
VIDEO - LWW Journalsjournals.lww.com/plasreconsurg/...Aesthetic_Surgery... · Reconstr. Surg. 119:...
16
VIDEO Baker Gordon Cosmetic Surgery Video Series Restoring Facial Shape in Face Lifting: The Role of Skeletal Support in Facial Analysis and Midface Soft-Tissue Repositioning (Baker Gordon Symposium Cosmetic Series) James M. Stuzin, M.D. Coconut Grove, Fla. Summary: Aesthetic analysis in facial rejuvenation has traditionally been sub- ordinate to technical solutions. While concerns regarding correction of facial laxity, a reduction in the depth of the nasolabial fold, and improvement of both the jowl and the jawline are worthy goals in rhytidectomy, the aesthetic concept of restoring facial shape to a more youthful appearance is equally important. Restoring facial shape in face lifting requires an understanding of how the face ages and then the formulation of a treatment plan that is individualized for the patient. Re-establishment of facial contour is significantly influenced by the re-elevation of descended facial fat through superficial musculoaponeurotic system manipulation; it can be approached through a variety of technical solutions. Underlying skeletal support affects not only the appearance of the face in youth but also how the face ages and influences the operative plan in terms of the requirements for fat repositioning. Formulating a treatment plan that is patient specific and based on the artistic goals as influenced by skeletal support is the key element for consistency in restoring facial shape in face lifting. (Plast. Reconstr. Surg. 119: 362, 2007.) T he works of Skoog 1 and Mitz and Peyronie 2 enlightened plastic surgeons to the possibil- ity of repositioning descended facial fat to the anatomic position of youth, providing an al- ternative to skin envelope tightening to enhance contour in the aging face. The recognition that sub-superficial musculoaponeurotic system (SMAS) dissection offered a technical solution for facial re- juvenation spawned multiple anatomic studies to delineate an accurate understanding of facial soft- tissue anatomy. 3–11 This later led to further investi- gations that more clearly defined both the anatomic and morphologic changes that occur in the aging face, leading to a plethora of technical approaches for facial rejuvenation. 12–29 In reviewing the litera- ture, good results were noted utilizing what appear to be very different technical approaches. In reality, most of these seemingly different technical proce- dures share a common theme that contour restora- tion is predominantly through the re-elevation of facial fat as opposed to skin envelope tightening. Although good results are possible through a variety of techniques, in my opinion, all techniques have advantages, disadvantages, and limitations, with the ultimate result often dependent on underlying skel- etal support and the quality of facial soft tissues for a particular patient. For me, the key to consistent results in face lifting is not the particular technique utilized but rather the preoperative aesthetic analysis and how the operative plan is individualized accord- ing to the aesthetic needs of the patient. In formulating a treatment plan, it is helpful to look at what produces surgical stigma following rhytidectomy. Perhaps it begins with the term “face lift,” a mechanical phrase suggesting that middle-aged faces become loose over time and that the surgeon’s primary goal in facial rejuve- nation is to tighten relaxed facial soft tissues. Un- fortunately, the surgical cause and effect of trying Received for publication January 5, 2006; accepted March 3, 2006. Reprinted and reformatted from the original article published with the January 2007 issue (Plast Reconstr Surg. 2007; 119:362–377). Copyright ©2012 by the American Society of Plastic Surgeons DOI: 10.1097/PRS.0b013e318250844c Please go to the online version of the Journal at www.PRSJournal.com to see the online streaming video associated with this article. www.PRSJournal.com 40S
Transcript of VIDEO - LWW Journalsjournals.lww.com/plasreconsurg/...Aesthetic_Surgery... · Reconstr. Surg. 119:...
VIDEO�Baker Gordon Cosmetic Surgery Video Series
Restoring Facial Shape in Face Lifting: TheRole of Skeletal Support in Facial Analysisand Midface Soft-Tissue Repositioning(Baker Gordon Symposium Cosmetic Series)
James M. Stuzin, M.D.
Coconut Grove, Fla.Summary: Aesthetic analysis in facial rejuvenation has traditionally been sub-ordinate to technical solutions. While concerns regarding correction of faciallaxity, a reduction in the depth of the nasolabial fold, and improvement of boththe jowl and the jawline are worthy goals in rhytidectomy, the aesthetic conceptof restoring facial shape to a more youthful appearance is equally important.Restoring facial shape in face lifting requires an understanding of how the faceages and then the formulation of a treatment plan that is individualized for thepatient. Re-establishment of facial contour is significantly influenced by there-elevation of descended facial fat through superficial musculoaponeuroticsystem manipulation; it can be approached through a variety of technicalsolutions. Underlying skeletal support affects not only the appearance of theface in youth but also how the face ages and influences the operative planin terms of the requirements for fat repositioning. Formulating a treatmentplan that is patient specific and based on the artistic goals as influenced byskeletal support is the key element for consistency in restoring facial shapein face lifting. (Plast. Reconstr. Surg. 119: 362, 2007.)
The works of Skoog1 and Mitz and Peyronie2
enlightened plastic surgeons to the possibil-ity of repositioning descended facial fat to
the anatomic position of youth, providing an al-ternative to skin envelope tightening to enhancecontour in the aging face. The recognition thatsub-superficial musculoaponeurotic system (SMAS)dissection offered a technical solution for facial re-juvenation spawned multiple anatomic studies todelineate an accurate understanding of facial soft-tissue anatomy.3–11 This later led to further investi-gations that more clearly defined both the anatomicand morphologic changes that occur in the agingface, leading to a plethora of technical approachesfor facial rejuvenation.12–29 In reviewing the litera-ture, good results were noted utilizing what appearto be very different technical approaches. In reality,most of these seemingly different technical proce-dures share a common theme that contour restora-
tion is predominantly through the re-elevation offacial fat as opposed to skin envelope tightening.Although good results are possible through a varietyof techniques, in my opinion, all techniques haveadvantages, disadvantages, and limitations, with theultimate result often dependent on underlying skel-etal support and the quality of facial soft tissues fora particular patient. For me, the key to consistentresults in face lifting is not the particular techniqueutilized but rather the preoperative aesthetic analysisand how the operative plan is individualized accord-ing to the aesthetic needs of the patient.
In formulating a treatment plan, it is helpfulto look at what produces surgical stigma followingrhytidectomy. Perhaps it begins with the term“face lift,” a mechanical phrase suggesting thatmiddle-aged faces become loose over time andthat the surgeon’s primary goal in facial rejuve-nation is to tighten relaxed facial soft tissues. Un-fortunately, the surgical cause and effect of trying
Received for publication January 5, 2006; accepted March3, 2006.Reprinted and reformatted from the original article publishedwith the January 2007 issue (Plast Reconstr Surg. 2007;119:362–377).Copyright ©2012 by the American Society of Plastic Surgeons
DOI: 10.1097/PRS.0b013e318250844c
Please go to the online version of the Journalat www.PRSJournal.com to see the onlinestreaming video associated with this article.
www.PRSJournal.com40S

to tighten a loose face too often produce a tightappearance to facial contour. This is not only un-natural but neither youthful nor rejuvenative. Inmy opinion, a better aesthetic concept than tryingto tighten a loose face is to restore facial shape. Toconsistently improve facial shape in face liftingrequires that the surgeon accurately understandthe anatomic changes that have occurred in agingfor a particular patient, appreciate the importanceof underlying skeletal support in formulating thetreatment plan, and incorporate his or her aes-thetic vision into a surgical destination that is ap-propriate for the specific patient.
CHANGES IN FACIAL SHAPEWITH AGING
As the human face ages, facial shape changes.Morphologic facial changes are multifactorial. Someof these (changes) are straightforward to address,while others remain difficult technical challenges. Aparadox for me has always been that facial anatomy
(in terms of basic soft-tissue architecture) is es-sentially unchanged from youth to middle age, butfacial appearance changes greatly over time and ispatient specific. Although each face ages differ-ently, there are common themes noted in all agingfaces, as described below.
Descent of Facial FatAs the human face ages, facial fat descends and
with it facial shape changes. Typically, the youthfulface is full of well-supported fat. Volumetric high-lights are located within facial aesthetic subunitsthat have a high density of retaining ligaments(malar, preparotid, and orbital rim) and serve tofixate this volume of fat to underlying structures.Juxtaposed to the volumetric fullness (or convex-ity) of the malar and preparotid region is com-monly a concavity within the submalar region,overlying the buccinator muscle and buccal recess.The combination of fullness in the malar regionand lateral cheek associated with submalar con-
Fig. 1. (Left) Age 25, the youthful face is full of well-supported facial fat, typically located overlying themalar eminence and along the lateral cheek, overlying the parotid and masseter. This is associated witha concavity or depression overlying the buccal recess just anterior to the masseter. The combination offullness in the malar region and lateral cheek associated with a concavity overlying the buccal recessaccounts for the angular, tapered appearance of the youthful face. (Right) Age 55. Thirty years later, theaesthetic effect of the descent of facial fat has become obvious, resulting in a change in facial shape.Typically, faces in middle age are square in their configuration, with little differential between malar high-light and midfacial fat. As facial fat is situated more inferiorly in the face, the face appears visually longer.The aesthetic consequences of a change in facial shape with aging are as important as the depth of thenasolabialfoldandfacialjowling.Forme,animprovementinfacialshaperemainsoneoftheprimarygoalsin facial rejuvenation. (Reprinted from Stuzin, J. M., Baker, T. J., and Baker, T. M. Refinements in face lifting:EnhancedfacialcontourusingVicrylmeshincorporatedintoSMASfixation.Plast.Reconstr.Surg.105:290,2000.)
Volume 129, Number 5S • Restoring Facial Shape in Face Lifting
41S

cavity and a well-defined mandibular border ac-counts for the angular, tapered appearance of theyouthful face.30
With aging, facial fat descends and facial shapechanges. In middle age, as ligamentous supportbecomes attenuated, facial fat volumetrically be-comes situated anteriorly and inferiorly in thecheek, producing a facial contour that is squarerin configuration with little differential betweenmalar highlights and midfacial fat. As facial fat issituated inferiorly in the face, older faces appearvertically longer than young faces (Fig. 1).
Volume Loss and Facial DeflationYoung faces are full of well-supported facial
fat. Over time, deflation of facial fat occurs andtends to be most apparent in regions of the facewith a high density of retaining ligaments.31,32 Forthis reason, areas noted to be volumetrically full inyouth (malar, preparotid, lateral and infraorbitalrim, and lateral chin) become volumetrically de-flated in middle age. With facial deflation, softtissue becomes less supported and therefore ap-pears lax. Youthful faces have a smooth blending
of contour between the aesthetic subunits of theface. Middle-aged faces, secondary to both defla-tion and facial fat descent, develop lines of de-marcation between one region of the face andanother that is intuitively identified as old. As partof the aesthetic treatment plan to improve facialshape, repositioning descended soft tissue intoareas of facial deflation improves shape, not onlyby restoring volume to the position noted in youthbut also by serving to blunt the lines of demarca-tion that develop with aging. Volumetric additionthrough secondary agents such as autologous fatinjection, dermal fat grafts, or other injectablesoft-tissue fillers can be useful in augmenting areasof facial deflation33,34 (Fig. 2).
Radial ExpansionNot all facial aging is vertical. A major chal-
lenge in facial rejuvenation is the radial expansionof facial soft tissue that occurs along specific areasof the midface. In youth, the skin and underlyingsubcutaneous fat are densely attached to the deepfacial fascia by retinacular fibers that transverseamong skin, subcutaneous fat, and superficial fas-
Fig. 2. (Left) Preoperative appearance of a 42-year-old patient with early facial aging resultingprimarilyfromdeflation.Notethehollowingeffectalongtheinfraorbitalandlateralorbitalrimsandpreparotid region, which are regions of high ligamentous density. (Right) Post-operative resultafter face and neck lift. Note that as anteriorly situated fat is brought into the upper lateral midface,it fills the areas of deflation, thereby blunting the lines of demarcation between aesthetic subunitsthat develop with age. Notice also the change in facial shape, which now appears more structuredand supported following facial fat repositioning.
Plastic and Reconstructive Surgery • Spring 2012
42S

Fig. 3. (Left) Preoperative appearance of a 59-year-old man after a 90-pound weight loss froma gastric bypass procedure. Notice the significant areas of facial deflation along the infraorbitalrim, lateral orbital rim, and malar region. Also notice the radial expansion of skin and fat lateralto the nasolabial fold, most marked on the right side. Not only does malar fat descend, butattenuation of the retinacular connections among skin, fat, and deep facial fascia lateral to thenasolabial line allows prolapse of soft tissue, which accentuates nasolabial prominence. (Right)Postoperatively, the areas of deflation along the infraorbital rim, lateral orbital rim, and malarregion are improved, as facial fat has been repositioned into these regions. The nasolabial foldsare somewhat improved after malar pad repositioning, butcorrection is incomplete, especiallyon the right. Malar pad elevation helps to flatten the prominent nasolabial fold but does littleto correct radial expansion, with the skin lateral to the nasolabial line remaining prolapsedfrom its attachments to the facial skeleton.
Volume 129, Number 5S • Restoring Facial Shape in Face Lifting
43S

cia and insert into the deep fascia and facial mus-culature. Over time, with prolonged animationsuch as smiling, the skin along the nasolabial lineis forced deep to the subcutaneous fat, positionedlateral to the nasolabial fold, attenuating theseretinacular attachments. Prolonged animation,therefore, forces the skin and fat lateral to thenasolabial fold to expand radially and prolapseoutward from the facial skeleton, accounting formuch of the nasolabial fold prominence in theaging face. Radial expansion lateral to the oralcommissure and marionette line similarly ac-counts for some degree of jowl prominence inmany middle-aged patients.31,32 Radial expansionis technically difficult to correct, because there arefew surgical solutions to re-establish the retinacu-lar attachments among skin, subcutaneous fat,and deep fascia. Because of this technical diffi-culty, incomplete correction in these regions iscommonly noted after a face lift, despite heroicefforts at repositioning descended facial fat(Fig. 3).
Role of Skeletal Support in Formulating aSurgical Treatment Plan
Facial shape and contour are intuitively eval-uated when analyzing a patient for facial rejuve-nation. Often the two-dimensional considerationsseen in photographs are the easiest aspects of ag-ing to identify, and such factors as nasolabial folddepth, jowl prominence, and cervical contour be-come the primary objectives to improve appear-ance in the middle-aged face. Although these fac-tors are certainly important considerations intreatment planning, the more subtle three-dimen-sional qualities of facial shape are equally impor-tant to evaluate and are greatly influenced by un-derlying skeletal support.
In evaluating facial shape during preoperativeanalysis, some of the major factors that I havefound helpful to consider are as follows:
1. Facial width, bizygomatic diameter, and malar volume.The emphasis in face lifting over the last 20 yearshas focused on malar pad elevation.6,12,14,15,17–20,28,29
While malar pad elevation and restoration of ma-lar highlights are important factors in improvingfacial shape, they need to be patient specific.Many patients present preoperatively with widefaces, strong malar eminences, and large malarvolume and have little evidence of malar fat de-scent. In these individuals, it is necessary to eval-uate preoperatively the degree of malar pad ele-vation required to improve facial shape. Whilelimited degrees of malar pad elevation can be
helpful in patients who present with wide bizygo-matic diameters, in general, if the malar volumeis significantly enhanced in these types of individ-uals, the aesthetic effect is to make a wide faceappear even wider on the frontal view postoper-atively (Fig. 4).
2. Facial length and the relative vertical heights of thelower and middle thirds of the face. Comparedwith patients with wide faces, patients whopresent with vertical maxillary excess oftenhave long, thin faces on the frontal view. Asfacial fat descends in middle age, it becomessituated anteriorly and inferiorly in the face,and the face appears even longer with age. Malarpad elevation and enhancing malar volume inthese types of patients are usually beneficial. Asmalar volume is enhanced and bizygomatic diam-eter is increased, the face appears wider on thefrontal view, detracting from the relatively exces-sive facial length (Fig. 5).
Fig. 4. Facial width and bizygomatic diameter reflect the under-lying degree of skeletal support. Patients who exhibit a strongmalar eminence and wide bizygomatic diameter often benefitfrom having malar highlights restored, but they usually do notrequire significant enhancement of malar volume (which willcause a wide face to appear wider postoperatively). Shaping con-siderations in these types of faces usually focus on improving theappearance of the lower two-thirds of the cheek, specifically ad-dressing jowl fat repositioning, and creating submalar hollow-ing, which improves the aesthetic relationship between the ma-lar and submalar regions.
Plastic and Reconstructive Surgery • Spring 2012
44S

3. Convexity of the malar region juxtaposed with theconcavity of the submalar region. In youth, facialfat is situated overlying the malar and prepa-rotid regions. This malar fullness is juxta-posed with a concavity within the submalarregion overlying the buccinator. As patientsage, the relationship between the malar and
submalar regions changes, and facial shapechanges with it. As facial fat descends andfacial deflation occurs, there is less volumeoverlying the malar eminence and an associ-ated increase in fullness in the submalar re-gion. As the aesthetic relationship betweenthe malar and submalar regions becomes
Fig. 5. Long,thinfacesoftenbenefitfromanenhancementofmalarvolume.SMASdissectionandfacialfatrepositioningcarriedanteriorlyoverthezygomaticeminenceallowthesurgeontorestoremalar volume, thereby increasing bizygomatic diameter. When malar volume is enhanced, theface appears wider, detracting from the relatively excessive facial length.
Volume 129, Number 5S • Restoring Facial Shape in Face Lifting
45S

Fig. 6. This patient demonstrates that the aesthetic relationship between the malarand submalar regions has a significant effect on facial shape. Youthful faces with atapered configuration typically exhibit a convexity or fullness in the malar region jux-taposed with submalar hollowing.
Fig. 7. Another patient with similar skeletal support photographed at age 51. In middleage, facial fat both descends and deflates, accounting for a change in the relationshipbetween the malar and submalar regions. Typically, there is a loss of volume in the malararea associated with an increase in fullness within the submalar region, blunting therelationship noted in youth. Facial shape becomes less tapered and squarer in config-uration, with less differential in highlights between the malar eminence and the sub-malar fat.
Plastic and Reconstructive Surgery • Spring 2012
46S

Fig. 8. (Left) Preoperative appearance. Note that facial shape is oval, secondary to malar de-flation associated with an increase in submalar fullness. (Right) Postoperatively, following ma-lar pad elevation, malar volume is enhanced in association with a restoration of submalarconcavity, producing a more angular appearance to facial shape.
Fig. 9. (Left) Preoperatively, this patient shows a similar blunting of the relationship betweenthe malar and submalar regions. (Right) Postoperative appearance. Enhancing malar volume(and bizygomatic diameter) and restoring the concavity within the submalar region make theface appear more angular, as well as vertically shorter.
Volume 129, Number 5S • Restoring Facial Shape in Face Lifting
47S

modified with time, there is a loss of theangular, tapered configuration in shapenoted in youth, and middle-aged faces oftenappear oval. With greater facial fat descentand an increase in submalar fullness, olderfaces appear square (Figs. 6 and 7).Preoperatively, an evaluation of the relation-ship between the malar and submalar regionson the frontal view, for me, is an essentialcomponent of aesthetic treatment planning.For many patients, a restoration of this rela-tionship by increasing malar highlights andmalar volume, in association with a restora-tion of concavity in the submalar region, be-comes a central component in improving fa-cial shape (Figs. 8 and 9).
THE VERTICAL HEIGHT OF THEMANDIBULAR RAMUS AND THE
HORIZONTAL LENGTH OFTHE MANDIBULAR BODY
The vertical height of the mandibular ramusand the horizontal length of the mandibular body
provide skeletal support for the lower two-thirds ofthe face. Patients who present with a normal man-dibular ramus height, as well as an adequate hor-izontal length of the mandibular body, usuallyhave excellent skeletal support for soft-tissue re-positioning and are, therefore, less of a surgicalchallenge. In contradistinction, patients with ashort mandibular ramus, an open mandibularplane angle, and a short mandibular body typicallyhave poor skeletal support for midface and peri-oral soft-tissue repositioning. These patients are agreater surgical challenge in restoring facial shapeand often benefit from volumetric augmentation,either alloplastic or autogenous, to enhance skel-etal support (Fig. 10).
TECHNICAL CONSIDERATIONS:PREOPERATIVE PLANNING
My experience in face lifting has centered onutilizing an extended SMAS technique11,20,30 to re-position descended midfacial fat superiorly to theanatomic position of youth. The incision design
Fig. 10. (Left) The underlying skeletal support from the mandible has a significant effect onthe surgeon’s ability to restore facial shape. Patients with a normal height to the mandibularramus and a long mandibular body are favorable surgical candidates, as there is significantskeletal support to aid in shaping through facial fat repositioning. (Right) In patients with aretrusive mandible, a short mandibular ramus associated with an open mandibular plane an-gle, there is less skeletal support to aid in facial shaping. These patients represent a greatersurgical challenge and often benefit from volumetric augmentation.
Plastic and Reconstructive Surgery • Spring 2012
48S

for this dissection is essentially an extension of astandard SMAS dissection anteriorly and superi-orly into the malar region, to allow access for therelease of the zygomatic, upper masseteric, andparotidocutaneous ligaments. Repositioned facialfat, in any subSMAS procedure, ends up beinglocated where it is sutured. For this reason, theincision design I utilize allows the versatility toreposition fat along the infraorbital rim, lateralorbital rim, malar eminence, and preparotid re-gions, depending on the aesthetic needs of thepatient (Fig. 11). Variations in extended SMASincision design, in terms of the superior and me-dial malar extent of the SMAS dissection, providethe surgeon with aesthetic versatility in terms ofrestoration of malar volume and facial width.
The biomechanics of SMAS repositioninghave previously been described and are influ-enced by the degree of release, the vector of fatrepositioning, and how the superficial fascia isfixated.35 As postoperative contour is dependenton each of these factors, preoperative planning
needs to be patient specific in terms of the degreeof SMAS release required, the vectors in whichfacial fat are repositioned, and the location andmethod for SMAS fixation.
RELEASEThe incision design of an extended SMAS dis-
section allows for complete release of the SMASfrom its underlying retaining ligamentous attach-ment in the lateral midface. As surgeons, there isa tendency to believe that a greater degree ofSMAS dissection equates with a better result, butthis has not been my experience. Rather, precisionin the degree of SMAS dissection and its releasefrom the retaining ligaments as dictated by theaesthetic needs of a patient increases surgical con-trol and consistency while minimizing morbidity.30
How much to release the SMAS, and how highand anterior to carry the SMAS dissection, needsto be decided preoperatively. In patients who pres-ent with adequate malar volume, wide bizygomaticdiameter, and little evidence of malar pad descent,it is usually unnecessary to carry the SMAS dissec-tion medial to the lateral orbital rim (although Iusually carry the dissection high within the malareminence to allow fat repositioning along the in-fraorbital and lateral orbital rims). Most com-monly, these patients require only a restoration ofmalar highlight and not significant anterior malarvolume enhancement. Limiting the SMAS dissec-tion to the lateral aspect of the malar eminencewill not increase facial width on the frontal view.Typically, the shaping considerations for these pa-tients are focused on reducing fullness in the sub-malar region. SubSMAS dissection along the lateralaspect of the zygomatic eminence provides exposureto the juxtaposed masseteric ligaments, allowing thesubmalar fat to be repositioned superiorly along theconcavity of the underlying buccinator, thereby re-storing submalar hollowing (Fig. 12).
Vertically long faces often benefit from carryingthe malar portion of the extended SMAS dissectionanteriorly, medial to the lateral orbital rim, so thatmalar volume restoration is performed along theanterior aspect of the zygomatic eminence. Carryingthe SMAS dissection more medially allows the sur-geon to enhance malar volume and restore malarhighlights anteriorly over the zygomatic eminence,thereby increasing facial width on the frontal view(Fig. 13).
VECTORS OF FAT ELEVATION:FACIAL ASYMMETRY
All patients exhibit some degree of facial asym-metry. Commonly, one side of the face is vertically
Fig. 11. The incision design for the extended SMAS dissection isan extension of a standard lateral SMAS dissection. The malaraspect of the dissection allows for the repositioning of facial fatalong the infraorbital and lateral orbital rims, as well as the res-toration of malar volume. The SMAS dissection just lateral to thezygomatic eminence provides access to the masseteric liga-ments to allow jowl fat elevation and restoration of submalarncavity. The dissection laterally in the cheek frees the SMAS fromthe parotid, providing for repositioning of the descended plat-ysma, thereby improving mandibular border contour.
Volume 129, Number 5S • Restoring Facial Shape in Face Lifting
49S

longer, and the short side of the face is usuallywider than the long side. Malar highlights aretypically more superiorly located on the long sideof the face, and with age, facial fat tends to de-scend in a more vertical direction on the long side.As facial asymmetry and facial skeletal configura-tion are asymmetric in most individuals, it followsthat the vectors of fat elevation (SMAS reposition-ing) should be specific for the right and the leftsides of the face.
The vector in which the SMAS is repositionedhas a significant effect on the location and volumeof elevated facial fat, thereby influencing facialshape. Decisions regarding the direction of SMASvectoring for the right and left sides of the face arebest determined preoperatively, as it is very diffi-cult to make aesthetic vector judgments intraop-eratively with the patient recumbent.
SMAS vectors influence postoperative facialshape. Vertical SMAS repositioning typically pro-vides a larger amount of fat for malar eminenceenhancement, as well as allowing for a reductionin fullness within the submalar region as fat isforced vertically along the concavity of the bucci-
nator. For this reason, vertical SMAS vectors areoften indicated to reshape round, full faces, al-lowing them to appear more tapered and thinnerpostoperatively (Fig. 14). If the SMAS is vectoredmore obliquely, less fat volume is brought into themalar region and a greater volume of fat is repo-sitioned into the submalar region. Oblique SMASrepositioning is helpful, therefore, in elderly pa-tients who appear gaunt over the buccal recess, asit allows the surgeon to volumetrically enhancethe submalar region (Fig. 15).
SMAS FIXATIONIn a two-layer SMAS-type face lift, the tension of
contouring is placed on the superficial fascia ratherthan the skin envelope. For this reason, the fascialquality and tensile strength of the superficial fasciahave an influence on both the longevity of the resultand the volume of fat that can be repositioned in-traoperatively and maintained postoperatively. Inother words, soft-tissue quality influences long-termcontour and is the primary reason why face lifts inyoung patients are more predictable.
Fig. 12. Patients with wide bizygomatic diameters and good underlying skeletal supporttypically do not require a significant anterior malar dissection to improve facial shape. Mostcommonly, the SMAS dissection in these patients (while kept high) is extended only as medialas the lateral orbital rim, so that malar volume restoration is limited to the lateral aspect of thezygomatic eminence. The shaping considerations for these types of faces usually emphasizereducing fullness within the submalar area, as well as jowl fat elevation. Notice that postop-eratively the patient’s face appears more tapered and thinner in morphology through facialfat repositioning without removal of facial fat.
Plastic and Reconstructive Surgery • Spring 2012
50S
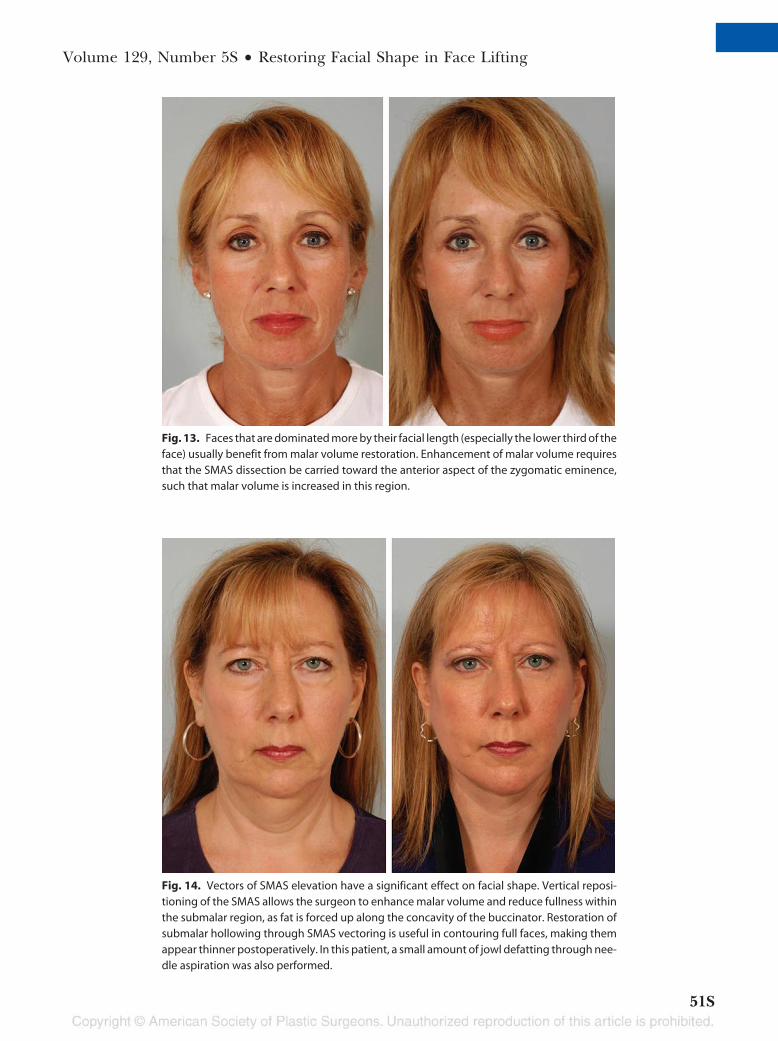
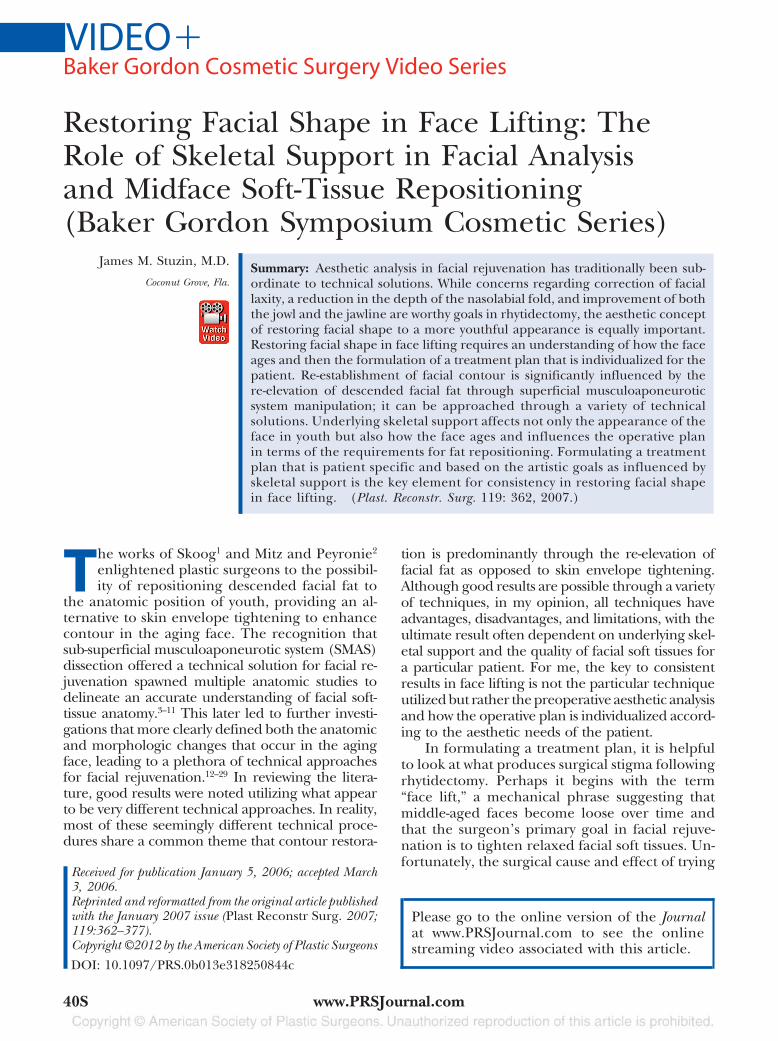
Fig. 13. Faces that are dominated more by their facial length (especially the lower third of theface) usually benefit from malar volume restoration. Enhancement of malar volume requiresthat the SMAS dissection be carried toward the anterior aspect of the zygomatic eminence,such that malar volume is increased in this region.
Fig. 14. Vectors of SMAS elevation have a significant effect on facial shape. Vertical reposi-tioning of the SMAS allows the surgeon to enhance malar volume and reduce fullness withinthe submalar region, as fat is forced up along the concavity of the buccinator. Restoration ofsubmalar hollowing through SMAS vectoring is useful in contouring full faces, making themappear thinner postoperatively. In this patient, a small amount of jowl defatting through nee-dle aspiration was also performed.
Volume 129, Number 5S • Restoring Facial Shape in Face Lifting
51S

In an effort to improve fascial quality in aSMAS-type face lift, for the last 10 years I haveincorporated Vicryl mesh into the SMASfixation.30 It is my observation that incorporatingVicryl mesh into SMAS fixation not only improvesthe longevity of these procedures but provides thesurgeon with greater aesthetic control in terms ofrestoring facial shape. Incorporating the Vicrylmesh allows the surgeon to secure the SMAS un-der greater tension (while preventing the su-tures from “cheese-wiring” through the SMAS),which allows the surgeon to reposition a greatervolume of fat into specific regions of the mid-face. Greater control in fixating repositioned fatprovides greater control in restoring facialshape (Fig. 16).
If malar volume requires enhancement, oncethe SMAS is initially fixated, adding a few more su-tures between the SMAS flap and the periosteum ofthe malar eminence allows the surgeon to imbricatemore malar fat superiorly over the zygoma, therebyincreasing malar volume. Essentially, this type ofstacking fixation imbricates malar fat onto bothmesh and zygomatic eminence, aesthetically result-ing in an increase in bizygomatic diameter.
If the predominant aesthetic problem is toreduce fullness within the submalar region, SMAS
release of the upper masseteric ligaments and ver-tically vectoring the SMAS tend to increase sub-malar hollowing. Adding fixation sutures justlateral to the malar eminence also accentuatessubmalar concavity. This method of SMAS vector-ing and fixation is useful in shaping round, fullfaces without having to overly rely on the removalof facial fat to improve facial shape.
Suturing in the preparotid region repositionsdescended platysma muscle superiorly over themandibular border, thereby accentuating man-dibular border and cervical contour. Adding su-tures into the SMAS fixation along the preparotidregion is also useful in providing volumetric en-hancement laterally in the cheek, improving anaesthetic subunit that typically deflates with age.
AESTHETIC EFFECT OF STRONGVERTICAL SKIN TENSION ON
FACIAL SHAPEStrong, vertical shifting of the cervicofacial flap
has traditionally been a maneuver utilized in manyface lift techniques. While skin envelope tighteningcan produce a dramatic effect in terms of the im-provement of facial laxity, the aesthetic effects ofvertical skin shift on facial shape have been poorlydelineated. Specifically, when skin is shifted in a
Fig. 15. This patient exhibits asymmetry in the submalar region preoperatively. Notice thatshe appears hollow and concave on the right, while she is fuller on the left side. For this reason,the SMAS was vectored obliquely on the right to volumetrically enhance the submalar re-gion, while it was vertically vectored on the left side to restore submalar hollowing andbalance the two sides of her face.
Plastic and Reconstructive Surgery • Spring 2012
52S

cephalad direction, the effect of skin tension com-monly produces a depression or flatness in thepreparotid region, an area that typically deflates withaging (Fig. 17). If the preparotid region remainsdeflated despite fat repositioning, vertical skin vec-toring will further depress and flatten this region. Inmy opinion, vertical skin shift all too often producesan unnatural tightness to facial shape, producing thetypical stigma associated with rhytidectomy. If thesurgeon has been successful in enhancing contourthrough repositioning descended facial fat, the useof strong vertical skin tension is neither desirable nornecessary to enhance the postoperative result.
CONCLUSIONSThirty years after the milestone work of Mitz and
Peyronie,2 plastic surgeons continue to struggle intheir quest for a perfect solution to rejuvenate theaging face. Over this time period, the surgical spec-
trum has swung from wide skin and SMAS dissectionto short-scar face lifts with imbrication or SMAS re-section, in an attempt to limit morbidity while im-proving consistency in results.23,36
In my opinion, surgical rejuvenation of the agingface suffers not from inadequate technical solutionsbut rather from the absence of a uniform method ofpreoperative analysis. Unlike rhinoplasty, in whichpreoperative analysis is defined by angles and mea-surements of length and projection, aging faces varygreatly in terms of skeletal support, volume of fat,fascial quality, and skin quality. The variability offacial shape from patient to patient, as well as howindividual patients age, makes a uniform system ofanalysis difficult. Artistic vision and artistic goals, asto what will aesthetically improve for a particularpatient, are also surgeon specific.
From my perspective, independent of tech-nique, the primary goal in face lifting is to improvefacial appearance while minimizing signs that asurgical procedure has been performed. Under-standing the nuances of superficial fascia reposi-tioning (repositioning facial fat), whether it beutilizing imbrication, SMAS resection, or formal
Fig. 16. Fixation of the superficial fascia affects facial shape. Theadvantage of incorporating Vicryl mesh into the SMAS fixation isthat it provides the surgeon with greater control in determiningthe position and volume of repositioned fat. Suturing in specificareas along the SMAS incision affects volume for a particular re-gion. Adding sutures in the malar region allows the surgeon tobring a greater amount of malar fat onto the zygomatic emi-nence, thereby enhancing malar volume. Adding sutures in theregion just lateral to the zygomatic eminence forces cheek fatsuperiorly along the concavity of the buccinator, thereby reduc-ing submalar fullness. Sutures placed in the preparotid regionforce descended platysma superiorly over the mandibular bor-der, thereby improving mandibular border contour.
Fig. 17. The aesthetic consequences of vertical redraping of thecervicofacial skin flap are much different from those for verticalSMAS redraping. Strong vertical shift of the skin flap not only pro-duces temporal hairline distortion but accentuates flatness in thepreparotidregion(whichtypicallydeflateswithage).Lateralflatnesscan produce a tight, unnatural appearance all too commonly asso-ciated with patients having undergone a rhytidectomy.
Volume 129, Number 5S • Restoring Facial Shape in Face Lifting
53S

SMAS flap elevation, provides the surgeon withonly a mechanism to restore facial shape. What iscritical to the end result is preoperative analysisand accurately delineating the aesthetic goals be-fore surgery. Formulating a treatment plan to re-store facial shape that is patient specific and basedon the volumetric requirements as influenced byunderlying skeletal support is the key element toincreasing consistency in face lifting. The techni-cal solution thereby becomes subservient to theaesthetic destination. Good surgeons can get goodresults through a variety of techniques as long asthere is an understanding of how to vary techniqueaccording to the aesthetic needs of the patient.
James M. Stuzin, M.D.3225 Aviation Avenue, Suite 100
Coconut Grove, Fla. [email protected]
DISCLOSUREThe author has no financial interests in any of the
products, devices, or drugs mentioned in this article.
REFERENCES1. Skoog, T. Plastic Surgery: New Methods and Refinements. Phila-
delphia: Saunders, 1974.2. Mitz, V., and Peyronie, M. The superficial musculoaponeu-
rotic system (SMAS) in the parotid and cheek area. Plast.Reconstr. Surg. 58: 80, 1976.
3. Lemmon, M. L., and Hamra, S. T. Skoog rhytidectomy: Afive-year experience with 577 patients. Plast. Reconstr. Surg.65: 283, 1980.
4. Owsley, J. Q., Jr. SMAS-platysma face lift: A bidirectionalcervicofacial rhytidectomy. Clin. Plast. Surg. 10: 429, 1983.
5. Jost, G., and Levet, Y. Parotid fascia and face lifting: A criticalevaluation of the SMAS concept. Plast. Reconstr. Surg. 74: 42, 1984.
6. Bosse, J. P., and Pappillon, J. Surgical anatomy of the SMASat the malar region. In Transactions of the 9th InternationalCongress of Plastic and Reconstructive Surgery. New York:McGraw-Hill, 1987. P. 348.
7. Ruess, W., and Owsley, J. Q. The anatomy of the skin and fasciallayers of the face in aesthetic surgery. Plast. Reconstr. Surg. 14: 677,1987.
8. Freilinger, G., Gruber, H., Happak, W., and Pechmann, U.Surgical anatomy of the mimic muscle system and the facialnerve: Importance for reconstructive and aesthetic surgery.Plast. Reconstr. Surg. 80: 686, 1987.
9. Furnas, D. W. The retaining ligaments of the cheek. Plast.Reconstr. Surg. 83: 11, 1989.
10. Thaller, S. R., Kim, S., Patterson, H., et al. The submuscularaponeurotic system (SMAS): A histologic and comparativeanatomy evaluation. Plast. Reconstr. Surg. 86: 690, 1990.
11. Stuzin, J. M., Baker, T. J., and Gordon, H. L. The relationshipof the superficial and deep facial fascias: Relevance to rhyt-idectomy and aging. Plast. Reconstr. Surg. 89: 441, 1992.
12. Hamra, S. T. The deep plane rhytidectomy. Plast. Reconstr.Surg. 86: 53, 1990.
13. Lambros, V. Fat contouring in the face and neck. Clin. Plast.Surg. 19: 401, 1992.
14. Mendelson, B. Correction of the nasolabial fold: ExtendedSMAS dissection with periosteal fixation. Plast. Reconstr. Surg.89: 822, 1992.
15. Barton, F. E., Jr. Rhytidectomy and the nasolabial fold. Plast.Reconstr. Surg. 90: 601, 1992.
16. Hamra, S. T. Composite rhytidectomy. Plast. Reconstr. Surg.90: 1, 1992.
17. Owsley, J. Q., Jr. Lifting the malar fat pad for correction of prom-inent nasolabial folds. Plast. Reconstr. Surg. 91: 463, 1993.
18. Connell, B. F., and Marten, T. J. The trifurcated SMAS flap:Three-part segmentation of the conventional flap for im-proved results in the midface, cheek and neck. Aesthetic Plast.Surg. 19: 415, 1995.
19. Ramirez, O. M. The subperiosteal approach for the correc-tion of the deep nasolabial fold and the central third of theface. Clin. Plast. Surg. 22: 341, 1995.
20. Stuzin, J. M., Baker, T. J., Gordon, H. L., and Baker, T. M.Extended SMAS dissection as an approach to midface reju-venation. Clin. Plast. Surg. 22: 295, 1995.
21. Baker, T. J., Gordon, H. L., and Stuzin, J. M. Surgical Reju-venation of the Face. 2nd Ed. St. Louis, Mo.: Mosby, 1996.
22. Marten, T. J. Face lifting planning and technique. Clin. Plast.Surg. 24: 269, 1997.
23. Baker, D. C. Lateral SMASectomy. Plast. Reconstr. Surg. 100: 509,1997.
24. Barton, F. E., Jr., and Kenkel, J. M. Direct fixation of themalar pad. Clin. Plast. Surg. 24: 329, 1997.
25. Hester, T. R. The trans-blepharoplasty approach to lower lidand midfacial rejuvenation revisited: The role and techniqueof canthoplasty. Aesthetic Surg. J. 18: 372, 1998.
26. Aston, S. J. Face lift with FAME technique. Presented at the32nd Annual Baker Gordon Symposium on Cosmetic Sur-gery, Mercy Hospital, Miami, Fla., February 1998.
27. Hamra, S. T. The zygorbicular dissection in composite rhytidec-tomy: An ideal midface plane. Plast. Reconstr. Surg. 102: 1646, 1998.
28. Little, J. W. Volumetric perceptions in midfacial aging with alteredpriorities for rejuvenation. Plast. Reconstr. Surg. 105: 252, 2000.
29. Little, J. W. Three-dimensional rejuvenation of the midface:Volumetric resculpture by malar imbrication. Plast. Reconstr.Surg. 105: 267, 2000.
30. Stuzin, J. M., Baker, T. J., and Baker, T. M. Refinements inface lifting: Enhanced facial contour using Vicryl mesh in-corporated into SMAS fixation. Plast. Reconstr. Surg. 105: 290,2000.
31. Lambros, V. S. Personal communication. 1999.32. Lambros, V. S. The kinetic changes associated with aging of
the upper eyelids, brow and forehead. Presented at the 37thAnnual Baker Gordon Symposium on Cosmetic Surgery,Miami, Fla., February 6, 2003.
33. Coleman, S. R. Structural Fat Grafting. St. Louis, Mo.: QualityMedical Publishing, 2004.
34. Coleman, S. R. Structural fat grafting. In F. Nahai (Ed.), TheArt of Anesthetic Surgery. St. Louis, Mo.: Quality Medical Pub-lishing, 2005. P. 289.
35. Mendelson, B. Surgery of the superficial musculoaponeuro-tic system: Principles of release, vectors, and fixation. Plast.Reconstr. Surg. 107: 1545, 2001.
36. Tonnard, P. L., Verpaele, A., and Gaia, S. Optimising resultsfrom minimal access cranial suspension lifting (MACS-Lift).Aesthetic Plast. Surg. 29: 213, 2005.
Plastic and Reconstructive Surgery • Spring 2012
54S

The video for this article was graciously provided by the Baker Gordon Cosmetic Surgery Symposiumarchives, and was edited for length and content from the full-length video. If you enjoyed this video,we encourage you to visit the Advanced Search page of the ASPS online store and type in �BakerGordon� in the description search box (http://www1.plasticsurgery.org/ebusiness4/ProductCatalog/FindProducts.aspx).
Volume 129, Number 5S • Restoring Facial Shape in Face Lifting
55S


![Berrant Facial Nerve Regeneration, Double-blind, Placebo-controlled Trial Using Subjective Endpoints. Plast Reconstr Surg 2005. 116, 36-43[2]](https://static.fdocuments.in/doc/165x107/577ce6c31a28abf10393818f/berrant-facial-nerve-regeneration-double-blind-placebo-controlled-trial-using.jpg)















