
Virus 2 and Emerging Infectious Diseases BIOM 1005 1905 March 2015.Pptv2
51
Emerging Infectious Diseases (II) BIOM 1005 BIOM1905
-
Upload
fahimrazmandeh -
Category
Documents
-
view
6 -
download
0
description
virus
Transcript of Virus 2 and Emerging Infectious Diseases BIOM 1005 1905 March 2015.Pptv2
Emerging Infectious Diseases(II)
BIOM 1005 BIOM1905

Learning Outcomes
To be able to give definition of emerging infectious disease
To provide named examples of recent viral emerging infectious diseases and their aetiological agents
To understand viral detection methods available including their advantages/disadvantages and their application in detecting viral disease
To understand treatment and vaccination methods available for use in viral disease
Emerging infectious diseases
Definition of an emerging infectious disease“emerging infections are those whose incidence in humans has increased within last 2 decades or threatens to increase in the near future – emergence may be due to spread of a new agent, or recognition of an infection present in population but has gone undetected, or realization that an established disease has an infectious origin”Emergence may also be used to describe the reappearance (or re-emergence) of a known infection after a decline in incidence

Emerging infectious diseases
Bacteria and parasites
TB MDR TB, MRSA, VRE (vancomycin resistant
enterococci), Multi-drug resistant Gram negative bacteria (such as Klebsiella, Acinetobacter, NDM-1) Ecoli0157, Ecoli0104
Zoonotic infections (animal or mosquito vectors for transmission)
Emerging infectious diseases
Zoonotic infections (animal or mosquito vectors for transmission)
Plasmodium spp Malaria (drug resistant protozoan)Campylobacter spp (bacterium)Cyclospora spp (travel-associated protozoan)Cryptosporidium spp (protozoan)Bacillus anthracis (bioterrorism)

Emerging viral infectious diseases
Avian Influenza (“Bird Flu”)Haemorrhagic viruses - Ebola, Lassa, DengueHepatitisHIV (Human Immunodeficiency Virus)Prion Diseases (Proteinaceous infectious particle PrP)
vCjD, BSE(bovine spongiform encephalitis)SARS (Severe Acute Respiratory Syndrome)West Nile VirusSwine Flu Virus

Emerging infectious diseasesTaylor et al (2001) number of human pathogen species (1407)

Influenza Virus
Influenza A and B (Influenza A has been responsible for pandemics (Spanish Flu) in past and has caused outbreaks every 2/3 years
Why?
Neuraminidase and Haemagglutinin (glycoproteins)
Influenza VirusInfluenza viruses have 3 main antigens
“S” or soluble antigen (protein in the ribonucleoprotein core of virus particle) all Influenza A viruses share common S antigen
Haemagglutinin – contained in radially-projecting spikes in the virus envelope, it is strain specific(15 subtypes) involved in virus attachment/penetration and membrane fusion
Neuraminidase – enzyme contained in virus envelope (9 subtypes) – it facilitates release of virions (cleaving sialic acid residues)
Influenza viruses are characterised into subtypes according to antigens of haemagglutinin (H) and neuraminidase (N) on the viral surface H5N1 subtype

Influenza Virus
Haemagglutinin and Neuraminidase
Influenza Virus
TreatmentAnnual Vaccination programme for those at risk – elderly, asthma, heart or respiratory complaints
Vaccine composition changes because virus mutates – WHO recommends 2006/2007 it should contain
A/New Caledonia/20/99 (H1N1)-like virusA/Wisconsin/67/2005 (H3/N2)-like virusB/Malaysia/2506/2004-like virus

Successful entrepreneur
Started his business 60 years ago with 20 eggs and second hand incubator
2008 company profits plunged….


Avian Influenza
Outbreak in UK
“Bernard Matthews” Turkey farm Holton, Suffolk (February 2007)
Importation into UK of turkey meat from a slaughterhouse 30 miles from the source of the Hungarian outbreak of avian flu Possibility that meat became cross-contaminated in the slaughterhouse with the virus → UK → into sheds housing live birds

Avian Influenza
Antiviral drugs offered to 480 people 310 of whom also received seasonal flu vaccination (HPA 2007)
No evidence of any of workers becoming infected with avian influenza
.

Avian Influenza
There were serious biosecurity shortfalls Bernard Matthews turkey plant
Government investigation found
holes in turkey sheds where birds, rats and mice could get in and spread the H5N1
leaking roofs, and uncovered bins from which seagulls were seen carrying off meat waste
Avian Influenza
71 birds died of H5N1 avian influenza
159,000 turkeys were slaughtered as a precaution
400 redundancies due to 40% drop in sales

Avian Influenza
Avian influenza is disease of birdsCaused by influenza viruses closely related to human influenza virusesTransmission to humans in close contact with poultry or other birdsOutbreak 175 cases of human disease (96 people have died)Possible pandemic if bird→human transmission becomes human→human (no herd immunity)Highly pathogenic H5N1 subtype

Avian Influenza
Transmission
Respiratory aerosol droplets, close contact
Outbreak originated China → Indonesia → Iraq → Africa (Nigeria), Turkey → Europe (Italy, Germany, France)

Avian Influenza
Control MeasuresSurveillance of birds (migratory/wild/poultry)Bird importation – quarantine measuresFrance - vaccination of poultry flocks
Treatment“Tamiflu” vaccine antiviral (poultry workers)Problem with vaccine is until pandemic starts do not know which strain therefore cannot predict which vaccine composition will be most useful

SARS VirusSARS (Severe Acute Respiratory Syndrome)
Originally this was a disease of unknown aetiology described in patients (Asia, North America, Europe)
March 2003 WHO issued a global health alert for authorities to be aware of a new atypical pneumonia called SARS which had been reported in SE Asia
Origin of disease thought to be in Guangdong Province in China
Between March and July 2003 >8,400 probable cases of SARS were reported in 32 countries
Most of patients 25-70yrs old (few cases in children) – close family members and hospital workers caring SARS patients

SARS Virus
64 yr old medical doctor from GuangDong Province China staying at Metropole Hotel Hong Kong develops disease – contact tracing by public health officials found he was index case which resulted in 94 cases of disease occurring
Spread by close contact
Disease spread rapidly by ease/frequency of international travel

SARS Virus
Cause of SARS now known to be a SARS coronavirus (SARS CoV) a new member of the coronavirus family
This virus family includes viruses which cause the common cold
At present no vaccine or specific treatment
Public Health systems continue to be vigilant and prepare for possible re-emergence of SARS (use of quarantine measures)
Since the outbreak in 2003 diagnostic methods have been developed for testing of virus – using PCR and serology

SARS Virus
Current Public Health Approach to Prevention and Control of SARS
Surveillance: case detection, verification and reportingCase management: isolation, infection control, treatment
and follow upManagement of contactsInformation education and travel adviceLab diagnosisContingency planningInternational collaborations WHO , CDC, HPAResearch and development

West Nile Virus (WNV)RNA virus (Flaviviridae)
Originally WNV found tropical/subtropical areas – arbovirus (arthropod borne)
First isolated in 1937 in West Nile district ofUganda
Host = birds, vector= mosquitoes
Causes meningoencephalitis
Late 1990s 62 people infected (7 die) of WNV in New York, USA
Since then WNV spread as far south as Florida and as far north as Canada → ?UK

West Nile Virus (WNV)
WNV Lifecycle - Transmission
West Nile Virus (WNV)Cause
Migrating wild birdsClimate changeUrbanisation
ControlSurveillance (testing sick/dead birds)No vaccine as yet although some are under developmentEducation regarding WNV transmissionElimination/reduction of suitable habitats for mosquitoesUse of larvicides – vector control
Swine FluSwine Flu
H1N1 'swine flu' pandemic virus emerged in Mexico (April 2009)
H1N1 spread around the world causing mild/asymptomatic disease in the majority of cases but severe illness and death in a small proportion of cases, particularly in more vulnerable groups In August 2010 WHO officially declared the H1N1(2009) pandemic over

Swine FluSwine Flu
EpidemiologyEpidemiology
First reported case in UK April 2009
Two waves of pandemic activity
First pandemic wave peaked July2009 - most affected areas were the West Midlands, London and central Scotland
Second pandemic wave peaked October 2009 (return to school)

Swine FluSwine Flu
Source HPA Epidemiological Report of Pandemic H1N1 (2010)Source HPA Epidemiological Report of Pandemic H1N1 (2010)
Swine Flu in UKSwine Flu in UK
EpidemiologyEpidemiology
474 deaths in UK (359 England)474 deaths in UK (359 England)
Most affected were <65yearsMost affected were <65years
Especially at risk from 6months to <65yrs those with underlying Especially at risk from 6months to <65yrs those with underlying chronic respiratory, neurological or heart condition were 10xs chronic respiratory, neurological or heart condition were 10xs more at risk of being hospitalisedmore at risk of being hospitalised Death was most likely in those with chronic neurological, chronic Death was most likely in those with chronic neurological, chronic liver and immunosuppression conditionsliver and immunosuppression conditions
Virus Detection MethodsElectron microscopyTissue Culture methodsImmunofluorescenceComplement fixationELISAMolecular methods PCR

Virus Detection Methods
Figure to show: Viral Shedding and Antibody Response in response to Avian Influenza infection
Electron Microscopy Electron Microscope
Expensive to run/maintain EM
Requires highly skilled staff
Labour intensive
Fewer clinical laboratories now use EM for confirming presence of virus in patient samples
Tissue culture methods – Gold Standard for viral detection
Viruses are obligate intracellular parasites requiring metabolically active cells to support their replication
All tissue cell cultures are available commercially – consisting of either
single layers of cells (monolayers) of metabolically active cells which adhere to either side of glass tube or
surface of a cover slip contained in a flat-bottomed shell vial

Tissue culture methods
Viral tissue culture mediaEarl’s or Hank’s medium (balanced salt solution)Eagle’s medium (minimum essential medium)Foetal calf serum

Tissue culture methods
Viruses which may be isolated include
Adenoviruses Cytomegalovirus (CMV) Echoviruses Enteroviruses, Herpes Simplex Virus (HSV)Influenza A & B Respiratory Syncytial Virus (RSV) Varicella zoster virus (VZV)

Tissue culture methods
AdvantagesIsolate viruses from patient samples Observation of specific cytopathic effects of viruses on tissue
culture cells using ordinary inverted microscope e.g. haemadsorption effects seen with influenza viruses (where added erythrocytes adhere to surface of infected cells)
Perform further confirmatory tests on these viral cultures such as immunofluorescence to confirm identity of virus
DisadvantagesRequire training and skilled staff to produce tissue culture media
free from bacterial and fungal contaminationRequire skilled virologist to examine the tissue culture cells and
ascertain presence of particular virusSome viruses may be slow growing (few weeks to grow)_Every 1-2 weeks need to change the viral tissue culture medium
in the tubes to ensure optimum growth of virus and cells – time consuming/problem of bacterial contamination

Use of Immunofluorescence (IF)
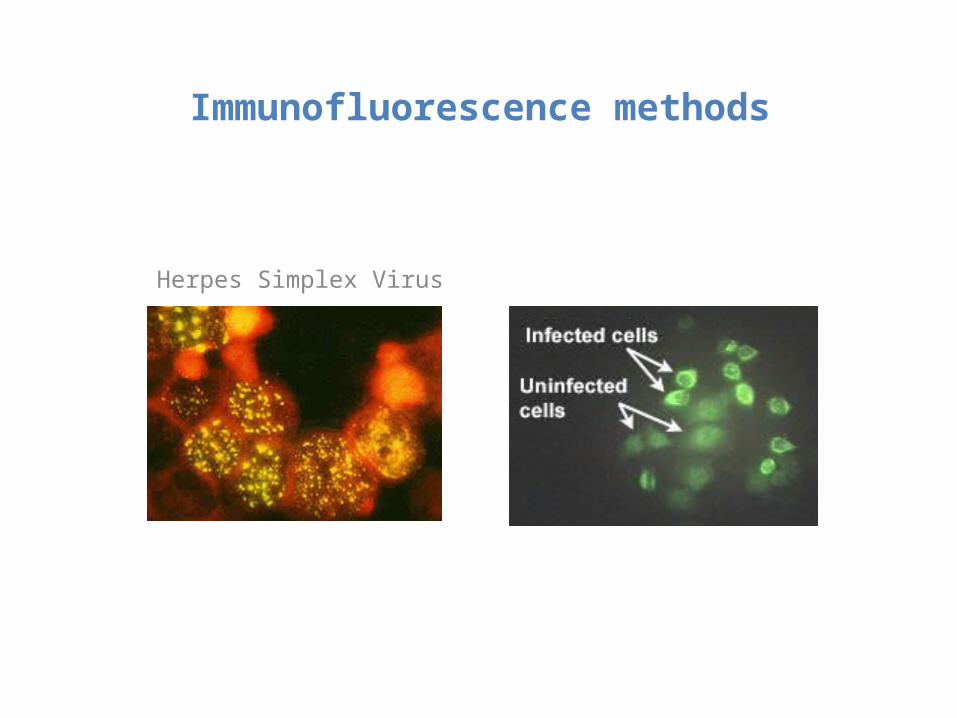
Virus antigen present in patient sample may be stained on a microscope slide using monoclonal viral antibody (tagged with a fluorescent dye-fluorescein) which recognises viral antigen – available commercially
Direct IF or Indirect IF may be used
IF demonstrates good specificity and sensitivity and is reasonably cheap howeverRequire skilled staff to interpret microscope slides, fluorescence microscope
Immunofluorescence methods
Viruses which may be diagnosed by immunofluorescence includes following
Adenoviruses Cytomegalovirus (CMV) Enteroviruses, Herpes Simplex Virus (HSV)Influenza A & B Respiratory Syncytial Virus (RSV)
Immunofluorescence methods
Herpes Simplex Virus

Serology
Detection of viral antibody in patient sera
Commercial kits available → Hepatitis, HIV testing amongst others
Advantages – automated analysers available (such as VIDAS) can process large numbers of patient samples quickly
Disadvantages – ££ cost of analysers/reagents

ELISA (Enzyme Linked Immunosorbent Assay)
Detection of viral antigen or antibody from patient sample - commercial kits
An antibody is tagged with an enzyme which reacts when suitable substrate is added later → visible colour change detected by use of spectrophotometer
Advantages – reliable and good for processing large numbers of samplesDisadvantages – may be expensive

Molecular methods-PCR (polymerase chain reaction)
Piece of viral DNA/RNA is amplified so that it may be detected
Advantage – very rapid results
Disadvantage – expensive and requires “clean” environment

Treatment and ControlVaccination e.g. MMR (measles, mumps, rubella) influenza vaccine
Antiviral Agents – antibiotics which work against bacteria/fungi are no use against viruses (acyclovir – good antiviral agent)
Misuse of antibiotics to treat viral infections → antibiotic resistance

Dengue fever outbreak in Europe October 2012
•Health Protection Agency (HPA) is aware of 18 confirmed cases and 191 probable cases of dengue fever in Madeira, Portugal since early October 2012,
•By 4 November 2012 there have been 517 laboratory confirmed cases of dengue fever reported in Madeira since the outbreak began (A further 631 probable cases have been reported)
•This is the first time that dengue fever has been reported in Madeira
•Dengue is a mosquito-borne (Aedes mosquito) viral infection (Dengue fever virus) all travellers should avoid mosquito bites when visiting area
•Causes a range of clinical symptoms from a mild flu-like illness to a more serious illness including rash and bone pain “break bone fever” and can sometimes lead to severe complications/death
•The health authorities in Madeira are investigating and implementing control and prevention measures, alongside a public awareness campaign
•Dengue fever cannot be passed from person to person as infection occurs after being bitten by the Aedes mosquito carrying the virus
•Laboratory confirmation of dengue fever restricted to reference laboratories which have Containment Level 4 laboratories e.g. Porton Down

Dengue fever• Mosquito Aedes aegypti identified as resident in Portugal since 2005 (also
found in other European countries) (Aedes albopictus)• Previously dengue infections found tropical and subtropical regions
Thailand/India/S.America (affecting 50-100million a year)• DEN1 strain in Madeira (flavivirus)• Also in Croatia, Greece and France• In Greece 1927-1928 dengue outbreak (thousands affected)• No Tx (vaccine development trials)• Control - eradicate vector mosquito
Oxitechttp://www.youtube.com/watch?v=-2pO_d4HAmc
Aedes aegypti feedinghttp://www.youtube.com/watch?v=dSm-N-C7BA0&feature=related

• Aedes aegypti is also a vector of chikungunya virus (Kenya and the Comoros Islands)
Aedes aegypti also a highly effective vector of Yellow Fever virus
• Yellow Fever occurs in South America and also West, Central and East Africa, where large severe epidemics have been recorded with tens of thousands of deaths (Yellow Fever vaccine available)

Self Directed ReadingEmerging Infectious Diseases
Which microbe was responsible for outbreak in Europe which caused HUS and was blamed initially on Spanish cucumbers/tomatoes?
NDM-1 has recently emerged in UK associated with medical tourism Which microbes are involved? Why is it a problem?
Dengue fever outbreak in Portugal – how is dengue virus detected in laboratory?
Ebola virus outbreak 2014
Effects of climate change on vector-borne diseaseshttp://www.hpa.org.uk/webc/HPAwebFile/HPAweb_C/1317135969235
Summary
Emerging viral diseases and causative agents
Viral detection methods
Treatment and control of emerging diseases


















