
yeditepeanatomy1.files.wordpress.com · Web viewthe LOWER limb 05 .02. 2014 Kaan Yücel M.D., Ph.D....
29
JOINTS OF THE LOWER LIMB 05 .02. 2014
Transcript of yeditepeanatomy1.files.wordpress.com · Web viewthe LOWER limb 05 .02. 2014 Kaan Yücel M.D., Ph.D....

JOINTS OF
THE LOWER LIMB
05 .02. 2014
Kaan YücelM.D., Ph.D.
http://yeditepeanatomy1.org

Dr.Kaan Yücel http://yeditepeanatomy1.org Joints of the lower limb
2

Dr.Kaan Yücel http://yeditepeanatomy1.org Joints of the lower limb
3
The joints of the lower limb include the articulations of the pelvic girdle—lumbosacral joints, sacroiliac joints, and pubic symphysis. The remaining joints of the lower limb are the hip joints, knee joints, tibiofibular joints, ankle joints, and foot joints.
The hip joint forms the connection between the lower limb and the pelvic girdle. It is a strong and stable joint.
Synovial joint type Multiaxial ball and socket type of synovial jointArticular surfaces: The head of the femur is the ball, and the acetabulum is the socket. The round head of
the femur articulates with the cup-like acetabulum of the hip bone.Knee joint is the largest and most superficial joint. Synovial joint type hinge type; allowing flexion and
extension; however, the hinge movements are combined with gliding and rolling and with rotation about a vertical axis. Articular surfaces The articular surfaces of the knee joint are characterized by their large size and their complicated and incongruent shapes.
The tibia and fibula are connected by two joints: the tibiofibular joint and the tibiofibular syndesmosis (inferior tibiofibular) joint. In addition, an interosseous membrane joins the shafts of the two bones.
The ankle joint (talocrural articulation) is located between the distal ends of the tibia and the fibula and the superior part of the talus. The trochlea (L., pulley) is the rounded superior articular surface of the talus. The medial surface of the lateral malleolus articulates with the lateral surface of the talus.Hinge-type
The many joints of the foot involve the tarsals, metatarsals, and phalanges. The important intertarsal joints are the subtalar (talocalcaneal) joint and the transverse tarsal joint (calcaneocuboid and talonavicular joints). Inversion and eversion of the foot are the main movements involving these joints. The other intertarsal joints (e.g., intercuneiform joints) and the tarsometatarsal and intermetatarsal joints are relatively small and are so tightly joined by ligaments that only slight movement occurs between them.

Dr.Kaan Yücel http://yeditepeanatomy1.org Joints of the lower limb
The joints of the lower limb include the articulations of the pelvic girdle—lumbosacral joints, sacroiliac
joints, and pubic symphysis. The remaining joints of the lower limb are the hip joints, knee joints, tibiofibular
joints, ankle joints, and foot joints.
1. Articulation between Acetabulum & Femur
2. Distinct feature of the joint Forms the connection between the lower limb and the pelvic girdle. It is a strong
and stable joint.
3. Synovial joint type Multiaxial ball and socket type of synovial joint
4. Articular disc No.
5. Articular surfaces The head of the femur is the ball, and the acetabulum is the socket. The round head of the
femur articulates with the cup-like acetabulum of the hip bone.
The head of the femur forms approximately two thirds of a sphere. Except for the pit or fovea for the
ligament of the femoral head, all of the head is covered with articular cartilage, which is thickest over weight-
bearing areas.
The acetabulum is formed by the fusion of three bony parts. The acetabular rim and lunate surface form
approximately three quarters of a circle; the missing inferior segment of the circle is the acetabular notch.
The lip-shaped acetabular labrum (L. labrum, lip) is a fibrocartilaginous rim attached to the margin of
the acetabulum, increasing the acetabular articular area by nearly 10%. The transverse acetabular ligament, a
continuation of the acetabular labrum, bridges the acetabular notch. As a result of the height of the rim and
labrum, more than half of the femoral head fits within the acetabulum. Centrally a deep non-articular part,
called the acetabular fossa, is formed mainly by the ischium.
6. Ligaments of the hip joint
Iliofemoral ligament [body's strongest ligament]
Ischiofemoral ligamentLigament of the head of the femurPubofemoral ligamentThe hip joints are enclosed within strong joint capsules, formed of a loose external fibrous layer (fibrous
capsule) and an internal synovial membrane.
Of the three intrinsic ligaments of the joint capsule below, it is the first one that reinforces and strengthens the
joint:
Iliofemoral ligament is located anteriorly and superiorly . This strong ligament is Y-shaped . The iliofemoral
ligament attaches to the anterior inferior iliac spine and the acetabular rim proximally and the intertrochanteric 4
1. HIP JOINT

Dr.Kaan Yücel http://yeditepeanatomy1.org Joints of the lower limb
line distally. The iliofemoral ligament is body's strongest ligament and specifically prevents hyperextension of
the hip joint during standing by screwing the femoral head into the acetabulum.
Pubofemoral ligament is located anteriorly and inferiorly. It arises from the obturator crest of the pubic bone
and passes laterally and inferiorly to merge with the fibrous layer of the joint capsule. This ligament blends with
the medial part of the iliofemoral ligament and tightens during both extension and abduction of the hip joint.
The pubofemoral ligament prevents overabduction of the hip joint.
Ischiofemoral ligament lies posteriorly. It arises from the ischial part of the acetabular rim. The ischofemoral
ligament is the weakest of the three ligaments. It spirals around the femoral neck, medial to the base of the
greater trochanter.
The ligaments and periarticular muscles (the medial and lateral rotators of the thigh) play a vital role in
maintaining the structural integrity of the joint.
Ligament of the head of the femur is primarily a synovial fold conducting a blood vessel. It is weak and of little
importance in strengthening the hip joint. Its wide end attaches to the margins of the acetabular notch and the
transverse acetabular ligament; its narrow end attaches to the fovea for the ligament of the head.
7. Movements of the hip joint
The hip joint is designed for stability over a wide range of movement. Next to the glenohumeral (shoulder)
joint, it is the most movable of all joints. During standing, the entire weight of the upper body is transmitted
through the hip bones to the heads and necks of the femurs. Hip movements are flexion-extension, abduction-
adduction, medial-lateral rotation, and circumduction.
During extension of the hip joint, the fibrous layer of the joint capsule, especially the iliofemoral ligament, is
tense; therefore, the hip can usually be extended only slightly beyond the vertical except by movement of the
bony pelvis (flexion of lumbar vertebrae). From the anatomical position, the range of abduction of the hip joint
is usually greater than for adduction. About 60° of abduction is possible when the thigh is extended, and more
when it is flexed. Lateral rotation is much more powerful than medial rotation.
Figure 1. Hip joint-anterior view5

Dr.Kaan Yücel http://yeditepeanatomy1.org Joints of the lower limb
http://3dsciencepics.com/the-anterior-view-of-hip-joint
1. Articulation between Femur and tibia, femur and patella
2. Distinct feature of the joint Largest and most superficial joint
3. Synovial joint type hinge type; allowing flexion and extension; however, the hinge movements are
combined with gliding and rolling and with rotation about a vertical axis
4. Articular disc No.
5. Articular surfaces The articular surfaces of the knee joint are characterized by their large size and their
complicated and incongruent shapes. The knee joint consists of three articulations:
Two femorotibial articulations (lateral and medial) between the lateral and the medial femoral and tibial
condyles.
One intermediate femoropatellar articulation between the patella and the femur.
The fibula is not involved in the knee joint.
6. Ligaments of the knee joint
Extracapsular (external) ligaments of the knee joint
The joint capsule is strengthened by five extracapsular or capsular (intrinsic) ligaments: patellar ligament,
fibular collateral ligament, tibial collateral ligament, oblique popliteal ligament, and arcuate popliteal ligament.
They are sometimes called external ligaments to differentiate them from internal ligaments, such as the
cruciate ligaments.
1. Patellar ligament is a thick firbrous band which is the distal part of the quadriceps tendon. It passes
6
2. KNEE JOINT

Dr.Kaan Yücel http://yeditepeanatomy1.org Joints of the lower limb
passes from the apex and adjoining margins of the patella to the tibial tuberosity. It is the anterior ligament of
the knee joint.
Collateral ligaments of the knee one on each side of the joint, stabilize the hinge-like motion of the knee.
They are tense when the knee is fully extended, contributing to stability while standing. As flexion proceeds,
they become increasingly loose, permitting and limiting (serving as check ligaments for) rotation at the knee.
2. Fibular collateral ligament (FCL; lateral collateral ligament) is a strong cord-like extracapsular ligament. It
extends inferiorly from the lateral epicondyle of the femur to the lateral surface of the fibular head.
3. Tibial collateral ligament (TCL; medial collateral ligament) is a strong, flat band that extends from the
medial epicondyle of the femur to the medial condyle and the superior part of the medial surface of the tibia.
The TCL, weaker than the FCL, is more often damaged. As a result, the TCL and medial meniscus are commonly
torn during contact sports such as football.
4. Oblique popliteal ligament arises posterior to the medial tibial condyle and passes superolaterally toward
the lateral femoral condyle.
5. Arcuate popliteal ligament arises from the posterior aspect of the fibular head, and spreads over the
posterior surface of the knee joint. It strengthens the joint capsule posterolaterally.
Intraapsular (internal) ligaments of the knee joint
The intra-articular ligaments within the knee joint consist of the cruciate ligaments and menisci.
1. Cruciate ligaments (L. crux, a cross) are located in the center of the joint and cross each other obliquely, like
the letter X.
1.1. Anterior cruciate ligament (ACL) is the weaker of the two cruciate ligaments.
Where is it? It arises from the anterior intercondylar area of the tibia, just posterior to the attachment of the
medial meniscus. The ACL attaches to the medial side of the lateral condyle of the femur.
Function? It limits posterior rolling (turning and traveling) of the femoral condyles on the tibial plateau during
flexion. It also prevents posterior displacement of the femur on the tibia and hyperextension of the knee joint.
1.2. Posterior cruciate ligament (PCL) is the stronger of the two cruciate ligaments.
Where is it? It arises from the posterior intercondylar area of the tibia. It attaches to the lateral surface of the
medial condyle of the femur.
Function?The PCL limits anterior rolling of the femur on the tibial plateau during extension. It also prevents
anterior displacement of the femur on the tibia or posterior displacement of the tibia on the femur and helps
prevent hyperflexion of the knee joint. In the weight-bearing flexed knee, the PCL is the main stabilizing factor
for the femur (e.g., when walking downhill).
2. Menisci of the knee joint (G. meniskos, crescent) are crescentic plates of fibrocartilage on the articular
surface of the tibia that deepen the surface and play a role in shock absorption. Wedge shaped in transverse 7
Dr.Kaan Yücel http://yeditepeanatomy1.org Joints of the lower limb
section, the menisci are firmly attached at their ends to the intercondylar area of the tibia. Their external
margins attach to the joint capsule of the knee.
2.1. Medial meniscus is C shaped, broader posteriorly than anteriorly. Its anterior end (horn) is attached to the
anterior intercondylar area of the tibia, anterior to the attachment of the ACL. Its posterior end is attached to
the posterior intercondylar area, anterior to the attachment of the PCL. Because of its widespread attachments
laterally to the tibial intercondylar area and medially to the TCL, the medial meniscus is less mobile on the tibial
plateau than is the lateral meniscus.
2.2. Lateral meniscus is nearly circular, smaller, and more freely movable than the medial meniscus. A strong
tendinous slip, the posterior meniscofemoral ligament, joins the lateral meniscus to the PCL and the medial
femoral condyle.
The coronary ligaments are portions of the joint capsule extending between the margins of the menisci
and most of the periphery of the tibial condyles. A slender fibrous band, transverse ligament of the knee, joins
the anterior edges of the menisci, tethering the menisci to each other during knee movements.
7. Movements of the knee joint
Flexion and extension are the main knee movements; some rotation occurs when the knee is flexed.
When the knee is fully extended with the foot on the ground, the knee passively “locks” because of medial
rotation of the femoral condyles on the tibial plateau (the “screw-home mechanism”). This position makes the
lower limb a solid column and more adapted for weight-bearing.
Although the knee joint is well constructed, its function is commonly impaired when it is hyperextended (e.g.,
in body contact sports).
8. Bursae around the knee joint There are at least 12 bursae around the knee joint because most tendons run
parallel to the bones and pull lengthwise across the joint during knee movements. The subcutaneous
prepatellar and infrapatellar bursae are located at the convex surface of the joint, allowing the skin to be able
to move freely during movements of the knee. The large suprapatellar bursa is especially important because an
infection in it may spread to the knee joint cavity.
STABILITY OF KNEE JOINT
The knee joint is relatively weak mechanically because of the incongruence of its articular surfaces, which has
been compared to two balls sitting on a warped tabletop.
The stability of the knee joint depends on:
(1) the strength and actions of the surrounding muscles and their tendons
(2) the ligaments that connect the femur and tibia.
Of these supports, the muscles are most important; therefore, many sport injuries are preventable through
appropriate conditioning and training.8

Dr.Kaan Yücel http://yeditepeanatomy1.org Joints of the lower limb
The erect, extended position is the most stable position of the knee. In this position the articular surfaces are
most congruent (contact is minimized in all other positions), the primary ligaments of the joint (collateral and
cruciate ligaments) are taut, and the many tendons surrounding the joint provide a splinting effect.
Figure 3. Knee jointhttp://www.kneejointsreplacement.com/anatomy-of-the-knee-joint
Figure 4. Right knee jointhttp://www.joinedagainst.org/new-as-research-on-ptf-joint
The tibia and fibula are connected by two joints: the tibiofibular joint and the tibiofibular syndesmosis (inferior
tibiofibular) joint. In addition, an interosseous membrane joins the shafts of the two bones. The interosseous
membrane not only links the tibia and fibula together, but also provides an increased surface area for muscle
9
3. TIBIOFIBULAR JOINTS
Dr.Kaan Yücel http://yeditepeanatomy1.org Joints of the lower limb
attachment. There are two apertures in the interosseous membrane, one at the top and the other at the
bottom, for vessels to pass between the anterior and posterior compartments of leg.
Tibiofibular joint (Superior tibiofibular joint)1. Articulation between tibia and fibula superiorly
2. Distinct feature of the joint -
3. Synovial joint type Plane type
4. Articular disc No.
5. Articular surfaces Flat facet on the fibular head and a similar articular facet located posterolaterally on the
lateral tibial condyle
6. Ligaments of the (superior) tibiofibular joint
The joint capsule is strengthened by anterior and posterior ligaments of the fibular head, which pass
superomedially from the fibular head to the lateral tibial condyle.
7. Movements of the knee joint
Slight movement of the joint occurs during dorsiflexion of the foot as a result of wedging of the trochlea of the
talus between the malleoli.
Tibiofibular syndesmosis (Inferior tibiofibular joint)1. Articulation between tibia and fibula, inferiorly
2. Distinct feature of the joint The integrity of the inferior tibiofibular joint is essential for the stability of the
ankle joint because it keeps the lateral malleolus firmly against the lateral surface of the talus.
3. Joint type compound fibrous joint. It is the fibrous union of the tibia and fibula by means of the interosseous
membrane (uniting the shafts) and the anterior, interosseous, and posterior tibiofibular ligaments (the latter
making up the inferior tibiofibular joint, uniting the distal ends of the bones).
4. Articular disc No.
5. Articular surfaces The rough, triangular articular area on the medial surface of the inferior end of the fibula
articulates with a facet on the inferior end of the tibia.
6. Ligaments of the tibiofibular syndesmosis
The strong deep interosseous tibiofibular ligament, continuous superiorly with the interosseous membrane,
forms the principal connection between the tibia and the fibula. The distal ends of the fibula and tibia are held
together by the inferior aspect of the interosseous membrane. The inferior part of this membrane spans the
narrow space between the fibular notch on the lateral surface of the distal end of the tibia and the
corresponding surface on the distal end of the fibula. This expanded end of the interosseous membrane is
reinforced by anterior and posterior tibiofibular ligaments. This firm linking together of the distal ends of the
tibia and fibula is essential to produce the skeletal framework for articulation with the foot at the ankle joint.10

Dr.Kaan Yücel http://yeditepeanatomy1.org Joints of the lower limb
7. Movements of the tibiofibular syndesmosis
Slight movement of the joint occurs to accommodate wedging of the wide portion of the trochlea of the talus
between the malleoli during dorsiflexion of the foot.
Figure 5. Superior tibiofibular jointhttp://en.wikipedia.org/wiki/File:Gray351.png
Figure 6. Inferior tibiofibular jointhttp://www.mananatomy.com/basic-anatomy/types-joints
11

Dr.Kaan Yücel http://yeditepeanatomy1.org Joints of the lower limb
Talocrural articulation
1. Articulation between distal ends of tibia and fibula with talus
2. Distinct feature one of the most vulnerable joints of the body
3. Joint type Hinge-type
4. Articular disc No.
5. Articular surfaces It is located between the distal ends of the tibia and the fibula and the superior part of the
talus. The trochlea (L., pulley) is the rounded superior articular surface of the talus. The medial surface of the
lateral malleolus articulates with the lateral surface of the talus.
6. Ligaments of the ankle joint
The ankle joint is reinforced laterally by the lateral ligament of the ankle. The lateral ligament of the ankle is
composed of three separate ligaments, the anterior talofibular ligament, the posterior talofibular ligament, and
the calcaneofibular ligament.
Anterior talofibular ligament, a flat, weak band that extends from the lateral malleolus to the neck of the
talus.
Posterior talofibular ligament, a thick, strong band that runs posteriorly from the malleolar fossa to the
lateral tubercle of the talus.
Calcaneofibular ligament, a round cord that passes from the tip of the lateral malleolus to the lateral
surface of the calcaneus.
12
4. ANKLE JOINT

Dr.Kaan Yücel http://yeditepeanatomy1.org Joints of the lower limb
The medial (deltoid) ligament is large, strong and triangular in shape. Its apex is attached above to the
medial malleolus and its broad base is attached below to a line that extends from the tuberosity of the
navicular bone in front to the medial tubercle of the talus behind.
The medial ligament is subdivided into four parts based on the inferior points of attachment:
the part that attaches in front to the tuberosity of the navicular and the associated margin of the plantar
calcaneonavicular ligament (spring ligament), which connects the navicular bone to the sustentaculum tali of
the calcaneus bone behind, is the tibionavicular part of the medial ligament;
the tibiocalcaneal part is more central and attaches to the sustentaculum tali of the calcaneus bone;
the posterior tibiotalar part attaches to the medial side and medial tubercle of the talus;
the fourth part (anterior tibiotalar part) is deep to the tibionavicular and tibiocalcaneal parts of the medial
ligament and attaches to the medial surface of the talus.
The medial ligament stabilizes the ankle joint during eversion and prevents subluxation (partial dislocation) of
the joint.
7. Movements of the ankle joint
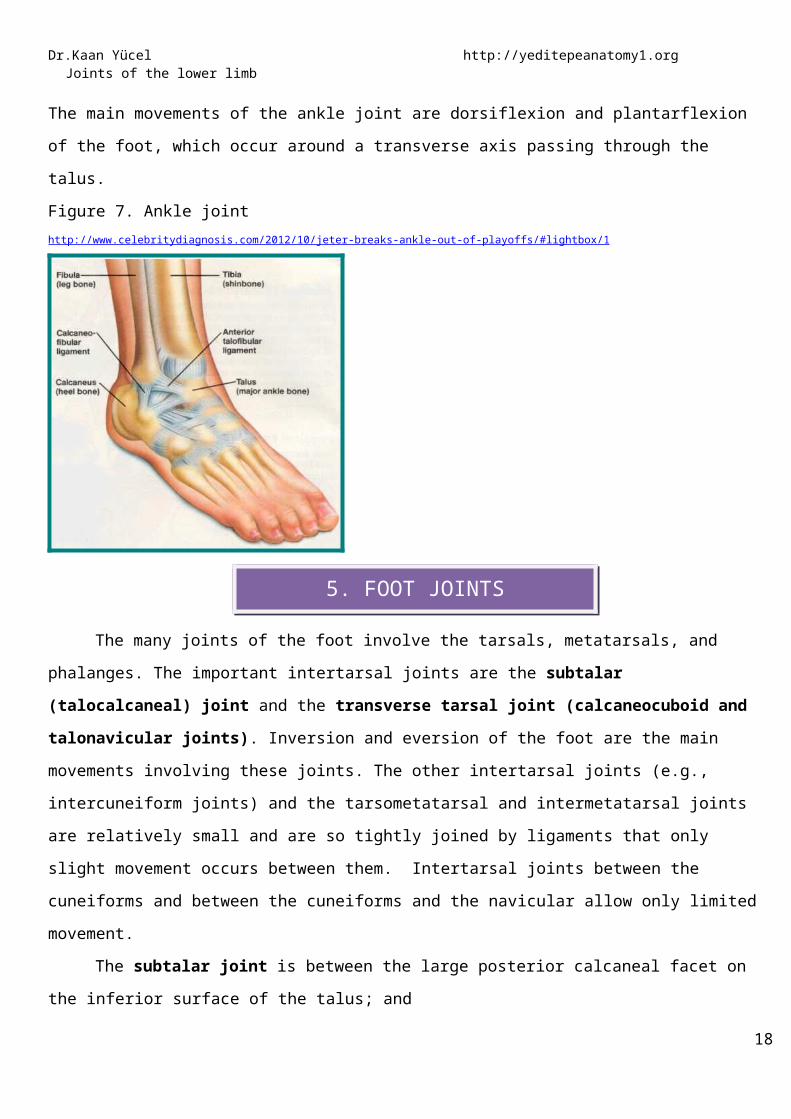
The main movements of the ankle joint are dorsiflexion and plantarflexion of the foot, which occur around a
transverse axis passing through the talus.
Figure 7. Ankle jointhttp://www.celebritydiagnosis.com/2012/10/jeter-breaks-ankle-out-of-playoffs/#lightbox/1
The many joints of the foot involve the tarsals, metatarsals, and phalanges. The important intertarsal
joints are the subtalar (talocalcaneal) joint and the transverse tarsal joint (calcaneocuboid and talonavicular
13
5. FOOT JOINTS

Dr.Kaan Yücel http://yeditepeanatomy1.org Joints of the lower limb
joints). Inversion and eversion of the foot are the main movements involving these joints. The other intertarsal
joints (e.g., intercuneiform joints) and the tarsometatarsal and intermetatarsal joints are relatively small and
are so tightly joined by ligaments that only slight movement occurs between them. Intertarsal joints between
the cuneiforms and between the cuneiforms and the navicular allow only limited movement.
The subtalar joint is between the large posterior calcaneal facet on the inferior surface of the talus; and
the corresponding posterior talar facet on the superior surface of the calcaneus. The subtalar joint allows
gliding and rotation, which are involved in inversion and eversion of the foot. Lateral, medial, posterior, and
interosseous talocalcaneal ligaments stabilize the joint. The interosseous talocalcaneal ligament lies in the
tarsal sinus. The subtalar joint occurs where the talus rests on and articulates with the calcaneus. The
anatomical subtalar joint is a single synovial joint between the slightly concave posterior calcaneal articular
surface of the talus and the convex posterior articular facet of the calcaneus. The interosseous talocalcaneal
ligament lies within the tarsal sinus, which separates the subtalar and talocalcaneonavicular joints and is
especially strong. Orthopaedic surgeons use the term subtalar joint for the compound functional joint
consisting of the anatomical subtalar joint plus the talocalcaneal part of the talocalcaneonavicular joint. The
subtalar joint (by either definition) is where the majority of inversion and eversion occurs, around an axis that is
oblique.
The talocalcaneonavicular and calcaneocuboid joints together form what is often referred to as the
transverse tarsal joint. At this joint, the midfoot and forefoot rotate as a unit on the hindfoot around a
longitudinal (AP) axis, augmenting the inversion and eversion movements occurring at the clinical subtalar joint.
Transection across the transverse tarsal joint is a standard method for surgical amputation of the foot.
The talocalcaneonavicular joint. It is a complex joint. The head of the talus articulates with the
calcaneus and plantar calcaneonavicular ligament (spring ligament) below and the navicular in front. The
talocalcaneonavicular joint allows gliding and rotation movements, which together with similar movements of
the subtalar joint are involved with inversion and eversion of the foot.
The joint is reinforced posteriorly by the interosseous talocalcaneal ligament;superiorly by the
talonavicular ligament, and inferiorly by the plantar calcaneonavicular ligament (spring ligament). The lateral
part of the talocalcaneonavicular joint is reinforced by the calcaneonavicular part of the bifurcate ligament,
which is a Y-shaped ligament superior to the joint. The base of the bifurcate ligament is attached to the anterior
aspect of the superior surface of the calcaneus and its arms are attached to:
the dorsomedial surface of the cuboid (calcaneocuboid ligament); and
the dorsolateral part of the navicular (calcaneonavicular ligament).
The calcaneocuboid joint is a synovial joint between: 14

Dr.Kaan Yücel http://yeditepeanatomy1.org Joints of the lower limb
the facet on the anterior surface of the calcaneus; and
the corresponding facet on the posterior surface of the cuboid.
The calcaneocuboid joint allows sliding and rotating movements involved with inversion and eversion of
the foot. The calcaneocuboid joint is reinforced by the bifurcate ligament and by the long plantar ligament and
the plantar calcaneocuboid ligament (short plantar ligament).
The plantar calcaneocuboid ligament (short plantar ligament) is short, wide, and very strong, and
connects the calcaneal tubercle to the inferior surface of the cuboid. It not only supports the calcaneocuboid
joint, but also assists the long plantar ligament in resisting depression of the lateral arch of the foot.
The long plantar ligament is the longest ligament in the sole of the foot and lies inferior to the plantar
calcaneocuboid ligament:
posteriorly, it attaches to the inferior surface of the calcaneus;
anteriorly, it attaches to inferior surface of the cuboid bone.
More superficial fibers of the long plantar ligament extend to the bases of the metatarsal bones.
The long plantar ligament supports the calcaneocuboid joint and is the strongest ligament, resisting
depression of the lateral arch of the foot.
The tarsometatarsal joints between the metatarsal bones and adjacent tarsal bones are plane joints
and allow limited sliding movements. The range of movement of the tarsometatarsal joint between the
metatarsal of the great toe and the medial cuneiform is greater than that of the other tarsometatarsal joints
and allows flexion, extension, and rotation.
The metatarsophalangeal joints are ellipsoid synovial joints between the sphere-shaped heads of the
metatarsals and the corresponding bases of the proximal phalanges of the digits. The metatarsophalangeal
joints allow extension and flexion, and limited abduction, adduction, rotation, and circumduction. Four deep
transverse metatarsal ligaments link the heads of the metatarsals together and enable the metatarsals to act as
a single unified structure. The interphalangeal joints are hinge joints that allow mainly flexion and extension.
They are reinforced by medial and lateral collateral ligaments and by plantar ligaments.
In the foot, flexion and extension occur in the forefoot at the metatarsophalangeal and interphalangeal
joints. Inversion is augmented by flexion of the toes (especially the great and 2nd toes), and eversion by their
extension (especially of the lateral toes). All bones of the foot proximal to the metatarsophalangeal joints are
united by dorsal and plantar ligaments. The bones of the metatarsophalangeal and interphalangeal joints are
united by lateral and medial collateral ligaments.
MAJOR LIGAMENTS OF THE FOOT
15

Dr.Kaan Yücel http://yeditepeanatomy1.org Joints of the lower limb
The major ligaments of the plantar aspect of the foot are the:
Plantar calcaneonavicular ligament (spring ligament)
Long plantar ligament.
Plantar calcaneocuboid ligament (short plantar ligament)
The plantar calcaneonavicular ligament (spring ligament) is a broad thick ligament that spans the space
between the sustentaculum tali behind and the navicular bone in front. It supports the head of the talus, takes
part in the talocalcaneonavicular joint, and resists depression of the medial arch of the foot.
The plantar calcaneocuboid ligament (short plantar ligament) is short, wide, and very strong, and connects the
calcaneal tubercle to the inferior surface of the cuboid. It not only supports the calcaneocuboid joint, but also
assists the long plantar ligament in resisting depression of the lateral arch of the foot.
The long plantar ligament is the longest ligament in the sole of the foot and lies inferior to the plantar
calcaneocuboid ligament:
posteriorly, it attaches to the inferior surface of the calcaneus between the tuberosity and the calcaneal
tubercle;
anteriorly, it attaches to a broad ridge and a tubercle on the inferior surface of the cuboid bone behind the
groove for the fibularis longus tendon.
More superficial fibers of the long plantar ligament extend to the bases of the metatarsal bones.
The long plantar ligament supports the calcaneocuboid joint and is the strongest ligament, resisting depression
of the lateral arch of the foot.
Figure 8.Ligaments of the foothttp://www.bartleby.com/107/illus354.html
16
6. ARCHES OF THE FOOT

Dr.Kaan Yücel http://yeditepeanatomy1.org Joints of the lower limb
Because the foot is composed of numerous bones connected by ligaments, it has considerable flexibility
that allows it to deform with each ground contact, thereby absorbing much of the shock. Furthermore, the
tarsal and metatarsal bones are arranged in longitudinal and transverse arches passively supported and actively
restrained by flexible tendons that add to the weight-bearing capabilities and resiliency of the foot. Thus much
smaller forces of longer duration are transmitted through the skeletal system.
The arches distribute weight over the foot, acting not only as shock absorbers but also as
springboards for propelling it during walking, running, and jumping. The resilient arches add to the foot's ability
to adapt to changes in surface contour. The weight of the body is transmitted to the talus from the tibia. Then it
is transmitted posteriorly to the calcaneus and anteriorly to the “ball of the foot” (the sesamoids of the 1st
metatarsal and the head of the 2nd metatarsal), and that weight/pressure is shared laterally with the heads of
the 3rd-5th metatarsals as necessary for balance and comfort.
Between these weight-bearing points are the relatively elastic arches of the foot, which become slightly
flattened by body weight during standing. They normally resume their curvature when body weight is removed.
The longitudinal arch of the foot is composed of medial and lateral parts. Functionally, both parts act as a unit
with the transverse arch of the foot, spreading the weight in all directions.
The medial longitudinal arch is composed of the calcaneus, talus, navicular, three cuneiforms, and three
metatarsals. The medial longitudinal arch is higher and more important than the lateral longitudinal arch.The
talar head is the keystone of the medial longitudinal arch.
The lateral longitudinal arch is much flatter than the medial part of the arch and rests on the ground during
standing. It is made up of the calcaneus, cuboid, and lateral two metatarsals.
The transverse arch of the foot runs from side to side. It is formed by the cuboid, cuneiforms, and bases of the
metatarsals.
The medial and lateral parts of the longitudinal arch serve as pillars for the transverse arch. The integrity of the
bony arches of the foot is maintained by both passive factors and dynamic supports.
Figure 14. Arches of the foothttp://www.tomsunderground.com/2012/01/20/the-case-for-minimalist-shoes-in-fitness-training
17
Dr.Kaan Yücel http://yeditepeanatomy1.org Joints of the lower limb
Congenital Dislocation of the HipThe stability of the hip joint depends on the ball-and-socket arrangement of the articular surfaces and
the strong ligaments. In congenital dislocation of the hip, the upper lip of the acetabulum fails to develop
adequately, and the head of the femur, having no stable platform under which it can lodge, rides up out of the
acetabulum onto the gluteal surface of the ilium.
Traumatic Dislocation of the HipTraumatic dislocation of the hip is rare because of its strength; it is usually caused by motor vehicle
accidents. However, should it occur, it usually does so when the joint is flexed and adducted. The head of the
femur is displaced posteriorly out of the acetabulum, and it comes to rest on the gluteal surface of the ilium
(posterior dislocation). The close relation of the sciatic nerve to the posterior surface of the joint makes it prone
to injury in posterior dislocations.
Arthritis of the Hip JointA patient with an inflamed hip joint will place the femur in the position that gives minimum discomfort
that is, the position in which the joint cavity has the greatest capacity to contain the increased amount of
synovial fluid secreted. The hip joint is partially flexed, abducted, and externally rotated.
Osteoarthritis, the most common disease of the hip joint in the adult, causes pain, stiffness, and
deformity. The pain may be in the hip joint itself or referred to the knee (the obturator nerve supplies both
joints). The stiffness is caused by the pain and reflex spasm of the surrounding muscles. The deformity is
flexion, adduction, and external rotation and is produced initially by muscle spasm and later by muscle
contracture.
Patellar Dislocations
18
CLINICAL ANATOMY

Dr.Kaan Yücel http://yeditepeanatomy1.org Joints of the lower limb
The patella is a sesamoid bone lying within the quadriceps tendon. The importance of the lower
horizontal fibers of the vastus medialis and the large size of the lateral condyle of the femur in preventing
lateral displacement of the patella has been emphasized. Congenital recurrent dislocations of the patella are
caused by underdevelopment of the lateral femoral condyle. Traumatic dislocation of the patella results from
direct trauma to the quadriceps attachments of the patella (especially the vastus medialis), with or without
fracture of the patella.
BunionsA bunion occurs on the medial aspect of the first metatarsophalangeal joint. This is an extremely
important area of the foot because it is crossed by tendons and ligaments, which transmit and distribute the
body's weight during movement. It is postulated that abnormal stresses in this region of the joint may produce
the bunion deformity.
Clinically, a bunion is a significant protuberance of bone that may include soft tissue around the medial
aspect of the first metatarsophalangeal joint. As it progresses, the toe appears to move toward the smaller
toes, producing crowding of the digits.
Degenerative joint disease/osteoarthritisDegenerative joint disease occurs throughout many joints within the body. Articular degeneration may
result from an abnormal force across the joint with a normal cartilage or a normal force with abnormal
cartilage.
Typically degenerative joint disease occurs in synovial joints and the process is called osteoarthritis. In
the joints where osteoarthritis occurs the cartilage and bony tissues are usually involved, with limited change
within the synovial membrane. The typical findings include reduction in the joint space, eburnation (joint
sclerosis), osteophytosis (small bony outgrowths), and bony cyst formation. As the disease progresses the joint
may become malaligned, its movement may become severely limited, and there may be significant pain.
The commonest sites for osteoarthritis include the small joints of the hands and wrist, and in the lower
limb, the hip and knee are typically affected, though the tarsometatarsal and metatarsophalangeal articulations
may undergo similar change.
The etiology of degenerative joint disease is unclear, but there are some associations, including genetic
predisposition, increasing age (males tend to be affected younger than females), overuse or underuse of joints,
and nutritional and metabolic abnormalities. Further factors include joint trauma and pre-existing articular
disease or deformity.
The histological findings of osteoarthritis consist of degenerative changes within the cartilage and the
subchondral bone. Further articular damage worsens these changes, which promote further abnormal stresses
upon the joint. As the disease progresses the typical finding is pain, which is usually worse on rising from bed 19

Dr.Kaan Yücel http://yeditepeanatomy1.org Joints of the lower limb
and at the end of a day's activity. Commonly it is aggravated by the extremes of movement or unaccustomed
exertion. Stiffness and limitation of movement may ensue.
Examination of the knee jointIt is important to establish the nature of the patient's complaint before any examination. The history
should include information about the complaint, the signs and symptoms, and the patient's lifestyle (level of
activity). This history may give a significant clue to the type of injury and the likely findings on clinical
examination, for example if the patient was kicked around the medial aspect of the knee, a valgus deformity
injury to the tibial collateral ligament might be suspected.
The examination should include assessment in the erect position, while walking, and on the couch. The
affected side must be compared with the unaffected side.
There are many tests and techniques for examining the knee joint, including the following.
Tests for anterior instabilityLachman's test-the patient lies on the couch and the examiner places one hand around the distal femur,
the other around the proximal tibia, and elevates the knee producing 20° of flexion. The patient's heel rests on
the couch. The examiner's thumb must be on the tibial tuberosity. The hand on the tibia applies a brisk
anteriorly directed force. If the movement of the tibia on the femur comes to a sudden stop, it is a firm
endpoint. If it does not come to a sudden stop, the endpoint is described as soft and is associated with a tear of
the anterior cruciate ligament.
Anterior drawer test-a positive anterior drawer test is when the proximal head of a patient's tibia can
be pulled anteriorly on the femur. The patient lies supine on the couch. The knee is flexed to 90° and the heel
and sole of the foot are placed on the couch. The examiner sits gently on the patient's foot, which has been
placed in a neutral position. The index fingers are used to check that the hamstrings are relaxed while the other
fingers encircle the upper end of the tibia and pull the tibia. If the tibia moves forward, the anterior cruciate
ligament is torn. Other peripheral structures, such as the medial meniscus or meniscotibial ligaments, must also
be damaged to elicit this sign.
Pivot shift test-there are many variations of this test. The patient's foot is wedged between the
examiner's body and elbow. The examiner places one hand flat under the tibia pushing it forward with the knee
in extension. The other hand is placed against the patient's thigh pushing it the other way. The lower limb is
taken into slight abduction by the examiner's elbow with the examiner's body acting as a fulcrum to produce
the valgus. The examiner maintains the anterior tibial translation and the valgus and initiates flexion of the
patient's knee. At about 20°-30° the pivot shift will occur as the lateral tibial plateau reduces. This test
demonstrates damage to the posterolateral corner of the knee joint and the anterior cruciate ligament.
Tests for posterior instability20

Dr.Kaan Yücel http://yeditepeanatomy1.org Joints of the lower limb
Posterior drawer test-a positive posterior drawer test occurs when the proximal head of a patient's tibia
can be pushed posteriorly on the femur. The patient is placed in a supine position and the knee is flexed to
approximately 90° with the foot in the neutral position. The examiner sits gently on the patient's foot placing
both thumbs on the tibial tuberosity and pushing the tibia backward. If the tibial plateau moves, the posterior
cruciate ligament is torn.
21


















