update 2007;28(1):23.
5. US Food and Drug Administration. Quininesulfate (marketed as Qualaquin): off-label(not approved by FDA) use of quinine. FDADrug Safety Newsletter 2009;2(2):113.
6. Medicines and Healthcare products Regula-tory Agency. Quinine: not to be used routinelyfor nocturnal leg cramps. Drug Safety Update2010;3(11):34.
7. US Food and Drug Administration. FDA
Drug Safety Communication: New riskmanagement plan and patient MedicationGuide for Qualaquin (quinine sulfate). 7August 2010.
8. Aster RH, Bougie DW. Drug-inducedimmune thrombocytopenia. N Engl J Med2007;357(6):5807.
9. Brinker AD, Beitz J. Spontaneous reports ofthrombocytopenia in association with quinine:clinical attributes and timing related to regula-tory action. Am J Hematol 2002;70(4):3137.
Risk of oral clefts in childrenborn to mothers takingtopiramate
United States of America The Foodand Drug Administration (FDA) is inform-ing the public of new data that show thatthere is an increased risk for the develop-
-
8/13/2019 who.drug information.pdf
13/52
111
WHO Drug Information Vol. 25, No. 2, 2011 Safety and Efficacy Issues
ment of oral clefts in infants of womentreated with topiramate (Topamax andgeneric products) during pregnancy.
Topiramate is an anticonvulsant used to
treat epilepsy. It is approved for use toprevent migraine headaches. Topiramateis being placed in Pregnancy Category Dindicating positive evidence of humanfetal risk but with potential benefits thatmay be acceptable in certain situationsdespite its risks.
Reference: FDA Drug Safety Communication,4 March 2011 at http://www.fda.gov/Drugs/DrugSafety
WHO training course onpharmacovigilance
A recent survey by the WHO Programmefor International Drug Monitoring identi-fied serious gaps in technical capacity forpharmacovigilance (PV) in resourcelimited settings. The Inter-regionalPharmacovigilance Training Course, heldin February 2011 in New Delhi, India, waspart of the WHO strategy to help establishminimum standards for PV as identified
by WHO and the Global Fund during aconsensus meeting in 2010.
The course identified leveraging oppor-tunities offered by liaison and sharingresources with lymphatic filariasis publichealth programmes. By introducing PVwithin mass preventive treatment cam-paigns, the quality of care and patientsafety within such programmes could besignificantly improved.
The specific objectives of the trainingcourse were to:
Raise awareness about public healthissues and patient safety in relation tothe use of medicines.
Demonstrate the importance of PVactivities in improving patient safety andtreatment outcomes.
Provide training on the latest tools inbasic adverse drug reaction (ADR)reporting, to enhance reporting withincountries and to the WHO Programmefor International Drug Monitoring.
Build or reinforce capacity of nationalPV centres.
Share experiences and challengesfaced in establishing or strengtheningPV programmes.
Establish networking among regulatoryagencies, PV centres, national ne-glected tropical diseases (NTD) controlprogrammes and WHO for information
sharing and providing assistance indetecting signals and making judgmentsbased on sound science.
Two participants per country attendedfrom Cambodia, Lao PDR, Maldives,Nepal and Viet Nam, with six participantsfrom India. Others represented thenational PV centre or the NTD controlprogramme.
The five-day course covered the followingtopics:
WHO Programme for International DrugMonitoring.
Establishing a PV centre; how to pro-mote reporting.
Vigibase (a WHO global database ofindividual case reports), VigiFlow (aweb-based case report managementsystem), WHO Adverse Reaction
Terminology and WHO Drug Dictionary.
Causality assessment.
Collaboration with public health pro-grammes and NTD control programmesin particular.
Risk management and the prevention ofADRs.
-
8/13/2019 who.drug information.pdf
14/52
112
WHO Drug Information Vol. 25, No. 2, 2011Safety and Efficacy Issues
Spontaneous monitoring systems are useful in detecting signals of relatively rare, serious orunexpected adverse drug reactions. A signal is defined as reported information on a possiblecausal relationship between an adverse event and a drug, the relationship being unknown orincompletely documented previously. Usually, more than a single report is required to gener-ate a signal, depending upon the seriousness of the event and the quality of the information.All signals must be validated before any regulatory decision can be made.
Rational use of medicines.
Communication in pharmacovigilance.
Development of country-specific action
plans for next year.
At the end of the course participantspresented draft plans of priority activitiesfor the next ten months for PV in theirsettings, with key deliverables, timelinesand expected outcomes.
Countries that are not yet members of theWHO Programme (Lao PDR, Maldives)described their plans to establish a PVcentre and join the Programme in the
future. Participants from Cambodia, anassociate member of the WHO Pro-
gramme, expressed their intention tobecome a full member by sending arequired number of ADR reports to theWHO Programme. Three countries thatare members of the WHO Programme
India, Nepal, and Viet Nam presentedplans to strengthen or expand theircurrent PV work by holding workshops onPV for stakeholders, improving collabora-tion between PV and public health pro-grammes and other actions. Participantsfrom Nepal and Viet Nam confirmed thatthe course was useful in establishingcollaboration for the first time between thenational PV and the NTD control pro-grammes.
Reference:World Health Organization.Pharmaceutical Newsletter, April 2011 athttp://www.who.int/medicines
-
8/13/2019 who.drug information.pdf
15/52
113
WHO Drug Information Vol. 25, No. 2, 2011
WHO Certification Scheme:questions and answers
Q1 What is the WHO CertificationScheme on the Quality of PharmaceuticalProducts Moving in International Com-merce?
A1 It is a Scheme developed by theWorld Health Organization (WHO) inresponse to the request of WHO MemberStates to facilitate international trade inpharmaceutical products between Mem-ber States.
Q2 When was the Scheme developed?
A2 It was first developed in 1975. Sincethen it has been revised in 1988, 1992and in 1997.
Q3 How can it facilitate trade in pharma-ceutical products?
A3 The Scheme is an administrativeinstrument that requires a participatingMember State (a certifying country), uponapplication by a commercially interestedparty (the applicant company), to certify/attest to the competent authority ofanother participating Member State (the
recipient country) that:
A specific pharmaceutical product isauthorized for marketing in the certifyingcountry, or if not, the reason why au-thorization has not been accorded.
The manufacturing facilities and opera-tions conform to good manufacturingpractices (GMP) as recommended byWHO.
The WHO Certification Scheme on the Quality of Pharmaceutical Products Movingin International Commerce is an international voluntary agreement mechanism whichprovides information to participating countries on the quality status of finished phar-maceutical products moving in international commerce. The primary focus of theScheme is the Certificate of a Pharmaceutical Product (CPP).
The WHO Expert Committee on Specifications for Pharmaceutical Preparations(ECSPP) recommended that the WHO Certification Scheme on the Quality of Phar-
maceutical Products Moving in International Commerce should be reviewed in linewith changing practices and rapid globalization of the pharmaceutical manufacturingsector, regulatory environment and procurement systems. However, the Schemecan only be opened for revision by decision of the World Health Assembly (1). As aninterim measure, the ECSPP requested that a question and answer document onthe functions of the Scheme should be prepared (2). Version one of the documenthas been developed with the aim of improving understanding of the objectives of theScheme and its implications for quality improvement and provision of effective, safemedicines by participating countries. Comments and suggestions on this documentmay be sent to Dr Samvel Azatyan, Medicines Regulatory Support Programme, WorldHealth Organization, 1211 Geneva 27, Switzerland, or e-mail: [email protected].
Quality Assurance Issues
WHO Certification Scheme
-
8/13/2019 who.drug information.pdf
16/52
114
WHO Drug Information Vol. 25, No. 2, 2011
Q4 Why is it called the WHO CertificationScheme?
A4 It is called the WHO CertificationScheme because it was developed byWHO in response to the request ofMember States.
Q5 How does the Scheme operate?
A5 The Scheme operates as follows:The certificate recipient authority has inits national medicine legislation or guide-lines a requirement for the submission ofa Certificate for a Pharmaceutical Product(CPP) for products being imported intothe country as a support to ensure thequality of the product being imported. (Insome countries the CPP forms part of thedossiers to be submitted to the medicinesregulatory authority (MRA) to have aproduct registered by the authority).
The applicant/importing company re-quests a CPP from the certifying authoritythrough the exporting company.
The certifying authority issues a CPP tothe importing/applicant company via the
exporting company. At the time of thedevelopment of the Scheme the under-standing was that a CPP would be sentdirectly to the recipient authority by theissuing authority.
Q6 Is the Scheme mandatory?
A6 No. The Scheme is not mandatory. Itis a voluntary agreement devised toenable countries with limited regulatorycapacity to obtain partial assurance from
exporting countries concerning thequality, safety and efficacy of the pharma-ceutical product they plan to import.
Q7 Can anyone issue a CPP?
A7 No. Only countries and regionalorganizations such as the EuropeanMedicines Agency (EMA) that are party tothe Scheme can issue a CPP.
Q8 How can a WHO Member State orregional organization be eligible for
participation in the Scheme?
A8 Any WHO Member State or regionalorganization intending to participate in theScheme may do so by notifying theDirector-General of WHO in writing:
Of its willingness to participate in theScheme.
Of any significant reservations it intendsto observe relating to its participation.
By providing the names and address ofits MRA or other competent authority.
Q9 Where can one find the list of organi-zations and countries party to theScheme?
A9 WHO publishes the names andaddresses of Member States party to theScheme. The list is available at http://www.who.int/medicines/areas/quality_safety/regulation_legislation/certification/en/index.html. A hard copy ofthe list is also published and distributed toMember States. The list is regularlyupdated.
Q10 Does the list of Member States andorganizations party to the Scheme
provide the names and addresses ofthose government organizations author-ized to sign and issue a CPP?
A10 Yes. The list provides the namesand full addresses of those government
organizations authorized to sign andissue a CPP. MRAs receiving a CPP canuse this list to check and verify if thecertificate they are receiving has beenissued by the authorized organization.
Q11 Is there any written document thatprovides detailed information on the WHOCertification Scheme?
Quality Assurance Issues
-
8/13/2019 who.drug information.pdf
17/52
115
WHO Drug Information Vol. 25, No. 2, 2011
A11 Yes. Guidelines for implementationof the WHO Certification Scheme on theQuality of Pharmaceutical ProductsMoving in International Commerce areavailable at http://www.who.int/medicines/areas/quality_safety/regulation_legislation/certification/guidelines/en/index.htmlhttp://www.who.int/medicines/areas/quality_safety/regulation_legislation/certification/guidelines/en/index.html.
Q12 What should Member States andregional organizations possess in order toissue a CPP to support the export phar-maceutical products?
A12 In order to issue a CPP, MemberStates and regional organizations shouldhave the following infrastructure andsystems in place:
An effective national licensing systemfor pharmaceutical products, manufac-turers and distributors.
GMP requirements consonant withthose recommended by WHO to whichall manufacturers of finished pharma-ceutical products (FPPs) are required to
conform.
Effective controls to monitor the qualityof pharmaceutical products registeredor manufactured within the country,including access to an independentquality control laboratory.
A national pharmaceutical inspectoratehaving the technical competence,experience and resources to assesswhether GMP and other controls areeffectively implemented and the legalpower to conduct appropriate investiga-tions.
The administrative capacity to issue therequired certificates, to institute inquiriesin the case of a complaint associatedwith a potentially serious quality defector other hazard and to notify WHO andother concerned parties.
Q13 Does WHO issue CPPs?
A13 No. WHO does not issue CPPs orany of the certificates described under theScheme.
Q14 Should a CPP issued by MemberStates bear the WHO emblem or refer tothe WHO acronym?
A14 No. Certificates should not bear theWHO emblem or the acronym. Use of theemblem or acronym creates the impres-sion that the certificate is issued or en-dorsed by WHO. This is an illegal act andcountries receiving such CPPs shouldreject them and report such practices to
WHO.
Q15 What products are covered underthe WHO Certification Scheme?
A15 Pharmaceutical products are cov-ered under the Scheme and include:
FPPs intended for administration tohuman beings.
Pharmaceutical products intended for
administration to food-producing ani-mals.
Active pharmaceutical ingredients(APIs). There is now a separate schemecalled the WHO pharmaceutical startingmaterials certification scheme (SMACS)which has guidelines on importation ofAPIs.
Q16 What are the different types ofCertificate that can be requested withinthe scope of the Scheme?
A16 Three types of certificate can berequested within the scope of theScheme:
A Certificate for a PharmaceuticalProduct (CPP) or Product Certificate(PC);
Quality Assurance Issues
-
8/13/2019 who.drug information.pdf
18/52
116
WHO Drug Information Vol. 25, No. 2, 2011
A Statement of Licensing Status ofPharmaceutical Product(s) (SLSPP);
Batch Certificate of a PharmaceuticalProduct (BCPP).
Q17 By whom and when is a Certificatefor a Pharmaceutical Product (CPP)issued?
A17 A CPP is issued by the competentauthority of the exporting country and isintended for use by the competent author-ity of the importing country:
When a pharmaceutical product isunder consideration for a product
licence/marketing authorization forimportation and sale in the importingcountry.
When administrative action is requiredto renew, extend, vary or review suchlicence.
Q18 When and by whom is a Statementof Licensing Status of PharmaceuticalProduct(s) (SLSPP) issued?
A18 An SLSPP is issued by the compe-tent authority of the exporting country andis intended for use by importing agentswhen considering bids in an internationaltender. It is requested by the importingagent as a condition for bidding.
Q19 What is a Batch Certificate?
A19 A Batch Certificate accompanies andattests to the quality and expiry date of aspecific batch or consignment that hasalready been licensed/approved formarketing in the importing country.
A batch certificate is usually issued by themanufacturer.
In case of biological products, a lotcertificate is issued by the competentauthority of the exporting country.
Q20 Is there a standard format forCPPs?
A20 Yes, there is a standard format. TheWHO standard format was last agreed bythe World Health Assembly in 1997 (1).
The standard WHO format for CPPsfacilitates understanding and review bythe recipient authority. It obliges certifyingauthorities to disclose important informa-tion to the importing country.
Recipient authorities should refrain fromobtaining data other than in the WHOstandard format or in addition to thestandard CPP format.
Certifying authorities should not issue afree-sale certificate. This has beenreplaced by the WHO format CPP.
Q21 Is the CPP evidence of quality,safety, efficacy review and approval?
A21 Yes, the CPP is based on theassumption that the authorities issuing aCPP have the capacity to assess thequality, safety, and efficacy (QSE) of theproduct they have approved for market-
ing.
Based on the intention of the Schemeand when evidence of approval in an-other country is required, a recipientauthority may request a CPP if it isunable to undertake a full review of QSEdata.
Q22 Does the CPP provide evidence ofgood manufacturing practices (GMP)
status?A22 Yes. The GMP declaration in theCPP refers to assurance of GMP for theproduct approved in the certifying countryat the stated manufacturing site.
In addition, certificates from medicinesregulatory authorities (MRAs) party to thePharmaceutical Inspection Cooperation
Quality Assurance Issues
-
8/13/2019 who.drug information.pdf
19/52
117
WHO Drug Information Vol. 25, No. 2, 2011
Scheme (PIC/S) and International Confer-ence on Harmonisation (ICH) (USA,Japan, and EU) provide evidence of GMPstatus.
Q23 What is the difference betweenapproval of the quality data in the submis-sion and evidence of GMP?
A23 Approval of the quality information ina submission is a determination of howthe applicant proposes to manufactureand control the quality of the product atthe time of manufacture and throughoutthe life of the product.
Evidence of GMP compliance confirms
that the applicant company has been ableto demonstrate that the manufacturingfacilities and operations conform to goodmanufacturing practices (GMP) asrecommended by WHO.
Q24 When would a CPP be required?
A24 When the CPP replaces either a fullor partial quality, safety and efficacy(QSE) review. The CPP would be acondition of approval but it would not berequired at the time of submission.
If local legislation stipulates provision of aCPP at the time of submission, theauthority review should comprise averification procedure with published,communicated timelines that should beshort and avoid delaying patient access.
Q25 Are there any alternatives to a CPPas evidence of approval by an MRA?
A25 In addition to the WHO CertificationScheme other forms of evidence include:
Product approval letters (or copies oflicences) from well-established MRAs,e.g., Australia, Canada, China, Den-mark, Finland, Germany, India, Japan,Norway, Republic of Korea, Spain,United Kingdom, United States ofAmerica.
Positive scientific opinion from theEuropean Medicines Agency (EMA).
Decisions of the European Commission.
Licensing/approval information on
regulatory authority web sites.
Evidence of approval on the UnitedStates Food and Drug Administrationweb site.
Q26 Is it necessary for a pharmaceuticalproduct to be exported from the samecountry as the certifying authority?
A26 No. It is not necessary for theproduct to be exported from the certifying
country as long as a declaration of GMPassurance appears on the CPP.
The Scheme was established on thebasis that the certifying country was alsothe country where finished productmanufacture took place and was, there-fore, the exporting country. Subsequentrevisions to the Scheme allow scope forCPPs to be issued by other referenceauthorities. Most certifying authorities
currently provide CPPs when the finishedproduct is not manufactured in the certify-ing country on the basis of GMP assur-ance.
Many authorities assume that certifyingauthorities issue CPPs even whenfinished product manufacture does notoccur in the certifying country. Strictadherence to the above assumptionpotentially limits licensing and registrationoptions and can delay the introduction or
affect the continued supply of neededmedicines.
Q27 Is it possible to obtain a CPP from acertifying authority that is not of thecountry where the manufacture of thefinished product takes place?
A27 Yes. The GMP declaration on theCPP will refer to assurance of GMP for
Quality Assurance Issues
-
8/13/2019 who.drug information.pdf
20/52
118
WHO Drug Information Vol. 25, No. 2, 2011
the product approved in the certifyingcountry at the stated site, even if themanufacturing site is in a different countrythan the issuing authority.
The Scheme has a provision that whenmanufacture takes place in a countryother than that where the product certifi-cate is issued, an attestation that suchmanufacture complies with GMP may stillbe provided as an attachment to theproduct certificate on the basis of inspec-tions undertaken for registration pur-poses.
Q28 Is it necessary for the CPP to comefrom the country where finished product
manufacture takes place?
A28 No. Although the Scheme was setup assuming that the certifying countrywas also the country where finishedproduct manufacture takes place, there isscope within the Scheme for CPPs to beissued by other authorities that canprovide independent assurance of theGMP compliance status.
There needs to be an appreciation of thecomplexity of manufacturing and sourcingroutes currently employed by companiesoperating internationally. WHO MemberStates may define the source differently:
Country of finished product manufac-ture.
Country of final packing.
Country of final release.
Country of headquarters of the pharma-ceutical company, etc.
A critical element is confirmation that allproduction/manufacturing/quality opera-tions are carried out according to GMP.
Due to complex modern sourcing routes,together with varying local regulatory
processes, approval in the country wherefinished product manufacture takes placemay be subsequent to that in othercountries. In this case it is a matter of
judgment whether it is necessary for theCPP to be issued from the country wherefinished product manufacture takes place.Preferred action, in order to speed uppatient access, would be to accept theCPP from the earlier approving country.In order to approve the product thecertifying authority must be assured ofGMP.
GMP implementation and complianceensures product quality. Any requirementfor an additional CPP for the release site,
if it is different from the product manufac-ture site, will delay patient access be-cause multiple CPPs provide no addi-tional value.
Q29 What is the significance of thedeclaration of marketing status (i.e.,whether the product is actually on themarket in the exporting country)?
A29 A declaration of marketing authoriza-tion approval is the aim of the CPP. It istrue that the WHO format CPP includesinformation on marketing status (if theproduct is actually on the market of theexporting country) but the Scheme alsohas a provision whereby the issuingauthority can indicate why the productmay not be marketed. In circumstanceswhere the product is not actually on themarket, the issuing authority can indicatethis on the certificate.
The actual presence on the market of theproduct depends on many other factors.The recipient authority should not requirethat a product be marketed in the certify-ing country.
Q30 Should recipient authorities requirea CPP from more than one certifyingauthority?
Quality Assurance Issues
-
8/13/2019 who.drug information.pdf
21/52
119
WHO Drug Information Vol. 25, No. 2, 2011
A30 No. They should not require a CPPfrom more than one certifying authority. AWHO-format CPP from a single certifyingauthority should provide appropriateevidence of approval and GMP status.
Q31 Is it necessary for recipient authori-ties to require GMP certificates in additionto a CPP?
A31 No. Since the CPP includes a GMPdeclaration, additional GMP certificatesare not necessary.
Following introduction of the WHO CPPsome authorities no longer issue GMPcertificates (e.g., US FDA).
In the presence of a CPP, separate GMPcertificates are redundant and are there-fore discouraged. CPPs should beaccepted (in particular from PIC/S andICH countries) as evidence of GMPstatus.
However, outside of the Scheme, thereare occasions when it is appropriate torequire a GMP certificate.
Q32 When a CPP forms part of a regula-
tory review, is it necessary to conduct asite inspection as well?
A32 An inspection should not be neces-sary when the GMP declaration on theCPP covers the product to be approved inthe recipient country.
Inspections outside of this condition are adecision which should be made by therecipient country. Mechanisms andsystems for recognizing inspections
carried out by other authorities is encour-aged to reduce duplication of inspections.
CPPs should be accepted (in particularfrom PIC/S and ICH countries) as evi-dence of GMP status. The decision toinspect should be made after a risk-basedassessment of the facility, taking intoaccount GMP and inspection statusprovided by other authorities.
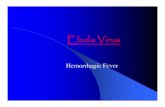
Q33 Imagine a situation in which com-pany A in one European country called Mproduces a pharmaceutical product calledX and the product is authorized formarketing in that country. Company Aalso produces X under contract manufac-turing in country Z in Asia and wants toexport it to country Y in Africa. Theauthority in the importing country Yrequires a CPP to approve importation.(See figure 1 overleaf.)
The questions are:
Q33a Is contract manufacturing ac-cepted?
A33a Yes. Contract manufacturing isaccepted under GMP.
Q33b In the case of a contract-manufac-tured product, from which country shouldthe authority in the importing country(receiving authority) accept the CPP?
A33b Country Z can issue a CPP if theproduct is registered by the authority ofcountry Z. If the product is not registeredin Z then the authority in Z cannot issue
the CPP.
If the contract-manufactured product isalso authorized for marketing in theEuropean country, then the Europeancountry can issue the certificate.
If the product is not registered in bothcountries, then the only country that canissue a certificate will be the Europeancountry, M. The authority of the Europeancountry will issue the CPP after it has
satisfied itself that the product undercontract manufacture is the same in allaspects as the one produced in its owncountry and that the product is producedin compliance with GMP.
Q34 Can a CPP also be used to provideevidence of an administrative review andapproval, e.g., as certification of accept-ability of a company name change?
Quality Assurance Issues
-
8/13/2019 who.drug information.pdf
22/52
120
WHO Drug Information Vol. 25, No. 2, 2011
A34 Yes. The CPP can also provideevidence of an administrative review andapproval (e.g., as certification of accept-ability of a company name change, or fora name change of the owner of a manu-facturing or production site) which oftenhappens in the context of companymergers and acquisitions.
For administrative approvals that nowinvolve a QSE review, recipient authori-ties should use alternatives to a CPP as apreferred and quicker option (see Ques-tion 9).
Issues related to manufacturing companyname change (administrative review) may
indeed create various practical difficultiesfor exportersimporters but are notassociated directly with safety/qualityconcerns and should be given lessprominence.
Q35 Imagine a situation in which aproduct is authorized for marketing in thecountry of manufacture but is not actuallyavailable on the market. Can the compe-
tent authority of the exporting countryissue a CPP to support export?
A35 Yes, it can issue a CPP. What itshould do is explain why it is not on themarket. One reason for not being on themarket could be that the disease/healthproblem for which the product is indicatedmay not be prevalent in the country.
Q36 Sometimes a country may wish toimport a special dosage form, strength orformulation of a certain known productand this particular product may not beregistered in the manufacturing country.Under such circumstances can the
authority of the exporting country issue aCPP?
A36 Yes. It can issue a CPP but it shouldexplain on the certificate that the particu-lar product is not authorized for marketingin the exporting country, that it has beenproduced based on the request of theimporting country and that manufacturingis in compliance with GMP.
Quality Assurance Issues
Figure 1. Question 33: contract manufacturing
CPP PRODUCT
Country Y in Africa
Importing
Company Aproduces X in a
European country M
Product X isregistered in that
country
Company A also con-tract manufactures X in
country Z in Asia
-
8/13/2019 who.drug information.pdf
23/52
121
WHO Drug Information Vol. 25, No. 2, 2011
Q37 Is it necessary to legalize the CPP?
A37 No. Legalization is not part of theWHO Scheme and it is not considered toprovide additional assurance of authentic-
ity. Approval status in key referencecountries is currently available as publicinformation.
Legalization should not be necessarysince an official governmental authority ofthe certifying country signs the CPP.Legalization delays availability of the CPPand thereby delays access to medicinesfor patients. If a recipient authority hasany doubts about the validity of a CPP itshould contact the certifying authority
directly.
Q38 What should receiving countries doin case of any doubt about a CPP?
A38 In case of any doubt, the competentauthorities of receiving countries shouldcommunicate directly with the authorizedbody that has issued the certificate orcontact WHO to clarify the matter.
Q39 Are certifying authorities penalized ifthey issue CPPs, but do not meet WHOrequirements for self-certification andsubsequent issue of CPPs?
A39 No. There is no penal system. WHOdoes not have the power to certify,inspect or penalize certifying authorities.
Q40 What are the main problems en-countered in the application of theScheme?
A40 A number of problems have been
reported during use of the Scheme, whichinclude:
Countries not party to the Scheme issuecertificates.
Authorities that do not meet the require-ments stated in the guidelines for theScheme issue certificates.
Some issuing authorities put the WHOemblem, logo or acronym on the certifi-cate, thereby creating the impression
that the certificate is authenticated byWHO.
References
1. WHO Certification Scheme on the Quality ofPharmaceutical Products Moving in Interna-tional Commerce. World Health Assemblyresolution WHA22.50 (1969), World HealthAssembly resolution WHA28.65 (1975), WorldHealth Assembly resolution WHA41.18 (1988),World Health Assembly resolution WHA45.29
(1992), and World Health Assembly resolutionWHA50.3 (1997) available at: http://www.who.int/governance
2. World Health Organization. Expert Commit-tee on Specifications for PharmaceuticalPreparations. Technical Report Series,2009;953:47-48 at http://www.who.int/medi-cines/publications.
Quality Assurance Issues
-
8/13/2019 who.drug information.pdf
24/52
122
WHO Drug Information Vol. 25, No. 2, 2011
Regulatory Action and News
Buflomedil: marketingauthorization suspended
France On 11 February 2011, theHealth Products Safety Agency(AFSSPS) suspended the marketingauthorization for buflomedil-containingproducts. This action was taken followingnotification of serious nervous and car-diac events especially during accidentalor voluntary overdose.
Reference: Spcialits base de Buflomdil Retrait de produits. 17 February 2011 athttp://www.afssaps.fr
Dolasetron mesylateintravenous injection:withdrawal
Canada The manufacturer of dolase-tron mesylate (Anzemet) has an-nounced withdrawal of the injectable
form. New data show that intravenousadministration of the injectable form ofdolasetron mesylate is associated withQTc prolongation to an extent which maypotentially result in serious arrhythmias atthe doses recommended for the preven-tion of nausea and vomiting associatedwith chemotherapy. Dolasetron mesylateinjectable is no longer indicated to pre-vent nausea and vomiting in adultsundergoing chemotherapy.
However, tablets for oral use may still beused as the risk of developing an abnor-mal heart rhythm with the oral form of thisdrug is considered less than that seenwith the injectable form.
Reference: Health Canada, Medeffect. 26April 2011. http://www.healthcanada.gc.ca/medeffect and http://www.hc-sc.gc.ca/dhp-mps/medeff/advisories-avis/new-neuf-advisories-avis-eng.php
Abiraterone acetate approvedfor late-stage prostate cancer
United States of America The Foodand Drug Administration (FDA) hasapproved abiraterone acetate (Zytiga) incombination with prednisone to treatpatients with metastatic castration-resistant prostate cancer who havereceived prior docetaxel.
Patients who received the Zytiga andprednisone combination had a medianoverall survival of 14.8 months comparedto 10.9 months for patients receiving theplacebo and prednisone combination.
The most commonly reported side effectsincluded joint swelling or discomfort, lowlevels of potassium in the blood, fluidretention (usually of the legs and feet),muscle discomfort, hot flashes, diarrhoea,urinary tract infection, cough, high blood
pressure, heartbeat disorders, urinaryfrequency, increased night-time urination,upset stomach or indigestion and upperrespiratory tract infection.
Reference: FDA News Release, 28 April 2011at http://www.fda.gov
Rituximab approved forWegener granulomatosis andmicroscopic polyangiitis
United States of America The Foodand Drug Administration (FDA) hasapproved rituximab (Rituxan) in combi-nation with glucocorticoids to treat pa-tients with Wegener granulomatosis (WG)and microscopic polyangiitis (MPA), tworare disorders that cause vasculitis.
Rituximab is an antibody that is manufac-tured through biotechnology methods.
-
8/13/2019 who.drug information.pdf
25/52
123
WHO Drug Information Vol. 25, No. 2, 2011 Regulatory Action and News
Safety and effectiveness was demon-strated in a single controlled trial in which197 patients with WG or MPA wereassigned at random to receive eitherRituxan plus glucocorticoids once aweek for four weeks or oral cyclophos-phamide plus glucocorticoids daily toinduce remission. After six months, 64%of patients treated with Rituxan hadcomplete remission compared to 53% ofpatients treated with cyclosphosphamide.
Rituximab carries a boxed warning forinfusion reactions. Other boxed warningsinclude severe mucocutaneous reactionsand progressive multifocal leukoence-phalopathy. Rituximab is not recom-
mended for use in patients with severe,active infections.
The most common side effects in studyparticipants with WG and MPA includedinfection, nausea, diarrhoea, headache,muscle spasms, and anaemia.
Rituximab, which has been marketedsince 1997, is also indicated for thetreatment of patients with non-Hodgkinlymphoma, chronic lymphocytic leukae-mia, and rheumatoid arthritis.
Reference: FDA News Release, 19 April 2011at http://www.fda.gov
Human normal immuno-globulin: lifting of suspension
European Union The EuropeanMedicines Agency Committee for Medici-nal Products for Human Use (CHMP) has
recommended the lifting of the suspen-sion of the marketing authorizations forhuman normal immunoglobulin 5% and10% (Octagam) and associated names,and the re-introduction of the medicineonto the market in the European Union.
The lifting of the suspension is subject toa change in the manufacturing process.Human normal immunoglobulin is an
intravenous solution used to strengthenthe bodys immune system.
The CHMP recommended the suspen-sion of the marketing authorizationsfollowing an unexpected increase inreports of thromboembolic reactions,including stroke, myocardial infarctionand pulmonary embolism in patientsreceiving the medicine.
An in-depth review of all available data onthe safety and quality issues identifiedpreviously has now been finalized. TheCHMP has concluded that the unex-pected presence of a pro-coagulant,factor XIa, was the main cause of the
thromboembolic events and that anumber of critical steps in the manufac-turing process could explain the presenceof substances that triggered the throm-boembolic events.
The Committees opinion has now beenforwarded to the European Commissionfor the adoption of a legally bindingdecision. It is expected that supply ofOctagam will resume shortly after theadoption of the Commission decision.
Reference: EMA Press Release, EMA/297816/2011, 14 April 2011 at http://www.ema.eu
Everolimus approved forpancreatic cancer
United States of America The Foodand Drug Administration (FDA) hasapproved everolimus (Afinitor) to treat
patients with progressive neuro-endocrinetumours located in the pancreas (PNET)that cannot be removed by surgery orhave become metastatic.
Neuro-endocrine tumours found in thepancreas are slow-growing and rare. It isestimated that there are fewer than 1000new cases in the United States eachyear.
-
8/13/2019 who.drug information.pdf
26/52
124
WHO Drug Information Vol. 25, No. 2, 2011Regulatory Action and News
The most commonly reported side effectsincluded stomatitis, rash, diarrhoea,fatigue, edema, abdominal pain, nausea,fever and headache.
Afinitor is also approved to treat pa-tients with advanced renal cell carcinomaafter they fail treatment with sunitinib orsorafenib, and patients with subependy-mal giant cell astrocytoma associatedwith tuberous sclerosis who cannot betreated with surgery.
Reference: FDA News Release, 6 May 2011at http://www.fda.gov
Boceprevir approved
for hepatitis C
United States of America The Foodand Drug Administration (FDA) hasapproved boceprevir (Victrelis) to treatcertain adults with chronic hepatitis C.Boceprevir is used for patients who stillhave some liver function and who eitherhave not been previously treated withdrug therapy for hepatitis C or who havefailed such treatment. Boceprevir isapproved for use in combination withpeginterferon alfa and ribavirin.
Safety and effectiveness of boceprevirwas evaluated in two phase III clinicaltrials with 1500 adult patients. In bothtrials, two-thirds of patients receivingboceprevir in combination with pegylatedinterferon and ribavirin experienced asignificantly increased sustained virologicresponse.
According to the US Centers for DiseaseControl and Prevention, about 3.2 millionpeople in the United States have chronichepatitis C. Most liver transplants per-formed in the United States are due toprogressive liver disease caused byhepatitis C virus infection.
Reference: FDA News Release, 13 May 2011at http://www.fda.gov
Linagliptin approvedfor type 2 diabetes
United States of America The Foodand Drug Administration (FDA) has
approved linagliptin (Tradjenta) tabletsfor use with diet and exercise, to improveblood glucose control in adults with Type2 diabetes which is the most commonform of the disease, affecting between 90and 95% of the 24 million diabetics in theUnited States.
Linagliptin was demonstrated to be safeand effective in eight double-blind, pla-cebo-controlled clinical studies involvingabout 3800 patients with Type 2 diabetes.
Linagliptin has been studied as a stand-alone therapy and in combination withother type 2 diabetes therapies includingmetformin, glimepiride, and pioglitazone.Linagliptin has not been studied in combi-nation with insulin, and should not beused to treat people with type 1 diabetesor in those who have diabetic ketoacido-sis.
Reference: FDA News Release, 2 May 2011at http://www.fda.gov
Naproxcinod: withdrawal ofmarketing authorizationapplication
European Union The EuropeanMedicines Agency (EMA) has beennotified by the manufacturer of its deci-sion to withdraw its application for acentralized marketing authorization forthe medicine naproxcinod (Beprana),
375 mg hard capsules.
Naproxcinod was intended to be used forthe relief of the signs and symptoms ofosteoarthritis of the knee and hip inadults.
In its official letter, the company statedthat their decision to withdraw the appli-
-
8/13/2019 who.drug information.pdf
27/52
125
WHO Drug Information Vol. 25, No. 2, 2011
cation was based on the fact that theCommittee for Medicinal Products forHuman Use (CHMP) considers that thedata provided do not allow it to concludeon a positive benefit-risk balance.
Reference: EMA Press Release, EMA/322628/2011, 20 April 2011 at http://www.ema.eu
Lumiracoxib: withdrawal ofmarketing authorizationapplication
European Union The EuropeanMedicines Agency (EMA) has beennotified by the manufacturer of its deci-
sion to withdraw its application for acentralized marketing authorization forthe medicine lumiracoxib (Joicela) 100mg film-coated tablets. Lumiracoxib wasintended to be used for symptomatic reliefin the treatment of osteoarthritis of theknee and hip in patients who are non-carriers of the DQA1*0102 allele.
In its official letter, the company statedthat its decision to withdraw the applica-tion was based on its inability to addressthe CHMP request to provide additionaldata within the timeframe allowed in thecentralized procedure.
Reference: EMA Press Release, EMA/309990/2011, 18 April 2011 at http://www.ema.eu
Erythropoietin: withdrawal ofmarketing authorizationapplication
European Union The EuropeanMedicines Agency (EMA) has beennotified by the manufacturer of its deci-
sion to withdraw its application for acentralized marketing authorization forthe medicine erythropoietin (Epostim),2000 IU/ 0.5 ml, 4000 IU/0.4 ml, and10 000IU/ml solution for injection in pre-filled syringes.
This medicine was intended to be usedfor the following indications:
Treatment of anaemia associated withchronic renal failure in paediatric andadult patients on haemodialysis andadult patients on peritoneal dialysis.
Treatment of severe anaemia of renalorigin accompanied by clinical symp-
toms in adult patients with renal insuffi-ciency not yet undergoing dialysis.
Treatment of anaemia and reduction oftransfusion requirements in adultpatients receiving chemotherapy forsolid tumours, malignant lymphoma ormultiple myeloma.
To increase the yield of autologousblood from patients in a predonationprogramme.
To reduce exposure to allogenic bloodtransfusions in adult non-iron deficientpatients prior to major elective ortho-paedic surgery.
In its official letter, the company statedthat its decision to withdraw the applica-tion was based on its inability to addressthe CHMPs request to provide additionaldata within the timeframe allowed in thecentralized procedure.
Reference: EMA Press Release, EMA/271900/2011, 6 April 2011 at http://www.ema.eu
Regulatory Action and News
-
8/13/2019 who.drug information.pdf
28/52
126
WHO Drug Information Vol. 25, No. 2, 2011
ATC/DDD Classification
The following anatomical therapeutic chemical (ATC) classifications and defined dailydoses (DDDs) were agreed by the WHO International Working Group for Drug Sta-tistics Methodology March 2011. Comments or objections to the decisions should beforwarded to the WHO Collaborating Centre for Drug Statistics Methodology [email protected]. The new ATC codes and DDDs will be considered final and be in-cluded in the January 2012 issue of the ATC index. The inclusion of a substance inthe lists does not imply any recommendation of use in medicine or pharmacy. TheWHO Collaborating Centre for Drug Statistics Methodology can be contacted throughe-mail at: [email protected].
ATC/DDD Classification (temporary)
ATC level INN/Common name ATC code
New ATC 5th level codes:abiraterone L02BX03aflibercept S01LA05axitinib L01XE17bosutinib L01XE14brentuximab vedotin L01XC12catridecacog B02BD11crizotinib L01XE16
dapagliflozin A10BX09dexlansoprazole A02BC06levomethadone N07BC05losartan and amlodipine C09DB06meloxicam, combinations M01AC56mipomersen C10AX11naproxen and misoprostol M01AE56pasireotide H01CB05perampanel N03AX22ruxolitinib L01XE18sipuleucel-T L03AX17tafamidis N07XX08
telaprevir J05AE11tesamorelin H01AC06vemurafenib L01XE15
ATC name changes
Previous New ATC code
Antigrowth hormones Somatostatin and analogues H01CBCalcium, combinations with Calcium, combinations with other drugs vitamin D and/or other drugs A12AXEnzyme inhibitors Aromatase inhibitors L02BG
-
8/13/2019 who.drug information.pdf
29/52
127
WHO Drug Information Vol. 25, No. 2, 2011
New DDDs:
INN/common name DDD Unit Adm.R ATC code
aspoxicillin 4 g P J01CA19
aztreonam 0.225 g Inhal. solution J01DF01bekanamycin 0.6 g P J01GB13carumonam 2 g P J01DF02cefbuperazone 2 g P J01DC13cefminox 4 g P J01DC12conestat alfa 3.5 TU P B06AC04desvenlafaxine 50 mg O N06AX23fingolimod 0.5 mg O L04AA27flomoxef 2 g P J01DC14histrelin 0.137 mg1 implant H01CA03isepamicin 0.4 g P J01GB11ribostamycin 1 g P J01GB10
tapentadol 0.4 g O N02AX06ticagrelor 0.18 g O B01AC24vernakalant 0.2 g P C01BG11
1. DDD assigned according to the total content of the implant.
Herbal medicinal products*
New ATC 5th level codes::
Name ATC code
St. Johns Wort N06AX25
2. Assessed and approved by regulatory authorities based on dossiers including efficacy, safety,and quality data (e.g., well-established use procedure in EU).
ATC/DDD Classification
.../...
-
8/13/2019 who.drug information.pdf
30/52
128
WHO Drug Information Vol. 25, No. 2, 2011
The following anatomical therapeutic chemical (ATC) classifications and defined dailydoses (DDDs) were agreed by the WHO International Working Group for Drug Sta-tistics Methodology in October 2010. They will be included in the January 2012 issueof the ATC index. The inclusion of a substance in the lists does not imply any recom-mendation of use in medicine or pharmacy. The WHO Collaborating Centre for DrugStatistics Methodology can be contacted at [email protected].
ATC/DDD Classification (final)
ATC level INN/Common name ATC code
New ATC level codes (other than 5th level):Drugs used in hereditary angioedema B06AC
New ATC 5th level codes:aspoxicillin J01CA19azilsartan medoxomil C09CA09bekanamycin J01GB13cabazitaxel L01CD04carumonam J01DF02cefbuperazone J01DC13cefminox J01DC12
cinchocaine S02DA04conestat alfa B06AC04dienogest G03DB08dimeticone P03AX05donepezil and memantine N06DA52doxylamine,combinations R06AA59ecallantide B06AC03emtricitabine, tenofovir disoproxil and rilpivirine J05AR08flomoxef J01DC14fluindione B01AA12
iloperidone N05AX14ipilimumab L01XC11meningococcus B, multi-component vaccine J07AH09metformin and linagliptin A10BD11metformin and saxagliptin A10BD10motavizumab J06BB17panobinostat L01XX42pentosan polysulfate sodium G04BX15
ATC/DDD Classification
.../...
-
8/13/2019 who.drug information.pdf
31/52
129
WHO Drug Information Vol. 25, No. 2, 2011
pirfenidone L04AX05ramipril and amlodipine C09BB07rilpivirine J05AG05secukinumab L04AC10sinecatechins D06BB12teduglutide A16AX08tetrachlorodecaoxide D03AX11vilazodone N06AX24von Willebrand factor B02BD10
ATC code changes:
INN/common name Previous ATC New ATC
alitretinoin D11AX19 D11AH04
C1-inhibitor, plasma derived B02AB03 B06AC01icatibant C01EB19 B06AC02
ATC name changes
Previous New ATC code
Agents for atopic dermatitis, excluding Agents for dermatitis, corticosteroids excluding corticosteroids D11AHOther cold combination preparations Other cold preparations R05X
New DDDs:
INN/common name DDD Unit Adm.R ATC code
asenapine 20 mg O N05AH05corifollitropin alfa 0.15 mg P G03GA09dienogest 2 mg O G03DB08eltrombopag 50 mg O B02BX05fampridine 20 mg O N07XX07flupirtine 0.4 g O N02BG07indacaterol 0.15 mg Inhal. powder R03AC18indometacin, combinations 0.1 g1 O,R M01AB51mifamurtide 0.7 mg P L03AX15prucalopride 2 mg O A03AE04roflumilast 0.5 mg O R03DX07velaglucerase alfa 300 U P A16AB10
1.refers to indometacin
ATC level INN/Common name ATC code
ATC/DDD Classification
-
8/13/2019 who.drug information.pdf
32/52
130
WHO Drug Information Vol. 25, No. 2, 2011ATC/DDD Classification
Herbal medicinal products*
New ATC 5th level codes::
Name ATC code
Horse chestnut, seeds C05CX03
*Assessed and approved by regulatory authorities based on dossiers includingefficacy, safety, and quality data (e.g., well-established use procedure in EU).
-
8/13/2019 who.drug information.pdf
33/52
131
WHO Drug Information Vol. 25, No. 2, 2011
Recent Publications,
Information and Events
Selection and use of medicines
World Health Organization The 18thmeeting of the WHO Expert Committeeon the Selection and Use of EssentialMedicines took place in Accra, Ghana on2125 March 2011. The purpose of themeeting was to review and update theWHO Model List of Essential Medicines(EML) as well as the WHO Model List ofEssential Medicines for Children (EMLc).
In accordance with its approved proce-dures, the Committee evaluated thescientific evidence on the comparativeeffectiveness, safety and cost effective-ness of medicines and updated the WHOModel List of Essential Medicines and theModel List of Essential Medicines forChildren. The Committee:
Approved the addition of 16 new medi-cines to the EML.
Approved the deletion of 13 medicinesfrom the EML.
Approved new indications for 4 medi-cines already listed on the EML.
Approved the addition of a new dosageform or strength for 4 medicines alreadyon the EML.
Rejected 9 applications for the addition
of a medicine to EML.
Approved the addition of 16 new medi-cines to the EMLc.
Approved the deletion of 15 medicinesfrom the EMLc,
Rejected 3 applications for the additionof a new medicine to the EMLc.
Some of the main recommendationsmade, in order of their appearance on theEML, were:
Section 6: addition of artesunate +amodiaquine combination tablet for thetreatment of malaria in adults andchildren, in line with current WHOtreatment guidelines. In making itsdecision, the 2011 Committee reviewedthe latest clinical evidence and the
information about licensing in severalcountries of the fixed dose combinationtablet. The Committee noted thatappropriate doses of both medicinescan also be achieved using combina-tions of the mono-component products,including as co-blistered presentations.
Section 10: addition of tranexamic acidinjection for the treatment of adultpatients with trauma and significant riskof ongoing haemorrhage. On the basisof the results of a very large trial of theuse of tranexamic acid specifically fortrauma patients including those whohave been in road traffic accidents, theCommittee concluded that there issufficient evidence to support theproposal that listing tranexamic acidmay contribute to a reduction in thiscause of death.
Section 18.5 : addition of glucagon
injection, 1 mg/ml to treat acute severehypoglycaemia in patients with diabe-tes, to support efforts in many countriesto ensure appropriate treatment of theincreasing number of patients withdiabetes. The Committee also recom-mended that careful attention be paid tothe cost of procuring glucagon andnoted that based on experience withother high cost medicines, such as
-
8/13/