Student work from Fleisher Silkscreen Intensive class, August 2013

4/29/17
1
VolumetoValueTransitionintheUSA
LeeA.Fleisher,M.D.RobertD.Dripps ProfessorandChairofAnesthesiology
PerelmanSchoolofMedicineattheUniversityofPennsylvaniaEmail:[email protected]
Acknowledgement:PatrickConway,MD(formerActingAdministratorofCMS)forsomeofhisslides

4/29/17
2
33
Unexplained Variation
Dartmouth Atlas of Healthcare
4
Value
• The core issue in health care is the value of health care delivered
• Value is the only goal that can unite the interests of all system participants
Value=Patienthealthoutcomesperdollarspent
Michael Porter NEJM 2010

4/29/17
3
5
• Triple Aim• better care for individuals• better health for populations• lower costs
6
The Six Goals of the National Quality Strategy
Make care safer by reducing harm caused in the delivery of care
Strengthen person and family engagement as partners in their care
Promote effective communication and coordination of care
Promote effective prevention and treatment of chronic disease
Work with communities to promote healthy living
Make care affordable
1
2
3
4
5
6

4/29/17
4
7
CMSsupportofhealthcareDeliverySystemReformwillresultinbettercare,smarterspending,andhealthierpeople
Keycharacteristics§ Producer-centered§ Incentivesforvolume§ Unsustainable§ FragmentedCare
SystemsandPolicies§ Fee-For-ServicePayment
Systems
Keycharacteristics§ Patient-centered§ Incentivesforoutcomes§ Sustainable§ Coordinatedcare
SystemsandPolicies§ Value-basedpurchasing§ AccountableCareOrganizations§ Episode-basedpayments§ MedicalHomes§ Quality/costtransparency
PublicandPrivatesectors
EvolvingfuturestateHistoricalstate
8
Value-Based Programs
• Goal is to reward providers and health systems that deliver better outcomes in health and health care at lower cost to the beneficiaries and communities they serve.
• Five Principles
- Define the end goal, not the process for achieving it
- All providers’ incentives must be aligned
- Right measure must be developed and implemented in rapid cycle
- CMS must actively support quality improvement
- Clinical community and patients must be actively engaged
VanLare JM, Conway PH. Value-Based Purchasing – National Programs to Move from Volume to Value. NEJM July 26, 2012

4/29/17
5
9
CMShasadoptedaframeworkthatcategorizespaymentstoproviders
Description
MedicareFee-for-Serviceexamples
§ Paymentsarebasedonvolumeofservicesandnotlinkedtoqualityorefficiency
Category1:FeeforService–NoLinktoValue
Category2:FeeforService–LinktoQuality
Category3:AlternativePaymentModelsBuiltonFee-for-ServiceArchitecture
Category4:Population-BasedPayment
§ Atleastaportionofpaymentsvarybasedonthequalityorefficiencyofhealthcaredelivery
§ Somepaymentislinkedtotheeffectivemanagementofapopulationoranepisodeofcare
§ Paymentsstilltriggeredbydeliveryofservices,butopportunitiesforsharedsavingsor2-sidedrisk
§ Paymentisnotdirectlytriggeredbyservicedeliverysovolumeisnotlinkedtopayment
§ Cliniciansandorganizationsarepaidandresponsibleforthecareofabeneficiaryforalongperiod(e.g.,≥1year)
§ LimitedinMedicarefee-for-service
§MajorityofMedicarepaymentsnowarelinkedtoquality
§ Hospitalvalue-basedpurchasing
§ PhysicianValueModifier
§ Readmissions/HospitalAcquiredConditionReductionProgram
§ AccountableCareOrganizations§Medicalhomes§ Bundledpayments§ ComprehensivePrimaryCareinitiative
§ ComprehensiveESRD§Medicare-MedicaidFinancialAlignmentInitiativeFee-For-ServiceModel
§ EligiblePioneerAccountableCareOrganizationsinyears3-5
§Marylandhospitals
Source:RajkumarR,ConwayPH,Tavenner M.CMS─engagingmultiplepayersinpaymentreform.JAMA2014;311:1967-8.
BlumenthalDetal.NEnglJMed2015;372:2451-2458.
Ten-Year Medicare Spending Projections, January 2010 through March 2015.

4/29/17
6
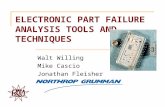
11
DuringJanuary2015,HHSannouncedgoalsforvalue-basedpaymentswithintheMedicareFFSsystem
OnMarch3,2016,PresidentObamaandHHSannouncedthat30percentofMedicarepaymentsaretiedtoqualitypaymentsthroughAPMs.Thisgoalwasachievedoneyearaheadofschedule!
12
2016
30%
85%
2018
50%
90%
Targetpercentageofpaymentsin‘FFSlinkedtoquality’and‘alternativepaymentmodels’by2016and2018
2014
~20%
>80%
2011
0%
~70%
GoalsHistoricalPerformance
AllMedicareFFS(Categories1-4)FFSlinkedtoquality(Categories2-4)Alternativepaymentmodels(Categories3-4)

4/29/17
7
14
PartnershipforPatientscontributestoqualityimprovements
Ventilator-Associated Pneumonia
Early Elective Delivery
Central Line-Associated
Blood Stream Infections
Venous thromboembolic complications
Re-admissions
LeadingIndicators,changefrom2010to2013
62.4% ↓ 70.4% ↓ 12.3% ↓ 14.2% ↓ 7.3% ↓
Datashowsfrom2010to2014…
87,0002.1 millionPATIENT HARM EVENTS AVOIDED
$20 billionIN SAVINGS

4/29/17
8
15
Legend: CL: controllimit;UCL: upper control limit; LCL: lower controllimit
ReadmissionRate
16
'Jaw-dropping': Medicare deaths,hospitalizations AND costs reduced
Sample consisted of 68,374,904 unique Medicare beneficiaries (FFS and Medicare Advantage).
Mortality, Hospitalizations, and Expenditures for the Medicare Population Aged 65 Years or Older, 1999-2013; Harlan M.Krumholz, MD, SM; Sudhakar V.Nuti, BA; Nicholas S. Downing,MD; Sharon-Lise T. Normand, PhD; YunWang, PhD; JAMA.
2015;314(4):355-365.; doi:10.1001/jama.2015.8035
1999 2013 Difference
All-cause mortality 5.30% 4.45% -0.85%
TotalHospitalizations/
100,000beneficiaries
35,274 26,930 -8,344
In-patientExpenditures/
Medicare fee-for-service beneficiary
$3,290 $2,801 -$489
End of LifeHospitalization (last 6months)/100 deaths
131.1 102.9 -28.2

4/29/17
9
17
Payment reform
• Traditional fee-for-service• Reduced
reimbursement• Bundled payments• Accountable Care
Organizations
18
Thebundledpaymentmodeltargets48conditionswithasinglepaymentforanepisodeofcare
Ø Incentivizesproviderstotakeaccountabilityforbothcostandqualityofcare
Ø FourModels- Model1:Retrospectiveacutecarehospitalstayonly- Model2:Retrospectiveacutecarehospitalstaypluspost-acutecare- Model3:Retrospectivepost-acutecareonly- Model4:Prospectiveacutecarehospitalstayonly
§ 337Awardeesandover1500EpisodeInitiators asofJanuary2016
BundledPaymentsforCareImprovementisalsogrowingrapidly
§ Durationofmodelisscheduledfor5years:§ Model1:AwardeesbeganPeriodofPerformancein
April2013§ Models2,3,4:AwardeesbeganPeriodof
PerformanceinOctober2013

4/29/17
10
Medicare Payment Prior to MACRA
The Sustainable Growth Rate(SGR)
• Established in 1997 to control the cost of Medicare paymentstophysicians
Fee-for-service (FFS) payment system,where clinicians are paid based onvolume of services, not value.
TargetMedicare
expenditures
Overallphysiciancosts
>IF Physicianpaymentscut
across the board
Each year, Congress passed temporary “doc fixes” to avert cuts(no fixin 2015would have meant a 21% cut in Medicare paymentstoclinicians)
20
Implications of MACRA
Clinician InvolvementRelationships/Partnerships/Arrangements will need to evolve in order to attract, retain, evaluate and optimize
Patient EngagementGreater coordination of care and two-sided risk for health care providers will raise the stakes for health care providers to foster closer ties with patients and help them actively manage their health
ReputationalMIPS Composite Performance Score (CPS) results will be made public and transparency will expose the good and the bad
Strategic/CompetitivePrioritizes strategic Physician Acquisition/Growth decisions related to who (Primary Care Physicians (PCPs)/Specialties, etc.), where, when, how (types of arrangements)
TechnologicalRequires robust clinical data capabilities (data governance, capture, collection, validation and reporting)
ClinicalRequires clinicians to change/ add incremental workflow and assess and improve clinical quality outcomes
Requires organization-wide collaboration and coordination of eligibility, multiple moving parts and regulatory requirements
FinancialAffects future Medicare reimbursement for all clinicians paid under the Medicare PFS
Key Impact Areas
The new MACRA law significantly impacts a number of key areas across health care providerorganizations
Operational

4/29/17
11
MIPS: First Stepto a Fresh Start
ü MIPS is a new program
ü MIPS provides clinicians the flexibility tochoose the activities andmeasuresthat aremostmeaningful totheir practice todemonstrateperformance.
Resource use
• Streamlines 3currently independent programs towork as oneandtoeaseclinician burden.
• Addsa fourth component topromote ongoing improvement andinnovation to clinical activities.
2aQuality
:Advancingcareinformation
Clinicalpracticeimprovementactivities
22
Traditional Model:Organize by Specialty and Discrete Service
Porter’s Integrated Practice Unit
Shared Ancillary ServicesSmoking Cessation Patient Education Substance Abuse
Primary Care
Physicians
Shared FacilitiesOperating Rooms
Chemotherapy Radiation Therapy Diagnostic Imaging
Pathology Lab
Emerging Model:Organize into Integrated Practice Units Around Conditions
Shared SpecialtiesAnesthesiologist
Cardiologist,Endocrinologist
& OtherSpecialties
Head & Neck Center
Medical Oncologists Surgical Oncologists Radiation Oncologists Dental Oncologists Radiologist Pathologist
NurseSocial Worker Patient Access Nutritionist PatientAdvocate
Facilities Outpatient Clinic Swallowing Lab Hearing Lab ProsthodonticLab
Outpatient Oncologist
SurgicalOncologist
Speech & Swallow
Dentist
Primary Care Physician
Radiation Oncologist
Radiologist
Pathologist
Anesthesiologist
22Source: Porter, Michael E., Jain, Sachin, The University of Texas MD Anderson Cancer Center: Interdisciplinary Cancer Care. February 26, 2013.

4/29/17
12
23
Why do we need to define value?
Bundled care-How do we divvy up the pie?
Traditional FFSFixed paymentLower fixed payment and share in any profit margin
Shouldtheanesthesiologistbeallowedtoshareinpotentialreward?
Doestheanesthesiologistwanttoassumeanyrisk?
24
Healthcare Consumerism

4/29/17
13
25
HCAHPS Patient Experience Domains
• Summary Measures• Communication with nurses (3 items)• Communication with doctors (3 items)• Responsiveness of hospital staff (2 items)• Pain management (2 items)• Communication about medicines (2 items)• Discharge information (2 items)
• Individual Measures• Cleanliness of hospital environment• Quietness of hospital environment
• Global Measures• Overall rating of hospital

4/29/17
14
27
28

4/29/17
15
29
RACI CHART
30
My vision
• When we transition from volume to value, we will need to be more engaged in patient care• Perioperative Care- SURGEON IS ACCOUNTABLE BUT MAY DELEGATE
• eg.Urology,OrthoatUCI,Kaiser• Decision making with regard to surgery- ANESTHESIOLOGIST AS
CONSULTANT• Intraoperative Management- ANESTHESIOLOGIST RESPONSIBLE• Postoperative Care- ICU- ANESTHESIOLOGIST RESPONSIBLE
• Ward- NURSESRESPONSIBLE,ANESTHESIOLOGISTORSURGEONORINTERNIST/HOSPITALISTINFORMEDABOUTPAIN
WHO IS ACCOUNTABLE- EG. CARDIAC SURGEONS DELEGATE TO ANESTHESIOLOGIST AT PENN
• Post-discharge- SURGEON ACCOUNTABLE BUT MAY DELEGATE TO INTERNIST

4/29/17
16
31
Ø Alternativepaymentmodelsgreaterthan50%ofpayments
- ACOs
- BundledPayments
- ComprehensivePrimaryCare
- OtherAPMs
Ø PrivatepayerandCMScollaborationcritical
Ø StatesandcommunitiesdrivingInnovationanddeliverysystemreform
Ø Increasingintegrationofpublichealthandpopulationhealthwithhealthcaredeliverysystem
Ø Patient-centered,coordinatedcareisthenorm
Ø Focusonqualityandoutcomes
FutureofHealthSystem