Venous Thromboembolism Prophylaxis
13
Mackay Hospital and Health Service PROCEDURE Document ID: C-PRO 111 V3.1 VENOUS THROMBOEMBOLISM PROPHYLAXIS MACKAY HOSPITAL AND HEALTH SERVICE 1. Purpose • Patients of the Mackay Hospital and Health Service (MHHS) should receive best practice care to prevent or minimise the impact of venous thromboembolism (VTE). • VTE prophylaxis includes appropriate risk assessment on admission to hospital and at regular intervals during the inpatient stay. If a VTE does occur the treatment should be optimised to prevent adverse outcomes by: o Appropriate use of the selection, timing and duration of antithrombotic agent(s); o Appropriate use of mechanical compression devices. 2. Scope This procedure applies to all staff of the MHHS who are mandated to assess every patient for the risk factors of VTE and implement a plan of care or document why the patient has not been prescribed the correct treatment. 3. Procedure for Venous Thromboembolism Prevention Assess the Risk of VTE On admission, all inpatients are to be assessed for the risk of developing VTE by the Medical Officer (MO), using the risk factors identified in this procedure. Once assessed, the risk should be marked on the VTE pre-printed order in the Medication Chart and documented in the patient’s Medical Record. Separate protocols exist for Medical, Surgical, Orthopaedic, Hip Fracture, and Intensive Care. Consider Risk: Benefit Ratio of Prophylaxis Consider contraindications to prophylaxis, including the risk of bleeding. If contraindications exist, document on the VTE pre-printed order in the Medication Chart and the patient’s Medical Record. Custodian/Review Officer: Clinical Directors Version no: V3.1 Applicable To: All Medical Staff Approval Date: 15/05/2017 Effective Date: 19/05/2017 Next Review Date: 16/05/2020 Approving Officer/s: Professor Philip Reasbeck Executive Director Medical Services Date: 15 May 2017 Supersedes: C-PRO 111 V2.0 (2014); C-PRO 111 V3.0 (2017) Key Words: VTE, Thromboembolism Prophylaxis Accreditation References: EQuIP National NS 3 11,12 Printed Copies are Uncontrolled Page 1 of 13
Transcript of Venous Thromboembolism Prophylaxis
Mackay Hospital and Health Service
PROCEDURE Document ID: C-PRO 111 V3.1
VENOUS THROMBOEMBOLISM PROPHYLAXIS MACKAY HOSPITAL AND HEALTH SERVICE
1. Purpose • Patients of the Mackay Hospital and Health Service
(MHHS) should receive best practice care to prevent or minimise the impact of venous thromboembolism (VTE).
• VTE prophylaxis includes appropriate risk assessment on admission to hospital and at regular intervals during the inpatient stay. If a VTE does occur the treatment should be optimised to prevent adverse outcomes by: o Appropriate use of the selection, timing and duration
of antithrombotic agent(s); o Appropriate use of mechanical compression
devices. 2. Scope This procedure applies to all staff of the MHHS who are mandated to assess every patient for the risk factors of VTE and implement a plan of care or document why the patient has not been prescribed the correct treatment. 3. Procedure for Venous Thromboembolism
Prevention Assess the Risk of VTE On admission, all inpatients are to be assessed for the risk of developing VTE by the Medical Officer (MO), using the risk factors identified in this procedure. Once assessed, the risk should be marked on the VTE pre-printed order in the Medication Chart and documented in the patient’s Medical Record. Separate protocols exist for Medical, Surgical, Orthopaedic, Hip Fracture, and Intensive Care. Consider Risk: Benefit Ratio of Prophylaxis Consider contraindications to prophylaxis, including the risk of bleeding. If contraindications exist, document on the VTE pre-printed order in the Medication Chart and the patient’s Medical Record.
Custodian/Review Officer: Clinical Directors Version no: V3.1 Applicable To: All Medical Staff Approval Date: 15/05/2017 Effective Date: 19/05/2017 Next Review Date: 16/05/2020 Approving Officer/s: Professor Philip Reasbeck Executive Director Medical Services Date: 15 May 2017 Supersedes: C-PRO 111 V2.0 (2014); C-PRO 111 V3.0 (2017) Key Words: VTE, Thromboembolism Prophylaxis Accreditation References: EQuIP National NS 3 11,12
Printed Copies are Uncontrolled Page 1 of 13
Procedure: Venous Thromboembolism Prophylaxis
Mackay Hospital and Health Service
Prescribe Appropriate Prophylaxis In Medication Chart. • If unsure, discuss with a registrar or consultant. • If deviating from the protocol, document reason(s) in the Patient’s Medical Record and
on the VTE pre-printed order in the Medication Chart. • If using Graduated Compression Stockings (GCS), refer to the Guidelines for
Graduated Compression Stockings. Consider use of Traction Socks (Anti-slip Socks) over GCS to prevent slipping on floors. Intermittent Pneumatic Compression (IPC) may include the use of devices which provide compression of the calves or feet.
• Consider foot compression if GCS or calf compression cuffs are not able to be correctly sized or are contraindicated.
Prepare for Discharge • The duration of prophylaxis is important. • In high risk patients duration of prophylaxis is recommended to be a minimum of 5
days. • If the acute condition is unresolved and the patient is not fully ambulant after 5 days,
prophylaxis should continue. Increasingly patients are being discharged early to continue their recuperation at home and may not be fully mobilising.
• It is important to be cautious with early discharge patients that may be convalescing and therefore still at risk of VTE, extended prophylaxis may be indicated.
• High risk patient groups where the value of extended prophylaxis should be continued for 4-6 weeks include patients following hip fracture or hip replacement and major curative cancer surgery, or 10-14 days in the case of knee replacement surgery. Obese or inactive patients who may be slow to ambulate will need to be assessed in this group and the duration of therapy planned.
• Where extended prophylaxis is indicated on discharge from hospital and where CrCL <30ml/min or bodyweight <50kg, consider an adjusted dose of dalteparin 2500 units daily on discharge.
• Ensure VTE prophylaxis is documented on the discharge summary and the plan of care is clearly articulated with clear instructions for ongoing care.
• Ensure patient is educated re signs and symptoms of VTE and return to care if concerned.
Obstetric Note Refer to Queensland state guidelines on VTE in pregnancy. These can be accessed at this link; http://www.health.qld.gov.au/qcg/documents/g-vte.pdf.
Printed Copies are Uncontrolled Page 2 of 13
Procedure: Venous Thromboembolism Prophylaxis
Mackay Hospital and Health Service
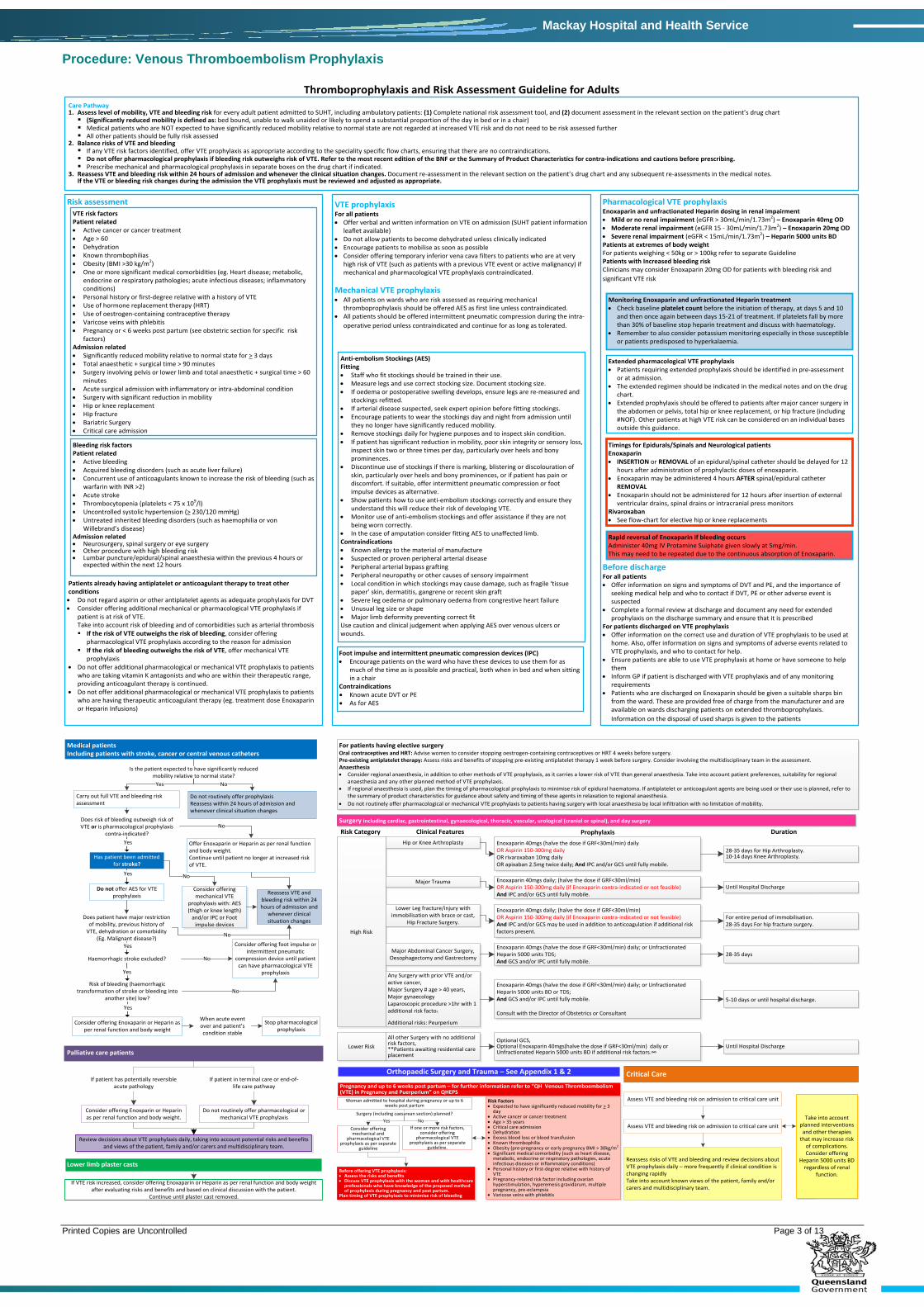
Thromboprophylaxis and Risk Assessment Guideline for AdultsCare Pathway1. Assess level of mobility, VTE and bleeding risk for every adult patient admitted to SUHT, including ambulatory patients: (1) Complete national risk assessment tool, and (2) document assessment in the relevant section on the patient’s drug chart (Significantly reduced mobility is defined as: bed bound, unable to walk unaided or likely to spend a substantial proportion of the day in bed or in a chair) Medical patients who are NOT expected to have significantly reduced mobility relative to normal state are not regarded at increased VTE risk and do not need to be risk assessed further All other patients should be fully risk assessed
2. Balance risks of VTE and bleeding If any VTE risk factors identified, offer VTE prophylaxis as appropriate according to the speciality specific flow charts, ensuring that there are no contraindications. Do not offer pharmacological prophylaxis if bleeding risk outweighs risk of VTE. Refer to the most recent edition of the BNF or the Summary of Product Characteristics for contra-indications and cautions before prescribing. Prescribe mechanical and pharmacological prophylaxis in separate boxes on the drug chart if indicated.
3. Reassess VTE and bleeding risk within 24 hours of admission and whenever the clinical situation changes. Document re-assessment in the relevant section on the patient’s drug chart and any subsequent re-assessments in the medical notes. If the VTE or bleeding risk changes during the admission the VTE prophylaxis must be reviewed and adjusted as appropriate.
Risk assessmentVTE risk factors Patient related• Active cancer or cancer treatment• Age > 60• Dehydration• Known thrombophilias• Obesity (BMI >30 kg/m2) • One or more significant medical comorbidities (eg. Heart disease; metabolic,
endocrine or respiratory pathologies; acute infectious diseases; inflammatory conditions)
• Personal history or first-degree relative with a history of VTE• Use of hormone replacement therapy (HRT) • Use of oestrogen-containing contraceptive therapy• Varicose veins with phlebitis• Pregnancy or < 6 weeks post partum (see obstetric section for specific risk
factors) Admission related• Significantly reduced mobility relative to normal state for > 3 days• Total anaesthetic + surgical time > 90 minutes• Surgery involving pelvis or lower limb and total anaesthetic + surgical time > 60
minutes• Acute surgical admission with inflammatory or intra-abdominal condition• Surgery with significant reduction in mobility• Hip or knee replacement• Hip fracture• Bariatric Surgery• Critical care admission
Bleeding risk factors Patient related• Active bleeding • Acquired bleeding disorders (such as acute liver failure) • Concurrent use of anticoagulants known to increase the risk of bleeding (such as
warfarin with INR >2) • Acute stroke • Thrombocytopenia (platelets < 75 x 109/l)• Uncontrolled systolic hypertension (> 230/120 mmHg) • Untreated inherited bleeding disorders (such as haemophilia or von
Willebrand’s disease) Admission related• Neurosurgery, spinal surgery or eye surgery• Other procedure with high bleeding risk • Lumbar puncture/epidural/spinal anaesthesia within the previous 4 hours or
expected within the next 12 hours
Patients already having antiplatelet or anticoagulant therapy to treat other conditions • Do not regard aspirin or other antiplatelet agents as adequate prophylaxis for DVT • Consider offering additional mechanical or pharmacological VTE prophylaxis if
patient is at risk of VTE. Take into account risk of bleeding and of comorbidities such as arterial thrombosis If the risk of VTE outweighs the risk of bleeding, consider offering
pharmacological VTE prophylaxis according to the reason for admission If the risk of bleeding outweighs the risk of VTE, offer mechanical VTE
prophylaxis• Do not offer additional pharmacological or mechanical VTE prophylaxis to patients
who are taking vitamin K antagonists and who are within their therapeutic range, providing anticoagulant therapy is continued.
• Do not offer additional pharmacological or mechanical VTE prophylaxis to patients who are having therapeutic anticoagulant therapy (eg. treatment dose Enoxaparin or Heparin Infusions)
Anti-embolism Stockings (AES) Fitting• Staff who fit stockings should be trained in their use. • Measure legs and use correct stocking size. Document stocking size. • If oedema or postoperative swelling develops, ensure legs are re-measured and
stockings refitted. • If arterial disease suspected, seek expert opinion before fitting stockings.• Encourage patients to wear the stockings day and night from admission until
they no longer have significantly reduced mobility. • Remove stockings daily for hygiene purposes and to inspect skin condition. • If patient has significant reduction in mobility, poor skin integrity or sensory loss,
inspect skin two or three times per day, particularly over heels and bony prominences.
• Discontinue use of stockings if there is marking, blistering or discolouration of skin, particularly over heels and bony prominences, or if patient has pain or discomfort. If suitable, offer intermittent pneumatic compression or foot impulse devices as alternative.
• Show patients how to use anti-embolism stockings correctly and ensure they understand this will reduce their risk of developing VTE.
• Monitor use of anti-embolism stockings and offer assistance if they are not being worn correctly.
• In the case of amputation consider fitting AES to unaffected limb. Contraindications• Known allergy to the material of manufacture• Suspected or proven peripheral arterial disease• Peripheral arterial bypass grafting• Peripheral neuropathy or other causes of sensory impairment• Local condition in which stockings may cause damage, such as fragile ‘tissue
paper’ skin, dermatitis, gangrene or recent skin graft• Severe leg oedema or pulmonary oedema from congrestive heart failure• Unusual leg size or shape• Major limb deformity preventing correct fitUse caution and clinical judgement when applying AES over venous ulcers or wounds.
VTE prophylaxis For all patients • Offer verbal and written information on VTE on admission (SUHT patient information
leaflet available) • Do not allow patients to become dehydrated unless clinically indicated• Encourage patients to mobilise as soon as possible• Consider offering temporary inferior vena cava filters to patients who are at very
high risk of VTE (such as patients with a previous VTE event or active malignancy) if mechanical and pharmacological VTE prophylaxis contraindicated.
Mechanical VTE prophylaxis• All patients on wards who are risk assessed as requiring mechanical
thromboprophylaxis should be offered AES as first line unless contraindicated. • All patients should be offered intermittent pneumatic compression during the intra-
operative period unless contraindicated and continue for as long as tolerated.
Foot impulse and intermittent pneumatic compression devices (IPC)• Encourage patients on the ward who have these devices to use them for as
much of the time as is possible and practical, both when in bed and when sitting in a chair
Contraindications• Known acute DVT or PE• As for AES
Pharmacological VTE prophylaxis Enoxaparin and unfractionated Heparin dosing in renal impairment • Mild or no renal impairment (eGFR > 30mL/min/1.73m2) – Enoxaparin 40mg OD • Moderate renal impairment (eGFR 15 - 30mL/min/1.73m2) – Enoxaparin 20mg OD• Severe renal impairment (eGFR < 15mL/min/1.73m2) – Heparin 5000 units BDPatients at extremes of body weight For patients weighing < 50kg or > 100kg refer to separate GuidelinePatients with Increased bleeding risk Clinicians may consider Enoxaparin 20mg OD for patients with bleeding risk and significant VTE risk
Monitoring Enoxaparin and unfractionated Heparin treatment• Check baseline platelet count before the initiation of therapy, at days 5 and 10
and then once again between days 15-21 of treatment. If platelets fall by more than 30% of baseline stop heparin treatment and discuss with haematology.
• Remember to also consider potassium monitoring especially in those susceptible or patients predisposed to hyperkalaemia.
Extended pharmacological VTE prophylaxis• Patients requiring extended prophylaxis should be identified in pre-assessment
or at admission. • The extended regimen should be indicated in the medical notes and on the drug
chart. • Extended prophylaxis should be offered to patients after major cancer surgery in
the abdomen or pelvis, total hip or knee replacement, or hip fracture (including #NOF). Other patients at high VTE risk can be considered on an individual bases outside this guidance.
Timings for Epidurals/Spinals and Neurological patientsEnoxaparin • INSERTION or REMOVAL of an epidural/spinal catheter should be delayed for 12
hours after administration of prophylactic doses of enoxaparin. • Enoxaparin may be administered 4 hours AFTER spinal/epidural catheter
REMOVAL• Enoxaparin should not be administered for 12 hours after insertion of external
ventricular drains, spinal drains or intracranial press monitorsRivaroxaban• See flow-chart for elective hip or knee replacements
Rapid reversal of Enoxaparin if bleeding occursAdminister 40mg IV Protamine Suiphate given slowly at 5mg/min.This may need to be repeated due to the continuous absorption of Enoxaparin.
Before discharge For all patients• Offer information on signs and symptoms of DVT and PE, and the importance of
seeking medical help and who to contact if DVT, PE or other adverse event is suspected
• Complete a formal review at discharge and document any need for extended prophylaxis on the discharge summary and ensure that it is prescribed
For patients discharged on VTE prophylaxis• Offer information on the correct use and duration of VTE prophylaxis to be used at
home. Also, offer information on signs and symptoms of adverse events related to VTE prophylaxis, and who to contact for help.
• Ensure patients are able to use VTE prophylaxis at home or have someone to help them
• Inform GP if patient is discharged with VTE prophylaxis and of any monitoring requirements
• Patients who are discharged on Enoxaparin should be given a suitable sharps bin from the ward. These are provided free of charge from the manufacturer and are available on wards discharging patients on extended thromboprophylaxis. Information on the disposal of used sharps is given to the patients
Medical patientsIncluding patients with stroke, cancer or central venous catheters
Is the patient expected to have significantly reduced mobility relative to normal state?
Carry out full VTE and bleeding risk assessment
Do not routinely offer prophylaxisReassess within 24 hours of admission and whenever clinical situation changes
Offer Enoxaparin or Heparin as per renal function and body weight. Continue until patient no longer at increased risk of VTE.
Does risk of bleeding outweigh risk of VTE or is pharmacological prophylaxis
contra-indicated?
Has patient been admitted for stroke?
Do not offer AES for VTE prophylaxis
Does patient have major restriction of mobility, previous history of
VTE, dehydration or comorbidity (Eg. Malignant disease?)
Haemorrhagic stroke excluded?
Risk of bleeding (haemorrhagic transformation of stroke or bleeding into
another site) low?
Yes
Yes
Yes
Yes
Consider offering Enoxaparin or Heparin as per renal function and body weight
Yes
For patients having elective surgeryOral contraceptives and HRT: Advise women to consider stopping oestrogen-containing contraceptives or HRT 4 weeks before surgery. Pre-existing antiplatelet therapy: Assess risks and benefits of stopping pre-existing antiplatelet therapy 1 week before surgery. Consider involving the multidisciplinary team in the assessment. Anaesthesia• Consider regional anaesthesia, in addition to other methods of VTE prophylaxis, as it carries a lower risk of VTE than general anaesthesia. Take into account patient preferences, suitability for regional
anaesthesia and any other planned method of VTE prophylaxis.• If regional anaesthesia is used, plan the timing of pharmacological prophylaxis to minimise risk of epidural haematoma. If antiplatelet or anticoagulant agents are being used or their use is planned, refer to
the summary of product characteristics for guidance about safety and timing of these agents in relaxation to regional anaesthesia. • Do not routinely offer pharmacological or mechanical VTE prophylaxis to patients having surgery with local anaesthesia by local infiltration with no limitation of mobility.
No
When acute event over and patient’s condition stable
Stop pharmacological prophylaxis
Consider offering foot impulse or intermittent pneumatic
compression device until patient can have pharmacological VTE
prophylaxis
No
No
Reassess VTE and bleeding risk within 24 hours of admission and
whenever clinical situation changes
Consider offering mechanical VTE
prophylaxis with: AES (thigh or knee length)
and/or IPC or Foot impulse devices
No
No
NoYes
Palliative care patients
If patient has potentially reversible acute pathology
If patient in terminal care or end-of-life care pathway
Consider offering Enoxparin or Heparin as per renal function and body weight.
Do not routinely offer pharmacological or mechanical VTE prophylaxis
Review decisions about VTE prophylaxis daily, taking into account potential risks and benefits and views of the patient, family and/or carers and multidisciplinary team.
Lower limb plaster casts
If VTE risk increased, consider offering Enoxaparin or Heparin as per renal function and body weight after evaluating risks and benefits and based on clinical discussion with the patient.
Continue until plaster cast removed.
Surgery including cardiac, gastrointestinal, gynaecological, thoracic, vascular, urological (cranial or spinal), and day surgery
No
Pregnancy and up to 6 weeks post partum – for further information refer to “QH Venous Thromboembolism (VTE) in Pregnancy and Puerperium” on QHEPS
Woman admitted to hospital during pregnancy or up to 6 weeks post partum
Before offering VTE prophylaxis: • Assess the risks and benefits• Discuss VTE prophylaxis with the woman and with healthcare
professionals who have knowledge of the proposed method of prophylaxis during pregnancy and post partum.
Plan timing of VTE prophylaxis to minimise risk of bleeding
Risk Factors• Expected to have significantly reduced mobility for > 3
day• Active cancer or cancer treatment• Age > 35 years• Critical care admission• Dehydration • Excess blood loss or blood transfusion• Known thrombophilia• Obesity (pre-pregnancy or early pregnancy BMI > 30kg/m2
• Significant medical comorbidity (such as heart disease, metabolic, endocrine or respiratory pathologies, acute infectious diseases or inflammatory conditions)
• Personal history or first-degree relative with history of VTE
• Pregnancy-related risk factor including ovarian hyperstimulation, hyperemesis gravidarum, multiple pregnancy, pre-eclampsia
• Varicose veins with phlebitis
Surgery (including caesarean section) planned?
Consider offering mechanical and
pharmacological VTE prophylaxis as per separate
guideline
If one or more risk factors, consider offering
pharmacological VTE prophylaxis as per separate
guideline.
Yes
Critical Care
Assess VTE and bleeding risk on admission to critical care unit
Assess VTE and bleeding risk on admission to critical care unit
Reassess risks of VTE and bleeding and review decisions about VTE prophylaxis daily – more frequently if clinical condition is changing rapidlyTake into account known views of the patient, family and/or carers and multidisciplinary team.
Take into account planned interventions
and other therapies that may increase risk
of complications. Consider offering
Heparin 5000 units BD regardless of renal
function.
Orthopaedic Surgery and Trauma – See Appendix 1 & 2
High Risk
Hip or Knee Arthroplasty Enoxaparin 40mgs (halve the dose if GRF<30ml/min) daily OR Aspirin 150-300mg daily OR rivaroxaban 10mg daily OR apixaban 2.5mg twice daily; And IPC and/or GCS until fully mobile.
28-35 days for Hip Arthroplasty. 10-14 days Knee Arthroplasty.
Major Trauma Enoxaparin 40mgs daily; (halve the dose if GRF<30ml/min)OR Aspirin 150-300mg daily (if Enoxaparin contra-indicated or not feasible)And IPC and/or GCS until fully mobile.
Until Hospital Discharge
Enoxaparin 40mgs daily; (halve the dose if GRF<30ml/min)OR Aspirin 150-300mg daily (if Enoxaparin contra-indicated or not feasible)And IPC and/or GCS may be used in addition to anticoagulation if additional risk factors present.
For entire period of immobilisation. 28-35 days For hip fracture surgery.
Lower Leg fracture/injury with immobilisation with brace or cast,
Hip Fracture Surgery.
Major Abdominal Cancer Surgery, Oesophagectomy and Gastrectomy
Enoxaparin 40mgs (halve the dose if GRF<30ml/min) daily; or Unfractionated Heparin 5000 units TDS; And GCS and/or IPC until fully mobile.
28-35 days
Any Surgery with prior VTE and/or active cancer, Major Surgery # age > 40 years, Major gynaecology Laparoscopic procedure >1hr with 1 additional risk factor.
Additional risks: Peurperium
Enoxaparin 40mgs (halve the dose if GRF<30ml/min) daily; or Unfractionated Heparin 5000 units BD or TDS; And GCS and/or IPC until fully mobile.
Consult with the Director of Obstetrics or Consultant
5-10 days or until hospital discharge.
Lower RiskAll other Surgery with no additional risk factors, **Patients awaiting residential care placement
Optional GCS, Optional Enoxaparin 40mgs(halve the dose if GRF<30ml/min) daily or Unfractionated Heparin 5000 units BD if additional risk factors.∞
Until Hospital Discharge
Risk Category Clinical Features Prophylaxis Duration
Printed Copies are Uncontrolled Page 3 of 13
Procedure: Venous Thromboembolism Prophylaxis
Mackay Hospital and Health Service
Guidelines for Graduated Compression Stockings Three types of mechanical devices are used in the prevention of Venous Thromboembolism. They are Graduated Compression Stockings (GCS), Intermittent Pneumatic Compression (IPC) and Foot Impulse Technology (FIT). Implementation Guidelines: To be implemented by nursing staff after MO orders on the National Inpatient Medication Chart. Mechanical compression devices must be measured and fitted for the individual patient. For measuring guidelines please refer to manufactures recommendations. Please Note: Knee length stockings should finish 3cm below the popliteal fossa. When applying graduated compression stockings ensure the patient is in a suitable position to avoid injury, e.g. supine on bed with the bed elevated to appropriate height. Apply the stocking over the feet and stand next to the patient, pulling the stocking up the calf towards you, not pushing away from you as this may cause strain or injury. Encourage the patient to assist with application. Always follow manufacturer’s instructions and utilise an applicator if available for faster and easier application. Document measurements and size of device provided for baseline measurements. Document compliance and usage of mechanical compression on the National Inpatient Medication Chart (NIMC) and / or nursing care plan. Patient’s condition may alter and staff will need to: Re-measure to ensure device fitting remains optimal; Notify treating medical team if contraindications become apparent; Avoid devices that restrict the application of the mechanical prophylaxis, e.g. Identification bracelets or wanderers alarms. Mechanical compression should be removed at least daily to allow for skin care and hygiene. Assess skin integrity at least every 8 hours. Those patients at very high risk of pressure injury may require increased frequency of monitoring. Patients identified as very high risk for pressure areas may not be suitable mechanical prophylaxis. Feet and legs should be dried before application of mechanical compression. Check each shift for correct placement, no restrictions to perfusion and satisfactory neurovascular status. Please Note: Stockings should not be rolled or folded at the ankle for mobilising or below the knee if too long. Patients should mobilise in appropriate enclosed footwear if GCS are insitu. If no appropriate footwear is available, then it is preferred that GCS are removed when mobilising and reapplied on return to bed / chair.
Printed Copies are Uncontrolled Page 4 of 13
Procedure: Venous Thromboembolism Prophylaxis
Mackay Hospital and Health Service
Where appropriate foot wear is not available, traction socks may be applied for mobilisation but should be removed upon returning to bed. Note: These are not to be used as bed socks. They are contraindicated in patients with a shuffling gait, impaired balance, or by physiotherapy assessment. Decision to cease mechanical compression is clinical, as with all prophylactic measures and should be documented. If the patient is sitting out of bed only and not ambulating, the IPC is to be kept on due to the risk of venous stasis. Mechanical compression should be applied prior to surgery whenever possible. Patients with Peripheral Arterial Disease (PAD) should generally not receive mechanical prophylaxis; it may be used in patients with PAD if the patient has had an appropriate vascular assessment completed by medical staff or vascular specialist nurses. Consider Foot Impulse Technology as first preference if mechanical compression is required after vascular assessment. Intermittent Pneumatic Compression and Graduated Compression Stockings can be combined in prophylaxis treatment. Please Note: When treating a DVT, intermittent pneumatic compression should not be used. A treatment compression stocking (Class II: 20-30 mm Hg) should be used. Duration: Mechanical compression should be continuous therapy from time of immobility to the return of full ambulation, unless specified by the treating medical team. Early ambulation is encouraged as the optimum measure of VTE prophylaxis and the use of mechanical prophylaxis should not impede this. IPC should be insitu for approximately of 20 hours / day to achieve maximum effectiveness. Patient Education: Education of patient and carer should be an important part of the care provided, and must encompass issues as the reason for using compression stockings, care of the skin and the need to monitor for swelling of the legs. Patients should be shown how to wear GCS correctly by a healthcare professional that has been trained in the application and management of the product and advised of the risks of discontinued or incorrect use. Care Each pair can be washed up to 30 times. Hand wash with a mild detergent in cold / warm water or delicate cycle machine wash. Wring out in towel. To be dried flat or hanging out of direct sunlight. Can be tumble dried or dried with a hairdryer up to temperatures of 90ºC. Printed Copies are Uncontrolled Page 5 of 13
Procedure: Venous Thromboembolism Prophylaxis
Mackay Hospital and Health Service
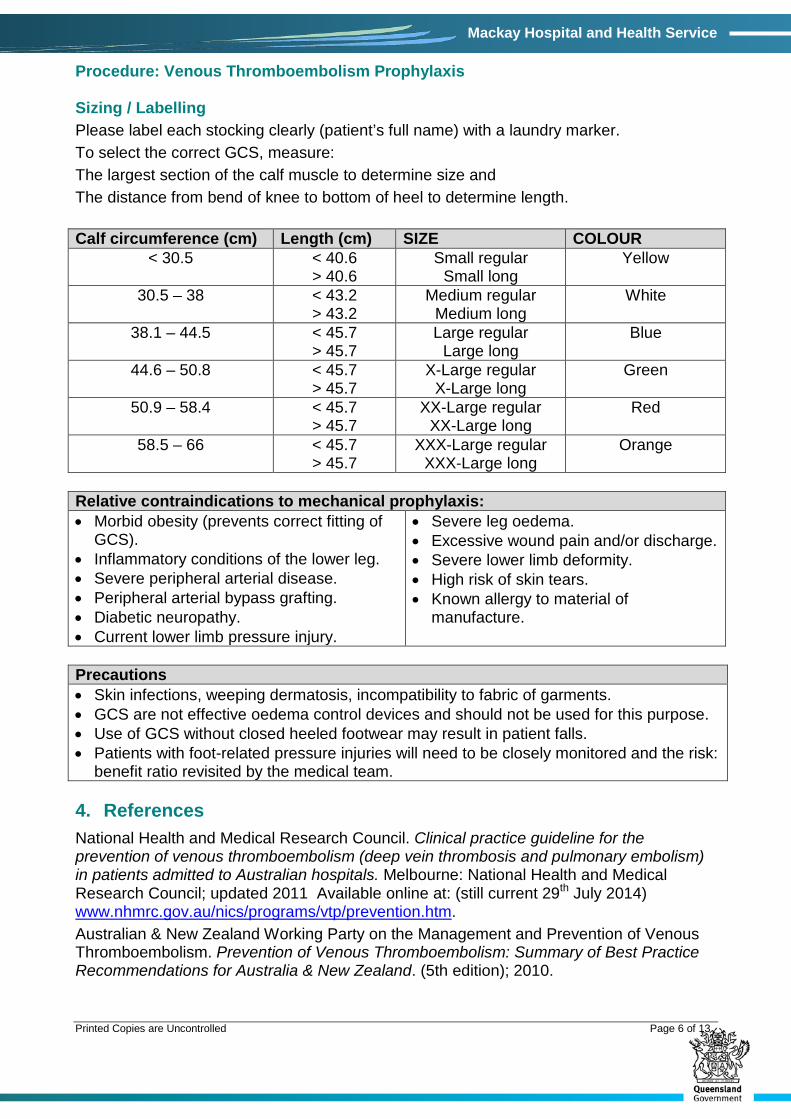
Sizing / Labelling Please label each stocking clearly (patient’s full name) with a laundry marker. To select the correct GCS, measure: The largest section of the calf muscle to determine size and The distance from bend of knee to bottom of heel to determine length. Calf circumference (cm) Length (cm) SIZE COLOUR
< 30.5 < 40.6 > 40.6
Small regular Small long
Yellow
30.5 – 38 < 43.2 > 43.2
Medium regular Medium long
White
38.1 – 44.5 < 45.7 > 45.7
Large regular Large long
Blue
44.6 – 50.8 < 45.7 > 45.7
X-Large regular X-Large long
Green
50.9 – 58.4 < 45.7 > 45.7
XX-Large regular XX-Large long
Red
58.5 – 66 < 45.7 > 45.7
XXX-Large regular XXX-Large long
Orange
Relative contraindications to mechanical prophylaxis: • Morbid obesity (prevents correct fitting of
GCS). • Inflammatory conditions of the lower leg. • Severe peripheral arterial disease. • Peripheral arterial bypass grafting. • Diabetic neuropathy. • Current lower limb pressure injury.
• Severe leg oedema. • Excessive wound pain and/or discharge. • Severe lower limb deformity. • High risk of skin tears. • Known allergy to material of
manufacture.
Precautions • Skin infections, weeping dermatosis, incompatibility to fabric of garments. • GCS are not effective oedema control devices and should not be used for this purpose. • Use of GCS without closed heeled footwear may result in patient falls. • Patients with foot-related pressure injuries will need to be closely monitored and the risk:
benefit ratio revisited by the medical team. 4. References National Health and Medical Research Council. Clinical practice guideline for the prevention of venous thromboembolism (deep vein thrombosis and pulmonary embolism) in patients admitted to Australian hospitals. Melbourne: National Health and Medical Research Council; updated 2011 Available online at: (still current 29th July 2014) www.nhmrc.gov.au/nics/programs/vtp/prevention.htm. Australian & New Zealand Working Party on the Management and Prevention of Venous Thromboembolism. Prevention of Venous Thromboembolism: Summary of Best Practice Recommendations for Australia & New Zealand. (5th edition); 2010. Printed Copies are Uncontrolled Page 6 of 13
Procedure: Venous Thromboembolism Prophylaxis
Mackay Hospital and Health Service
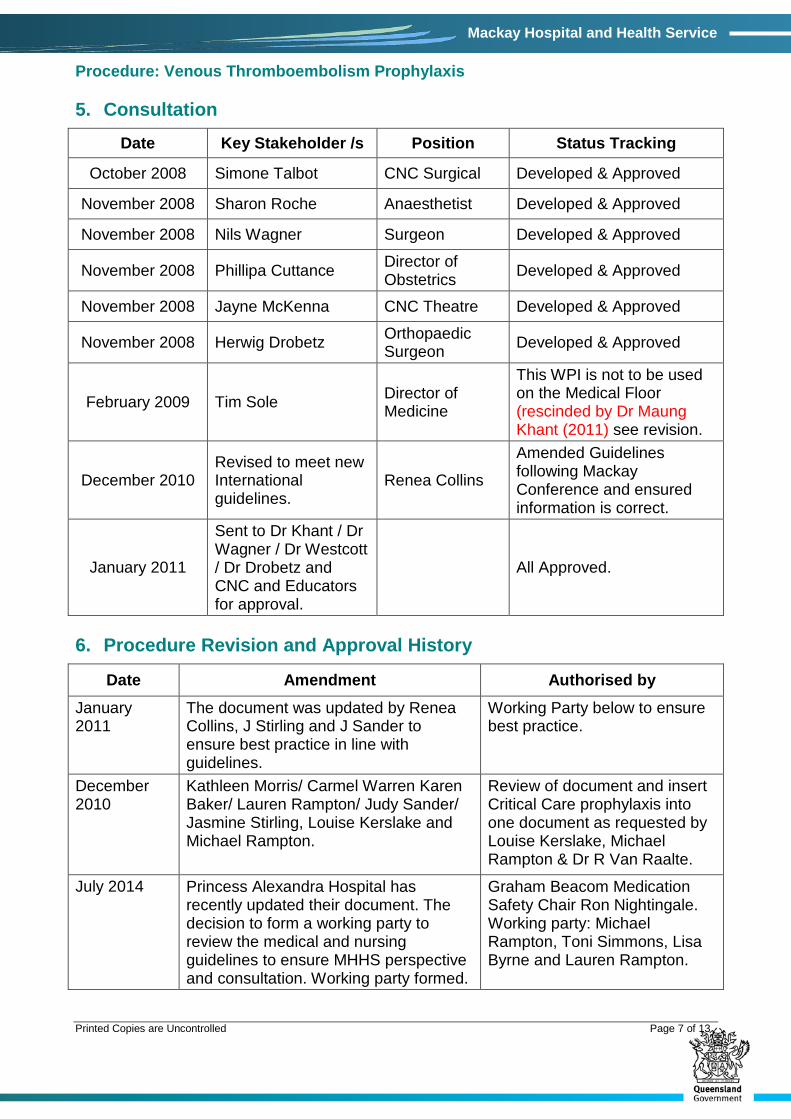
5. Consultation
Date Key Stakeholder /s Position Status Tracking
October 2008 Simone Talbot CNC Surgical Developed & Approved
November 2008 Sharon Roche Anaesthetist Developed & Approved
November 2008 Nils Wagner Surgeon Developed & Approved
November 2008 Phillipa Cuttance Director of Obstetrics Developed & Approved
November 2008 Jayne McKenna CNC Theatre Developed & Approved
November 2008 Herwig Drobetz Orthopaedic Surgeon Developed & Approved
February 2009 Tim Sole Director of Medicine
This WPI is not to be used on the Medical Floor (rescinded by Dr Maung Khant (2011) see revision.
December 2010 Revised to meet new International guidelines.
Renea Collins
Amended Guidelines following Mackay Conference and ensured information is correct.
January 2011
Sent to Dr Khant / Dr Wagner / Dr Westcott / Dr Drobetz and CNC and Educators for approval.
All Approved.
6. Procedure Revision and Approval History
Date Amendment Authorised by January 2011
The document was updated by Renea Collins, J Stirling and J Sander to ensure best practice in line with guidelines.
Working Party below to ensure best practice.
December 2010
Kathleen Morris/ Carmel Warren Karen Baker/ Lauren Rampton/ Judy Sander/ Jasmine Stirling, Louise Kerslake and Michael Rampton.
Review of document and insert Critical Care prophylaxis into one document as requested by Louise Kerslake, Michael Rampton & Dr R Van Raalte.
July 2014 Princess Alexandra Hospital has recently updated their document. The decision to form a working party to review the medical and nursing guidelines to ensure MHHS perspective and consultation. Working party formed.
Graham Beacom Medication Safety Chair Ron Nightingale. Working party: Michael Rampton, Toni Simmons, Lisa Byrne and Lauren Rampton.
Printed Copies are Uncontrolled Page 7 of 13
Procedure: Venous Thromboembolism Prophylaxis
Mackay Hospital and Health Service
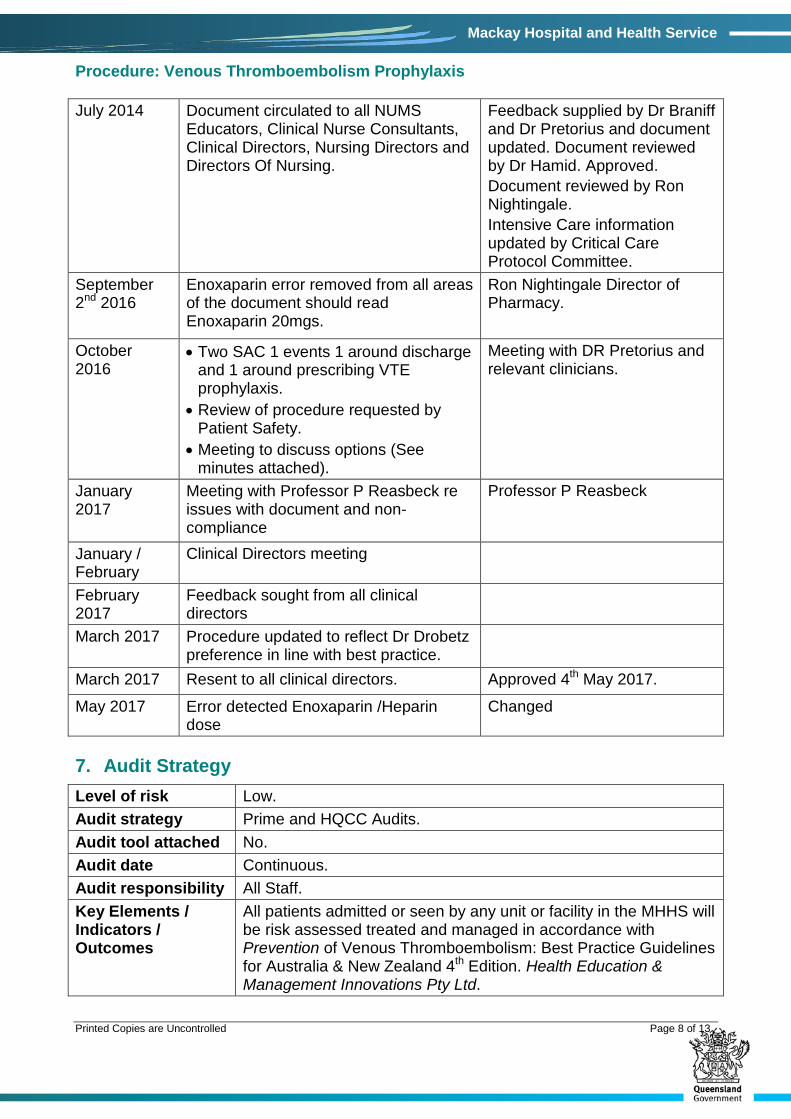
July 2014 Document circulated to all NUMS Educators, Clinical Nurse Consultants, Clinical Directors, Nursing Directors and Directors Of Nursing.
Feedback supplied by Dr Braniff and Dr Pretorius and document updated. Document reviewed by Dr Hamid. Approved. Document reviewed by Ron Nightingale. Intensive Care information updated by Critical Care Protocol Committee.
September 2nd 2016
Enoxaparin error removed from all areas of the document should read Enoxaparin 20mgs.
Ron Nightingale Director of Pharmacy.
October 2016
• Two SAC 1 events 1 around discharge and 1 around prescribing VTE prophylaxis.
• Review of procedure requested by Patient Safety.
• Meeting to discuss options (See minutes attached).
Meeting with DR Pretorius and relevant clinicians.
January 2017
Meeting with Professor P Reasbeck re issues with document and non-compliance
Professor P Reasbeck
January / February
Clinical Directors meeting
February 2017
Feedback sought from all clinical directors
March 2017 Procedure updated to reflect Dr Drobetz preference in line with best practice.
March 2017 Resent to all clinical directors. Approved 4th May 2017.
May 2017 Error detected Enoxaparin /Heparin dose
Changed
7. Audit Strategy Level of risk Low. Audit strategy Prime and HQCC Audits. Audit tool attached No. Audit date Continuous. Audit responsibility All Staff. Key Elements / Indicators / Outcomes
All patients admitted or seen by any unit or facility in the MHHS will be risk assessed treated and managed in accordance with Prevention of Venous Thromboembolism: Best Practice Guidelines for Australia & New Zealand 4th Edition. Health Education & Management Innovations Pty Ltd.
Printed Copies are Uncontrolled Page 8 of 13
Procedure: Venous Thromboembolism Prophylaxis
Mackay Hospital and Health Service
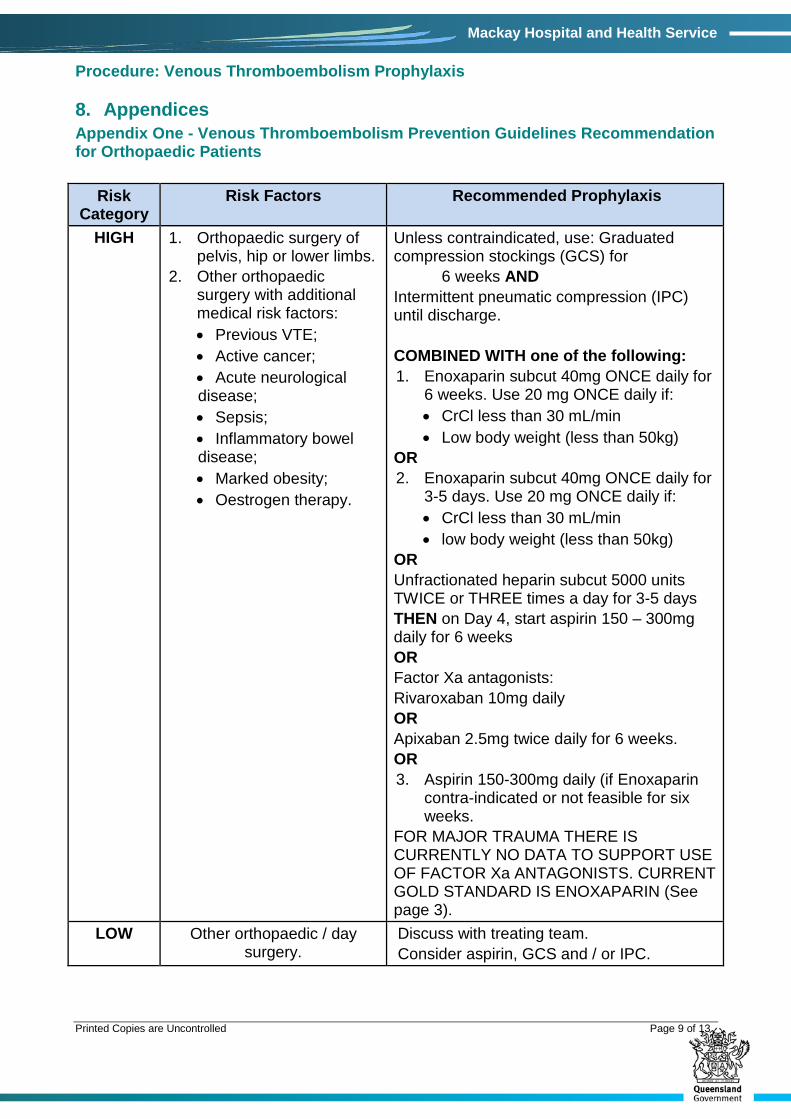
8. Appendices Appendix One - Venous Thromboembolism Prevention Guidelines Recommendation for Orthopaedic Patients
Risk Category
Risk Factors Recommended Prophylaxis
HIGH 1. Orthopaedic surgery of pelvis, hip or lower limbs.
2. Other orthopaedic surgery with additional medical risk factors: • Previous VTE; • Active cancer; • Acute neurological disease; • Sepsis; • Inflammatory bowel disease; • Marked obesity; • Oestrogen therapy.
Unless contraindicated, use: Graduated compression stockings (GCS) for 6 weeks AND Intermittent pneumatic compression (IPC) until discharge. COMBINED WITH one of the following: 1. Enoxaparin subcut 40mg ONCE daily for
6 weeks. Use 20 mg ONCE daily if: • CrCl less than 30 mL/min • Low body weight (less than 50kg)
OR 2. Enoxaparin subcut 40mg ONCE daily for
3-5 days. Use 20 mg ONCE daily if: • CrCl less than 30 mL/min • low body weight (less than 50kg)
OR Unfractionated heparin subcut 5000 units TWICE or THREE times a day for 3-5 days THEN on Day 4, start aspirin 150 – 300mg daily for 6 weeks OR Factor Xa antagonists: Rivaroxaban 10mg daily OR Apixaban 2.5mg twice daily for 6 weeks. OR 3. Aspirin 150-300mg daily (if Enoxaparin
contra-indicated or not feasible for six weeks.
FOR MAJOR TRAUMA THERE IS CURRENTLY NO DATA TO SUPPORT USE OF FACTOR Xa ANTAGONISTS. CURRENT GOLD STANDARD IS ENOXAPARIN (See page 3).
LOW Other orthopaedic / day surgery.
Discuss with treating team. Consider aspirin, GCS and / or IPC.
Printed Copies are Uncontrolled Page 9 of 13
Procedure: Venous Thromboembolism Prophylaxis
Mackay Hospital and Health Service
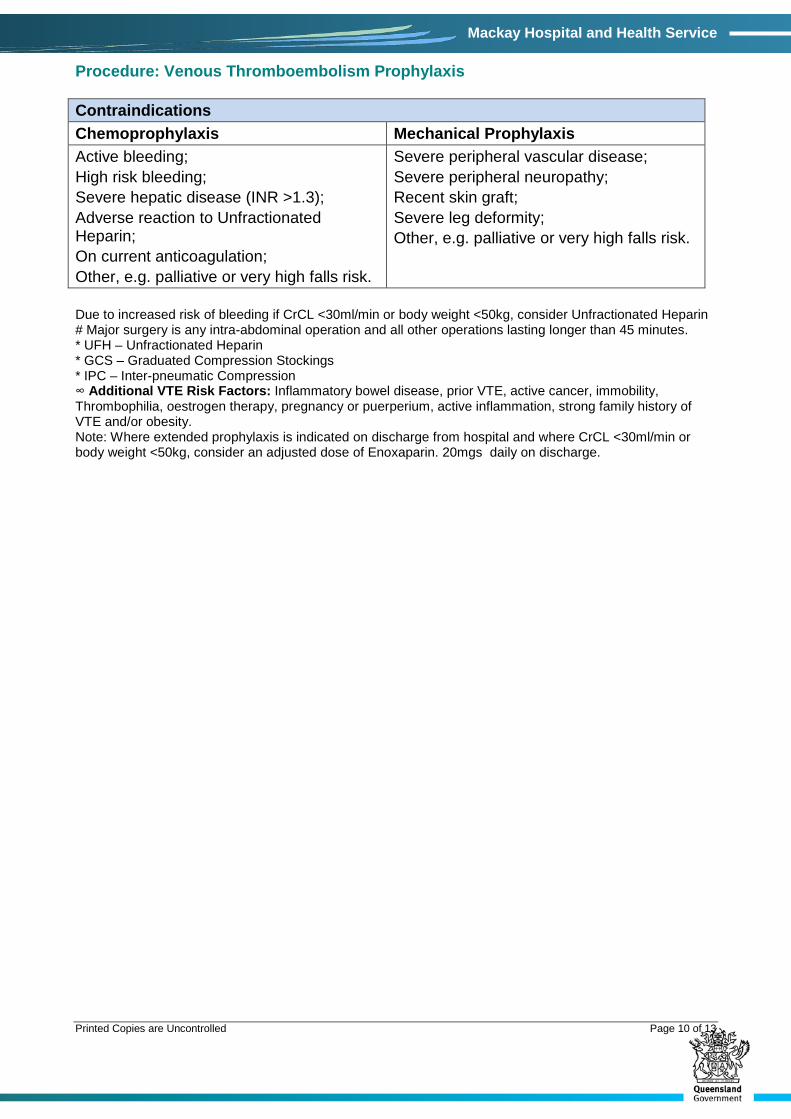
Contraindications
Chemoprophylaxis Mechanical Prophylaxis
Active bleeding; High risk bleeding; Severe hepatic disease (INR >1.3); Adverse reaction to Unfractionated Heparin; On current anticoagulation; Other, e.g. palliative or very high falls risk.
Severe peripheral vascular disease; Severe peripheral neuropathy; Recent skin graft; Severe leg deformity; Other, e.g. palliative or very high falls risk.
Due to increased risk of bleeding if CrCL <30ml/min or body weight <50kg, consider Unfractionated Heparin # Major surgery is any intra-abdominal operation and all other operations lasting longer than 45 minutes. * UFH – Unfractionated Heparin * GCS – Graduated Compression Stockings * IPC – Inter-pneumatic Compression ∞ Additional VTE Risk Factors: Inflammatory bowel disease, prior VTE, active cancer, immobility, Thrombophilia, oestrogen therapy, pregnancy or puerperium, active inflammation, strong family history of VTE and/or obesity. Note: Where extended prophylaxis is indicated on discharge from hospital and where CrCL <30ml/min or body weight <50kg, consider an adjusted dose of Enoxaparin. 20mgs daily on discharge.
Printed Copies are Uncontrolled Page 10 of 13
Procedure: Venous Thromboembolism Prophylaxis
Mackay Hospital and Health Service
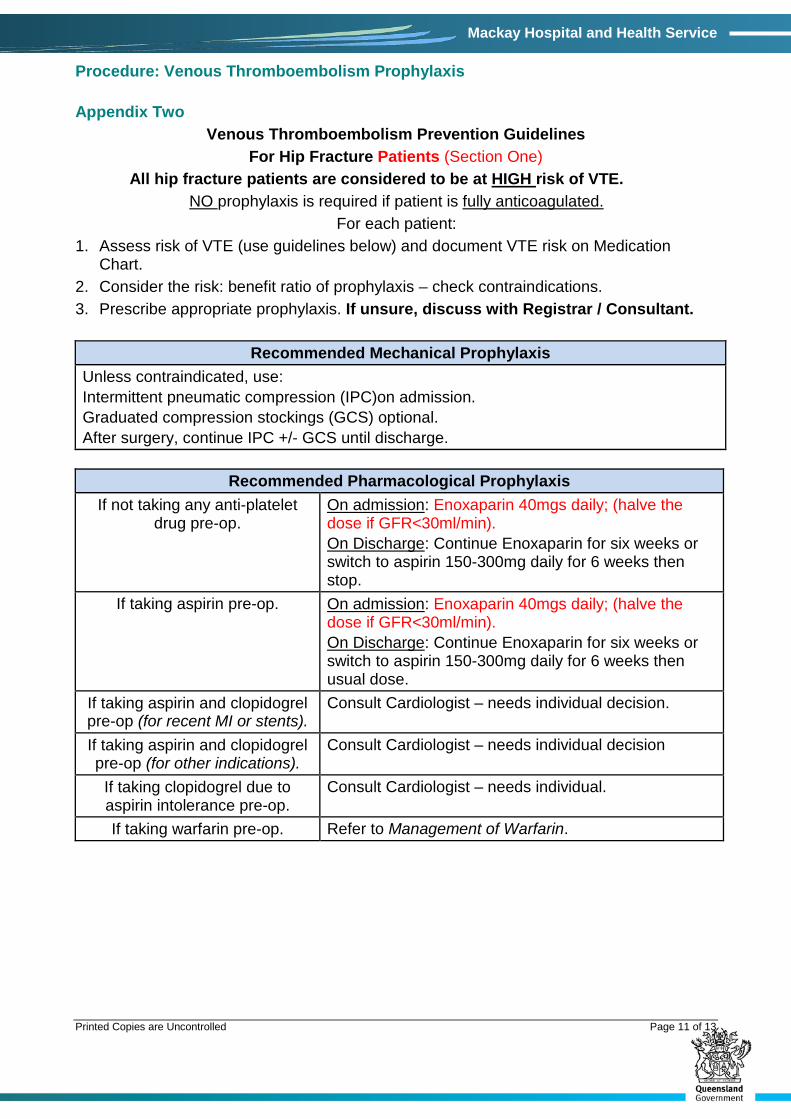
Appendix Two Venous Thromboembolism Prevention Guidelines
For Hip Fracture Patients (Section One) All hip fracture patients are considered to be at HIGH risk of VTE.
NO prophylaxis is required if patient is fully anticoagulated. For each patient:
1. Assess risk of VTE (use guidelines below) and document VTE risk on Medication Chart.
2. Consider the risk: benefit ratio of prophylaxis – check contraindications. 3. Prescribe appropriate prophylaxis. If unsure, discuss with Registrar / Consultant.
Recommended Mechanical Prophylaxis Unless contraindicated, use: Intermittent pneumatic compression (IPC)on admission. Graduated compression stockings (GCS) optional. After surgery, continue IPC +/- GCS until discharge.
Recommended Pharmacological Prophylaxis
If not taking any anti-platelet drug pre-op.
On admission: Enoxaparin 40mgs daily; (halve the dose if GFR<30ml/min). On Discharge: Continue Enoxaparin for six weeks or switch to aspirin 150-300mg daily for 6 weeks then stop.
If taking aspirin pre-op. On admission: Enoxaparin 40mgs daily; (halve the dose if GFR<30ml/min). On Discharge: Continue Enoxaparin for six weeks or switch to aspirin 150-300mg daily for 6 weeks then usual dose.
If taking aspirin and clopidogrel pre-op (for recent MI or stents).
Consult Cardiologist – needs individual decision.
If taking aspirin and clopidogrel pre-op (for other indications).
Consult Cardiologist – needs individual decision
If taking clopidogrel due to aspirin intolerance pre-op.
Consult Cardiologist – needs individual.
If taking warfarin pre-op. Refer to Management of Warfarin.
Printed Copies are Uncontrolled Page 11 of 13
Procedure: Venous Thromboembolism Prophylaxis
Mackay Hospital and Health Service
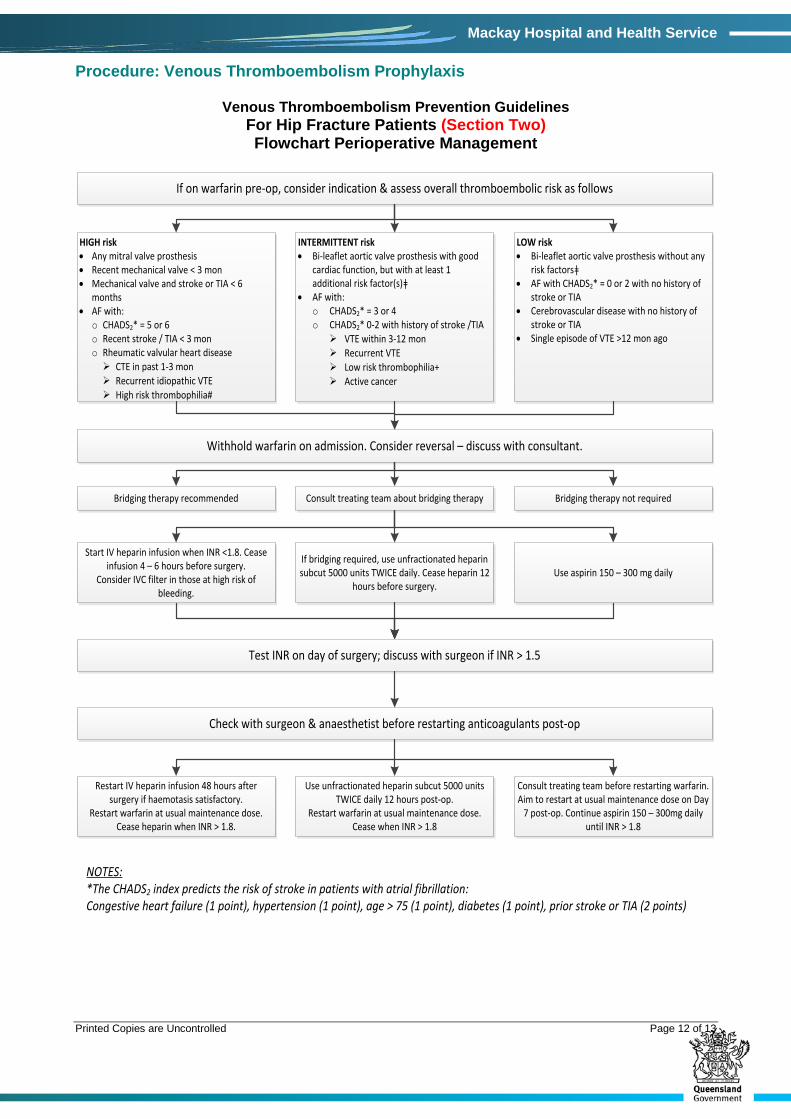
Venous Thromboembolism Prevention Guidelines For Hip Fracture Patients (Section Two) Flowchart Perioperative Management
If on warfarin pre-op, consider indication & assess overall thromboembolic risk as follows
HIGH risk• Any mitral valve prosthesis• Recent mechanical valve < 3 mon• Mechanical valve and stroke or TIA < 6
months• AF with:
o CHADS2* = 5 or 6o Recent stroke / TIA < 3 mono Rheumatic valvular heart disease CTE in past 1-3 mon Recurrent idiopathic VTE High risk thrombophilia#
INTERMITTENT risk• Bi-leaflet aortic valve prosthesis with good
cardiac function, but with at least 1 additional risk factor(s)ǂ
• AF with:o CHADS2* = 3 or 4o CHADS2* 0-2 with history of stroke /TIA VTE within 3-12 mon Recurrent VTE Low risk thrombophilia+ Active cancer
LOW risk• Bi-leaflet aortic valve prosthesis without any
risk factorsǂ• AF with CHADS2* = 0 or 2 with no history of
stroke or TIA • Cerebrovascular disease with no history of
stroke or TIA• Single episode of VTE >12 mon ago
Withhold warfarin on admission. Consider reversal – discuss with consultant.
Bridging therapy recommended Consult treating team about bridging therapy Bridging therapy not required
Start IV heparin infusion when INR <1.8. Cease infusion 4 – 6 hours before surgery.
Consider IVC filter in those at high risk of bleeding.
If bridging required, use unfractionated heparin subcut 5000 units TWICE daily. Cease heparin 12
hours before surgery.Use aspirin 150 – 300 mg daily
Test INR on day of surgery; discuss with surgeon if INR > 1.5
Check with surgeon & anaesthetist before restarting anticoagulants post-op
Restart IV heparin infusion 48 hours after surgery if haemotasis satisfactory.
Restart warfarin at usual maintenance dose. Cease heparin when INR > 1.8.
Use unfractionated heparin subcut 5000 units TWICE daily 12 hours post-op.
Restart warfarin at usual maintenance dose. Cease when INR > 1.8
Consult treating team before restarting warfarin. Aim to restart at usual maintenance dose on Day
7 post-op. Continue aspirin 150 – 300mg daily until INR > 1.8
NOTES:*The CHADS2 index predicts the risk of stroke in patients with atrial fibrillation:Congestive heart failure (1 point), hypertension (1 point), age > 75 (1 point), diabetes (1 point), prior stroke or TIA (2 points)
Printed Copies are Uncontrolled Page 12 of 13
Procedure: Venous Thromboembolism Prophylaxis
Mackay Hospital and Health Service
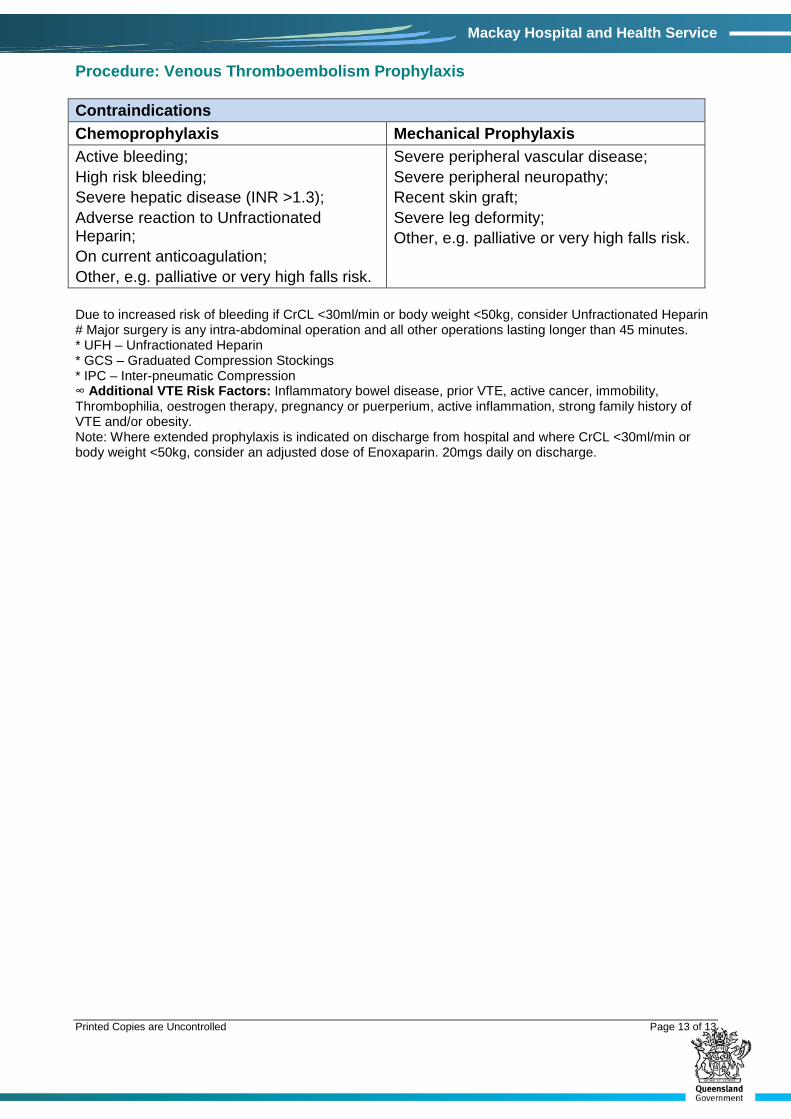
Contraindications Chemoprophylaxis Mechanical Prophylaxis Active bleeding; High risk bleeding; Severe hepatic disease (INR >1.3); Adverse reaction to Unfractionated Heparin; On current anticoagulation; Other, e.g. palliative or very high falls risk.
Severe peripheral vascular disease; Severe peripheral neuropathy; Recent skin graft; Severe leg deformity; Other, e.g. palliative or very high falls risk.
Due to increased risk of bleeding if CrCL <30ml/min or body weight <50kg, consider Unfractionated Heparin # Major surgery is any intra-abdominal operation and all other operations lasting longer than 45 minutes. * UFH – Unfractionated Heparin * GCS – Graduated Compression Stockings * IPC – Inter-pneumatic Compression ∞ Additional VTE Risk Factors: Inflammatory bowel disease, prior VTE, active cancer, immobility, Thrombophilia, oestrogen therapy, pregnancy or puerperium, active inflammation, strong family history of VTE and/or obesity. Note: Where extended prophylaxis is indicated on discharge from hospital and where CrCL <30ml/min or body weight <50kg, consider an adjusted dose of Enoxaparin. 20mgs daily on discharge.
Printed Copies are Uncontrolled Page 13 of 13