“When Sleep Plays Coy”
31
7/10/2019 1 “When Sleep Plays Coy” * The Management of Insomnia in Hospice Care By: Joelle Potts, PharmD, BCGP July 9th & 10th, 2019 *From “Insomniac” by Maya Angelou Conflict of Interest and Disclosures of Relevant Financial Relationships The planners and presenters (spouse/domestic partner) of this educational activity have disclosed no healthcare related conflicts of interest, commercial interest, or have any related financial relationships/support. The material in this presentation is for informational and educational purposes only and is not a substitute for medical advice, diagnosis, or treatment provided by a qualified health care provider. All information contained in this presentation is protected by copyright and remains the property of ProCare HospiceCare. All rights are reserved.
Transcript of “When Sleep Plays Coy”

7/10/2019
1
“When Sleep Plays Coy”*
The Management of Insomnia in Hospice CareBy: Joelle Potts, PharmD, BCGP
July 9th & 10th, 2019
*From “Insomniac” by Maya Angelou
Conflict of Interest and Disclosures of Relevant Financial
Relationships
The planners and presenters (spouse/domestic partner) of this educational activity have disclosed no healthcare related conflicts of interest, commercial interest, or have any related financial relationships/support.
The material in this presentation is for informational and educational purposes only and is not a substitute for medical advice, diagnosis, or treatment provided by a qualified health care provider. All information contained in this presentation is protected by copyright and remains the property of ProCare HospiceCare. All rights are reserved.

7/10/2019
2
Contact Hours –Nursing
1.0 Contact Hour
ProCare HospiceCare is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center’s Commission on Accreditation. (P-0544, 3/31/2021)
Successful Completion Criteria
• Register for theactivity
• Complete and submitthe sign-in sheet
• View the entirepresentation
• Complete and submitthe participantevaluation
• Certificate will beemailed uponcompletion of thecriteria
The material in this presentation is for informational and educational purposes only and is not a substitute for medical advice, diagnosis, or treatment provided by a qualified health care provider. All information contained in this presentation is protected by copyright and remains the property of ProCare HospiceCare. All rights are reserved.

7/10/2019
3
Objectives
Review the physiology of sleep vs. wakefulness and “normal” sleep aswell as the types of sleep disorders
Identify common causes of insomnia and/or disrupted sleep, focusingon those most relevant to the elderly and hospice populations
Describe non-pharmacologic measures to improve sleep, including“sleep hygiene” practices
Evaluate pharmacologic therapies that can be used for sleep,emphasizing those most commonly used and/or appropriate forhospice patients
The Physiology of Sleep vs. Wakefulness: Homeostatic System
Homeostasis = balance, equilibrium
AKA sleep/wake restorative process – balances sleep and wakefulness
Appears to control NREM (non-rapid eye movement) and slow wave sleep(stages 3 and 4)
Sleep is a primary drive
Adenosine
Induces sleepiness; levels accumulate the longer you’re awake
Effects blocked by caffeine
Winter WC. Kryger M, Kryger E. Mystakidou K, et al.
The material in this presentation is for informational and educational purposes only and is not a substitute for medical advice, diagnosis, or treatment provided by a qualified health care provider. All information contained in this presentation is protected by copyright and remains the property of ProCare HospiceCare. All rights are reserved.

7/10/2019
4
The Physiology of Sleep vs. Wakefulness: Circadian System
AKA day-night cycle, sleep-wake rhythm – regulates timing of sleepand wakefulness
Affects the distribution of REM sleep
Suprachiasmatic Nucleus (SCN) = biological clock, circadianpacemaker of the brain
SCN wakefulness drive counteracts the homeostatic drive’s dip inalertness in the afternoon
Affected by light and dark; synchronized by light
Melatonin induces sleepiness
Produced in conditions of darkness… darkness signals retinal cells suprachiasmatic nucleus (SCN) pineal gland releases melatonin
Dopp JM, Phillips BG. Kryger M, Kryger E. Mystakidou K, et al. Winter WC.
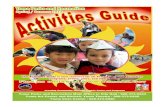
Stages of Sleep
Dopp JM, Phillips BG. Mystakidou K, et al. Bubble diagram from Winter WC. Hypnogram from Neubauer DN.
Awake
Dream
Sleep
Dream (REM) Sleep
DeepSleep
Light Sleep
REM (rapid eye movement) vs. NREM (non-rapid eye movement)
4 Stages of NREM sleep
Stage 1: Stage between wakefulness and asleep
Stage 3 and 4: Metabolic activity and brain waves slow, AKA delta sleep orslow-wave sleep
The material in this presentation is for informational and educational purposes only and is not a substitute for medical advice, diagnosis, or treatment provided by a qualified health care provider. All information contained in this presentation is protected by copyright and remains the property of ProCare HospiceCare. All rights are reserved.
7/10/2019
5
Other Neurochemistry Involved
NREM sleep: Mediated by GABA and adenosine
REM sleep
Turned on by cholinergic cells
Turned off by dorsal raphe nucleus, locus coeruleus, and nucleusparabrachialis lateralis (the latter two are primarily noradrenergic)
Dopamine has an alerting effect; decreases in dopamine promotesleepiness
Wakefulness
Norepinephrine and acetylcholine
Histamine and neuropeptides (e.g. substance P) and corticotropin-releasing factor
Dopp JM, Phillips BG.
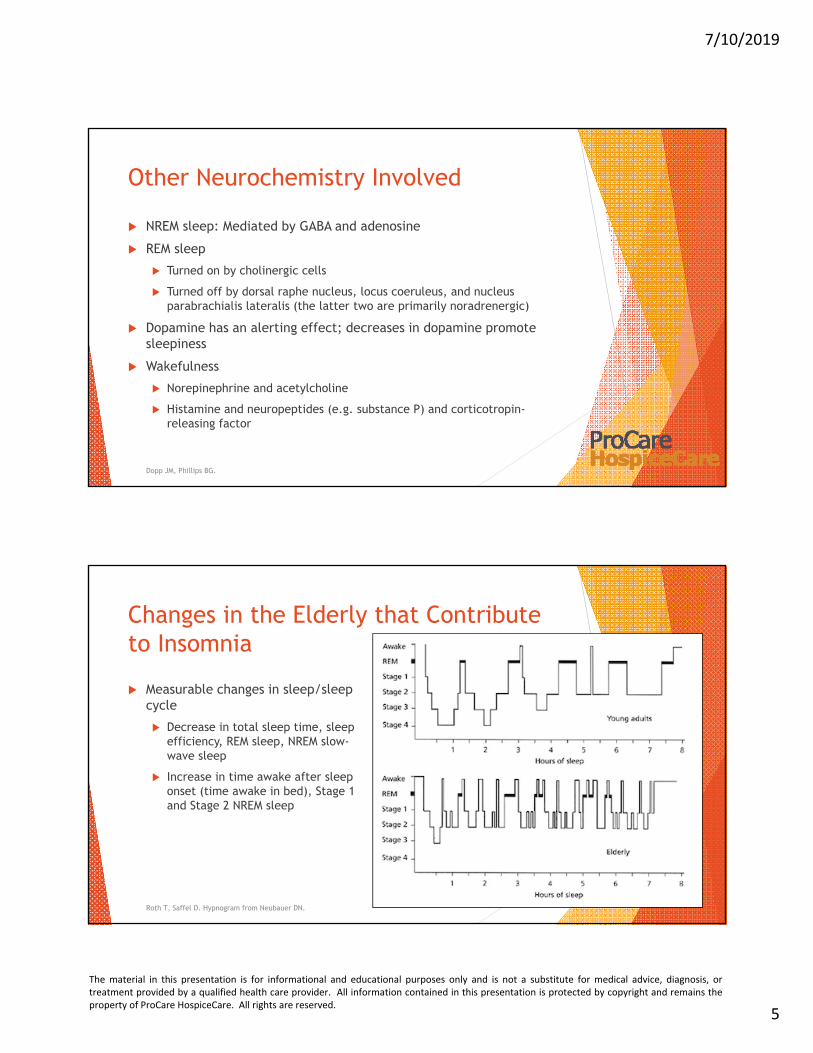
Changes in the Elderly that Contribute to Insomnia
Measurable changes in sleep/sleepcycle
Decrease in total sleep time, sleepefficiency, REM sleep, NREM slow-wave sleep
Increase in time awake after sleeponset (time awake in bed), Stage 1and Stage 2 NREM sleep
Roth T, Saffel D. Hypnogram from Neubauer DN.
The material in this presentation is for informational and educational purposes only and is not a substitute for medical advice, diagnosis, or treatment provided by a qualified health care provider. All information contained in this presentation is protected by copyright and remains the property of ProCare HospiceCare. All rights are reserved.

7/10/2019
6
Changes in the Elderly that Contribute to Insomnia, continued
Physiological/chemical changes
Age-related changes in the Suprachiasmatic Nucleus (SCN), the circadianpacemaker
Increase in Orexin A as we age – wakefulness transmitter
Older people tend to go to sleep and wake earlier (Advanced Sleep-Phase Syndrome)
Increased prevalence in insomnia-causing conditions (e.g. prostate, hipimpairment, pulmonary disease/obstructive sleep apnea,depression/late-life stressors)
Do we need less sleep as we age?
National Sleep Foundation recommends 7-9 hours of sleep for young adults(18-25) and adults (26-64), and 7-8 hours of sleep for older adults (65+)
Roth T, Saffel D. Kryger M, Kryger E.
Sleep Disorders Per DSM-5 (Diagnostic and Statistical Manual of Mental Disorders, 5th Edition)
Insomnia disorder
Hypersomnolence disorder
Narcolepsy
Breathing-related sleep disorders (e.g. central sleep apnea, obstructive sleepapnea)
Circadian rhythm sleep disorders (e.g. jet lag, shift work sleep disorder)
Non-REM sleep arousal disorders
Nightmare disorder
REM sleep behavior disorder
Restless legs syndrome (RLS)
Substance- or medication-induced sleep disorder
Dopp JM, Phillips BG.
The material in this presentation is for informational and educational purposes only and is not a substitute for medical advice, diagnosis, or treatment provided by a qualified health care provider. All information contained in this presentation is protected by copyright and remains the property of ProCare HospiceCare. All rights are reserved.

7/10/2019
7
Insomnia
Defined as difficulty falling asleep, difficulty staying asleep, and/orhaving non-restorative sleep
Is subjective
Primary insomnia vs. secondary/comorbid insomnia
Prevalence:
Approx. 30% of adults report one or more of these symptoms above
In chronically ill non-cancer patients: more common in women and olderadults
In cancer patients: more common in younger patients; those with breastand lung cancer have higher rates of sleep disturbances
Other chronic diseases associated with sleep disturbances: HIV/AIDS,COPD, liver disease, degenerative brain diseases (e.g. Alzheimer’s)
Dopp JM, Phillips BG. Mystakidou K, et al.
Common Etiologies of Insomnia
Situational
Work/financialstress, major lifeevents, interpersonalconflict
Jet lag, shift work
Medical
Cardiovascular(arrhythmias,angina, heart failure)
Respiratory (asthma,sleep apnea)
Chronic pain
Endocrine disorders(diabetes,hyperthyroidism)
GI (GERD, ulcers)
Neurologic (delirium,epilepsy, Parkinson’s)
Pregnancy
Psychiatric
Mood disorders(depression, mania)
Anxiety disorders(e.g. GAD, OCD)
Substance abuse(alcohol or sedative-hypnotic withdrawal)
Dopp JM, Phillips BG.
The material in this presentation is for informational and educational purposes only and is not a substitute for medical advice, diagnosis, or treatment provided by a qualified health care provider. All information contained in this presentation is protected by copyright and remains the property of ProCare HospiceCare. All rights are reserved.
7/10/2019
8
Common Etiologies of Insomnia, continued: Pharmacologically Induced
Anticonvulsant – e.g. lamotrigine
Central adrenergic blocker – e.g. beta-blockers: metroprolol, propranolol,sotalol
Diuretics
SSRI antidepressant – e.g. citalopram, fluoxetine, fluvoxamine,venlafaxine, paroxetine
Steroids
Stimulants – e.g. methylphenidate, theophylline, caffeine
Others: donepezil, clonidine, pseudoephedrine, ciprofloxacin, levofloxacin
Dopp JM, Phillips BG. Foral P, Knezevich J, Dewan N, Malesker M. LexiComp drug monographs.
Non-Pharmacologic Measures: Stimulus Control
Establish regular sleep and wake times (including weekends)
Sleep only as much as needed to feel rested
Use the bed only for sleep or intimacy
Go to bed only when sleepy, avoid long periods of wakefulness in bed
Do not read or watch TV in bed; don’t use the bed for working or lounging
Dopp JM, Phillips BG. Winter WC. Patel D, et al.
The material in this presentation is for informational and educational purposes only and is not a substitute for medical advice, diagnosis, or treatment provided by a qualified health care provider. All information contained in this presentation is protected by copyright and remains the property of ProCare HospiceCare. All rights are reserved.

7/10/2019
9
Non-Pharmacologic Measures: Stimulus Control, continued Avoid trying to force sleep
If you do not fall asleep within 20-30 minutes, get up and perform arelaxing activity until drowsy. Repeat as often as necessary.
But… Note that the 20-30 minute rule is somewhat arbitrary and cancause stress/anxiety; there are benefits to simply “resting” in bed, key isnot becoming anxious about not sleeping. If it is consistently taking youlonger than 20-30 minutes to fall asleep, you’re likely going to bed tooearly and should go to bed later.
Avoid blue spectrum light from devices (including television)
Avoid daytime naps; may take a brief (20-30 minute) nap, early inthe day
Schedule worry time during the day; do not take your troubles tobed
Dopp JM, Phillips BG. Winter WC. Patel D, et al.
Non-Pharmacologic Measures: Sleep Hygiene Exercise routinely
3-4 times weekly, but at least 6 hours before bedtime
Create comfortable sleep environment
Avoid temperature extremes, loud noises, illuminated (and/or ticking) clocks inthe bedroom
Cooler environmental temperatures typically contribute to higher-quality sleep
Discontinue or reduce use of alcohol, caffeine, and nicotine
Avoid drinking large amounts of liquid in the evening, to prevent overnighttrips to the bathroom
Do something relaxing and enjoyable before bedtime
Dopp JM, Phillips BG. Winter WC. Patel D, et al.
The material in this presentation is for informational and educational purposes only and is not a substitute for medical advice, diagnosis, or treatment provided by a qualified health care provider. All information contained in this presentation is protected by copyright and remains the property of ProCare HospiceCare. All rights are reserved.

7/10/2019
10
Other Non-Pharmacologic Measures
Hot bath or shower before bed improved sleep quality
Exposure to green spaces and nature – found to improve sleep,especially in men
Sleep restriction
Restrict time in bed to the number of hours of actual sleep (i.e. to theamount of sleep needed), until sleep efficiency improves
If sleep efficiency remains lower than 85% after 10 days, restrict sleeptime in bed by 15-30 minutes until sleep efficiency improves; time in bedis gradually increased by 15-30 minutes when time asleep exceeds 85% oftotal time in bed
Winter WC. Roth T, Saffel D. Patel D, et al.
Other Non-Pharmacologic Measures, continued
Relaxation techniques
E.g. progressive muscle tensing/relaxing, guided imagery, paceddiaphragmatic breathing, meditation
Appropriate use of light vs. dark…
To combat Advanced Sleep-Phase Syndrome (ASPS)… Many elderly peoplesit in darkened houses/rooms in the evening; encourage them to sit inlight in the evening as appropriate
If getting to sleep is a problem… Keep environment dim at the end of theday
Once in bed, make room as dark as possible/safe/appropriate; ifnightlights are needed, keep them out of line of vision
Winter WC. Roth T, Saffel D. Patel D, et al.
The material in this presentation is for informational and educational purposes only and is not a substitute for medical advice, diagnosis, or treatment provided by a qualified health care provider. All information contained in this presentation is protected by copyright and remains the property of ProCare HospiceCare. All rights are reserved.

7/10/2019
11
Non-Pharmacologic Measures: Cognitive Behavioral Therapy for Insomnia (CBT-I or CBTI)
Targets factors that perpetuate insomnia over time (e.g. dysregulationof sleep drive, sleep-related anxiety, sleep-interfering behaviors)
Based on elements of sleep hygiene and behavior modification
vs. sleep hygiene alone… which has been found to be less effective thanCBT-I in studies
First-line therapy for all forms of insomnia, for all patients
Per the Guidelines of the Agency for Healthcare Research and Quality(2014) and American College of Physicians (ACP) (2016), and the AmericanAcademy of Sleep Medicine (AASM)
ACP cautiously recommends adding pharmacologic therapy when CBT-I isunsuccessful
Schroeck JL, et al. Mitchell MD, et al. Chung KF, et al. Sateia MJ, et al.
Non-Pharmacologic Measures: CBT-I Data Overall: CBT-I is at least as effective when compared to sleep medications,
and effects may be more durable than medications
Can improve time to sleep onset and time awake after sleep onset
CBT-I has greater effect on subjective measures of sleep than on objectivemeasures (e.g. polysomnography, actigraphy) – but insomnia can be a highlysubjective problem
Studies demonstrate the long-term effectiveness of CBT-I and itssuperiority over medications (benzodiazepines and non-benzodiazepines);appears to be more effective than medications at 6-12 months aftertreatment is complete
The downside:
Conflicting data re: short-term effectiveness of CBT-I vs. medications(benzodiazepines, zolpidem, zopiclone) at 4 to 8 weeks; more research needed
Improvements typically not seen until 3-4 weeks into treatment
Schroeck JL, et al. Mitchell MD, et al.
The material in this presentation is for informational and educational purposes only and is not a substitute for medical advice, diagnosis, or treatment provided by a qualified health care provider. All information contained in this presentation is protected by copyright and remains the property of ProCare HospiceCare. All rights are reserved.

7/10/2019
12
Drug Treatments
Terminology/Measures of Sleep Quality
Sleep-onset latency (or sleep latency) = the length of time it takes totransition from full wakefulness to sleep (following bedtime)
Sleep maintenance = the ability to stay asleep, measured by totalsleep time
Total sleep time = the total time asleep after sleep onset
Quality of sleep = subjective, patient-reported measure; definitioncan vary by measurement tool and patient perceptions
Schroeck JL, et al. Sateia MJ, et al.
The material in this presentation is for informational and educational purposes only and is not a substitute for medical advice, diagnosis, or treatment provided by a qualified health care provider. All information contained in this presentation is protected by copyright and remains the property of ProCare HospiceCare. All rights are reserved.

7/10/2019
13
Benzodiazepines
FDA-approved for treatment of short-term insomnia:
temazepam (Restoril®)
triazolam (Halcion®)
flurazepam
quazepam (Doral®)
estazolam
Mechanism of action: Bind to GABA receptors in CNS, inhibitingneuronal excitation
Generally: Reduce time to REM sleep, shorten sleep-onset latency, anddecrease nocturnal awakenings
Schroeck JL, et al. PL Detail-Document.
Benzodiazepines, continued Elderly have increased sensitivity to benzodiazepines d/t changes in the
GABA neurotransmitter system, and d/t age-related changes inpharmacokinetics and pharmacodynamics
Elderly are more predisposed to ataxia, sedation, and cognitive impairment
All except temazepam have prolonged elimination half-life in elderly
Flurazepam and quazepam have long half-life and active metabolites – avoid inelderly
Triazolam, estazolam, and temazepam do not have clinically significant activemetabolites
“LOT” drugs are preferred in elderly: Lorazepam, Oxazepam, Temazepam
Can develop physical dependence, and/or have rebound/withdrawalsymptoms with discontinuation, especially with high doses; increased riskof falls
2019 AGS Beers Criteria® Update: Generally avoid in elderly
Schroeck JL, et al. PL Detail-Document. 2019 Beers Criteria® Update. Kryger M, Kryger E.
The material in this presentation is for informational and educational purposes only and is not a substitute for medical advice, diagnosis, or treatment provided by a qualified health care provider. All information contained in this presentation is protected by copyright and remains the property of ProCare HospiceCare. All rights are reserved.

7/10/2019
14
Benzodiazepines, FDA-Approved for Insomnia, continued
Temazepam (Restoril®)
Onset of action: approx. 1 hour
Duration: 6-10 hours
Improves sleep onset and maintenance
Triazolam (Halcion®)
Onset of action: within 30 minutes
Duration: 2-5 hours
Improves sleep-onset latency
Not first-line d/t potential for rebound insomnia, anterograde amnesia,psychological dependence, anxiety
Schroeck JL, et al. PL Detail-Document.
Benzodiazepines, FDA-Approved for Insomnia, continued
Estazolam
Onset of action: 1-2 hours
Duration: 6-10 hours
Specific use: Sleep onset and maintenance
Flurazepam and Quazepam (Doral®)
Onset of action: 1-2 hours
Duration: 10-20 hours
Specific use: Sleep onset and maintenance
Long half-life and active metabolites, avoid in elderly
Schroeck JL, et al. PL Detail-Document.
The material in this presentation is for informational and educational purposes only and is not a substitute for medical advice, diagnosis, or treatment provided by a qualified health care provider. All information contained in this presentation is protected by copyright and remains the property of ProCare HospiceCare. All rights are reserved.

7/10/2019
15
Benzodiazepines Used Off-Label for Insomnia: Lorazepam (Ativan®), Oxazepam
Lorazepam
Onset of action: approx. 30 minutes
Typically used for secondary insomnia (e.g. d/t anxiety)
Improves sleep maintenance, not sleep onset
Oxazepam
Onset of action: 30-60 minutes
May be effective for sleep-onset insomnia
Duration of effect for insomnia: unclear
PL Detail-Document.
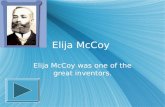
Nonbenzodiazepine GABAA Agonists (non-BzRAs, a.k.a. “Z” Drugs) Zolpidem (Ambien®), zaleplon (Sonata®), eszopiclone (Lunesta®)
GABA receptor complex = multicomponent, transmembranereceptor with multiple binding sites
GABAA complex is the major inhibitory receptor in the CNS; isassociated with sedation, anxiolysis, muscle relaxation,amnesia, and other cognitive effects
Lexicomp drug monographs. Schroeck JL, et al. Image from: Jacob TC, Moss SJ, Jurd R. GABAA receptor trafficking and its role in the dynamic modulation of neuronal inhibition. Nature Reviews Neuroscience. May 1, 2008; 9: 331-343.
Is composed of 5 subunits (α, β, and γ), with each subunit appearing toproduce a drug’s unique pharmacologic effects…. The α1 subunit mediates sedation/hypnotic effects; α2, α3, and α5 subunits mediate anxiolyticpathways; several different receptors control anticonvulsant, ataxic, muscle-relaxing effects
Benzodiazepines bind nonselectively to GABAA α subunits; the non-BzRAsbind more selectively to the α1 subunits
The material in this presentation is for informational and educational purposes only and is not a substitute for medical advice, diagnosis, or treatment provided by a qualified health care provider. All information contained in this presentation is protected by copyright and remains the property of ProCare HospiceCare. All rights are reserved.

7/10/2019
16
Non-BzRAs: FDA Adds Boxed Warning
April, 2019 -- For zolpidem, zaleplon, and eszopiclone
Can cause complex sleep behaviors, including sleepwalking, sleepdriving, and engaging in other activities while not fully awake – hasresulted in serious injuries and fatalities
Incidents can occur after first dose or after longer period of use, inpatients without any prior history of these behaviors, and even at thelowest recommended doses
Adding contraindication against use of these drugs in patients whohave experienced such an episode after taking them
Brooks M.
Non-BzRAs: Zolpidem (Ambien®)
Mechanism of action: Short-acting, GABAA α1-selective, with lesseraffinity for α2 and α3 receptors
Decreases sleep-onset latency and improves total sleep time in elderly
Dosage forms: IR tablet, ER tablet, SL tablet, oral spray
Maximum recommended dose of 5mg in females or elderly
Onset: 30 minutes
Duration (for IR, ER, oral spray, Edluar® SL tab): approx. 8 hours
Intermezzo® SL tab: approx. 4 hours
2019 Beers Criteria® Update: Avoid in elderly
Cost: Average for generic zolpidem IR tablets is approx. $2.60 per tablet,although can vary widely; other dosage forms can be significantly higher
Lexicomp zolpidem monograph. Schroeck JL et al. PL Detail-Document. 2019 Beers Criteria® Update.
The material in this presentation is for informational and educational purposes only and is not a substitute for medical advice, diagnosis, or treatment provided by a qualified health care provider. All information contained in this presentation is protected by copyright and remains the property of ProCare HospiceCare. All rights are reserved.

7/10/2019
17
Non-BzRAs: Zaleplon (Sonata®)
Mechanism of action: Binds selectively to the GABAA α1 subunit
Improves sleep-onset latency and sleep quality
Caution in liver impairment
Onset: 30 minutes
Duration: approx. 4 hours
Shortest duration of all the “Z” drugs; can be used for nighttime wakeningif more than 4 hours of potential sleep remain
Rebound insomnia more likely with higher doses
2019 Beers Criteria® Update: Avoid in elderly
Cost: approx. $3.70 per capsule (for generic)
Lexicomp zaleplon monograph. Schroeck JL et al. PL Detail-Document. 2019 Beers Criteria® Update.
Non-BzRAs: Eszopiclone (Lunesta®) Mechanism of action: Precise mechanism unknown; thought to result from
interaction with GABA-receptor complexes close to benzodiazepinereceptors Active metabolite contributes to sleep induction and maintenance effects
1mg dose improves sleep-onset latency; 2mg dose improves sleep-onsetlatency and sleep maintenance Typical adult dosing: 1mg PO immediately before bedtime, may be increased
to 2mg or 3mg
In elderly or debilitated patients, or concurrent use with strong CYP3A4inhibitors: maximum dose is 2mg
Onset: 30 minutes
Duration: approx. 8 hours
2019 Beers Criteria® Update: Avoid in elderly
Cost: approx. $12 per tablet (for generic; regardless of strength)
Lexicomp eszopiclone monograph. Schroeck JL et al. Eszopiclone Prescribing information. PL Detail-Document. 2019 Beers Criteria® Update.
The material in this presentation is for informational and educational purposes only and is not a substitute for medical advice, diagnosis, or treatment provided by a qualified health care provider. All information contained in this presentation is protected by copyright and remains the property of ProCare HospiceCare. All rights are reserved.

7/10/2019
18
Melatonin Receptor Agonist: Ramelteon(Rozerem®) Mechanism of action: Selective agonist of melatonin receptors MT1 and MT2
in the SCN of the hypothalamus
MT1 induces sleepiness, MT2 influences regulation of circadian rhythms; is moreselective for MT1 vs. MT2 and has a higher affinity for MT1 than melatonin
Longer half-life than melatonin
Improves sleep-onset latency
Onset: 30 minutes
Duration: approx. 8 hours
Some cautions with liver impairment (not recommended in severeimpairment)
Minimal ADEs; no withdrawal effects or rebound insomnia vs. placebo
Cost: approx. $15.50 per tablet (for brand, not available generically)
Lexicomp ramelteon monograph. Schroeck JL, et al. PL Detail-Document.
Orexin Antagonist: Suvorexant(Belsomra®) Mechanism of action: Blocks wake-promoting neuropeptides orexin A
and B, which is thought to inhibit activation of the arousal system andsuppress wake drive
Improves sleep induction and maintenance
Onset: 30 minutes
Duration: approx. 7 hours
Requires minimum of 7 hours of planned sleep
Minimal ADEs; no rebound or withdrawal effects noted whendiscontinued
Cost: approx. $14 per tablet (for brand, not available generically;regardless of strength)
Lexicomp suvorexant monograph. Schroeck JL, et al. PL Detail-Document.
The material in this presentation is for informational and educational purposes only and is not a substitute for medical advice, diagnosis, or treatment provided by a qualified health care provider. All information contained in this presentation is protected by copyright and remains the property of ProCare HospiceCare. All rights are reserved.

7/10/2019
19
Antidepressants
Typically used when patient has comorbid depression, or when otheroptions have failed
Sedating d/t antihistamine, anticholinergic, serotonin, and/oradrenergic antagonism activities
Lack data from randomized trials re: use in primary insomnia (exceptdoxepin)
Schroeck JL, et al.
Antidepressants: Trazodone (Desyrel®) Off-label use for insomnia
Mechanism: Serotonin reuptake inhibitor/antagonist; 5HT2a receptorantagonist; also blocks histamine (H1) and alpha1-adrenergic receptors
Has low anticholinergic activity vs. doxepin
Improvement in total sleep time, sleep efficiency, sleep continuity,number of awakenings; prolongs slow-wave sleep (including stages 3 and4); prolongs REM latency without affecting the proportion of REM sleep
In Alzheimer’s patients: Improved total sleep time and nighttime percentageof sleep vs. placebo
More data on its efficacy for secondary insomnia (i.e. d/t depression) vs.primary insomnia
Onset: 30-60 minutes
Duration: Unclear; half-life prolonged in elderly
Dose can be titrated q3-4 days (d/t relatively short half-life)
Schroeck JL, et al. PL Detail-Document. Lexicomp trazodone monograph.
The material in this presentation is for informational and educational purposes only and is not a substitute for medical advice, diagnosis, or treatment provided by a qualified health care provider. All information contained in this presentation is protected by copyright and remains the property of ProCare HospiceCare. All rights are reserved.

7/10/2019
20
Antidepressants: Mirtazapine (Remeron®) Off-label use for insomnia
Mechanism: Central presynaptic alpha2-adrenergic antagonist effects increase therelease of norepinephrine and serotonin; potent antagonist of 5-HT2 and 5-HT3serotonin receptors and H1 histamine receptors; moderate alpha1-adrenergic andmuscarinic antagonist; also enhances noradrenergic neurotransmission whichincreases the synthesis of melatonin Has low anticholinergic activity vs. doxepin
Lower doses cause more sedation, can also increase appetite
Improves sleep-onset latency, sleep maintenance, and total sleep time (reducesnighttime awakenings)
Onset: Not available Steady state achieved after approx. 5 days of treatment
In one study: Improvements as early as 2 weeks after initiation
Increased risk of RLS
2019 Beers Criteria® Update: Use with caution in elderly, may exacerbate or causeSIADH or hyponatremia (monitor sodium levels when initiating or changing doses)
Schroeck JL, et al. PL Detail-Document. Lexicomp mirtazapine monograph. 2019 Beers Criteria® Update.
Tricyclic Antidepressants: Doxepin (Silenor®)
Silenor® (3-6mg dose) has FDA-approved indication for primary insomnia
Also available as Sinequan® (10mg and higher): FDA-approved indication fordepression, off-label use for insomnia and chronic urticaria
Mechanism: At low doses (3-6mg): Histamine antagonist (specifically H1);high selectivity for histamine receptors, and little to no effect onserotonin and adrenergic receptors
Anticholinergic side effects (at higher doses)
Improves sleep maintenance; increases total sleep time by approx. 30minutes
Onset of action: 30 minutes
Duration of effect: Unclear
2019 Beers Criteria® Update: Avoid doses higher than 6mg/day in theelderly; safety profile of doses <6mg/day comparable to placebo
Schroeck JL, et al. PL Detail-Document. Lexicomp doxepin monograph. 2019 Beers Criteria® Update.
The material in this presentation is for informational and educational purposes only and is not a substitute for medical advice, diagnosis, or treatment provided by a qualified health care provider. All information contained in this presentation is protected by copyright and remains the property of ProCare HospiceCare. All rights are reserved.

7/10/2019
21
Tricyclic Antidepressants: Amitriptyline(Elavil®) Off-label for insomnia
Mechanism: Inhibits reuptake of serotonin and/or norepinephrine in CNS
Onset: unclear
Duration: unclear
Limited studies re: efficacy for insomnia, especially in elderly population
No longer recommended for insomnia d/t availability of newer agents andmeds with fewer ADEs
Anticholinergic adverse effects, can cause orthostatic hypotension
Increased half-life and reduced clearance in elderly (increasing risk of ADEs)
2019 Beers Criteria® Update: Avoid in elderly
Bottom line… Not recommended for insomnia
Schroeck JL, et al. 2019 Beers Criteria® Update. LexiComp amitriptyline monograph.
Other Prescription Drugs: Antipsychotics E.g. haloperidol (Haldol®), quetiapine (Seroquel®), risperidone
(Risperdal®), olanzapine (Zyprexa®), ziprasidone (Geodon®)
Some typical (1st generation) antipsychotics are highly sedating (e.g.chlorpromazine, clozapine, thioridazine) – but haloperidol is about as sedatingas most atypical (2nd generation) antipsychotics
Olanzapine and quetiapine are the most sedating of the atypicals (and moresedating than haloperidol)
Mechanism: Sedating effects appear related to affinity for histamine H1and serotonin type 2A receptors in CNS (varies among the meds)
Often used in patients with insomnia –AND- behaviors, major depressivedisorder, or an organic brain syndrome
Very limited data re: use in insomnia alone
2019 Beers Criteria® Update: Avoid in elderly
General consensus: Don’t use for insomnia/sleep effects alone, asbenefits don’t outweigh the risksSchroeck JL, et al. Lexi-Drugs Comparison of Antipsychotic Adverse Effects [table]. Mystakidou K, et al. 2019 Beers Criteria® Update.
The material in this presentation is for informational and educational purposes only and is not a substitute for medical advice, diagnosis, or treatment provided by a qualified health care provider. All information contained in this presentation is protected by copyright and remains the property of ProCare HospiceCare. All rights are reserved.

7/10/2019
22
Other Prescription Drugs: Gabapentin(Neurontin®)
May be helpful for patients with insomnia –AND- restless legs syndrome(RLS) (off-label use) or chronic neuropathic pain
Mechanism: Structural analog of GABA, but does not bind to GABAA orGABAB receptors or appear to influence synthesis or uptake of GABA;interacts with presynaptic alpha2-delta1 subunit on voltage-gated calciumchannels, appears to modulate release of excitatory neurotransmitters
Drowsiness is common ADE
Renal dosing required
Not typically used for insomnia/sleep effects alone
Schroeck JL, et al. Lexicomp gabapentin monograph.
OTC Sleep Aids: Antihistamines Diphenhydramine (Benadryl®; also found in many “PM” products);
doxylamine
Mechanism: First-generation antihistamines (H1-receptor antagonists)
Can have anticholinergic ADEs: dry eyes/mouth, blurred vision, constipation,urinary retention, confusion/memory impairment, orthostatic hypotension,tachycardia
Can cause psychomotor impairment, dizziness, incoordination in elderly
Onset
Diphenhydramine: 30-60 minutes
Doxylamine: 30 minutes
2019 Beers Criteria® Update: Avoid in elderly
Limited evidence on safety and efficacy when used for insomnia
Tolerance can develop with regular use
Schroeck JL, et al. PL Detail-Document. Kryger M, Kryger E. 2019 Beers Criteria® Update.
The material in this presentation is for informational and educational purposes only and is not a substitute for medical advice, diagnosis, or treatment provided by a qualified health care provider. All information contained in this presentation is protected by copyright and remains the property of ProCare HospiceCare. All rights are reserved.

7/10/2019
23
OTC Herbal Supplements: Melatonin
Mechanism of action (endogenous): Hormone produced by the pinealgland, released at night; binds to MT1 and MT2 receptors in SCN, resultingin suppression of neuronal activity
Production is controlled by light -- inhibited by environmental light andstimulated by darkness. Duration of melatonin production varies throughoutthe year (shorter during the summer and longer during the winter).
Secretion starts at approx. 9pm; levels rise during evening hours, peak in themiddle of the night (2-3am), and remain low during the day
In elderly…
Peak melatonin levels tend to decrease with advanced age, d/t decreasedsecretion at night and altered hormone regulation (via renal/hepaticchanges, body composition changes) increasing risk for conditions relatedto circadian rhythms
Other possible causes of decreased endogenous melatonin levels:
Cancer, mood disorders, decreased renal function, medications
Schroeck JL, et al. Davis L. Natural Products Database melatonin monograph.
OTC Herbal Supplements: Melatonin, continued Melatonin supplements can mimic the function of endogenous melatonin
Evening administration: Advances circadian rhythm and induces sleep onset
Recommended dosing: Use lowest possible dose (maximum of 1-2mg inelderly; 3-5mg in non-elderly), given 1 hour before bedtime
Melatonin supplements increase endogenous melatonin in a dose-dependentmanner; 0.3mg dose produces supraphysiological levels in older adults; higherdoses can cause prolonged elevated melatonin levels and possiblydesensitization/loss of effectiveness, may regain effectiveness at lower doses
Avoid controlled-release forms in older adults
Conflicting results re: efficacy of melatonin supplementation in studies; isgenerally well tolerated; sedative effects can last for up to 7 hours, maycause residual daytime sedation
Schroeck JL, et al. Davis L. Kryger M, Kryger E. Natural Products Database melatonin monograph.
The material in this presentation is for informational and educational purposes only and is not a substitute for medical advice, diagnosis, or treatment provided by a qualified health care provider. All information contained in this presentation is protected by copyright and remains the property of ProCare HospiceCare. All rights are reserved.

7/10/2019
24
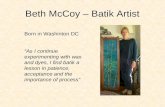
AASM 2017 Guideline for Pharmacologic Treatment of Chronic Insomnia in Adults (Summary of Recommendations)
Drug (Trial Dose) Sleep Onset Insomnia Sleep Maintenance Insomnia
temazepam (15mg) X X
triazolam (0.25mg) X
zolpidem (10mg) X X
zaleplon (5mg, 10mg) X
eszopiclone (2mg, 3mg) X X
ramelteon (8mg) X
doxepin (3mg, 6mg) X
suvorexant (10mg, 15/20mg, 20mg) X
Sateia MJ, et al.
This table is an excerpt of recommendations, does not include here drugs that are “notrecommended for either”
Guidelines are for general adult population (not hospice-specific); also note dosesstudied
AASM used the GRADE approach (Grades of Recommendation, Assessment, Development,and Evaluation) to assess the quality of evidence (i.e. strength of evidence in publisheddata) -- all of their recommendations have a “weak” GRADE strength.
American Geriatrics Society (AGS) Beers Criteria®
“Intent of Criteria: …The criteria are intended for use in adults 65years and older in all ambulatory, acute, and institutionalized settingsof care, except for the hospice and palliative care settings.[emphasis added] …The intention of the AGS Beers Criteria® is toimprove medication selection; educate clinicians and patients; reduceadverse drug events; and serve as a tool for evaluating quality ofcare, cost, and patterns of drug use of older adults. … the goal of the2019 update continues to be improving the care of older adults byreducing their exposure to PIMs [Potentially InappropriateMedications] that have an unfavorable balance of benefits and harmscompared with alternative treatment options. …The AGS BeersCriteria® are not meant to be applied in a punitive manner.Prescribing decisions are not always clear-cut, and clinicians mustconsider multiple factors, ….”2019 Beers Criteria® Update.
The material in this presentation is for informational and educational purposes only and is not a substitute for medical advice, diagnosis, or treatment provided by a qualified health care provider. All information contained in this presentation is protected by copyright and remains the property of ProCare HospiceCare. All rights are reserved.

7/10/2019
25
AGS Beers Criteria®: Drugs to Be Avoided (Summary)
Benzodiazepines (includes: estazolam, lorazepam, oxazepam,temazepam, triazolam, flurazepam, quazepam)
Elderly have increased sensitivity and decreased metabolism of long-actingagents; in general, all increase risk of cognitive impairment, delirium, falls,fractures, and motor vehicle crashes in older adults; may be appropriate forseizures, REM sleep behavior disorder, benzodiazepine or ethanolwithdrawal, severe GAD, periprocedural anesthesia
Non-BzRAs (“Z” drugs: zolpidem, zaleplon, eszopiclone)
ADEs similar to benzodiazepines in older adults (e.g. delirium, falls,fractures); increased ED visits/hospitalizations; motor vehicle crashes;minimal improvement in sleep latency and duration
2019 Beers Criteria® Update.
AGS Beers Criteria®: Drugs to Be Avoided (Summary),continued
Anticholinergics (diphenhydramine (PO), doxylamine)
Highly anticholinergic, clearance reduced with advanced age; use insituations such as acute treatment of severe allergic reaction may beappropriate
Antidepressants (doxepin >6mg/day; amitriptyline)
Highly anticholinergic, sedating, cause orthostatic hypotension; safetyprofile of low-dose doxepin (<6mg/day) is comparable to that of placebo
Antipsychotics, 1st and 2nd generation (haloperidol, quetiapine,risperidone, olanzapine, ziprasidone)
Avoid, except in schizophrenia or bipolar disorder, or for short-term use asantiemetic during chemotherapy; increased risk of CVA/stroke, greater rateof cognitive decline and mortality in dementia
2019 Beers Criteria® Update.
The material in this presentation is for informational and educational purposes only and is not a substitute for medical advice, diagnosis, or treatment provided by a qualified health care provider. All information contained in this presentation is protected by copyright and remains the property of ProCare HospiceCare. All rights are reserved.

7/10/2019
26
Quiz Question #1 M.A., 68-year-old female hospice patient with breast cancer and hypothyroidism;
reports insomnia – specifically difficulty getting to sleep, states she “can’t turn hermind off” when she lays down at night; she is worried about the relationship betweenher two daughters who are estranged from each other and what will happen to thefamily once she is gone; patient’s pain is very well controlled; prognosis is likelyapprox. 5-6 months; husband is primary caregiver and is with her 24/7, excellentmonitoring; she has not yet tried anything for insomnia.
Medications: morphine ER 15mg po BID; morphine 20mg/mL 5-10mg po q2h PRNpain/sob; prochlorperazine 5-10mg po q6h PRN n/v; senna-S 1 tab po BID;levothyroxine 50mcg po qam
Which of the following would be the BEST option(s) to consider at this time?
A) Ramelteon (Rozerem®)
B) Lorazepam
C) Gabapentin
D) Non-pharmacologic measures such as meeting with social worker and/or chaplain, worry-journaling, meditation, etc.
E) B and D
Quiz Question #1 M.A., 68-year-old female hospice patient with breast cancer, and hypothyroidism;
reports insomnia – specifically difficulty getting to sleep, states she “can’t turn hermind off” when she lays down at night; she is worried about the relationship betweenher two daughters who are estranged from each other and what will happen to thefamily once she is gone; patient’s pain is very well controlled; prognosis is likelyapprox. 5-6 months; husband is primary caregiver and is with her 24/7, excellentmonitoring; she has not yet tried anything for insomnia.
Medications: morphine ER 15mg po BID; morphine 20mg/mL 5-10mg po q2h PRNpain/sob; prochlorperazine 5-10mg po q6h PRN n/v; senna-S 1 tab po BID;levothyroxine 50mcg po qam
Which of the following would be the BEST option(s) to consider at this time?
A) Ramelteon (Rozerem®)
B) Lorazepam
C) Gabapentin
D) **Non-pharmacologic measures such as meeting with social worker and/or chaplain,worry-journaling, meditation, etc.**
E) B and D
The material in this presentation is for informational and educational purposes only and is not a substitute for medical advice, diagnosis, or treatment provided by a qualified health care provider. All information contained in this presentation is protected by copyright and remains the property of ProCare HospiceCare. All rights are reserved.

7/10/2019
27
Quiz Question #1 M.A., 68-year-old female hospice patient with breast cancer, and hypothyroidism;
reports insomnia – specifically difficulty getting to sleep, states she “can’t turn hermind off” when she lays down at night; she is worried about the relationship betweenher two daughters who are estranged from each other and what will happen to thefamily once she is gone; patient’s pain is very well controlled; prognosis is likelyapprox. 5-6 months; husband is primary caregiver and is with her 24/7, excellentmonitoring; she has not yet tried anything for insomnia.
Medications: morphine ER 15mg po BID; morphine 20mg/mL 5-10mg po q2h PRNpain/sob; prochlorperazine 5-10mg po q6h PRN n/v; senna-S 1 tab po BID;levothyroxine 50mcg po qam
Which of the following would be the BEST option(s) to consider at this time?
A) Ramelteon (Rozerem®)
B) Lorazepam
C) Gabapentin
D) **Non-pharmacologic measures such as meeting with social worker and/or chaplain,worry-journaling, meditation, etc.** --OR--
E) **B and D**
Quiz Question #2 J.K., 76-year-old male hospice patient with COPD and BPH; patient states that he
is having trouble sleeping at night, especially staying asleep; wife reports thatpatient seems sad and depressed lately; breathing and BPH symptoms are well-managed on current regimen and patient denies pain; patient does not havedementia; patient has not tried an antidepressant in the past; prognosis is approx.3 months.
Medications: albuterol/ipratropium neb 1 vial inh 4 times daily; albuterol neb0.083% 1 vial inh q4h PRN sob/wheezing; albuterol HFA inhaler 90mcg 2 puffs inhq4h PRN sob/wheezing, when away from home; prednisone 5mg po qam;morphine 20mg/mL 5mg po/sl q2h PRN pain/sob; lorazepam 0.5mg 1 tab po q4hPRN anxiety/sob; tamsulosin 0.4mg po once daily; senna-S 1 tab po BID PRNconstipation
Which of the following would be the BEST option(s) to consider at this time?
A) Melatonin
B) Trazodone
C) Zolpidem (Ambien®)
D) Non-pharmacologic measures such as meeting with a social worker and/or chaplain
E) B and D
The material in this presentation is for informational and educational purposes only and is not a substitute for medical advice, diagnosis, or treatment provided by a qualified health care provider. All information contained in this presentation is protected by copyright and remains the property of ProCare HospiceCare. All rights are reserved.

7/10/2019
28
Quiz Question #2 J.K., 76-year-old male hospice patient with COPD and BPH; patient states that he
is having trouble sleeping at night, especially staying asleep; wife reports thatpatient seems sad and depressed lately; breathing and BPH symptoms are well-managed on current regimen and patient denies pain; patient does not havedementia; patient has not tried an antidepressant in the past; prognosis is approx.3 months.
Medications: albuterol/ipratropium neb 1 vial inh 4 times daily; albuterol neb0.083% 1 vial inh q4h PRN sob/wheezing; albuterol HFA inhaler 90mcg 2 puffs inhq4h PRN sob/wheezing, when away from home; prednisone 5mg po qam;morphine 20mg/mL 5mg po/sl q2h PRN pain/sob; lorazepam 0.5mg 1 tab po q4hPRN anxiety/sob; tamsulosin 0.4mg po once daily; senna-S 1 tab po BID PRNconstipation
Which of the following would be the BEST option(s) to consider at this time?
A) Melatonin
B) Trazodone
C) Zolpidem (Ambien®)
D) Non-pharmacologic measures such as meeting with a social worker and/or chaplain
E) **B and D**
Quiz Question #3
R.P., 84-year-old male hospice patient with Parkinson’s disease and HTN; hasrecently developed overnight agitation/hallucinations, and as a result, sleeps verylittle at night, per caregiver; prognosis is unclear, but likely 1-2 months.
Medications: carbidopa/levodopa 25/100mg 1 tab po TID; morphine 20mg/mL 5mgpo/sl q4h PRN pain/sob; lorazepam 0.5mg 1 tab po q4h PRN anxiety/restlessness;metoprolol succinate 25mg 1 tab po once daily; senna-S 2 tabs po BID
Which of the following would be the BEST option(s) to try at this time?
A) Haloperidol scheduled every evening and PRN
B) Risperidone every evening
C) Quetiapine every evening
D) Temazepam every evening
E) Non-pharmacologic measures such as relaxation techniques, meeting with chaplainand/or social worker, CBT-I, etc.
F) C and E
The material in this presentation is for informational and educational purposes only and is not a substitute for medical advice, diagnosis, or treatment provided by a qualified health care provider. All information contained in this presentation is protected by copyright and remains the property of ProCare HospiceCare. All rights are reserved.

7/10/2019
29
Quiz Question #3
R.P., 84-year-old male hospice patient with Parkinson’s disease and HTN; hasrecently developed overnight agitation/hallucinations, and as a result, sleeps verylittle at night, per caregiver; prognosis is unclear, but likely 1-2 months.
Medications: carbidopa/levodopa 25/100mg 1 tab po TID; morphine 20mg/mL 5mgpo/sl q4h PRN pain/sob; lorazepam 0.5mg 1 tab po q4h PRN anxiety/restlessness;metoprolol succinate 25mg 1 tab po once daily; senna-S 2 tabs po BID
Which of the following would be the BEST option(s) to try at this time?
A) Haloperidol scheduled every evening and PRN
B) Risperidone every evening
C) **Quetiapine every evening**
D) Temazepam every evening
E) Non-pharmacologic measures such as relaxation techniques, meeting with chaplainand/or social worker, CBT-I, etc.
F) C and E
Key Points
Insomnia is often a result of another condition (e.g. pain, anxiety).Treat and/or resolve causes of insomnia first whenever possible,before starting an anti-insomnia medication.
Use non-pharmacologic measures whenever possible and appropriate
There is not a “one size fits all” anti-insomnia drug treatment; if thefirst option tried is ineffective, may need to adjust dose or switch to adifferent medication
Always use the lowest effective dose, monitor for adverse effects, andfrequently re-evaluate for effectiveness with any drug therapy
The material in this presentation is for informational and educational purposes only and is not a substitute for medical advice, diagnosis, or treatment provided by a qualified health care provider. All information contained in this presentation is protected by copyright and remains the property of ProCare HospiceCare. All rights are reserved.

7/10/2019
30
Questions?
Any additional questions: [email protected]
References Winter WC. The Sleep Solution: Why Your Sleep is Broken and How to Fix it. Berkley, Penguin Random House
LLC, New York. 2017.
Kryger M, Kryger E. What every pharmacist should know about sleep. ASCP Webinars; UAN: 0203-0000-18-076-H01-P. November 3, 2018.
Mystakidou K, Penangiotou I, Parpa E, Tsilika E. Sleep Disorders. Chapter in: Oxford Textbook of Palliative Medicine, 5th Edition; Cherny NI, Fallon MT, Kaasa S, Portenoy RK, Currow DC, Eds. Oxford University Press, UK. 2015. 457-66.
Dopp JM, Phillips BG. Sleep-Wake Disorders. Chapter in: Pharmacotherapy: A Pathophysiologic Approach, 10th Edition; DiPiro JT, et al, Eds. McGraw-Hill Education, New York. 2017. 1111-22.
Neubauer DN. Sleep problems in the elderly. Am Fam Physician. 1999 May 1; 59(9): 2551-8.
Roth T, Saffel D. Knowledge-based home study webcast; Activity No.: 0798-0000-18-204-H01. Challenges in Optimally Managing Insomnia in the Elderly. Release date: 12/27/2018. Available via FreeCE.com.
Drug monographs. Lexicomp Online, Hudson, Ohio: Wolters Kluwer Clinical Drug Information, Inc., © 2019; last accessed 6/25/2019.
Foral P, Knezevich J, Dewan N, Malesker M. Medication-induced sleep disturbances. The Consultant Pharmacist; June 2011; 26(5): 414-25.
Patel D, Steinberg J, Patel P. Insomnia in the elderly: A review. Journal of Clinical Sleep Medicine; June 15, 2018; 14(6): 1017-24.
Schroeck JL, et al. Review of safety and efficacy of sleep medications in older adults. Clinical Therapeutics. Nov 2016; 38(11): 2340-2372.
Mitchell MD, Gehrman P, Perlis M, Umscheid CA. Comparative effectiveness of cognitive behavioral therapy for insomnia: a systematic review. BMC Family Practice 2012 13:40.
The material in this presentation is for informational and educational purposes only and is not a substitute for medical advice, diagnosis, or treatment provided by a qualified health care provider. All information contained in this presentation is protected by copyright and remains the property of ProCare HospiceCare. All rights are reserved.
7/10/2019
31
References, continued Chung KF, et al. Sleep hygiene education as a treatment of insomnia: a systematic review and meta-
analysis. Fam Pract. 2018 Jul 23; 35(4): 365-375. [abstract]
Sateia MJ, Buysse DJ, Krystal AD, Neubauer DN, Heald JL. Clinical practice guideline for the pharmacologic treatment of chronic insomnia in adults: An American Academy of Sleep Medicine clinical practice guideline.Journal of Clinical Sleep Medicine. 2017; 13(2): 307-80.
PL Detail-Document, Comparison of Insomnia Treatments. Pharmacist’s Letter/Prescriber’s Letter. July 2014. Last modified January 2015.
2019 American Geriatrics Society Beers Criteria® Update Expert Panel. American Geriatrics Society 2019 Updated AGS Beers Criteria® for potentially inappropriate medication use in older adults. J Am Geriatr Soc 00:1-21, 2019. Available at: https://onlinelibrary.wiley.com/doi/epdf/10.1111/jgs.15767?referrer_access_token=nuwHd-eomXh0G4EfAX5qnIta6bR2k8jH0KrdpFOxC65t_FokpdxHvL7WaxkN527h7l3s9xxEMlD4211T518cxliTQ0jUZJvkCe39nbq3eDhQWopbDFzcvt3mr4h2_zLJKd88FJm52y49oOnFCvVuDA%3D%3D [last accessed 5/18/2019]
Brooks, Megan. FDA Adds Boxed Warning to Insomnia Drugs. Medscape. April 30, 2019.
Lunesta® (eszopiclone) prescribing information. Sunovion Pharmaceuticals Inc, Marlborough, MA, USA; 2014. Revised 5/2014.
Comparison of Antipsychotic Adverse Effects [table]. Lexicomp Online, Lexi-Drugs Online, Hudson, Ohio: Wolters Kluwer Clinical Drug Information, Inc., © 2019; last updated 3/26/2019. [accessed 5/4/2019]
Melatonin. Natural Products Database, via Lexicomp Online, Hudson, Ohio: Wolters Kluwer Clinical Drug Information, Inc., © 2019; last updated 4/19/2019. [accessed 5/15/2019]
Davis L. Melatonin: Shining some light on the hormone of darkness. ASCP Webinars; UAN: 0203-0000-18-022-H01-P. May 23, 2018.
The material in this presentation is for informational and educational purposes only and is not a substitute for medical advice, diagnosis, or treatment provided by a qualified health care provider. All information contained in this presentation is protected by copyright and remains the property of ProCare HospiceCare. All rights are reserved.