· Web viewAmal Taha Abo-elghiet 2, Abeer Refai y 3 Aya Y Badran 1 Departement of Dermatology,...
22
Pattern Of Direct Immunofluorescence (DIF) in the diagnosis of Pemphigus Azza M Abdel-Megaid 1 , Hisham D Gaber 1 , Amal Taha Abo- elghiet 2 , Abeer Refaiy 3 Aya Y Badran 1 1. Departement of Dermatology, Veneareology and Andrology. 2. Departement of Histology. 3. Departement of Pathology. Abstract: Background: Immunofluorescence (IF) is a reliable biochemical staining technique for the detection of antibodies, which are bound to antigen in the tissue or circulating in body fluids. The relative simplicity and accuracy of the technique has made immunofluorescence an unavoidably powerful technique in the diagnosis of bullous diseases. Objectives: To detect the pattern of direct immunofluorescence (DIF) in the diagnosis of pemphigus. Methods: Thirty-six patients with pemphigus disease were enrolled in our study. The age of whom ranged from 21to 73 years with a mean age ± SD of 46.94±14.6 years Two skin biopsies (one from the bullous lesion and the other one from adjacent area) were taken from
Transcript of · Web viewAmal Taha Abo-elghiet 2, Abeer Refai y 3 Aya Y Badran 1 Departement of Dermatology,...

Pattern Of Direct Immunofluorescence (DIF) in the
diagnosis of PemphigusAzza M Abdel-Megaid1, Hisham D Gaber1, Amal Taha Abo-elghiet2,
Abeer Refaiy3 Aya Y Badran1
1. Departement of Dermatology, Veneareology and Andrology.2. Departement of Histology.3. Departement of Pathology.
Abstract:
Background: Immunofluorescence (IF) is a reliable biochemical staining
technique for the detection of antibodies, which are bound to antigen in the
tissue or circulating in body fluids. The relative simplicity and accuracy of the
technique has made immunofluorescence an unavoidably powerful technique in
the diagnosis of bullous diseases.
Objectives: To detect the pattern of direct immunofluorescence (DIF) in the
diagnosis of pemphigus.
Methods: Thirty-six patients with pemphigus disease were enrolled in our study.
The age of whom ranged from 21to 73 years with a mean age ± SD of
46.94±14.6 years Two skin biopsies (one from the bullous lesion and the other
one from adjacent area) were taken from each patient, lesional biopsy specimens
were used for histopathological examination after standard processing, while
perilesional skin samples were used for performing direct immunofluorescence.
Results: DIF was positive in all patients with pemphigus vulgaris (PV), showing
intraepidermal deposition of immunoglobulins and complement 3 (C3). IgG was
seen in all of them (100%), while C3 was also observed in 38.4% patients, and
IgM was positive in (3.8%) in a similar pattern.
Conclusion: Immunofluorescence (IF) studies are an important part of the
laboratory evaluation of immunologically mediated bullous dermatoses and have

become standard procedures for accurately diagnosing patients with these
disorders.
Key words: Direct Immunofluorescence, Autoimmune bullous disorders,
pemphigus.
Introduction:
Autoimmune bullous skin diseases are organ-specific autoimmune
diseases associated with pathogenic autoantibodies against structural proteins
that maintain cell-cell and cell-matrix adhesions in the skin and mucous
membranes (Sitaru and Zilliken, 2005). Antibodies may target the basement
membrane zone or interepidermal cell adhesion. Deposition of antibody can be
shown at the level of blister formation, at sites adjacent to blisters and in
uninvolved skin. The immunoreactant involved varies with the disease, but is
typically IgG or, less commonly, IgA or C3. The sites of antibody binding
(‘target antigen’) have been identified and characterized in most diseases
(Taghipour and Wojnarowsk, 2009).
The classification of autoimmune bullous dermatoses relies on histologic
criteria, primarily according to the localization of bullae; so, intraepidermal and
subepidermal bullous dermatoses are distinguished (Rados, 2011).
There is a great need for rapidly establishing the diagnosis of these
disorders since they may run a severe and potentially life-threatening course
(Kneisel A and Hertl M, 2011).
While histopathological examinations provide evidence for the level of
blister formation, immunofluorescence microscopy has been established to
identify tissue-bound and circulating autoantibodies. Direct
immunofluorescence microscopy represents the gold standard for detecting
tissue-bound autoantibodies. Indirect immunofluorescence microscopy with
defined tissue substrates is considered the first step in detecting circulating
autoantibodies. Confirmatory tests such as enzyme-linked-immunosorbent assay
(ELISA), immunoblot or immunoprecipitation analyses are performed utilizing
recombinant proteins or keratinocyte extract (Kneisel A and Hertl M, 2011).
Two types of Immunofluorescence are present, direct
immunofluorescence (DIF) and indirect immunofluorescence (IIF). DIF helps
detect molecules such as immunoglobulins and complement components within
biopsy specimens. The ideal site for the biopsy specimen depends on the type of
disorder. For bullous diseases, DIF is performed using perilesional skin, that is,
normal-appearing skin immediately adjacent to a lesion (vesicle, bulla, urticarial
plaque, or erythematous patch), as the immune deposits are partially or
completely degraded in inflamed or blistered skin, and DIF may be falsely
negative(Mutasim and Adams, 2001).
Aim of the study: To detect the pattern of direct immunofluorescence in the
diagnosis of pemphigus.
Subjects and Methods: The study was conducted at the department of Dermatology, Andrology
and Venereology, Assiut University Hospital during the period of 2013-2015 on
36 patients with pemphigus, after exclusion of patients on corticosteroids and/or
any immunosuppressive agent at, or one month before the time of the study.
Age, sex, type of lesions, site, mucous membrane affection, duration,
associated symptoms, previous treatment, other system affection and a
written informed consent were signed by every patient.
Two skin biopsies (one from the bullous lesion and the other one from
adjacent area) were taken from each patient after local anesthesia using a
6mm punch.
Lesional biopsy specimens were collected in 10% formalin solution and
used for histopathological examination after standard processing. The

sections were stained with hematoxylin and eosin and examined under the
light microscope. Perilesional skin samples were used for performing
direct immunofluorescence using a 6 mm punch from perilesional
skin,samples quickly frozen in liquid nitrogen at (-196 C), processesd
and stained using the following antisera: anti-IgG, anti-IgA, anti-IgM and
anti-C3(manufactured by Thermo Fisher Scientific Company). Then
imaged by Olympus camera attached to Olympus epifluoerescence
microscope (Olympus, Japan). Evaluation of biopsy sections was made by
positive and negative marks only.
Statistical analysis:
All analyses were performed with the SPSS 20.0 software.Categorical
variables were described by number and percent (N, %), where continuous
variables described by mean and standard deviation (Mean, SD). Continuous
variables were tested for normal distribution using Kolmogorove Smirnov
test.
Results
Among patients with pemphigus, pemphigus vulgaris (PV) was the most
frequent disease 26/36 (72.7%), followed by pemphigus foliaceous (PF) 7/36
(19.4%), and lastly pemphigus herpetiformis (PH) 3/36 (8.3%). The age of this
group ranged from 21to 73 years with a mean age ± SD of 46.94±14.6 years. In
this group males were more frequent among patients having PV and PF, while
all PH patients were females (Table 1).

Table (1): Age and sex distribution in patients with pemphigus
DiseaseSex, n (%) Age
mean+SD (range)Male Female
Pemphigus (n=36)20(55.6
%)16(44.4%
)46.94±14.6(21-73)
Pemphigus Vulgaris (26)16(61.5%
) 10(38.5%)43.88±15.06(21-73)
Pemphigus Foliaceous (7) 4(57.1%) 3(42.9%) 57.57±10.67(45-72) Pemphigus
Herpetiformis(3) 0(0%) 3(100%) 46.67±7.64(40-55)
Histopathological examination of all patients clinically diagnosed as PV
(n=26) confirmed the diagnosis histopathologically. Their biopsies showed
supra-basal intra-epidermal bullae, acantholytic cells and tombstones appearance
(figure1).
Fig.1. Histopathological examination of lesional skin in PV (H&E x100).
Patients with PF, all patients clinically diagnosed as PF (n=7) had
confirmed the diagnosis histopathologically. Their biopsies showed subcorneal
intra-epidermal bullae with mixture of inflammatory cells (figure 2).

Fig.2. Histopathological examination of lesional skin in PF (H&Ex100).
We had 3 female patients presented with itchy grouped vesicular lesions,
and were clinically diagnosed as dermatitis herpetiformis (DH) or pemphigus
herpetiformis (PH), on examination of their biopsies with H &E, all patients
showed subcorneal blister with polymorphs and esinophils, so the diagnosis of
DH was excluded. And we describe them as having PH (Figure 3).
Fig.3. Histopathological examination of lesional skin in PH (H&E,x100).
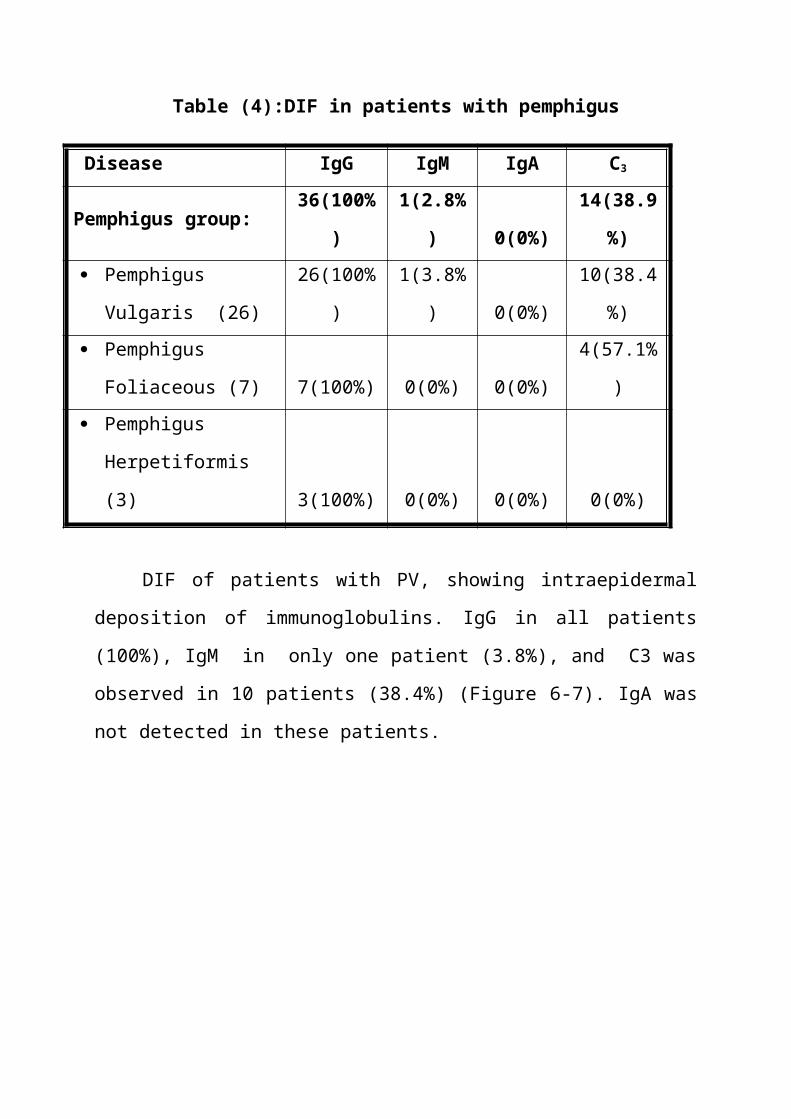
DIF was positive in all patients with pemphigus (100%), showing
intraepidermal deposition of immunoglobulins and complement 3 (C3).

Table (4):DIF in patients with pemphigus
Disease IgG IgM IgA C3
Pemphigus group: 36(100%) 1(2.8%) 0(0%) 14(38.9%) Pemphigus Vulgaris
(26) 26(100%) 1(3.8%) 0(0%) 10(38.4%)
Pemphigus Foliaceous
(7) 7(100%) 0(0%) 0(0%) 4(57.1%)
Pemphigus
Herpetiformis (3) 3(100%) 0(0%) 0(0%) 0(0%)
DIF of patients with PV, showing intraepidermal deposition of
immunoglobulins. IgG in all patients (100%), IgM in only one patient (3.8%),
and C3 was observed in 10 patients (38.4%) (Figure 6-7). IgA was not detected
in these patients.
Fig. 6. Direct immunofluorescence findings in PV showing deposition of IgG
in the intercellular spaces of the epidermis (x100).

Fig.7. Direct immunofluorescence findings in PV showing deposition of C3
in the intercellular spaces of the epidermis (x100).
DIF in patients with PF showed intraepidermal deposition of
immunoglobulins, mainly in the upper part of the epidermis, but this pattern
cannot be seen in all patients, and the diagnosis was helped by clinical,
pathological and ELISA result. IgG was seen in all patients (100%), while
C3 was also observed in 4 (71.4%) patients.
Fig.8.:Direct immunofluorescence findings in PF showing deposition of
IgG in the intercellular spaces of the epidermis (x100).

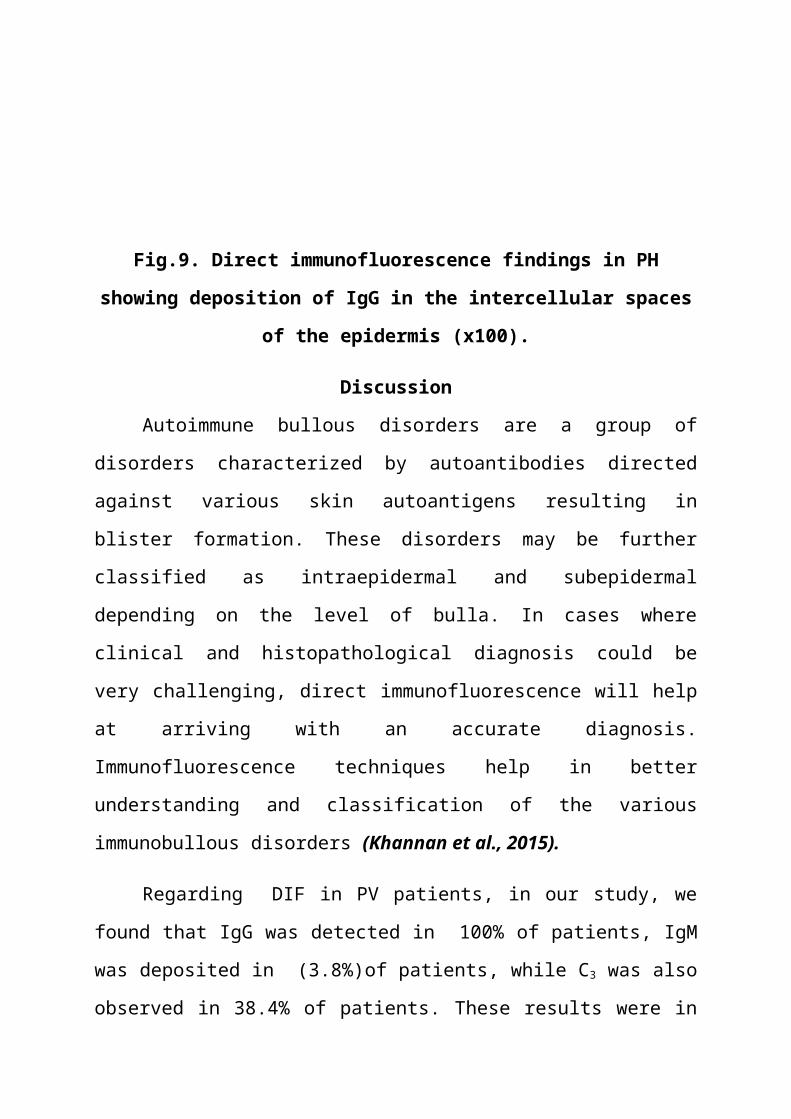
DIF was positive in all patients with PH showed intraepidermal deposition
of immunoglobulins, mainly in the upper part of the epidermis , but this pattern
cannot be seen in all patients, and the diagnosis was helped by clinical,
pathological and ELISA result. IgG was seen in all of them (100%) (Figure 9).
Fig.9. Direct immunofluorescence findings in PH showing deposition of IgG
in the intercellular spaces of the epidermis (x100).
Discussion
Autoimmune bullous disorders are a group of disorders characterized by
autoantibodies directed against various skin autoantigens resulting in blister
formation. These disorders may be further classified as intraepidermal and
subepidermal depending on the level of bulla. In cases where clinical and
histopathological diagnosis could be very challenging, direct
immunofluorescence will help at arriving with an accurate diagnosis.
Immunofluorescence techniques help in better understanding and classification
of the various immunobullous disorders (Khannan et al., 2015).
Regarding DIF in PV patients, in our study, we found that IgG was
detected in 100% of patients, IgM was deposited in (3.8%)of patients, while C3
was also observed in 38.4% of patients. These results were in the agreement
with Kabir et al., 2009, who found that 87.5% of PV patients showed
intercellular lace like deposition of IgG in the whole thickness of the epidermis.
They stated that the diagnosis of blistering diseases can often made on the basis
of clinical features but in some cases it may be possible to produce only
differential diagnosis, they also stated that less than 50% of clinical diagnosis
showed concordance with the final diagnosis in their study. DIF study has a
definitive role in distinguishing immune mediated blistering diseases from
others. They concluded that DIF technique combined with routine histology is a
useful method in distinguishing most of immunobullous diseases, if not all.
A similar study done by Monsef et al., 2012 found that all cases of PV
had positive DIF in intercellular region; IgG was detected in all (100%) of
patients, IgM in 11.1% of patients and C3 in 33.3% of patients. They concluded
that immunofluorescence tests are sensitive diagnostic methods for autoimmune
bullous diseases.
Another study done by Khannan et al., 2015 found that 100% of cases
with PV showed deposition of IgG in intercellular region, while C3 was also
observed in 84% of patients.
In patients with pemphigus foliaceus (n=7), DIF was positive in all
patients in the present study showing intraepidermal deposition of
immunoglobulins, mainly in the upper part of the epidermis, but this pattern
cannot be seen in all patients. IgG was seen in all of them (100%), while C 3 was
observed in (57.1%) of patients. Similar results were obtained by Kabir et al.,
2009 who found that IgG was positive in all patients with pemphigus foliaceus
(100%) in the intercellular substance (ICS) in the full thickness of epidermis.
Also, Khannan et al., 2015 found that 100% of cases with PF showed ICS
deposition of IgG.
Huang et al., 2007, stated that in some cases of pemphigus, the results
of immunofluorescence staining may be identical in PV and PF. Similarly,
Khandpur et al., 2010 stated that in a majority of the cases, the diagnosis of PV
and PF, the two major variants of pemphigus, rests upon clinical, histological
and immunofluorescence features, however, at times, differentiation between
these two variants, and between pemphigus and other vesicobullous disorders is

a diagnostic challenge as the DIF shows a similar fluorescence pattern in PV and
PF. In these cases ELISA may have a role in the differentiation between the two
variants.
Conclusions
Immunofluorescence (IF) studies are an important part of the laboratory
evaluation of immunologically mediated bullous dermatoses and have
become standard procedures for accurate diagnosis of patients with these
disorders.
Immunofluorescence studies are considered the ‘gold standard’ for the
diagnosis of autoimmune blistering diseases.
Limitations
Small sample size of the study.
The rarity of some types of pemphigus (eg. Pemphigus herpetiformis).
References.
Alireza Monsef, Mahmood Farshchian, Mohammad Jafari, Mehdi
Farshchian. Immunofluorescence Pattern of Autoimmune Bullous
Diseases in Iranian Patients. Iranian Journal of Pathology 2012, 7 (4),
231.
C. K. Khannan, R. Bhat, A retrospective study of clinical,
histopathological and direct immunofluorescence spectrum of
immunobullous Disorders, International Journal of Scientific and
Research Publications,5(2015)2250.
Kabiirr AN,,1 Das RK,, 2 Kamall M. Direct Immunofluorescence Test of
Skin Biopsy Samples – Results of 204 Cases. Dinajpur Med Col J 2009; 2
(1):8-12.

Khandpur S, Sharma V, Sharma A, Pathria G and Satyam A (2010):
Comparison of enzyme-linked immunosorbent assay test with
immunoblot assay in the diagnosis of pemphigus in Indian patients. Indian
Journal of Dermatology, Venereology and Leprology: 76,(1):27.
Kneisel A and Hertl M. Autoimmune bullous skin diseases. Part 2:
diagnosis and therapy. Journal der Deutschen Dermatologischen
Gesellschaft, 2011; 9 (11)927.
Mutasim D, Adams B. Immunofluorescence in dermatology. J Am
AcadDermatol 2001; 45:803.
Radoš J Autoimmune blistering diseases: Histologic meaning .Clin
Dermatol 2011; 29 (4):377.
Sitaru C, Zillikens D. Mechanisms of blister induction by autoantibodies.
Exp Dermatol 2005; 14:861.
Taghipour K, Wojnarowsk. Autoimmune and other blistering diseases.
Medicine; 2009; 37(6), 291.
كلية الطب األمراض الجلدية و قسم
التناسلية
نمط الوميض الفلوريسيني المناعي المباشر في تشخيص مرض الفقاعالطبيبة/ آيه يوسف محمد بدران
مدرس مساعد بقسم األمراض الجلدية والتناسليةوأمراض الذكورة
تحت إشراف أ.د/ عزه محفوظ عبد المجيد
أستاذ األمراض الجلدية والتناسلية وأمراض الذكورةكلية الطب ــ جامعة أسـيوط
أ.د/ أمل طـــه أبوالغيطأستاذ الهستولوجيا
كليه الطب – جامعه أسيوطد/هشام دياب جابر
مدرس بقسم األمراض الجلدية والتناسلية وأمراض الذكورةكلية الطب ــ جامعة أسـيوط
2016

:المقدمة تضم األمراض الفقاعية المناعية العديــد من األنــواع ، تشــترك جميعهــا في-
وجود أجسام مضادة للبروتينات التى تحافــظ على التصــاق الخاليــا ببعضــهاالبعض في الجلد وكذلك في األغشية المخاطية.
حيث تقوم هذه االجسام المضاده بفصل خاليــا الجلــد واالغشــيه المخاطيــه- عن بعضــها البعض ممــا يــؤدي الي ظهــور الفقاعــات الجلديــه والتقرحــات
بالجلد واالغشيه المخاطيه. وتختلف االعراض الظاهره في المريض حسب مكــان االنفصــال, حيث انــه-
من الممكن ان يكون االنفصال في طبقه االدمه او في طبقه البشره. و تعتمد هــذه األمــراض في تشخيصــها على : الفحص اإلكليــنيكي ، الفحص-
المجهري والفحص المجهري الفلوريسيني المناعي وكذلك اســتخدام تقنيــة إليزا وغيرها من الفحوصات التي تعتمد على وجــود األجســام المضــادة في
الدم. ــةحيث يقوم الفحص الم- جهري بتحديد ما إذا كان اإلنفصال موجود في طبق
األدمة أم بطبقــة البشــره , ولكن ال يمكن االعتمــاد علي الفحص المجهــري وحـــده في التشـــخيص ، حيث البـــد من اســـتخدام الفحص المجهـــري الفلوريسيني المناعي بطريقتيــة المباشــرة )حيث تؤخــذ العينــة من الجلــد(والغير مباشرة ) حيث تؤخذ العينة من الدم( وكذلك استخدام تقنية إ ليزا.
أهـداف البحث : تحديد طريقة ترسب األجسام المضادة في المرضــى المصــابين بــاألمراض
الفقاعية المناعية بالجلد وتحديد نوعها ومكانها.
: وتشــتمل هــذه المجموعــة على المرضــى م""ريض36 تضــمنت هــذه الدراسة الفقاع الشائع " الفقاع الورقيالمصابون بمرض الفقاع بأنواعه المختلفة )
(" الفقاع الحلئي . مرضى7 مريض يعانون من مرض الفقاع الشائع و 26وقد وجد أن
3يعانون من مرض الفقاع الورقي و مريض يعانون من مرض الفقاع.الحلئي
عام73 إلى 21وقد كان متوسط أعمارهم يتراوح من ولقد وجد بالفحص المجهري الفلوريسيني المناعي في مرض الفقاع
(الجلوبولين المناعي جالشائع أن ) (IgG) في100موجود بنسبة % (الجلوبولين المناعي مالمرضى، أما ) (IgM) 3.8وجد بنسبة %،
%، وجميعها موجودة في طبقة38.4وجد بنسبة C3 وكذلك المتمم الثالث .البشرة بالجلد بين الخاليا وبعضها
:وعن مرض الفقاع الحلئي وجد بالفحص المجهري الفلوريسيني المناعي في مرض الفقاع الشائع أن
الجلوبولين المناعي ج) (IgG) في المرضى100موجود بنسبة % .