
What is the impact of water sanitation ... - BMJ Global Health · Hunter PR. What is the impact of...
14
1 Bouzid M, et al. BMJ Glob Health 2018;3:e000648. doi:10.1136/bmjgh-2017-000648 What is the impact of water sanitation and hygiene in healthcare facilities on care seeking behaviour and patient satisfaction? A systematic review of the evidence from low-income and middle- income countries Maha Bouzid, 1 Oliver Cumming, 2 Paul R Hunter 1 Research To cite: Bouzid M, Cumming O, Hunter PR. What is the impact of water sanitation and hygiene in healthcare facilities on care seeking behaviour and patient satisfaction? A systematic review of the evidence from low-income and middle-income countries. BMJ Glob Health 2018;3:e000648. doi:10.1136/ bmjgh-2017-000648 Handling editor Soumitra Bhuyan ► Additional material is published online only. To view please visit the journal online (http://dx.doi.org/10.1136/ bmjgh-2017-000648). Received 15 November 2017 Revised 22 February 2018 Accepted 15 March 2018 1 Norwich School of Medicine, University of East Anglia, Norwich, UK 2 Department of Disease Control, Faculty of Infectious and Tropical Diseases, London School of Hygiene and Tropical Medicine, London, UK Correspondence to Dr Maha Bouzid; [email protected] ABSTRACT Patient satisfaction with healthcare has clear implications on service use and health outcomes. Barriers to care seeking are complex and multiple and delays in seeking care are associated with significant morbidity and mortality. We sought to assess the relationship between water, sanitation and hygiene (WASH) provision in healthcare facilities (HCF) and patient satisfaction/care seeking behaviour in low-income and middle-income countries. Pubmed and Medline Ovid were searched using a combination of search terms. 984 papers were retrieved and only 21 had a WASH component warranting inclusion. WASH was not identified as a driver of patient satisfaction but poor WASH provision was associated with significant patient dissatisfaction with infrastructure and quality of care. However, this dissatisfaction was not sufficient to stop patients from seeking care in these poorly served facilities. With specific regard to maternal health services, poor WASH provision was the reason for women choosing home delivery, although providers’ attitudes and interpersonal behaviours were the main drivers of patient dissatisfaction with maternal health services. Patient satisfaction was mainly assessed via questionnaires and studies reported a high risk of courtesy bias, potentially leading to an overestimation of patient satisfaction. Patient satisfaction was also found to be significantly affected by expectation, which was strongly influenced by patients’ socioeconomic status and education. This systematic review also highlighted a paucity of research to describe and evaluate interventions to improve WASH conditions in HCF in low-income setting with a high burden of healthcare- associated infections. Our review suggests that improving WASH conditions will decrease patience dissatisfaction, which may increase care seeking behaviour and improve health outcomes but that more rigorous research is needed. INTRODUCTION The water, sanitation and hygiene (WASH) attributable burden of disease is large and concentrated within low-income and middle-income countries (LMIC). A total of 842 000 diarrhoeal disease deaths (of which, 361 000 occurred in children under 5 years old) were attributed to inadequate WASH in 145 countries. 1 Despite considerable progress in improving access to WASH services under the Millennium Development Goals (MDGs), a significant proportion of the world’s poor still lack access to safe WASH. 2 However, reporting for the MDGs focused on WASH access in the community. By contrast, there has been little exploration of the impact of inadequate WASH provision in healthcare facilities (HCF) in LMIC. In 2015, WHO and Key questions What is already known? ► A WHO/Unicef report (2015) highlighted the lack of adequate water, sanitation and hygiene (WASH) provision in many healthcare facilities (HCF) in low-income and middle-income countries (LMIC). ► Patient satisfaction and care seeking behaviour have been extensively used to monitor and improve the quality of care. ► The evidence on the contribution of poor WASH to patient dissatisfaction and care seeking behaviour is unclear. What are the new findings? ► This systematic review sought to assess the relationship between WASH in HCF and patient satisfaction/care seeking behaviour in LMIC. ► Our findings showed that WASH status was not the main driver of patient satisfaction as other factors were more significant to users. ► Nevertheless, poor WASH provision was associated with significant patient dissatisfaction and stopped women from seeking care at maternity services. ► This is the first systematic review to be published on this topic. on June 1, 2020 by guest. Protected by copyright. http://gh.bmj.com/ BMJ Glob Health: first published as 10.1136/bmjgh-2017-000648 on 9 May 2018. Downloaded from
Transcript of What is the impact of water sanitation ... - BMJ Global Health · Hunter PR. What is the impact of...

1Bouzid M, et al. BMJ Glob Health 2018;3:e000648. doi:10.1136/bmjgh-2017-000648
What is the impact of water sanitation and hygiene in healthcare facilities on care seeking behaviour and patient satisfaction? A systematic review of the evidence from low-income and middle-income countries
Maha Bouzid,1 Oliver Cumming,2 Paul R Hunter1
Research
To cite: Bouzid M, Cumming O, Hunter PR. What is the impact of water sanitation and hygiene in healthcare facilities on care seeking behaviour and patient satisfaction? A systematic review of the evidence from low-income and middle-income countries. BMJ Glob Health 2018;3:e000648. doi:10.1136/bmjgh-2017-000648
Handling editor Soumitra Bhuyan
► Additional material is published online only. To view please visit the journal online (http:// dx. doi. org/ 10. 1136/ bmjgh- 2017- 000648).
Received 15 November 2017Revised 22 February 2018Accepted 15 March 2018
1Norwich School of Medicine, University of East Anglia, Norwich, UK2Department of Disease Control, Faculty of Infectious and Tropical Diseases, London School of Hygiene and Tropical Medicine, London, UK
Correspondence toDr Maha Bouzid; M. Bouzid@ uea. ac. uk
AbsTrACTPatient satisfaction with healthcare has clear implications on service use and health outcomes. Barriers to care seeking are complex and multiple and delays in seeking care are associated with significant morbidity and mortality. We sought to assess the relationship between water, sanitation and hygiene (WASH) provision in healthcare facilities (HCF) and patient satisfaction/care seeking behaviour in low-income and middle-income countries. Pubmed and Medline Ovid were searched using a combination of search terms. 984 papers were retrieved and only 21 had a WASH component warranting inclusion. WASH was not identified as a driver of patient satisfaction but poor WASH provision was associated with significant patient dissatisfaction with infrastructure and quality of care. However, this dissatisfaction was not sufficient to stop patients from seeking care in these poorly served facilities. With specific regard to maternal health services, poor WASH provision was the reason for women choosing home delivery, although providers’ attitudes and interpersonal behaviours were the main drivers of patient dissatisfaction with maternal health services. Patient satisfaction was mainly assessed via questionnaires and studies reported a high risk of courtesy bias, potentially leading to an overestimation of patient satisfaction. Patient satisfaction was also found to be significantly affected by expectation, which was strongly influenced by patients’ socioeconomic status and education. This systematic review also highlighted a paucity of research to describe and evaluate interventions to improve WASH conditions in HCF in low-income setting with a high burden of healthcare-associated infections. Our review suggests that improving WASH conditions will decrease patience dissatisfaction, which may increase care seeking behaviour and improve health outcomes but that more rigorous research is needed.
InTroduCTIonThe water, sanitation and hygiene (WASH) attributable burden of disease is large and concentrated within low-income and middle-income countries (LMIC). A total of 842 000 diarrhoeal disease deaths (of which,
361 000 occurred in children under 5 years old) were attributed to inadequate WASH in 145 countries.1 Despite considerable progress in improving access to WASH services under the Millennium Development Goals (MDGs), a significant proportion of the world’s poor still lack access to safe WASH.2 However, reporting for the MDGs focused on WASH access in the community. By contrast, there has been little exploration of the impact of inadequate WASH provision in healthcare facilities (HCF) in LMIC. In 2015, WHO and
Key questions
What is already known? ► A WHO/Unicef report (2015) highlighted the lack of adequate water, sanitation and hygiene (WASH) provision in many healthcare facilities (HCF) in low-income and middle-income countries (LMIC).
► Patient satisfaction and care seeking behaviour have been extensively used to monitor and improve the quality of care.
► The evidence on the contribution of poor WASH to patient dissatisfaction and care seeking behaviour is unclear.
What are the new findings? ► This systematic review sought to assess the relationship between WASH in HCF and patient satisfaction/care seeking behaviour in LMIC.
► Our findings showed that WASH status was not the main driver of patient satisfaction as other factors were more significant to users.
► Nevertheless, poor WASH provision was associated with significant patient dissatisfaction and stopped women from seeking care at maternity services.
► This is the first systematic review to be published on this topic.
on June 1, 2020 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2017-000648 on 9 May 2018. D
ownloaded from

2 Bouzid M, et al. BMJ Glob Health 2018;3:e000648. doi:10.1136/bmjgh-2017-000648
BMJ Global Health
Unicef assessed WASH status in 66 101 HCF in 54 LMIC.3 This assessment showed that 38% of facilities lacked access to water, 19% had no improved sanitation and 35% had no soap and water facilities. The issue of lack of WASH in HCF is of paramount importance because vulnerable populations are over-represented in these settings and the risk of infection and death is heightened. There is a growing awareness about this issue at a national and inter-national level and an intergovernmental commitment to address this inequity. Indeed, progress on WASH provi-sion in healthcare settings is currently being monitored as part of the Sustainable Development Goals (SDGs).4–6
Healthcare-associated infections (HCAI) are a major challenge in LMIC, where it has been estimated that the risk is 2–20 times higher than in developed countries.7 The highest rates of HCAI have been reported from the Eastern Mediterranean and South East Asia regions (11.8% and 10%, respectively) but this is an under-estimation due to poor recording and lack of patient follow-up.7 As most HCAI are transmitted via the hands of healthcare workers through direct contact or environ-mental contamination, hand washing remains the single most important preventive strategy.7 8 The importance of WASH in healthcare settings was established long ago by the work of Alexander Gordon9 and Ignaz Semmelweis10 with regard to puerperal fever in the 18th and 19th centu-ries and more recently with regard to HCAI outbreaks where unsafe water or hygiene have been implicated.11–14 In contrast to high-income countries, there is relatively little evidence on the burden of HCAI in LMIC. A recent systematic review estimated that HCAI prevalence in LMIC was 15.5 per 100 patients, compared with 7.1 and 4.5 per 100 patients, in Europe and USA, respectively.15 It is plausible that much of this excess is due to inadequate WASH. However, the disease burden associated with inadequate WASH provision is likely greater than the HCAI burden alone. Indeed, inadequate WASH could have large impacts on health outcomes through its influ-ence on patient satisfaction, care seeking behaviour and staff morale.
The barriers to care seeking are characterised using the three delays model developed by Thaddeus and Maine16
comprising: delays in deciding to seek care (primary delay), delays in reaching the health facility (secondary delay) and delays in receiving quality care once at the health facility (tertiary delay).17 Delays in receiving care have been estimated to be responsible for 30% newborn deaths in Uganda,17 45% of child deaths from diarrhoea and acute respiratory infections in Mexico18 and an increased odds of intrauterine fetal death of 6.6 (95% CI 1.6 to 26.3) for over an hour delays among Women in Afghanistan.19
Care seeking barriers are multiple and include care-takers’ failure to identify early danger signs that should trigger appropriate care seeking behaviour, cost (espe-cially for medication), distance to the facility, imped-iments related to weather or social unrest, lack of supervision for other children at home, lack of trans-port and, particularly relevant to this review, dissatisfac-tion with the quality of care.20 Afsana and colleagues21 consider that barriers to using hospital care are mainly related to care quality, especially for maternity services (often inadequate, unaffordable, insufficiently staffed and lacking medically trained professionals). Patient satisfaction is a commonly used indicator of health-care quality and was shown to affect service use, clinical outcomes and patient retention.22 It is considered a reli-able measure to understand patients’ needs and to make strategic decisions to improve care quality.23 However, no standardised system exists and a wide range of patient satisfaction indicators have been used as highlighted in a recent systematic review.23 The aim of this systematic review was to assess the impact of poor WASH provision in HCF in LMIC on two relevant indicators of healthcare quality: patient satisfaction and care seeking behaviour.
MeTHodsThe review methods are reported in accordance with the ‘Preferred Reporting Items for Systematic Reviews and Meta-Analyses’ (PRISMA)24 (checklist: online supple-mentary file 1).
search strategy and inclusion criteriaPubmed and Medline Ovid were searched in March 2016 for articles published in English after the year 2000 using the search terms outlined in table 1. A combination of specific and broad search terms was used in order to retrieve all relevant papers. ‘Developing countries’ was included as a search term in two out of five searches so as not to exclude relevant studies. LMIC were classified based on income level as defined by the World Bank data. No restrictions on study design and duration were applied. Reference lists were manually scanned for addi-tional relevant papers, which were included if eligible. Papers that had no WASH component were excluded.
data extraction and analysisRelevant data were extracted from all included papers using a standardised form. These data were: geographic
Key questions
What do the new findings imply? ► Inadequate WASH provision in HCF in LMIC may increase the risk of healthcare-associated infections (HCAI).
► Beyond the HCAI burden, poor WASH provision may increase patient dissatisfaction and limit care seeking behaviour, leading to adverse health outcomes.
► Improving WASH provision in HCF should be prioritised as a means of addressing HCAI but also to address patient satisfaction and encourage timely care seeking.
► Global best practice guidelines combined with concerted action at the national policy level would support progress in ensuring adequate WASH provision in HCF in LMIC.
on June 1, 2020 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2017-000648 on 9 May 2018. D
ownloaded from
Bouzid M, et al. BMJ Glob Health 2018;3:e000648. doi:10.1136/bmjgh-2017-000648 3
BMJ Global Health
location, type of study, type of healthcare facility, inter-vention (if any) and main findings. All quantitative and qualitative findings were recorded. Data were summa-rised narratively and no meta-analysis was conducted because of the heterogeneity between studies and use of different indicators of patient satisfaction.
resulTsThis systematic review assessed the effect of WASH in HCF on two quality of care outcomes: patient satisfaction and care seeking behaviour. Although WASH was rarely the primary focus of the included studies, all included some assessment of WASH conditions in HCF and their impact on patient satisfaction and/or care seeking behav-iour.
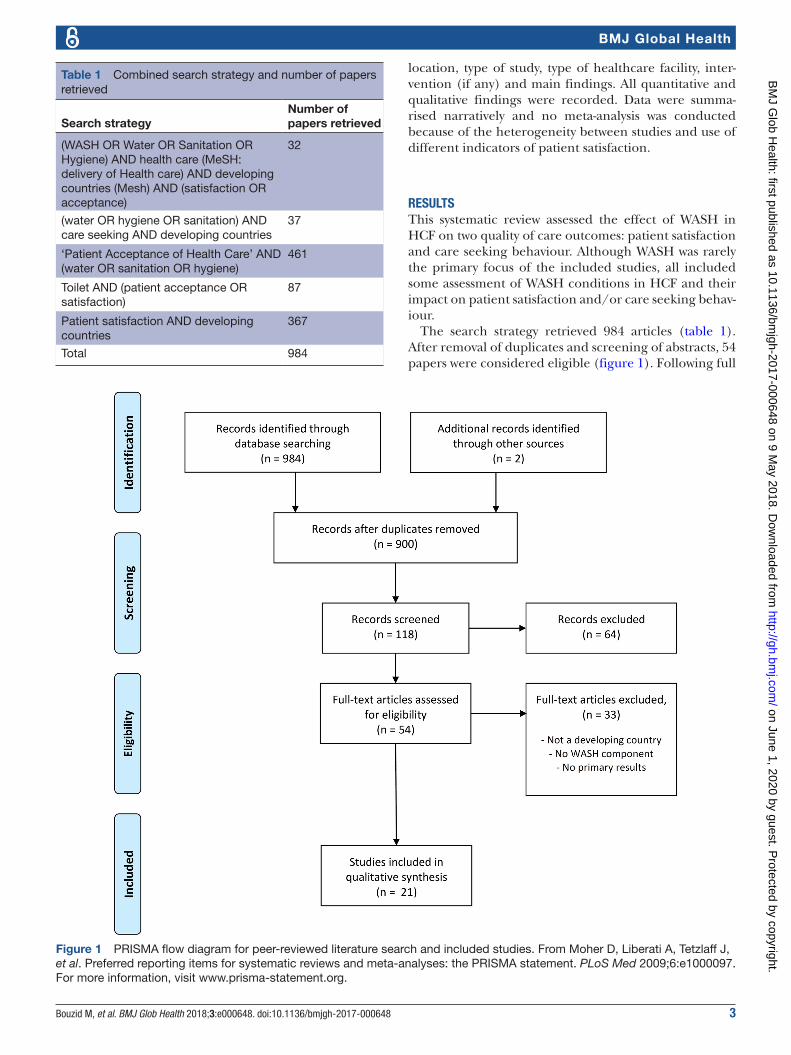
The search strategy retrieved 984 articles (table 1). After removal of duplicates and screening of abstracts, 54 papers were considered eligible (figure 1). Following full
Table 1 Combined search strategy and number of papers retrieved
Search strategyNumber of papers retrieved
(WASH OR Water OR Sanitation OR Hygiene) AND health care (MeSH: delivery of Health care) AND developing countries (Mesh) AND (satisfaction OR acceptance)
32
(water OR hygiene OR sanitation) AND care seeking AND developing countries
37
‘Patient Acceptance of Health Care’ AND (water OR sanitation OR hygiene)
461
Toilet AND (patient acceptance OR satisfaction)
87
Patient satisfaction AND developing countries
367
Total 984
Figure 1 PRISMA flow diagram for peer-reviewed literature search and included studies. From Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 2009;6:e1000097. For more information, visit www.prisma-statement.org.
on June 1, 2020 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2017-000648 on 9 May 2018. D
ownloaded from

4 Bouzid M, et al. BMJ Glob Health 2018;3:e000648. doi:10.1136/bmjgh-2017-000648
BMJ Global Health
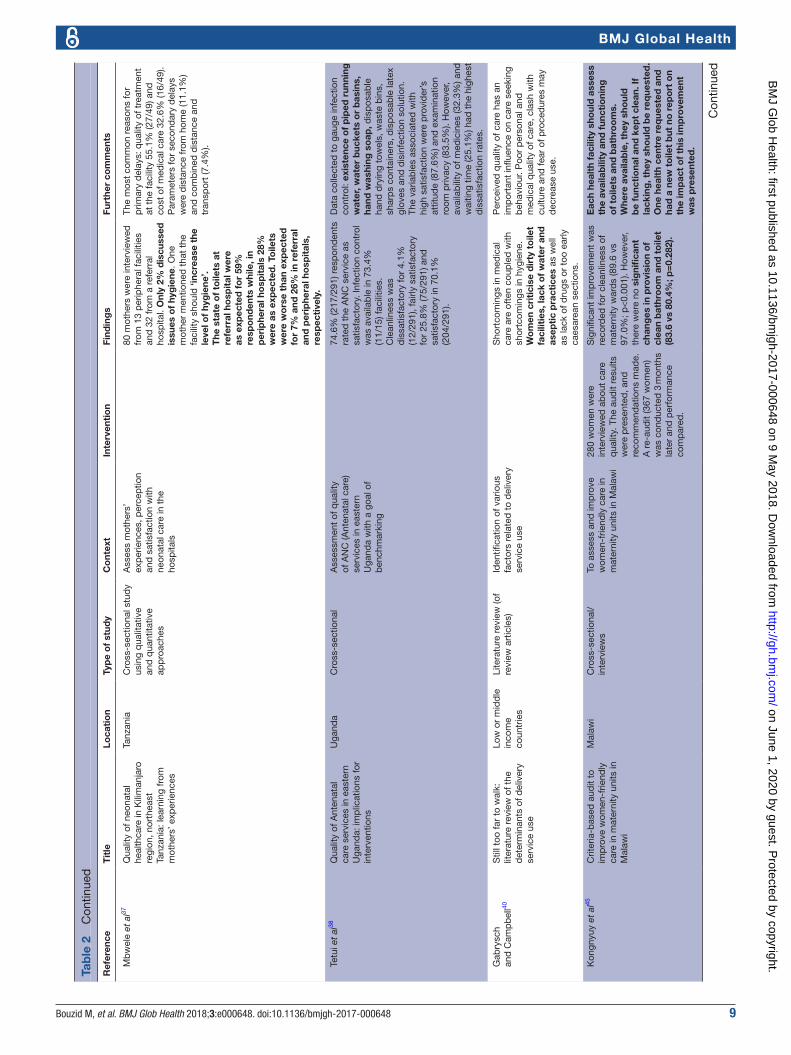
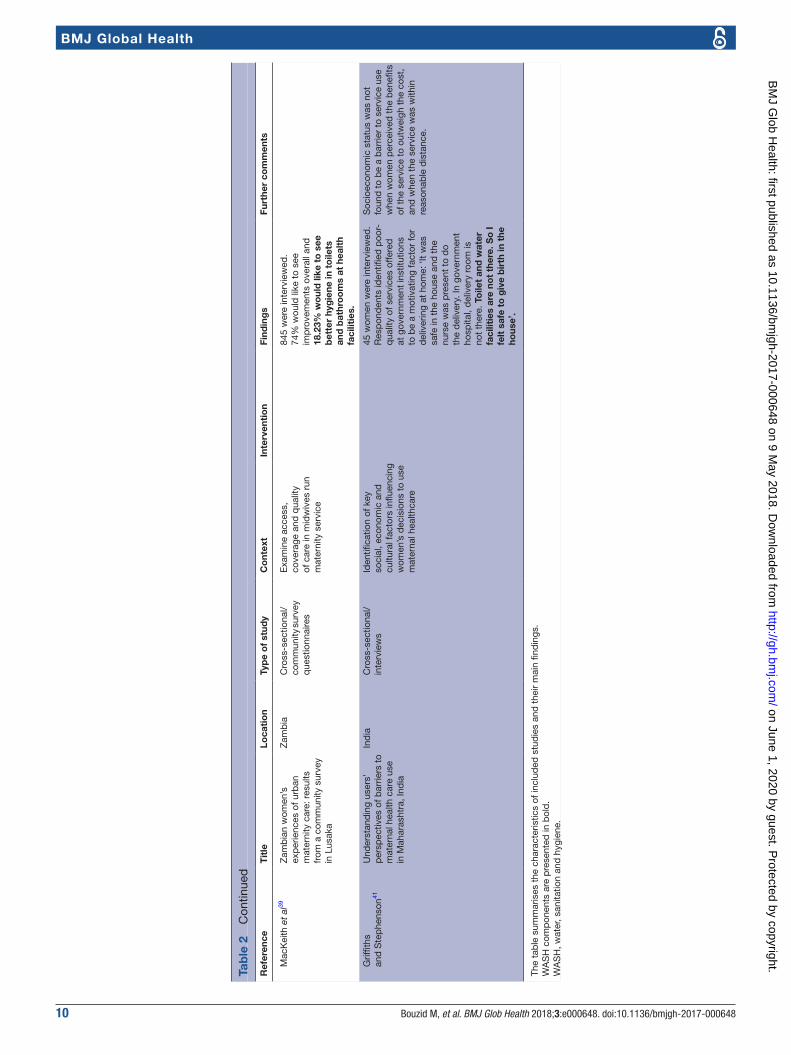
text scanning, only 21 papers were found to have a WASH component and were therefore included. The details of the papers and extracted data are presented in table 2. Included papers covered various countries, settings and healthcare delivery systems. There were studies from India (n=4), Uganda (3), Ethiopia (2), Nigeria (2), Tanzania (2), Kenya (1), South Africa (1), Malawi (1), Burkina Faso (1), Madagascar (1) and Zambia (1). All but three studies were cross-sectional (18/21), with one case control study, two review studies and one systematic review.
The level of satisfaction with WASH provision was reported in most studies. However, some studies reported on composite indicators of patient satisfaction and these were also noted. The papers were categorised according to the type of healthcare system, in particular, find-ings for maternity services were presented separately. Additionally, three papers investigated improvement interventions.
WAsH in HCF other than maternity servicesSeveral papers reported patient dissatisfaction rates with WASH in non-maternal health service. Woldeyohanes and colleagues assessed patient satisfaction with in-patient services in Ethiopia and reported 81.5% were dissatisfied with toilet cleanliness (table 2).25 A study in antiretroviral treatment clinic in Ethiopia showed a lower, but signifi-cant, dissatisfaction with toilet cleanliness (35.3%).26 The authors highlighted the importance of maintaining good hygiene levels, especially for patients with HIV/AIDS. Ezegwui and colleagues investigated patients’ satisfaction with eye care hospital in Nigeria and found that 71.7% of patients were dissatisfied with toilet facilities (only one toilet for patients and no running tap water).27 A study of rural healthcare system in India highlighted the link between poor WASH provision and patient dissatisfac-tion, with 50% respondents reporting that in surveyed government hospitals toilets are either ‘not at all usable’ or ‘dirty needed cleaning’.28 In addition, 3% of health facilities did not have toilets and drinking water was avail-able in only 55% of hospitals. The authors concluded that provision of clean toilets with privacy and safe drinking water would improve client satisfaction.28 While all these studies reported low patient satisfaction with WASH provision, a study in an eye care hospital in India reported high patient satisfaction with toilets (83.2%), water facilities (99.4%) and cleanliness (99.4%).29 Indeed, no respondent judged these as poor. However, 16.9% did not answer the toilet question. It is unclear if WASH provision was adequate in the HCF investigated as the paper was not focused on WASH, thus this informa-tion was not provided.
Khamis and colleagues investigated patient satisfac-tion with quality of care in an outpatient department in Tanzania using perception and expectation questions and calculating mean gap score between the two compo-nents.30 The study reported high overall dissatisfaction with quality of care, with a mean gap score of −2.88.30 The
mean gap score was −0.5 and −0.67 for general cleanliness and sufficient chairs and toilets, respectively (table 2), showing a moderate level of dissatisfaction.30
Mohammed and colleagues assessed the responsiveness of healthcare services for insured patients in Nigeria.31 One of the responsiveness domains was quality of facilities, which included provision of clean toilets in the hospital. Only 42.8% of users were satisfied with the quality of facilities and low-income users reported better quality of services than high-income users.31 Westaway and colleagues investigated interpersonal and organisational dimensions of patient satis-faction in a diabetic clinic for black patients in South Africa and found that the most important items for satisfaction were availability of a seat and a toilet in the waiting area and cleanliness.32
In a study investigating quality of care and contraceptive use in Kenya, 78.5% of facilities had running water; however, facility infrastructure and patient satisfaction indicators were not associated with contraceptive use.33 The cost of service and toilet facilities were the main areas of dissatisfaction.
Glick investigated the reliability of exit surveys frequently used to assess patient satisfaction.34 The respondents’ opin-ions were collected and answers were compared between exit and household surveys. Courtesy bias was found to influence respondents’ answers resulting in overestimates of patient satisfaction from exit surveys. This bias was stronger for subjective questions such as treatment by staff and consultation quality compared with objective questions such as facility conditions.34
WAsH in maternity servicesNine out of 21 studies focused on WASH conditions specif-ically around maternal health services, covering antenatal, delivery and postnatal care. Srivastava and colleagues conducted a systematic review investigating determinants of women’s satisfaction with maternal healthcare in devel-oping countries and covered all three dimensions: struc-ture, process and outcome.35 A good physical environment was found to be associated with a positive assessment of the health facility. In Bangladesh, when availability of services (a composite of waiting area and time, drinking water and clean toilet) was rated good, mothers were more satisfied with care quality.35 Cleanliness and maintenance of hygiene were also significant determinants of satisfaction in Bang-ladesh, Gambia, Thailand, India and Iran. Interpersonal behaviour, specifically provider courtesy and non-abuse, were the most widely reported determinants of women satisfaction.35 However, other factors influenced perceived maternal satisfaction including access, cost, socioeconomic status and reproductive history.35
Steinmann and colleagues assessed women’s satisfac-tion with latrines and hand washing stations in rural India and their impact on care seeking behaviour.36 They reported significant discrepancies between public and private health facilities. The average number of latrines per HCF was 2.4 (1.3 in public and 3.5 in private facil-ities). One healthcare centre had no latrine and dedi-cated latrines for woman were rarely available.36 The
on June 1, 2020 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2017-000648 on 9 May 2018. D
ownloaded from

Bouzid M, et al. BMJ Glob Health 2018;3:e000648. doi:10.1136/bmjgh-2017-000648 5
BMJ Global Health
Tab
le 2
Im
pac
t of
WA
SH
in h
ealth
care
faci
litie
s on
pat
ient
sat
isfa
ctio
n an
d c
are
seek
ing
beh
avio
ur
Ref
eren
ceT
itle
Loca
tio
nTy
pe
of
stud
yC
ont
ext
Inte
rven
tio
nFi
ndin
gs
Furt
her
com
men
ts
Wat
er a
nd s
anit
atio
n
W
old
eyoh
anes
et
al25
Per
ceiv
ed p
atie
nt
satis
fact
ion
with
in-
pat
ient
ser
vice
s at
Jim
ma
Uni
vers
ity S
pec
ializ
ed
Hos
pita
l, S
outh
wes
t E
thio
pia
Eth
iop
iaC
ross
-sec
tiona
lTh
is s
tud
y ai
ms
to
mea
sure
and
des
crib
e th
e le
vel o
f pat
ient
sa
tisfa
ctio
n w
ithin
in
-pat
ient
hea
lthca
re
serv
ices
Toile
t cl
eanl
ines
s: 1
8.5%
(3
5/18
9) w
ere
sati
sfied
w
hile
81.
5% (1
54/1
89)
wer
e d
issa
tisfi
ed. 7
6.6%
(1
45/1
89) w
ere
satis
fied
with
cl
eanl
ines
s of
the
war
d.
Res
earc
h cl
early
iden
tified
a li
nk
bet
wee
n p
atie
nt o
utco
mes
and
p
atie
nt s
atis
fact
ion
scor
es.
Te
ssem
a an
d A
dna
e26A
sses
smen
t of
an
tiret
rovi
ral t
reat
men
t (A
RT)
car
e se
rvic
e p
rovi
sion
in T
igra
y R
egio
n he
alth
cen
ters
, Nor
th
Eth
iop
ia
Eth
iop
iaC
ross
-sec
tiona
lP
erce
ived
leve
ls o
f clie
nts’
sa
tisfa
ctio
n w
ith h
ealth
se
rvic
es a
t A
RT
clin
ic le
vel
in h
ealth
cen
tres
Hig
h sc
ores
of s
atis
fact
ion
wer
e re
por
ted
for
cour
tesy
an
d r
esp
ect
95.8
0%
(684
/714
) and
priv
acy
93.2
8%
(666
/714
).A
cces
s an
d c
lean
lines
s to
la
trin
es w
ere
not
alw
ays
asse
ssed
. To
ilet
clea
nlin
ess
was
uns
atis
fact
ory
fo
r 35
.32%
(243
/688
).
Ad
just
ed O
R fo
r sa
tisfa
ctio
n w
as
2.22
(95%
CI 1
.62
to 6
.32)
fo
r to
ilet
clea
nlin
ess.
Mea
sure
s su
ch a
s in
crea
sing
acc
ess
to A
RT
serv
ice,
av
ailin
g cl
ean
toile
t an
d A
RT
dru
gs m
ay fu
rthe
r in
crea
se c
lient
sa
tisfa
ctio
n.C
lean
to
ilets
are
req
uire
d
esp
ecia
lly f
or
HIV
/AID
S p
atie
nts
to p
reve
nt o
pp
ort
unis
tic
and
no
n-o
pp
ort
unis
tic
coin
fect
ions
.
Tu
mlin
son
et a
l33Q
ualit
y of
car
e an
d
cont
race
ptiv
e us
e in
ur
ban
Ken
ya
Ken
yaC
ross
-sec
tiona
lTh
e st
udy
hyp
othe
sis
is t
hat
poo
r q
ualit
y of
fa
mily
pla
nnin
g se
rvic
e p
rovi
sion
is a
bar
rier
to
cont
race
ptiv
e us
e
78.5
% o
f fa
cilit
ies
(204
/260
) ha
ve r
unni
ng w
ater
.Fa
cilit
y in
fras
truc
ture
and
mos
t as
pec
ts o
f clie
nt s
atis
fact
ion—
incl
udin
g p
rivac
y is
sues
, am
ount
of
info
rmat
ion
give
n, w
aitin
g tim
e an
d
over
all s
atis
fact
ion—
wer
e un
rela
ted
to
con
trac
eptiv
e us
e.
G
aluk
and
e et
al43
Dev
elop
ing
hosp
ital
accr
edita
tion
stan
dar
ds
in
Uga
nda
Uga
nda
Cro
ss-s
ectio
nal
Acc
red
itatio
n is
not
wel
l es
tab
lishe
d in
mos
t d
evel
opin
g co
untr
ies
for
seve
ral r
easo
ns, i
nclu
din
g in
suffi
cien
t in
cent
ives
, in
suffi
cien
t tr
aini
ng a
nd a
sh
orta
ge o
f hum
an a
nd
mat
eria
l res
ourc
es
Sel
f-as
sess
men
t ho
spita
l acc
red
itatio
n to
ol d
evel
oped
for
a re
sour
ce-l
imite
d c
onte
xt.
Am
ong
accr
edita
tion
item
s (1
) phy
sica
l inf
rast
ruct
ure
and
(2) i
nfec
tion
cont
rol
and
was
te m
anag
emen
t ar
e re
leva
nt t
o W
AS
H. 2
7.5%
(1
1/40
) hos
pita
ls w
ere
not
trac
king
infe
ctio
n ra
tes
and
32
.5%
(13/
40) h
ad fu
nctio
nal
ster
ilisa
tion
equi
pm
ent.
Goo
d p
erfo
rman
ce w
as m
easu
red
in
ava
ilab
ility
of e
qui
pm
ent
and
ru
nnin
g w
ater
, 24
hour
s st
aff
calls
sys
tem
s, c
linic
al g
uid
elin
es
and
was
te s
egre
gatio
n. P
oor
per
form
ance
was
mea
sure
d in
ca
re fo
r th
e vu
lner
able
, sta
ff liv
ing
qua
rter
s, p
hysi
cian
per
form
ance
re
view
s, p
atie
nt s
atis
fact
ion
surv
eys
and
ste
rilis
ing
equi
pm
ent.
O
kwar
o et
al44
Cha
lleng
ing
logi
cs o
f co
mp
lex
inte
rven
tion
tria
ls: c
omm
unity
p
ersp
ectiv
es o
f a
heal
th c
are
imp
rove
men
t in
terv
entio
n in
rur
al
Uga
nda
Uga
nda
Cro
ss-s
ectio
nal
Att
ract
pat
ient
s to
hea
lth
cent
res
thro
ugh
imp
rove
d
serv
ices
and
att
itud
es
of s
taff
and
bet
ter
man
agem
ent
of fe
vers
The
inte
rven
tion
aim
s to
enh
ance
qua
lity
of
care
at
pub
lic h
ealth
ce
ntre
s an
d b
y ex
tens
ion
imp
rove
mal
aria
-rel
ated
he
alth
ind
icat
ors
in
com
mun
ity c
hild
ren
Man
y he
alth
cen
tres
la
cked
run
ning
wat
er a
nd
elec
tric
ity.
Imp
rove
men
ts in
an
timal
aria
l dru
g av
aila
bili
ty
wer
e no
ted
but
com
mun
ity
mem
ber
s w
ere
dis
app
oint
ed
with
the
qua
lity
of c
are
rece
ived
.P
atie
nts
cont
inue
d t
o se
ek
care
at
heal
th c
entr
es t
hey
cons
ider
ed in
adeq
uate
.
The
inte
rven
tion
targ
eted
mal
aria
co
ntro
l to
the
excl
usio
n of
oth
er
dis
ease
s or
bas
ic in
fras
truc
ture
su
ch a
s in
-pat
ient
fac
iliti
es o
r cl
ean
wat
er.
Req
uest
s b
y p
atie
nts
to in
crea
se t
he
num
ber
of h
ealth
wor
kers
, exp
and
b
uild
ings
and
sp
ace
with
in fa
cilit
ies,
p
rovi
de
clea
n w
ater
and
ele
ctric
ity,
in-p
atie
nt s
ervi
ces,
and
cle
an
toile
ts w
ere
rep
orte
d.
E
zegw
ui e
t al
27P
atie
nts’
sat
isfa
ctio
n w
ith
eye
care
ser
vice
s in
a
Nig
eria
n te
achi
ng h
osp
ital
Nig
eria
Cro
ss–s
ectio
nal
Eva
luat
e p
atie
nts’
sa
tisfa
ctio
n w
ith t
he c
are
rece
ived
71.7
% (2
20/3
07) w
ere
not
sati
sfied
wit
h to
ilet
faci
litie
s. T
here
is o
nly
one
to
ilet
for
pat
ient
s an
d t
here
is
no
run
ning
tap
.
The
mai
n ar
eas
of d
issa
tisfa
ctio
n w
ere
the
cost
of s
ervi
ce a
nd t
oile
t fa
cilit
ies.
Con
tinue
d
on June 1, 2020 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2017-000648 on 9 May 2018. D
ownloaded from

6 Bouzid M, et al. BMJ Glob Health 2018;3:e000648. doi:10.1136/bmjgh-2017-000648
BMJ Global Health
Ref
eren
ceT
itle
Loca
tio
nTy
pe
of
stud
yC
ont
ext
Inte
rven
tio
nFi
ndin
gs
Furt
her
com
men
ts
K
ham
is a
nd N
jau30
Pat
ient
s’ le
vel o
f sa
tisfa
ctio
n on
qua
lity
of h
ealth
car
e at
M
wan
anya
mal
a ho
spita
l in
Dar
es
Sal
aam
, Ta
nzan
ia
Tanz
ania
Cro
ss-s
ectio
nal
Det
erm
ine
pat
ient
s’
leve
l of s
atis
fact
ion
on
the
qua
lity
of h
ealth
care
d
eliv
ered
at
the
out-
pat
ient
dep
artm
ent
422
pat
ient
s w
ere
enro
lled
. M
ean
gap
sco
re w
as
(−2.
88±
3.1)
ind
icat
ing
over
all
dis
satis
fact
ion
with
the
q
ualit
y of
car
e.R
esp
ond
ents
wer
e d
issa
tisfie
d w
ith g
ener
al
clea
nlin
ess
(−0.
50; p
<0.
001)
, an
d s
uffi
cien
t ch
airs
and
to
ilets
(−0.
67; p
<0.
001)
.
The
que
stio
nnai
re is
div
ided
into
fiv
e d
imen
sion
s (ta
ngib
les,
rel
iab
ility
, re
spon
sive
ness
, ass
uran
ce a
nd
emp
athy
) to
det
erm
ine
pat
ient
s’
leve
l of s
atis
fact
ion.
The
mea
n ga
p
scor
e is
cal
cula
ted
as
the
diff
eren
ce
bet
wee
n m
ean
per
cep
tion
scor
e an
d m
ean
exp
ecta
tion
scor
e.
M
oham
med
et
al31
Ass
essi
ng r
esp
onsi
vene
ss
of h
ealth
car
e se
rvic
es
with
in a
hea
lth in
sura
nce
sche
me
in N
iger
ia: u
sers
’ p
ersp
ectiv
es
Nig
eria
Ret
rosp
ectiv
e, c
ross
-se
ctio
nal s
urve
yIn
sure
d u
sers
’ p
ersp
ectiv
es o
f the
ir he
alth
care
ser
vice
s’
resp
onsi
vene
ss
42.8
% (3
41/7
96) o
f use
rs
wer
e sa
tisfie
d w
ith t
he q
ualit
y of
faci
litie
s.Th
is in
clud
ed h
avin
g en
ough
sp
ace,
sea
ting
pla
ces
and
fr
esh
air
in r
oom
s an
d w
ard
s as
wel
l as
a cl
ean
faci
lity
and
cl
ean
toile
ts in
the
ho
spit
al.
Low
-inc
ome
insu
red
use
rs
rep
orte
d b
ette
r q
ualit
y of
fa
cilit
ies
than
hig
h-in
com
e us
ers
(p<
0.00
1).
Res
pon
sive
ness
is in
clud
ed in
p
atie
nt s
atis
fact
ion
and
qua
lity
of
care
lite
ratu
re, a
nd r
efer
s to
the
w
ay in
div
idua
ls a
re t
reat
ed a
nd
the
envi
ronm
ent
in w
hich
the
y ar
e tr
eate
d.
‘Qua
lity
of b
asic
faci
litie
s’
(cle
an w
aiti
ng r
oo
ms,
to
ilet
faci
litie
s, e
xam
inat
ion
room
s an
d s
urro
und
ings
) is
imp
orta
nt
to p
atie
nts
in t
heir
exp
erie
nce
of
resp
onsi
vene
ss.
R
ay e
t al
28A
n as
sess
men
t of
rur
al
heal
th c
are
del
iver
y sy
stem
in s
ome
area
s of
W
est
Ben
gal-
an o
verv
iew
Ind
iaC
ross
-sec
tiona
l ob
serv
atio
nal s
tud
yId
entif
y ex
tent
of
utili
satio
n of
hea
lthca
re
faci
litie
s an
d u
nder
stan
d
heal
thca
re s
eeki
ng
beh
avio
ur in
the
co
mm
unity
13.9
7% (6
3/45
1) w
ere
dis
sati
sfied
wit
h ca
re
qua
lity.
27%
and
23%
cl
ient
s re
po
rted
tha
t to
ilets
w
ere
‘no
t at
all
usab
le’ a
nd
‘dir
ty n
eed
ing
cle
anin
g’,
resp
ectiv
ely
(n=
174)
. S
afe
dri
nkin
g w
ater
was
av
aila
ble
in 5
5% o
f th
e fa
cilit
ies
(n=
18).
Res
tro
om
s w
ere
eith
er o
f p
oo
r q
ualit
y o
r th
e cl
ient
s d
id n
ot
use
them
, whi
le t
hey
wer
e no
t av
aila
ble
in 3
% o
f he
alth
fa
cilit
ies.
Cle
anlin
ess
of t
he p
rem
ises
, fac
e-lif
t (o
f pub
lic h
ealth
cen
tres
), an
d c
lean
to
ilet
with
priv
acy
and
ava
ilab
ility
o
f sa
fe d
rink
ing
wat
er c
ould
im
pro
ve c
lient
sat
isfa
ctio
n in
rur
al
heal
thca
re d
eliv
ery
syst
ems.
S
udha
n et
al29
Pat
ient
sat
isfa
ctio
n re
gard
ing
eye
care
se
rvic
es a
t te
rtia
ry
hosp
ital o
f cen
tral
Ind
ia
Ind
iaD
escr
iptiv
e st
udy
To e
valu
ate
pat
ient
s'
satis
fact
ion
rega
rdin
g ey
e ca
re s
ervi
ces
The
maj
ori
ty o
f re
spo
nden
ts
wer
e hi
ghl
y sa
tisfi
ed w
ith
toile
t 83
.2%
(133
/160
), w
ater
fac
iliti
es 9
9.4%
(1
59/1
60) a
nd c
lean
lines
s (1
59/1
60).
16.9
% (2
7/16
0)
did
no
t an
swer
the
to
ilet
que
stio
n an
d o
ne e
ach
for
wat
er a
nd c
lean
lines
s q
uest
ion.
Tab
le 2
C
ontin
ued
Con
tinue
d
on June 1, 2020 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2017-000648 on 9 May 2018. D
ownloaded from

Bouzid M, et al. BMJ Glob Health 2018;3:e000648. doi:10.1136/bmjgh-2017-000648 7
BMJ Global Health
Ref
eren
ceT
itle
Loca
tio
nTy
pe
of
stud
yC
ont
ext
Inte
rven
tio
nFi
ndin
gs
Furt
her
com
men
ts
W
esta
way
et
al32
Inte
rper
sona
l and
or
gani
zatio
nal d
imen
sion
s of
pat
ient
sat
isfa
ctio
n:
the
mod
erat
ing
effe
cts
of
heal
th s
tatu
s
Sou
th A
fric
aA
cro
ss-s
ectio
nal
anal
ytic
al s
tud
y d
esig
nTo
iden
tify
the
und
erly
ing
dim
ensi
ons
of p
atie
nt
satis
fact
ion
in d
iab
etic
cl
inic
for
bla
ck p
atie
nts
263
pat
ient
s w
ere
surv
eyed
. Th
e m
ost
imp
orta
nt it
ems
for
satis
fact
ion
wer
e av
aila
bili
ty
of a
sea
t in
the
wai
ting
area
(0
.73)
, ava
ilab
ility
of
a to
ilet
in t
he w
aiti
ng a
rea
(0.7
0)
and
cle
anlin
ess
(0.7
0).
Am
eniti
es a
nd a
ttrib
utes
of c
are
wer
e ce
ntra
l to
the
orga
nisa
tiona
l d
imen
sion
of p
atie
nt s
atis
fact
ion.
G
iven
leng
thy
wai
ting
tim
es
in S
out
h A
fric
a’s
pub
lic h
ealt
h fa
cilit
ies,
it is
no
t su
rpri
sing
tha
t th
e av
aila
bili
ty o
f a
seat
and
to
ilet
in t
he w
aiti
ng a
rea
feat
ured
so
pro
min
entl
y. C
lean
lines
s w
as
also
per
ceiv
ed a
s an
imp
orta
nt
satis
fact
ion
area
.
G
lick34
How
rel
iab
le a
re s
urve
ys
of c
lient
sat
isfa
ctio
n w
ith
heal
thca
re s
ervi
ces?
E
vid
ence
from
mat
ched
fa
cilit
y an
d h
ouse
hold
d
ata
in M
adag
asca
r
Mad
agas
car
Cro
ss-s
ectio
nal
Inve
stig
atio
n of
the
re
liab
ility
of e
xit
surv
eys
by
com
par
ing
pat
ient
sa
tisfa
ctio
n ou
tcom
es
to p
opul
atio
n-b
ased
ho
useh
old
sur
veys
An
app
eara
nce
ind
ex (m
ean
of b
inar
y in
dic
ator
s fo
r d
irtin
ess,
hum
idity
dam
age,
d
ecay
of w
alls
, floo
rs a
nd
ceili
ngs,
evi
den
ce o
f ins
ects
an
d c
ond
itio
n o
f to
ilet
faci
litie
s (p
rese
nce
and
cl
eanl
ines
s)) w
as c
alcu
late
d.
The
app
eara
nce
ind
ex w
as
0.84
in h
ouse
hold
sur
veys
an
d 0
.91
in e
xit
surv
eys
for
the
sam
e fa
cilit
ies.
The
nu
mb
er o
f res
pon
den
ts w
ere
262
and
770
, res
pec
tivel
y.
The
find
ings
sug
gest
tha
t re
por
ted
sa
tisfa
ctio
n in
exi
t su
rvey
s is
bia
sed
st
rong
ly u
pw
ard
for
sub
ject
ive
que
stio
ns r
egar
din
g tr
eatm
ent
by
staf
f and
con
sulta
tion
qua
lity,
b
ut n
ot
for
rela
tive
ly o
bje
ctiv
e q
uest
ions
ab
out
fac
ility
co
ndit
ion
and
sup
plie
s.
Wat
er, s
anit
atio
n an
d h
ygie
ne in
mat
erni
ty s
ervi
ces
S
rivas
tava
et
al35
Det
erm
inan
ts o
f wom
en’s
sa
tisfa
ctio
n w
ith m
ater
nal
heal
th c
are:
a r
evie
w o
f lit
erat
ure
from
dev
elop
ing
coun
trie
s
Dev
elop
ing
coun
trie
sS
yste
mat
ic r
evie
wId
entif
y d
eter
min
ants
of
wom
en’s
sat
isfa
ctio
n w
ith m
ater
nity
car
e in
d
evel
opin
g co
untr
ies
Goo
d p
hysi
cal e
nviro
nmen
t w
as s
igni
fican
t in
wom
en’s
p
ositi
ve a
sses
smen
t of
the
he
alth
faci
lity
and
mat
erna
l ca
re s
ervi
ces.
In B
angl
ades
h,
mot
hers
who
rat
ed t
he
avai
lab
ility
of s
ervi
ces
at
the
faci
lity
(a c
omp
osite
of
wai
ting
area
, dri
nkin
g w
ater
, cl
ean
toile
t an
d w
aitin
g tim
e)
as ‘g
ood
’ wer
e si
gnifi
cant
ly
mor
e sa
tisfie
d w
ith c
are
than
th
ose
who
rat
ed t
he s
ervi
ces
as ‘p
oor’
.C
lean
lines
s, g
ood
ho
usek
eep
ing
serv
ices
an
d m
aint
enan
ce o
f hy
gie
ne w
ere
rep
orte
d a
s d
eter
min
ants
of s
atis
fact
ion
in B
angl
ades
h, G
amb
ia,
Thai
land
, Ind
ia a
nd Ir
an.
Det
erm
inan
ts o
f mat
erna
l sa
tisfa
ctio
n co
vere
d a
ll th
ree
dim
ensi
ons
of c
are:
str
uctu
re,
pro
cess
and
out
com
e. S
truc
tura
l el
emen
ts in
clud
ed g
ood
phy
sica
l en
viro
nmen
t, c
lean
lines
s, a
nd
avai
lab
ility
of a
deq
uate
hum
an
reso
urce
s, m
edic
ines
and
sup
plie
s.
Acc
ess,
cos
t, s
ocio
econ
omic
st
atus
and
rep
rod
uctiv
e hi
stor
y al
so in
fluen
ced
per
ceiv
ed m
ater
nal
satis
fact
ion.
Pro
cess
of c
are
dom
inat
ed
the
det
erm
inan
ts o
f mat
erna
l sa
tisfa
ctio
n. In
terp
erso
nal b
ehav
iour
w
as t
he m
ost
wid
ely
rep
orte
d
det
erm
inan
t, p
artic
ular
ly a
roun
d
pro
vid
er b
ehav
iour
in t
erm
s of
co
urte
sy a
nd n
on-a
bus
e.
Tab
le 2
C
ontin
ued
Con
tinue
d
on June 1, 2020 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2017-000648 on 9 May 2018. D
ownloaded from

8 Bouzid M, et al. BMJ Glob Health 2018;3:e000648. doi:10.1136/bmjgh-2017-000648
BMJ Global Health
Ref
eren
ceT
itle
Loca
tio
nTy
pe
of
stud
yC
ont
ext
Inte
rven
tio
nFi
ndin
gs
Furt
her
com
men
ts
S
tein
man
n et
al36
Ava
ilab
ility
and
sa
tisfa
ctor
ines
s of
latr
ines
an
d h
and
was
hing
st
atio
ns in
hea
lth fa
cilit
ies,
an
d r
ole
in h
ealth
see
king
b
ehav
ior
of w
omen
: ev
iden
ce fr
om r
ural
Pun
e d
istr
ict,
Ind
ia
Ind
iaC
ross
-sec
tiona
l/q
uest
ionn
aire
-bas
edIn
vest
igat
ion
of t
he
WA
SH
infr
astr
uctu
re in
sm
all h
ealth
faci
litie
s an
d
surv
ey o
f exp
ecta
tions
an
d s
atis
fact
ion
amon
g w
omen
12 h
ealt
h fa
cilit
ies
wer
e as
sess
ed (6
pri
vate
and
6
pub
lic).
The
mea
n nu
mb
er
of
latr
ines
per
hea
lthc
are
faci
lity
was
2.4
(ran
ge
0–8)
, b
ut w
as lo
wer
in p
ublic
(m
ean
1.3;
ran
ge
0–2)
tha
n in
pri
vate
fac
iliti
es (m
ean
3.5;
ran
ge
1–8)
. One
fac
ility
ha
d n
o la
trin
e an
d o
ne h
ad
an u
nim
pro
ved
latr
ine.
Gen
eral
ly, o
ne h
and
w
ashi
ng s
tati
on
(tap
) was
av
aila
ble
per
latr
ine
but
tw
o p
ublic
fac
iliti
es d
id n
ot
have
any
han
d w
ashi
ng
stat
ions
. The
mea
n nu
mb
er
of
hand
was
hing
sta
tio
ns
was
0.8
(ran
ge
0–2)
in p
ublic
fa
cilit
ies
and
3.7
(ran
ge:
1–
8) in
pri
vate
fac
iliti
es.
So
ap w
as o
ften
mis
sing
fr
om
han
d w
ashi
ng s
tati
ons
(6
/12)
. Ded
icat
ed la
trin
es
for
wo
men
wer
e ra
re.
WA
SH
inst
alla
tio
ns in
hea
lth
faci
litie
s ar
e g
ener
ally
acc
epta
ble
in
pri
vate
fac
iliti
esw
hile
im
pro
vem
ents
are
nee
ded
in
som
e g
ove
rnm
ent
faci
litie
s.W
om
en e
xpec
t W
AS
H p
rovi
sio
n in
hea
lth
faci
litie
s, a
nd v
iew
the
ir
qua
lity
in a
bro
ader
fra
mew
ork
of
‘cle
anlin
ess’
, whi
ch t
hey
cons
ider
w
hen
cho
osi
ng f
acili
ties
.K
ey W
AS
H f
eatu
res
imp
ort
ant
to
wo
men
are
: num
ber
of
latr
ines
, th
eir
clea
nlin
ess
and
ava
ilab
ility
o
f w
ater
and
acc
esso
ries
(suc
h as
d
ustb
ins)
.O
ther
fact
ors,
suc
h as
a g
ood
re
put
atio
n, w
ell-
resp
ecte
d a
nd
com
pet
ent
doc
tors
wer
e co
nsid
ered
m
ore
imp
orta
nt t
han
WA
SH
sta
tus.
For
amb
ulat
ory
vis
its,
incl
udin
g
child
bir
th, W
AS
H s
tatu
s w
as s
een
as le
ss c
riti
cal t
han
for
pro
long
ed
hosp
ital
isat
ion.
P
hilib
ert
et a
l42N
o ef
fect
of u
ser
fee
exem
ptio
n on
per
ceiv
ed
qua
lity
of d
eliv
ery
care
in
Bur
kina
Fas
o: a
cas
e-co
ntro
l stu
dy
Bur
kina
Fas
oA
qua
si-e
xper
imen
tal
des
ign
with
bot
h in
terv
entio
n an
d
cont
rol g
roup
s
Ass
essi
ng w
heth
er
wom
en’s
sat
isfa
ctio
n w
ith
del
iver
y ca
re is
influ
ence
d
by
a to
tal f
ee e
xem
ptio
n
In t
he in
terv
entio
n gr
oup
, d
eliv
ery
care
is fr
ee o
f ch
arge
at
heal
th c
entr
es
870
wom
en w
ere
inte
rvie
wed
. 60
0 in
inte
rven
tion
grou
p a
nd
270
in c
ontr
ol g
roup
. 90%
w
ere
satis
fied
with
del
iver
y ca
re in
bot
h in
terv
entio
n an
d
cont
rol g
roup
s.Th
e p
oore
st w
omen
wer
e m
ore
high
ly s
atis
fied
with
d
eliv
ery
envi
ronm
ent
than
the
w
ealth
iest
one
s, e
spec
ially
co
ncer
ning
hyg
iene
and
co
mfo
rt.
Qua
lity
of c
are
was
ass
esse
d u
sing
th
ree
com
pon
ents
: car
e p
rovi
der
-p
atie
nt in
tera
ctio
n, n
ursi
ng c
are
and
d
eliv
ery
envi
ronm
ent.
Pat
ient
s ar
e of
ten
incl
ined
by
cour
tesy
to
resp
ond
pos
itive
ly t
o q
uest
ions
on
satis
fact
ion
with
car
e q
ualit
y. T
his
leve
l of c
ourt
esy
is
high
er fo
r in
terp
erso
nal r
elat
ions
hip
s b
etw
een
care
pro
vid
ers
and
p
atie
nts.
Oth
er b
iase
s: in
timid
atio
n b
y m
ale
inte
rvie
wer
and
non
-sam
plin
g of
re
mot
e ho
useh
old
s.
Tab
le 2
C
ontin
ued
Con
tinue
d
on June 1, 2020 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2017-000648 on 9 May 2018. D
ownloaded from
Bouzid M, et al. BMJ Glob Health 2018;3:e000648. doi:10.1136/bmjgh-2017-000648 9
BMJ Global Health
Ref
eren
ceT
itle
Loca
tio
nTy
pe
of
stud
yC
ont
ext
Inte
rven
tio
nFi
ndin
gs
Furt
her
com
men
ts
M
bw
ele
et a
l37Q
ualit
y of
neo
nata
l he
alth
care
in K
ilim
anja
ro
regi
on, n
orth
east
Ta
nzan
ia: l
earn
ing
from
m
othe
rs’ e
xper
ienc
es
Tanz
ania
Cro
ss-s
ectio
nal s
tud
y us
ing
qua
litat
ive
and
qua
ntita
tive
app
roac
hes
Ass
ess
mot
hers
’ ex
per
ienc
es, p
erce
ptio
n an
d s
atis
fact
ion
with
ne
onat
al c
are
in t
he
hosp
itals
80 m
othe
rs w
ere
inte
rvie
wed
fr
om 1
3 p
erip
hera
l fac
ilitie
s an
d 3
2 fr
om a
ref
erra
l ho
spita
l. O
nly
2% d
iscu
ssed
is
sues
of
hyg
iene
. One
m
othe
r m
entio
ned
tha
t th
e fa
cilit
y sh
ould
‘inc
reas
e th
e le
vel o
f hy
gie
ne’.
The
sta
te o
f to
ilets
at
refe
rral
ho
spit
al w
ere
as e
xpec
ted
fo
r 59
%
resp
ond
ents
whi
le, i
n p
erip
hera
l ho
spit
als
28%
w
ere
as e
xpec
ted
. To
ilets
w
ere
wo
rse
than
exp
ecte
d
for
7% a
nd 2
6% in
ref
erra
l an
d p
erip
hera
l ho
spit
als,
re
spec
tive
ly.
The
mos
t co
mm
on r
easo
ns fo
r p
rimar
y d
elay
s: q
ualit
y of
tre
atm
ent
at t
he fa
cilit
y 55
.1%
(27/
49) a
nd
cost
of m
edic
al c
are
32.6
% (1
6/49
). P
aram
eter
s fo
r se
cond
ary
del
ays
wer
e d
ista
nce
from
hom
e (1
1.1%
) an
d c
omb
ined
dis
tanc
e an
d
tran
spor
t (7
.4%
).
Te
tui e
t al
38Q
ualit
y of
Ant
enat
al
care
ser
vice
s in
eas
tern
U
gand
a: im
plic
atio
ns fo
r in
terv
entio
ns
Uga
nda
Cro
ss-s
ectio
nal
Ass
essm
ent
of q
ualit
y of
AN
C (A
nten
atal
car
e)
serv
ices
in e
aste
rn
Uga
nda
with
a g
oal o
f b
ench
mar
king
74.6
% (2
17/2
91) r
esp
ond
ents
ra
ted
the
AN
C s
ervi
ce a
s sa
tisfa
ctor
y. In
fect
ion
cont
rol
was
ava
ilab
le in
73.
4%
(11/
15) f
acili
ties.
Cle
anlin
ess
was
d
issa
tisfa
ctor
y fo
r 4.
1%
(12/
291)
, fai
rly s
atis
fact
ory
for
25.8
% (7
5/29
1) a
nd
satis
fact
ory
in 7
0.1%
(2
04/2
91).
Dat
a co
llect
ed t
o ga
uge
infe
ctio
n co
ntro
l: ex
iste
nce
of
pip
ed r
unni
ng
wat
er, w
ater
buc
kets
or
bas
ins,
ha
nd w
ashi
ng s
oap
, dis
pos
able
ha
nd d
ryin
g to
wel
s, w
aste
bin
s,
shar
ps
cont
aine
rs, d
isp
osab
le la
tex
glov
es a
nd d
isin
fect
ion
solu
tion.
The
varia
ble
s as
soci
ated
with
hi
gh s
atis
fact
ion
wer
e p
rovi
der
’s
attit
ude
(87.
6%) a
nd e
xam
inat
ion
room
priv
acy
(83.
5%).
How
ever
, av
aila
bili
ty o
f med
icin
es (3
2.3%
) and
w
aitin
g tim
e (2
5.1%
) had
the
hig
hest
d
issa
tisfa
ctio
n ra
tes.
G
abry
sch
and
Cam
pb
ell40
Stil
l too
far
to w
alk:
lit
erat
ure
revi
ew o
f the
d
eter
min
ants
of d
eliv
ery
serv
ice
use
Low
or
mid
dle
in
com
e co
untr
ies
Lite
ratu
re r
evie
w (o
f re
view
art
icle
s)Id
entifi
catio
n of
var
ious
fa
ctor
s re
late
d t
o d
eliv
ery
serv
ice
use
Sho
rtco
min
gs in
med
ical
ca
re a
re o
ften
cou
ple
d w
ith
shor
tcom
ings
in h
ygie
ne.
Wo
men
cri
tici
se d
irty
to
ilet
faci
litie
s, la
ck o
f w
ater
and
as
epti
c p
ract
ices
as
wel
l as
lack
of d
rugs
or
too
early
ca
esar
ean
sect
ions
.
Per
ceiv
ed q
ualit
y of
car
e ha
s an
im
por
tant
influ
ence
on
care
see
king
b
ehav
iour
. Poo
r p
erso
nal a
nd
med
ical
qua
lity
of c
are,
cla
sh w
ith
cultu
re a
nd fe
ar o
f pro
ced
ures
may
d
ecre
ase
use.
K
ongn
yuy
et a
l45C
riter
ia-b
ased
aud
it to
im
pro
ve w
omen
-frie
ndly
ca
re in
mat
erni
ty u
nits
in
Mal
awi
Mal
awi
Cro
ss-s
ectio
nal/
inte
rvie
ws
To a
sses
s an
d im
pro
ve
wom
en-f
riend
ly c
are
in
mat
erni
ty u
nits
in M
alaw
i
280
wom
en w
ere
inte
rvie
wed
ab
out
care
q
ualit
y. T
he a
udit
resu
lts
wer
e p
rese
nted
, and
re
com
men
dat
ions
mad
e.
A r
e-au
dit
(367
wom
en)
was
con
duc
ted
3 m
onth
s la
ter
and
per
form
ance
co
mp
ared
.
Sig
nific
ant
imp
rove
men
t w
as
reco
rded
for
clea
nlin
ess
of
mat
erni
ty w
ard
s (8
9.6
vs
97.0
%; p
<0.
001)
. How
ever
, th
ere
wer
e no
sig
nifi
cant
ch
ang
es in
pro
visi
on
of
clea
n b
athr
oo
m a
nd t
oile
t (8
3.6
vs 8
0.4%
; p=
0.28
2).
Eac
h he
alth
fac
ility
sho
uld
ass
ess
the
avai
lab
ility
and
fun
ctio
ning
o
f to
ilets
and
bat
hro
om
s.
Whe
re a
vaila
ble
, the
y sh
oul
d
be
func
tio
nal a
nd k
ept
clea
n. If
la
ckin
g, t
hey
sho
uld
be
req
uest
ed.
One
hea
lth
cent
re r
eque
sted
and
ha
d a
new
to
ilet
but
no
rep
ort
on
the
imp
act
of
this
imp
rove
men
t w
as p
rese
nted
.
Tab
le 2
C
ontin
ued
Con
tinue
d
on June 1, 2020 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2017-000648 on 9 May 2018. D
ownloaded from
10 Bouzid M, et al. BMJ Glob Health 2018;3:e000648. doi:10.1136/bmjgh-2017-000648
BMJ Global Health
Ref
eren
ceT
itle
Loca
tio
nTy
pe
of
stud
yC
ont
ext
Inte
rven
tio
nFi
ndin
gs
Furt
her
com
men
ts
M
acK
eith
et
al39
Zam
bia
n w
omen
’s
exp
erie
nces
of u
rban
m
ater
nity
car
e: r
esul
ts
from
a c
omm
unity
sur
vey
in L
usak
a
Zam
bia
Cro
ss-s
ectio
nal/
com
mun
ity s
urve
y q
uest
ionn
aire
s
Exa
min
e ac
cess
, co
vera
ge a
nd q
ualit
y of
car
e in
mid
wiv
es r
un
mat
erni
ty s
ervi
ce
845
wer
e in
terv
iew
ed.
74%
wou
ld li
ke t
o se
e im
pro
vem
ents
ove
rall
and
18
.23%
wo
uld
like
to
see
b
ette
r hy
gie
ne in
to
ilets
an
d b
athr
oo
ms
at h
ealt
h fa
cilit
ies.
G
riffit
hs
and
Ste
phe
nson
41U
nder
stan
din
g us
ers’
p
ersp
ectiv
es o
f bar
riers
to
mat
erna
l hea
lth c
are
use
in M
ahar
asht
ra, I
ndia
Ind
iaC
ross
-sec
tiona
l/in
terv
iew
sId
entifi
catio
n of
key
so
cial
, eco
nom
ic a
nd
cultu
ral f
acto
rs in
fluen
cing
w
omen
’s d
ecis
ions
to
use
mat
erna
l hea
lthca
re
45 w
omen
wer
e in
terv
iew
ed.
Res
pon
den
ts id
entifi
ed p
oor-
qua
lity
of s
ervi
ces
offe
red
at
gov
ernm
ent
inst
itutio
ns
to b
e a
mot
ivat
ing
fact
or fo
r d
eliv
erin
g at
hom
e: ‘I
t w
as
safe
in t
he h
ouse
and
the
nu
rse
was
pre
sent
to
do
the
del
iver
y. In
gov
ernm
ent
hosp
ital,
del
iver
y ro
om is
no
t th
ere.
To
ilet
and
wat
er
faci
litie
s ar
e no
t th
ere.
So
I fe
lt s
afe
to g
ive
bir
th in
the
ho
use’
.
Soc
ioec
onom
ic s
tatu
s w
as n
ot
foun
d t
o b
e a
bar
rier
to s
ervi
ce u
se
whe
n w
omen
per
ceiv
ed t
he b
enefi
ts
of t
he s
ervi
ce t
o ou
twei
gh t
he c
ost,
an
d w
hen
the
serv
ice
was
with
in
reas
onab
le d
ista
nce.
The
tab
le s
umm
aris
es t
he c
hara
cter
istic
s of
incl
uded
stu
die
s an
d t
heir
mai
n fin
din
gs.
WA
SH
com
pon
ents
are
pre
sent
ed in
bol
d.
WA
SH
, wat
er, s
anita
tion
and
hyg
iene
.
Tab
le 2
C
ontin
ued
on June 1, 2020 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2017-000648 on 9 May 2018. D
ownloaded from

Bouzid M, et al. BMJ Glob Health 2018;3:e000648. doi:10.1136/bmjgh-2017-000648 11
BMJ Global Health
mean number of hand washing stations was 2.3 (0.8 for public and 3.7 for private facilities), with two public centres lacking any hand washing facilities. WASH provi-sion is generally acceptable in private healthcare centres but needs improvement in government facilities.36 Good reputation, competent and respected doctors and ability to deal with complications were the main factors influencing the choice of HCF. For ambulatory care, including child birth, WASH provision was considered less important compared with prolonged hospitalisation settings.36
Mbwele and colleagues investigated the quality of neonatal healthcare in Tanzania.37 Two per cent of mothers commented on hygiene issues and one mother suggested that improvements in hygiene were needed. Most respondents reported that the condition of toilets was as expected, while a few found them worse than expected (table 2).37 The main reason for primary delay was quality of treatment followed by cost of medical care, while secondary delay was due to distance from home, transport and complaints about unfriendliness of care workers. Tetui and colleagues investigated the quality of antenatal care in Uganda and reported that 74.6% of respondents were satisfied with care quality, while 70% were satisfied with cleanliness.38 Although data on piped water and hand washing were collected as part of the assessment, no report on WASH and patient satisfac-tion was provided. Infection control was a major focus and 73.4% HCF were deemed to have good infection control measures.38 MacKeith and colleagues assessed women’s experience of urban maternity care in Zambia and reported that 74% would like to see general improve-ments; however, only 18.23% clearly expressed the need for better hygiene in toilets and bathrooms.39
Gabrysch and colleagues reported that women criticise dirty toilets, lack of water and aseptic practices, high-lighting combined shortcomings in personal interaction, medical care and hygiene.40 They concluded that the perceived quality of care had a major influence on care seeking behaviour.40 Griffiths and colleagues investigated users’ perspectives of barriers to maternal healthcare use in India through identification of key social, economic and cultural factors influencing women’s decision to seek maternal care.41 Quality of care and safety issues as well as lack of WASH provision were motivating women to give birth at home. A respondent stated, ‘It was safe in the house and the nurse was present to do the delivery. In the government hospital, the delivery room is not there. Toilet and water facilities are not there. So I felt safer to give birth in the house’.41 Socioeconomic status was not a barrier to service use when women considered the benefit to outweigh the cost, providing it was within reasonable distance.41 Philibert and colleagues reported that, in Burkina Faso, socioeconomic status influences patients’ expectation and satisfaction, with the poorest women more satisfied with delivery environment than the wealth-iest ones.42 Courtesy bias leads women to respond more positively to care quality questions, which does not reflect
their true opinion.42 Courtesy bias was more pronounced for interpersonal relationships between patients and care providers,42 which is in accordance with the findings of Glick (in a non-maternity setting).34
Improvement interventions and accreditation in HCFDeveloping accreditation standards in Ugandan hospitals was investigated by Galukande and colleagues.43 Accred-itation items included physical infrastructure, infection control and waste management. While the majority of hospitals reported having infection control protocol in place, only half were recording needle stick injuries and vermin control.43 Perhaps more surprisingly, 27.5% hospi-tals were not tracking infection rates even for caesarean sections. In addition, the authors reported inadequate capacity to sterilise equipment in all hospitals, which would contribute to HCAI.43 The study reported good provision of running water but no mention of sanitation. Okwaro and colleagues investigated community percep-tion of healthcare improvement intervention in rural Uganda.44 The formative research showed that many HCF (in this case malaria treatment centres) lacked running water. Following the intervention, antimalarial drug availability has improved; however, other require-ments including more health workers, provision of clean water and clean toilets have not been addressed. There-fore, this intervention was not sufficient to elicit major changes or influence patients’ decision about healthcare use.44 Indeed, several patients continued to seek care at inadequate heath centres. The authors reported that the main limitation of such an intervention is the focus on a particular disease and therefore failing to address multiple inadequacies observed in HCF in LMIC.
One paper investigated a criteria-based audit to improve a maternity unit in Malawi, where an initial audit resulted in the formulation of recommendations and a second audit 3 months later would report on any observed improvements.45 Significant improvements in cleanliness were achieved post audit; however, no significant changes in provision of clean toilets and bathrooms were noted.45 The authors reported that one health facility requested and obtained a new toilet, which should contribute to address the issue of inadequate WASH provision in healthcare setting.45
dIsCussIonPatient satisfaction is a good indicator of quality of care provided and impacts on care seeking behaviour. In the reviewed studies, inadequate WASH in HCF was associ-ated with increased patient dissatisfaction and was even a barrier to service use in some settings (most notably maternity services). This systematic review of current evidence has informed a conceptual model of patient dissatisfaction, detailing relevant factors and repercus-sions of low patient satisfaction (figure 2). In this model, patient dissatisfaction results in delayed care seeking, poor health outcomes and reduced staff morale. Good
on June 1, 2020 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2017-000648 on 9 May 2018. D
ownloaded from

12 Bouzid M, et al. BMJ Glob Health 2018;3:e000648. doi:10.1136/bmjgh-2017-000648
BMJ Global Health
infrastructure including adequate WASH provision is an integral part to high quality of healthcare. Inadequate WASH provision is one of the elements influencing patient dissatisfaction, though it was not found to be a major driver. Other factors relevant in resource-poor settings were significantly influencing patient satisfaction and care seeking behaviours in LMIC. The relative impor-tance of WASH on patient satisfaction is context-specific and depends on the type of healthcare service and the length of stay. Indeed, the lack of safe WASH facilities in delivery rooms was frequently cited as the reason for women to prefer home delivery. Women expect HCF to have adequate WASH, and rightly so, as this is pivotal for their human right, dignity and infection prevention. Achieving this, however, remains a distant prospect in many healthcare settings in LMIC.
The limitations of this study include a relatively small publication window (2000–2016), which was chosen to exclude historic (or outdated) WASH provision and a search strategy that could have been further opti-mised to retrieve all relevant papers. Potential further limitations are the difficulty of retrieving eligible LMIC research, likely to be published in national journals not indexed in the databases searched and studies are not necessarily indexed properly (particularly regarding LMIC status/country affiliation). Finally, the studies included were mostly cross-sectional with potentially biased outcome measures and perhaps more importantly no study designed to specifically assess the causal effect of WASH provision on patient satisfaction and/or care seeking behaviour was found. The limitations of some of the included studies are related to study design, such
as small sample size, lack of randomisation and patient recruitment procedures, as well as outcome measures such as heterogeneous indicators of patient satisfaction and potentially biased findings.
This review focused on WASH and patient satisfac-tion/care seeking because of the large disease burden associated with delayed care seeking. The link between perceived quality of care and attendance at HCF (patients who received quality care tend to return and recommend the facility to relatives) was supported by several studies and the WHO recommends the evaluation of patients’ satisfaction for the improvement of HCF.46 However, perceived quality of care is highly subjective. It includes satisfaction with the outcome, the interventions and the service received (staff friendliness, availability of supplies and waiting times) as well as objective measures of care quality such as facility infrastructure, equipment and staffing.40 However, even these measures are subjective because they depend on the discrepancy between expec-tation and reality, strongly influenced by socioeconomic traits and subpopulation groups. Indeed, it was reported that wealthier women and patients with higher education were consistently less satisfied with delivery environment and quality of care, respectively.31 42 It was noted, however, that factors other than WASH actually drive the selection and use of health facility.36 Therefore, it is perhaps not surprising that patients continue to use HCF with inade-quate WASH provision (table 2).44
The evaluation of patient satisfaction is usually performed using patient questionnaires, administered at either the HCF or households. It has been shown that exit questionnaires tend to overestimate patient
Figure 2 Conceptual model of implications of patient dissatisfaction with care quality. The model details the interactions between patient dissatisfaction, inadequate WASH provision, care seeking behaviour and health outcomes. WASH, water, sanitation and hygiene.
on June 1, 2020 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2017-000648 on 9 May 2018. D
ownloaded from

Bouzid M, et al. BMJ Glob Health 2018;3:e000648. doi:10.1136/bmjgh-2017-000648 13
BMJ Global Health
satisfaction level due to courtesy bias (although this was mainly for treatment by staff and consultation quality and not facility condition).34 Intimidation bias was also reported when female interviewees felt intimidated by a male interviewer.42 Therefore, household surveys may provide more reliable estimates of patient satisfaction.34 However, household surveys could also yield biased results as they are associated with substantial under-reporting of healthcare use, especially when the recall period was over 1 month.47
The availability of skilled birth attendants is crucial to provide emergency obstetric care and reduce maternal and newborn mortality.48 This is part of the official guid-ance and improving WASH provision should increase use of maternal health services in LMICs. Concernedly, a study reported higher mortality rates after obstetric care.49 The reasons were: seeking help very late and in crit-ical condition and lack of timely and adequate care once at the health facility. Birth attendants may not provide socioculturally appropriate and respectful care leading to poor uptake.48 Previous delivery by a male provider made women choose home delivery during the subsequent pregnancy (OR 3.90; 95% CI 2.30 to 6.65).46 It was stated that ‘efforts aimed at improving maternal and child health in developing countries should take cognisance of the sociodemographic and cultural underpinnings of maternal health seeking behaviour’.50 Complaints of abuse, neglect and poor treatment are common in mater-nity services.51 Therefore, in addition to improving facil-ities’ infrastructure, care quality and cost-effectiveness, improvements in maternity services should also address providers’ attitudes and interpersonal behaviours.48 This highlights the scale and complexity of the issues investi-gated and the high number of shortcomings that need to be addressed.
The importance of WASH in HCF extends beyond patient satisfaction and care seeking behaviour because inadequate WASH may also be associated with a signif-icant burden of HCAI. Poor sanitary conditions and hand hygiene in hospital settings would result in several gastrointestinal and opportunistic infections. Unfortu-nately, poor hand washing practices around birth are still prevalent and continue to pose risks to mother and baby. In an observational study, the proportion of birth attendants who washed their hands prior to assisting with delivery was 24% in India, 69% in Bangladesh and 32% in Nepal.52 Hand washing of birth attendants was asso-ciated with 49% reduction in maternal mortality (OR 0.51, 95% CI 0.28 to 0.93)52 and 19% (range 1%–34%) reduction in all cause neonatal mortality.53 Effective hand washing in HCF has benefits for a wide range of other HCAI,54 although adherence to good hand hygiene practices is a persistent challenge. Addressing this issue requires changes in both behaviour and infrastructure; hand hygiene practices will only improve if healthcare workers are motivated to change their behaviour and when adequate facilities (taps with running water and soap) are available.
ConClusIonThe provision of adequate WASH in HCF is important to protect vulnerable populations and reduce HCAI. However, WASH provision is still inadequate in many HCF in LMIC. This systematic review assessed the impact of WASH provision on care seeking behaviour and patient satisfaction. Our review suggests that improving WASH conditions will decrease patience dissatisfaction, which may increase care seeking behaviour and improve health outcomes but that more rigorous research is needed.
Contributors PRH conceptualised the study. MB did literature search, paper screening, data collection and manuscript writing. OC assisted with topic selection and discussion. All authors contributed to the manuscript.
Funding MB was partially supported by the Water, Sanitation, Hygiene and Health programme at the WHO. PRH is supported by the National Institute for Health Research (NIHR) Health Protection Research Units in Gastrointestinal Infections and Emergency Preparedness and Response in partnership with Public Health England (PHE).
disclaimer The views expressed are those of the authors and not necessarily those of the NHS, the NIHR, the Department of Health or PHE. The funders had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
data sharing statement No additional data are available.
open Access This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: http:// creativecommons. org/ licenses/ by/ 4. 0/
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
REFERENCES 1. Prüss-Ustün A, Bartram J, Clasen T, et al. Burden of disease from
inadequate water, sanitation and hygiene in low- and middle-income settings: a retrospective analysis of data from 145 countries. Trop Med Int Health 2014;19:894–905.
2. UNICEF, WHO. Progress on sanitation and drinking water – 2015 update and MDG assessment. 2015 http:// files. unicef. org/ publications/ files/ Progress_ on_ Sanitation_ and_ Drinking_ Water_ 2015_ Update_. pdf (accessed 14 Aug 2017).
3. WHO/UNICEF. Water, sanitation and hygiene in health care facilities: urgent needs and actions. Meeting Report.. 2015 www. who. int/ water_ sanitation_ health/ facilities/ wash- in- hcf- geneva. pdf (accessed 17 Mar 2016).
4. Unicef WHO. Scoping Study: Preparing for SDG reporting of WASH in health care facilities in the East Asia and Pacific Region. 2017 https://www. washinhcf. org/ fileadmin/ user_ upload/ documents/ SDG- WASH- HCF- EAPRO- FINAL. pdf (accessed 14 Aug 2017).
5. Unicef WHO. Scoping Study: Are data available to monitor the SDGs for WASH in schools and health care facilities in the Latin America and Caribbean region? 2017 https://www. washinhcf. org/ fileadmin/ user_ upload/ documents/ SDG- WASH- institutions- LACRO- FINAL. pdf (accessed 14 Aug 2017).
6. Velleman Y, Mason E, Graham W, et al. From joint thinking to joint action: a call to action on improving water, sanitation, and hygiene for maternal and newborn health. PLoS Med 2014;11:e1001771.
7. Shahida SM, Islam A, Dey BR, et al. Hospital acquired infections in low and middle income countries: root cause analysis and the development of infection control practices in Bangladesh. Open J Obstet Gynecol 2016;06:28–39.
8. Pittet D, Allegranzi B, Boyce J. World Health Organization World Alliance for Patient Safety First Global Patient Safety Challenge Core Group of Experts. The World Health Organization
on June 1, 2020 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2017-000648 on 9 May 2018. D
ownloaded from

14 Bouzid M, et al. BMJ Glob Health 2018;3:e000648. doi:10.1136/bmjgh-2017-000648
BMJ Global Health
Guidelines on Hand Hygiene in Health Care and their consensus recommendations. Infect Control Hosp Epidemiol 2009;30:611–22.
9. Gordon A. A treatise on the epidemic puerperal fever of Aberdeen. 1795 https://archiveorg/details/treatiseonepidem00gord (accessed 14 Aug 2017).
10. Semmelweis I. Etiology, concept and prophylaxis of childbed fever. 1861 http:// graphics8. nytimes. com/ images/ blogs/ freakonomics/ pdf/ the% 20etiology,% 20concept% 20and% 20prophylaxis% 20of% 20childbed% 20fever. pdf (accessed 08 Nov 2016).
11. Ferranti G, Marchesi I, Favale M, et al. Aetiology, source and prevention of waterborne healthcare-associated infections: a review. J Med Microbiol 2014;63(Pt 10):1247–59.
12. Merlani GM, Francioli P. Established and emerging waterborne nosocomial infections. Curr Opin Infect Dis 2003;16:343–7.
13. Squier C, Yu VL, Stout JE. Waterborne nosocomial infections. Curr Infect Dis Rep 2000;2:490–6.
14. Weber DJ, Anderson D, Rutala WA. The role of the surface environment in healthcare-associated infections. Curr Opin Infect Dis 2013;26:338–44.
15. Allegranzi B, Bagheri Nejad S, Combescure C, et al. Burden of endemic health-care-associated infection in developing countries: systematic review and meta-analysis. Lancet 2011;377:228–41.
16. Thaddeus S, Maine D. Too far to walk: maternal mortality in context. Soc Sci Med 1994;38:1091–110.
17. Waiswa P, Kallander K, Peterson S, et al. Using the three delays model to understand why newborn babies die in eastern Uganda. Trop Med Int Health 2010;15:964–72.
18. Bojalil R, Kirkwood BR, Bobak M, et al. The relative contribution of case management and inadequate care-seeking behaviour to childhood deaths from diarrhoea and acute respiratory infections in Hidalgo, Mexico. Trop Med Int Health 2007;12:1545–52.
19. Hirose A, Borchert M, Niksear H, et al. The role of care-seeking delays in intrauterine fetal deaths among 'near-miss' women in Herat, Afghanistan. Paediatr Perinat Epidemiol 2012;26:388–97.
20. Nasrin D, Wu Y, Blackwelder WC, et al. Health care seeking for childhood diarrhea in developing countries: evidence from seven sites in Africa and Asia. Am J Trop Med Hyg 2013;89:3–12.
21. Afsana K, Rashid SF. The challenges of meeting rural Bangladeshi women's needs in delivery care. Reprod Health Matters 2001;9:79–89.
22. Prakash B. Patient satisfaction. J Cutan Aesthet Surg 2010;3:151–5. 23. Batbaatar E, Dorjdagva J, Luvsannyam A, et al. Determinants of
patient satisfaction: a systematic review. Perspect Public Health 2017;137.
24. Moher D, Shamseer L, Clarke M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev 2015;4:1.
25. Woldeyohanes TR, Woldehaimanot TE, Kerie MW, et al. Perceived patient satisfaction with in-patient services at Jimma University Specialized Hospital, Southwest Ethiopia. BMC Res Notes 2015;8:285.
26. Tessema SB, Adane MM. Assessment of antiretroviral treatment (ART) care service provision in Tigray Region health centers, North Ethiopia. BMC Health Serv Res 2015;15:368.
27. Ezegwui IR, Okoye OI, Aghaji AE, et al. Patients' satisfaction with eye care services in a Nigerian teaching hospital. Niger J Clin Pract 2014;17:585–8.
28. Ray SK, Basu SS, Basu AK. An assessment of rural health care delivery system in some areas of West Bengal-an overview. Indian J Public Health 2011;55:70–80.
29. Sudhan A, Khandekar R, Deveragonda S, et al. Patient satisfaction regarding eye care services at tertiary hospital of central India. Oman J Ophthalmol 2011;4:73–6.
30. Khamis K, Njau B. Patients' level of satisfaction on quality of health care at Mwananyamala hospital in Dar es Salaam, Tanzania. BMC Health Serv Res 2014;14:400.
31. Mohammed S, Bermejo JL, Souares A, et al. Assessing responsiveness of health care services within a health insurance scheme in Nigeria: users' perspectives. BMC Health Serv Res 2013;13:502.
32. Westaway MS, Rheeder P, Van Zyl DG, et al. Interpersonal and organizational dimensions of patient satisfaction: the moderating effects of health status. Int J Qual Health Care 2003;15:337–44.
33. Tumlinson K, Pence BW, Curtis SL, et al. Quality of care and contraceptive use in Urban Kenya. Int Perspect Sex Reprod Health 2015;41:69–79.
34. Glick P. How reliable are surveys of client satisfaction with healthcare services? Evidence from matched facility and household data in Madagascar. Soc Sci Med 2009;68:368–79.
35. Srivastava A, Avan BI, Rajbangshi P, et al. Determinants of women's satisfaction with maternal health care: a review of literature from developing countries. BMC Pregnancy Childbirth 2015;15:97.
36. Steinmann P, Bratschi MW, Lele P, et al. Availability and satisfactoriness of latrines and hand washing stations in health facilities, and role in health seeking behavior of women: evidence from rural Pune district, India. Journal of Water, Sanitation and Hygiene for Development 2015;5:474–82.
37. Mbwele B, Ide NL, Reddy E, et al. Quality of neonatal healthcare in Kilimanjaro region, northeast Tanzania: learning from mothers' experiences. BMC Pediatr 2013;13:68.
38. Tetui M, Ekirapa EK, Bua J, et al. Quality of Antenatal care services in eastern Uganda: implications for interventions. Pan Afr Med J 2012;13:27.
39. MacKeith N, Chinganya OJ, Ahmed Y, et al. Zambian women's experiences of urban maternity care: results from a community survey in Lusaka. Afr J Reprod Health 2003;7:92–102.
40. Gabrysch S, Campbell OM. Still too far to walk: literature review of the determinants of delivery service use. BMC Pregnancy Childbirth 2009;9:34.
41. Griffiths P, Stephenson R. Understanding users' perspectives of barriers to maternal health care use in Maharashtra, India. J Biosoc Sci 2001;33:339–59.
42. Philibert A, Ridde V, Bado A, et al. No effect of user fee exemption on perceived quality of delivery care in Burkina Faso: a case-control study. BMC Health Serv Res 2014;14:120.
43. Galukande M, Katamba A, Nakasujja N, et al. Developing hospital accreditation standards in Uganda. Int J Health Plann Manage 2016;31.
44. Okwaro FM, Chandler CI, Hutchinson E, et al. Challenging logics of complex intervention trials: community perspectives of a health care improvement intervention in rural Uganda. Soc Sci Med 2015;131:10–17.
45. Kongnyuy EJ, Mlava G, van den Broek N. Criteria-based audit to improve women-friendly care in maternity units in Malawi. J Obstet Gynaecol Res 2009;35:483–9.
46. Faye A, Niane M, Ba I. Home birth in women who have given birth at least once in a health facility: contributory factors in a developing country. Acta Obstet Gynecol Scand 2011;90:1239–43.
47. Ansah EK, Powell-Jackson T. Can we trust measures of healthcare utilization from household surveys? BMC Public Health 2013;13:853.
48. Ith P, Dawson A, Homer CS. Women's perspective of maternity care in Cambodia. Women Birth 2013;26:71–5.
49. Ronsmans C, Chowdhury ME, Koblinsky M, et al. Care seeking at time of childbirth, and maternal and perinatal mortality in Matlab, Bangladesh. Bull World Health Organ 2010;88:289–96.
50. Olusanya BO, Alakija OP, Inem VA. Non-uptake of facility-based maternity services in an inner-city community in Lagos, Nigeria: an observational study. J Biosoc Sci 2010;42:341–58.
51. Kyomuhendo GB. Low use of rural maternity services in Uganda: impact of women's status, traditional beliefs and limited resources. Reprod Health Matters 2003;11:16–26.
52. Seward N, Prost A, Copas A, et al. Using observational data to estimate the effect of hand washing and clean delivery kit use by birth attendants on maternal deaths after home deliveries in rural Bangladesh, India and Nepal. PLoS One 2015;10:e0136152.
53. Blencowe H, Cousens S, Mullany LC, et al. Clean birth and postnatal care practices to reduce neonatal deaths from sepsis and tetanus: a systematic review and Delphi estimation of mortality effect. BMC Public Health 2011;11 Suppl 3(Suppl 3):S11.
54. Murni I, Duke T, Triasih R, et al. Prevention of nosocomial infections in developing countries, a systematic review. Paediatr Int Child Health 2013;33:61–78.
on June 1, 2020 by guest. Protected by copyright.
http://gh.bmj.com
/B
MJ G
lob Health: first published as 10.1136/bm
jgh-2017-000648 on 9 May 2018. D
ownloaded from


















