viz.,...Diffusional, viz., pulmonary scleroderma. The two cases to be presented demonstrate...
8
CARDIAC FAILURE SECONDARY TO INEFFECTIVE BELLOWS ACTION OF THE CHEST CAGE By JAMES A. FELTMAN, WALTER NEWMAN, ARTHUR SCHWARTZ, DANIEL J. STONE, AND FRANCIS J. LOVELOCK (From the Cardio-Pulmonary Laboratory and the Medical Service at the Bronx Veterans Administration Hospital, Bronx, N. Y.) (Submitted for publication April 7, 1952; accepted June 13, 1952) Baldwin, Cournand, and Richards (1) have de- scribed the following classification of pulmonary insufficiency: 1. Ventilatory a. Restrictive, viz., pulmonary fibrosis, ky- phoscoliosis. b. Obstructive, viz., pulmonary emphysema. 2. Alveolar-respiratory a. Distributive, viz., pulmonary emphysema. b. Diffusional, viz., pulmonary scleroderma. The two cases to be presented demonstrate ventilatory insufficiency of the restrictive type due ,in the first instance to primary neuromuscular dysfunction and in the second to chronic pleural disease with resulting calcification and restriction of the underlying parenchyma and diaphragm. Of particular interest was the development of con- gestive heart failure in both of these patients. These cases represent examples of cardiac failure secondary to an ineffective bellows action of the chest cage without significant intrinsic pulmonary disease. CASE REPORTS Case 1 This 34 year old white male was well until 1945 when he noted the gradual onset of weakness of the right side of the face. A few months later he began to have bilateral jaw weakness, and difficulty in swallowing food with regurgitation of fluid through the nose. In 1947 there was onset of occasional diplopia. He was admitted to this hospital on three different occasions between Janu- ary 1947 and November 1948 and on all these admissions showed signs and symptoms of bulbar involvement. These signs and symptoms persisted with little change except for development of dysarthria. In November 1949 he complained of difficulty in maintaining erect posture and he was readmitted for his fourth and final admission. At this time the patient stated he had noted dyspnea on exertion for the preceding one and a half years and dur- ing the month before admission, cyanosis of the lips had become apparent. On admission the patient appeared chronically ill without respiratory distress but with cyanosis of the lips, nailbeds, and skin. There was a marked dysarthria. His chest cage moved very little on normal respiration but he had good expansion with effort and could clear most of his cyanosis with forced breathing. The heart was not remarkable on examination except for a markedly ac- centuated P2. The lungs were clear to percussion and auscultation. The abdominal examination was within normal limits. Neurological examination revealed the right pupil to be larger than the left, and both reacted sluggishly to light and accommodation. The external ocular movements were normal but he had diplopia in all fields. The disc margins were slightly blurred nasally and he had small hemorrhages about the discs. His gait was normal. There was weakness of the jaw, right facial, palatal, tongue, neck, and shoulder muscles with fasciculations noted in these groups. In addition there was atrophy of the masseters, platysmae, tongue, neck and shoulder muscles. There were a few fasciculations of the triceps muscles but no weakness or atrophy. The deep tendon reflexes of the arms were two to three plus bilaterally and there was greater finger stretch on the left than on the right. The abdominal reflexes were diminished bilaterally. There was no atrophy or weak- ness of the legs and the sensory examination was normal. Laboratory examinations including complete blood count, urine analysis, blood chemistries, spinal fluid, serol- ogy, chest X-ray, skull plates, and electrocardiographs were all within normal limits. The patient's neurological status remained unchanged while under observation and adequate nutrition was main- tained with tube feeding. Two months after admission a medical consultation was requested because of increasing cyanosis. At this time marked cyanosis was observed without respiratory distress. Expansion of the chest cage during ordinary breathing was minimal but with forced inspiration he was capable of a three inch chest expansion. The lungs were clear and examination of the heart was unremarkable except for an accentuated second pulmonic sound. Abdominal examination was negative. There was no peripheral edema or venous en- gorgement. The red blood count was 6.75 million with a hemoglobin of 19.4 grams and a hematocrit of 64%. Fluoroscopic examination revealed the trachea to be in the midline and the motion of the bony framework was good. There was normal radiolucency of the lung fields. The range of motion of the right diaphragm was one 762
Transcript of viz.,...Diffusional, viz., pulmonary scleroderma. The two cases to be presented demonstrate...

CARDIAC FAILURE SECONDARYTO INEFFECTIVE BELLOWSACTION OF THE CHESTCAGE
By JAMESA. FELTMAN, WALTERNEWMAN,ARTHURSCHWARTZ,DANIEL J. STONE, ANDFRANCIS J. LOVELOCK
(From the Cardio-Pulmonary Laboratory and the Medical Service at the Bronx VeteransAdministration Hospital, Bronx, N. Y.)
(Submitted for publication April 7, 1952; accepted June 13, 1952)
Baldwin, Cournand, and Richards (1) have de-scribed the following classification of pulmonaryinsufficiency:
1. Ventilatorya. Restrictive, viz., pulmonary fibrosis, ky-
phoscoliosis.b. Obstructive, viz., pulmonary emphysema.
2. Alveolar-respiratorya. Distributive, viz., pulmonary emphysema.b. Diffusional, viz., pulmonary scleroderma.
The two cases to be presented demonstrateventilatory insufficiency of the restrictive type due,in the first instance to primary neuromusculardysfunction and in the second to chronic pleuraldisease with resulting calcification and restrictionof the underlying parenchyma and diaphragm. Ofparticular interest was the development of con-gestive heart failure in both of these patients.These cases represent examples of cardiac failuresecondary to an ineffective bellows action of thechest cage without significant intrinsic pulmonarydisease.
CASE REPORTS
Case 1
This 34 year old white male was well until 1945 whenhe noted the gradual onset of weakness of the right sideof the face. A few months later he began to have bilateraljaw weakness, and difficulty in swallowing food withregurgitation of fluid through the nose. In 1947 therewas onset of occasional diplopia. He was admitted tothis hospital on three different occasions between Janu-ary 1947 and November 1948 and on all these admissionsshowed signs and symptoms of bulbar involvement.These signs and symptoms persisted with little changeexcept for development of dysarthria. In November 1949he complained of difficulty in maintaining erect postureand he was readmitted for his fourth and final admission.At this time the patient stated he had noted dyspnea onexertion for the preceding one and a half years and dur-ing the month before admission, cyanosis of the lips hadbecome apparent.
On admission the patient appeared chronically illwithout respiratory distress but with cyanosis of the lips,nailbeds, and skin. There was a marked dysarthria. Hischest cage moved very little on normal respiration buthe had good expansion with effort and could clear mostof his cyanosis with forced breathing. The heart wasnot remarkable on examination except for a markedly ac-centuated P2. The lungs were clear to percussion andauscultation. The abdominal examination was withinnormal limits. Neurological examination revealed theright pupil to be larger than the left, and both reactedsluggishly to light and accommodation. The externalocular movements were normal but he had diplopia in allfields. The disc margins were slightly blurred nasallyand he had small hemorrhages about the discs. His gaitwas normal. There was weakness of the jaw, rightfacial, palatal, tongue, neck, and shoulder muscles withfasciculations noted in these groups. In addition there wasatrophy of the masseters, platysmae, tongue, neck andshoulder muscles. There were a few fasciculations of thetriceps muscles but no weakness or atrophy. The deeptendon reflexes of the arms were two to three plusbilaterally and there was greater finger stretch on theleft than on the right. The abdominal reflexes werediminished bilaterally. There was no atrophy or weak-ness of the legs and the sensory examination was normal.
Laboratory examinations including complete bloodcount, urine analysis, blood chemistries, spinal fluid, serol-ogy, chest X-ray, skull plates, and electrocardiographswere all within normal limits.
The patient's neurological status remained unchangedwhile under observation and adequate nutrition was main-tained with tube feeding. Two months after admission amedical consultation was requested because of increasingcyanosis. At this time marked cyanosis was observedwithout respiratory distress. Expansion of the chestcage during ordinary breathing was minimal but withforced inspiration he was capable of a three inch chestexpansion. The lungs were clear and examination ofthe heart was unremarkable except for an accentuatedsecond pulmonic sound. Abdominal examination wasnegative. There was no peripheral edema or venous en-
gorgement. The red blood count was 6.75 million with a
hemoglobin of 19.4 grams and a hematocrit of 64%.Fluoroscopic examination revealed the trachea to be inthe midline and the motion of the bony framework was
good. There was normal radiolucency of the lung fields.The range of motion of the right diaphragm was one
762

CARDIAC FAILURE AND INEFFECTIVE BELLOWSACTION
inch; that of the left diaphragm one-half inch. Therewas no diaphragmatic paralysis. The lung fields wereclear. Examination of the heart revealed slight left ven-tricular rounding, moderate right ventricular enlargement,and marked enlargement of the pulmonary conus. Theelectrocardiograph demonstrated evidence of right ven-tricular hypertrophy. Venous pressure was 180 mm. ofcitrate and decholin circulation time 28 seconds. Becauseof these findings, the patient was digitalized. There wasa five pound diuresis, and the venous pressure and circu-lation time returned to normal. Following this the pa-tient was studied in the cardiopulmonary laboratory(Table I). Early in June 1950, despite vigorous therapy,he went into intractable congestive heart failure anddied.
Autopsy examination revealed the following pertinentfindings. There was clubbing of the fingers and moderatesubcutaneous edema. The lungs showed a moderate de-gree of congestion with occasional scattered areas ofchronic pneumonitis in the lower lobes, probably on anaspirational basis. There was no gross or microscopicevidence of significant emphysema or fibrosis. The heart
was enlarged weighing 500 grams. The coronary arteries,myocardium, endocardium and valvular leaflets were nor-mal. The right ventricular chamber was dilated and theright ventricular wall hypertrophied measuring 1 cm. inthickness. The pulmonic valve ring was dilated meas-uring 10 cm. in circumference. The right auricle wasslightly dilated as was the tricuspid valve ring whichmeasured 14.5 cm. in circumference. The left atrium andmitral valve were normal. The left ventricular wall wasslightly hypertrophied to approximately 1.5 cm. in thick-ness. The aortic valve was normal in size and appear-ance. The pulmonary arteries showed mild atheroscleroticchanges. The gastrointestinal tract, biliary system, geni-tourinary tract, spleen, pancreas, adrenals, thyroid, lymphnodes, and skeletal system were all normal. There waschronic passive congestion of the liver, spleen and kid-neys. The liver weighed 1,750 grams and the spleen 220grams. The central nervous system, including brain andspinal cord, showed no distinctive lesions on multiplesections with different staining techniques including Ma-hon's. The peripheral nerves were normal.
Despite the negative autopsy findings, it was the opin-
xi. ItlM!S OF PUMOIARYMOUCTIONSTuDIRs I cAsz 1 2 a
Case 1
Lung Toloes Prdz1te1 ObservedVital Capacity(lying) c. 477022c.
Residual air, c.c. 1180 1005
Total capacity, c.c. 5950 3680
II.A. % 20 .27?.C.
ALv. N2 % (2.5 1.77
II. maximumm BreathingCapacity, L/Sin 119 38
III. Basal Ventilation/ain 3.30 3.33L/M2 B.S.A. ± 0.65
IT. Reepiratory G&aSO 12Arterial Blood
CO2 contentvol.. %
02 saturation %
PCO2 -. Eg.
p02H RgC
ht
48.5± 4.5
9612
40
96
7.4
V. Calculated Alveolar-Arterial Gradient on
Room Air 0 to 12 Norma
763
Rai kser.
64.4 72.4
73.3 65.5
84
49
7.2 (aemc.)

J. A. FELTMAN, W. NEWMAN,A. SCHWARTZ,D. J. STONE, AND F. J. LOVELOCK
ZTmL (Continued)
I, Lung Volmes
vital Capacity(Wng) c.0.Residal air, 0.c.Total Capacity, c. c.
R.: %Al v. i,2
II. Xazi BreathingCapacity L/nin.
3800
12205020
24
9000
880
18900
42
less than 2.5 lose than 2.5
90 380
OResults inaccurate becaeso of poor cooperation.
II.
Ventilation/ai.L/X2 B.S.A.
02 Intake In cc/K2B.S.A.
02 Remove in ccfLventilation
IV. Respiratory Gases inArterial Blood
ResPgeiets babed
3.20+ 0.65 6.4
129i 13
46.8t 7.1
161
8.70 12.*±
480+ 74 390
54.8 31.8± 6.2
002 content vols. %
02 saturation %pC02 M. Rg.P02 M. Rg.PR
RestPredltce abedn2
48.5 58.34.5
96t2 92.3
40 69
95 66
7.4
Alv. p02 _. HgArt. p02 -. Hg.
Room Art. p002 mm. Hg.air Alveolar-arterial gradientbreathing Dead space l.
Dead space % tidal airph calculated
AMv. p02Art. p02Alveolar-arterial gradientDead space ml.Dead space tidal sirph calcuated
ion of the neurological service that this patient's clinicalpicture could best be explained by ascribing the changes toamyotrophic lateral sclerosis.
Case 2
A 56 year old Puerto Rican male was admitted to thehospital because of increased dyspnea and orthopnea forthree weeks, and a non-productive cough for a fewdays. In 1921 and 1925 the patient had "pleurisy." In1936 he was told that he had "calcifications in his chest."In 1946 he was refused employment because of an ab-normal chest X-ray. Three years before admission therewas an episode of wheezing and undue shortness of breathwhich lasted a few days and then ceased spontaneously.During the two years prior to admission there was ankleedema. Because of the increase in dyspnea the patientsought hospitalization.
At the time of admission the patient's temperature was
1030 F., pulse 116. He was orthopneic and cyanotic.Examination of the chest disclosed poor expansion bi-laterally with more limitation on the right. There was
dullness over the lower half of the right lung field and atthe left base with diminished breath sounds and tactile fre-mitus over these areas. There were moist rales at theleft base with occasional wheezing over the right upper
lung field. The second pulmonic sound was accentuated.The liver edge was two finger breadths below the rightcostal margin, and tender. There was two plus pretibialedema.
The blood count on admission revealed a normal whiteblood count and differential. The red blood count was
6.0 million, hemoglobin 18.5 grams, and the hematocritwas 62%. An X-ray of the chest disclosed extensive cal-cification surrounding the lower two-thirds of both lung
T.
Recovery54.7
84.6
breathing(29.25%)
7066694
19356
7.27
118106
13178
557.27
764

CARDIAC FAILURE AND INEFFECTIVE BELLOWSACTION 765
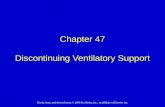
FIG. 1A. CASE 2 DEMONSTRATINGCALCIFIED PLEURITIS AND CARDIAC ENLARGMENTBEFORETHERAPYFIG. 1B. AFrER THERAPYDEMONSTRATINGRETURNOF HEART SIZE TO NORMAL
fields and an increase in the transverse diameter of theheart (Figure 1A). An electrocardiogram was con-sistent with right ventricular hypertrophy. The venouspressure on admission was 280 mm. of citrate.
The patient was treated with penicillin and bed rest forthe first five days with no change in the clinical course.
On the fifth hospital day the patient was digitalized,placed on a low salt diet, and oxygen was administered in-termittently by mask. Later that day he became semi-stuporous. He was placed in an oxygen tent and givenmercurial diuretics. Shortly thereafter he became coma-tose although the cyanosis diminished. The stupor per-
TABLE II
P02 02 Capac. 02 Sat. pCO2 CO2 count.m. Eg. Vole. % % mm. EC. Vol. ,%
6/1/51Room airimmediately afteroxygen tent withnarcosis
6/4/51Breathing roomair
6/6/51Respirator withnasal oxygen
6/12/51Respirator withnasal oxygen
26 22.2
55 20.1
98 19.7
147* 20.2
39.2
87.6
98.9
96 59.3
57 62.4
68 61.1
100 51 59.4
Inaccurate. above range of applicability of bubble technic.
ph
7.14
7.40
7.30
7.42
765

J. A. FELTMAN, W. NEWMAN,A. SCHWARTZ,D. J. STONE, AND F. J. LOVELOCK
sisted until the patient was removed from the oxygen tentfor routine' care the following day. Arterial blood studiessuggested that carbon dioxide narcosis was responsible forthe coma (Table II). In order to combat the CO2 nar-cosis, artificial respiration with the Pneumatic BalanceResuscitator was initiated. Within a short time the patientwas more alert and there was no cyanosis. A phlebotomywas also performed. Artificial respiration was discontin-ued later that day, and the patient maintained satisfactoryclinical progress for the next 48 hours. The blood gasstudies reflected this improvement. Although the pa-tient had improved considerably, oxygen therapy wasagain administered because of the anoxia disclosed by thearterial blood studies. Artificial respiration was reinsti-tuted by means of a Drinker-Collins respirator, and oxy-gen was administered by nasal catheter. This was con-tinued for one week along with penicillin, bronchodilatorsand continued digitalis therapy, phlebotomy, low salt diet,and occasional mercurial diuretics. At the end of thisperiod the patient was relatively asymptomatic and thesigns of congestive heart failure had disappeared. Fol-low-up X-rays disclosed that the heart size had returnedto normal (Figure IB). Fluoroscopy revealed the pleuralcalcifications, no motion of the rib cage, and restrictionof diaphragmatic motion. Complete pulmonary functionstudies were performed one month after recovery fromthe acute episode (Table I). Three months after dis-charge the patient was seen in the Follow-up Clinic. Hewas asymptomatic and capable of climbing two flights ofstairs. Digitalis therapy and a low salt diet were con-tinued.
METHODS
The measurement of residual air volume was done us-ing an open circuit method in which the nitrogen of thelungs is washed out by continuous inhalation of pureoxygen and collected over a period of seven minutes. Anindex of intrapulmonary mixing was obtained by sam-pling of the alveolar air at the end of this period (1).
The measurements of lung volumes and maximumbreathing capacity were obtained using the spirographictechnique (1).
Arterial blood samples were obtained from the brachialartery using an indwelling Cournand-type needle. Theblood was collected by the technique described by Riley,Proemmel and Franke (2), using heparin to preventclotting and a small globule of mercury in the syringe tofacilitate mixing. The oxygen content and capacity andthe carbon dioxide content were determined on duplicatesamples using the Van Slyke-Neill apparatus (3). Allsamples checked within 0.2 volume %.
The arterial blood tensions of oxygen and of carbondioxide were determined directly in mm. of mercury, us-ing the direct method of Riley (2). Duplicate measure-ments were made using two Roughton-Scholander syr-inges, and all samples checked within 2 mm. of mercury.Expired air samples were collected in duplicate simul-taneously with the blood specimens. Oxygen intake andcarbon dioxide output were calculated from the percentage
of oxygen and carbon dioxide found in these expired airsamples, as determined in a Scholander gas analyzer (4).The duplicate measurements checked within 0.04%.
Arterial blood samples and expired air were collectedunder basal conditions with the patients breathing roomair, high, and low oxygen concentrations, each for twentyminute periods when indicated. Finally oxygen saturationwas determined after one minute of standard exercise andthe expired gas during the exercise was collected in aDouglas bag and analyzed. During the five minute re-covery period the expired air was collected and analyzed.The expired air, except during exercise, was collected inthe Tissot apparatus and the spirogram attached per-mitted calculation of the respiratory rate and tidal airunder the various conditions. The alveolar-arterial gra-dients were calculated from the data obtained accordingto the method of Lilienthal, Riley, Proemmel and Franke(5).
Values for pH were calculated from line charts of theHenderson-Hasselbalch equation (6).
COMMENTS
Case 1 disclosed a markedly reduced vital ca-pacity, total capacity and maximum breathing ca-pacity. The residual air and alveolar nitrogenafter breathing pure oxygen for seven minutes werenormal. The ratio of residual air to total capacitywas slightly but not significantly increased and re-flected the decrease in total capacity. Thus the lungvolume studies revealed principally a reduction invital capacity which was due primarily to themarked limitation of diaphragmatic excursion.The normal residual air and alveolar nitrogen indi-cated the absence of any significant degree ofemphysema. During the performance of the maxi-mumbreathing capacity an element of fatigue wasapparent in that the patient was unable to maintainthe depth or speed of ventilation uniformly for the12 second interval. This was probably due tomuscle anoxia and weakness associated withchronic disease. In addition, a satisfactory depthof respiration could not be established presumablyas a result of impaired diaphragmatic excursion.Finally an adequate speed of ventilation could notbe established because of muscular weakness andpoor coordination. The total basal ventilation wasnormal but the effective alveolar ventilation wasgrossly inadequate as reflected by the high ar-terial pCO2. Despite the presence of strong stimulifor hyperventilation (high arterial pCO2 and lowarterial pH and PO2) the resting ventilation wasnormal. This would suggest decreased sensitivity
766

CARDIAC FAILURE AND INEFFECTIVE BELLOWSACTION
of the respiratory center to chemical stimuli. Inaddition, the polycythemia may have been an ag-gravating factor (7). The inadequate alveolarventilation resulted from the fact that too large aproportion of the total ventilation was wasted inventilating the dead space as a result of the shal-low breathing. It is of interest to note that thispatient's resting ventilation was less than 10% ofhis maximum breathing capacity which would ac-count for the absence of dyspnea at rest in thepresence of severe anoxemia (1). The arterialCO2 content was elevated but not commensuratewith the pCO2 so that the pH was decreased. Thearterial PO2 and oxygen saturation were markedlyreduced and the latter decreased even further afterstandard exercise. These changes were due solelyto inadequate alveolar ventilation. The calculatedalveolar-arterial gradient on room air, assumingan RQof 0.8 to 0.9, was normal. Because of thepatient's muscle weakness he was unable to keepa mouthpiece in place for prolonged periods of time,and the RQof 0.8 to 0.9 was therefore assumed.
Case 2 demonstrated marked decrease in all lungvolumes. The observed figures for the vital ca-pacity, total capacity and maximum breathing ca-pacity probably were inaccurate since the patientdid not appear to cooperate fully during the per-formance of these tests. The ratio of residualair to total capacity was high due to the fact thatthe total capacity reduction was out of proportionto that of the residual air. The maximum breath-ing capacity was reduced. These changes wereprimarily due to the chronic constrictive calcificpleuritis which interfered with the bellows actionof the chest cage. The high ratio of residual air tototal capacity was not a reflection of emphysemasince the alveolar nitrogen was less than 2.5%.The tracings showed no graphic evidence of a pro-longed expiratory phase. There was no evidencefor impairment of gas exchange. Ventilation stud-ies demonstrated that the patient was hyperven-tilating at rest and during exercise, presumablyas a response to the high arterial pCO2and anoxia.This patient's calcific constrictive pleuritis mark-edly reduced his effective alveolar ventilation.Thus, his respirations were rapid but shallow andprobably did little more than wash out the deadspace. This caused a high arterial pCO2 and CO2content and anoxia. There was no indication ofsignificant abnormalities of gas exchange since
the gradient studies were within normal limits(5, 8).
The patient was admitted with an acute pul-monary infection. This was enough to accentu-ate the anoxia and thereby increase the pulmonaryhypertension and precipitate cardiac failure. Hewas treated with antibiotics, bronchodilators, digi-talis, phlebotomy, and oxygen. The use of con-tinuous oxygen therapy in patients with chronicanoxia has been known to produce CO2 narcosis(9-13) and this patient was a vivid example ofthis phenomenon (Table II). The PneumaticBalance Resuscitator probably represented a lifesaving procedure at this time. The use of therespirator permitted continuous use of oxygentherapy without the threat of the return of CO2narcosis. This will be discussed in another paper(14).
DISCUSSION
Wehave presented two patients whose primarydifficulty was a defective bellows action of the chestcage. In the first case this was due to disease ofthe neuromuscular system. In the second case thepatient had extensive calcific pleuritis of undeter-mined etiology which interfered with the mobilityof the thoracic wall. In the latter instance thereundoubtedly existed some degree of pulmonary
DWMNETBN.LS AdCfO 01 53 CENT CAUE
Decrease In Fermie In Hovital cepacity breathing paoitt
_RAeduealveolar ventilation
Iceased arterial pCO2Vith re iratory acidoets
Decresed etivity Arterial offgesof repertory center n--- rationto chemical stimuli
P0olcythesia Myocardial hypoxia
Pulmonaryhypertension
Ventricular wyrtropby.dilatation ar failure
FIG. 2. SEQUENCEOF EVENTSWHICHMAYHAVEOc-CURRM IN Two CASES WITH AN INEFFECTIVE BmOwsACTION OF THE CHESTCAGE
767

J. A. FELTMAN, W. NEWMAN,A. SCHWARTZ,D. J. STONE, AND F. J. LOVELOCK
disease, probably on a tuberculous basis. In viewof the entire clinical picture and pulmonary func-tion studies, we are inclined to believe that pa-renchymal disease contributed little if any to theabnormalities observed.
In both these patients (Figure 2) the de-fective bellows action resulted in a reduction invital capacity, maximum breathing capacity, andineffective alveolar ventilation manifested by ahigh arterial pCO2 and arterial oxygen unsatura-tion. The anoxia was probably a stimulus for theproduction of the polycythemia (15). The hyper-capnia, anoxia, and polycythemia all representedfactors favoring medullary center damage whichthese patients demonstrated. There is evidenceto indicate that both polycythemia (7) and anoxia(16, 17) may lead to pulmonary hypertension andeventually cardiac failure which these patientsalso manifested. In both these patients the normalchanges in circulatory dynamics associated withthe mechanics of respiration were undoubtedlyaltered (18). No objective studies were made toevaluate these factors.
Finally, it is of interest to correlate the situa-tion in primary polycythemia with the sequence ofevents in these two cases. In the former instancethere is polycythemia which we believe may leadto hypoxemia (7). In the latter we have ineffec-tive bellows action of the chest cage leading tohypoxemia and secondary polycythemia. Evi-dently, once polycythemia and hypoxemia haveoccurred, the subsequent tendency to develop con-gestive heart failure probably depends upon simi-lar mechanisms, viz., myocardial hypoxia and pul-monary hypertension.
SUMMARY
Two cases of ventilatory insufficiency of therestrictive type resulting in congestive heart fail-ure have been presented. There was no evidenceof significant intrinsic pulmonary disease. Thesequence of events leading to heart failure arediscussed.
ACKNOWLEDGMENTS
The authors wish to acknowledge their appreciation toDr. Richard L Riley for his many helpful comments inthe preparation of this manuscript, and to Mrs. BlancheDevlin for her invaluable aid in the laboratory procedures.
REFERENCES
1. Baldwin, E. de F., Cournand, A., and Richards, D.W., Jr., Pulmonary insufficiency. I. Physiologicalclassification, clinical methods of analysis, stand-ard values in normal subjects. Medicine, 1948,27, 243.
2. Riley, R. L., Proemmel, D. D., and Franke, R. E., Adirect method for determination of oxygen and car-bon dioxide tensions in blood. J. Biol. Chem., 1945,161, 621.
3. Van Slyke, D. D., and Neill, J. M., The determina-tion of gases in blood and other solutions by vac-uum extraction and manometric measurements. I.J. Biol. Chem., 1924, 61, 523.
4. Scholander, P. F., Analyzer for accurate estimationof respiratory gases in one-half cubic centimetersamples. J. Biol. Chem., 1947, 167, 235.
5. Lilienthal, J. L., Jr., Riley, R. L., Proemmel, D. D.,and Franke, R. E., An experimental analysis in manof the oxygen pressure gradient from alveolar airto arterial blood during rest and exercise at sealevel and altitude. Am. J. Physiol., 1946, 147, 199.
6. Van Slyke, D. D., and Sendroy, J., Jr., Studies of gasand electrolyte equilibria in blood. XV. Linecharts for graphic calculations by the Henderson-Hasselbalch equation, and for calculating plasmacarbon dioxide content from whole blood con-tent. J. Biol. Chem., 1928, 79, 781.
7. Newman, W., Feltman, J. A., and Devlin, B., Pul-monary function studies in polycythemia vera. Am.J. Med., 1951, 11, 706.
8. Rahn, H., Effects of unequal blood flow and ventila-tion upon the alveolar-arterial gradient. FederationProc., 1949, 8, 129.
9. Barach, A. L., and Richards, D. W., Jr., Effects oftreatment with oxygen in cardiac failure. Arch.Int. Med., 1931, 48, 325.
10. Barach, A. L., Effect of low and high oxygen ten-sions on mental functioning. J. Aviation Med.,1941, 12, 30.
11. Comroe, J. H., Jr., Bahnson, E. R., and Coates, E. O.,Jr., Mental changes occurring in chronically an-oxemic patients during oxygen. therapy. J. A.M. A., 1950, 143, 1044.
12. Davies, C. E., and Mackinnon, J., Neurological ef-fects of oxygen in chronic cor pulmonale. Lancet,1949, 2, 883.
13. Donald, K., Neurological effects of oxygen. Lancet,1949, 2, 1056.
14. Stone, D. J., Schwartz, A., Newman, W., Feltman,J. A., and Lovelock, F. J., The precipitation bypulmonary infection of anoxia, cardiac failure, andrespiratory acidosis: pathogenesis and treatment.Am. J. Med., to be published.
768

CARDIAC FAILURE AND INEFFECTIVE BELLOWSACTION
15. Viault, Sur la quantity d'oxygene contenue dans lesang des animaux des hauts plateaux de l'Ameriquedu Sud. Compt. rend. Acad. Sc., 1891, 112, 295.
16. Motley, H. L., Cournand, A., Werko, L., Himmel-stein, A., and Dresdale, D., The influence of shortperiods of induced acute anoxia upon pulmonaryartery pressures in man. Am. J. Physiol., 1947,150, 315.
17. Westcott, R. N., Fowler, N. O., Scott, R. C., Hauen-stein, V. D., and McGuire, J., Anoxia and humanpulmonary vascular resistance. J. Clin. Invest.,1951, 30, 957.
18. Lawson, H. D., Bloomfield, R. A., and Cournand, A.,The influence of the respiration on the circulationin man. Am. J. Med., 1946, 1, 315.
769