
Vol. 25 No. 3 May-June 2012 INTENSIVE CARE · In-HospItal Breast FeedIng WarmIng Human mIlk ......
24
neonatal INTENSIVE CARE Vol. 25 No. 3 May-June 2012 SPECIAL SUPPLEMENT IN-HOSPITAL BREAST FEEDING WARMING HUMAN MILK FITTING BREAST SHIELDS BREAST PUMPING HYGIENE HMBANA GUIDELINES HUMAN MILK STORAGE
Transcript of Vol. 25 No. 3 May-June 2012 INTENSIVE CARE · In-HospItal Breast FeedIng WarmIng Human mIlk ......
neonatalINTENSIVE CARE
Vol. 25 No. 3May-June 2012
SPECIAL SUPPLEMENT
In-HospItal Breast FeedIngWarmIng Human mIlkFIttIng Breast sHIeldsBreast pumpIng HygIeneHmBana guIdelInesHuman mIlk storage

2 neonatal INTENSIVE CARE Supplement 2012
Table of Contents3 Improving In-Hospital Breastfeeding Management for the
Late PretermMaria Lennon, RN, MSN, CNM, IBCLCIt is essential for a mother and her family to be educated on the importance of breastmilk and how it provides not only optimal nutrition for her late preterm infant but also helps protect from disease and improved developmental outcomes.
7 Best Practices for Warming Human Milk in a Hospital SettingJean Rhodes, PhD, CNM, IBCLCHuman milk feedings in the hospital setting involve a complex matrix of issues related to the intricate nature of human milk and the potential hazards of milk storage and preparation. Through the use of innovative technology, and with effective clinical implementation, the Medela Waterless Milk Warmer may help maintain the optimal integrity of human milk feeds for hospitalized infants.
10 Correctly Fitting Breast Shields: A Guide for CliniciansIrene Murphy Zoppi, RN, MSN, IBCLCClinicians need to know how the pump components work together and how to ensure mothers are using correctly sized breast shields… Clinicians should know specific breast shield sizing criteria that are straightforward and can be easily interpreted and taught to mothers.
13 Evidence-Based Recommendations for Breast Pumping HygieneJean Rhodes, PhD, CNM, IBCLCExpressing human milk as hygienically as possible will diminish the risk of pathogenic contamination and decrease microbial growth in stored human milk; however, the process is fragile and any break in technique can lead to undesired results.
16 Current Breast Pump Recommendations for NICU Mothers: 2011 HMBANA Guidelines – an Essential ResourceJean Rhodes, PhD, CNM, IBCLCCurrent best practice standards continue to recommend the use of hospital-grade electric pumps when infants cannot go to breast or when they cannot breastfeed effectively.
20 Human Milk Storage in the NICU – Summarizing the Research – What You Should KnowAmy O’Malley, RN, MSNTo decide which storage guidelines are appropriate, the age and health of the infant as well as other factors must be considered. With high-risk infants, the safest approach is to minimize contamination and use appropriate storage conditions for the shortest storage time possible.
6 neonatal INTENSIVE CARE Vol. 24 No. 4 n July-August 2011
Arie L. Alkalay, MDClinical Professor of PediatricsUCLA School of MedicineLos Angeles, CA
M. A. Arif, MDProfessor of Pediatrics & Head, NeonatologyNational Institutes of Child HealthKarachi, Pakistan
Muhammad Aslam, MDInstructor in Pediatrics, Harvard Medical SchoolNeonatologist & Director of EducationNeonatology and Newborn Medicine UnitDepartment of PediatricsMassachusetts General Hospital for ChildrenBoston, MA
Edward Austin, MDAssistant Clinical ProfessorPediatric SurgeryUniversity of California-San FranciscoSan Francisco, CA
Richard L. Auten, MDAssistant Professor of PediatricsDuke University Medical CenterDurham, NC
Bruce G. Bateman, MDDepartment of Obstetrics & GynecologyUniversity of VirginiaCharlottesville, VA
David D. Berry, MDWake Forest University School of MedicineWinston-Salem, NC
D. Spencer Brudno, MDAssociate Professor of PediatricsMedical Director, Pediatric TherapyMedical College of GeorgiaAugusta, GA
Curtis D. Caldwell, NNPUNM School of MedicineDepartment of PediatricsAlbuquerque, NM
Ed Coombs, MA, RRTSr. Marketing Manager – VentilationDraeger Medical, Telford, PA
Jonathan H. Cronin, M.D.Assistant Professor of Pediatrics, Harvard Medical SchoolChief, Neonatology and Newborn Medicine UnitDepartment of PediatricsMassachusetts General Hospital for ChildrenBoston, MA
Michael P. Czervinske, RRTNeonatal and Pediatric Critical CareUniversity of Kansas Medical CenterKansas City, KS
Professor Adekunle H. DawoduChairman of PediatricsFaculty of Medicine and Health SciencesUnited Arab Emirates UniversityAl Anin, UAE
Jayant Deodhar, MDAssociate Professor of Clinical PediatricsChildren’s Hospital CenterCincinnati, OH
Leonard Eisenfeld, MDAssociate Professor of PediatricsUniversity of Connecticut School of MedicineDivision of NeonatologyConnecticut Children’s Medical CenterHartford, CT
Sami Elhassani, MDNeonatologistSpartanburg, SC
Ivan Frantz, III, MDProfessor of PediatricsChief, Division of Newborn MedicineTufts University School of MedicineBoston, MA
Philippe S. Friedlich, MDAssistant Professor of PediatricsKeck School of MedicineUniversity of Southern CaliforniaLos Angeles, CA
G. Paolo Gancia, MDNeonatologist, Terapia IntensivaNeonatale-NeonatologiaCuneo, Italy
George A. Gregory, MDProfessor of Pediatrics and AnesthesiaUniversity of CaliforniaSan Francisco, CA
William R. Halliburton, RRT, RCPNeonatal Respiratory Care CoordinatorDepartment of Respiratory CareHillcrest Baptist Medical CenterWaco, TX
Mary Catherine Harris, MDAssociate Professor of PediatricsDivision of NeonatologyUniversity of Pennsylvania School of MedicineThe Children’s Hospital of MedicinePhiladelphia, PA
David J. Hoffman, MDClinical Associate Professor of PediatricsPenn State College of MedicineStaff NeonatologistThe Reading Hospital and Medical CenterWest Reading, PA
Michael R. Jackson, RRTNewborn Intensive Care UnitBeth Israel HospitalBoston, MA
Chang-Ryul Kim, MDAssociate Professor of PediatricsCollege of MedicineHanyang University Kuri HospitalSeoul, South Korea
David M. Kissin BS, RRTPerinatal/Pediatric SpecialistMaine Medical Center, Portiand, ME
Sheldon Korones, MDDirector of Newborn CenterCollege of MedicineMemphis, TN
Scott E. Leonard, MBA, BA, RRTChief Administrative DirectorDepartment of Respiratory Care ServicesUMass Memorial Medical CenterWorcester, MA
Raymond Malloy, BS, RRTDirector of Pulmonary CareThomas Jefferson University HospitalPhiladelphia, PA
Paul J. Mathews, PhD, RRT, FCCM, FCCP, FAARCAssociate Professor of Respiratory CareUniversity of Kansas Medical CenterKansas City, KS
William Meadow, MDAssociate ProfessorDepartment of PediatricsThe University of ChicagoChicago, IL
David G. Oelberg, MDCenter for Pediatric ResearchEastern Virginia Medical SchoolChildren’s Hospital of The King’s DaughtersNorfolk, VA
Rahmi Ors, MDChief, Division of NeonatologyAtaturk School of MedicineErzurum, Turkey
T. Michael O’Shea, MD, MPHChief, Neonatology DivisionWake Forest University School of MedicineWinston-Salem, NC
G. Battisita Parigi, MDAssociate Professor of Pediatric SurgeryUniversity of Pavia, Italy
Richard Paul, MDChief, Maternal & Fetal MedicineDepartment of Obstetrics & GynecologyUniversity of Southern CaliforniaLos Angeles, CA
Max Perlman, MDProfessor of PediatricsThe Hospital for Sick ChildrenToronto, Ontario, Canada
Boris Petrikovsky, MDProfessor of Obstetrics and GynecologyNassau Health Care CorporationEast Meadow, NY
Arun Pramanik, MDProfessor of PediatricsSection of NeonatologyLouisiana State UniversityHealth Sciences Center, Shreveport, LA
Benamanahalli K. Rajegowda, MDChief of NeonatologyLincoln Medical and Mental Health CenterProfessor of Clinical PediatricsWeill Medical College of Cornell University, NY
Koravangattu Sankaran, FRCP(C), FAAP, FCCMProfessor of Pediatrics and Director of Neonatology and Neonatal ResearchDepartment of PediatricsRoyal University HospitalUniversity of SaskatchewanSaskatoon, Saskatchewan, Canada
Istvan Seri, MD, PhDProfessor of PediatricsHead, USC Division of Neonatal MedicineUniversity of Southern California, Los Angeles, CA
Tushar A. Shah, MD, MPHDivision of NeonatologyCincinnati Children’s Hospital Medical CenterCincinnati, OH
Dave Swift, RRTOttawa Hospital – Civic SiteCampus Coordinator (Professional Practice) & Special Care Nursery Charge TherapistRespiratory Therapy Team LeadNational Office of the Health Care Emergency Response Team (NOHERT)Subject Matter ExpertHealth Canada
Otwell D. Timmons, MDAssistant Professor of PediatricsUniversity of Utah Medical CenterSalt Lake City, UT
Maya Vazirani, MD, FAAPBoard Certified Neonatology and Pediatrics, Lancaster, CA
Max Vento, MDAssociate Professor of PediatricsChief, Pediatric ServicesNeonatologia Hospital Virgin del ConsueloValencia, Spain
Dharmapuri Vidyasagar, MDProfessor of Pediatrics Department of PediatricsUniversity of IllinoisChicago, IL
Editorial Advisory Board
ISSN1062-2454Publishedseventimeseachyearby
Goldstein and Associates, Inc.10940WilshireBlvd.,Suite600LosAngelesCA90024Phone:310-443-4109Fax:310-443-4110E-mail:[email protected]:www.nicmag.ca
PublisherSteveGoldstein
EditorLesPlesko
Senior EditorLaszloSandor
Associate EditorJordanaHammeke
Design, Typography, Prepress and Production Managementhttp://accugraphics.net
Circulation, Coverage, Advertising Rates: Completedetailsregardingcirculation,coverage,advertisingrates,spacesizes,andsimilarinfor-mationareavailabletoprospectiveadvertisers.Closingdateis45daysprecedingdateofissue.
Change of Address noticesshouldbesentpromptlytoCirculationDepartment:provideoldmailinglabelaswellasnewaddress:includezipcodeorpostalcode.Allowtwomonthsforchange.
Editorial Contributions maybesentbye-mailandwillbehandledwithreasonablecare:however,publishersassumenoresponsibilityforsafetyofartwork,photographs,ormanuscripts.Everyprecautionistakentoensureaccuracy,butthepublisherscannotacceptresponsibilityforthecorrectnessoraccuracyofinformationsuppliedhereinorforanyopinionexpressed.Editorialclosingdateisthefirstdayofthemonthprecedingmonthofissue.
©2012byGoldstein&Associates,Inc.Allrightsreserved.Reproductioninwholeorinpartwithoutwrittenpermissionisstrictlyprohibited.

neonatal INTENSIVE CARE Supplement 2012 3
IntroductionThe late preterm population, from 34 0/7 to 36 6/7 weeks gestation, represents 8.8% of all births. Compared to babies born at term, late preterm infants are at increased risk of postbirth morbidities and mortality. According to the March of Dimes Perinatal Center, “babies born just a few weeks too soon are six times more likely to die in their first week of life than their term counterparts and three times more likely to die before their first birthday.”1
There is also a subcategory of term births called “early term,” from 37 0/7 to 38 6/7 weeks of gestation. Evidence indicates that these infants also have increased risks of neonatal morbidity and mortality when compared with those born later at term.2
During the last six weeks of pregnancy, fetal organ systems are continuing to mature to prepare the baby for extrauterine life. Late preterm (LPT) infants have to grow and mature outside the uterus in a less-than ideal environment. These babies are born with developmental and physiologic immaturities which predispose them to: • increased risk of feeding difficulties, • infection, • temperature instability, • hypoglycemia, • jaundice, and • respiratory distress.
Breastfeeding is indisputably the recommended feeding for infants. While the latest CDC data indicate that the US has met the 2010 Healthy People Goal of 75% breastfeeding initiation,3 data also show that a high percentage of mothers who initiate breastfeeding are frequently unable to continue for more than a few days or weeks. In particular, LPT infants and their mothers are vulnerable to breastfeeding problems and other morbidities related to decreased milk production and low milk intake, yet it is these same infants who need the unique protective properties of human milk and can especially benefit from the interaction of breastfeeding itself.
Healthcare providers of LPT infants must be proactive in their assessments and have specialized knowledge and skills to manage early breastfeeding and prevent lactation-associated morbidities. Strategies should be used which minimize the risk of inadequate intake by the infant and maximize the volume of the mother’s milk supply.
Importance of Human Milk for the Late Preterm Infant Human milk is not only the best nutrition for human infants, it provides well-documented protection from a wide range of infectious diseases and is optimal for brain and central nervous system development.4
Colostrum, the early milk present in the breasts during late pregnancy and the first few days after birth, is a vital food for the newly born human infant. Colonization of the infant’s GI tract begins during the birth process and early feedings of colostrum, loaded with pre and probiotics, provide the environment in which commensal bacteria thrive.
Vulnerability of LPT Infants to Breastfeeding DifficultiesMothers who deliver late preterm infants may be at risk for delayed onset of lactation. These mothers are likely to have underlying health problems or pregnancy complications which may cause this delay. Any one or a combination of the following conditions may result in a delay of lactogenesis II (the change from colostrum to copious milk production): • maternal stress during labor and delivery, • diabetes mellitus, • pregnancy-induced hypertension, • prolonged rupture of membranes, • Chorioamnionitis, • obesity, and • delivery by cesarean-section.5,6
Late preterm infants, despite their vulnerability to complications after birth, are often initially cared for in the general maternity population using feeding guidelines for healthy, full-term infants. This can be a problem. Even though a 34-to 37-weeker may look
Improving In-Hospital Breastfeeding Management for the Late Preterm InfantMaria Lennon, RN, MSN, CNM, IBCLC
Maria Lennon is a Clinical Education Specialist employed by Medela,
Inc. She began her extensive nursing career in North Carolina working
in hospital, public health, university education and private practice
settings and has been working with mothers and babies in establishing
normal lactation, problem management, and special situations for over
30 years. She is a Certified Nurse-Midwife and has been continuously
Board-Certified as a Lactation Consultant since the first exam was given in
1985. Lennon established one of the first in-hospital lactation centers in
North Carolina and developed a 5-day Breastfeeding Educator Program
for health care professionals. She worked with the North Carolina State
WIC Office developing breastfeeding programs, educational materials,
and community coalitions to improve breastfeeding services all across
the state. In addition, she spent several years coordinating Perinatal
Outreach Education for the East Carolina University School of Medicine
and has received recognition for her contribution to Nursing Leadership
and Service. Previous to 2000, she was director of a faculty-based nurse-
midwifery program associated with New Hanover Hospital and the
University of North Carolina Department of OB-GYN. For many years she
volunteered her services as a La Leche League Leader, served for two years
on the editorial staff of the Journal of Human Lactation and is a member of
the American College of Nurse-Midwives, AWHONN and Sigma Theta Tau.
This article was provided by Medela.
4 neonatal INTENSIVE CARE Supplement 2012
robust and healthy at birth, their looks can be deceiving. Many of their physiologic systems are immature and the baby may have little reserve to maintain cardio-respiratory and metabolic stability.
Late preterm infants are at risk for feeding problems, especially when breastfeeding. Studies indicate that adequate vacuum pressures are important for the baby to get enough milk.7 The coordination of sucking, swallowing and breathing is gestationally related and is a critical skill necessary for latching on to the breast, maintaining vacuum and transferring adequate volumes of milk.8
The brain weight of a 35-weeker is only 60% of that of a term infant; over the next five weeks, cortical volume increases along with maturation of the brain stem, neuronal and synaptic functions. Due to central nervous system immaturity late preterm infants: • have immature state regulation, • sleep more, • have diminished muscle tone, and • exhibit immature sucking patterns, and are therefore often unable to consume an adequate volume of milk when fed exclusively at breast.
In the first few days of lactation, milk volumes are limited9 and only small amounts of colostrum are available to the suckling infant. Because of their various immaturities, LPT infants may not be able to extract the milk that is in the breasts and their energy needs may far outweigh their intake.10,11
After lactogenesis II, effective infant suckling and the removal of the available milk from the breasts are critical to establishing adequate milk volumes of approximately 500-700 mLs per 24 hours.11 Recent research shows that milk production at six days post-birth is related to milk production at 6 weeks postpartum.12 Thus early and frequent removal of colostrum and breastmilk in the first few days after birth is an important step in laying the foundation for a plentiful long term milk supply. Supportive clinical practices in the first few days post-partum are critical to help mothers in initiating and producing milk volumes that will be adequate for their infant’s growth and development.
Strategies/Technology to Improve Breastfeeding OutcomesClose attention and vigilant assessment are necessary to anticipate and prevent complications. For the late preterm infant, the priorities in breastfeeding management are to ensure adequate nutritional intake and maximize maternal milk volume. A set of feeding orders or a clearly defined plan of care specifically for the LPT infants will help ensure careful monitoring.
Immediate post-birth period: Skin to Skin Contact is EssentialContinuous skin-to-skin contact is comforting, decreases stress levels for both the baby and mother and allows for early breastfeeding. Any interventions should be delayed until after the first feeding. Separating the baby from the mother causes increased crying, increased heart and respiratory rate and the release of stress hormones, all of which can deplete energy reserves and lead to hypoglycemia.
The infant should be placed prone, directly skin-to-skin on the mother’s abdomen/chest and gently dried. Both baby and mother are covered with a warm blanket and a cap placed on the baby’s head to conserve heat. The mother is an optimal source of heat
and, except under unusual circumstances, the infant should remain with the mother throughout the recovery period.4 The evidence is clear that skin to skin contact improves thermal response and increases blood glucose and cardio-respiratory stability, and a Cochrane Database Review in 2007 reported that “babies were more likely to breastfeed and to breastfeed longer, if they had early skin-to-skin contact.”13
The First FeedingBreastfeeding should be an essential component of delivery room care. Every opportunity should be made for the infant to breastfeed in the first hour after birth as this is an important part of the infant’s transition to life outside the womb. The first breastfeeding of colostrum provides calories, begins the colonization of the infant’s intestine with lactobacilli, has a laxative effect and increases meconium clearance.
Within the first hour or two after birth if the LPT infant does not latch, the mother should be shown how to express colostrum which should be stored for later feeding to the infant, if needed. If the mother and infant will be separated for any length of time (ie for NICU observation or care, etc), she should initiate breastpumping as soon as possible and within 6 hours after birth.
In-Hospital Breastfeeding ManagementFamily-centered couplet care provides optimal opportunities to breastfeed and allows for close assessment by the bedside nurse. A lactation consult within the first 24 hours and daily thereafter, is ideal. A feeding plan which takes into account the LPT infant’s unique vulnerabilities should be developed and communicated to the family and all the staff. Breastfeeding should be observed at least every shift and an assessment made of the effectiveness of milk transfer. Mothers should be educated on the unique needs of their babies and on the use of supportive positions while breastfeeding which help the baby feed more effectively. Extended skin-to skin contact is recommended as again, it helps to maintain temperature, cardio-respiratory and metabolic stability and allows for frequent opportunities to breastfeed. Mothers should be instructed to watch for early feeding cues and to breastfeed their LPT infants every 2-3 hours or at least 8 times in 24 hours.14 Some LPTs are able to effectively suckle at the breast for 15-20 minutes 8 to 10 times in a 24-hour period, but many are not.11
Many late preterm babies tire easily and, if after several attempts (10 to 15 minutes maximum) the baby does not latch, the baby should be fed the colostrum previously expressed and stored. Mothers should be pumping their breasts after feeding attempts or approximately every 3 hours, using an evidence-based double electric breastpump, to stimulate the breasts and remove the available milk until their late preterm infants are able to feed appropriately. If the baby exhibits signs of inadequate intake,

neonatal INTENSIVE CARE Supplement 2012 5
ie excessive weight loss, poor feeding, significant jaundice, some supplemental feedings may be required. Hubbard, et al recommends the following (breastmilk) volumes every 2 to 3 hours: 5 to 10 mL on the first day of life, 10 to 20 mL on day 2 and 20 to 30 mL on day three.10
Lactation Technology to Improve Breastfeeding Outcomes If the LPT infant has difficulty feeding at the breast, there are several tools designed to assist both mother and baby in obtaining an adequate milk supply.
Hospital Grade Electric Breastpump Helps Mother Maintain Her Milk SupplyUse of a double electric breastpump based on current evidence will help mothers stimulate their breasts, initiate, express and maintain an adequate milk supply to feed their baby.
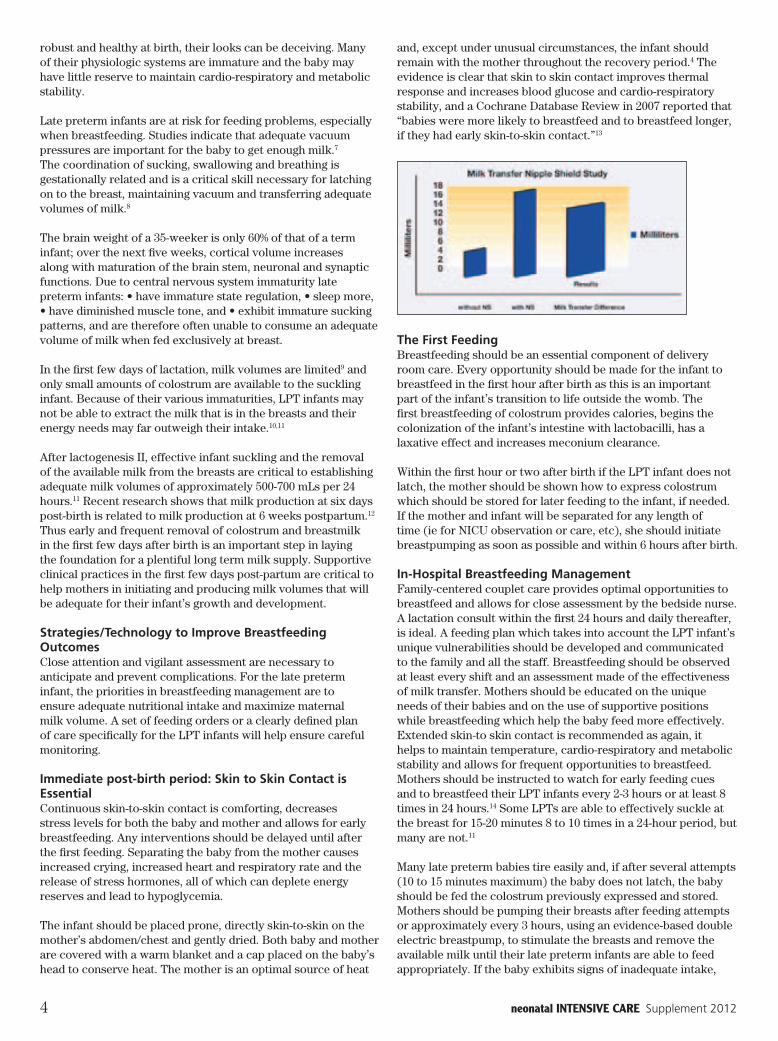
Nipple Shields Help Baby SuckA nipple shield helps the baby compensate for a weak suck and may increase intake at the breast in those babies that are having trouble feeding. A weak suck causes inadequate vacuum pressures to remove milk. Research with preterm infants has shown that some babies are able to breastfeed more effectively and efficiently with the use of an ultrathin silicone nipple shield.15
Test Weight Scale Helps Reassure that Baby is Getting Enough MilkThe use of test weights with an electronic scale that is accurate to within 1-2 grams offers a valid measurement of intake after a breastfeeding. Babies need to be weighed under the exact same conditions (same clothing, diaper, leads, etc) before and after breastfeeding. The weight increase in grams is commensurate with the baby’s intake in milliliters. This information is helpful to the provider in determining adequacy of at-breast feedings and in determining the need for supplemental volumes of milk.
Supplemental Nursing System Helps Mother and Baby A supplemental nursing system allows baby to get supplemental breastmilk via a tube while breastfeeding even if the LPT infant’s suck is weak and not providing adequate vacuum. It rewards the infant for sucking efforts and helps further promote at-breast feedings and the mother/baby bond.
Discharge PlanningIn planning for hospital discharge, the priorities in breastfeeding the late preterm infant at home remain the same—to ensure adequate nutrition for the baby and maximize the mother’s milk supply.
Patient and family education is critical to breastfeeding success. They need to understand that their baby is immature and has special feeding needs which may take a few weeks to resolve—often until 40-42 weeks corrected gestational age.9
The feeding plan (see list of recommended components) should be communicated both verbally and in writing to the family. A hospital-grade electric breastpump can be rented for home use and should be used until the baby is gaining weight adequately and milk volume is well-established.
The late preterm infant will continue to need close monitoring and follow-up after hospital discharge for the development of (or worsening) jaundice, weight gain issues, and breastfeeding assessment. An initial outpatient office visit or in-home visit should occur within 24 to 48 hours and then every two to four days if needed.10
Education is CriticalIn their list of Best Practices, the California Perinatal Quality Care Collaborative says, “Healthcare providers caring for late preterm infants should have the knowledge, skills and attitude to support adequate nutrition and maintain optimal communication with parents and each other. Intrapartum, postpartum and special care policies and practices should support nutrition (including breastfeeding) in a coordinated, consistent manner.”16
The evidence is clear that increased duration of breastfeeding provides innumerable health benefits to both mothers and babies that can last a lifetime.2,4 It is essential for a mother and her family to be educated on the importance of breastmilk and how it provides not only optimal nutrition for her late preterm infant but also helps protect from disease and improved developmental outcomes. Teaching families about the possible challenges they may encounter and giving them resources on how to overcome them has been shown to help increase the success and duration of breastfeeding in the special late preterm population. For more information on how to get comprehensive education for your staff and for your patients go to www.LatePretermEducation.com.
References1 http://www.marchofdimes.com/prematurity/index_
professionals_1157.asp#head82 Engle, WA, Kominiarek, MA. Late preterm infants, early
term infants and timing of elective deliveries. Clinics in Perinatology. 2008 Jun;35(2):325-41.
3 Centers for Disease Control and Prevention Breastfeeding Report Card–United States, 2010. Accessed from www.cdc.gov/breastfeeding/data/reportcard2.htm 10-14-2010.
4 American Academy of Pediatrics, Section on Breastfeeding. Breastfeeding and the use of human milk. Pediatrics. 115(2) February 2005, pp 496-506.
5 Hurst NM. Recognizing and treating delayed or failed lactogenesis II. Journal of midwifery and women’s health. 2007; 52(6):588-594.
6 Hartmann PE & Cregan M. Lactogenesis and the effects of insulin-dependent diabetes mellitus and prematurity. Journal of Nutrition 2001;131(11):3016-3020S.
7 Geddes DR et al. Geddes, D.T., Kent, J.C., Mitoulas, L.R. and Hartmann, P.E. Tongue movement and intra-oral vacuum in breastfeeding infants. Early Human Development 2008 (84): 471-477.
8 Lau C et al. Coordination of suck-swallow and swallow respirations in preterm infants. Acta Pediatrica 2003; 92:721-727.
9 Santoro, et al. Colostrum ingested during the first day of life by exclusively breastfed healthy newborn infants. Journal of Pediatrics 2010;Jan 156(1) 29-32.
Feeding Plan Considerations• protect the milk supply• pumping plan • use of nipple shield • in-home weight checks • signs of feeding readiness and successful milk transfer • determine need for supplementary feedings

6 neonatal INTENSIVE CARE Supplement 2012
10 Hubbard, Stellwagen, et al. The late preterm infant: A little baby with big needs. Contemporary Pediatrics 2007.
11 Meier PP, Furman LM & Degenhardt M. Increased lactation risk for late preterm infants and mothers: Evidence and management strategies to protect breastfeeding. Journal of Midwifery and Women’s Health 2007; 52:579-887.
12 Hill PD, Aldag JC. Milk volume on day 4 and outcome predictive of lactation adequacy at 6 weeks of mothers on non-nursing preterm infants. Journal of Perinatal and Neonatal Nursing. 2005;19:273-282.
13 Moore ER, Anderson GC & Bergman N. Early skin-to-skin contact for mothers and their healthy newborn infants. Cochrane Database of Systematic Reviews. 2007, Issue 3, Article number: CD003519. DOI:10. 1002/14651858. CD003519.pub2.
14 The Academy of Breastfeeding Medicine.Clinical Protocol #10: Breastfeeding the near-term infant (35-37 weeks gestation) 2004. www.bfmed.org. Accessed 10/12/2010.
15 Meier PP, Brown LP, Hurst NM, et al. Nipple shields for preterm infants: Effect on milk transfer and duration of breastfeeding. Journal of Human Lactation 2000;16:106–114.
16 California Perinatal Quality Care Collaborative Toolkit:Late preterm infant toolkit. 2007. www.cpqcc.org accessed 10/12/2010.

neonatal INTENSIVE CARE Supplement 2012 7
IntroductionBreastfeeding is the gold standard for feeding and nourishing the human infant. But when infants are unable to feed at breast – as in the case of hospitalized preterm or compromised infants – mother’s milk feedings via enteral feeding systems, bottles or special feeding devices are undeniably the next best option.
The science of human milk feeding in the neonatal intensive care unit is constantly evolving. While the majority of research related to NICU breastmilk feedings has focused on storage of human milk, enteral feeding processes and fortification of human milk, surprisingly little research has explored the clinical process of milk preparation for feeds. For example, according to the Human Milk Banking Association of North America (HMBANA),1 there are no studies on the optimal method of some of these basic processes such as thawing human milk for feedings. The 2006 HMBANA Guidelines for Best Practice for Expressing, Storing and Handling Human Milk in Hospitals, Homes and Child Care Settings are based on research evidence, are inferred from Food Safety Guidelines or, in the absence of scientific evidence, are based on reasoned opinions of experts. Gaps in the literature, particularly related to handling human milk in the NICU setting, should be re-examined in the light of new evidence and current technology. This article will summarize the science of human milk feedings in the hospital setting and propose a new standard of care with a waterless milk warmer. Key points are emphasized, including:• delivering the maximum benefit of human milk to the
hospitalized infant by safely thawing and warming milk.• eliminating the possibility of water bath associated nosocomial
infections.• standardizing the temperature of infant feedings to the most
physiologic temperature range (body temperature).• reducing process variation and guesswork commonly
associated with feeding preparation. • maximizing clinical time at the bedside.
Benefits of Human MilkIn addition to species-specific macronutrients, human milk contains multiple immunologic factors such as secretory IgA (sIgA), lactoferrin, lysozyme, leukocytes and the bifidus factor that protect the fragile newborn from bacterial, viral and fungal
infections.2-4 Human milk – rich in antioxidants, prostaglandins, cytokines, epidermal growth factors, sIgA and lysozyme – is also capable of suppressing potentially devastating inflammatory processes in the preterm or sick infant. Inflammation originating in the infant’s intestinal tract can predispose the infant to both feeding intolerance and the potentially devastating disease, necrotizing enterocolitis (NEC).5 Inflammation can damage other organ systems of the preterm infant, increasing the risk of chronic lung disease, retinopathy of prematurity and adverse neuro-developmental outcomes.6 Preterm infants fed mothers’ own milk are shown to have decreased risks of both feeding intolerance and NEC when compared to preterm infants fed infant formula.7-11
The benefits of human milk accumulate in a dose response manner: the greater the overall quantity of milk an infant receives, the greater the benefit to the infant. The concept of dose response is relevant not only to the percentage of human milk feeds, but also to the duration of human milk feeds over days, weeks and months. Thus the longer an infant receives mother’s milk, the greater the overall benefit. Specifically, studies suggest that the more mother’s milk a preterm infant receives during the NICU stay, the lower the infant’s risks are of NEC, late onset sepsis and enteral feeding intolerance.9,12 In extremely low birth weight infants, intakes of higher amounts of human milk during the NICU stay result in lower risks of rehospitalization after discharge as well as higher Bayley mental developmental index scores and Bayley behavioral score percentiles for up to 30 months’ corrected age.13,14
At body temperature, 37°C (98°F), fresh human milk is an intricate living bioactive fluid with all essential properties – including macronutrients, anti-infective and anti-inflammatory components – intact. While fresh human milk is ideal for infant feeds it is not always available for hospitalized infants. Therefore, optimal handling and storage are critical in the NICU setting.
Temperature Effects of Human MilkHuman milk is sensitive to the effects of temperature changes.15-18 In the NICU, the separation of mothers and infants dictates milk storage in refrigerators or freezers; however, the process of freezing human milk inactivates some of its anti-infective properties.1 Preparation of human milk for feedings involves additional processes – thawing, fortification and heating – that can also alter human milk composition.15,19-22 As previously mentioned, research on the actual processes of preparing human
Best Practices for Warming Human Milk in a Hospital SettingJean Rhodes, PhD, CNM, IBCLC
Jean Rhodes is an independent consultant for Medela. She has 30 years
of experience as a nurse, lactation consultant, nurse-midwife, educator
and researcher. Rhodes was formerly with the Medical University of South
Carolina. This article was provided by Medela.

8 neonatal INTENSIVE CARE Supplement 2012
milk for feedings is incomplete. While there are no studies of the best process for thawing frozen human milk, there are studies of the impact of heat on human milk. Studies on pasteurized milk (heated to 62°C/144ºF for 30 minutes) demonstrate measurable heat related changes: immunologic and anti-inflammatory components such as SIgA, lactoferrin, and lysozyme are decreased and beneficial probiotic bacteria and white blood cells are destroyed.4,23
Temperature can affect not only the beneficial components of human milk but also the preterm infant’s ability to tolerate feeds. A study by Gonzalez and associates24 demonstrates this sensitivity of very low birth weight preterm infants to feeding temperatures. In this study, infants were fed milk prepared at 3 different temperatures: cool temperature (10°C/50°F), room temperature (24°C/75°F) and body temperature (37°C/98.6°F). The authors found that preterm infants fed milk at body temperature had the least amount of gastric residuals and greater feeding tolerances. Conversely, infants fed milk at cool temperatures had the highest milk residuals and the greatest incidence of feeding intolerance. The authors concluded that warming milk to body temperature might promote greater feeding tolerance in very low birth weight (VLBW) preterm infants.
Current Practice StandardsThe 2006 HMBANA Guidelines for Best Practice for Expressing, Storing and Handling Human Milk in Hospitals, Homes and Child Care Settings recommends specific processes with rationale for the safe handling of human milk. Guidelines for thawing frozen milk include: • Thawing milk quickly in a container of warm water not to
exceed 37°C/98°F • Avoiding milk contamination from water getting on or under
the container lid• Refrigerating milk before it is completely thawed and while ice
crystals are still present.
HMBANA guidelines for warming human milk for feeding include:• Warming individual feedings in a container of warm water or
under running warm water• Protecting the container from contamination in the water• Noting that communal warming systems may not have clean
water.1
HMBANA guidelines are often recognized as the standard of practice recommended by professional organizations and practitioners. However, in NICU settings, human milk is thawed and warmed through a variety of methods not always in compliance with HMBANA recommendations. Human milk is often heated in cups of warm-to-hot tap water, in containers of water from instant heat faucets or in water-based feeding warmers. Water from instant heat faucets can reach 87°C (189°F), well above the HMBANA recommendation and at a point of potentially de-activating anti-infection properties in human milk.
Thawing and warming of milk with water involves a complex interplay of several factors including the milk volume, milk temperature at the beginning of the warming process, size of the milk container and the water temperature. Determining the exact point of thaw to include the presence of small amounts of ice crystals requires constant oversight of the warming
process. Determining when milk is at a desired temperature is inexact, often subjective and can be time consuming. Therefore, oversight of the thawing and warming of human milk can reduce nursing time for clinical care in the NICU.
Contamination of Hospital Tap WaterFor 40 years, hospital tap water has been identified as a potential source of nosocomial infections from bacteria and other contaminants including Cryptosporidium parvum, Legionelle spp, E Coli and Pseudomonas aeruginosa.25-29 Patients at high risk of infection due to waterborne pathogens include AIDS patients, organ transplant recipients, oncology patients and neonates.30 Healthcare-associated infections from water supplies have been identified in hospital nurseries. As recently as 2009, 23 strains of Pseudomonas aeruginosa were found in the water supply of a children’s hospital in the US.31 In another report Buyukyavuz, et al,26 identified Staphylococcus and Klebsiella pneumoniae in hospital tap water used to heat infant milk. These bacteria were determined to be directly responsible for an outbreak of septicemia in the hospital’s neonatal intensive care unit.
Squier28 and Angelbeck30 have explained the process of microbial contamination of hospital tap water. A slime layer or biofilm containing microorganisms adheres to the lumen of pipes and fixtures in municipal and hospital plumbing systems and in hospital water tanks. Patient exposure to waterborne microorganisms can occur through any exposure to tap water including bathing, drinking, contact with medical equipment wet with water or health care provider hands rinsed in water. When tap water is used to warm infant feedings, there is potential for contamination of not only the container and the milk but also the nurse’s hands. Squier recommends using dry-warming devices to heat fluids that come in contact with patients. In concurrence, the CDC in their 2003 Guideline for Infection Control in Health-Care Facilities,32 suggested facilities remove sources of contaminated water whenever possible. These guidelines clearly recognize that moist environments and water-based solutions can serve as reservoirs for waterborne microorganisms in hospital settings.
The Medela Waterless Milk WarmerThe Medela Waterless Milk Warmer eliminates the possibility of contamination caused by tap water by using forced dry convection heat instead of water to thaw and/or warm milk. The Waterless Milk Warmer uses a fan that circulates air over heated coils found in the lid of the device. The heating profile is controlled by a software program and maintained with safe operating limits through a series of thermal sensors and safety shutoffs, eliminating the guesswork involved in heating human milk to an optimal range. The Waterless Milk Warmer safely thaws frozen milk to 4°C in less than 30 minutes. (Temperatures may vary depending on the container used.) Thawed milk will contain small amounts of ice crystals, per HMBANA guidelines, indicating the milk has not been over-heated. The Waterless Milk Warmer also warms milk quickly and efficiently to body temperature range of 30 to 38ºC (86 to100ºF). At the end of its operating cycle, the milk warmer alerts staff by a visual indicator and a low volume alarm but will continue to keep milk temperature stable for 30 minutes.
The Waterless Milk Warmer is easy to keep clean because of the use of disposable liners. Liners fit in the compartment that holds the milk container or syringe. Each liner is assigned

neonatal INTENSIVE CARE Supplement 2012 9
to a particular patient and can be labeled with the patient’s information, date and time.
The Waterless Milk Warmer can be used with a variety of containers. As previously noted, the benefits of human milk are proportional to the amount an infant receives over time. In the early days of expression, mothers may produce very small quantities of colostrum or milk. During this time, preterm infants may receive very small trophic feeds to stimulate gut maturation, foster gut motility and support the infant’s immune system. The Waterless Milk Warmer accommodates these small amounts of milk in syringes ranging from 1-60 mL. As feeding volumes increase, the warmer will handle containers or bottles from various manufacturers up to 250 mL.
In summary, human milk feedings in the hospital setting involve a complex matrix of issues related to the intricate nature of human milk and the potential hazards of milk storage and preparation. Through the use of innovative technology, and with effective clinical implementation, the Medela Waterless Milk Warmer may help maintain the optimal integrity of human milk feeds for hospitalized infants.
References1 Jones F, Tully MR. Best practice for expressing, storing and
handling human milk in hospitals, homes and child care settings. Raleigh, NC: HumanMilk Banking Association of North America, Inc.; 2006.
2 Hale TW, Hartmann P. Textbook of human lactation. Amarillo, Texas: Hale Publishing, L.P.; 2007.
3 Riordan J, Wambach K. Breastfeeding and human lactation. Boston: Jone and Bartlett; 2010.
4 Lawrence RA, Lawrence RM. Breastfeeding: A guide for the medical profession. 6th ed. Philadelphia: Elsevier Mosby; 2005.
5 Claud EC, Walker WA. Hypothesis: inappropriate colonization of the premature intestine can cause neonatal necrotizing enterocolitis. FASEB J 2001;15:1398-403.
6 Schanler RJ. The use of human milk for premature infants. Pediatr Clin North Am 2001;48:207-19.
7 Lucas A, Cole TJ. Breast milk and neonatal necrotising enterocolitis. Lancet 1990;336:1519-23.
8 Schanler RJ, Shulman RJ, Lau C. Feeding strategies for premature infants: beneficial outcomes of feeding fortified human milk versus preterm formula. Pediatrics 1999;103:1150-7.
9 Meinzen-Derr J, Poindexter B, Wrage L, Morrow AL, Stoll B, Donovan EF. Role of human milk in extremely low birth weight infants’ risk of necrotizing enterocolitis or death. J Perinatol 2009;29:57-62.
10 Taylor SN, Basile LA, Ebeling M, Wagner CL. Intestinal permeability in preterm infants by feeding type: mother’s milk versus formula. Breastfeed Med 2009;4:11-5.
11 Sisk PM, Lovelady CA, Dillard RG, Gruber KJ, O’Shea TM. Early human milk feeding is associated with a lower risk of necrotizing enterocolitis in very low birth weight infants. J Perinatol 2007;27:428-33.
12 Bisquera JA, Cooper TR, Berseth CL. Impact of necrotizing enterocolitis on length of stay and hospital charges in very low birth weight infants. Pediatrics 2002;109:423-8.
13 Vohr BR, Poindexter BB, Dusick AM, et al. Persistent beneficial effects of breast milk ingested in the neonatal intensive care unit on outcomes of extremely low birth weight infants at 30 months of age. Pediatrics 2007;120:e953-9.
14 Vohr BR, Poindexter BB, Dusick AM, et al. Beneficial effects of breast milk in the neonatal intensive care unit on the developmental outcome of extremely low birth weight infants at 18 months of age. Pediatrics 2006;118:e115-23.
15 Igumbor EO, Mukura RD, Makandiramba B, Chihota V. Storage of breast milk: effect of temperature and storage duration on microbial growth. Cent Afr J Med 2000;46:247-51.
16 Silvestre D, Lopez MC, March L, Plaza A, Martinez-Costa C. Bactericidal activity of human milk: stability during storage. Br J Biomed Sci 2006;63:59-62.
17 Ankrah NA, Appiah-Opong R, Dzokoto C. Human breastmilk storage and the glutathione content. J Trop Pediatr 2000;46:111-3.
18 Lawrence RA. Milk banking: the influence of storage procedures and subsequent processing on immunologic components of human milk. Adv Nutr Res 2001;10:389-404.
19 Chan GM, Lee ML, Rechtman DJ. Effects of a human milk-derived human milk fortifier on the antibacterial actions of human milk. Breastfeed Med 2007;2:205-8.
20 Chan GM. Effects of powdered human milk fortifiers on the antibacterial actions of human milk. J Perinatol 2003;23:620-3.
21 Lessaris KJ, Forsythe DW, Wagner CL. Effect of human milk fortifier on the immunodetection and molecular mass profile of transforming growth factor-alpha. Biol Neonate 2000;77:156-61.
22 Quan R, Yang C, Rubinstein S, Lewiston NJ, Stevenson DK, Kerner JA, Jr. The effect of nutritional additives on anti-infective factors in human milk. Clin Pediatr (Phila) 1994;33:325-8.
23 Czank C, Prime DK, Hartmann B, Simmer K, Hartmann PE. Retention of the immunological proteins of pasteurized human milk in relation to pasteurizer design and practice. Pediatr Res 2009;66:374-9.
24 Gonzales I, Duryea EJ, Vasquez E, Geraghty N. Effect of enteral feeding temperature on feeding tolerance in preterm infants. Neonatal Netw 1995;14:39-43.
25 Sanchez-Carrillo C, Padilla B, Marin M, et al. Contaminated feeding bottles: the source of an outbreak of Pseudomonas aeruginosa infections in a neonatal intensive care unit. Am J Infect Control 2009;37:150-4.
26 Buyukyavuz BI, Adiloglu AK, Onal S, Cubukcu SE, Cetin H. Finding the sources of septicemia at a neonatal intensive care unit: newborns and infants can be contaminated while being fed. Jpn J Infect Dis 2006;59:213-5.
27 Anaissie EJ, Penzak SR, Dignani MC. The hospital water supply as a source of nosocomial infections: a plea for action. Arch Intern Med 2002;162:1483-92.
28 Squier C, Yu VL, Stout JE. Waterborne Nosocomial Infections. Curr Infect Dis Rep 2000;2:490-6.
29 Rutala WA, Weber DJ. Water as a reservoir of nosocomial pathogens. Infect Control Hosp Epidemiol 1997;18:609-16.
30 Angelbeck JA, G.A. O, Canonica FP, Cervia JS. Hopsital water: A source of concren for infections. Managing Infection Control 2006:44-54.
31 Tasker F. Hospital’s water supply under scrutiny. Miami Herald 2009 June 12, 2009.
32 CDC. Guidelines for environmental infection control in health-care facilities. In: (HICPAC) HICPAC, ed.: MMWR; 2003:1-42.
10 neonatal INTENSIVE CARE Supplement 2012
As clinicians we know that breast milk is the preferred nutrition for human infants.1 This is especially true for premature and immuno-compromised infants in the NICU. Research indicates that mothers’ milk protects infants from prematurity-specific morbidities and their associated long-term sequelae. In fact, evidence demonstrates that the more exclusive mother’s milk the infant receives over the longest period of time the greater the protection.2,3,4,5,6
In the NICU, an infants’ prematurity often prohibits the ability to feed at the breast and requires mothers to find evidence-based methods for expressing their breast milk. Due to the overwhelming evidence of the protection breast milk provides, mothers of premature infants are encouraged to begin breast milk expression early after delivery. The use of a hospital-grade, double electric breast pump has been recommended for pump dependent NICU mothers in helping achieve adequate volumes of breast milk.7,8,9,10
Clinicians who work with pump dependent mothers should be knowledgeable about how a breast pump works and how to help mothers get the most milk during their pumping sessions. In this article, the importance of proper breast shield fit and its impact on milk supply is explored. This article will identify criteria for clinicians to use to assess proper fitting of breast shields, which is essential to successful breast pumping.
How a Breast Pump WorksThe function of a breast pump is to simulate the sucking action of a breastfeeding infant. This is accomplished by applying vacuum in rhythmic cycles to the mother’s nipple and areola through a funnel-shaped breast shield. The breast shield is that portion of the breast pump collection kit that comes in direct contact with the mother’s breast, nipple and areola areas. As the breast pump cycles, the nipple and areola are drawn into the tunnel of the breast shield by the vacuum generated from the pump. Breast milk is expressed from the breast as a result of both the vacuum (negative pressure) from the pump and the milk ejection (positive pressure) experienced by the mother. The expressed breast milk is then collected into an attached container. Milk expression by a breast pump should be comfortable and effectively drain all available milk.
Breast Shield Fit Can Impact Mother’s Milk SupplyBreast shields should be evaluated while the mother is pumping to ensure they correctly fit the mother’s nipple and areola anatomy. Careful evaluation of how the mother’s nipple responds as it is being drawn into the breast shield tunnel is advised. Breast shields can be either too small or too big for the mother. Breast shields that are too small may result in nipple soreness and pain, skin tissue breakdown and even excoriated nipples. As a result a mother may find pumping so painful she does not wish to continue. Any breakdown in the skin surrounding the nipples and areola may predispose the mother to develop mastitis.11 Abrupt cessation of pumping may also result in mastitis. Breast shields that are too large for a mother’s anatomy may cause similar skin irritation.
An incorrect fit may also result in incomplete breast emptying. Incomplete breast emptying leads to milk stasis within the breast. If milk stasis occurs, a milk protein known as the Feedback Inhibitor of Lactation (FIL) remains in the breast as well. FIL acts locally on breast tissue resulting in the down regulation of milk volume. Over time, a mother’s milk supply may be critically affected leading to inadequate or decreased volume.12 Ultrasound research on the lactating breast by Ramsay determined that milk ducts within the breast were easily compressible.13 An ill-fitting breast shield may impede breast milk drainage by occluding the ducts also resulting in milk stasis, the presence of FIL and the eventual down regulation of a mother’s milk supply.
For many years, the importance of selecting a breast shield that would fit a mother was not known. Different breast shield sizes
Correctly Fitting Breast Shields: A Guide for CliniciansIrene Murphy Zoppi, RN, MSN, IBCLC
Irene Zoppi currently serves as a Clinical Education Specialist for
Medela, Inc. In this role, she acts as a vital resource for groups assisting
breastfeeding mothers and infants. She has been frequently interviewed
on radio and online regarding breastfeeding issues for mothers and
clinicians. Zoppi spent many years caring for new families in antenatal,
labor and delivery, postpartum and NICU settings and was involved
in direct patient care and family-based education. She has extensive
experience teaching in a variety of nursing education programs where
she consistently received the Outstanding Lecturer title awarded by
her students. She produced a video presentation on nursing students’
involvement in Community Health Nursing for the National League for
Nursing. Ms. Zoppi, an IBCLC since 2000 and former 1st Lieutenant in
the Army Nurse Corps, has authored numerous continuing educational
programs for health professionals on topics ranging from breastfeeding
support to evidence-based practices on the use of human milk. She has
been instrumental in developing hands-on education for clinical staff
regarding breastpump technology. Irene graduated from Boston University
with a master’s degree in Parent Child Health Nursing and is a member of
Sigma Theta Tau. This article was provided by Medela.

neonatal INTENSIVE CARE Supplement 2012 11
were limited and did not fit anatomical differences in nipple sizes. Just as mothers’ breasts come in many sizes, so do their nipples. Many mothers may have experienced unnecessary pain while pumping which may have led to early cessation of breastfeeding. Manufacturers of breast pumps now provide multiple sizes of breast shields that make pumping comfortable and effective.
Finding the Proper FitKnowing how to select a correct size for each pumping mother is critical to her pumping success. Visible inspection of the diameter and/or length of a mother’s nipples is inadequate in determining correct breast shield sizing. The nipple is comprised of elastic tissue that is capable of stretching and elongating. During breastfeeding, a healthy infant creates oral vacuum pressures that elongate the nipple two to three times its normal resting size.14 The vacuum generated by the breast pump will cause similar nipple stretching. Correct breast shield sizing, therefore can only be made by witnessing the mother while she pumps. To determine the correct breast shield fit, one must watch how the mother’s nipples respond to the vacuum applied by each cycle of the pump and how her nipples are drawn into the breast shield tunnel. It is also important to ask the mother for feedback on how pumping feels to her. It may be necessary to experiment with multiple breast shield sizes to find a suitable fit.
Mothers may find that their anatomy requires the use of two different sized breast shields.14 Asymmetry of paired body structures is documented within other species of animals and may result in the need for two different breast shield sizes used at the same time by the same mother.15 Even when a correct fit is determined, a mother may require additional assessments over the course of her pumping history. There may be a lot of variation in what feels and looks appropriate from one day in her lactation to another. Meier et al documented pump dependant NICU mothers’ need for different breast shield sizes over the course of their lactation.15 As a mother progresses through lactation, the need for a different breast shield size may change.
Consider the mother who has given birth by cesarean delivery after many hours of labor with epidural anesthesia. It would not be uncommon for this mother to receive copious amounts of intravenous fluid during her labor and delivery. After delivery, the intravenous fluid exits the intracellular compartment and enters the extravascular compartment (third spacing) resulting in very edematous areas of the body. This is often seen in a mother’s puffy face, swollen hands and feet, but also can exhibit as fluid collects around the nipple and areola area. This fluid shift may not be seen on the mother’s first day post-partum but on subsequent days. A correctly fitted breast shield for this mother on her first day post-partum would not necessarily fit or feel comfortable on subsequent days. She would require assessment for a larger breast shield. Resizing of her breast shields may also be necessary when her milk volume increases, commonly seen on days three to five after birth. When complete diuresis of excess fluid has occurred, the mother may find her breast shield size requires resizing once again.
The Role of Clinicians Clinicians who work with pump dependent mothers need to be cognizant of criteria used to assure a correct breast shield fit. They should demonstrate competency in making clinical assessments regarding correct breast shield fit. These assessments are necessary interventions to ensure mothers
are pumping using appropriate products and need to be a standard of care for pump dependent mothers. Clinicians can teach mothers how to make similar essential assessments while pumping their breast milk.
Fitting Criteria Ensuring breast shields are correctly fitted requires knowledge of specific fitting criteria. Fitting criteria is as follows:
1. The nipple should be centered in the breast shield and move freely in the tunnel. The nipple should not rub against the sides of the breast shield tunnel. Mothers with large breasts may not be able to visualize their nipples and may require assistance to center their nipples in the breast shield. Once the vacuum of the pump starts, the mother may need to break the suction and center her nipple in the breast shield again. She may need to do this several times to achieve a good nipple position. It is also important to reinforce with the mother to be careful not to push the shields into her breast tissue when she positions or holds the shields. Ramsay’s research demonstrated milk ducts and glandular tissue lie underneath the area where breast shields are positioned against the breast.13 Pressing the shields “too hard” can result in damage to these ducts and glandular tissue.
2. Minimal or no areola tissue should be pulled into the tunnel. When a breast shield is correctly fitted, minimal or no areola tissue will be pulled into the tunnel of the shield. Excessive areola tissue pulled into the breast shield tunnel can also lead to tissue damage.
3. There should be gentle motion of the breast each time the pump cycles. This gentle, subtle motion suggests that the breast is getting proper stimulation while pumping. The breast seems to pulsate with each suction cycle very much like what happens when a healthy, term baby breast feeds.
4. Pumping should be comfortable. If criteria are followed pumping should feel comfortable to the mother.
5. The breasts should be well drained. The breasts should feel soft after each pumping session. They should be examined after pumping to check for areas of tenderness or areas that have not fully drained. The area not fully drained may feel firm or hard suggesting the milk duct located in that part of the breast has been inadequately drained by a potentially ill-fitting breast shield.14, 18 The mother may need to pump longer or get a different size breast shield. Clinicians should explain to mothers that if they find that part of the breast is not draining, they should seek the help of a clinician or lactation consultant.
A Helpful Teaching ToolThe use of an easily remembered acronym may help to reinforce these fitting criteria with both clinicians and pump dependent mothers. The acronym “COMFY” identifies the objective fitting criteria described in this article.
C – Centered nipple which moves freely in the tunnelO – Only little or no areola tissue pulled into the tunnelM – Motion of the breast is gentle and rhythmic with each cycle
of the pumpF – Feels comfortable pumpingY – You find a well drained breast. If an area of the breast still
feels full or a bit firmer, the milk duct in that area of the breast may not be empty.

12 neonatal INTENSIVE CARE Supplement 2012
The COMFY acronym is a simple teaching tool that emphasizes criteria used to correctly fit breast shields. It is easy for both clinicians and mothers to learn and to remember. Laminated cards detailing COMFY fitting guidelines can easily be affixed to all breast pumps within the hospital setting. Clinicians can reinforce these fitting techniques whenever they are instructing mothers how to use a breast pump and mothers can easily refer to them each time they pump within the hospital setting.
ConclusionClinicians can make a tremendous difference in the pumping experience of pump dependent mothers. Clinicians working in the NICU with pump dependent mothers require information on the function and use of breast pump equipment. They need to know how the pump components work together and how to ensure mothers are using correctly sized breast shields. These clinicians should know specific breast shield sizing criteria that are straightforward and can be easily interpreted and taught to mothers. Use of the acronym, COMFY may help clinicians and mothers understand and remember the specific criteria for a correctly fitted breast shield. Knowledge of these fitting criteria need not be complex for the clinician or for the mother.
Clinicians should demonstrate competency correctly sizing breast shields with mothers who pump breast milk. Correct breast shield sizing helps to ensure mothers will be comfortable while pumping. With this important knowledge and guidance from clinicians, mothers may be protected from injury and will be sure that their breasts are adequately emptied each time they use a breast pump.
References1 American Academy of Pediatrics, Section on Breastfeeding.
Breastfeeding and the Use of Human Milk. Pediatrics 2005; 115:496–506.
2 Meinzen-Derr J, Poindexter B, Wrage L, Morrow AL, Stoll B, Donovan EF. Role of human milk in extremely low birth weight infants’ risk of necrotizing enterocolitis or death. J Perinatol. 2009;29(1):57-62.
3 Sisk PM, Lovelady CA, Dillard RG, Gruber KJ, O’Shea TM. Early human milk feeding is associated with a lower risk of necrotizing enterocolitis in very low birth weight infants. J Perinatol. 2007;27(7):428-33.
4 Sisk PM, Lovelady CA, Gruber KJ, Dillard RG, O’Shea TM. Human milk consumption and full enteral feeding among infants who weigh </= 1250 grams.Pediatrics 2008; 121(6):e1528-33.
5 Vohr BR, Poindexter BB, Dusick AM, McKinley LT, Wright LL, Langer JC, Poole WK; Beneficial effects of breast milk in the neonatal intensive care unit on the developmental outcome of extremely low birth weight infants at 18 months of age. Pediatrics 2006; 118: e115-123.
6 Vohr BR, Poindexter BB, Dusick AM, McKinley LT, Higgins RD, Langer JC, Poole WK. Persistent beneficial effects of breast milk ingested in the neonatal intensive care unit on outcomes of extremely low birth weight infants at 30 months of age. Pediatrics 2007; 120(4):e953-959.
7 Hurst NC, Meier PP. ‘Breastfeeding the preterm Infant’ p. 431, Ch. 13 in Breastfeeding and Human Lactation, 4th edition, 2010 by Jan Riordan and Karen Wambach, Jones and Bartlett Publishers, Sudbury, MA.
8 Academy Of Breastfeeding Medicine (ABM). Clinical Protocol Number #12: Transitioning the Breastfeeding/Breastmilk-fed Premature Infant from the Neonatal Intensive Care Unit to
Home. 2004 Sep. 9 Quality Improvement Toolkit, California Perinatal Quality
Care Collaborative, rev. 2008.10 Spatz DL. “State of the Science: Use of Human Milk and
Breast-feeding for Vulnerable Infants” (2006) J of Perinatl Neonat Nurs. Vol 20:1; 51-55.
11 Jones E, Hartmann PE. Milk Expression. Ch 5:77. in “Feeding and nutrition in the preterm infant. 2005 by Elizabeth Jones and Caroline King, Elsevier Churchill Livingstone, London, England.
12 Wilde CJ, Addey CVP, Boddy LM, Peaker M. Autocrine regulation of milk secretion by a protein in milk. Biochem. J. 1995; 305:51-58.
13 Ramsay DT, Kent JC, Hartmann RA, Hartmannn PE. Anatomy of the lactating human breast redefined with ultrasound imaging. J. Anat. 2005;206:525–534.
14 Woolridge MW. The ‘anatomy’ of infant sucking. Midwifery. 1986; 2(4): 164-71.
15 Meier PP. Choosing a correctly-fitted breastshield. Accessed on January 10, 2011 from http://www.medelabreastfeedingus.com/tips-and-solutions/13/choosing-a-correctly-fitted-breastshield.
16 Moller AP, Thornhill R. Bilateral symmetry and sexual selection: A meta-analysis. Am Nat 1998;151;174-192.
17 Meier PP, Motykowski JE, Zuleger JL. Choosing a correctly-fitted breastshield for milk expression. Medela Messenger 2004, 2.1:8-9.
18 Jones E, Hitlon S. Correctly fitting breast shields are the key to lactation success for pump dependent mothers following preterm delivery. J Neonatal Nurs. 2009; 15:14-17.
Additional Resources regarding pain as a causative factor for lactation cessation:• Damato EG, Dowling DA, Standing TS, Schuster SD.
Explanation for cessation of breastfeeding in mothers of twins. J Hum Lact 2005; 21(3):296-304.
• Riordan J, Bibb D, Miller M, Rawlins T. Predicting breastfeeding duration using the LATCHbreastfeeding assessment tool. 2001; J Hum Lact 17(1):20-23.
• Dick MJ, Evans ML, Arthurs JB, Barnes JK, Caldwell RS, Hutchins SS, Johnson LK. Predicting early breastfeeding attrition.2002; J Hum Lact 18(1):21-27.
• Wambach KA, Cohen SM. Breastfeeding experiences of urban adolescent mothers.J Pediatr Nurs. 2009 ; 24(4):244-54.

neonatal INTENSIVE CARE Supplement 2012 13
This article discusses the research evidence for best practices in breast pumping hygiene. Contamination of human milk can occur at any or all of several steps in the collection, storage, preparation and administration of human milk for infant feedings, however, for the purposes of this review we will focus specifically and sequentially on the processes involved in mother’s own milk expression by breast pump.
Pathogens in human milkFresh human milk is not sterile but rather contains a wide variety of organisms including non-pathogenic or commensal bacteria, pathogenic bacteria, viruses, mycobacteria and fungi.1-7 Studies vary on quantities of bacteria in human milk. In one study, 100% of collected human milk samples contained bacteria.4 In general the majority of identified organisms are non-pathogenic commensal skin flora from the mother’s nipple or breast, eg, coagulase-negative Staphylococcus epidermidis, diphtheroids, and Streptococcus viridans or are organisms which have migrated via the enteromammary pathway to the breast – such as Bifidobacteria or Lactobacilli – which protect the newborn’s gastrointestinal system.3,8 However, potentially pathogenic bacteria are also common in human milk. Staphylococcus aureus including MRSA, B-hemolytic streptococci, Pseudomonas species, Klebsiella, Proteus species, and enterobacteria are often cited as the most frequent.2-5,9 Of interest to practitioners in the neonatal intensive setting, human milk from mothers of preterm infants has been found by Thompson et al to have higher bacteria levels – non-pathogenic and pathogenic – than human milk from term mothers.1 Also of interest is a finding by Boo and associates that human milk pumped at home has higher contamination levels than milk expressed in the hospital.7
Breast hygieneIn the 1970s and 1980s, breast cleaning prior to pumping and culturing of breastmilk prior to its administration to NICU infants were common practices. Studies on the value of additional breast cleaning beyond daily hygiene prior to pumping are conflicting. Costa in 1989 found additional breast cleaning to be beneficial in reducing human milk bacterial colony counts10 while Thompson et al in 1997 found breast washing with Phisoderm to be no more effective than water alone in reducing bacteria.1 Currently, the Human Milk Banking
Association of North America (HMBANA) and the Academy of Breastfeeding Medicine (ABM) recommend normal maternal body (breast) hygiene but no additional cleaning prior to human milk expression.11,12
Hand hygiene and cleaningAdequate hand cleaning prior to breast pumping is, without a doubt, one of the most important factors in reducing bacteria and pathogens in human milk. Hand cleaning and drying options offer an interesting layer of complexity to the formation of recommendations for mothers. In terms of cleaning methods, we will first examine non-washing and washing methods of hand disinfection followed by issues related to drying options.
While the most frequent method of hand cleaning in a hospital setting is with alcohol rubs, there is insufficient data at this time as to how these methods might impact breast milk collection. Alcohol rubs have been implemented in hospitals and elsewhere for their convenience of use (no sink required) and are supported by the CDC for use in the health care setting for staff. Alcohol rubs are effective when used correctly,13-15 may be more effective than hand washing in removing spores,16 but are not as effective as hand washing in eliminating C difficile.17 HMBANA guidelines acknowledge the use of alcohol rubs as a method to decontaminate hands in the hospital but do not explicitly state they are recommended for use before expressing or handling human milk or feeding equipment.11
Hand washing is often cited as the first line of defense against infection. In the present context, washing may be preferable to other forms of hand hygiene because it does not pose the risk of chemical (alcohol) contact with the breast and human milk. At this time, the literature is inconclusive in terms of results and recommendations for washing with non-antibacterial soap or antibacterial soap in breast pumping mothers. The general concern about antimicrobial soaps is the risk of bacterial resistance18,19 the removal of commensal bacteria that serve a role in protecting skin surfaces20 and the potential effect on T cell maturation.20 For health care workers, the CDC guidelines for hand hygiene recommend hand washing with either non-antimicrobial soap or antimicrobial soap and water when hands are visibly dirty or soiled. Hot water should be avoided because it can damage skin. In addition, the CDC recommends using an alcohol-based rub or an anti-microbial soap to decontaminate health care worker hands between patients and prior to specific patient care activities.14 Lactating mothers are not health care personnel, however, they are in contact with hospital
Evidence-Based Recommendations for Breast Pumping HygieneJean Rhodes, PhD, CNM, IBCLC
Jean Rhodes PhD, CNM, IBCLC has 30 years of experience as a nurse,
lactation consultant, nurse-midwife, educator and researcher. Formerly
with the Medical University of South Carolina, she is now an independent
consultant. This article was provided by Medela.

14 neonatal INTENSIVE CARE Supplement 2012
pathogens as soon as they enter the hospital. Elevator buttons, door handles, intercoms, sink handles, objects in the infant’s environment and waiting areas are just a few examples of potential fomites. Therefore, the use of antimicrobial soaps for hand washing might be of benefit prior to breast pumping in the hospital environment but use of antimicrobial soaps may not be necessary in the home.
Research of hand washing techniques with soap and water vary as to length of washing time and amounts of soap. The CDC guidelines for health care workers recommend applying an amount of soap as recommended by the soap manufacturer and washing for at least 15 seconds, covering all surfaces of the hands and fingers before rinsing and drying.14 Fuls et al found improved cleaning with an increase in wash time to 30 seconds and use of approximately 3 grams of soap volume.21 In situations where manufacturer recommendations are not known, longer times and generous amounts of soap may be prudent. Lastly, more research is needed in the area of hand washing soaps for health care situations. For example, Contreras et al found hand washing with dishwashing soaps to be 100 times more effective than antimicrobial hand soaps in inactivating respiratory syncytial virus.22
Hand drying presents a variety of options for consideration including paper towels, cloth towels, and forced-air dryers. Infection control literature suggests clean disposable paper towel, the most common source of hand drying in hospitals and frequently used in homes, are the most hygienic method of hand drying.14,23-25 However, paper towels which may be wet or contaminated are not recommended. Literature comparing paper and cloth towels on dispenser rolls found cloth towels to be more at risk for contamination.26 Data comparing individual cloth towels to paper towels used in the home is not available.
Forced-air dryers are available in hospitals, public locations and work environments. Hot forced-air hand dryers appear to be safe in most environments,27 however, in hospital environments forced-air hand dryers may disperse bacteria, contributing to air borne contamination.28 (Obviously, coughing, sneezing and expectorating in the process of hand washing and human milk collection can also introduce airborne pathogens in the equation.) More than one study suggests that when using forced-air dryers, hands should not be rubbed together as this increases the numbers of bacteria on dried hands.29,30
Lastly, in terms of hand hygiene, fingernails and jewelry have been found to be factors in post-cleaning bacterial colonization of hands. The evidence-based 2002 CDC recommendations for health care workers’ hand hygiene include not wearing artificial fingernails or extensions, avoiding chipped nail polish, keeping nail tips to less than ¼ inch long, and subungual areas clean. Multiple studies also suggest the presence of rings can negatively impact attempts at hand cleaning. Ring wearing has been associated with 10-fold higher median skin organism colony counts, hand contamination with Staphylococcus aureus, gram-negative bacilli and Candida species.31-33 Furthermore, the more rings an individual wears, the greater the contamination even after hand cleaning.32 While these studies are on health care personnel, they present valuable information for mothers who are practicing hand hygiene prior to breast pumping.
Cleaning Pump EquipmentBreast pumps, like all hospital equipment, are potential carriers
of pathogenic microorganisms. Improper cleaning of breast pumps and pump parts can increase the risk of expressed human milk contamination.11,12 External surfaces of hospital breast pumps, particularly those touched by mothers or staff in the process of pumping, should be disinfected between users. At Rush Presbyterian, Meier has empowered NICU mothers to assume a primary role in their infants’ care, including responsibility for cleaning hospital breast pumps before use with quick cleaning disinfecting wipes.34,35 In addition to pumps, in the hospital and at home, the surface upon which cleaned pump parts are to be placed prior to drying should be disinfected with disinfecting solutions or wipes. If recommended by the solution’s manufacturer, the surface should be rinsed after disinfection with clean water to prevent solution contamination of washed parts. Hands should also be washed after disinfecting pumps and surfaces to prevent breast or human milk contact with disinfectant chemicals.
Pump parts that come in contact with human milk should be completely separated and thoroughly cleaned after use. Even in the case of no human milk collection during a pumping session, pump parts should be cleaned. Washing is the most common method of cleaning in hospital settings. After the pump parts are disassembled, they should be rinsed in cool water to remove human milk residue, especially human milk proteins.11 Parts should be washed with soap and water, either under running water or in a clean bowl or basin designated for this purpose.11 Although not specifically mentioned in the lactation literature, clean paper towels or clean unused cloth towels can be used with soap and water to clean parts as they create friction and remove surface contaminants. Patient specific bottle and nipple brushes can be used to clean parts, especially tight crevices. Sponges are generally discouraged and not appropriate in hospital settings because they trap microorganisms. In the home environment, if they have to be used, sponges should be disinfected by microwaving them (damp) for 2-4 minutes.36 Given the information above on hand washing, the use of antimicrobial soaps for pump part cleaning might be appropriate in some settings. Because of the high levels of bacteria in drains and sinks and on faucet handles, pump parts should not be placed in the sink for washing and faucet handles should be turned off with a clean paper towel.11,14,37
After washing, parts should be rinsed thoroughly then placed on a disinfected surface for drying. A clean paper or cloth towel may be placed on top of the surface to collect dripping water. If the pump parts came in a sterile hard plastic container, this packaging can serve as a temporary surface. As with hand washing, clean paper towels may be used for drying in the hospital or at home. Clean cloth towel drying may be acceptable providing the towel has not been used since laundering. Air-drying is another option but not realistic in some situations where mothers share pumping space with others or if mothers need to leave the cleaning area. Once clean and dry, pump parts should be removed from the sink area to prevent contamination. Reconnect and place with the pump, so parts are ready for the next use. HMBANA recommends cleaning pump parts after rinsing in the dishwasher as an alternative to washing by hand.11 Most dishwashers now also have heat boost and air-drying options.
It is not necessary to clean tubing unless it comes in contact with human milk or other substances. In these cases, or if condensation appears in the tubing, the manufacturer’s instructions for cleaning should be followed. Pump tubing,
neonatal INTENSIVE CARE Supplement 2012 15
connectors to the pump and all other pump parts, are not to be shared between mothers.
After cleaning pump parts you may sanitize in boiling water for at least 10 minutes or with microwave bags, following manufacturer’s instructions. While there are no specific recommendations in the lactation research literature at this time regarding the use of these additional disinfecting measures, there are no known disadvantages. As data emerges about the bacterial growth on “cleaned” (or rather, inadequately cleaned) breast pump parts and in newly expressed human milk, these additional options may become recommended practices.
Expressing human milk as hygienically as possible will diminish the risk of pathogenic contamination and decrease microbial growth in stored human milk, however, the process is fragile and any break in technique can lead to undesired results. Unfortunately, health care workers themselves are often non-compliant with basic infection control practices such as proper hand cleaning, use of rings and fingernail condition.14,38,39 Health education with rationale regarding pumping hygiene should be provided to mothers, fathers and other family members but also to health care staff. Observance of poor hygienic practices in staff caring for hospitalized infants can undermine infection control best practices.
Basic Recommendations for Pumping Hygiene• Maintain short, clean natural fingernails with un-chipped
polish. Avoid wearing rings.• Prior to pumping, prepare a surface for cleaned pump parts:
disinfect, rinse if necessary and cover with clean paper towel or freshly laundered cloth towel.
• Wash hands thoroughly with soap and warm water for 20-30 seconds.
• Turn the sink off with a clean dry paper towel. • Dry hands with clean paper towels or a freshly laundered cloth
towel. • If soap is not available, use a generous amount of alcohol hand
rub to clean all hand surfaces but avoid touching breasts or interior surfaces of clean pumping parts or rinse the alcohol off with water.
• Pump breasts.• After pumping, wash all pump parts that would normally come
in contact with human milk after every use whether human milk was obtained or not.
• Separate pump parts, rinse with cool water, and then wash under warm running water or in a clean bowl/container specified for this purpose only.
• Dry pump parts with clean paper towels, cloth towels or air dry.
• Remove pump parts from sink area.• Reassemble pump parts with clean hands.• Store in a safe location.
Additional Recommendations for Initial Pumping in the Hospital• Hospital staff should disinfect breast pumps between patients
per infection control guidelines.• Provide infant’s mother and family education re: pumping
techniques and hygiene.• Mothers may need assistance with hand hygiene if they are
confined to bed.
Additional Recommendations for Pumping at Home or Work• Wash pump parts in the kitchen area, not in the bathroom.• A dishwasher may be used for washing of pump parts. Some
manufacturer’s suggest top rack only, be sure to follow manufacturer’s cleaning instructions. Use hot water boost and air-drying if available.
Additional Recommendations for Pumping in NICU/Nurseries• Mother or staff must disinfect pump before use with antiseptic
spray or wipes per manufacturer recommendations.• Do not use anyone else’s pump parts including tubing and
pump connectors. • Notify nursery staff of problems with paper towels, soap or
disinfecting materials.
References1 Thompson N, Pickler RH, Munro C, Shotwell J.
Contamination in expressed breast milk following breast cleansing. Journal of human lactation: official journal of International Lactation Consultant Association 1997;13:127-30.
2 Novak FR, Almeida JA, Warnken MB, Ferreira-Carvalho BT, Hagler AN. Methicillin-resistant Staphylococcus aureus in human milk. Mem Inst Oswaldo Cruz 2000;95:29-33.
3 Lawrence RAaL, R.M. Breastfeeding: A Guode for the Medical Profession. 7th ed. Maryland Heights, Missouri: Elsevier Mosby; 2011.
4 Eidelman AI, Szilagyi G. Patterns of bacterial colonization of human milk. Obstetrics and gynecology 1979;53:550-2.
5 Carroll L, Osman M, Davies DP, McNeish AS. Bacteriological criteria for feeding raw breast-milk to babies on neonatal units. Lancet 1979;2:732-3.
6 Carroll L, Osman M, Davies DP. Does discarding the first few millilitres of breast milk improve the bacteriological quality of bank breast milk? Archives of disease in childhood 1980;55:898-9.
7 Boo NY, Nordiah AJ, Alfizah H, Nor-Rohaini AH, Lim VK. Contamination of breast milk obtained by manual expression and breast pumps in mothers of very low birthweight infants. The Journal of hospital infection 2001;49:274-81.
8 Perez PF, Dore J, Leclerc M, et al. Bacterial imprinting of the neonatal immune system: lessons from maternal cells? Pediatrics 2007;119:e724-32.
9 Meier P, Wilks S. The bacteria in expressed mothers’ milk. MCN The American journal of maternal child nursing 1987;12:420-3.
10 Costa KM. A comparison of colony counts of breast milk using two methods of breast cleansing. Journal of obstetric, gynecologic, and neonatal nursing: JOGNN / NAACOG 1989;18:231-6.
11 Jones F, Tully MR. Best practice for expressing, storing and handling human milk in hospitals, homes and child care settings. Raleigh, NC: HumanMilk Banking Association of North America, Inc.; 2006.
12 ABM. ABM clinical protocol #8: human milk storage information for home use for full-term infants (original protocol March 2004; revision #1 March 2010). Breastfeed Med 2010;5:127-30.
13 Kac G, Podglajen I, Gueneret M, Vaupre S, Bissery A, Meyer G. Microbiological evaluation of two hand hygiene procedures achieved by healthcare workers during routine patient care: a randomized study. The Journal of hospital

16 neonatal INTENSIVE CARE Supplement 2012
infection 2005;60:32-9.14 Boyce JM, Pittet D. Guideline for Hand Hygiene in Health-
Care Settings. Recommendations of the Healthcare Infection Control Practices Advisory Committee and the HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force. Society for Healthcare Epidemiology of America/Association for Professionals in Infection Control/Infectious Diseases Society of America. MMWR Recomm Rep 2002;51:1-45, quiz CE1-4.
15 Widmer AE, Dangel M. Alcohol-based handrub: evaluation of technique and microbiological efficacy with international infection control professionals. Infection control and hospital epidemiology: the official journal of the Society of Hospital Epidemiologists of America 2004;25:207-9.
16 D’Antonio NN, Rihs JD, Stout JE, Yu VL. Revisiting the hand wipe versus gel rub debate: is a higher-ethanol content hand wipe more effective than an ethanol gel rub? American journal of infection control 2010;38:678-82.
17 Oughton MT, Loo VG, Dendukuri N, Fenn S, Libman MD. Hand hygiene with soap and water is superior to alcohol rub and antiseptic wipes for removal of Clostridium difficile. Infection control and hospital epidemiology: the official journal of the Society of Hospital Epidemiologists of America 2009;30:939-44.
18 Tan L, Nielsen NH, Young DC, Trizna Z. Use of antimicrobial agents in consumer products. Archives of dermatology 2002;138:1082-6.
19 Aiello AE, Larson EL, Levy SB. Consumer antibacterial soaps: effective or just risky? Clinical infectious diseases: an official publication of the Infectious Diseases Society of America 2007;45 Suppl 2:S137-47.
20 Levy SB. Antibacterial household products: cause for concern. Emerging infectious diseases 2001;7:512-5.
21 Fuls JL, Rodgers ND, Fischler GE, et al. Alternative hand contamination technique to compare the activities of antimicrobial and nonantimicrobial soaps under different test conditions. Applied and environmental microbiology 2008;74:3739-44.
22 Contreras PA, Sami IR, Darnell ME, Ottolini MG, Prince GA. Inactivation of respiratory syncytial virus by generic hand dishwashing detergents and antibacterial hand soaps. Infection control and hospital epidemiology: the official journal of the Society of Hospital Epidemiologists of America 1999;20:57-8.
23 Griffith CJ, Obee P, Cooper RA, Burton NF, Lewis M. The effectiveness of existing and modified cleaning regimens in a Welsh hospital. J Hosp Infect 2007;66:352-9.
24 Harrison WA, Griffith CJ, Ayers T, Michaels B. Bacterial transfer and cross-contamination potential associated with paper-towel dispensing. Am J Infect Control 2003;31:387-91.
25 Harrison WA, Griffith CJ, Michaels B, Ayers T. Technique to determine contamination exposure routes and the economic efficiency of folded paper-towel dispensing. Am J Infect Control 2003;31:104-8.
26 Gustafson DR, Vetter EA, Larson DR, et al. Effects of 4 hand-drying methods for removing bacteria from washed hands: a randomized trial. Mayo Clin Proc 2000;75:705-8.
27 Matthews JA, Newsom SW. Hot air electric hand driers compared with paper towels for potential spread of airborne bacteria. J Hosp Infect 1987;9:85-8.
28 Ngeow YF, Ong HW, Tan P. Dispersal of bacteria by an electric air hand dryer. Malays J Pathol 1989;11:53-6.
29 Snelling AM, Saville T, Stevens D, Beggs CB. Comparative evaluation of the hygienic efficacy of an ultra-rapid hand dryer vs conventional warm air hand dryers. J Appl Microbiol
2011;110:19-26.30 Yamamoto Y, Ugai K, Takahashi Y. Efficiency of hand drying
for removing bacteria from washed hands: comparison of paper towel drying with warm air drying. Infect Control Hosp Epidemiol 2005;26:316-20.
31 Hoffman PN, Cooke EM, McCarville MR, Emmerson AM. Micro-organisms isolated from skin under wedding rings worn by hospital staff. Br Med J (Clin Res Ed) 1985;290:206-7.
32 Trick WE, Vernon MO, Hayes RA, et al. Impact of ring wearing on hand contamination and comparison of hand hygiene agents in a hospital. Clinical infectious diseases: an official publication of the Infectious Diseases Society of America 2003;36:1383-90.
33 Salisbury DM, Hutfilz P, Treen LM, Bollin GE, Gautam S. The effect of rings on microbial load of health care workers’ hands. American journal of infection control 1997;25:24-7.
34 Meier PP, Engstrom JL, Mingolelli SS, Miracle DJ, Kiesling S. The Rush Mothers’ Milk Club: breastfeeding interventions for mothers with very-low-birth-weight infants. Journal of obstetric, gynecologic, and neonatal nursing: JOGNN / NAACOG 2004;33:164-74.
35 Meier P. Storage, handling & feeding of human milk in the NICU. In: medelaeducation.com.
36 Bitton G. “Microbial inactivation by microwave radiation in the home environment”. J Environ Health 2007;69:6, 63.
37 Squier C, Yu VL, Stout JE. Waterborne Nosocomial Infections. Curr Infect Dis Rep 2000;2:490-6.
38 Hautemaniere A, Cunat L, Diguio N, et al. Factors determining poor practice in alcoholic gel hand rub technique in hospital workers. J Infect Public Health 2010;3:25-34.
39 Kennedy AM, Elward AM, Fraser VJ. Survey of knowledge, beliefs, and practices of neonatal intensive care unit healthcare workers regarding nosocomial infections, central venous catheter care, and hand hygiene. Infection control and hospital epidemiology: the official journal of the Society of Hospital Epidemiologists of America 2004;25:747-52.

neonatal INTENSIVE CARE Supplement 2012 17
Helping mothers of NICU infants establish and maintain adequate milk production is a challenging task for health care providers. Many of these mothers have preexisting medical conditions with superimposed pregnancy complications, some of which – such as diabetes, obesity, and thyroid disease – can negatively impact milk production.1 The emotional stress associated with preterm delivery is also known to impact milk production. Compounding these obstacles, many of these mothers did not plan to breastfeed, much less pump. Thus, hospital and community practitioners have very important roles in breastfeeding education, advocacy and support.
In the past six years alone, the lactation literature has exploded with clinical studies, scientific discoveries and professional practice protocols. Along with this new information comes concern – especially in neonatal intensive care (NICU) settings – that practices be kept current and evidence based. Therefore, an essential resource for clinicians is the Human Milk Banking Association of North America’s (HMBANA) 3rd edition of Best Practice for Expressing, Storing and Handling Human Milk in Hospitals, Homes, and Child Care Settings.
While the HMBANA guidelines cover many topics, the focus of this paper is to examine the 2011 HMBANA breast pump recommendations for situations in which infants are unable to breastfeed for extended periods of time. The 2011 HMBANA guidelines recommend a hospital-grade breast pump for mothers whose infants cannot breastfeed “for an extended period of time” or when an infant “is not feeding effectively.”2
Breast pumps work through a combination of suction strength (vacuum pressure) and suction pattern (frequency of cycles per minute). By observing term infants at breast, Kent et al3 found infant sucking patterns change over the course of a breastfeeding session. At the beginning of breastfeeding and prior to milk ejection, infants suck rapidly. This pattern changes to a slower and deeper suction pattern as the milk ejects. Using ultrasound imaging, Kent et al3 verified milk ejection is critical to the overall process of milk removal from the breast. And by comparing the effect of different pumping patterns on milk ejection, they were able to determine the most effective pumping patterns for milk expression. Hospital-grade pumps with computer technology
have been programmed to mimic variations in infant sucking thereby improving the degree and speed of breast emptying.4
Breast pump suction control and suction patterns are important factors in removing adequate amounts of milk to stimulate milk synthesis. Both are also important factors in patient comfort. In a 2008 study5 involving a hospital-grade electric pump, researchers determined each mother had a maximum level of suction that is still comfortable for her. To find this level, pumping women increased the pump suction to the point of beginning discomfort, and then decreased the suction to a point of comfort. When women used their own maximum, but still comfortable, vacuum levels they obtained higher milk volumes and milk higher in fat. Pain with pumping may indicate the suction level is too high (though there may be many reasons for nipple pain). Obviously, the more comfortable a woman is while pumping, the more likely she is to continue.
As a large percentage of NICU infants immediately post birth are simply unable to breastfeed and their mothers may have difficulty for many reasons establishing milk supply, a hospital-grade pump is recommended because as HMBANA states:• Mid-sized electric pumps sold for individual use tend to work
best for mothers who have established a milk supply and are breastfeeding on a regular basis as well as pumping.
• Small electric/battery operated/and hand pumps may work for occasional use once the milk supply is well established.
Sisk et al6 support these sentiments in a recent qualitative study. In this study of the supports and barriers to milk expression, the authors interviewed 32 mothers of very low birth weight infants. While subjects included women who planned to breastfeed as well as who did not plan to breastfeed or pump, all women in the study ultimately chose to pump for their preterm infants. The authors noted that NICU mothers who used primarily small electric or manual breast pumps had great difficulty establishing a pumping routine and adequate milk supply because pumps were ineffective at emptying their breasts.
In addition, for more than twenty years, research has found that hospital-grade pumps also express a greater volume of breastmilk than hand expression or manual pumps. The research has shown that hospital-grade pumps empty the breasts better, increasing the fat content of composite milk.7-9 In a study cited by HMBANA, Slusher et al10 compared expressed breastmilk volumes obtained via pumping to those obtained by hand expression. This study was conducted in a Nigerian NICU where
Current Breast Pump Recommendations for NICU Mothers: 2011 HMBANA Guidelines – an Essential ResourceJean Rhodes, PhD, CNM, IBCLC
Jean Rhodes, PhD, CNM, IBCLC has 30 years of experience as a nurse,
lactation consultant, nurse-midwife, educator and researchers. Formerly
of the Medical University of South Carolina, she is now an independent
consultant. This article was provided by Medela.

18 neonatal INTENSIVE CARE Supplement 2012
hand expression was the norm. Their results suggested mothers who used a hospital grade breast pump expressed significantly more milk than mothers who hand expressed. In general, improved volumes of expressed milk indicate better breast emptying.
Daly et al11 studied the degree of breast emptying and the effect of timing between pumping sessions on rates of milk synthesis. They found the degree of breast emptying impacted breast milk synthesis more than the frequency of breast pumping. Thus they concluded mothers produce more milk if they are able to more fully empty the breast. Lastly, Slusher et al9 in another study of Nigerian NICU mothers found a hospital-grade electric pump facilitated the collection of hindmilk. During a weeklong hindmilk intervention, mothers increased their average daily milk volumes using a hospital-grade electric breast pump when compared to their milk volumes via hand expression. Furthermore, the infants fed pump-expressed hindmilk had improved weight gains, both during the intervention and after discharge. For example, the mean infant weight gain prior to the hindmilk intervention was 10.1 grams/day. During the intervention mean weight gains increased to 18.8 grams/day and remained elevated over pre-intervention baseline for at least two weeks after discharge.
For the first time, the new HMBANA guidelines include a discussion of “hands on pumping” or the combination of breast massage, hand expression and pumping with an effective pump. Morton et al12 described an increase in milk removal in mothers of preterm infants <31 weeks who consistently practiced manual colostrum expression and breast massage along with breast pumping. Most lactation practitioners have observed mothers spontaneously augmenting breast pumping with a variety of manual techniques. The combination of methods makes sense in the context of pumping as healthy infants express milk from the breast by a combination of suction and breast compression. Hands on pumping, therefore, helps compensate for the absence of breast compression in pump dependent mothers.
A new recommendation in the 2011 HMBANA guidelines is evaluation of pump flanges for proper fit. In 2004, Meier et al13 discussed problems associated with poorly fitted breastshields. These included incomplete milk removal, nipple trauma and pain. The majority of hospital-grade pumps come with the option of different size breastshields. Meier and colleagues recommended evaluating NICU mothers frequently for flange fit as their nipples can change size more than once over the course of extended breast pumping. Indicators of a properly fitted breastshield include: the nipple is centered and will move easily in the tunnel of the flange, none of the areola (or only a small amount) will be pulled into the tunnel, there is a gentle rhythmic motion of the breast with each cycle of the pump, pumping is comfortable, the nipples are not painful, blanched or cracked and the breasts are well drained.13
Listening to what women say about their breast pumping experiences is also important. A 2008 Cochrane Review: Methods of Milk Expression for Lactating Women14 examined the issues of efficiency and acceptability of all methods of expressing human milk. Twelve studies on milk expression met their criteria for review. Most studies either compared sequential to simultaneous pumping or compared methods of expression (hand expression, manual pump or electric pump) to one another. No studies compared two or more hospital-grade pumps. The authors
concluded, “…no one type of pump…is suitable for all mothers and all circumstances.” More importantly, they identified in the milk expression literature a lack of attention to the issue of maternal satisfaction.
Since 2008, qualitative researchers have looked more closely at the experiences of women who are breast pumping. Like the study by Sisk et al6 above, other studies have explored mothers’ perceptions of breast pumping. Clemons et al15 in 2010 questioned breastfeeding mothers about their experiences of milk expression, either by hand or by pump. While the majority of women preferred breast pumps to hand expression, reasons given for not liking a pump included that it was ineffective or painful. Certainly these concerns should inform practice and breast pump standards. Studies like these as well as those by Meier et al16,17 and Kent et al5 – all of which highlight the importance of maternal feedback – are needed if our goal is to advocate for mothers expressing milk for their hospitalized infants.
In summary, we have reviewed the research evidence supporting the 2011 HMBANA guidelines on breast pump selection for NICU mothers. Current best practice standards continue to recommend the use of hospital-grade electric pumps when infants cannot go to breast or when they cannot breastfeed effectively.
References1 Lawrence RA, Lawrence, RM. Breastfeeding: A Guide for
the Medical Profession. 7th ed. Maryland Heights, Missouri: Elsevier Mosby; 2011.
2 Jones F. Best practice for expressing, storing and handling human milk in hospitals, home, and child care settings. Fort Worth, Texas: HMBANA;2011.
3 Kent JC, Ramsay DT, Doherty D, Larsson M, Hartmann PE. Response of breasts to different stimulation patterns of an electric breast pump. J Hum Lact. May 2003;19(2):179-186; quiz 187-178, 218.
4 Mitoulas LR, Lai CT, Gurrin LC, Larsson M, Hartmann PE. Effect of vacuum profile on breast milk expression using an electric breast pump. Journal of human lactation : official journal of International Lactation Consultant Association. Nov 2002;18(4):353-360.
5 Kent JC, Mitoulas LR, Cregan MD, et al. Importance of vacuum for breastmilk expression. Breastfeed Med. Mar 2008;3(1):11-19.
6 Sisk P, Quandt S, Parson N, Tucker J. Breast milk expression and maintenance in mothers of very low birth weight infants: supports and barriers. Journal of human lactation : official journal of International Lactation Consultant Association. Nov 2010;26(4):368-375.
7 Boutte CA, Garza C, Fraley JK, Stuff JE, Smith EO. Comparison of hand- and electric-operated breast pumps. Hum Nutr Appl Nutr. Dec 1985;39(6):426-430.
8 Green D, Moye L, Schreiner RL, Lemons JA. The relative efficacy of four methods of human milk expression. Early human development. Apr 1982;6(2):153-159.
9 Slusher T, Hampton R, Bode-Thomas F, Pam S, Akor F, Meier P. Promoting the exclusive feeding of own mother’s milk through the use of hindmilk and increased maternal milk volume for hospitalized, low birth weight infants (<1800 grams) in Nigeria: a feasibility study. Journal of human lactation : official journal of International Lactation Consultant Association. May 2003;19(2):191-198.

neonatal INTENSIVE CARE Supplement 2012 19
10 Slusher T, Slusher IL, Biomdo M, Bode-Thomas F, Curtis BA, Meier P. Electric breast pump use increases maternal milk volume in African nurseries. J Trop Pediatr. Apr 2007;53(2):125-130.
11 Daly SE, Kent JC, Owens RA, Hartmann PE. Frequency and degree of milk removal and the short-term control of human milk synthesis. Exp Physiol. Sep 1996;81(5):861-875.
12 Morton J, Hall JY, Wong RJ, Thairu L, Benitz WE, Rhine WD. Combining hand techniques with electric pumping increases milk production in mothers of preterm infants. J Perinatol. Nov 2009;29(11):757-764.
13 Meier P, Motykowski JE, Zuleger JL. Choosing a correctly-fitted breastshield for milk expression. Medela Messenger. Vol 21. McHenry IL: Medela, Inc; 2004:1.
14 Becker GE, McCormick FM, Renfrew MJ. Methods of milk expression for lactating women. Cochrane database of systematic reviews. 2008(4):CD006170.
15 Clemons SN, Amir LH. Breastfeeding women’s experience of expressing: a descriptive study. Journal of human lactation: official journal of International Lactation Consultant Association. Aug 2010;26(3):258-265.
16 Meier PP, Engstrom JL, Hurst NM, et al. A comparison of the efficiency, efficacy, comfort, and convenience of two hospital-grade electric breast pumps for mothers of very low birthweight infants. Breastfeed Med. Sep 2008;3(3):141-150.
17 Meier P, Hurst N, Rodriguez N, et al. Comfort and effectiveness of the Symphony breast pump for mothers of preterm infants: comparison of three suction patterns. Advances in experimental medicine and biology. 2004;554:321-323.

20 neonatal INTENSIVE CARE Supplement 2012
An overwhelming body of evidence demonstrates that feeding human milk to premature and other compromised infants in the NICU greatly reduces the risk of necrotizing enterocolitis, late onset sepsis, enteral feed intolerance and other serious morbidities.1-8 Further evidence shows that human milk directly impacts the health outcomes of premature infants in a dose-response manner – greater amounts of human milk feeding offer greater protection.8-10 Since mothers of premature infants are often pump-dependent and many have to return to work before their infant is ready to feed at breast, proper storage of human milk is essential.
There has been much research on this topic regarding both the nutritive and protective components as well as the bacterial content of human milk. Due to the variants in each study, findings may appear to conflict. It is important to note that each study should be weighed based on its particular parameters and variants. According to the 2011 Human Milk Banking Association of North America (HMBANA) Guidelines, studies recommending longer storage periods at room temperature or in the refrigerator have typically focused on bacteriological safety without considering the effects on the components of human milk.(HMBANA p. 44)11 Alternatively, more recent studies focusing on human milk components have noted concerns on the effects of lipids, proteins and other milk components while not addressing bacterial load.12
HMBANA guidelines also note that to decide which storage guidelines are appropriate, the age and health of the infant as well as other factors must be considered. With high-risk infants, the safest approach is to minimize contamination and use appropriate storage conditions for the shortest storage time possible.(HMBANA p. 44)11 This article will summarize research-
based information on proper storage techniques and best practice recommendations from experts that will minimize potential contamination while best protecting the integrity of the protective benefits of the milk for infants in the NICU.
Collection of Human Milk Research shows human milk is not sterile as it contains bacteria including flora from the mothers’ skin and that most contamination of stored milk is found to have occurred during collection.12 While most bacteria found in human milk is safe for baby, careful collection and storage will help prevent additional contamination of the milk.(HMBANA p. 2)11
Manufacturers’ cleaning guidelines of breastpumps, breastpump kit parts and collection containers should be followed. When using a breastpump, mothers should first clean the pump with a manufacturer approved cleaning agent. The pump should be wiped down between each use especially when shared between mothers.(HMBANA p.17)11 Any surface that the mother touches should be cleaned. After cleaning the pump the mother should wash her hands.
Always washing hands before handling breastpump kit parts and collection containers which come in contact with human milk is an important and unfortunately sometimes forgotten step. ABM Clinical Protocol for Human Milk Storage states, “Unclean hands may transmit viruses and bacteria, some of which can cause illness. Studies show that human milk containing fewer bacteria at the time of expression develops less bacterial growth during storage and has higher protein levels compared to milk that has an abundance of bacteria.”
Collection ContainersHuman milk in the NICU should be collected and stored in sterile FDA-approved food grade containers that are BPA-free. Research shows that while lipid-soluble nutrients may stick to the surface of these containers, the concentration of immunoglobulin A and amount of white blood cells are not markedly affected. Use of polyethylene containers was associated with a 60% drop in immunoglobulin A. Another study showed that stainless steel containers demonstrated a decline in cell count and viability compared to polyethelene and glass.. Therefore, stainless steel containers should not be used.13
Using sterile containers helps prevent introducing additional bacteria to the milk. Milk storage bags are not recommended for storing milk for feeding in the NICU based on research which
Human Milk Storage in the NICU – Summarizing the Research – What You Should KnowAmy O’Malley, RN, MSN
Amy O’Malley began her practice as a pediatric nurse at Children’s Memorial
Hospital in Chicago where she was later appointed Director of Nursing
Resources. She spent several years on the faculty at Loyola University School
of Nursing in Chicago. There, O’Malley taught pediatrics and community
health and served as the Project Manager for Loyola’s school-based health
center at Proviso High School, an HRSA funded project providing primary
healthcare and preventive services. O’Malley has presented nationally and
authored numerous book chapters. Her most recent publications include
chapters on “Evidence-Based Practice” and “Organizing and Planning
Care” in the 2008 Nursing Management and Leadership textbook. She
graduated from Loyola University Chicago with a master’s degree in Health
Systems Management, is a member Sigma Theta Tau and currently works as
the Director of Education and Clinical Services for Medela Inc.

neonatal INTENSIVE CARE Supplement 2012 21
shows milk stored in polyethylene bags loses up to 60 percent of secretory IgA(HMBANA p. 20)11 If your facility does not use sterile containers be sure to follow the manufacturer’s guidelines for cleaning.
Labeling Collection containers must be labeled properly and should be stored in a per patient section of either the refrigerator or freezer. The labels should clearly indicate patient name as well as the time and date of expression. Containers should be rotated so the oldest milk is fed first. Once that milk is thawed, a new time and date should be added to the label as thawed milk should be fed within 24 hours.(HMBANA pgs. 2, 44)11
Storing Human Milk at Room TemperatureThe evidence shows that freshly expressed human milk best preserves its nutritional and bioactive components. In fresh milk, living cells work to phagocytize the bacteria and therefore the bacterial colony count in freshly expressed milk decreases over the first several hours.14 This means that freshly expressed milk can be safely kept right at the bedside for less than 4 hours in which time often two feedings may occur. Unfortunately, in the NICU, mothers are often not able to provide freshly expressed milk. Refrigerated and frozen storage methods are a necessity.
Transporting methods will depend on length of time between the milk expression and mothers’ arrival in the NICU. Mothers should be given clear instruction on proper storage during transport per their specific needs.
Feeding ColostrumPreterm colostrum has higher concentrations of anti-infectives, anti-inflammatories, growth factors and other protective substances than does term colostrum. It should be fed as soon as possible in early feedings. The first milk is especially important and should be labeled and fed in order of expression.15, 16
Storing Human Milk in the RefrigeratorOver the years there have been a number of published studies regarding the refrigeration of human milk. Study results have varied with recommendations from no longer than 48 hours to others that reported evidence showed 72 hours for fortified milk maintained milk’s integrity, to recommendations from HMBANA of safe refrigeration for up to eight days.13 These studies focus on bacterial colony counts.
In a study published in 2010 in The Journal of Pediatrics, Slutzah et al looked at refrigerator storage of human milk at 4°C for 96 hours in the NICU, showing that at this temperature, and for this length of time, the integrity of milk was not negatively impacted.17 The study found that “mother’s milk may be stored in the NICU at refrigerator temperature of 4°C for 96 hours without compromising its overall integrity as assessed by bacterial colony counts, white blood cell counts, osmolality, pH and concentrations of sIgA, lactoferrin protein, total fat and free fatty acids.”
HMBANA recommends that freshly expressed milk be fed or refrigerated immediately. If a refrigerator is not available, the milk may be refrigerated within 4 hours. Continuous feeds can therefore be given over a four hour period. If fortifiers have been added to the milk, the human milk should be fed or refrigerated right away.(HMBANA pgs 2, 44)11
Storing Human Milk in the FreezerThe process of freezing human milk destroys its living cells and interrupts phagocytosis. Studies show the viral load in milk such as Cytomegalovirus (CMV) is reduced significantly but not destroyed. In addition the bioavailability and concentration of some protective components are reduced.14
Some medical centers such as Rush University Medical Center, Chicago, IL recommend that NICUs store frozen human milk on site for their patients as this is the only way to ensure control over storage conditions which should be monitored on a regular basis. Industrial freezers are recommended as they are the standard of care for adult nutrition. Studies vary on suggested length of time milk should be frozen. HMBANA guidelines, based on numerous studies recommend that a three month period is optimal and should not be kept for longer than 12 months at -20°C or lower.(HMBANA pgs 2, 44)11 While there is little research on refreezing human milk, experts agree that once thawed frozen human milk should be fed or discarded and not refrozen. [A note on odor: some mothers may question the odor of frozen milk; this can be a result of lipase not being inactivated during freezing so human milk can partially self-digest, resulting in a sour odor. Research demonstrates that this milk is still safe to feed. Scalding the milk prior to freezing to 180°F will inactivate the lipase and decrease the odor. (HMBANA p. 31)11]
Freezing Human MilkDo not pour room temperature human milk into a container with frozen milk; rather, chill freshly expressed milk before adding it to frozen milk. Be cautious: each time a container is opened allows another opportunity for contamination. Experts recommend filling containers only ¾ full (as frozen milk expands and a new container should be used each time a mother pumps.(HMBANA p. 22)11
Thawing Human MilkSterile technique for handling should be used to prevent introducing additional pathogens. Milk should be warmed to body temperature. Clinicians should note that studies show that feeding human milk at room temperature may actually be harmful to very low birth weight infants.18
Milk can be thawed using a number of different methods. Milk can be thawed in a container of warm water; however milk can become contaiminated by non-sterile water seeping under the lid of the container.(HMBANA p.28)11 Milk can be thawed slowly at room temperature, however, should be refridgerated before it is completely thawed and still has ice crystals. It is essential to gently agitate the thawed milk prior to feeding to ensure uniform distribution of fat and micronutrients.(HMBANA p. 28)11 Be sure to properly label when the milk is removed from the freezer. In addition, research has noted microbial contamination of hospital tap water and recommended dry-warming devices to heat fluids that come in contact with patients.19-25 In its 2003 Guideline for Infection Control in Health-Care Facilities, the CDC recognizes that water-based solutions can serve as reservoirs for waterborne microorganisms in hospital settings.26 Therefore, some experts suggest an optimal method is a milk warmer that circulates warm air to safely warm and thaw milk.
ConclusionEvidence demonstrates that feeding human milk to premature and other compromised infants in the NICU greatly reduces the risk of necrotizing enterocolitis, late onset sepsis, enteral feed

22 neonatal INTENSIVE CARE Supplement 2012
intolerance and other serious morbidities.1-8 Further evidence shows that human milk directly impacts the health outcomes of premature infants in a dose-response manner – greater amounts of human milk feeding offer greater protection.8-10 Since mothers of premature infants are often pump-dependent and many have to return to work before their infant is ready to feed at breast, proper storage of human milk is essential. Research-based information on proper storage techniques and best practice recommendations from experts will minimize potential contamination while best protecting the integrity of the protective benefits of the milk for infants in the NICU.
References1 Sisk PM, Lovelady CA and Dillard RG. Effect of education
and lactation support on maternal decision to provide human milk for very-low-birth-weight infants. Adv Exper Med Bio 554: 307-11, 2004.
2 Sisk PM, Lovelady CA, Gruber KJ, Dillard RG, O’Shea TM. Early human milk feeding is associated with a lower risk of necrotizing enterocolitis in very low birthweight infants. J Perinatol 162: 428-433, 2007.
3 Sisk PM, Lovelady CA, Gruber KJ, Dillard RG, O’Shea TM. Human milk consumption and full enteral feeding among infants who weigh ≤ 1250 grams. Pediatrics 121: 1528e-1533e, 2008.
4 Jennifer A. Bisquera, MD; Timothy R. Cooper, MD; and Carol Lynn Berseth, MD. Impact of Necrotizing Enterocolitis on Length of Stay and Hospital Charges in Very Low Birth Weight Infants. Pediatrics 109 (3), 423-428, 2002.
5 Payne NR, Carpenter JH, Badger GJ, Horbar JD, Rogowski J. Marginal increase in cost and excess length of stay associated with nosocomial bloodstream infections in surviving very low birth weight infants. Pediatrics 114 (2): 348-55, 2004.
6 Hylander AM, Strobino DM, Dhanireddy R. Human Milk Feedings and Infection Among Very Low Birth Weight Infants. Pediatrics 102; e38, 1998.
7 Fanaroff AA, Stoll BJ, Wright LL, et al. Trends in Neonatal Morbidity & Mortality for VLBW Infants AJOBGYN 196 (2):147, el-8, Feb. 2007.
8 Furman L, Taylor G, Minich N, Hack M. The effect of maternal milk on neonatal morbidity of very low-birth-weight infants. Arch Pediatr Adolesc Med 157 (1): 66-71, 2003.
9 Vohr BR, Poindexter BB, Dusick AM; McKinley LT, Wright LL, Langer JC, Poole WK, and for the NICHD Neonatal Research Network. Beneficial effects of breast milk in the neonatal intensive care unit on the developmental outcome of extremely low birthweight infants at 18 months of age. Pediatrics 118: 115-123, 2006.
10 Vohr BR, Poindexter BB, Dusick AM; McKinley LT, Higgins RD, Langer JC, Poole WK, and for the NICHD Neonatal Research Network. Persistent beneficial effects of breast milk ingested in the neonatal intensive care unit on outcomes of extremely low birthweight infants at 30 months of age. Pediatrics 120: e953-959, 2007.
11 Jones, F. Best Practice for Expressing, Storing and Handling Human Milk in Hospitals, Homes and Child Care Settings, Second Edition. The Human Milk Banking Association of North America, (HMBANA) 2011.
12 Ogundele, M. Effects of storage on the physiochemical and antibacterial properties of human milk. British Journal of BioMedical Science, Aug. 2002.
13 English, A, The Academy of Breastfeeding Medicine Protocol Committee, ABM Clinical Protocol #8 Human Milk Storage Information for Home Use for Full-Term Infants;
Breastfeeding Medicine Vol 5 Num 3, 127-130, 2010.14 Jones E., King C., Spencer A. Feeding and Nutrition in the
Preterm Infant. 2005; 35.15 Mathur NB, Swarkadas AM, Sharma VK, et al. Antiinfective
factors in preterm human colostrum. Acta Pediatria Scandinavia 79: 1039-1044, 1990.
16 Rodriguez NR, Meier PP, Groer MW, Zeller JM. Oropharyngeal administration of colostrum to extremely low birthweight infants: Theoretical perspectives. J Perinatol : 1-7, 2008.
17 Slutzah M, Codipilly CN, Potak D, et al. Refrigerator storage of expressed human milk in the neonatl intensive care unit. J Pediatr 2010; 156: 26-28.
18 Gonzales I, Duryea EJ, Vasquez E, Geraghty N. Effect of enteral feeding temperature on feeding tolerance in preterm infants. Neonatal Netw 1995; 14: 39-43.
19 Sanchez-Carrillo C, Padilla B, Marin M, et al. Contaminated feeding bottles: the source of an outbreak of Pseudomonas aeruginosa infections in a neonatal intensive care unit. Am J Infect Control 2009;37:150-4.
20 Buyukyavuz BI, Adiloglu AK, Onal S, Cubukcu SE, Cetin H. Finding the sources of septicemia at a neonatal intensive care unit: newborns and infants can be contaminated while being fed. Jpn J Infect Dis 2006;59:213-5.
21 Anaissie EJ, Penzak SR, Dignani MC. The hospital water supply as a source of nosocomial infections: a plea for action. Arch Intern Med 2002;162:1483-92.
22 Squier C, Yu VL, Stout JE. Waterborne Nosocomial Infections. Curr Infect Dis Rep 2000;2:490-6.
23 Rutala WA, Weber DJ. Water as a reservoir of nosocomial pathogens. Infect Control Hosp Epidemiol 1997;18:609-16.
24 Angelbeck JA, G.A. O, Canonica FP, Cervia JS. Hopsital water: A source of concren for infections. Managing Infection Control 2006:44-54.
25 Tasker F. Hospital’s water supply under scrutiny. Miami Herald 2009 June 12, 2009.
26 CDC. Guidelines for environmental infection control in health-care facilities. In: (HICPAC) HICPAC, ed.: MMWR; 2003:1-42.

AdPage 23
Keep the connection.™Medela, Inc., P.O. Box 660, 1101 Corporate Drive, McHenry, IL 60051-0660 Phone: (800) 435-8316 or (815) 363-1166 Fax: (815) 363-1246 Email: [email protected] is a registered trademark of Medela Holding AG. Waterless Milk Warmerand Keep the connection are trademarks of Medela, Inc. 1547630 A © 2011 Medela
Use the safer practice to prepare human milk.
Waterless Milk Warmer™
Eliminates contamination risk of warming milk with tap water.
The CDC reports that high risk patients are among those at the greatest risk of infection caused by waterborne microorganisms.1
Call or email your localMedela Consultant for a demonstration.
1. Centers for Disease Control and Prevention. (2003) Guidelines for Environmental Infection Control in Health-Care Facilities. Recommendations of CDC and Healthcare Infection Control Practices Advisory Committee (HICPAC). MMWR, 52(RR10):1-42.

AdPage 24
Keep the connection.™
1547
761
A 0
212
© 2
012
Med
ela,
Inc.
For more information contact your Medela representative or visit www.medela.com.
Educate
Pump
Collect & Store
PrepareFeed
Diagnose
benefi ts of breastmilk . . .
Medela supports
your effortsto help mothers provide
the life-giving
to home.. . . from hospital
Professional Mom Baby Ad 1547761 A.indd 1 3/16/12 8:46 AM


















