
WCCG PRIMARY CARE COMMITTEE PT1 - Wandsworth CCG · Councillor Paul Ellis (PE) London Borough of...
88
WCCG PRIMARY CARE COMMITTEE PT1 MEETING 4 September 2018 09:30 PUBLISHED 31 August 2018
Transcript of WCCG PRIMARY CARE COMMITTEE PT1 - Wandsworth CCG · Councillor Paul Ellis (PE) London Borough of...

WCCG PRIMARY CARE COMMITTEE PT1
MEETING4 September 2018 09:30
PUBLISHED31 August 2018

W A N D S W O R T H C C G P A G E 1 O F 1
Board Intelligence Hub template
Primary Care Committee Agenda 4th September at 9:30 East Putney
Meeting of the Primary Care Committee
Tuesday, 4th September 2018
9:30 – 11:00
73-75 Upper Richmond Road, East Putney
AGENDA – PART 1
P A R T A | M E E T I N G O P E N S T A R T D U R A T I O N
A01 Apologies, Declarations, Quorum CV 9:30 5 mins
A02 Chair’s Opening Remarks CV 9:35 5 mins
A03 Minutes 5th June 2018: Approval and Status
of Actions CV 9:40 5 mins
P A R T B | D E C I S I O N S A N D D I S C U S S I O N S
B01 Primary Care at Scale Update KD 9:45 30 mins
B02 Terms of Reference CV 10:15 15 mins
B03 Primary Care Operating Model NS 10:30 15 mins
B04 Primary Care Commissioning Update (incl
Finance Report)
KS, EG,
NMcD 10:45 10 mins
B05 Any Other Business CV 10:55 5 mins
P A R T C | P A R T 1 M E E T I N G C L O S E
C01 Chair’s Closing Remarks CV
C02 Close of Part 1
11:00
W A N D S W O R T H C C G P A G E 1 O F [ X ] W A N D S W O R T H C C G P A G E 1 O F [ X ]

Agenda
Location Date Owner Time
Putney 4/09/18 09:30
Agenda
1. Part A: Meeting Open
1.1. A01 Apologies, Declarations, Quorum 09:30
1.2. A02 Chair's Opening Remarks 09:35
1.3. A03 Minutes: Approval and Status of Actions 09:40
1.4. A04 Items for AOB
2. Part B: Decisions and Discussions
2.1. B01 Primary Care at Scale - Proposed Use of Funding 09:45
2.2. B02 Terms of Reference 10:15
2.3. B03 Primary Care Operating Model 10:30
2.4. B04 Integrated Primary Care Update 10:45
2.5. B05 Any Other Business 10:55
3. Part C: Meeting Close
3.1. C01 Chair's Closing Remarks
1.Part A
: Meeting O
pen2.
Part B: D
ecisions and Discussions
3.Part C
: Meeting C
lose
3

Contents
Page
1. Part A: Meeting Open 5
1.1. A01 Apologies, Declarations, Quorum 5
1.2. A02 Chair's Opening Remarks
1.3. A03 Minutes: Approval and Status of Actions 8
1.4. A04 Items for AOB
2. Part B: Decisions and Discussions 12
2.1. B01 Primary Care at Scale - Proposed Use of Funding 12
2.2. B02 Terms of Reference
2.3. B03 Primary Care Operating Model 22
2.4. B04 Integrated Primary Care Update 83
2.5. B05 Any Other Business
3. Part C: Meeting Close
3.1. C01 Chair's Closing Remarks
1.Part A
: Meeting O
pen2.
Part B: D
ecisions and Discussions
3.Part C
: Meeting C
lose
4

Name
Current position (s) held in the
CCG i.e. Governing Body member;
Committee member; Member
practice; CCG employee or other
Do you
have any
interests
to
declare?
(Y or N)
Declared Interest
(Name of the organisation and nature of business)
Fin
an
cia
l In
tere
st
No
n-F
ina
nc
ial
pro
fes
sio
na
l
Inte
res
t
No
n-F
ina
nc
ial
Pe
rso
na
l In
tere
st
Ind
ire
ct
Inte
res
t
Nature of Interest
From To
Action taken to
mitigate risk
James Blythe Managing Director
Merton CCG Governing Body
Wandsworth CCG Board
Member of Executive Management
Team
Member of Primary Care Commissioning
Committee
LDU Finance Committee in Common
Member of Integrated Governance
Quality Committee
Y
1. Wife is an employee of St George's University Hospitals NHS
Foundation Trust and has a specialist training number with HEE
South London
1 1. May 2017 1. I am not present
at specific
discussions relating
to the relevant
service.
Neil McDowell Director of Finance
Member of Governing Body
Member of Finance Committee
Member of Audit & Governance
Committee
Member of Primary Care Commissioning
Committee
Member of Executive Management
Committee
Member of Integrated Governance and
Quality Committee
Y
1. Spouse employed by Guildford and Waverley CCG as CFO
Julie Hesketh Director of Quality and Corporate
Governance
Member of Governing Body
Member of Executive Management
Committee
Member of Integrated Governance and
Quality Committee
Member of Audit and Governance
Committee
Y
1. Personal involvement in Richmond Education Network (not for
profit organisation). This is done outside of CCG hours.
Andy McMylor Director of Primary Care Transformation
Member of Governing Body
Member of Executive Management
Committee
Member of Primary Care Commissioning
Committee
N
No Interests Declared
Register of Interests 2018/19 (updated August 2018)
1.P
art A: M
eeting O
pen
2.Part B
: Decisions and D
iscussions3.
Part C: M
eeting Close
5

Name
Current position (s) held in the
CCG i.e. Governing Body member;
Committee member; Member
practice; CCG employee or other
Do you
have any
interests
to
declare?
(Y or N)
Declared Interest
(Name of the organisation and nature of business)
Fin
an
cia
l In
tere
st
No
n-F
ina
nc
ial
pro
fes
sio
na
l
Inte
res
t
No
n-F
ina
nc
ial
Pe
rso
na
l In
tere
st
Ind
ire
ct
Inte
res
t
Nature of Interest
From To
Action taken to
mitigate risk
John Atherton Director of Performance Improvement
Member of Governing Body
Member of Primary Care Commissioning
Committee
Member of Integrated Governance and
Quality Committee
Member of Executive Management
Committee
N
No interests declared
Josh Potter Director of Commissioning Member
of Governing Body
Member of Executive Management
Committee
Member of Primary Care
Commissioning Committee
Member of Integrated Governance
and Quality Committee
N
No interests declared
Stephen Hickey Lay Member,
Governance Wandsworth - Health and
Wellbeing Board; Wandsworth CCG -
Governing Body (Vice Chair);
Finance Committee in Common; Audit
Committee (Chair); Remuneration
Committee (Chair);
Workforce Committee;
Primary Care Committee; Integrated
Quality & Governance Committee
Y
1. Trustee for Merton Community Transport Charity 1 1. 01/12/2017 Transparency if
relevant issues
arise
Mike Lane Governing Body voting member
CCG Deputy Clinical Chair
Joint Wandle Locality Lead
South West London - Clinical Advisory
Group member
Clinical Lead for Maternity Clinical
Design Group
Member of Integrated Governance
Quality Committee
Wandsworth Primary Care Committee
Y
1. GP Partner - Grafton Medical Partners.
2. GP Partner - Lambton Road Medical Partnership.
3. Practice is a member of Battersea Healthcare CIC but Dr Lane
holds no director post and has no specific responsibilities within
that organisation other than those of other member GP.
4. London Maternity Lead, Royal College of General Practitioners.
5. Volunteer Doctor - Crisis Homeless charity.
6. Volunteer Doctor - St Johns Ambulance Charity.
7. Member - National Maternity Transformation Board
Stakeholder
1
2
3
4
5
6
7
1. 1999
2. 2013
3. 2014
4. 2006
5. 2006
6. 2016
7. 2016
1-7 Adherence to
COI policy
1.P
art A: M
eeting O
pen
2.Part B
: Decisions and D
iscussions3.
Part C: M
eeting Close
6
Name
Current position (s) held in the
CCG i.e. Governing Body member;
Committee member; Member
practice; CCG employee or other
Do you
have any
interests
to
declare?
(Y or N)
Declared Interest
(Name of the organisation and nature of business)
Fin
an
cia
l In
tere
st
No
n-F
ina
nc
ial
pro
fes
sio
na
l
Inte
res
t
No
n-F
ina
nc
ial
Pe
rso
na
l In
tere
st
Ind
ire
ct
Inte
res
t
Nature of Interest
From To
Action taken to
mitigate risk
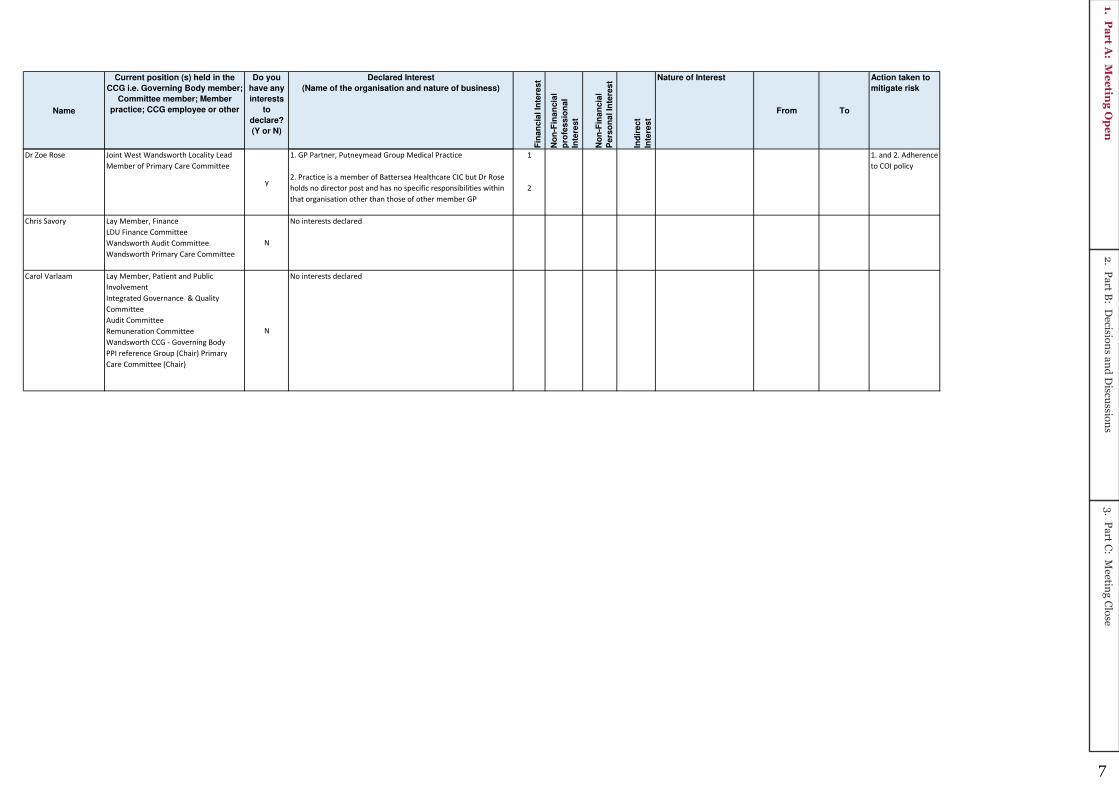
Dr Zoe Rose Joint West Wandsworth Locality Lead
Member of Primary Care Committee
y
1. GP Partner, Putneymead Group Medical Practice
2. Practice is a member of Battersea Healthcare CIC but Dr Rose
holds no director post and has no specific responsibilities within
that organisation other than those of other member GP
1
2
1. and 2. Adherence
to COI policy
Chris Savory Lay Member, Finance
LDU Finance Committee
Wandsworth Audit Committee
Wandsworth Primary Care Committee
N
No interests declared
Carol Varlaam Lay Member, Patient and Public
Involvement
Integrated Governance & Quality
Committee
Audit Committee
Remuneration Committee
Wandsworth CCG - Governing Body
PPI reference Group (Chair) Primary
Care Committee (Chair)
N
No interests declared
1.P
art A: M
eeting O
pen
2.Part B
: Decisions and D
iscussions3.
Part C: M
eeting Close
7

1
Minutes of the meeting of the Primary Care Commissioning Committee (Part 1) held on
5th June 2018
Chair: Carol Varlaam Present: Voting Members Carol Varlaam (CV) Lay Member, Patient and Public Involvement Dr Nicola Jones (NJ) CCG Chair Nick Cuff (NC) Associate Lay Member Julie Hesketh (JHe) Director of Quality and Governance Neil McDowell (NM) Director of Finance Andrew McMylor (AMc) Director of Primary Care Transformation Non-Voting Members Dr Zoe Rose (ZR) West Wandsworth LCG Lead Dr Nicola Williams (NW) Clinical Director Battersea Mr James Gillespie (JG) Wandsworth Healthwatch Councillor Paul Ellis (PE) London Borough of Wandsworth In attendance:
Katharine Denton (KD) Deputy Director of Primary Care Development Emma Gillgrass (EG) Locality Management Lead Battersea; Merton
and Wandsworth CCGs Kate Symons (KS) Acting Head of Delegated Primary Care
Commissioning, Wandsworth & Merton LDU Nora Simon (NS) NHS England Tony Foote (TF) Note Taker, NEL CSU
18/011
Apologies, Declarations, Quorum
Apologies were received from: Stephen Hickey, Chris Savory, Dr Mike Lane, John Atherton, William Cunningham-Davis, James Blythe.
No conflicts of interest were declared.
With regard to quoracy, CV noted that, with only six voting members should be present, the meeting was not quorate.
18/012
Clinical Chair’s Opening Remarks
CV referred back to the issue of quoracy and that the Terms of Reference had been scheduled for review at his meeting – however, there were deferred to the September meeting. At that meeting there would be a full review, with particular regard to the membership and quoracy requirements.
18/013
Minutes of Previous Meeting on 6th March 2018
The minutes of the previous meeting on 6th March 2017 were agreed as an accurate record.
18/014
Primary Care at Scale – Proposed Use of Funding
KD presented this item and explained that strong Primary Care, specifically
1.P
art A: M
eeting O
pen
2.Part B
: Decisions and D
iscussions3.
Part C: M
eeting Close
8

2
General Practice, was at the heart of any high quality and sustainable health system. With this in mind, national literature increasingly describes practices working together or ‘at scale’ as a solution to many of the challenges facing Primary Care, having benefits for patients and practices themselves as well as the wider health system.
Although there was no single definition for ‘Primary Care at Scale, there have been identified five key components:
- Comprehensive population based - Systems, information and quality improvement - Organisational capabilities - Effective governance and stewardship - Building collaborative system partnerships
The Wandsworth GP Federation was commissioned to complete an initial scoping exercise for developing Primary Care at Scale across the Borough. This was completed and the project was now looking to move on to the implementation and delivery phase at pace.
Wandsworth CCG initiated discussions with practices across the Borough regarding Primary Care at Scale in October 2017 at a Joint Locality Members Forum meeting. Practices identified the GP Federation as being a key enabler for delivering Primary Care at Scale. It was also recognised that stakeholder engagement and bottom up development would be critical to the successful development of Primary Care at Scale and the GP Federation had already established strong working links with key stakeholders and practices across the borough enabling productive conversations and developing ways to improve or change to benefit the system as a whole.
A paper detailing the allocation of new funding of circa £600,000 to the Primary Care at Scale work programme in Wandsworth was approved by the CCG’s Board and the South West London Committee in Common in March 2018. The proposed use of this funding was as follows:
Objectives Budget Phase 1 Working Group Facilitation £30,000 Practice Protected Time £65,000 Workforce Development & Retention £45,000 Project Management £71,500 Quality System £50,000 Legal & Financial Advice £17,500 Procurement £10,000 Nurse Training £20,000 Pilots £20,000 Phase 2 GP Network Leadership & Governance £54,500 Project Management £71,500 Practice Protected Time £42,500 Legal & Financial Advice £20,000 Practice Protected Time £42,500 Total £600,000
The Committee asked how the contract with the GP Federation would be monitored. KD explained that this would be done as follows:
- Monthly monitoring meetings - KPIs for sub-contractors - KOIs for overarching issues
1.P
art A: M
eeting O
pen
2.Part B
: Decisions and D
iscussions3.
Part C: M
eeting Close
9

3
- Regular CQRG meetings - Regular Transformation meetings
NJ felt there should be more detail about IT issues included in the proposal as well as greater transparency as to what use the funds were being put to.
The Primary Care Committee APPROVED the proposal for the use of funding.
18/015
Integrated Primary Care Update Report (inc. Finance Report)
KS presented this item and highlighted the following issues:
PMS & GMS Update All Practices received their GMS equivalent PMS Offer in March and all nine practices have retuned their signed contact. Accordingly, the CCG will be meeting the government requirement for full PMS and GMS equalisation by 2020.
Testing of reporting and monitoring systems has been undertaken with local LMC Practices and constructive comments have been received. These have been fed into the final templates and the Primary Care Team will continue to report the progress against the KPI’s to the Committee on a six monthly basis.
The Begg Practice Boundary Change This Practice submitted an application to NHS England and the CCG to reduce the practice catchment area from that which is presently agreed. This request was made by the Practice in order to remain sustainable under the growing pressures of an increasing list size; which has grown 56% in three years. The practice reported that there were 13 patients who would reside outside of the proposed boundary change, however the practice reported that they would continue to provide these patients with the same level of service including home visits.
The Primary Care Operational Group (PCOG) reviewed this and agreed the change in boundary in principle subject to the Practice providing further evidence of Patient Participation Group (PPG) support of the boundary change and assurances of the capacity of other local practices that may be impacted by the change. This information was provided and, following a capacity analysis conducted by NHSE, the PCOG were able to confirm the initial decision to support the proposed boundary change.
Changes and Updates to the NHS England Primary Care Policy Guidance The Committee was asked to note an updated version of the NHSE Primary Medical Care Policy and Guidance Manual (PGM). The policy document has been updated to reflect the changing landscape in primary care co-commissioning and includes a new chapter on Discretionary Payments.
Providing Primary Care Services to Care Home Residents Following an earlier update to the PCC on some of the queries raised about registering care home patients with local practices, a detailed communication was sent to all Wandsworth Practices confirming their contractual requirements. Unfortunately, local care homes were still reporting difficulties in registering their residents at local practices and, therefore, further discussions were needed locally.
The issue of primary care provision to care home residents continued to prove challenging and The Federation would look at the key issues of providing on going primary care management to such patients.
Joint Primary Care Quality Review Group (PCQRG) Update EG presented this item and explained that at its May meeting the Joint PCQRG
1.P
art A: M
eeting O
pen
2.Part B
: Decisions and D
iscussions3.
Part C: M
eeting Close
10

4
discussed how the learning from the review of CQC reports and the discussions of the group could be disseminated more widely across both CCGs. There was a specific focus on sharing the learning from CQC inspections, specifically highlighting the common themes that were identified across where practices were asked to make improvements. The paper also provided detailed examples of those areas where practices had been rated as outstanding, and it was agreed that these were a positive list of examples of good practice that should be shared with all practices.
The Primary Care Committee NOTED the Integrated Primary Care Update Report.
NM then presented the Primary Care Finance Report and highlighted the following:
- The Primary Care budget reported a year-end underspend of £569k. - There was a small underspend of £32k within core budgets, partially off-
setting the cost pressure of locum costs. - The overspend on PMS core budgets includes £100k overspend on
payment to the Royal Hospital for Neuro-Disability. - Premises costs were £387k below budget. - A underspend of £71k on the DES budget. - The retained GPs’ scheme was £101k over budget. - Overspend on GP and Central Prescribing Budget: this included factored
in the revised cost pressure of £1.5m relating to NCSO. - Prescribing achieved its planned level of QIPP. - An underspend of £48k on other areas of primary care.
The Primary Care Committee NOTED the Primary Care Finance Report.
18/016
Any Other Business
There was no additional business for consideration.
18/017 Close of Part 1
ACTIONS
Item Lead
Clinical Chair’s Opening Remarks CV informed the Committee that the issue of quoracy and that the Terms of Reference had been scheduled for review at his meeting – however, there were deferred to the September meeting. At that meeting there would be a full review, with particular regard to the membership and quoracy requirements.
MA
1.P
art A: M
eeting O
pen
2.Part B
: Decisions and D
iscussions3.
Part C: M
eeting Close
11
W A N D S W O R T H C C G P A G E 1 O F 2
Strictly Confidential Board Intelligence Hub template
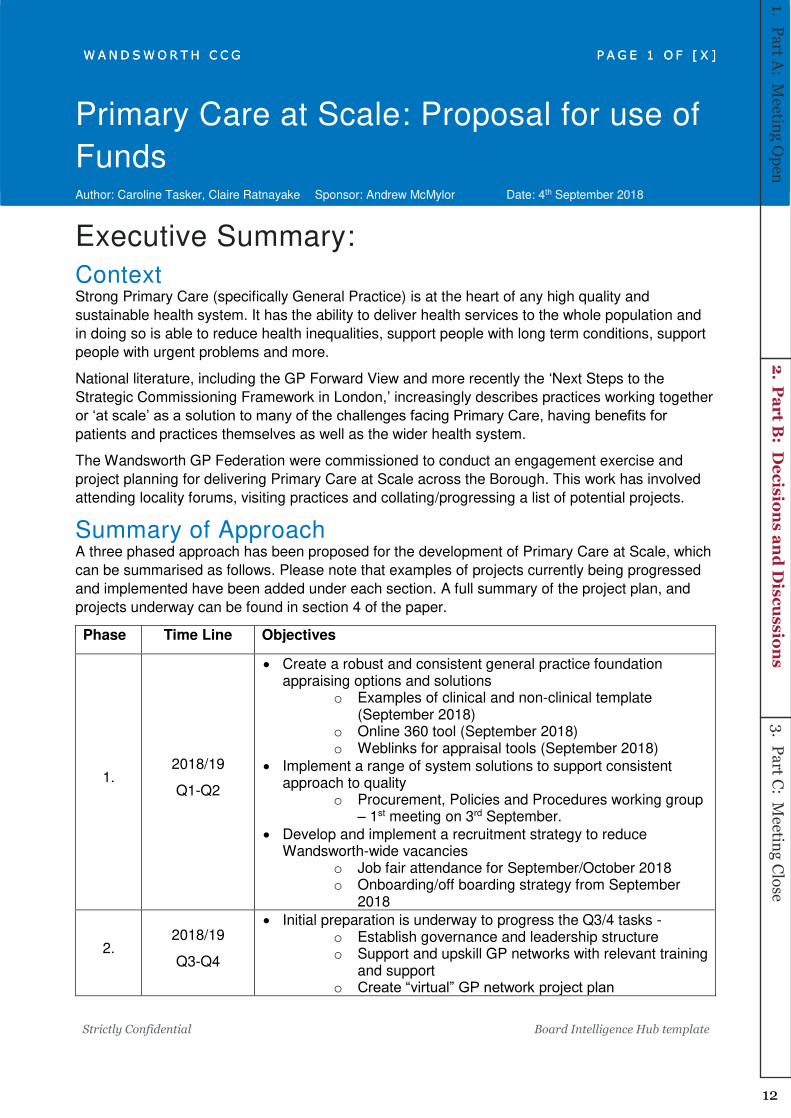
Primary Care at Scale: Proposal for use of
Funds Author: Caroline Tasker, Claire Ratnayake Sponsor: Andrew McMylor Date: 4th September 2018
Executive Summary:
Context Strong Primary Care (specifically General Practice) is at the heart of any high quality and
sustainable health system. It has the ability to deliver health services to the whole population and
in doing so is able to reduce health inequalities, support people with long term conditions, support
people with urgent problems and more.
National literature, including the GP Forward View and more recently the ‘Next Steps to the
Strategic Commissioning Framework in London,’ increasingly describes practices working together
or ‘at scale’ as a solution to many of the challenges facing Primary Care, having benefits for patients and practices themselves as well as the wider health system.
The Wandsworth GP Federation were commissioned to conduct an engagement exercise and
project planning for delivering Primary Care at Scale across the Borough. This work has involved
attending locality forums, visiting practices and collating/progressing a list of potential projects.
Summary of Approach A three phased approach has been proposed for the development of Primary Care at Scale, which
can be summarised as follows. Please note that examples of projects currently being progressed
and implemented have been added under each section. A full summary of the project plan, and
projects underway can be found in section 4 of the paper.
Phase Time Line Objectives
1. 2018/19
Q1-Q2
Create a robust and consistent general practice foundation appraising options and solutions
o Examples of clinical and non-clinical template (September 2018)
o Online 360 tool (September 2018) o Weblinks for appraisal tools (September 2018)
Implement a range of system solutions to support consistent approach to quality
o Procurement, Policies and Procedures working group – 1st meeting on 3rd September.
Develop and implement a recruitment strategy to reduce Wandsworth-wide vacancies
o Job fair attendance for September/October 2018 o Onboarding/off boarding strategy from September
2018
2. 2018/19
Q3-Q4
Initial preparation is underway to progress the Q3/4 tasks - o Establish governance and leadership structure o Support and upskill GP networks with relevant training
and support o Create “virtual” GP network project plan
W A N D S W O R T H C C G P A G E 1 O F [ X ]
W A N D S W O R T H C C G P A G E 1 O F [ X ]
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
12

W A N D S W O R T H C C G P A G E 2 O F 2
Strictly Confidential Board Intelligence Hub template
2019/20 Launch GP network project plan (Q1)
Monitor progress against plan
3. 2-5 year plan Whole population budgets
Ongoing individual practice visits will run alongside the three phase approach to ensure local aims
and related benefits are considered as part of the project implementation phase.
Input Sought Input Received The Primary Care Committee are asked to
note the progress made to date and to
approve the direction of travel for this
programme.
As recommended by NHS England, funding
and delivery will be delegated to Battersea
Healthcare Community Interest Company
as a variation to the MCP contract. This is
aligned with the originally stated aims and
objectives of the MCP; to be the key vehicle
for delivery of Primary Care Transformation
and ensure achievement of the
requirements set out in the London
Strategic Commissioning Framework for
Primary Care.
Governance and monitoring of delivery will
be carried out as part of the wider MCP
governance structure.
Initial approach agreed by Wandsworth
Primary Care Committee in March 2018.
Proposal for use of funding, including early
release of Q1 money to the GP Federation to
kick-start implementation plan, was approved
by the Wandsworth and Merton Executive
Management Team in April 2018.
Plans have also been approved as part of a
South West London led, NHS England
Assurance process which took place on the 9th
May 2018.
Input from practices has been sought via
locality forums and individual practice visits.
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
13
1
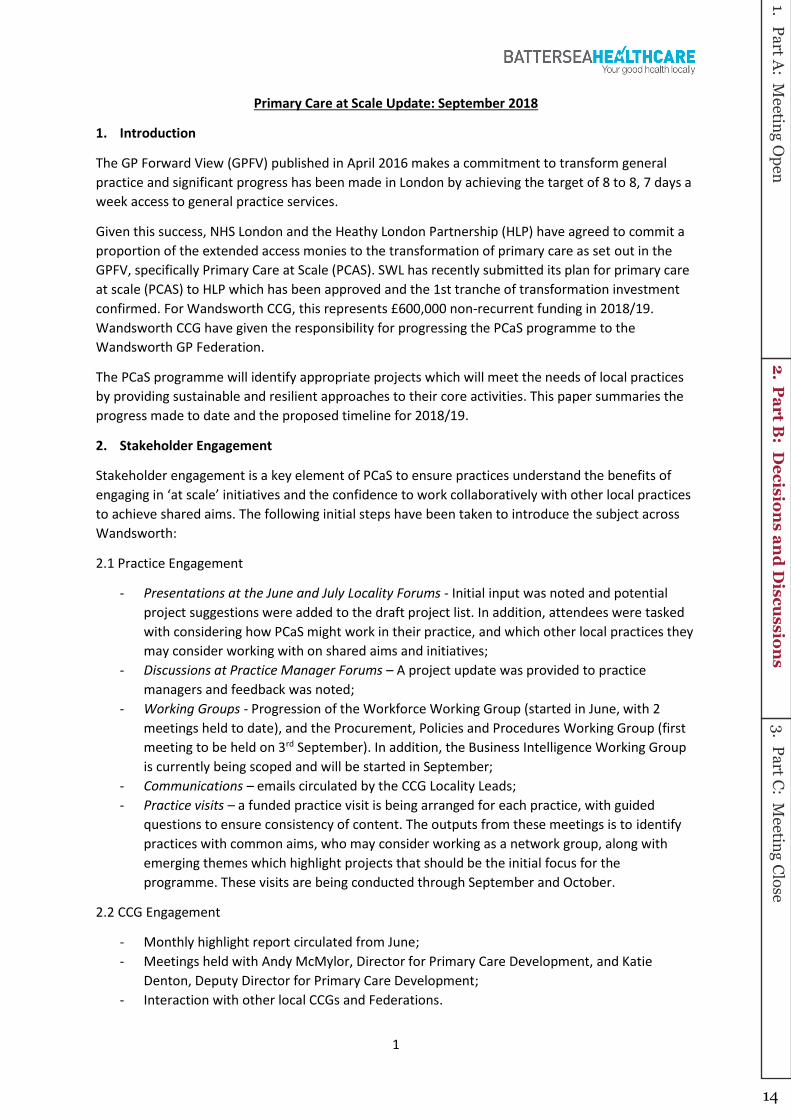
Primary Care at Scale Update: September 2018
1. Introduction
The GP Forward View (GPFV) published in April 2016 makes a commitment to transform general
practice and significant progress has been made in London by achieving the target of 8 to 8, 7 days a
week access to general practice services.
Given this success, NHS London and the Heathy London Partnership (HLP) have agreed to commit a
proportion of the extended access monies to the transformation of primary care as set out in the
GPFV, specifically Primary Care at Scale (PCAS). SWL has recently submitted its plan for primary care
at scale (PCAS) to HLP which has been approved and the 1st tranche of transformation investment
confirmed. For Wandsworth CCG, this represents £600,000 non-recurrent funding in 2018/19.
Wandsworth CCG have given the responsibility for progressing the PCaS programme to the
Wandsworth GP Federation.
The PCaS programme will identify appropriate projects which will meet the needs of local practices
by providing sustainable and resilient approaches to their core activities. This paper summaries the
progress made to date and the proposed timeline for 2018/19.
2. Stakeholder Engagement
Stakeholder engagement is a key element of PCaS to ensure practices understand the benefits of
e gagi g i at s ale i itiati es a d the o fide e to o k olla o ati ely ith othe lo al p a ti es to achieve shared aims. The following initial steps have been taken to introduce the subject across
Wandsworth:
2.1 Practice Engagement
- Presentations at the June and July Locality Forums - Initial input was noted and potential
project suggestions were added to the draft project list. In addition, attendees were tasked
with considering how PCaS might work in their practice, and which other local practices they
may consider working with on shared aims and initiatives;
- Discussions at Practice Manager Forums – A project update was provided to practice
managers and feedback was noted;
- Working Groups - Progression of the Workforce Working Group (started in June, with 2
meetings held to date), and the Procurement, Policies and Procedures Working Group (first
meeting to be held on 3rd September). In addition, the Business Intelligence Working Group
is currently being scoped and will be started in September;
- Communications – emails circulated by the CCG Locality Leads;
- Practice visits – a funded practice visit is being arranged for each practice, with guided
questions to ensure consistency of content. The outputs from these meetings is to identify
practices with common aims, who may consider working as a network group, along with
emerging themes which highlight projects that should be the initial focus for the
programme. These visits are being conducted through September and October.
2.2 CCG Engagement
- Monthly highlight report circulated from June;
- Meetings held with Andy McMylor, Director for Primary Care Development, and Katie
Denton, Deputy Director for Primary Care Development;
- Interaction with other local CCGs and Federations.
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
14

2
2.3 Patient Engagement
- PCaS discussed at patient forums and suggestions included in the project ideas being
collated.
Going forwards, all the above points will be continued. In addition, research is currently being
conducted to ascertain whether facilitated groups to discuss aims and networking grouping would
be beneficial. This is potentially seen as phase 2 of the engagement plan.
3. Project Planning And Key Milestones
The PCaS project plan is currently on track with all tasks and related milestones. The broad headings
of the tasks being completed to date are:
- Engagement
- PCaS documentation
- Establishing working groups
- Project implementation
- Evaluation
4. Progress against plan by end of September
A 3 phased approach was initially signed off by Wandsworth CCG for Battersea Healthcare CIC to
progress the Primary Care at Scale programme. The 3 phases are:
Phase 1: April – September 2018
- Establish 3 network groups
- Review projects and scope out project plans
Phase 2a: October 2018 – March 2019
- Initiating 4 pilots
- Start discussions with practices about network models
- Develop governance framework
- Develop leadership structure with clear responsibilities
- Support and upskill GP networks and create delivery plan
Phase 2b: January 2019 onwards
- Launch GP network delivery plan
- Provide ongoing support and monitor progress
Phase 3: 2-5 year plan
An update of progress against these milestones can be found in Appendix 1. A summary of the full
PCaS project plan and the main tasks being progressed to date are:
- Engagement
o General engagement (ongoing, update as per section 2)
o Facilitation sessions (ongoing, initial review of usefulness of this underway)
o Discussed at patient forums, and information fed into the feedback being collated
(ongoing)
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
15
3
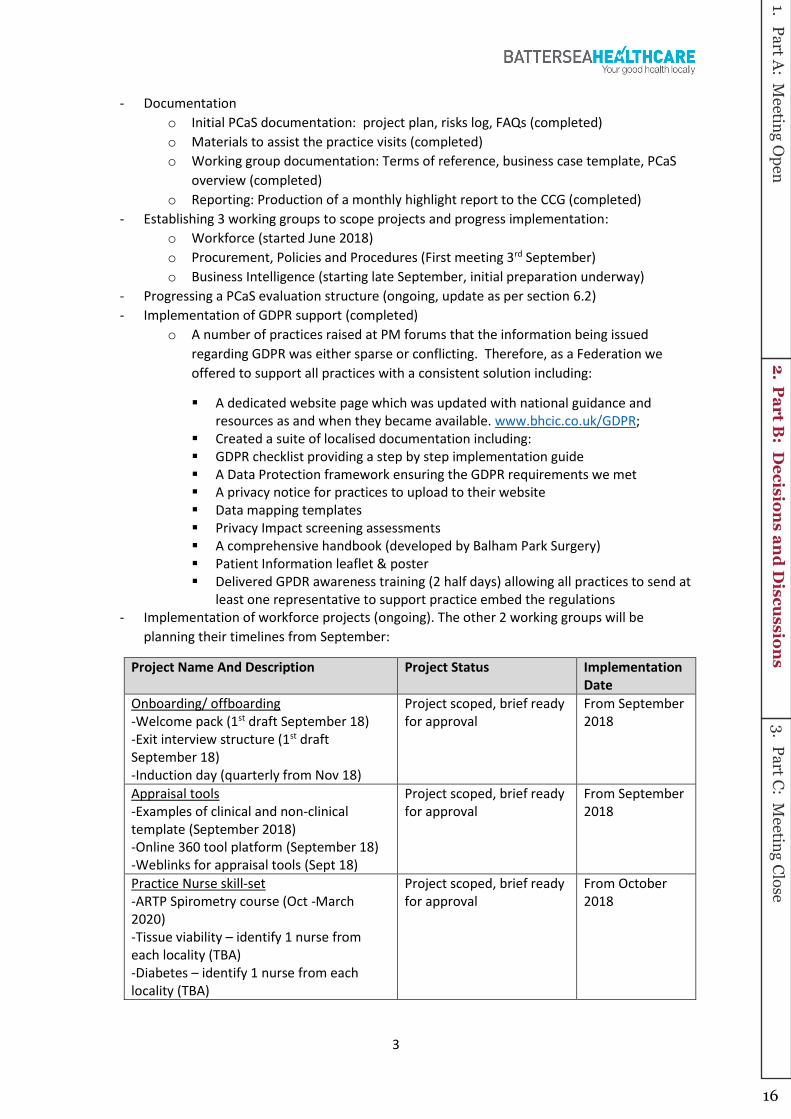
- Documentation
o Initial PCaS documentation: project plan, risks log, FAQs (completed)
o Materials to assist the practice visits (completed)
o Working group documentation: Terms of reference, business case template, PCaS
overview (completed)
o Reporting: Production of a monthly highlight report to the CCG (completed)
- Establishing 3 working groups to scope projects and progress implementation:
o Workforce (started June 2018)
o Procurement, Policies and Procedures (First meeting 3rd September)
o Business Intelligence (starting late September, initial preparation underway)
- Progressing a PCaS evaluation structure (ongoing, update as per section 6.2)
- Implementation of GDPR support (completed)
o A number of practices raised at PM forums that the information being issued
regarding GDPR was either sparse or conflicting. Therefore, as a Federation we
offered to support all practices with a consistent solution including:
A dedicated website page which was updated with national guidance and
resources as and when they became available. www.bhcic.co.uk/GDPR;
Created a suite of localised documentation including:
GDPR checklist providing a step by step implementation guide
A Data Protection framework ensuring the GDPR requirements we met
A privacy notice for practices to upload to their website
Data mapping templates
Privacy Impact screening assessments
A comprehensive handbook (developed by Balham Park Surgery)
Patient Information leaflet & poster
Delivered GPDR awareness training (2 half days) allowing all practices to send at
least one representative to support practice embed the regulations
- Implementation of workforce projects (ongoing). The other 2 working groups will be
planning their timelines from September:
Project Name And Description Project Status Implementation
Date
Onboarding/ offboarding
-Welcome pack (1st draft September 18)
-Exit interview structure (1st draft
September 18)
-Induction day (quarterly from Nov 18)
Project scoped, brief ready
for approval
From September
2018
Appraisal tools
-Examples of clinical and non-clinical
template (September 2018)
-Online 360 tool platform (September 18)
-Weblinks for appraisal tools (Sept 18)
Project scoped, brief ready
for approval
From September
2018
Practice Nurse skill-set
-ARTP Spirometry course (Oct -March
2020)
-Tissue viability – identify 1 nurse from
each locality (TBA)
-Diabetes – identify 1 nurse from each
locality (TBA)
Project scoped, brief ready
for approval
From October
2018
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
16

4
Group consultations
-Development of group consultation
programme (9 months)
Project scoped, brief being
progressed
TBA – to start
2018/19
Wandsworth locum bank
-Meetings held with Lantum and
MylocumManager
-Soft launch and testing (Oct 2018 to
March 19)
-Practice feedback/evaluation (September
2019)
Project scoped, brief being
completed mid-September
Implementation
starting October
2018
Wandsworth nurse training model
-Research (October 2018)
-Recruit nurses - train the trainer (Nov-Dec
18)
Project scoped, brief being
progressed
Proposed launch
date April 2019
Recruitment support
-Job fair attendance (September and
October 2018)
-BMJ bulk buying of adverts
Project implemented and
ongoing
Implemented
Portfolio roles
-Finalise roles (September 2018)
-Advertise roles (Oct-Dec 18)
-Interview roles (Mid Dec 18)
project scoped, brief ready
for approval
February
resource start
dates
The aim of PCaS is to provide a sustainable and resilient primary care structure, which offers a
quality service to patients. Although many of the PCaS projects create this sustainability through
improved back office functions, or by providing a resilient workforce, there are some projects that
have a direct impact on patient services. These projects are:
- ARTP Spirometry Course – additional access to this training will provide more nurses
qualified to adequately diagnose patients with lung problems
- Tissue viability nurse training – t ai i g o e u se pe lo ality ill e su e a t ai the t ai e model for additional nurse training. This will ensure greater access to nurses for patients
requiring treatment for wounds and ulcers
- Diabetes specialist nurse training - t ai i g o e u se pe lo ality ill e su e a t ai the t ai e odel fo additional nurse training. This will ensure greater access to nurses for
diabetic specific consultations and related treatment
- Developing group consultations – development of this model will provide an additional
option for patient care. This model allows for patients with the same diagnosis to attend
group sessions to learn about their condition.
-
5. Financial Summary
The following table provides a high-level summary of the PCaS spending to date:
Primary Care at Scale – 2018/19
Workstream Estimated Cost
General PCaS:
- Working group meetings
- Legal advice
- Practice engagement
- Project Management
£80,000
Workforce projects £60,000
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
17

5
There is a total budget of £600,000 for the PCaS programme in 2018/19. The remaining sum will be
spent on progressing the projects identified by practices and the 3 workstream working groups as
well as conducting a PCaS evaluation. This spend will be scoped over the next few months.
6. Assurance Process
6.1 Business Case review
All PCaS project leads will complete a short business case with the Working Group Project Manager.
These business cases will be reviewed by the GP Federation and approved as per their alignment to
the PCaS objectives to create resilience and sustainability in general practice. It should be noted that
so e p oje ts ill e o side ed ui k i s , hilst othe s ay e ui e esea h to as e tai thei viability.
6.2 Evaluation Process
To ensure the PCaS programme is meeting the aims and objectives for Wandsworth, development of
a robust evaluation process is currently underway. An external provider will be used to perform the
evaluation and the GP Federation are in discussion with potential candidates.
The evaluation will:
- Review progress against the initial aims and objectives set out in the Strategic
Commissioning Framework and assess the general direction of travel for the PCaS
programme;
- Use the aims identified in the practice visits to assess how the PCaS projects are meeting
requirements;
- Review and measure the benefits/outcomes of the projects;
- Demonstrate resilience and sustainability of primary care.
From initial research, the evaluation may be structured in 2 phases:
- Phase 1 will include an evaluation of the workforce projects initiated to date, along with
general evaluation of the approach to the Primary Care at Scale programme;
- Phase 2 will include evaluations of all 3 workstreams and an overarching view of the
direction of travel for the programme.
External evaluators and approaches are currently being assessed, with a view to selecting one to
progress this work in September.
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
18

6
7. Programme Timeline For 2018/19
The following summaries the high-level tasks scheduled for the PCaS programme until the end of
2018:
8. Next steps
The PCaS programme will continue to progress tasks against the over-arching project plan.
As part of the original PCaS proposal outlined in Appendix 1, 3-4 pilots were identified as an initial
starting point (due to commence in Q3 and 4). Workforce pilots and GDPR support are already
underway, with further projects being identified as the other 2 working groups are started in
September.
To progress the practice network group discussions which were initiated in the June locality forums,
individual practice visits are now being conducted to identify practice aims and to obtain their views
on how network groups could be implemented. The main purpose of these visits is to find practices
with similar aims and to match projects that meet their requirements. In addition to the visits,
research is also being conducted to assess the viability of using facilitated sessions (once the
network grouping exercise is complete) so the newly formed groups can meet to discuss their shared
aims and implementation of locally agreed projects.
As discussed in section 6.2, an evaluation process is currently being developed to assess the success
of the initial PCaS engagement, with a view to a more detailed evaluation being run once the
network groups are established. The aim is to have an initial evaluation completed by the end of
2018, and the more detailed evaluation run at the end of 2018/19 or the beginning of 2019/20. The
outcomes of these evaluations will be used to inform the future development of PCaS projects and
the network groups.
Engagement
•Locality forums, emails (Ongoing)
•Collating project ideas (Ongoing)
•Practice visits (September - October)
Projects
•Workforce - projects progressing (Ongoing)
•Procurement/Policies - scoping (from early September)
•Business Intelligence - scoping (from late September)
Evaluation
•Research best evaluation option (August)
•Agree approach (September)
•Run Phase 1 of the evaluation (October-December)
Network Groups
•Review practice aims noted from visits (November)
•Consider grouping of practices - aims/preferences (November - December)
•Progress network grouping (from January 2019)
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
19

7
Appendices
Appendix 1: Original PCAS Proposal and completed actions
Phase 1: 2018/19 Q1-Q2 Outcomes
Comprehensive solution work up:
Establish three working groups (governance
and procurement, information technology /
business intelligence, and workforce) with
practice representatives and subject matter
experts as leads. COMPLETED
Working groups to review initial scoping
outputs with objective and transparent
evaluation tools creating a proposed project
plan. WORKFORCE COMPLETED, OTHER 2
STREAMS ARE BEING COMPLETED IN
SEPTEMBER
Project plans authorised by relevant
stakeholders and shared with practices.
PROJECT BRIEFS HAVE BEEN DRAFTED AND
FULL REVIEW MEETING ARRANGED FOR 8TH
OCTOBER
Enact project plan with agreed project
assurance tools. COMPLETED AS PART OF THE
PROJECT BRIEF
Meet phase Strategic Commissioning
Framework requirements.
Reducing trend of vacancies across all
staff groups.
Increased retention especially within
practice manager group.
Stable temporary workforce accessed
through non-agency routes.
Portfolio roles crossing acute and
community sectors.
Greater use of e platforms offering
patients increased choice and staff
different ways of working.
Comprehensive quality system which is
centrally developed and locally owned.
Easy access to high quality goods and
services reducing unit costs and
overheads.
Practices engaged through protected
time and resources to support change.
GP networks pilots which are underway
and on target to deliver outcomes.
Strong GP networks with appropriate
leadership and governance
infrastructure.
All GP networks have developed a
credible delivery plan.
Phase 2a: 2018/19 Q3&Q4
Establishing GP networks:
Initiate four pilots to road test GP networks
INITIAL DISCUSSIONS UNDERWAY AND
WORKFORCE PROJECTS BEING INITIATED.
PILOTS WILL ALSO BE IDENTIFIED FROM THE
OTHER 2 WORKING GROUPS
Enable practices to discuss local GP network
models and opportunities with access to
technical or professional support. INITIAL
RESEARCH INTO HOW TO ACHIEVE THIS IS
BEING CONDUCTED (POTENTIAL TO HIOLD
FACILITATED SESSIONS)
Develop a governance framework which
provides appropriate oversight and assurance.
Develop a leadership structure with clear
responsibilities.
Support and upskill GP networks with relevant
training and support.
Create GP network delivery plan.
Phase 2b: 2019 Q1+
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
20
8
Launch GP network delivery plan (Q1).
Provide ongoing support and access to
specialist advice as and when required.
Monitor progress against delivery plan.
Active and collaborative GP networks
delivering a clear plan with ownership
and effective solutions.
Stakeholders who are regularly informed
and aware of plans across the network.
Open and inclusive cross GP network
knowledge sharing.
Phase 3: 2-5 year plan
Whole population budgets.
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
21

P A G E 1 O F 5
Revised London Primary Care Commissioning Operating Model
Author: NHS England London Region Sponsor: Nora Simon/Kate Denton Date: 4th September 2018
Executive Summary
Context
The Primary Care Commissioning Operating Model (Appendix A) was developed in April
2015 and sets out how NHS England (London) region’s STP Primary Care Contracting Teams will consistently support CCGs with joint or delegated co-commissioning
arrangements.
The Operating Model provides the standard offer of NHS England in terms of supporting
Primary Care Commissioning activities. This document has been endorsed and approved
by NHS England Primary Care management Board, which includes STP Primary Care
Leads, prior to consideration by Primary Care Commissioning Committees.
Primary Care Commissioning Committees (PCCC’s) were asked to adopt the first version of the Operating Model in autumn 2015. The Operating Model has been revised to include
up to date National and London policies, procedures and guidance. It also summarises the
reporting required to support decision making and associated responsibilities, together with
committee, governance, processes and capabilities.
The revised Operating Model also reflects the geographical alignments of NHS England
Teams with London’s 5 STP footprints. PCCCs across London are being asked to consider
the revised documentation for endorsement and adoption.
PCCC Members will be aware that there are a significant number of National and London
policies, guidance and procedures that sit behind the Operating Model, which will be used
by STP Primary Care Teams following the approval.
It is expected that there will be a regular need to review the Operating Model on an annual
basis, as a minimum. However it is not intended that non-material changes should result in
PCCCs needing to sign off such amendments, as these could be delegated by PCCCs to
Managing Directors.
Question(s) this paper addresses
The main changes to the Operating Model and its accompanying documentation are:
M E R T O N & W A N D S W O R T H L O C A L D E L I V E R Y U N I T
W A N D S W O R T H P R I M A R Y C A R E C O M M I T T E E P A G E 1 O F [ X ]
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
22

P A G E 2 O F 5
1. The language in the document has been updated to reflect the fact that from the 1st
April 2018 all CCGs across London will be level 3 delegated commissioners
2. NHS England functions are laid out in a table on Page 19 and 20, and are the
functions for decision making that were agreed under the delegation commissioning
terms of reference. There were updated to include more up to date Strategy and
Policy contracting decisions (e.g. resilience and sustainability of general practice),
and no longer includes potential activity figures which are out of date and no longer
relevant given that committees have been established for 3 years.
The table also describes whether a National or London policy or Standard Operating
Procedure exists to support decision making.
3. The revised GP Quality and Performance Reporting Requirements are set out on
Pages 20 to 23, agreed by the STP Primary Care Leads, following a review facilitated
by NHS England.
4. Pan-London responsibilities have been updated on Page 47 onwards, in recognition
of the STP alignments of the 5 former London Primary Care Commissioning and
Contracting Teams.
5. The London Standard Operating Procedures/ Policies have been refreshed to ensure
they include agreements across London since the previous version was signed off in
April 2015.
6. The NHS England GP Policy Manual, on which the Operating Model is based on, has
also been updated with changed to the Special Allocation Scheme and more specific
guidance on managing patient’s dispersals.
Input Sought
The Primary Care Committee are asked to ratify the revised London Primary Care Operating
Model.
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
23

P A G E 3 O F 5
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
24

P A G E 4 O F 5
For Reference Edit as appropriate:
1. The following were considered when preparing this report:
The long-term implications [Not applicable]
The risks [Yes]
The Operating Model will mitigate the risk of making decisions that do not align
with National or London policies, procedures and/or guidance.
Impact on our reputation [Not applicable]
Impact on our patients [Not applicable]
Impact on our providers [Not applicable]
Impact on our finances [Yes]
The Operating Model will be primarily discharged through the STP Primary
Care Team, and should therefore be cost neutral in terms of producing
recommendations and PCCC decision making.
Specific policies, procedures and/or guidance may have specific service
related cost implications.
Equality impact assessment [Yes]
The Operating Model enable consistent and standardised considerations to be
taken on GP contractual matters
Patient and public involvement [Not applicable]
Please explain your answers:
1. This paper relates to the following corporate objectives:
Commission high quality services which improve outcomes and reduce
inequalities [Yes ]
Make the best use of resources, continually improve performance and deliver
statutory responsibilities [Yes]
Continually improve delivery by listening to and collaborating with our patients,
members, stakeholders and communities [Not applicable]
Transform models of care to improve access, ensuring that the right model of care
is delivered in the right setting [Not applicable]
Develop the CCG as a continuously improving and effective commissioning
organisation [Yes]
Please explain your answers:
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
25

P A G E 5 O F 5
2. Executive Summaries should not exceed 1 page. [My paper does comply]
3. Papers should not ordinarily exceed 10 pages including appendices.
[My paper does not comply]
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
26

1
Operating Model
Co-Commissioning of Primary Care
Services
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
27
2
Document filename: Operating Model
Directorate / programme Primary Care Commissioning
Project Primary Care Commissioning
Document reference
Project manager Anne Whateley Status For Approval
Owner Primary Care Management
Board/ Primary Care Committees
Version 16.0
Author Patrick Newton Version issue date 08/03/2018
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
28

3
Operating model: Co commissioning of primary care
Document management
Revision history
Version Date Summary of changes
1.0 22.04.15 First draft
2.0 23.04.15 Revision following Christina Windle review
3.0 30.04.15 Revision following Heads of Primary Care review
4.0 30.04.15 Draft for review by David Sturgeon
5.0 05.05.15 Review by Primary Care Commissioning and Primary Care Management
Board
6.0 03.06.15 Draft updated following comments
7.0 09.06.15 Updated to reference initial comments from CCGs (to be approved in
PCMB)
8.0 20.07.15 Draft updated to reflect agreed comments
9.0 14.08.15 Updated following discussion at co-commissioning meeting
10.0 09.09.15 Updated following discussion at co-commissioning meeting
11.0 22.09.15 Final draft for approval
11.1 02.10.15 Factual amendments post approval by SE London (Joint Status of SE London Committees. Some minor editorial changes
12.0 01.06.17 Updated to reflect the geographical assignment of NHSE staff at lead
CCGs for each STP footprint
13.0 30.10.2017 Updated to reflect comments from CCG leads
13.01 01.12.2017 Revised version endorsed by the December PCMB
14.0 26.01.2018 Updated to reflect amendments for BHR CCGs
15.0 14.02.2018 Updated to incorporate the arrangements for GP Quality Performance
reporting
16.0 08.03.2018 Updated to reflect amendments regarding Occupational Health arrangements and new Director of Primary Care Commissioning
Reviewers This document must be reviewed by the following people before being shared externally:
Reviewer name Title/responsibility Date Version
Anne Whateley Director of Primary Care Commissioning
Jill Webb Head of Primary Care
Julie Sands Head of Primary Care
William Cunningham-Davis Head of Primary Care
Alison Goodlad Head of Primary Care
Vanessa Piper Head of Primary Care
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
29

4
Approved by This document must be approved by the following groups:
NHS England:
Name Signature Title Expected
Date
Version
David Slegg (in
recognition of approval at the Primary Care
Management Board)
Regional Director for Finance (London)
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
30

5
Following sign off by NHS England (London), this document must be accepted by each of the co-
commissioning committees. These groups are therefore shown below:
Co-Commissioning Committees:
Area Signature Title Expected
Date
Version
Barnet CCG
Primary Care Committees In Common
Camden CCG
Haringey CCG
Enfield CCG
Islington CCG
Croydon CCG Primary Care Committee
Kingston CCG Primary Care Committee
Merton CCG Primary Care Committee
Richmond CCG Primary Care Committee
Sutton CCG Primary Care Committee
Wandsworth CCG Primary Care Committee
Bexley CCG Primary Care Committee
Bromley CCG Primary Care Committee
Greenwich CCG Primary Care Committee
Lambeth CCG Primary Care Committee
Lewisham CCG Primary Care Committee
Southwark CCG Primary Care Committee
Brent CCG Primary Care Committee
Ealing CCG Primary Care Committee
Hammersmith and Fulham CCG
Primary Care Committee
Central London CCG Primary Care Committee
West London CCG Primary Care Committee
Hounslow CCG Primary Care Committee
Harrow CCG Primary Care Committee
Hillingdon CCG Primary Care Committee
Tower Hamlets CCG Primary Care Committee
Waltham Forest CCG Primary Care Committee
Newham CCG Primary Care Committee
Barking & Dagenham, Havering & Redbridge
CCGs
Primary Care
Commissioning Committee (Committee
in Common)
City and Hackney CCG Primary Care Committee
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
31
6
Related documents (to be updated)
Title Owner Location
NWL Terms of Reference Primary Care Committee North West London
NCL Terms of Reference for
Joint Committee v0.2
Primary Care Committees in
Common North Central London
SWL Terms of Reference Primary Care Committee South West London
Annex F – Delegated TOR Tower Hamlets v0.1
Primary Care Committee Tower Hamlets
Annex F – Delegated TOR
Waltham Forest v1.0 Primary Care Committee Waltham Forest
Annex F – Delegated TOR
Newham v final Primary Care Committee Newham
Barking & Dagenham, Havering and Redbridge –
Updated Annex F (TOR)
Primary Care Commissioning Committee (Committee in
Common
Barking & Dagenham, Havering and Redbridge
Document control The controlled copy of this document is maintained by NHS England. Any copies of this document held outside of that area, in whatever format (e.g. paper, email attachment), are considered to have
passed out of control and should be checked for currency and validity.
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
32

7
Contents Document management ....................................................................................................3
Revision history ...............................................................................................................3
Reviewers........................................................................................................................3
Approved by ....................................................................................................................4
Related documents (to be updated)..................................................................................6
Document control.............................................................................................................6
1. Introduction ..................................................................................................................9
1.1 Purpose of this document ...................................................................................9
1.2 Operating model processes for individual committees......................................9
1.3 Defining co-commissioning .............................................................................. 10
1.4 Terminology:...................................................................................................... 11
1.5 Differences between Joint and Delegated Committees.................................... 11
1.6 Responsibilities remaining with NHS England ................................................. 11
2. Decision Making ......................................................................................................... 12
2.1 Decision making principles ............................................................................... 12
2.2 Decision making process .................................................................................. 12
2.3 GP Performance and Quality Reporting Requirements ........ Error! Bookmark not
defined.
2.3.5 Conflicts of interest ............................................................................................ 24
2.3.5 Other decision-making processes – finance and strategy.................................... 25
2.4 Other potential Committee responsibilities ...................................................... 27
3. Governance and people ............................................................................................. 28
3.1 Committee constitution ..................................................................................... 28
3.2 Committee resourcing ....................................................................................... 28
4. Processes & Capabilities ............................................................................................ 29
4.1 Meeting process: ............................................................................................... 29
4.1.1 Agenda contents ............................................................................................ 29
4.2 Meeting Papers .................................................................................................. 30
4.3 Meeting in private .............................................................................................. 30
5. Annexes..................................................................................................................... 31
Annex Introduction ...................................................................................................... 31
Annex 1: Detailed processes ....................................................................................... 32
Annex 2: Section 13Z - CCG statutory duties ............................................................. 42
Annex 3: Performer Contract Decision Making Process ............................................ 43
Annex 4 - Safeguarding – responsibilities at different levels of CCG co-
commissioning delegation .......................................................................................... 45
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
33
8
Annex 5 – Pan London Responsibilities of NHS England STP Based Teams............ 47
Annex 6 – Pan London Fora ........................................................................................ 55
Annex 7 - Template for Future NHS Access………………………………………………………………………59
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
34

9
1. Introduction
1.1 Purpose of this document This document sets out NHS England national and London region policy and guidance to
inform, the way that NHS England (London) primary care commissioning and contracting
teams will support CCGs which have moved to joint or delegated co-commissioning
arrangements (as of April 2017).
As this document provides the standard offer of NHS England in terms of supporting Primary
Care Commissioning activities, this document will need to be signed off by NHS England
(through the Primary Care Management Board) and then CCG Commissioning Committees,
before it is considered final.
It is important to note that some specific details (i.e. the contact points for different
committees/ areas) will differ per committee and these added details should be cross
referenced with committee terms of reference or other supporting documents.
Governance of this document and processes
Once this document has been signed off by both parties, any variance from the processes
described here will need to be agreed between the Committee and NHS England (through
the Primary Care Management Board) as:
Having no impact on support (for example changes to the contact to be involved in
urgent decision making) and can therefore be adopted for a specific Committee
Is an adjustment or improvement to the process which would be beneficial for all
Committees and therefore should be made as a change to standard processes (for
example reporting format or processes which makes the reporting cycle more
efficient or information more easily understood)
Is a required change for a specific Committee(s) and therefore a change request will
need to be logged (i.e. additional reporting).
Agreement of these changes will require sign off at the Primary Care Management Board
and then with Primary Care (Co) Commissioning Committees before it can be considered
confirmed. This may require resource and/ or cost implication assessments, and the
ownership for any impact of these would need to be discussed as part of the agreement
discussions.
Updates of and additions to working policies and guidance, referred to by this document,
may be approved by Accountable Officers and NHS England (London). Any changes would
be considered and approved by London Region’s Primary Care Management Board.
1.2 Operating model processes for individual committees As mentioned above, this document aims to provide a standardised version of the operating
model. However the below details will need to be discussed in each individual committee,
and therefore decisions relating to the below are seen as acceptable levels of customisation
within this standard model:
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
35
10
Inc
rea
sin
g C
CG
co
ntr
ol
Standard policies to assist decision making should be reviewed and agreed by the
committee; the committee may wish to add others
The sub-committee structure is likely to be different per committee. This should follow
the principles defined here and be discussed and agreed with NHS England if
involved.
The CCG representative(s) to be contacted in the event of urgent decisions being
required.
These elements should be discussed and agreed as part of committee discussions, and
should be included as appendices or linked documents.
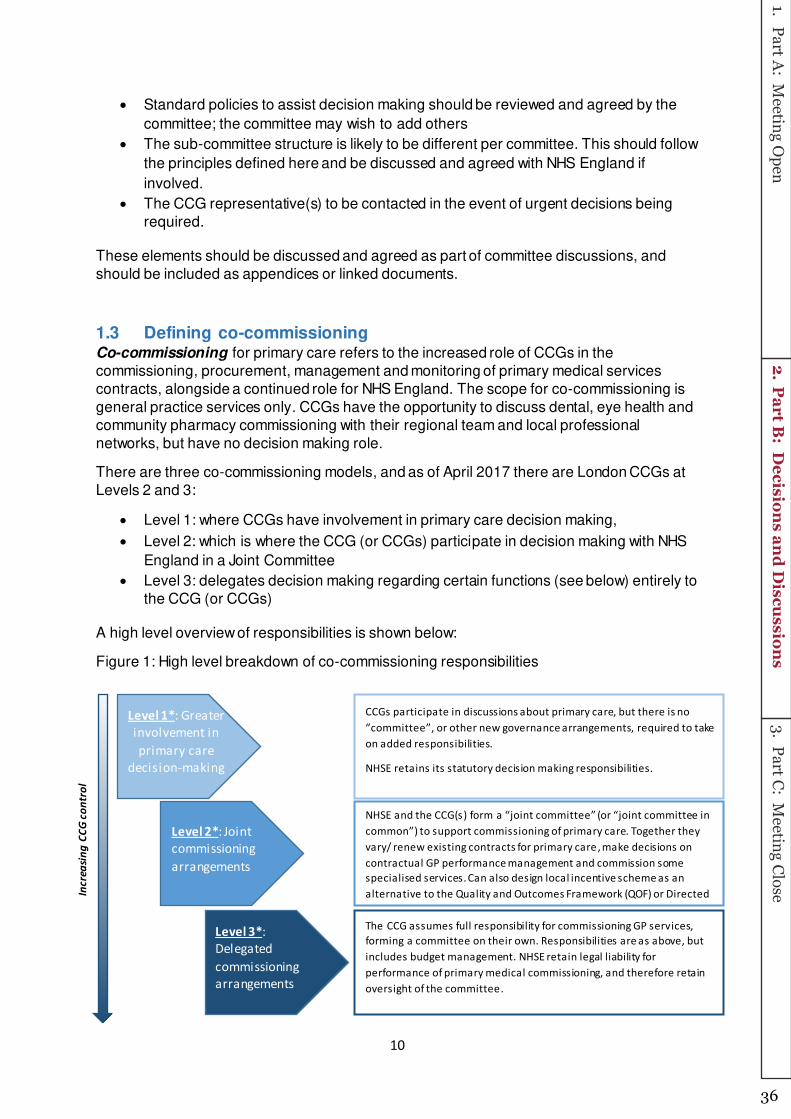
1.3 Defining co-commissioning Co-commissioning for primary care refers to the increased role of CCGs in the
commissioning, procurement, management and monitoring of primary medical services
contracts, alongside a continued role for NHS England. The scope for co-commissioning is
general practice services only. CCGs have the opportunity to discuss dental, eye health and
community pharmacy commissioning with their regional team and local professional
networks, but have no decision making role.
There are three co-commissioning models, and as of April 2017 there are London CCGs at
Levels 2 and 3:
Level 1: where CCGs have involvement in primary care decision making,
Level 2: which is where the CCG (or CCGs) participate in decision making with NHS
England in a Joint Committee
Level 3: delegates decision making regarding certain functions (see below) entirely to
the CCG (or CCGs)
A high level overview of responsibilities is shown below:
Figure 1: High level breakdown of co-commissioning responsibilities
Level 1*: Greater
involvement in
primary care
decision-making
Level 2*: Joint
commissioning
arrangements
Level 3*:
Delegated
commissioning
arrangements
CCGs participate in discussions about primary care, but there is no
o ittee , or other e go er a e arra ge e ts, required to take
on added responsibilities.
NHSE retains its statutory decision making responsibilities.
NHSE and the CCG(s for a joi t o ittee or joi t o ittee i o o to support o issio i g of pri ary are. Together they
vary/ renew existing contracts for primary care , make decisions on
contractual GP performance management and commission some
specialised services. Can also design local incentive scheme as an
alternative to the Quality and Outcomes Framework (QOF) or Directed
The CCG assumes full responsibility for commissioning GP services,
forming a committee on their own. Responsibilities are as above, but
includes budget management. NHSE retain legal liability for
performance of primary medical commissioning, and therefore retain
oversight of the committee.
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
36

11
Figure 1: Co-Commissioning Levels
1.4 Terminology: At levels 2 and 3, co-commissioning decision making is conducted through a, or several,
‘committee(s)’, which is joint with NHS England, or delegated. The committee could either
consist of:
Committees of single CCGs (with or without NHS England)
Committees in common of more than one CCG (with or without NHS England)
For simplicity, throughout this document, the body which conducts decision making
for co-commissioning is referred to simply as “the committee”, and it may refer to any of the parameters above. Where different processes are required for joint or delegated
committees, these are called out.
1.5 Differences between Joint and Delegated Committees The move to co-commissioning, means that certain decisions (see Figure 2) which were
previously conducted directly by NHS England, will now be made by the body constituted to
support the level of co-commissioning each CCG has applied for – i.e. committees with NHS
England (for joint commissioning) or without NHS England (for delegated commissioning).
Regardless of whether the CCGs are conducting Joint or Delegated commissioning, the
functions enacted will be for the most part the same; the main difference is whether NHS
England is part of the decision making process or not. It should be noted that there will be a
joint responsibility for ensuring quality, through the reporting of performance data
It should be noted that the CCG may ask NHS England to attend and/ or present papers at
delegated committees, but this should be done on request and NHS England will not be a
voting member.
1.6 Responsibilities remaining with NHS England At all levels of co-commissioning, NHS England will retain a role in supporting delivery of
commissioning and contracting functions. This will be discharged by NHSE teams that will be
accommodated by a lead CCG for each of London’s STPs. Also the following responsibilities
will remain with NHS England and will not be included in joint or delegated committees:
Continuing to set nationally standing rules to ensure consistency and delivery goals
outlined in the Mandate set by government.
The terms of GMS contracts and any nationally determined elements of PMS and
APMS contracts will continue to be set out in the respective regulations/ directions.
Functions relating to individual GP performance management (medical performers’ lists for GPs, appraisal and revalidation).
Administration of payments to GPs.
Patient list management will remain with NHS England.
Capital expenditure functions.
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
37

12
2. Decision Making
2.1 Decision making principles One of the exceptions to this as a standard document across all committees is that there
may be some variation as to what and how decisions are made in the commit tees. Decisions
will be taken in line with the criteria set out in each committee’s Terms of Reference. In
addition to principles of good practice which are set out in the Next Steps in Co-
Commissioning document, conflicts of interest policy, terms of reference etc., the following
principles should be considered:
Any urgent decisions made outside of the committee should be based on what
is necessary to maintain patient care; wherever possible decisions will be taken
within the committee.
In the event that an urgent decision is required and action must be taken to
maintain patient care outside of a committee, NHS England will communicate
with the contact nominated in the committee’s terms of reference (via phone
and email) to ensure that an urgent unplanned decision is made to maintain
and safeguard patient care.
2.2 Decision making process Co-commissioning of Primary Care will enable committees to take full or partial responsibility
for many decisions which previously sat with NHS England. Any CCG functions which are to
be delegated into this committee are not included here.
Decisions have been classified into three types in order to help capacity in the committee.
These types are:
1. Decision making through policies which therefore require minimal/ do not require
discussion because there is a clear approved policy which provides clarity on the
action required
2. Urgent decisions which cannot wait until the committee. These decisions require
emergency processes (see below)
3. Decisions to be discussed in the committee. Other General Practice
commissioning decisions should be made within the committee. It is expected in
many cases recommendations will be made into the committee from pre-work or sub-
committees as appropriate.
These decision types and the related processes can be seen in the below processes:
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
38
13
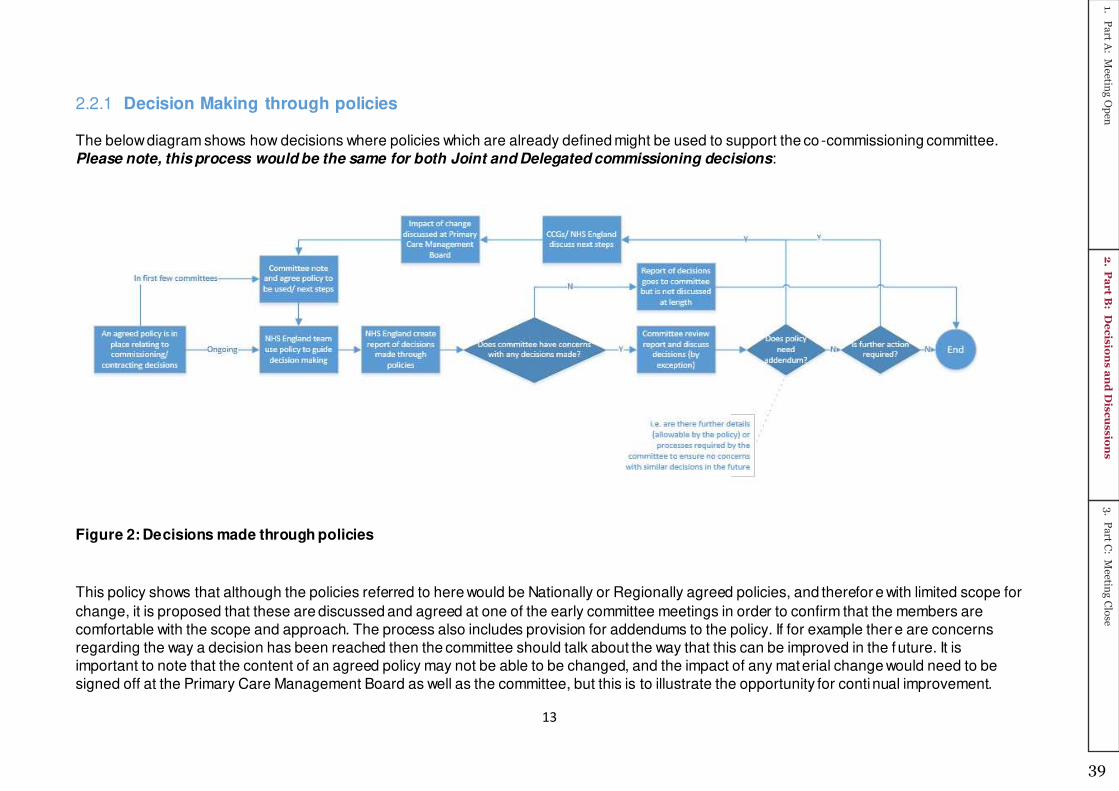
2.2.1 Decision Making through policies
The below diagram shows how decisions where policies which are already defined might be used to support the co -commissioning committee.
Please note, this process would be the same for both Joint and Delegated commissioning decisions:
Figure 2: Decisions made through policies
This policy shows that although the policies referred to here would be Nationally or Regionally agreed policies, and therefor e with limited scope for
change, it is proposed that these are discussed and agreed at one of the early committee meetings in order to confirm that the members are
comfortable with the scope and approach. The process also includes provision for addendums to the policy. If for example ther e are concerns
regarding the way a decision has been reached then the committee should talk about the way that this can be improved in the f uture. It is
important to note that the content of an agreed policy may not be able to be changed, and the impact of any material change would need to be
signed off at the Primary Care Management Board as well as the committee, but this is to illustrate the opportunity for continual improvement.
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
39
14
The purpose of this process is to relieve agenda pressure in the committee. If there are any
decisions or elements of the report which the committee would like to discuss, this can be
done and should be offered by the chair at the start of the meeting.
2.2.1.1 Decisions with defined policies
The decisions which can be made through defined policies will be discussed and agreed by
each co-commissioning committee, however the expected decisions where policies are
expected to be used to make decisions:
List closure
Boundary changes
Discretionary payments
Contractual changes
There are several other areas where standard operating processes or policies exist, but it is
expected that decisions will still need to be made within the committee and therefore are not
included here. The full list of potential decisions with policies can be found in Figure 5.
2.2.2 Urgent decision making:
‘Urgent’ is defined in this document as a decision which cannot be made within a committee because of timing and nature of the decision. The main co-commissioning committee is
accountable for all decisions, and should agree to the decision process for this and expected
circumstances where this would arise and these agreed arrangements should be reflected in
the relevant terms of reference. It is important to note that there are two types of urgent
decisions. These are described below, with suggested processes.
It should be noted however that the process and individuals involved should be decided and
agreed by the Primary Care Committee, and this should be reflected in their terms of
reference (either referring to this operating model and providing details of the individuals to
be involved or outlining any changes within the agreed principles).
2.2.2.1 Urgent unplanned decisions
An urgent unplanned decision arises when something unexpected occurs that requires
immediate action. For example if a practice goes bankrupt a decision will need to be made
immediately in order to support the patients on the registered list.
The below principles apply to urgent unplanned decisions:
o Wherever possible, only decisions necessary to maintain patient care should
be taken outside of the committee
o The terms of reference of co-commissioning committees should set out
member’s responsibilities for making urgent decisions The NHS England team
accommodated at the lead CCG will communicate with this contact (by phone/
email) to ensure a decision is made which will be:
A joint decision between the NHS England and CCG representatives if
operating in joint commissioning, or
The CCG is asked to make a decision in delegated commissioning
o In the event that the CCG is made aware of the need to make an urgent
decision, they are:
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
40
15
Required to communicate with NHS England to make the decision
together if operating in joint commissioning
Able to communicate with NHS England if they require support/ advice
to make the decision in delegated commissioning
The below diagram shows how urgent unplanned decisions might be made. Please note,
these processes would be the same for both Joint and Delegated commissioning
decisions:
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
41
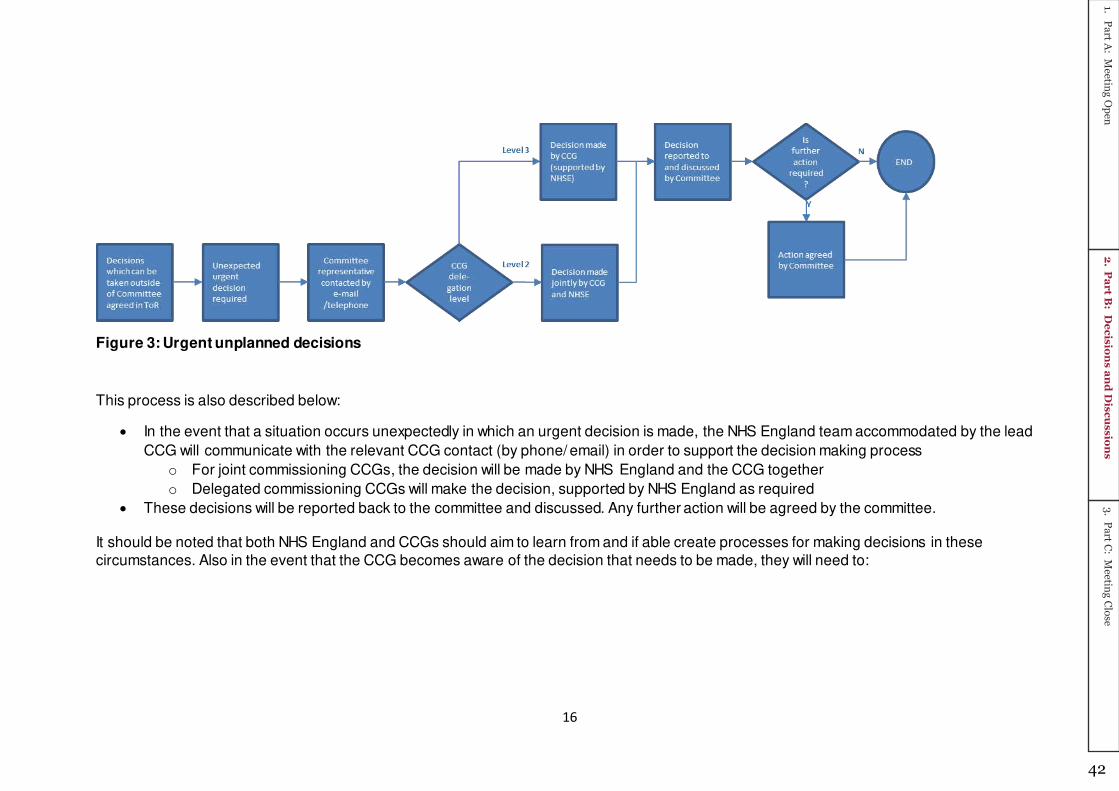
16
Figure 3: Urgent unplanned decisions
This process is also described below:
In the event that a situation occurs unexpectedly in which an urgent decision is made, the NHS England team accommodated by the lead
CCG will communicate with the relevant CCG contact (by phone/ email) in order to support the decision making process
o For joint commissioning CCGs, the decision will be made by NHS England and the CCG together
o Delegated commissioning CCGs will make the decision, supported by NHS England as required
These decisions will be reported back to the committee and discussed. Any further action will be agreed by the committee.
It should be noted that both NHS England and CCGs should aim to learn from and if able create processes for making decisions in these
circumstances. Also in the event that the CCG becomes aware of the decision that needs to be made, they will need to:
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
42

17
In joint commissioning – communicate with NHS England (the relevant Head of
Primary Care or Director of Primary Care) in order to jointly make the decision
In delegated commissioning, the CCG may wish to seek advice or support from NHS
England but is not obligated too. They should however inform them of the decision as
there may be impacts or other communications which should reflect the decision
made.
Some CCGs have outlined a process if the decision making window is longer (for example
two weeks), allowing them to bring together a slightly bigger group of people (e.g. Chief
officers, the chair of the committee and NHS England representatives). This enables
decisions to be more widely considered and tested however it is noted that it may be
challenging to gather a wider group at short notice, and it is suggested that virtual or
telephone discussions may be easier. CCGs are advised to make the process of planned and
unplanned urgent decision making clear in their committee TOR.
2.2.2.2 Urgent planned decisions
There may be some decisions which are expected, but:
Cannot be made at an earlier committee as, for example there is insufficient
information
Must be made before the next committee
This means that decisions do need to be made through an urgent process, but that some
planning can be undertaken ahead of the decision. Specific arrangements and decision
rights, for each CCG, should be referenced in their Terms of Reference. The principle of how
this should operate is shown below:
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
43

18
Figure 4: Urgent planned decisions
This process is also described below:
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
44

19
In the event that a decision cannot be taken in the committee because sufficient
information is not known, or there are some other inhibiting circumstances, planning
should be undertaken as much as possible to ensure the committee is able to input
into the decision making process
Therefore any elements of the decision or process relating to the decision should be
discussed, and if necessary a sub or working group may be set up to continue work
towards this decision
o Please note, there may be an existing group or sub-committee which would
undertake this work.
These decisions will be reported back to the committee and discussed. Any further
action will be agreed by the committee.
It should be noted that both NHS England and CCGs should aim to learn from and if
able create processes for making decisions in these circumstances. CCGs are advised
to make the process of planned and unplanned urgent decision making clear in their
committee TOR.
2.2.3 Main decision types required
2.2.3.1 Business as usual decisions
The table below sets out of the main formerly NHS England functions which will now be
decided in the committee. This includes a recommendation as to the type of decision the
committee will be asked to make (this is not confirmed until this document has been
approved by each committee).
Name Function Committee decisions
needed (section 2.2)
Decision possible
with approved policy (s 2.2.1)
Need for urgent
decisions (s 2.2.2)
Does a national/London SOP/policy/report exist?
Determin - ation of key decisions or requests
List Closure Yes
List suspension Yes
Practice mergers/ moves Yes
Boundary Changes Yes
Securing services through APMS contracts
Yes – options appraisal doc
PMS (review s etc) Yes
Discretionary Payments Yes (Appeal/ complaint SOP)
Remedial and breach notices
Yes (Contractual issues of concern)
CQC Inadequate & Requires Improvement ratings
Yes – National (Inadequate) Yes – London (Requires Improv ement) .
Contract termination-e.g. Death/ Bankruptcy/ CQC
Yes (bankruptcy, and options)
Contractual changes (contentious/ important)
Contractual changes (transactional)
Yes (Contract signatory changes)
Locum reimbursements Yes Yes plus London FAQ, which is being considered f or national adoption
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
45
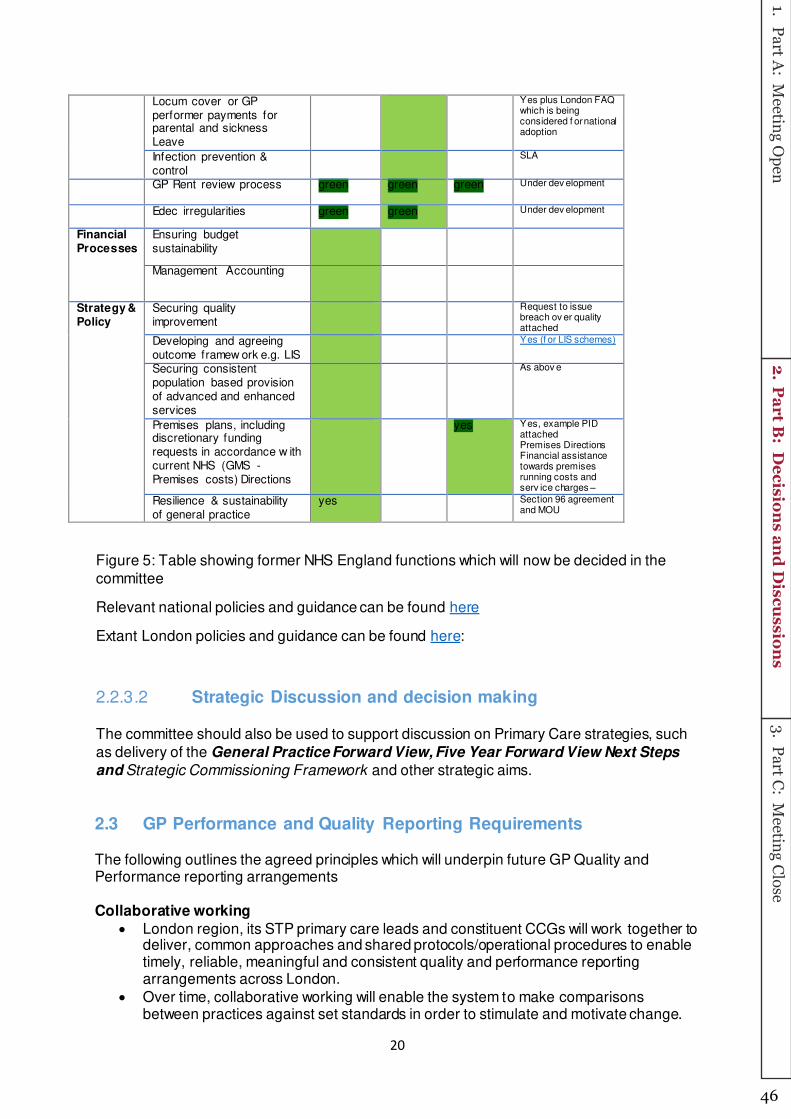
20
Locum cover or GP performer payments for parental and sickness Leave
Yes plus London FAQ which is being considered f or national adoption
Infection prevention & control
SLA
GP Rent review process green green green Under dev elopment
Edec irregularities green green Under dev elopment
Financial Processes
Ensuring budget sustainability
Management Accounting
Strategy & Policy
Securing quality improvement
Request to issue breach ov er quality attached
Developing and agreeing outcome framew ork e.g. LIS
Yes (f or LIS schemes)
Securing consistent population based provision of advanced and enhanced services
As abov e
Premises plans, including discretionary funding requests in accordance w ith current NHS (GMS - Premises costs) Directions
yes Yes, example PID attached Premises Directions Financial assistance towards premises running costs and serv ice charges –
Resilience & sustainability of general practice
yes Section 96 agreement and MOU
Figure 5: Table showing former NHS England functions which will now be decided in the
committee
Relevant national policies and guidance can be found here
Extant London policies and guidance can be found here:
2.2.3.2 Strategic Discussion and decision making
The committee should also be used to support discussion on Primary Care strategies, such
as delivery of the General Practice Forward View, Five Year Forward View Next Steps
and Strategic Commissioning Framework and other strategic aims.
2.3 GP Performance and Quality Reporting Requirements The following outlines the agreed principles which will underpin future GP Quality and Performance reporting arrangements Collaborative working
London region, its STP primary care leads and constituent CCGs will work together to deliver, common approaches and shared protocols/operational procedures to enable timely, reliable, meaningful and consistent quality and performance reporting arrangements across London.
Over time, collaborative working will enable the system to make comparisons between practices against set standards in order to stimulate and motivate change.
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
46

21
In recognition that there are further developments in quality and performance data and information, a minimum of an annual review of the London quality and performance offer will be undertaken with STP PC leads at the Primary Care Management Board.
NHS England will:
Provide standardised data reports, cut at different aggregated levels e.g. Practice, CCG, STP, Regional, National
Adhere to a planned refresh and publication schedule.
Clarify what can and can’t be shared and/or what can be shared through the NHS England team, but cannot be accessed by CCGs/STPs directly, based on clear Information Governance requirements.
Where NHSE governance allows, upload dashboards, data and analytical information onto the FutureNHS platform, which is a single accessible work space, for named STP/CCGs users to access
Will enable comparisons to be made between practices and used by STPs/CCGs against set standards over time in order to stimulate and motivate change.
STPs and/or CCGs will:
• Develop capacity to support standard reporting and analysis at STP/CCG level, subject to local agreement
• Be responsible for presentation, analysis and the ‘so what? Subject to local agreement.
• Target areas where quality needs improving based on local needs, which will also enable focus on specific issues e.g. DNA rates.
• Determine what data they use from the NHS England repository and may choose to use more up to date information, subject to its availability
• Share dashboards/tools that have been developed or are under development to promulgate good practice/what works
• Make a clear differentiation between what is information/data provided to review quality standards and that which is used to monitor performance in respect of contractual obligations and compliance
• Offer training to practices to support improved completion of returns, where required
Dashboards, data and analytical information and frequency of reporting
Whilst recognising that STP/CCG access to some NHS England data had not yet been
authorised by the latter, the initial list of reports and information available will consist of:
Resilience & Sustainability Tool (see yellow cells in Annex 1 for data items and reporting frequency)
CQC ratings trend analysis (monthly)
GPPS (General Practice Patient Survey) trend analysis, focused on questions relating to accessing services, coordinated care and patient experience (annual)
London Complaints dashboard (monthly)
Under development:
HEE workforce data
FFT trend analysis
Awaiting NHS England authorisation clearance:
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
47
22
Primary Care Activity Report (see red cells in Annex 1 including reporting frequency). NHS England STP contract management teams will provide information on items such as list closures; temporary list suspension; breaches; contractual disputes in the meantime (most up to date information provided, based on report timing)
GPFV Dashboard (see white cells in Annex 1, including reporting frequency). A small number of the extended access metrics will be shortly published externally. In time all of it will be and it will be gradually incorporated into reports.
Other information supplied by NHS England STP contract management teams:
Performer concerns being addressed by NHS England’s Medical Directorate that may impact on GP contracts (most up to date information provided, based on report timing)
Access to Dashboards, data and analytical information
FutureNHS will be the collaborative online resource that will allow NHS England London
region to host and share the latest iterations of dashboard reports each month. NHS England
will setup the workspace and invite delegates to join.
The list of delegates will include CCGs, STPs and primary care contracting team nominated
representatives across London.
As this process develops and governance requirements allow, additional dashboards/reports
will be included and shared as part of the Operating Model.
Attached is a template (Annex 7) that should be shared via STP leads with relevan t
stakeholders, and populated with the required information, following which it should be sent
back to Adrian Mccloskey [email protected] who will enable access.
Access to FutureNHS can take place from the beginning of January, subject to when STP
leads return their completed templates
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
48

23
Data sources and reporting frequency
Data Source Frequency
Active practices Quarterly
Branch practices Quarterly
Registered patients Quarterly
Practice size Annual
Delegation arrangements Annual
Contract type Annual
Dispensing practice Annual
Deprivation Annual
Patient demographics Annual
Workforce overview Quarterly/Bi-annual depending on measures
Workload reporting Frequency TBD
CQC ratings Monthly
Complaints Monthly
QOF Annual
GPPS Annual
FFT Annual
Average payments Annual
Patient online (POMI) Monthly
Extended access Bi-annual/Quarterly depending on source
Provider development measures for care redesign Monthly
Estates and Technology Transformation Fund Monthly
Secondary care measures (e.g. A&E attendance, elective admissions etc) Monthly
Care coordination (e.g. Care Navigators and Medical Assisstants) Quarterly
Online consultation systems Quarterly
Practice closures Annual
Procurement exercises Annual
Section 96 discretionary payments Annual
Patient list closures Annual
Patient and public participation planning and asssessment forms Annual
Contractual reviews Annual
Contractual disputes Annual
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
49
24
2.3.5 Conflicts of interest
All committees must adhere to the conflicts of interest guidance1 and this must also be
adhered to for any sub groups set up to support the committee.
1 i .e. Managing conflicts of interest: Revised statutory guidance for CCGs and Code of Conduct guides
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
50

25
2.3.5 Other decision-making processes – finance and strategy
Finance
Joint Co-Commissioning Committees
For Joint Committees, NHS England Finance teams accommodated at Lead CCGs will
continue to do all financial and management accounting. However, it will produce monthly
financial reports (for instance, covering spending against forecast and narrative on variance)
which will be provided to each CCG. The CCG may then choose to add information to these
reports before they are submitted to the committee(s).
Delegated Co-Commissioning Committees
For Delegated Committees, transactions for delegated functions will be posted directly to the
CCG’s ledger., NHS England Finance teams accommodated at Lead CCGs will be
responsible for reporting, and management accounting of primary care costs. The CCG may
also make further queries of NHSE, to support this process. Management accounting
activities will likely include, but not be restricted to:
Month end procedures
Accruals, prepayments, and any payments additional to those in the financial plan
The production of monthly & quarterly CCG management reports at GP practice or
locality level to ensure robust financial forecasts and analyse variances to ensure
they are explained
Practice list size analysis by CCG locality for GM/system report downloads
Quarterly forecasting on CQRS
Additional year end tasks including working papers and support to AOB process
Liaise with internal and external audit as required.
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
51

26
Figure 7: Process map showing financial processes
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
52

27
2.4 Other potential Committee responsibilities In addition to the above standard processes, there are other Primary Care elements which
the Committee is expected to be involved in. Some of these areas are listed below however
it should be noted that further discussions are required as to how these would be enacted
and supported between NHS England teams accommodated at Lead CCGs and the CCGs
at different co-commissioning levels. Further delegation from NHS England to CCGs will not
be made without agreement, and without consideration of the resource implications of such
delegation.
Item Committee Requirement
Appeals and disputes
The committee is asked to note the standard operating procedure for managing appeals and disputes submitted by GPs in relation to their GP contract.
Counter Fraud Ensuring that proper processes are in place to prevent fraud within the NHS
Interpreting services Ensure that patients can access interpreting services when using GP practices.
Occupational Health The committee shall ensure that GPs have access to occupational health services in accordance with national guidance
Controlled drugs reporting
The Committee is responsible for ensuring that practices are complying with legal requirements for use of controlled drugs and that CCGs and NHSE have proper controls in place to maintain patient safety. The RT will carry out reporting, analysis and compliance that aids this.
Safeguarding To set policy and to set the expectation that GP Practices have effective safeguarding systems in place in accordance with statutory requirements, national guidance and Pan London Policy/ Procedures. CCGs will be responsible for ensuring that the GP services commissioned have effective safeguarding arrangements in place to improve the well-being of children and adults. The CCG will proactively support Primary Care through advising on training and good practice guidance and monitoring safeguarding issues, providing assurance to NHSE that there is compliance with safeguarding standards. Further detail on responsibilities for safeguarding are provided under Annex 4.
Incident management
For both serious and non-serious incident management, the Committee is responsible for ensuring that there are proper processes in place for the reporting and review of incidents, so that they can be identified and managed. The CCG and NHS E will support and contribute to investigations, as required.
Domestic Homicide Reviews
The Committee will ensure that GPs contribute to domestic homicide reviews, where necessary. The CCG and NHS E will support this where their resources are appropriate. Further detail on responsibilities for safeguarding are provided under Annex 4.
Communications For CCGs at level 3 delegation, lead responsibility will be determined by what is appropriate, on the merits of each communication. NHS England remains responsible for communications for CCGs at level 2 delegation.
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
53

28
Figure 8: Other potential Committee responsibilities
3. Governance and people
3.1 Committee constitution While much of the decision-making processes will be determined by Committees/ Joint
Committees, the constitution of the Committees themes have been set by NHSE, as a
condition of co-commissioning. The following are the criteria for a Committee (for Level
Three co-commissioning), and for a Joint Committee (for Level Two co-commissioning).
Figure 9: Committee and Joint Committee constitution
Other Committee attendees
In the interests of transparency and the mitigation of conflicts of interest , other interested
local representative bodies have the right to join the joint committee as non-voting attendees,
such as LMC, HealthWatch and Health and Wellbeing members. Invitees should be
determined in line with national guidance, and local terms of reference. Attendees should be
agreed so as to support alignment in decision making across the local health and social care
system. Other organisations may be invited, and as the committee meets openly it is likely
that members of the public and others will attend.
3.2 Committee resourcing There will not be a nationally-determined model of resourcing for co-commissioning, and
there is a recognition of the additional workload these new ways of working will result in . We
Committee is made up entirely of CCG
members (NHS England will not be
members of the board).
The Chair and Vice/Deputy Chair of the
committee are CCG Lay Members.
There is a secretary, responsible for
minutes, actions, the agenda, and
reporting back Committee decisions to
the CCGs.
NHS England will also have access to the
minutes etc. from the board for
assurance purposes, and all of these
documents will also be publically
available on CCG websites.
Committee includes representation of
both CCG and NHS England members
and both bodies have equal voting
representation*
The Chair and Vice/Deputy Chair of the
committee are CCG Lay Members.
There is a secretary, responsible for
minutes; actions, the agenda, and
reporting back Committee decisions to
NHS England and CCGs; and these will
also be publicly available on CCG
websites
Level Two: Joint Committee Level Three: Delegated Committee
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
54

29
expect, therefore, local dialogue between CCGs and their regional teams to determine how
the Committees can access the existing primary care team support, recognising that
CCGs are taking on significant responsibilities from NHSE, and therefore will require
access to a fair share of the regional team’s primary care commissioning staff resources
Area teams need to retain a degree of this resource, in order to safely and effectively
continue with their remaining responsibilities.
Currently, there is no possibility of additional administrative resources from NHS England at
this time, but this will be kept under review.
4. Processes & Capabilities
4.1 Meeting process: It is proposed that the method of operating the committee should follow processes already
established in CCG’s. The below illustrates a standard process for meeting setup:
Figure 10: Meeting process map
4.1.1 Agenda contents It will be important for engagement between NHS England and CCGs ahead of meetings,
particularly in cases where a particularly significant matter is on the agenda to be discussed.
This may involve the need for additional meetings, or for information from NHS England to
inform thinking. This will be particularly important for delegated commissioning, where NHS
England will not be participating in the committee discussion. Each Committee should set out
how this engagement will take place, as well as when, in the standard meeting process set
out above (Figure 10), submissions will be accepted for discussion at each meeting.
In general, clear and active engagement with NHS England, as well as the Committee sub
groups, will help inform the content of the agenda we expect that agendas are likely to have
the following components:
Standard agenda items, which might involve items that can be expected at each
meeting, such as an overview of finance and performance reports.
Work-plan items, such as a review of the annual budget or developing a Primary
Care Strategy, which is determined by the known upcoming work
Length of meeting cycle, and regularity of meetings, to be defined by Committee/ Joint Committee
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
55

30
Any other items, which could include submissions from NHSE, sub groups, and the
CCG.
There will also need to be a determination for whether part of the meeting needs to be in
private. The process for determining the privacy of meetings is set out in 4.2, below.
4.2 Meeting Papers As outlined in the reporting section on page 21, papers created by NHS England should be
submitted to the committee secretary 4 days before the papers are circulated in order to
allow time for them to be reviewed and comments and adjustments made.
It is expected according to standard meeting processes that papers may be circulated a
week before the meeting, although this should be determined by each committee and
referenced in their terms of reference.
It is important that requirements in terms of papers and presenters is made clear by the time
the agenda is finalised. Working groups and sub-committees should have clarity regarding
upcoming meetings and how work should feed into these boards, including the timelines
required.
Delegated CCGs should also ensure that where advice, recommendations or papers a re
required from NHS England, that this is sought and discussed in advance. The CCG may or
may not request NHS England presents the paper at the committee.
4.3 Meeting in private As standard, the Committee meetings will be held in public. However, the Committee may
require to close part of the meeting on account of the matters to be discussed. Only
members of NHS statutory bodies, that are bound by standard NHS confidentiality
agreements are expected to attend the closed part of meetings. Only attendees of the private
part of the meeting will receive the papers for that part of the agenda. If necessary it may be
important to redact names and other details from the minutes.
It may be appropriate for the committee to seek the views of the audit chairs once a definition
of this policy has been created for each committee. Below is some guidance which
Committees may wish to consider:
Whenever publicity would be prejudicial to the public interest by reason of the
confidential nature of the business to be transacted or for other special reasons
stated in the resolution and arising from the nature of that business or of the
proceedings; or
If the discussion is commercially sensitive; or
Where the matter being discussed is part of an ongoing investigation; or
For any other reason permitted by the Public Bodies (Admission to Meetings) Act
1960 as amended or succeeded from time to time.
The provision for private meetings should only be used where required (as per the criteria
above). Where the discussion is not as sensitive, other mechanisms could potentially be
used, such as anonymising the reports. Additionally, Members of the Committee shall
respect confidentiality requirements as set out in the CCG Constitution and Standing Orders.
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
56

31
5. Annexes
Annex Introduction The annexes included with this document aim to provide further detail to elements of the
Operating model where it is too detailed to include in the main body of the text. These are
not meant to be read as continuous chapters, but are included as reference material if
required. A short description of the purpose of each annex is included in a table below:
Annex Reference/ Name Purpose Annex 1: Detailed processes – including differences in responsibility by delegation level
This is the detailed memorandum of understanding aiming to outline the relative responsibilities of the CCG, NHS England and “the committee”. The committee includes both joint and delegated committees. This can be used if more detail is required on process and ownership, however it is suggested that where activities are unclear it may be beneficial to discuss with an NHS England or CCG colleague.
Annex 2: 13Z – CCG Statutory duties This lists the duties which effect the CCG that NHS England does not have liability for under section 13Z. This is included for its reference to roles and responsibilities.
Annex 3: Performer Contract Decision Making Process
This process aims to outline the decision making process specifically related to contract decisions arising from performer issues. It links into the overall decision making process flows (section 2).
Annex 4: Safeguarding – responsibilities at different levels of CCG co-commissioning delegation
This annex provides a high level analysis of responsibilities related to safeguarding at different levels of co-commissioning:
Annex 5: Pan London Responsibilities of NHS England STP Based Teams
This annex provides a list of matters dealt with on a pan-London basis, with lead NHS England STP based team responsibilities
Annex 6: Pan London Fora This annex provides an overview of pan-London Primary Care for a, their remit and membership
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
57

32
Annex 1: Detailed processes The tables below set out the key Co-Commissioning responsibilities and tasks of the Committee, the CCGs and NHS England.
Responsibilities Tasks/ Standard
Definition The Committee CCG NHS E The Committee CCG NHS E
1. Determination of key decisions/ requests
Determination to secure services through an APMS contract either a consequence of a practice vacancy, a finding that there are inadequate services in the area or following a contract expiration
To decide whether it is appropriate to undertake a procurement to appoint an APMS provider where there is a vacancy or a contract has expired. In making this decision the Committee must ensure that it is a viable and vfm service that will meet the needs of the current and future population, addresses inequalities, improves quality choice and access. The Committee is responsible for ensuring that appropriate engagement processes are in place to support decision making
To secure & provide, to the RT, local intelligence and feedback to support decision making. The CCG shall also provide relevant local strategic context to support decision making. The CCG may, if appropriate, agree additional resourcing for the service. To work jointly with the RT and local representative to identify new or alternative solutions to address the practice vacancy and additional local KPI requirements.
To secure & provide necessary information to support decision : - performance and service data; - equality impact assessment; - needs assessment; - available funding, including transitional funding; -service viability; - feedback from stakeholders and the CCG; -relevant guidance. To implement the decision of the Committee. To work jointly with the RT and local representative to identify new or alternative solutions to address the practice vacancy
Tasks: 1. Determine whether procurement is the best option in the interests of patients and the public and that no other options are viable to secure adequate services 2. Assure that correct processes have been followed, particularly in relation to patient and stakeholder engagement; 3. Confirm that the contract is affordable; 4. Confirm that the service is viable 5. Set tolerances for the cost and timeframe for implementation. 6. Ensure that an equality impact assessment has been undertaken 7. Ensure that the proposed procurement processes are undertaken in accordance with SFI's and regulations. Standard: Maintain a record of the decision, particularly in relation to potential conflicts of interest; Notify RT of decision with details of agreed funding and tolerances for implementation;
Tasks: 1. Provide local intelligence to the RT to support their report: 2. Provide relevant information about local strategies to be included in the RT report: 3. Where necessary present paper to The Committee, with RT 4. Where appropriate, secure additional CCG funding to support a new service prior to the Committee's determination 5. Provide relevant specifications and data to support local KPI's. Standard: To provide relevant information to the RT within 15 WD's of the request. To ensure that the Committee has information to support their decision making, including confirmation of any funding the CCG intends to make available for the service.
Tasks: 1. Undertake required needs assessment, feasibility analysis, financial modelling and impact assessments to support the decision making process. 2. Implement an appropriate engagement plan. 3. Work jointly with the CCG to identify any local KPI's or other commissioning opportunities. 4. Identify and secure any additional resources required to support options. 5. Establish a procurement project team to implement the Committee's decision, if required. 6. To maintain and update a database of fixed term contracts. 7. To procure the service in accordance with directions, regulations and guidance. Standard: To process in accordance with regulatory requirements, Relevant SFI's and agreed procurement processes.
Procurement of new Services under APMS agreements
The Committee is responsible for approving a preferred provider following procurement process following the evaluation process
The CCG is responsible for providing local standards and specifications to address local issues of access, quality and choice
The RT shall develop and implement procurement policies & programmes aimed RT securing new APMS providers.
Tasks: Develop local standards and KPI's to be incorporated into APMS contracts. Support providers to ensure optimum delivery. Communicate with local stakeholders as required.
Tasks: Develop London standards and KPI's to be incorporated in APMS Contracts. Standard: Use standard frameworks to secure services and ensure good value for money - Support providers to ensure optimum delivery. Standard: Procure APMS in line with the agreed commissioning strategy - Initiate formal procurement activity for each APMS scheme, within terms of any national procurement support. - Sign off/ finalise contracts with preferred bidder. - Agree/ implement the local mobilisation plan. - Undertake appropriate checks prior to service commencement (for example, premises inspection). - Make provision for emergency primary medical care services in the event of an unforeseen circumstance.
Determination of a requests; - to close a branch practice; -for practice mergers; -PMS partnerships; -List Closures; -Rent Reviews
To consider and determine requests in a timely manner following appropriate consultation and in accordance with statutory requirements and agreed policy; ensuring that any decision will secure continuity of services and provide benefits for patients and the public. The Committee will pay due considerations to Strategic imperatives and Statutory
To secure & provide, to the RT, local intelligence and feedback to support decision making. The CCG shall also provide relevant local strategic context to support decision making.
To secure & provide necessary information to support decision: - performance and service data; - feedback from stakeholders and the CCG; -relevant guidance. To implement the decision of the Committee.
Tasks: 1. Determine request; 2. Assure that correct processed have been followed, particularly in relation to patient and stakeholder engagement; 3. Provide minutes and decision rationale 4. Ensure continuity services as a consequence of their decision: 5. Maintain records of all decisions; 6. Respond to questions and queries relevant to the decision, including FOI requests.. Standard: Provide decision and rationale within 5 WD of the meeting:
Tasks: 1. Provide local intelligence to the RT to support their report: 2. Provide relevant information about local strategies to be included in the RT report: 3. Work jointly with RT to ensure patient benefit and service continuity; 4. Where necessary present paper to The Committee, with RT . Standard: All requested information to be provided within 10 WD: To make available relevant staff for meetings and case conferences pertinent to the decision
Tasks: 1. Processing the application; 2. Engagement/consultation with stakeholders and patients; 3. Notifying the CCG and The Committee secretariat ; 4. Preparing & presenting the report to the Committee, using agreed format; 5. Issue decision letters/ notices; 6. Support any practice closure using agreed protocol; 7. Updating databases and notifying 111 via CSU. Standard: To process in accordance with:
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
58

33
Responsibilities Tasks/ Standard
Definition The Committee CCG NHS E The Committee CCG NHS E
requirements to secure primary care services to meet the current and future needs of the population.
- Ensure that service continuity is not compromised as a consequence of their decision: - Ensure patient and public benefits are secured: - Acknowledge all queries within 5 WD offering full response within 20 WD: - Comply with FOI timescales
- National & London SOP; - Regulations- Contract and Patient Public engagement
GP Practices list maintenance
The Committee is responsible for decisions on any ad hoc list maintenance requests and for the setting of cleansing periods
NHS England is responsible for commissioning a process of practice list maintenance and will liaise with NHS Shared Business services and any other external partner as part of that.
Issue of Contract Breach Notice
To determine whether a provider has breached the terms of their contract and to make a proportionate decision as to whether: -a remedial or breach notice is warranted; -the practice should be asked to submit a improvement plan; -no action is required under the circumstances. To review outcome of remediation /improvement plans.
To identify & manage any resulting risk to services they commission as a consequence of an adverse finding. To provide support or facilitation for any relevant improvement plan/actions
To investigate concerns and provide evidence where a contract has been breached together with any mitigation offered by the provider using an agreed London template: To implement decisions
Tasks: 1. Review evidence and confirm that a contract has been breached; 2. determine the most appropriate and proportionate response to the breach taking account of relevant mitigation . Standard: Provide decision and rationale within 5 WD of the meeting: Ensure that service continuity is not compromised as a consequence of their decision: Ensure that there is a formal review of the outcome of all remediation and improvement plans.
Tasks: The CCG may be informed of concerns when a finding has been made, if it is relevant to any contract held between them and the provider. .
Tasks: 1. Identify concerns: 2. Investigate concerns: 3. Notify the provider of concerns and any evidence to support they have breached the contract: 4. Present evidence of the breach to the The Committee along with any mitigation provided by the provider: 5. Issue notices to the provider: 6. follow up remedial actions /action plans 7. liaise with the CQC and carry out actions to support registration 8. Produce format for local notices and breaches. Standard: Contract Regulations; National SOP Local protocols
Contract Termination
Determine the appropriateness of contract termination
To identify & manage any resulting risk to services they commission as a consequence of an adverse finding. To provide support or facilitation for any relevant improvement plan/actions
To investigate concerns and provide evidence where a contract has been breached together with any mitigation offered by the provider using an agreed London template: To implement decisions
Tasks: 1. Review evidence and confirm that a contract has been breached; 2. determine the most appropriate and proportionate response to the breach taking account of relevant mitigation . Standard: Provide decision and rationale within 5 WD of the meeting: Ensure that service continuity is not compromised as a consequence of their decision: Ensure that there is a formal review of the outcome of all remediation and improvement plans.
Tasks: The CCG may be informed of concerns when a finding has been made, if it is relevant to any contract held between them and the provider.
Tasks: Develop contract termination documentation, systems and processes. - Prepare Reports and Evidence for the Committee, securing necessary legal advice. - Issue termination notices. - Develop action plans to manage termination of contracts and implement in consultation with and supported by stakeholders. Update the contractor database with sanction information.
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
59

34
Responsibilities Tasks/ Standard
Definition The Committee CCG NHS E The Committee CCG NHS E
Contractual Payments
The Committee is responsible for assuring that systems and processes are in place to ensure accurate and prompt payments to GP Practices in accordance with Contracts, Agreements, The SFE and SFI's
The CCG is responsible for notifying the Committee of any systematic failure to promptly pay GP Providers in accordance with the Contract / Agreements and SFE, setting out how this is to be addressed
NHS E is responsible for notifying the Committee of any systematic failure to promptly pay GP Providers in accordance with the Contract / Agreements and SFE, setting out how this is to be addressed
Tasks: 1. Review evidence and confirm that a contract has been breached;2. determine the most appropriate and proportionate response to the breach taking account of relevant mitigation . Standard: Provide decision and rationale within 5 WD of the meeting:Ensure that service continuity is not compromised as a consequence of their decision:Ensure that there is a formal review of the outcome of all remediation and improvement plans.
Tasks: The CCG may be informed of concerns when a finding has been made, if it is relevant to any contract held between them and the provider.
Tasks: - Agree appropriate contract variations (for example, list size changes) including their input to payment systems. - Calculate any agreed local quality and outcomes framework arrangement. - Calculate the impact of key performance indicators on contractual payments (alternative provider medical services contracts). - Determine entitlements to personal allowances (for example, seniority/ locum reimbursement). - Calculate and pay enhanced services that are specified nationally.- Calculate payments for GP registrars in respect of salary, mileage and travel grants. - Calculate prescribing and dispensing drug payments. - Calculate entitlements under the GP retainer/ GP returner and flexible career schemes.- Calculate payments in respect of the dispensary service quality scheme. Administer superannuation regulations, including all deductions, in relation to joiners, leavers, retirements, increased benefits, adjustments and pay these to the pensions division. - Administer and validate GP annual certificates. - Administer GP locum and GP- Solo contributions. - Provide the NHS pension assurance statement.- For suspended contractors, ascertain the individual’s entitlements, advise the contractor, validate all documentation, and adjust payment accordingly.
Disputes and Appeals
The Committee is responsible for agreeing a policy and procedure for managing appeals and disputes submitted by GP's in relation to their GP Contract. This includes ensuring there is a local resolution process and that a Panel is established to consider disputes and appeals where local resolution is not successful.
Tasks: The Committee shall establish a Panel who will consider any appeal or dispute.. Standard: The Committee shall ensure that all decisions are made in accordance with the Contract Regulations, SFE, SOP and previous determinations.
Tasks: The RT shall : 1. Ensure that contractors receive a clear and concise notice setting out any determination under the contract; 2. Implement local resolution where a contractor disputes a determination; 3. Where Local Resolution is not successful notify the Committee of the need to establish a Panel; 4. Provide a report to the Panel setting out their rationale and evidence in support of their decision; 5. Present evidence & representations to the Panel 6. Notify the contractor of the outcome; 7. Provide information as required by the Litigation authority in relation to any appeal
2. Financial processes
Determine total budget requirements for all primary care services, including premises and information technology
The Committee is responsible for ensuring that financial balance is secured and maintained.
Under Delegated Arrangements the CCG CFO will approve the financial plan plus any in year revisions
NHS England finance teams accommodated at lead CCGs will carry out the day to day financial management tasks, including the production of monthly reports showing spending vs the agreed budget and variance analysis.
Tasks: Ensure appropriate financial controls are in place to securely manage the budgets.. Standard: Operates in accordance with NHSE or CCG SFIs.
Tasks: a) Maintain control total for revenue and capital limits and agreement of RFTs
Tasks: b) Financial Planning & Reporting including input to monthly board report, external reports, financial plan submissions and in year review of plans, budget setting & team co-ordination, month end overview. non ISFE reports to region, QIPP reporting.
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
60
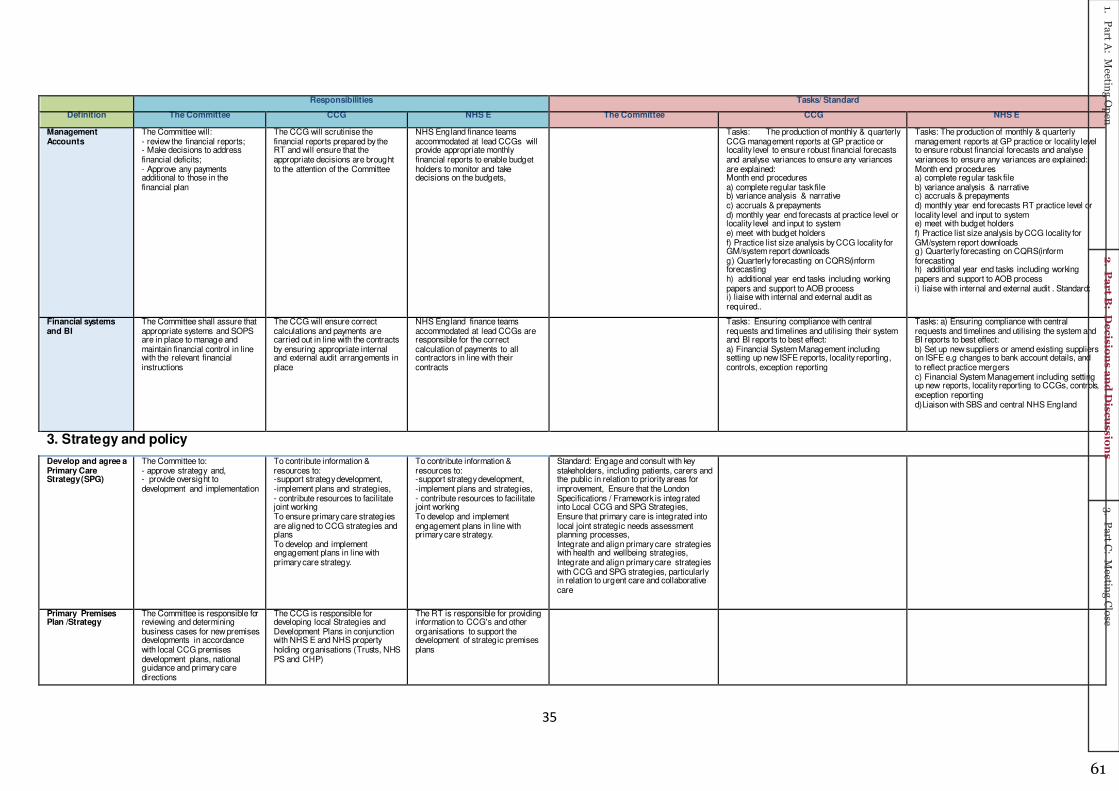
35
Responsibilities Tasks/ Standard
Definition The Committee CCG NHS E The Committee CCG NHS E
Management Accounts
The Committee will: - review the financial reports; - Make decisions to address financial deficits; - Approve any payments additional to those in the financial plan
The CCG will scrutinise the financial reports prepared by the RT and will ensure that the appropriate decisions are brought to the attention of the Committee
NHS England finance teams accommodated at lead CCGs will provide appropriate monthly financial reports to enable budget holders to monitor and take decisions on the budgets,
Tasks: The production of monthly & quarterly CCG management reports at GP practice or locality level to ensure robust financial forecasts and analyse variances to ensure any variances are explained: Month end procedures a) complete regular task file b) variance analysis & narrative c) accruals & prepayments d) monthly year end forecasts at practice level or locality level and input to system e) meet with budget holders f) Practice list size analysis by CCG locality for GM/system report downloads g) Quarterly forecasting on CQRS(inform forecasting h) additional year end tasks including working papers and support to AOB process i) liaise with internal and external audit as required..
Tasks: The production of monthly & quarterly management reports at GP practice or locality level to ensure robust financial forecasts and analyse variances to ensure any variances are explained: Month end procedures a) complete regular task file b) variance analysis & narrative c) accruals & prepayments d) monthly year end forecasts RT practice level or locality level and input to system e) meet with budget holders f) Practice list size analysis by CCG locality for GM/system report downloads g) Quarterly forecasting on CQRS(inform forecasting h) additional year end tasks including working papers and support to AOB process i) liaise with internal and external audit . Standard:
Financial systems and BI
The Committee shall assure that appropriate systems and SOPS are in place to manage and maintain financial control in line with the relevant financial instructions
The CCG will ensure correct calculations and payments are carried out in line with the contracts by ensuring appropriate internal and external audit arrangements in place
NHS England finance teams accommodated at lead CCGs are responsible for the correct calculation of payments to all contractors in line with their contracts
Tasks: Ensuring compliance with central requests and timelines and utilising their system and BI reports to best effect: a) Financial System Management including setting up new ISFE reports, locality reporting, controls, exception reporting
Tasks: a) Ensuring compliance with central requests and timelines and utilising the system and BI reports to best effect: b) Set up new suppliers or amend existing suppliers on ISFE e.g changes to bank account details, and to reflect practice mergers c) Financial System Management including setting up new reports, locality reporting to CCGs, controls, exception reporting d)Liaison with SBS and central NHS England
3. Strategy and policy
Develop and agree a Primary Care Strategy (SPG)
The Committee to: - approve strategy and, - provide oversight to development and implementation
To contribute information & resources to: -support strategy development, -implement plans and strategies, - contribute resources to facilitate joint working To ensure primary care strategies are aligned to CCG strategies and plans To develop and implement engagement plans in line with primary care strategy.
To contribute information & resources to: -support strategy development, -implement plans and strategies, - contribute resources to facilitate joint working To develop and implement engagement plans in line with primary care strategy.
Standard: Engage and consult with key stakeholders, including patients, carers and the public in relation to priority areas for improvement, Ensure that the London Specifications / Framework is integrated into Local CCG and SPG Strategies, Ensure that primary care is integrated into local joint strategic needs assessment planning processes, Integrate and align primary care strategies with health and wellbeing strategies, Integrate and align primary care strategies with CCG and SPG strategies, particularly in relation to urgent care and collaborative care
Primary Premises Plan /Strategy
The Committee is responsible for reviewing and determining business cases for new premises developments in accordance with local CCG premises development plans, national guidance and primary care directions
The CCG is responsible for developing local Strategies and Development Plans in conjunction with NHS E and NHS property holding organisations (Trusts, NHS PS and CHP)
The RT is responsible for providing information to CCG's and other organisations to support the development of strategic premises plans
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
61
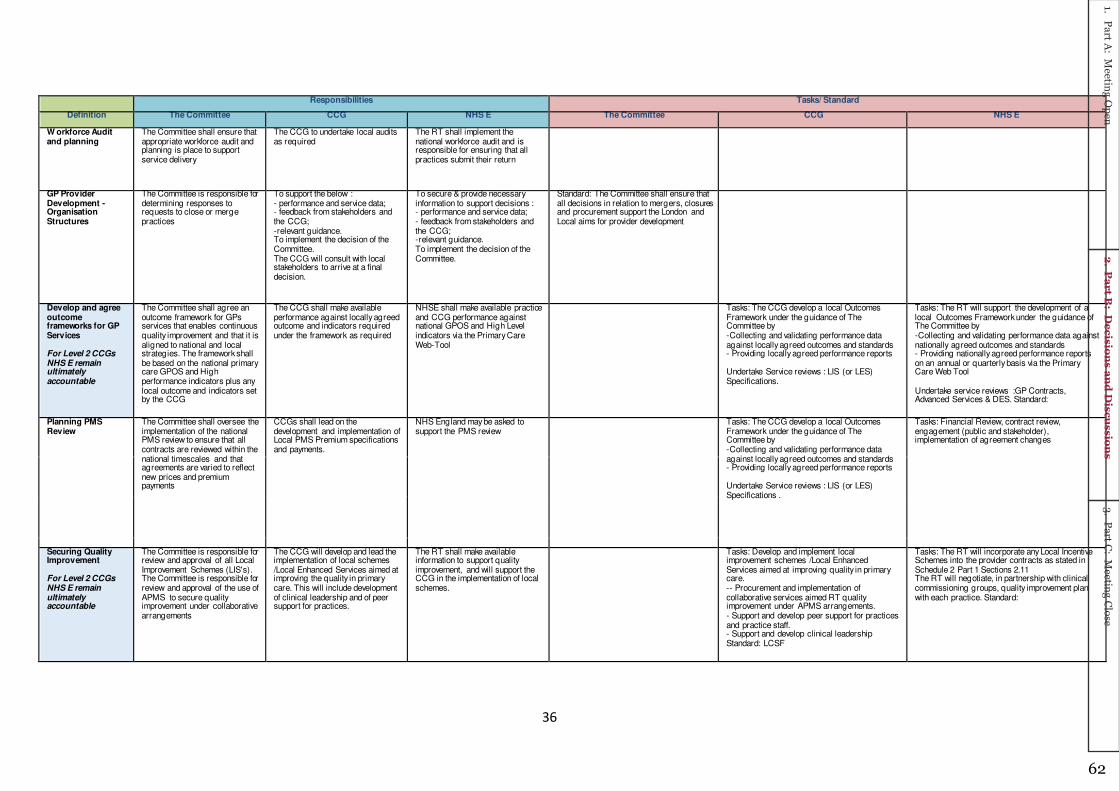
36
Responsibilities Tasks/ Standard
Definition The Committee CCG NHS E The Committee CCG NHS E
W orkforce Audit and planning
The Committee shall ensure that appropriate workforce audit and planning is place to support service delivery
The CCG to undertake local audits as required
The RT shall implement the national workforce audit and is responsible for ensuring that all practices submit their return
GP Provider Development -Organisation Structures
The Committee is responsible for determining responses to requests to close or merge practices
To support the below : - performance and service data; - feedback from stakeholders and the CCG; -relevant guidance. To implement the decision of the Committee. The CCG will consult with local stakeholders to arrive at a final decision.
To secure & provide necessary information to support decisions : - performance and service data; - feedback from stakeholders and the CCG; -relevant guidance. To implement the decision of the Committee.
Standard: The Committee shall ensure that all decisions in relation to mergers, closures and procurement support the London and Local aims for provider development
Develop and agree outcome frameworks for GP Services For Level 2 CCGs NHS E remain ultimately accountable
The Committee shall agree an outcome framework for GPs services that enables continuous quality improvement and that it is aligned to national and local strategies. The framework shall be based on the national primary care GPOS and High performance indicators plus any local outcome and indicators set by the CCG
The CCG shall make available performance against locally agreed outcome and indicators required under the framework as required
NHSE shall make available practice and CCG performance against national GPOS and High Level indicators via the Primary Care Web-Tool
Tasks: The CCG develop a local Outcomes Framework under the guidance of The Committee by -Collecting and validating performance data against locally agreed outcomes and standards - Providing locally agreed performance reports Undertake Service reviews : LIS (or LES) Specifications.
Tasks: The RT will support the development of a local Outcomes Framework under the guidance of The Committee by -Collecting and validating performance data against nationally agreed outcomes and standards - Providing nationally agreed performance reports on an annual or quarterly basis via the Primary Care Web Tool Undertake service reviews :GP Contracts, Advanced Services & DES. Standard:
Planning PMS Review
The Committee shall oversee the implementation of the national PMS review to ensure that all contracts are reviewed within the national timescales and that agreements are varied to reflect new prices and premium payments
CCGs shall lead on the development and implementation of Local PMS Premium specifications and payments.
NHS England may be asked to support the PMS review
Tasks: The CCG develop a local Outcomes Framework under the guidance of The Committee by -Collecting and validating performance data against locally agreed outcomes and standards - Providing locally agreed performance reports Undertake Service reviews : LIS (or LES) Specifications .
Tasks: Financial Review, contract review, engagement (public and stakeholder), implementation of agreement changes
Securing Quality Improvement For Level 2 CCGs NHS E remain ultimately accountable
The Committee is responsible for review and approval of all Local Improvement Schemes (LIS's). The Committee is responsible for review and approval of the use of APMS to secure quality improvement under collaborative arrangements
The CCG will develop and lead the implementation of local schemes /Local Enhanced Services aimed at improving the quality in primary care. This will include development of clinical leadership and of peer support for practices.
The RT shall make available information to support quality improvement, and will support the CCG in the implementation of local schemes.
Tasks: Develop and implement local improvement schemes /Local Enhanced Services aimed at improving quality in primary care. -- Procurement and implementation of collaborative services aimed RT quality improvement under APMS arrangements. - Support and develop peer support for practices and practice staff. - Support and develop clinical leadership Standard: LCSF
Tasks: The RT will incorporate any Local Incentive Schemes into the provider contracts as stated in Schedule 2 Part 1 Sections 2.11 The RT will negotiate, in partnership with clinical commissioning groups, quality improvement plan with each practice. Standard:
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
62

37
Responsibilities Tasks/ Standard
Definition The Committee CCG NHS E The Committee CCG NHS E
Securing Directed Enhanced Provision
The Committee shall review uptake and performance of all national DES and where necessary direct CCG's and RT's to take action to improve uptake or develop alternative local schemes
To support implementation as directed within the specifications
To support implementation as directed within the specifications. To provide information to the Committee on uptake and performance
Tasks: The CCG shall support local implementation and training as required under the national specification.
Tasks: The RT will disseminate all national DES specifications to practices together with local implementation guidance and a sign up sheet in accordance with the national timetable/ MOU (KPI's).
Securing Advanced Service Provision
The Committee shall review uptake and performance of all additional service provision and where necessary direct CCG's and RT's to take action to improve uptake or develop alternative local schemes
To provide information to the Committee about uptake and performance of non GP providers, making recommendations where additional services should be commissioned
To provide information to the Committee about uptake and performance of GP (& Pharmacy) providers, making recommendations where additional services should be commissioned
Tasks: Where necessary to direct the CCG or RT to take action to improve service provision.
Tasks: Procure additional services from non GP providers where practices do not wish to undertake them.
Tasks: Agree opt outs from the general medical services contract. Discuss locally the provision of additional services (where practices wish not to undertake them) with clinical commissioning groups.
Development of Policies and Procedures
The Committee shall approve all Local and endorse all London policies procedures in line with regulations
Tasks: Develop and maintain policies and procedures in line with regulations.
Contract Maintenance
The Committee shall ensure that the RT and CCG maintain all GP contracts in line with national and local variations and that systems are place to implement material changes
The RT will be responsible for the carrying out of several responsibilities specifically highlighted in the Delegation Agreement, including: 1. Managing Contract Variations The RT shall report, by exception, any failure to properly maintain contract documentation and provide an action plan to address this oversight
Tasks: - Issue national standard contract variations in line with changes to regulations. - Produce and issue local contractor specific variations (including, partnership changes, relocations, and mergers). - Implement changes to relevant systems to contractor payments. - Raise contract variations which may have a significant impact on the delivery of patient services and finances with localities and commissioners. - Maintain the contractor data base, including hard copies of all signed contracts for primary care providers, pertinent to the geographical area covered by the local regional team (including contract variations and breaches).
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
63

38
Responsibilities Tasks/ Standard
Definition The Committee CCG NHS E The Committee CCG NHS E
Quality Assurance GP Services For Level 2 CCGs NHS E remain ultimately accountable
The Committee will review reports to ensure GP's services are safe and meet all national and local standards. This will be monitored through an annual report on performance and the use of exception reports as required or as a result of a critical incident - Monitor activity on performers lists alongside practice performance data to generate a complete picture of quality
The RT will provide a regular quality report, based on the national framework to The Committee to support locality-wide quality assurance of primary care. This will include exception reports as required.
Tasks: Support practices and performers in the achievement of their quality improvement plan.
Tasks: The RT shall, using the national GPOS, High Level indicators, practice E-Declarations & CQC reports: 1. Collate Compliance Reports 2. Assess practice performance from analysed data and identify priorities for further interrogation 3. Provide an Annual Performance Report and any exception reports 4. Conduct contractual compliance and quality reviews, developing and agreeing action plans to address performance issues with contractors.. - Support each clinical commissioning group in the development of a primary medical care quality improvement strategy involving all practices . - The RT will support the CCG with information to establish any cause for concern and act accordingly, including a quality review where necessary and performance management arrangements for poorly performing practices. In particular the RT will ensure that: 1. It maintains regular and effective collaboration with the CQC and responds to CQC assessments 2. Ensure and Monitor Practice remedial action plans .
Develop processes and systems to ensure fair, open and transparent decision making
The CCG is responsible for implementing processes and systems as required by the Committee
The RT is responsible for implementing processes and systems as required by the Committee
4. Other Counter fraud To ensure that proper processes
are in place to prevent fraud within the NHS
Where CCGs hold contracts with GPs in their own name, where they contract and fund the services e.g. Enhanced Services, CCGs would continue to be allocated these allegations for investigation.
Implementation of the Deloitte Counter-Fraud service Deloitte will need to liaise with primary care staff who would have performance information in relation to GP contracts or perform Post Payment Verification visits
Tasks: Issue notification of stolen prescription forms or persons attempting to obtain drugs by deception, to GPs, pharmacists, counter fraud, drug squads and other interested parties.
Interpreting Services To ensure that patients have access to interpreting services when using GP practices
FOI For Level 2 CCGs NHS E remain ultimately accountable
Dependant on source of information as to owner of FOI responsibility
Tasks: To provide any information that the CCG holds about GP services as requested under the FOI act. Standard:
Tasks: To provide any information that the RT holds about GP services as requested under the FOI act.
Occupational Health The Committee shall ensure that GP practices have access to occupational health services in accordance with national guidance
Tasks: To secure contracts and access to OH services in line with the national guidance.
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
64

39
Responsibilities Tasks/ Standard
Definition The Committee CCG NHS E The Committee CCG NHS E
EPRR The Committee shall ensure that the RT and CCG develop strategies and plans to respond to rising tides, major incidents and service failure.
- Responding to local service disruption. - Responding to major service disruption. - Planning for major service disruption. - Flu Pandemic Planning. - Other Public Health Responses (e.g Ebola). - Issuing Communications to practices.
Implementation of Premises Directions
Approval of DV Rent Reviews, responding reimbursement appeals; Approval of discretionary payments for SDLT, Legal Fees and Development costs to practices; Procurement of Support for the Development of Strategic business cases; Approval of improvement grants; Approval of business cases for new premises / expansion; Approval of capital schemes; Approval of business cases for new premises /expansion
The RT shall bring to The Committee's attention as part of the regular reporting any matters requiring decision in relation to the Premises Cost Directions Functions including but not limited to: - new payments applications - existing payments revisions
Tasks: The CCG will respond to any requests from NHS England for relevant information to support the assurance of primary care commissioning.
Tasks: The RT will provide sufficient information to support The Committee's decision. Following decision from The Committee the RT is responsible for carrying out all subsequent payments. The RT must liaise where appropriate with NHS Property Services Ltd., Community Health Partnerships Ltd and NHS Shared Business Services.
Information sharing The Committee is responsible for ensuring that information relevant to assure the quality of primary care commissioning is shared in accordance with legislation and guidance.
The CCG is responsible for making available any information required to assure the quality of primary care commissioning as provided within IG rules
The RT is responsible for making available any reasonable and available information required to support primary care commissioning.
Tasks: The CCG will respond to any requests from NHS England for relevant information to support the assurance of primary care commissioning.
Tasks: The RT will respond to any requests from NHS England around information sharing as specified and will be responsible for auditing and ensuring that providers accurately record and report information.
Controlled drugs reporting
The Committee is responsible for ensuring that practices are complying with legal requirements for use of controlled drugs and CCGs and NHSE have proper controls in place to maintain patient safety
The RT will carry out any reporting, analysis, compliance or investigations involving controlled drugs.
Tasks: The CCG shall 1. Analyse prescribing data available 2. Complete the periodic self-assessments / self-declarations. 3. Report all incidents and other concerns to NHS England’s CDAO.
Tasks: The RT will support The Committee to comply with its obligations under Controlled Drugs regulations by Reporting all complaints
Safeguarding – children
To ensure that GP Practices have effective safeguarding systems in place in accordance with statutory requirements and national guidance and Pan London Policy and Procedures . Ensure appropriate response from primary care to safeguarding enquiries and serious case reviews (including approval of IMRs)
Support and facilitate Primary Care to proactively improve the safety and wellbeing of children registered within the practice setting, providing assurance to NHSE that practices are compliant with safeguarding standards.
To monitor and review compliance with safeguarding standards
Tasks: The RT will ensure that: 1. GP Contracts include requirements for safeguarding; and 2. GP practices annually declare compliance; The CCG shall provide representation at the LSCB. The CCG shall support GPs in engaging with serious case reviews, safeguarding adult reviews and domestic homicide reviews. Would recommend that NHSE RT approve GP IMRs. NHSE shall approve GP IMRs.
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
65

40
Responsibilities Tasks/ Standard
Definition The Committee CCG NHS E The Committee CCG NHS E
Safeguarding – adult To ensure that GP Practices have effective safeguarding systems in place in accordance with statutory requirements, NHSE national safeguarding guidance and Pan London Policy and Procedures Ensure appropriate response from primary care to safeguarding enquiries and serious case reviews (including approval of IMRs)
Support and facilitate Primary Care to proactively improve the safety and wellbeing of those adults most vulnerable registered within the practice setting, providing assurance to NHSE that practices are compliant with safeguarding standards.
To monitor and review compliance with safeguarding standards through CCG
Tasks: The RT will ensure that: 1. GP Contracts include requirements for safeguarding; and 2. GP practices annually declare compliance; NHSE shall approve GP IMRs. CCG shall have oversight of training compliance relating to safeguarding, MCA and Prevent. CCG is a statutory member of the LSAB and shall agree appropriate representation from health services including primary care
Domestic homicide Ensure that GPs contribute to domestic homicide reviews – where relevant and where necessary take action to remedy any oversight, including sharing and embedding learning to improve outcomes for service users.
To support practices in undertaking DHR where resources are held by the CCG
To support practices in undertaking DHR where resources are not held by the CCG
Tasks: Provide funding and advice where resources are not held by the CCG Provide representation at DHR Panels.
Serious incidents The Committee shall ensure processes are in place to report and review incidents so that serious incidents can be identified and managed. This includes reviewing the outcome of SI investigations and where necessary making recommendations to improve patient safety
To support and contribute to investigations
To support and contribute to investigations. To monitor compliance
Tasks: The RT will ensure that: 1. GP Contracts include requirements for reporting incidents; and 2. GP practices annually declare compliance; - Provide Advice and guidance to primary care practitioners and practice staff who wish to report an incident; Co-ordinate SI case management, including evaluation of final report; Liaison with NHS England Performance and Revalidation team regarding performance concerns.
Incident management
The Committee shall ensure that there are proper processes in place for GP practices to report incident (subject to a national review) and shall review reports on incidents at least once annually or where necessary by exception. The Committee shall make recommendations where necessary as a consequence on incident reports
To support and contribute to investigations
To support and contribute to investigations. To monitor compliance
Tasks: The RT will ensure that: 1. GP Contracts include requirements for incident management; and 2. GP practices annually declare compliance; Regularly log into the NRLS site to access any eForms (reported incidents); Ensure reported incidents are assessed to determine if SIs – and manage accordingly; Provide expert guidance on NRLS form/function.
Central Alerting System (CAS) Alerts
The Committee shall ensure that processes are in place to ensure that CAS alerts are disseminated in accordance with guidance.
To monitor compliance Tasks: The RT will ensure that: 1. GP Contracts include requirements for incident management; and 2. GP practices annually declare compliance; Regularly log into the NRLS site to access any eForms (reported incidents); Ensure reported incidents are assessed to determine if SIs – and manage accordingly; Provide expert guidance on NRLS form/function.
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
66

41
Responsibilities Tasks/ Standard
Definition The Committee CCG NHS E The Committee CCG NHS E
Engagement and Consultation For Level 2 CCGs NHS E remain ultimately accountable
The Committee shall ensure that all parties comply with statutory requirements to consult and engage with stakeholders. This is includes reporting to Local OSC, Healthwatch and HWB
For undertaking local engagement Engagement related to strategic planning Engagement linked to changes in urgent care or LES Engagement and consultation associated with changes to GP services, including: -closures, - premises development, - mergers
Supporting engagement and consultation associated with changes to GP services
Tasks: Consultation with LMC Presentations to OSC. HWB and Healthwatch
Tasks: Notification letters to patients Consultation letters to patients and stakeholders, with wording agreed with CCGs
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
67
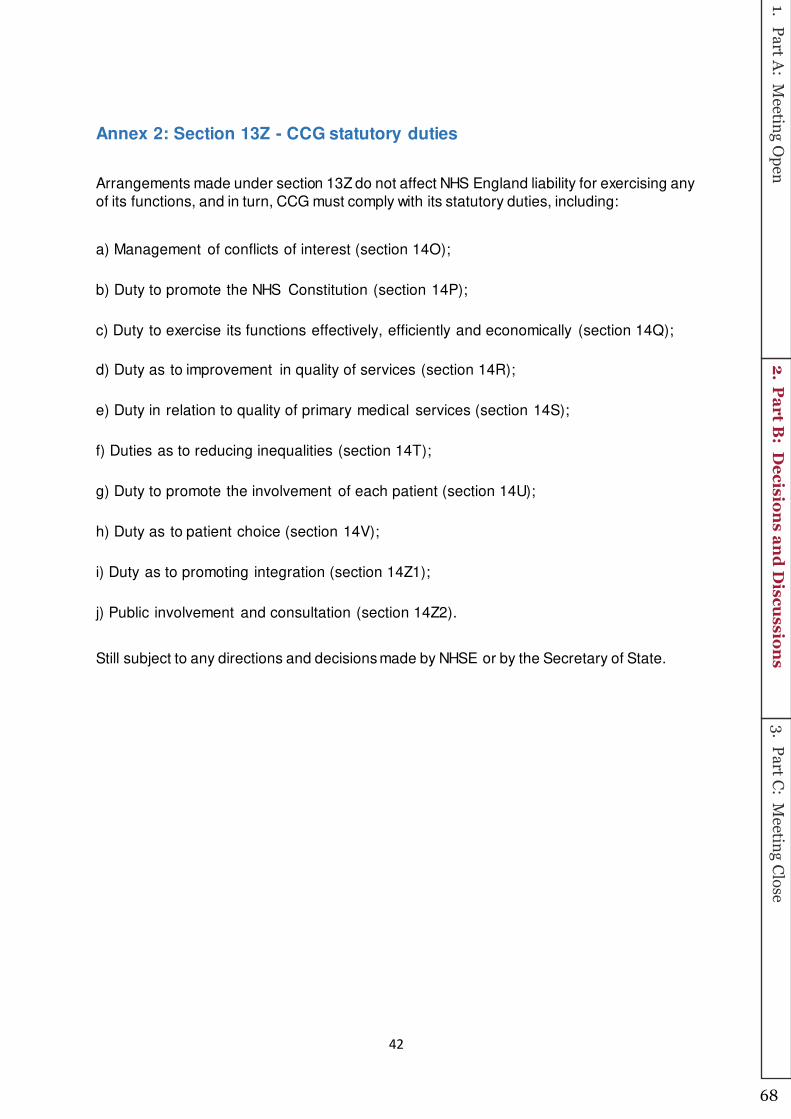
42
Annex 2: Section 13Z - CCG statutory duties
Arrangements made under section 13Z do not affect NHS England liability for exercising any
of its functions, and in turn, CCG must comply with its statutory duties, including:
a) Management of conflicts of interest (section 14O);
b) Duty to promote the NHS Constitution (section 14P);
c) Duty to exercise its functions effectively, efficiently and economically (section 14Q);
d) Duty as to improvement in quality of services (section 14R);
e) Duty in relation to quality of primary medical services (section 14S);
f) Duties as to reducing inequalities (section 14T);
g) Duty to promote the involvement of each patient (section 14U);
h) Duty as to patient choice (section 14V);
i) Duty as to promoting integration (section 14Z1);
j) Public involvement and consultation (section 14Z2).
Still subject to any directions and decisions made by NHSE or by the Secretary of State.
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
68

43
Annex 3: Performer Contract Decision Making Process
Figure 11 – Interface between the Performer Management and Contract Issue processes
Interface between the Performer Management and Contract Issue processes
Co er s a out perfor er perfor a e ay o e to NH“ E gla d’s atte tio through a u er of channels, including:
- Complaints from patients;
- Whistle-blowers;
- CCGs;
- CQC;
- GMC or other professional regulator;
- MPs; or
- The Police.
Concern raised
PAG
PLDP
Appropriate body
investigates and
takes action (may be
joint investigation)
Closed
Contract issue
process (CCG or
CCG/NHS E)
Contractual issue
Individual performer issue
Concerns may come through a number of
channels:
- Complaints
- Whistle blowers
- CCGS
- CQC
- GMC
- MPs
- Police
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
69
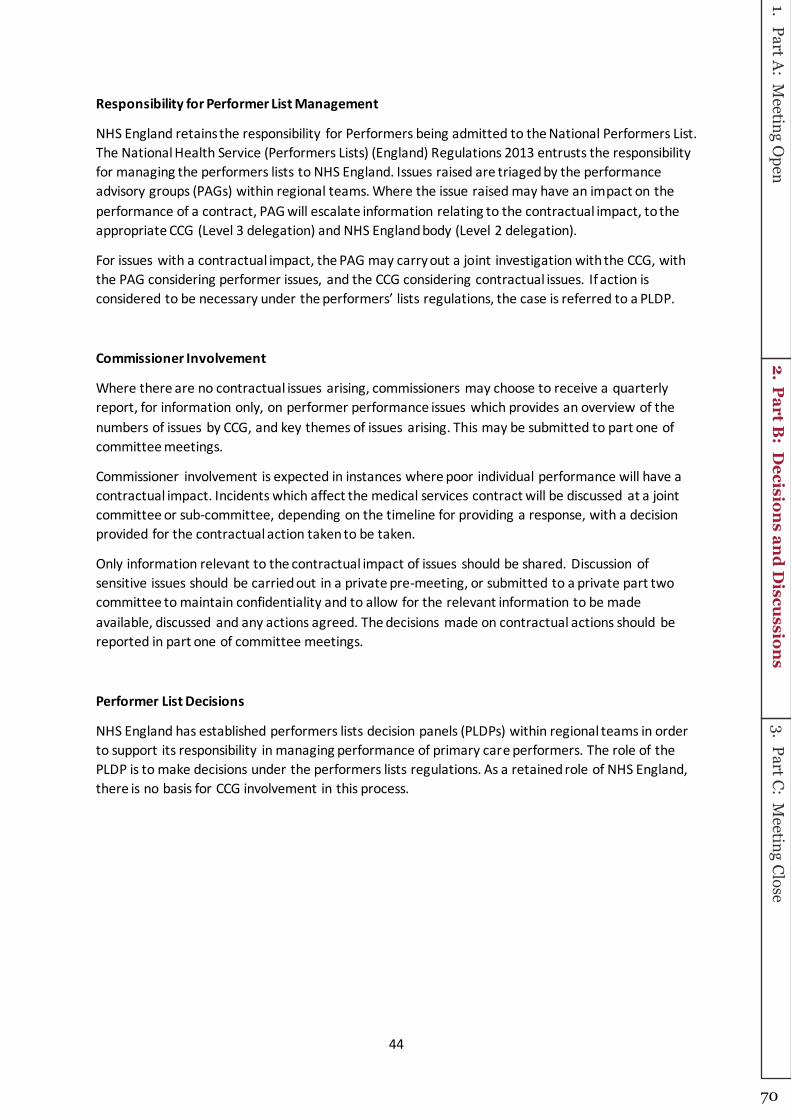
44
Responsibility for Performer List Management
NHS England retains the responsibility for Performers being admitted to the National Performers List.
The National Health Service (Performers Lists) (England) Regulations 2013 entrusts the responsibility
for managing the performers lists to NHS England. Issues raised are triaged by the performance
advisory groups (PAGs) within regional teams. Where the issue raised may have an impact on the
performance of a contract, PAG will escalate information relating to the contractual impact, to the
appropriate CCG (Level 3 delegation) and NHS England body (Level 2 delegation).
For issues with a contractual impact, the PAG may carry out a joint investigation with the CCG, with
the PAG considering performer issues, and the CCG considering contractual issues. If action is
o sidered to e e essary u der the perfor ers’ lists regulatio s, the ase is referred to a PLDP.
Commissioner Involvement
Where there are no contractual issues arising, commissioners may choose to receive a quarterly
report, for information only, on performer performance issues which provides an overview of the
numbers of issues by CCG, and key themes of issues arising. This may be submitted to part one of
committee meetings.
Commissioner involvement is expected in instances where poor individual performance will have a
contractual impact. Incidents which affect the medical services contract will be discussed at a joint
committee or sub-committee, depending on the timeline for providing a response, with a decision
provided for the contractual action taken to be taken.
Only information relevant to the contractual impact of issues should be shared. Discussion of
sensitive issues should be carried out in a private pre-meeting, or submitted to a private part two
committee to maintain confidentiality and to allow for the relevant information to be made
available, discussed and any actions agreed. The decisions made on contractual actions should be
reported in part one of committee meetings.
Performer List Decisions
NHS England has established performers lists decision panels (PLDPs) within regional teams in order
to support its responsibility in managing performance of primary care performers. The role of the
PLDP is to make decisions under the performers lists regulations. As a retained role of NHS England,
there is no basis for CCG involvement in this process.
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
70

45
Annex 4 - Safeguarding – responsibilities at different levels of CCG co-commissioning delegation
Task Level 2 Level 3
IMR sign off Joint sign off process CCG sign off
Named GPs* – role
transfer
Financial transfer
Recruitment
Training
MOU in place
Costs met from
delegated budget
HR process with NHS
England, joint
appointment panel
Responsibility for
training sits with NHS
England
MOU in place
Costs met from
delegated budget
Recruitment process
and appointment panel
under CCG control
Responsibility for
training sits with CCG
LSCB attendance Based on risk based
approach NHS England
and CCG attendance
Based on risk based
approach CCG
attendance
Domestic homicide Attendance at panel
and support to GP to
complete IMR
negotiated with CCG
CCG attends panel and
supports GP to
complete IMR if
required
Performance issues NHS England leads on
any performance issues
NHS England leads on
any performance issues
CQC safeguarding
issues in practices
NHS England and/or
CCG, by negotiation,
CCG follow up
individual issues raised
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
71

46
The table below provides a high level analysis of responsibilities related to safeguarding at different levels of co-commissioning:
dependent on each regional arrangements
Further detail related to the functions expected of fully delegated (level 3 CCGs) is shown below. The Nursing directorate would retain oversight of these
responsibilities, and it is important to note that the tasks might vary dependant on area etc.:
Summary of responsibilities Overview of tasks (not exhaustive)
Provide advice for GPs
undertaking investigations
relating to primary care
safeguarding issues
Manage named GP roles
Contribute to the system wide
oversight of safeguarding
Quality monitoring and
improvement of primary care
Approval final IMRs or investigations
including DH panels
Ensure any actions resulting from
investigations
Recruit, line manage and provide
training for role
Represent health system at
safeguarding boards
Undertake safeguarding assurance of
practices. Follow up on practice issues
identified at CQC inspections, review
trends and themes
follow up individual
issues raised by CQC
with practices
Themes/trends shared
with CCG
by CQC with practices
Themes/trends shared
with CCG
Primary care
safeguarding quality
assurance
Jointly NHS England
and CCG responsibility
CCG responsibility
Quality improvement CCG responsibility,
working with NHS
England
CCG responsibility,
working with NHS
England
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
72

47
Annex 5 – Pan London Responsibilities of NHS England STP Based Teams Category Responsibilities Lead STP Responsibilities Other STP responsibilities Forum Lead Notes
T&F Contract Management
policies/
Standard Operating
Framework
Task and Finish proposals to ensure
consistency. One engagement with local
committees
Comment and agree PCMB TBD for each task
T&F Homeless specification Input to Public Health initiative from a
primary care commissioning perspective
Comment and agree PCMB NWL & NEL Time limited
Contract
Management
Infection Control SLA Oversight of SLA with NEL CSU. Delivering
infection control framework which gives
assurance that primary care and dental
practitioners are meeting required
standards.
Activities include:
- quarterly SLA performance review
meetings with NHSE dental lead
- negotiation of annual budget
- ensuring network meetings are
operational where CCGs have local
arrangements in place to undertake
aspect of GP/dental infection prevention
and control support or monitoring visits
- annual review of specification to agree
priority visits, informed by liaison with STP
leads
- dissemination of arrangements,
including reinforcement of process flow
for urgent and planned visits
- negotiation of revisions to audit tool for
general practice, as and when necessary
with London LMC reps
- Feedback on service priorities
- implementation of STP day to day process,
based on agreed process flows for planned
and urgent visits
- Feedback on any issues of concern in terms
of SLA activities undertaken by NELCSU to lead
- provision of STP footprint information/data,
as requested by lead
- attendance at ad hoc meetings that may be
called
PCMB SEL To be reviewed annually
Retained Business Rates and Rent
Review - Backlog
Challenge session on business rates and
rent; QIPP measure for practices
Feedback PCMB SWL Time limited
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
73
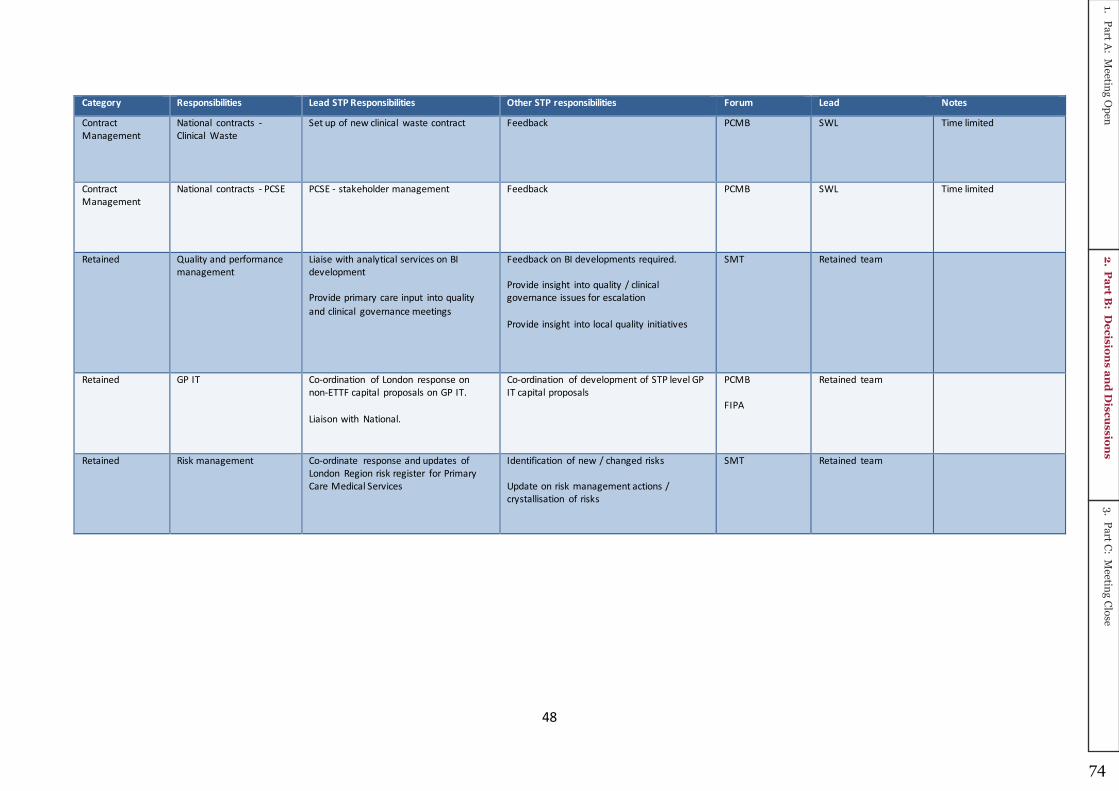
48
Category Responsibilities Lead STP Responsibilities Other STP responsibilities Forum Lead Notes
Contract
Management
National contracts -
Clinical Waste
Set up of new clinical waste contract Feedback PCMB SWL Time limited
Contract
Management
National contracts - PCSE PCSE - stakeholder management Feedback PCMB SWL Time limited
Retained Quality and performance
management
Liaise with analytical services on BI
development
Provide primary care input into quality
and clinical governance meetings
Feedback on BI developments required.
Provide insight into quality / clinical
governance issues for escalation
Provide insight into local quality initiatives
SMT Retained team
Retained GP IT Co-ordination of London response on
non-ETTF capital proposals on GP IT.
Liaison with National.
Co-ordination of development of STP level GP
IT capital proposals
PCMB
FIPA
Retained team
Retained Risk management Co-ordinate response and updates of
London Region risk register for Primary
Care Medical Services
Identification of new / changed risks
Update on risk management actions /
crystallisation of risks
SMT Retained team
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
74

49
Category Responsibilities Lead STP Responsibilities Other STP responsibilities Forum Lead Notes
Retained APMS Responsibilities include:
- complete and update the suite of
toolkits, templates and guidance
produced for the programme in order
that they can be shared with
commissioners for future use (London
retained responsibility).
- maintain and update the baseline
number of, and information about,
contracts identified as to be procured,
negotiated, extended or continued
(London information is dependent upon
STPs maintaining up to date baselines).
- identify a list of contracts for primary
medical services expiring before the end
of each financial year for which
commissioners will need to determine
commissioning options
- ensure the London APMS contract,
including Schedules, is brought up to date
and reporting arrangements finalised
(London retained responsibility).
- manage the arrangements for updating
and putting in place required contract
variations of all London APMS live
contracts (London initial responsibility).
-
- procurement of STP APMS contracts in
tranches, based on same consistent
timelines (London retained function)
-Designate STP programme lead
- Input of STP strategic commissioning
intentions into the development of
procurement programme.
- designate procurement lead responsibilities
either on a contract by contract, or STP basis
- undertake required commissioning
activities, strictly in line with agreed
project/programme timetable including (but
not limited to):
- strategic review of expiring APMS contracts
- preparation of report to PCCCs and feedback
on outcome to Programme lead (CCG
responsibility)
- patient engagement events(CCG
responsibility)
- preparation of MOIs, including liaison with
current APMS provider and input to ITT, in
collaboration with relevant CCG(CCG
responsibility)
- prepare report on outcome of patient
engagement (CCG responsibility)
- respond to clarification questions(CCG
responsibility)
-support site visits to practice premises(CCG
responsibility)
- evaluation and moderation of ITT responses,
based on agreed London (or STP)
arrangements (CCG responsibility)
- nominated officer to attend interview
panels(CCG responsibility)
- mobilisation of new APMS contracts(CCG
responsibility)
-attendance at local project or STP programme
meetings (CCG responsibility)
NOTE – this is not an exhaustive list of
activities but is indicative of type of activities
STP Programme leads are responsible for co-
ordinating, regardless of whether APMS
contracts are procured on a London or STP
footprint basis. In addition, all activities must
be undertaken with strict adherence to
procurement programme timescales
approved.
PCMB
FIPA
Retained procurement
team
Role of Band 8b London
Asst Head to maintain
best practice tools
STPs responsible for
Programme
management, linking in
to consistent London
procurement
programme
See revised lead
responsibilities to be
discussed at extraordinary
PCMB meeting on 15th
September 17
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
75
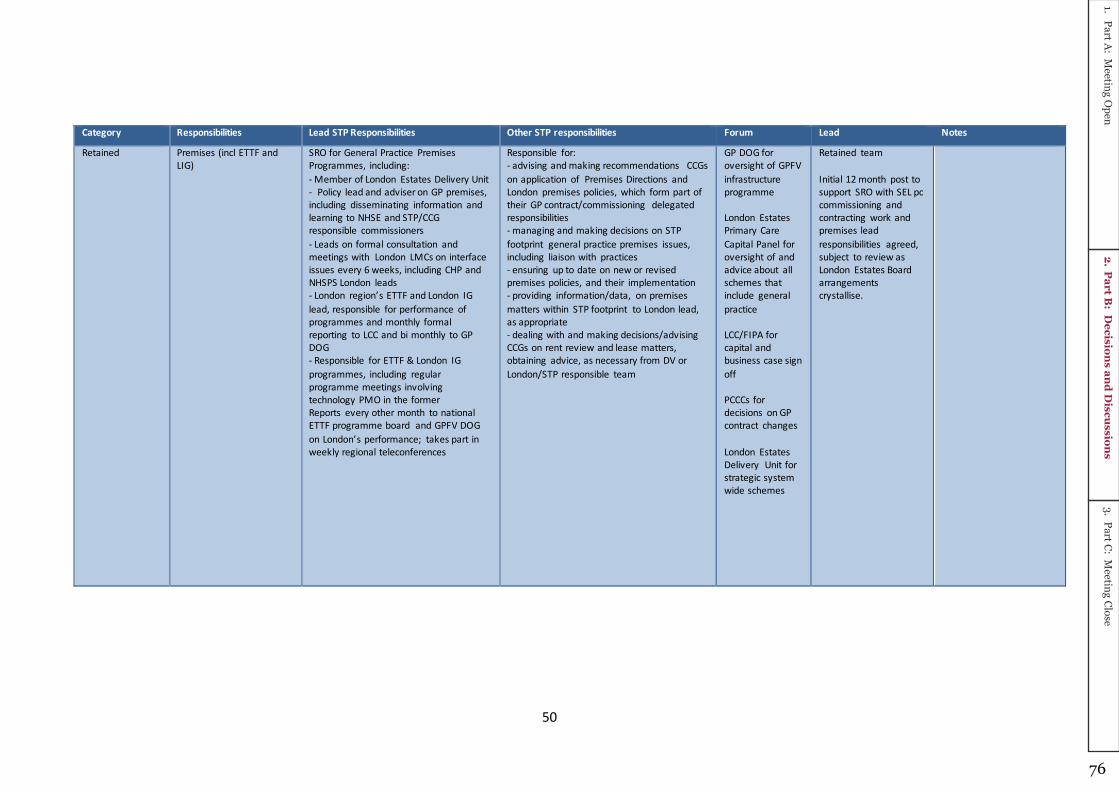
50
Category Responsibilities Lead STP Responsibilities Other STP responsibilities Forum Lead Notes
Retained Premises (incl ETTF and
LIG)
SRO for General Practice Premises
Programmes, including:
- Member of London Estates Delivery Unit
- Policy lead and adviser on GP premises,
including disseminating information and
learning to NHSE and STP/CCG
responsible commissioners
- Leads on formal consultation and
meetings with London LMCs on interface
issues every 6 weeks, including CHP and
NHSPS London leads
- Lo do regio ’s ETTF a d Lo do IG lead, responsible for performance of
programmes and monthly formal
reporting to LCC and bi monthly to GP
DOG
- Responsible for ETTF & London IG
programmes, including regular
programme meetings involving
technology PMO in the former
Reports every other month to national
ETTF programme board and GPFV DOG
o Lo do ’s perfor a e; takes part i weekly regional teleconferences
Responsible for:
- advising and making recommendations CCGs
on application of Premises Directions and
London premises policies, which form part of
their GP contract/commissioning delegated
responsibilities
- managing and making decisions on STP
footprint general practice premises issues,
including liaison with practices
- ensuring up to date on new or revised
premises policies, and their implementation
- providing information/data, on premises
matters within STP footprint to London lead,
as appropriate
- dealing with and making decisions/advising
CCGs on rent review and lease matters,
obtaining advice, as necessary from DV or
London/STP responsible team
GP DOG for
oversight of GPFV
infrastructure
programme
London Estates
Primary Care
Capital Panel for
oversight of and
advice about all
schemes that
include general
practice
LCC/FIPA for
capital and
business case sign
off
PCCCs for
decisions on GP
contract changes
London Estates
Delivery Unit for
strategic system
wide schemes
Retained team
Initial 12 month post to
support SRO with SEL pc
commissioning and
contracting work and
premises lead
responsibilities agreed,
subject to review as
London Estates Board
arrangements
crystallise.
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
76

51
Category Responsibilities Lead STP Responsibilities Other STP responsibilities Forum Lead Notes
and supports national ETTF team on
policy matters that affect London
- Leads design and oversees
implementation of STP and CCG
communication plans in the context of
new or revised policy and operational
requirements, supported by relevant
colleagues.
- Responsible for establishment &
management of commissioner led London
Estates Primary Care Capital Panel to
repla e Lo do ’s Pipeli e, supported y ETTF band 6 and ETTF PMOs & London IG
Programme lead.
- Responsible for bi annual review of
Lo do ’s ETTF Pipeli e
- Development & oversight of
i ple e tatio of Lo do ’s poli y of financial assistance for GPs with running
costs & services charges, in collaboration
with Finance lead & providing national
support to roll out
Retained Media, MP
correspondence, FOIs (pan
London)
Co-ordinate and manage responses to
queries
Provide information and locally agree
responses
By
correspondence
Retained team
Project PMS Lead customer of CSU PMO Progress reporting
Sharing leading practice
LMC engagement
PMS stakeholder
reference group
NWL
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
77

52
Category Responsibilities Lead STP Responsibilities Other STP responsibilities Forum Lead Notes
T&F For example:
- Violent patient scheme
- Minor surgery portal
- Caretaking framework
- Occupational health
service procurement
Lead on development of pan-London
approach
Input into T&F group.
Local implementation.
PCMB TBD per T&F
NEL have been leading on
a task and finish group for
moving to new primary
care occupational health
arrangements in line with
national guidance.
Following procurement, as
from 1st December 2017
there are now three
providers, contracted to
provide a limited range of
OH services, funded by
commissioners. This will
entail a small amount of
contract management
going forward covering
both dental and general
practices. This contract
management will be a
retained function.
Working Group Enhanced Services Lead on development of process to
implement national ES
Provide input into development
Ensure pan-London approach followed
Working Group
Recommendations
to PCMB
NWL
Working Group CQRS Systems lead to escalate issues and to
ensure Primary Care staff trained on CQRS
Liaise with lead on any CQRS issues Virtual network NWL
Assigned STP
team
responsibility
EPRR Not applicable To act as liaison point for in-hours incident
management
Not applicable Individual STPs
Assigned STP
team
responsibility
Quality and performance
management
Not applicable Production of reports for Committees Not applicable Individual STPs
Assigned STP
team
responsibility
National Primary Care
Leads
Attend HoPC and PC-DOG Input into meetings
Note output of meetings
SMT HoPC
Assigned STP
team
responsibility
CAS alerts Not applicable Cascade CAS alerts highlighted by Nursing
Directorate
Not applicable Individual STPs
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
78

53
Category Responsibilities Lead STP Responsibilities Other STP responsibilities Forum Lead Notes
STP responsibility Resilience Planning - e.g.
Winter / Bank Holiday
opening
Not applicable Ensure Primary Care included in resilience
planning
Provide information to NHSE L assurance
process
Not applicable A&E Boards
STP responsibility Complaints Not applicable To include in quality reporting
Feedback on local complaints management
Feedback on complaints process
Not applicable STP Complaints Leads
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
79

54
Forum Description Frequency Invitees
PCMB Part 1 Issues with operation of MOU Bi-monthly Deputy Regional Director
Regional Director of POD
Director of Primary Care Commissioning
STP Leads
Part 2 GP & DOP commissioning matters of pan-London interest (incl
agree T&F groups)
Non-delegated financial issues
As above, plus:
Heads of Primary Care
DOPs Regional Lead
NHSE Finance Senior Reps
NHSE Medical Directorate Reps
NHSE Nursing Directorate Reps
DCOs
Part 3 Assurance Deputy Regional Director
Director of Primary Care Commissioning
DCOs
SMT Operational and staffing issues
Emerging National or pan-London guidance
Suggest Task and Finish Groups
Fortnightly Director
HoPC
Assistant HOPC
DOPs Regional Lead
DOPs Assistant Regional Lead
DOPs Heads
All staff meeting National and pan-London developments
Staff development sessions
Team news
Quarterly All NHSE Primary Care Commissioning Staff
All staff call National and pan-London developments
Team news
Monthly All NHSE Primary Care Commissioning Staff
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
80
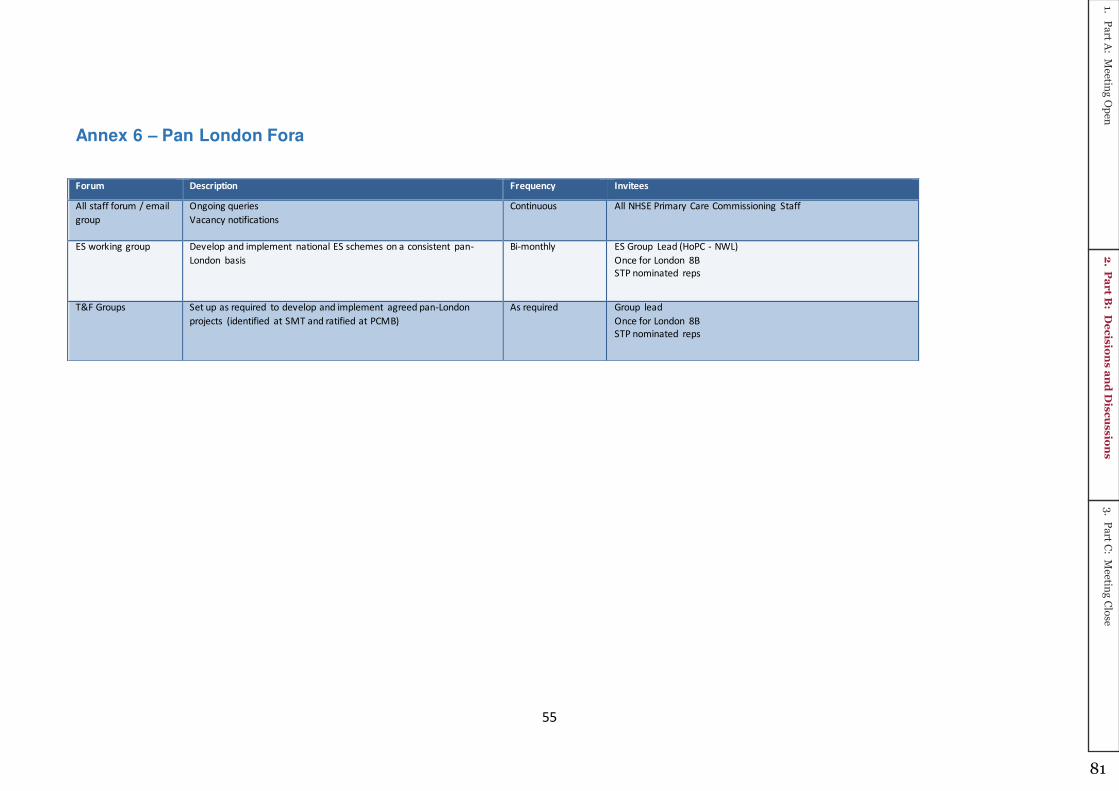
55
Annex 6 – Pan London Fora
Forum Description Frequency Invitees
All staff forum / email
group
Ongoing queries
Vacancy notifications
Continuous All NHSE Primary Care Commissioning Staff
ES working group Develop and implement national ES schemes on a consistent pan-
London basis
Bi-monthly ES Group Lead (HoPC - NWL)
Once for London 8B
STP nominated reps
T&F Groups Set up as required to develop and implement agreed pan-London
projects (identified at SMT and ratified at PCMB)
As required Group lead
Once for London 8B
STP nominated reps
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
81

56
Annex 7 – Template - Access for FutureNHS
The template below should be shared via STP leads with relevant stakeholders, and populated with the required information, following
which it should be sent back to Adrian Mccloskey [email protected] who will enable access.
Access to FutureNHS can take place from the beginning of January, subject to when STP leads return their completed templates :
Name Role CCG or STP? Organisation Name Email Address
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
82

General Purpose – Integrated Primary Care
Commissioning Paper Author: Kate Symons & Emma Gillgrass Sponsor: Andrew McMylor Date: September 2018
Executive Summary
Context
This is report provides the Primary Care Committee with an update on how delegated
Primary Care commissioning is being managed in Wandsworth; providing an update on
some of the key programmes of work.
Question(s)/ topics this paper addresses 1. How do we propose to monitor the PMS KPIs?
2. Joint Primary Care Quality Review Group (PCQRG) Update
3. What general contracting decisions have been made in the last quarter?
Conclusion 1. We propose to establish a local PMS Review Group, who will review the KPI retunrs on
a quarterly and annual basis as required. Learning from reviewing the KPI indicators will
be reported into both the Primary Care Quality Review Group and well as the Primary
Care Ops group as appropriate, with the final oversight of performance undertaken by
the Primary Care Committee
2. The GP patients Survey results have been published, a full report on the survey results
will be discussed at the Primary Care Quality Review Group in September, and a more
detailed update brought back to the next Committee.
3. The Committee are asked to note the decisions taken over the last quarter.
Input Sought The Committee are asked to note the detail included within this paper, and the progress
made under delegate commissioning arrangements.
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
83

The Report
A N A L Y S I S
1. How do we propose to monitor the PMS KPIs?
In 2016/17 the CCG undertook a review of the PMS Premium indicators in Wandsworth as
part of a nationally directed review process. As part of this process we had the opportunity
to review the old PMS indicators and engage clinicians in the development of new service
specification requirements that were clinically appropriate and strategically important, whilst
also ensuring that we continued to support sustainability across practices in Wandsworth.
A PMS Working Group was established and regular meetings took place with the Local
Medical Council (LMC) in order to develop and refine our approach; as well as agreeing
what we will be included in our local PMS Premium Offer. We utilised the opportunity
afforded to us under delegated primary care commissioning to look at the quality of the
previous indicators and work in a more broader sense to ensure that the new indicators are
fit for purpose, provide value for money, and clinical appropriate for the population of
Wandsworth
In total there are 39 Practices in Wandsworth; 28 of which are PMS Practices, 9 GMS and
2 APMS Practices.
We rolled out the developed PMS Premium indicators to all our PMS practices during the
end of 2017, early 2018 with all PMS Practices signing up to the new PMS Contract and
local Premium. We subsequently rolled out PMS KPI’s to our GMS Practices; with a phased implementation beginning from April 2018; achieving full equalisation by 2020.
As part of our delegated commissioning responsibility the CCG are also responsible for the
oversight of the PMS KPIs and the performance management of practices achieving these
indicators.
As such we are now in a position to begin to review these locally developed indicators as
part of the process of continuous improvement, review and reflection of the suitability of
each of those implemented.
What are the PMS Premium Indicators in Wandsworth?
The Wandsworth PMS Premium Indicators are made up of the following:
Improvement in the provision of a comprehensive annual diabetes review (8 care
processes) in Primary Care
Supporting the uptake of Influenza Vaccination in Primary Care
Supporting Improvement in the Uptake of Childhood Immunisations
Supporting the uptake of Bowel Cancer Screening in Primary Care
Increasing the use of Referral Management Software in Primary Care
Make A Difference (MAD) Alerts
Registered Patients in Deprived Areas
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
84

Supporting the Management of Children in Primary Care (Under 5’s)
What about the GMS Practices?
There are nine GMS Practices in Wandsworth, all of which have signed up to delivering the
PMS premium Indicators from 1st April 2018 onwards. In line with national requirements the
GMS indicators will be implemented on a phased approach in order to achieve full
equalisation by 2020.
The following details the agreed phasing for the indicators:
2018/19 Diabetes, Bowel Cancer Screening & Make a Difference Alerts (MAD)
2019/20 Addition of Childhood Immunisations, Deprivation and Children Under 5
2020 Addition of Flu Vaccination
How do we propose to monitor these indicators?
A standardised data collection template has been designed by the SWL Primary Care
Contracting Team, as they will be collecting the data on our behalf. This template details
the reporting requirements for each indicator, and as well as the format for reporting on
action planning, or where further performance feedback on the indicator is required.
It is the monitoring of areas that the SWL Team require input in from a local perspective; in
terms of the content on the action plans, and deciding on the best way to follow up these
area where required.
The Area’s that will be monitored via an Action Plan include: Diabetes action plan reviewing the baseline data and identifying areas for
improvement
Action plan based on review of flu vaccination rates for over 65’s
Action plan for improvement on childhood immunisation rates – annual lessons
learned action plan following this
Seldom Heard Group visit lessons learned feedback template
Examples of the practices engagement with the relevant services for their deprived
populations
Sharing learning from these reports will also be an important way of adding value to the
PMS Indicators. It may be through local review that examples of good practice are identified,
or learning can be shared where practices have made significant progress in increasing
certain rates, i.e bowel screening uptake. Ensuing that we have a local intelligence when
reviewing the data will provide a more robust review of these data returns, allowing for local
context where appropriate.
Who will review the indicators?
It is proposed that a local PMS Review Group will be established to look at the KPI returns,
on a quarterly and annual basis as required by the specific indicator. This group will include;
SWL primary care team lead
Locality Managers
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
85

Head of Primary Care Quality
Clinical Lead for Quality and local clinical leads as appropriate
Head of delegated commissioning
Where zero returns are made, or practices report a reduction towards meeting a target then
the group can review this data in light of any other local intelligence and agree whether there
should be any follow-up support provided to the practice. Conversely, where practice may
show significant improvements then the group can agree an approach to sharing good
practice/learning.
It is anticipated that the initial review meetings will focus on the baseline returns and action
plans, as well as ensuring the practice are able to provide the required information. This will
give an initial review as to the suitability of the KPIs as well as the use of the searches and
templates by each practice.
Subsequent review of the returns will enable the review of the suitability of the KPI indicators,
to ensure that we are getting full value and realising the anticipated benefits of each
indicator.
How do we plan to share the learning?
It is anticipated that learning will be shared more widely on an annual basis, as practice may
choose to implement improvements in a staged approach and therefore the full impact
and/or benefit of the indicators will not be realised until the full year.
We will however be mindful where early feedback indicates that certain KPIs may not be
appropriate or suitable to monitor, or where searches do not provide the appropriate data
i.e regular zero returns.
Learning from reviewing the KPI indicators will be reported into both the Primary Care
Quality Review Group and well as the Primary Care Ops group as appropriate, with the final
oversight of performance undertaken by the Primary Care Committee. Where areas of good
and even poor practice can be identified, then these groups can agree the best approach to
share this learning more widely; this may include locality updates or working with the
Practice Support Team to provide specific support where required.
Working with the LMC
One of the key success points of the PMS Review in Wandsworth was the engagement with
our local LMC colleagues to develop locally driven, fit for purpose indicators. With this is
mind the CCG aims to continue this engagement with the LMC in the review of the KPIs on
an annual basis to ensure that we continuously review the suitability of each indicator.
2. Joint Primary Care Quality Review Group (PCQRG) Update
GP Patient Survey 2018 - Wandsworth
The GP Patient survey is a national, annual survey, administered by Ipsos MORI on behalf
of NHS England. It provides practice level data about patients’ experiences of their GP
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
86
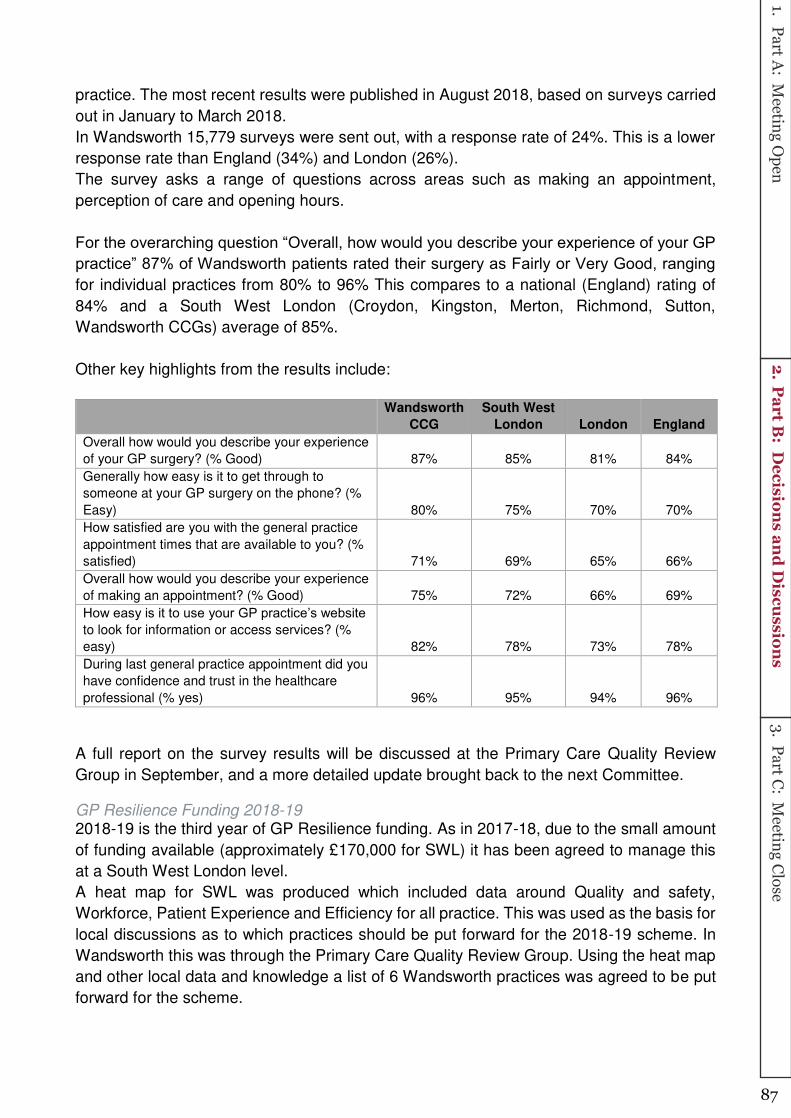
practice. The most recent results were published in August 2018, based on surveys carried
out in January to March 2018.
In Wandsworth 15,779 surveys were sent out, with a response rate of 24%. This is a lower
response rate than England (34%) and London (26%).
The survey asks a range of questions across areas such as making an appointment,
perception of care and opening hours.
For the overarching question “Overall, how would you describe your experience of your GP practice” 87% of Wandsworth patients rated their surgery as Fairly or Very Good, ranging for individual practices from 80% to 96% This compares to a national (England) rating of
84% and a South West London (Croydon, Kingston, Merton, Richmond, Sutton,
Wandsworth CCGs) average of 85%.
Other key highlights from the results include:
Wandsworth
CCG
South West
London London England
Overall how would you describe your experience
of your GP surgery? (% Good) 87% 85% 81% 84%
Generally how easy is it to get through to
someone at your GP surgery on the phone? (%
Easy) 80% 75% 70% 70%
How satisfied are you with the general practice
appointment times that are available to you? (%
satisfied) 71% 69% 65% 66%
Overall how would you describe your experience
of making an appointment? (% Good) 75% 72% 66% 69%
How easy is it to use your GP practice’s website to look for information or access services? (%
easy) 82% 78% 73% 78%
During last general practice appointment did you
have confidence and trust in the healthcare
professional (% yes) 96% 95% 94% 96%
A full report on the survey results will be discussed at the Primary Care Quality Review
Group in September, and a more detailed update brought back to the next Committee.
GP Resilience Funding 2018-19 2018-19 is the third year of GP Resilience funding. As in 2017-18, due to the small amount
of funding available (approximately £170,000 for SWL) it has been agreed to manage this
at a South West London level.
A heat map for SWL was produced which included data around Quality and safety,
Workforce, Patient Experience and Efficiency for all practice. This was used as the basis for
local discussions as to which practices should be put forward for the 2018-19 scheme. In
Wandsworth this was through the Primary Care Quality Review Group. Using the heat map
and other local data and knowledge a list of 6 Wandsworth practices was agreed to be put
forward for the scheme.
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
87

Practices were also offered the opportunity to self-nominate for the 2018-19 scheme and 9
Wandsworth practices put themselves forward, 2 of which had already been identified by
the CCG. The self-nominations were reviewed by the Primary Care Operational Group to
ensure they met the criteria for resilience support and 8 were approved.
The process for identifying and agreeing the specific packages for support is being managed
across all the SWL resilience practices and CCGs will be provided with regular update
reports.
3. What general Primary Care Contracting decisions have been made in the last quarter?
The following details the primary care contracting decision made in the last quarter; under
business as usual arrangements. Where the contractual changes are detailed these
decision would have been made through the usual governance arrangements; and therefore
taken at Committee level.
C O N C L U S I O N
The Committee are asked to note the ongoing work that has been jointly implemented
across Primary Care under delegated commissioning arrangements.
1.Part A
: Meeting O
pen2.
Part B
: Decision
s and
Discu
ssions
3.Part C
: Meeting C
lose
88


















