
What Does Women’s Health Care Look Like in the VA? Elizabeth M. Yano, PhD, MSPH; Bevanne...
17
What Does Women’s Health Care What Does Women’s Health Care Look Like in the VA? Look Like in the VA? Elizabeth M. Yano, PhD, MSPH; Elizabeth M. Yano, PhD, MSPH; Bevanne Bean-Mayberry, MD, MHS; Ismelda Canelo, Bevanne Bean-Mayberry, MD, MHS; Ismelda Canelo, MPA; MPA; Andrew B. Lanto, MA; Donna L. Washington, MD, Andrew B. Lanto, MA; Donna L. Washington, MD, MPH MPH VA Greater Los Angeles HSR&D Center of Excellence VA Greater Los Angeles HSR&D Center of Excellence UCLA Schools of Public Health and Medicine UCLA Schools of Public Health and Medicine Academy Health Academy Health Washington DC Washington DC June 10, 2008 June 10, 2008 Center for the Study of Healthcare Provider Behavior
-
Upload
bathsheba-bennett -
Category
Documents
-
view
215 -
download
2
Transcript of What Does Women’s Health Care Look Like in the VA? Elizabeth M. Yano, PhD, MSPH; Bevanne...

What Does Women’s Health Care Look What Does Women’s Health Care Look Like in the VA?Like in the VA?
Elizabeth M. Yano, PhD, MSPH; Elizabeth M. Yano, PhD, MSPH; Bevanne Bean-Mayberry, MD, MHS; Ismelda Canelo, MPA; Bevanne Bean-Mayberry, MD, MHS; Ismelda Canelo, MPA;
Andrew B. Lanto, MA; Donna L. Washington, MD, MPHAndrew B. Lanto, MA; Donna L. Washington, MD, MPHVA Greater Los Angeles HSR&D Center of ExcellenceVA Greater Los Angeles HSR&D Center of Excellence
UCLA Schools of Public Health and MedicineUCLA Schools of Public Health and Medicine
Academy Health Academy Health Washington DC Washington DC June 10, 2008 June 10, 2008
Center for the Study ofHealthcare Provider Behavior

BackgroundBackground
Changing demographics of militaryChanging demographics of military– 15% of active military, 17% of National 15% of active military, 17% of National
Guard/Reserves and 20% new recruits are womenGuard/Reserves and 20% new recruits are women
Women veterans among fastest growing Women veterans among fastest growing segments of new users of VA health caresegments of new users of VA health care– Overall about 11% market penetrationOverall about 11% market penetration– As high as 40% of OEF/OIF electing to use VAAs high as 40% of OEF/OIF electing to use VA
Women veterans who use the VA have unique Women veterans who use the VA have unique health care needshealth care needs– Lower functional status vs. male vets, non-vet womenLower functional status vs. male vets, non-vet women– Special mental health care needs (PTSD, MST)Special mental health care needs (PTSD, MST)

BackgroundBackground
Gaps in care historically documentedGaps in care historically documented– Congressional eligibility reforms changed array of Congressional eligibility reforms changed array of
services to be made available to women veteransservices to be made available to women veteransIncluding mandated provision of gender-specific servicesIncluding mandated provision of gender-specific services
Considerable debate about how best to organize Considerable debate about how best to organize care for women veteranscare for women veterans– Numerical minority creates challengesNumerical minority creates challenges– VA providers with limited exposure to womenVA providers with limited exposure to women
VHA faces considerable challenges in meeting VHA faces considerable challenges in meeting women veterans’ health care needswomen veterans’ health care needs– Complicated casemix, growing caseload, service mixComplicated casemix, growing caseload, service mix
ObjectiveObjective
To evaluate how VA women’s health care is To evaluate how VA women’s health care is organized and how well VA is adapting to women organized and how well VA is adapting to women veterans’ health care needsveterans’ health care needs– VHA Handbook 1330.1 recommends specific primary VHA Handbook 1330.1 recommends specific primary
care delivery models for womencare delivery models for womenSeparate women’s health clinicsSeparate women’s health clinics
Designated women’s health providers in general primary careDesignated women’s health providers in general primary care
– Legislation requires attention to privacy and Legislation requires attention to privacy and appropriate service availabilityappropriate service availability

Design and SampleDesign and Sample
Time-series organizational surveysTime-series organizational surveys– Key informants at network, facility, clinic levelsKey informants at network, facility, clinic levels– 2001 and 20072001 and 2007
National census of all VA health care facilities National census of all VA health care facilities serving 200+ women veteransserving 200+ women veterans– Respondents included all VA regional network Respondents included all VA regional network
directors, chiefs of staff, senior WH cliniciansdirectors, chiefs of staff, senior WH clinicians– Focus on clinic-level results (82% and 86% RRs)Focus on clinic-level results (82% and 86% RRs)– Facilities represent 80% of women veterans seen in Facilities represent 80% of women veterans seen in
VA settingsVA settings
Focus on clinic-level resultsFocus on clinic-level results
Survey DevelopmentSurvey Development
Domain development anchored in diffusion Domain development anchored in diffusion theory and Donabedian structure-process-theory and Donabedian structure-process-outcome frameworkoutcome framework
Expert panel review and priority-setting of Expert panel review and priority-setting of domains using modified Delphi techniquesdomains using modified Delphi techniques– Representatives from VA and non-VARepresentatives from VA and non-VA– Experience`e with different care model variationsExperience`e with different care model variations
Iterative survey item/scale development, Iterative survey item/scale development, cognitive interviews and pilot testingcognitive interviews and pilot testing
MeasuresMeasures
Clinic structure/operationsClinic structure/operations– General PC, women’s, gyn and mental healthGeneral PC, women’s, gyn and mental health– Half-day sessions open, service availabilityHalf-day sessions open, service availability
Privacy/sensitivityPrivacy/sensitivity– Physical space arrangements (exclusive, reserved vs. Physical space arrangements (exclusive, reserved vs.
shared exam rooms and waiting rooms)shared exam rooms and waiting rooms)– % same-gender providers available% same-gender providers available
Service availability Service availability (VA vs. not, on vs. offsite)(VA vs. not, on vs. offsite)– Basic women’s health services (e.g., paps, mamms)Basic women’s health services (e.g., paps, mamms)– Specialized women’s health services (e.g., breast Specialized women’s health services (e.g., breast
cancer surgery, prenatal care)cancer surgery, prenatal care)
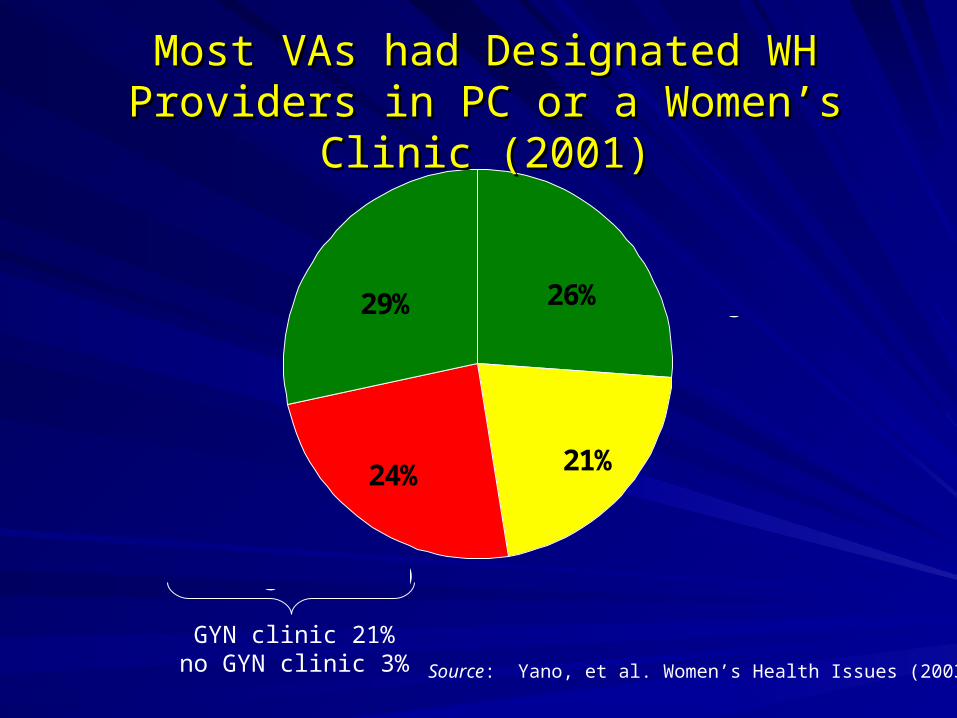
21%24%
26%29%
Women's Health Clinics (WHC)
ONLY
Designated WHProvider in Integrated
PC ONLY
WHC AND Designated WH
Provider in Integrated PC
Integrated PC(no designated WH)
GYN clinic 21%no GYN clinic 3% Source: Yano, et al. Women’s Health Issues (2003)
Most VAs had Designated WH Providers in PC Most VAs had Designated WH Providers in PC or a Women’s Clinic (2001)or a Women’s Clinic (2001)
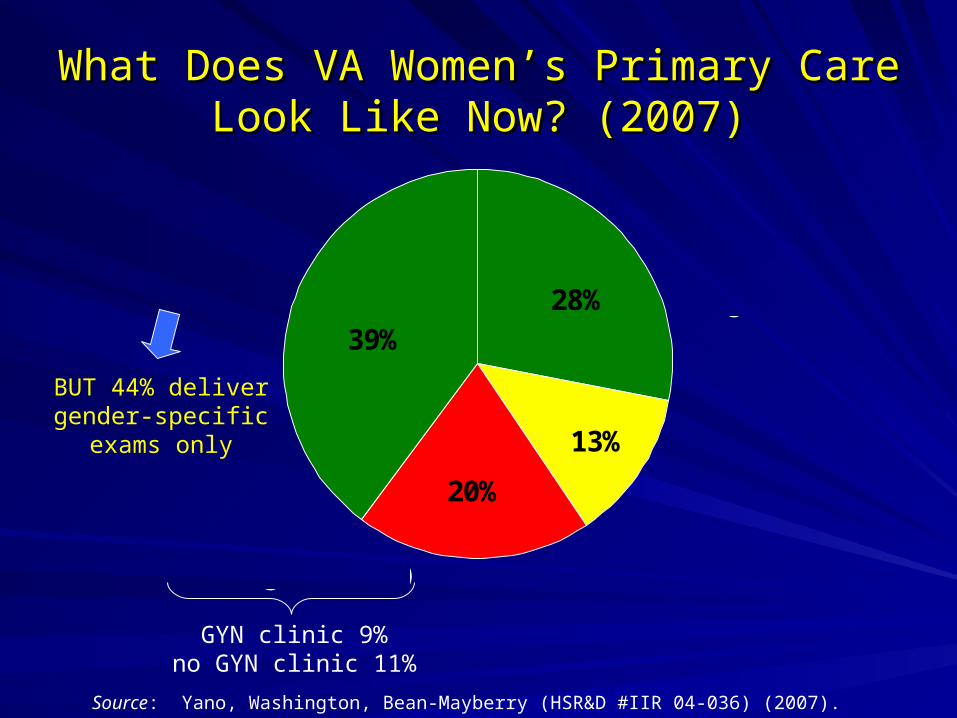
What Does VA Women’s Primary Care Look What Does VA Women’s Primary Care Look Like Now? (2007)Like Now? (2007)
13%
20%
28%39%
Women's Health Clinics (WHC)
ONLY
Designated WHProvider in Integrated
PC ONLY
WHC AND Designated WH
Provider in Integrated PC
Integrated PC(no designated WH)
Source: Yano, Washington, Bean-Mayberry (HSR&D #IIR 04-036) (2007).
BUT 44% delivergender-specific
exams only
GYN clinic 9%no GYN clinic 11%
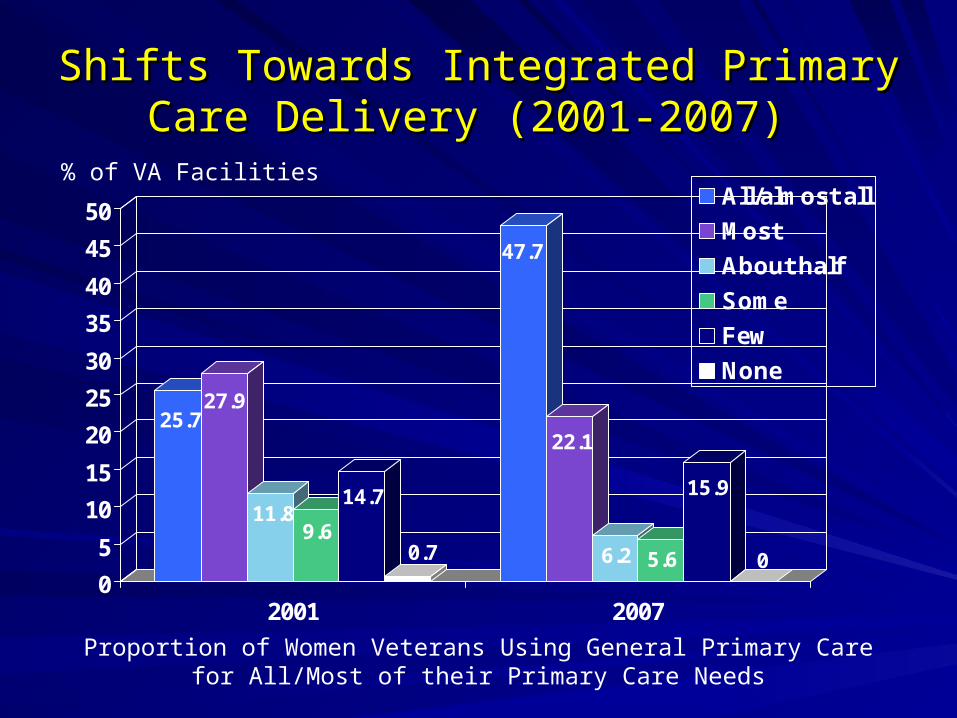
Shifts Towards Integrated Primary Care Shifts Towards Integrated Primary Care Delivery (2001-2007) Delivery (2001-2007)
25.727.9
11.89.6
14.7
0.7
47.7
22.1
6.2 5.6
15.9
00
5
10
15
20
25
30
35
40
45
50
2001 2007
All/almost all
Most
About half
Some
Few
None
% of VA Facilities
Proportion of Women Veterans Using General Primary Carefor All/Most of their Primary Care Needs
Integrated Primary Care (2007)Integrated Primary Care (2007)
42% of VAs have designated WH providers in 42% of VAs have designated WH providers in general PC to whom women veterans are general PC to whom women veterans are preferentially assignedpreferentially assigned– 56% have 56% have oneone for whole PC practice for whole PC practice– 9% have 9% have oneone in each PC team in each PC team– 18% have a WH primary care team18% have a WH primary care team– Others: randomly assigned, count NPs, no specificsOthers: randomly assigned, count NPs, no specifics
Lack adequate clinical expertise in WH (p<.05)Lack adequate clinical expertise in WH (p<.05)Lack same-gender providers (p<.01) Lack same-gender providers (p<.01) (32% vs. 74%)(32% vs. 74%)
Designated WH providers only available Designated WH providers only available 6 half-6 half-day sessions/weekday sessions/week
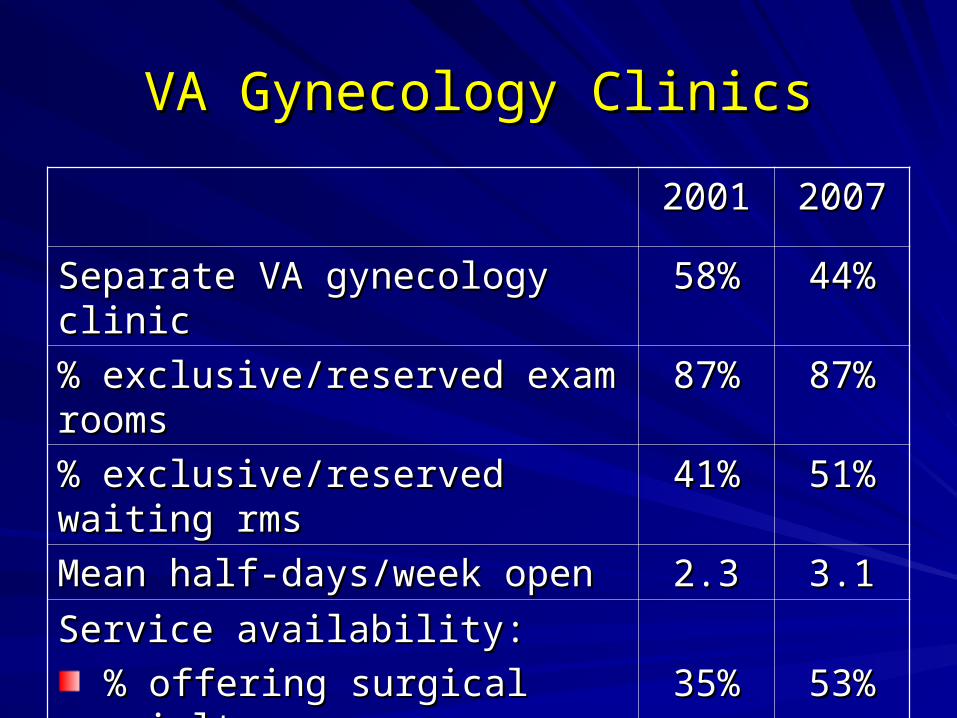
VA Gynecology ClinicsVA Gynecology Clinics
20012001 20072007
Separate VA gynecology clinicSeparate VA gynecology clinic 58%58% 44%44%
% exclusive/reserved exam rooms% exclusive/reserved exam rooms 87%87% 87%87%
% exclusive/reserved waiting rms% exclusive/reserved waiting rms 41%41% 51%51%
Mean half-days/week openMean half-days/week open 2.32.3 3.13.1
Service availability:Service availability:
% offering surgical specialty% offering surgical specialty
% offering obstetrical care% offering obstetrical care
35%35%
10%10%
53%53%
7%7%

VA Mental Health Care for WomenVA Mental Health Care for Women
20012001 20072007
% designated WH providers in % designated WH providers in general outpatient mental healthgeneral outpatient mental health
mean half-days/week openmean half-days/week open
% same-gender provider avail*% same-gender provider avail*
43%43%
5.75.7
41%41%
34%34%
6.96.9
69%69%
% separate women’s MH clinic% separate women’s MH clinic
% exclusive/reserved rooms% exclusive/reserved rooms
% exclusive/reserved waiting rms% exclusive/reserved waiting rms
% same-gender providers*% same-gender providers*
mean half-days/week openmean half-days/week open
11%11%
14%14%
33%33%
67%67%
4.44.4
12%12%
58%58%
38%38%
63%63%
5.85.8*All/most of the time

Women’s Health Service AvailabilityWomen’s Health Service Availability
0% 20% 40% 60% 80% 100%
Menopausalmanagement
Endometrialbiopsy
Vaginitisevaluation
Screeningmammography
Cervical cancerscreening
Onsite VA
Other VA
Non-VANon-VA referrals
Available onsite
Available onsite
Available onsite
Available onsite Other VA
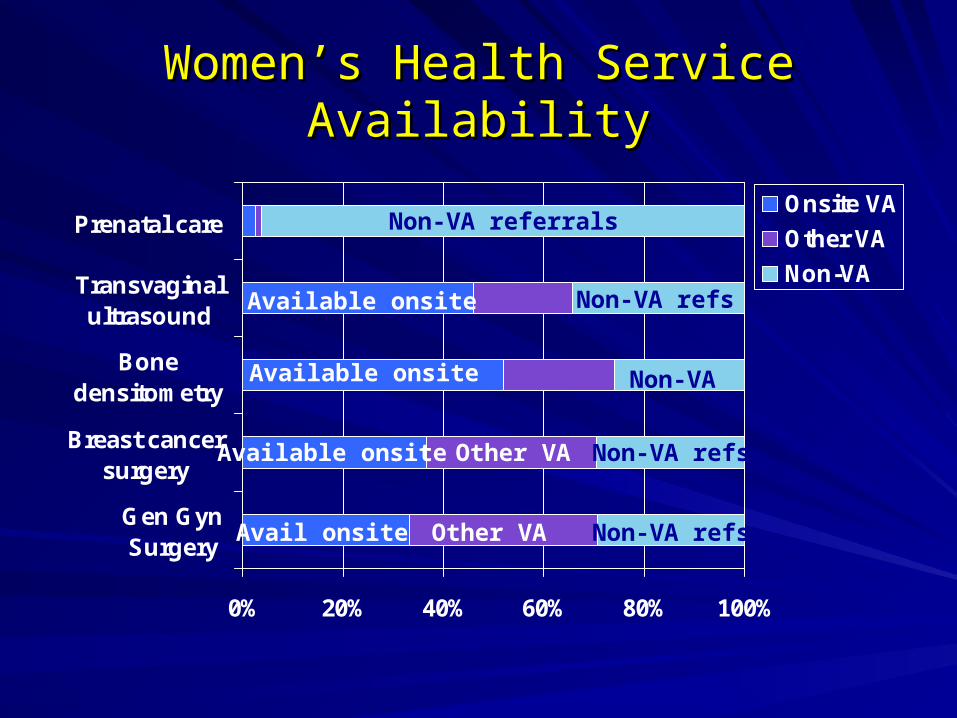
Women’s Health Service AvailabilityWomen’s Health Service Availability
0% 20% 40% 60% 80% 100%
Gen GynSurgery
Breast cancersurgery
Bonedensitometry
Transvaginalultrasound
Prenatal careOnsite VA
Other VA
Non-VAAvailable onsite
Available onsite
Available onsite Other VA
Other VA
Non-VA referrals
Non-VA refs
Non-VA refs
Non-VA refsAvail onsite
Non-VA
ConclusionsConclusions
Designating a WH provider in general PC a Designating a WH provider in general PC a common approachcommon approach– Meaning of designation unclear (training, clinical Meaning of designation unclear (training, clinical
experience, organizational supports)experience, organizational supports)
Growth of women’s clinics balanced by focus on Growth of women’s clinics balanced by focus on gender-specific examsgender-specific exams– Increased fragmentation rather than one-stop Increased fragmentation rather than one-stop
shopping modelshopping model– Gender-sensitive mental health provision lagsGender-sensitive mental health provision lags
VA facilities split in decision to improve onsite VA facilities split in decision to improve onsite capability to deliver WH care (build vs. buy)capability to deliver WH care (build vs. buy)
ImplicationsImplications
VA will continue to face challenges in ensuring VA will continue to face challenges in ensuring high-quality care for women veteranshigh-quality care for women veterans– Recent influx increases demand for evidence-based Recent influx increases demand for evidence-based
management solutionsmanagement solutions
Early evidence demonstrates better outcomes Early evidence demonstrates better outcomes for separate women’s clinics for:for separate women’s clinics for:– Gender-specific processes of care (e.g., paps)Gender-specific processes of care (e.g., paps)– Patient ratings of care (e.g., accessibility, continuity)Patient ratings of care (e.g., accessibility, continuity)– But less clear advantages for gender-neutral quality But less clear advantages for gender-neutral quality
(e.g., diabetes quality, colorectal cancer screening)(e.g., diabetes quality, colorectal cancer screening)
Future work needed to develop evidence-based Future work needed to develop evidence-based implementation plans that map to local structureimplementation plans that map to local structure















![Yano Et Al., 1997 Prediction of the Concentrations of EtOH and AcOH[1]](https://static.fdocuments.in/doc/165x107/577cd52d1a28ab9e789a1519/yano-et-al-1997-prediction-of-the-concentrations-of-etoh-and-acoh1.jpg)

