Updates in venous thromboembolism
101
-
Upload
gamal-agmy -
Category
Health & Medicine
-
view
842 -
download
1
Transcript of Updates in venous thromboembolism

Updates in Venous
Thromboembolism
Gamal Rabie Agmy, MD, FCCP Professor of Chest Diseases, Assiut university
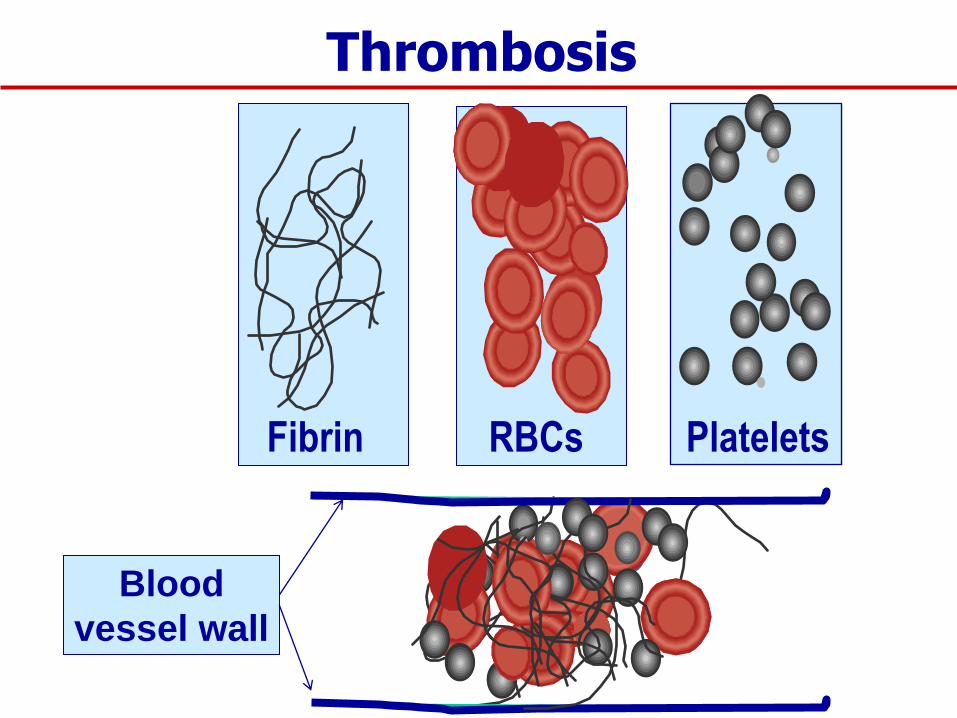
Fibrin Platelets RBCs
Thrombosis
Blood
vessel wall
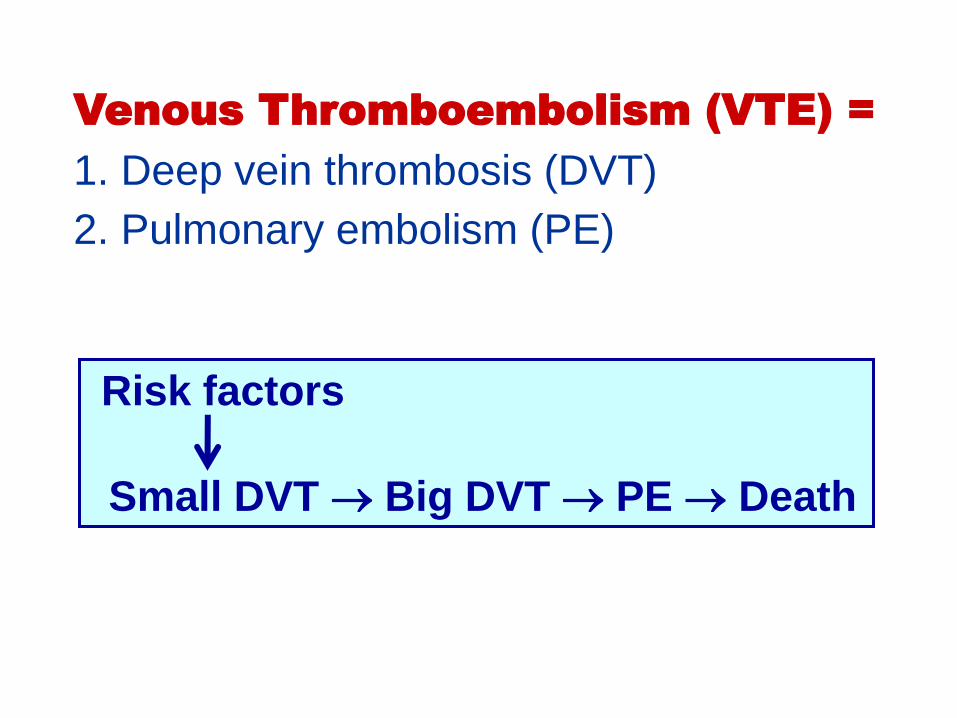
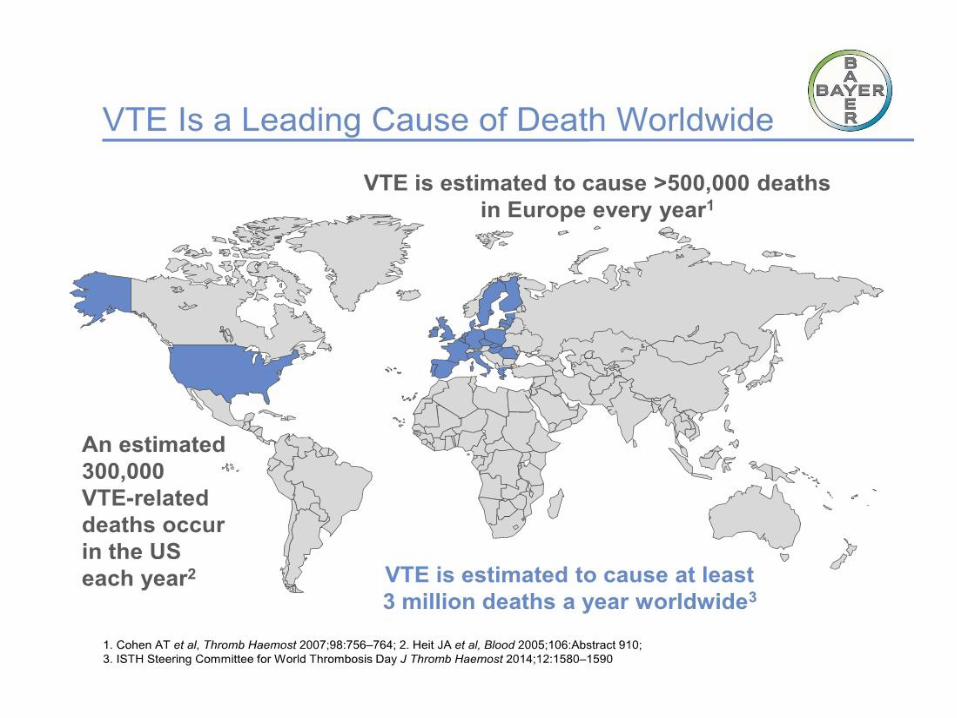
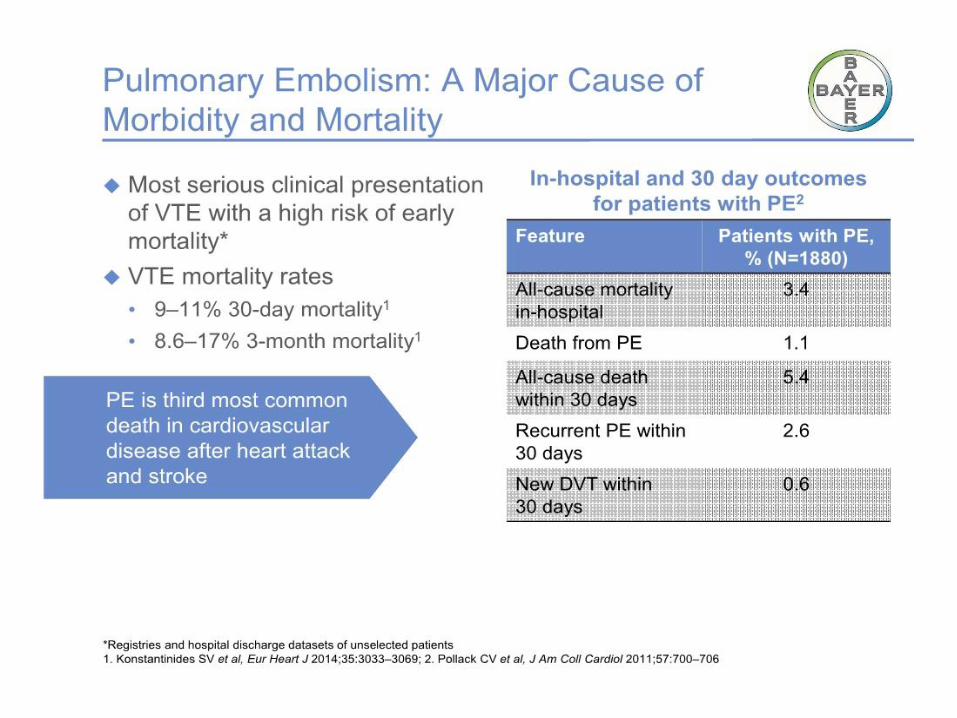
Venous Thromboembolism (VTE) =
1. Deep vein thrombosis (DVT)
2. Pulmonary embolism (PE)
Risk factors
Small DVT Big DVT PE Death
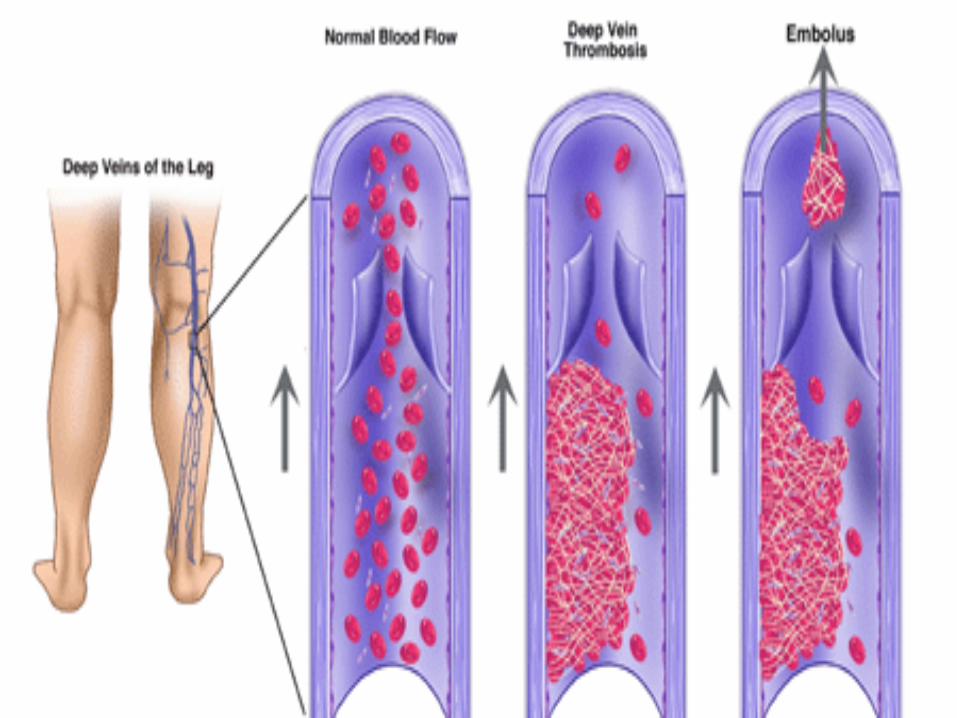
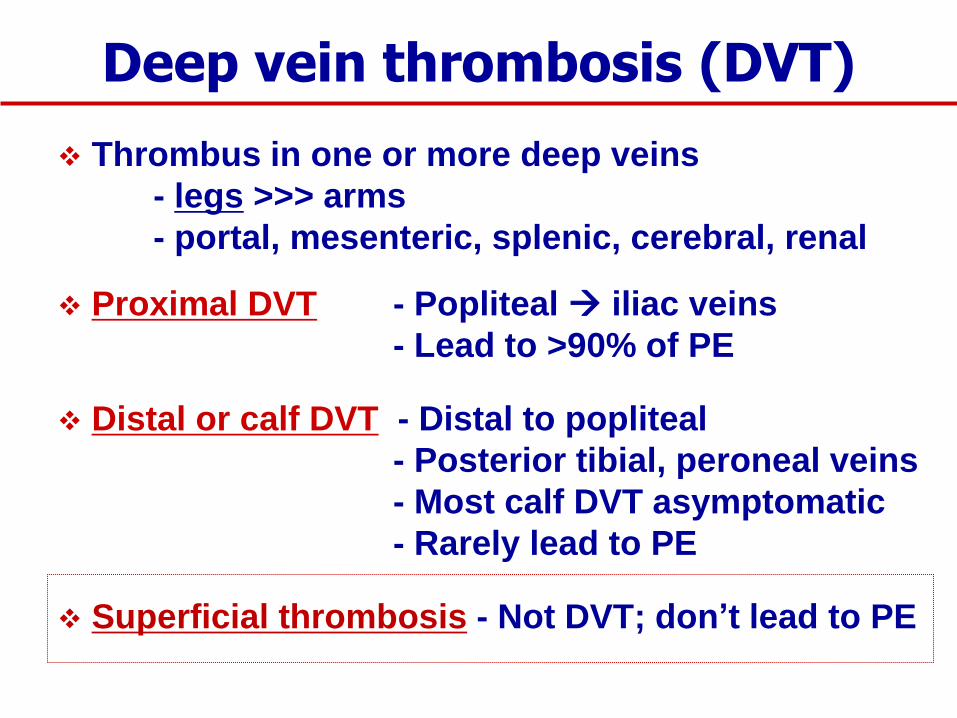
Deep vein thrombosis (DVT)
Thrombus in one or more deep veins
- legs >>> arms
- portal, mesenteric, splenic, cerebral, renal
Proximal DVT - Popliteal iliac veins
- Lead to >90% of PE
Distal or calf DVT - Distal to popliteal
- Posterior tibial, peroneal veins
- Most calf DVT asymptomatic
- Rarely lead to PE
Superficial thrombosis - Not DVT; don’t lead to PE
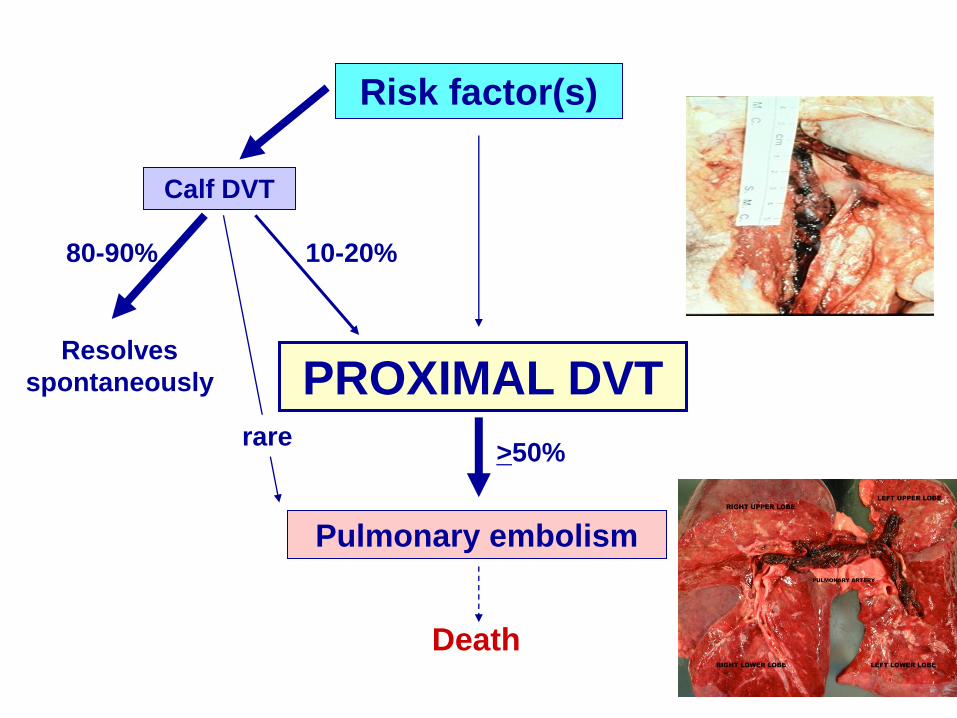
Risk factor(s)
PROXIMAL DVT
Calf DVT
Resolves
spontaneously
80-90% 10-20%
Pulmonary embolism
Death
>50% rare
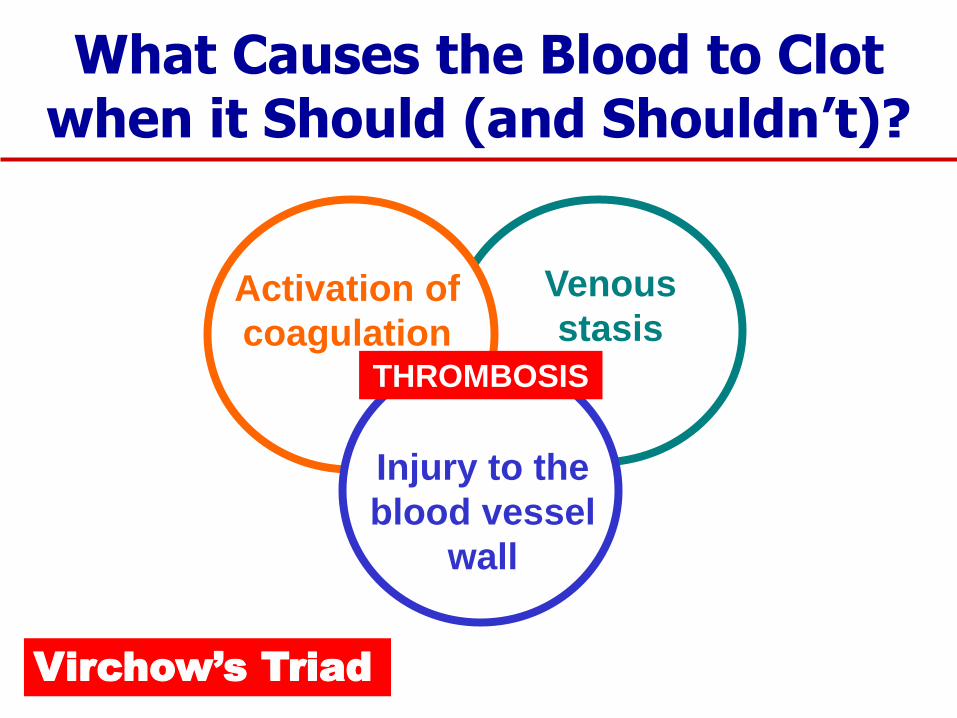
What Causes the Blood to Clot when it Should (and Shouldn’t)?
Venous
stasis Activation of
coagulation
Injury to the
blood vessel
wall
THROMBOSIS
Virchow’s Triad
Procedure-related:
Cancer > benign
Open > laparoscopic
GA > regional anesthesia
Duration of procedure
VTE Risk Factors in General Surgery
Patient-related: Age
Previous VTE
Obesity
Reduced mobility
Infection
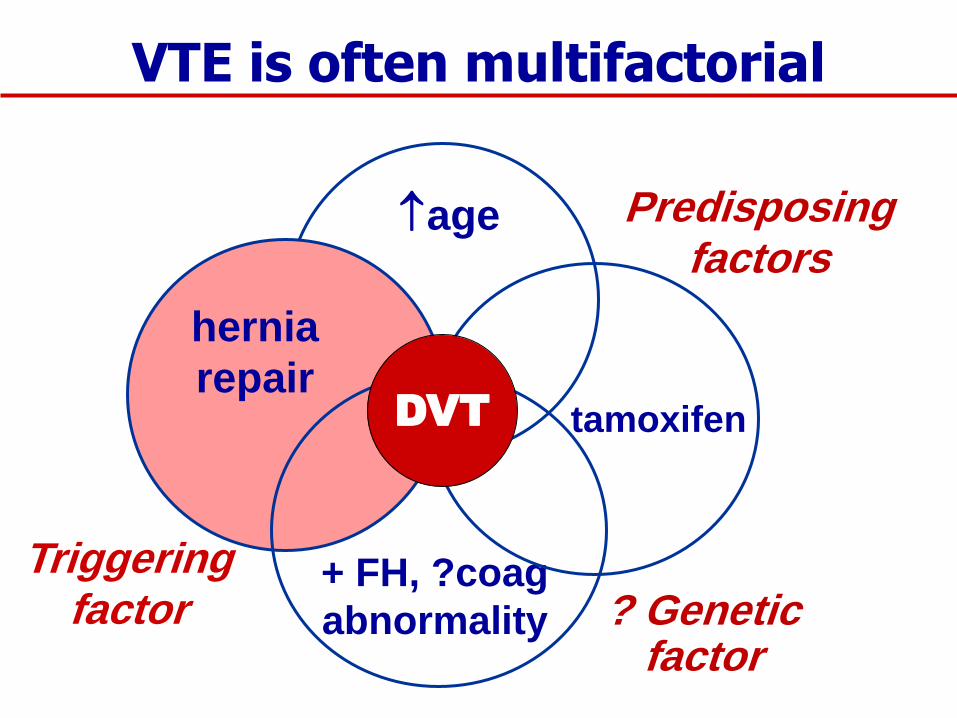
+ FH, ?coag
abnormality
tamoxifen
hernia
repair
age
Triggering factor
Predisposing factors
? Genetic factor
DVT
VTE is often multifactorial




D-dimer (“D-dummer”)
Formed by effect of plasmin on fibrin
Increased in VTE
Also increased:
Generally useless; may be misleading
NEVER done on inpatients or patients at high
risk of having a positive result
Virtually no role in surgical patients
plasmin
Fibrin FDPs (incl D-dimer)
after surgery
trauma
cancer
acute infection
inflammatory disease
liver disease
uncomplicated pregnancy
healthy elderly
etc

Appearance of Pulmonary Embolus on CTPA
◙ The key diagnostic findings of PE on CTPA are central or wall-
adherent filling defects in the pulmonary arteries leading to either
complete or partial obstruction. There are a number of mimickers of
PE, which can be divided into anatomic and technical mimickers.
Familiarity with these helps to avoid diagnostic errors. These pitfalls
are discussed later in this tutorial. In the CTPA sequence of images
below scroll to see the filling defects created by the PE.
◙ Below you can find the CTPA of an acute PE in first image, followed by a
1-month follow-up and then a 1-year follow-up.
A
B C
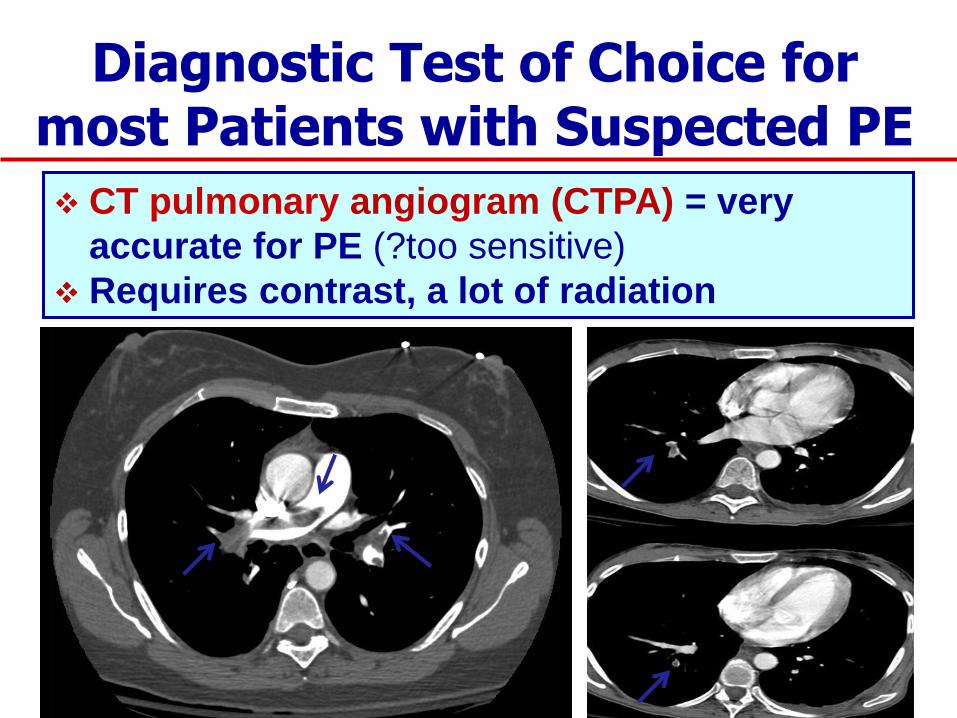
Diagnostic Test of Choice for most Patients with Suspected PE
CT pulmonary angiogram (CTPA) = very
accurate for PE (?too sensitive)
Requires contrast, a lot of radiation
Ultrasonography
◙ If there is an ultrasound confirmation of deep venous thrombosis
(DVT) associated with pulmonary symptoms, this may indirectly
confirm the diagnosis of PE. Since therapy is often the same for both
conditions, further investigation to exclude PE may not be necessary.
Prevalence of DVT is 82% in patients with PE
◙ Compression Duplex ultrasound is the primary diagnostic test for
DVT in patients having proximal leg symptoms, with a reported
sensitivity and specificity of 97 and 94%, respectively. Although the
diagnosis of a DVT below the knee is more controversial, reported
prevalence of lower limb (infra-popliteal level) DVT is as low as 13%
in the patients with proven acute PE. Major restrictions of US
imaging limiting its sensitivity in the diagnosis of DVT are the
challenging evaluation of calf veins, iliac veins and the inferior vena
cava as well as its operator/equipment dependency.
Ultrasonography

Ultrasonography

Ultrasonography
Schematic representation of the parenchymal, pleural and vascular features
associated with pulmonary embolism.(Angelika Reissig, Claus Kroegel.
Respiration 2003;70:441-452 )

V/Q Scan
◙ Pulmonary perfusion scanning was the most widely utilized
screening test to rule out clinically important pulmonary embolism
prior to the advent of computed tomography pulmonary angiography
(CTPA). It has been shown that a normal test result almost certainly
excludes the presence of pulmonary embolism.
◙ A high probability ventilation-perfusion (VQ) scan usually indicates
the presence of clinically significant PE. 88% of patients with a high
probability VQ scan had angiographic evidence of PE in the PIOPED I
study.
◙ However, in patients with a prior history of PE and high probability
VQ scans the presence of acute PE was proven in only 74%
angiographically. In addition, of all patients diagnosed with acute PE
in the PIOPED I study, only 41% had a scan pattern thought to
represent a high probability VQ scan.
V/Q Scan
◙ Patients presenting in either the intermediate or indeterminate group of
VQ scans are difficult to interpret and the technique is also not helpful in
patients with a low probability scan in the setting of a high clinical
suspicion. Unfortunately, the majority of patients undergoing perfusion
scanning have nondiagnostic results (more than 60% of all patients in the
PIOPED I study). Also, in the PIOPED II study, VQ scanning has been
used for the diagnosis or exclusion of PE evaluated by CTA. Only 30% of
all patients had a high probability and normal VQ findings. It is for this
reason that other screening techniques for PE have been developed.
◙ Compression Duplex ultrasound is the primary diagnostic test for DVT
in patients having proximal leg symptoms, with a reported sensitivity and
specificity of 97 and 94%, respectively. Although the diagnosis of a DVT
below the knee is more controversial, reported prevalence of lower limb
(infra-popliteal level) DVT is as low as 13% in the patients with proven
acute PE. Major restrictions of US imaging limiting its sensitivity in the
diagnosis of DVT are the challenging evaluation of calf veins, iliac veins
and the inferior vena cava as well as its operator/equipment dependency.
The addition of a ventilation scan improves the overall test performance
only marginally.
Magnetic Resonance Pulmonary Angiography (MRPA)
◙ Magnetic resonance pulmonary angiography (MRPA), although still
considered a second-line imagine technique behind CTPA, has been
gaining acceptance in the evaluation of VTE. In contrast to CT, MR
imaging does not expose the patient to ionizing radiation, and its
main contrast agent, gadolinium chelate, shows a much lower
potential for allergic reactions and nephrotoxicity than does
iodinated contrast. There is however the risk of developing
nephrogenic systemic fibrosis (NSF) in patients on dialysis or with
renal insufficiency (reference). However, longer acquisition times and
poorer spatial resolution have historically limited its applicability in
the imaging of the pulmonary arterial system.
Magnetic Resonance Pulmonary Angiography (MRPA)
◙ Magnetic resonance pulmonary angiography (MRPA), although still
considered a second-line imagine technique behind CTPA, has been
gaining acceptance in the evaluation of VTE. In contrast to CT, MR
imaging does not expose the patient to ionizing radiation, and its
main contrast agent, gadolinium chelate, shows a much lower
potential for allergic reactions and nephrotoxicity than does
iodinated contrast. There is however the risk of developing
nephrogenic systemic fibrosis (NSF) in patients on dialysis or with
renal insufficiency (reference). However, longer acquisition times and
poorer spatial resolution have historically limited its applicability in
the imaging of the pulmonary arterial system.
Magnetic Resonance Pulmonary Angiography (MRPA)
◙ As MR techniques improve these historic limitations are slowly
being overcome. The advent of more rapid imaging sequences in
conjunction with parallel imaging has diminished motion artifact,
allowing for improved resolution of the pulmonary vascular system.
Additionally, dynamic imaging during contrast injection now offers
the functional information of perfusion imaging. The systemic
venous structures can be simultaneously evaluated, using MR
venography (MRV), to assess for pelvic and lower extremity VTE.
Recent published literature suggests that MR imaging of acute VTE
(MRI, MRPA, MR perfusion, MRV) indeed may rival the accuracy of CT
in the detection of VTE and PE (at least centrally). These data have
yet to be validated in larger prospective studies. As it continues to
evolve, MR imaging is expected to play an increased role in the
future evaluation of PE.
MR Direct Thrombus Imaging
◙ MR direct thrombus imaging (MRDTI) makes use of direct
detection of methemoglobin in a thrombus, which appears bright on
T1-weighted sequences owing to its T1 shortening effect. Utilization
of this endogenous contrast permits visualization of a thrombus
without the use of any contrast agent (hence the term “direct
thrombus imaging”), and it is non-invasive. MRDTI can be used to
detect subacute thrombosis. Deep vein thrombosis and pulmonary
embolism can be both confirmed by MRDTI. Also, it does allow the
detection of venous thromboembolic disease with a single imaging
modality. The most significant advantage of MRDTI is the direct
visualization of the thrombus, while other sequences rely on the
detection of thrombus through a filling defect. Another advantage is
that MRDTI allows to differentiate between old and new clots (high
signal intensity indicates subacute thrombosis).
MR Direct Thrombus Imaging
◙ Several studies have been performed to determine the efficacy of
MRDTI in detection of thrombus. In a study comparing MRDTI with
contrast venography the sensitivity of MRDTI was 96% in 338
patients. In a smaller PE study involving 13 patients the sensitivity
and specificity of MRDTI was 100% for both. MRDTI allowed the
detection of three additional emboli not seen on conventional
pulmonary angiography. A randomized trial of MRDTI for diagnosis of
pulmonary embolism in 157 patients demonstrated similar patient
outcomes compared with more extensive diagnostic strategies,
including CT, VQ and D-dimer testing. These results make it possible
that MRDTI may have a significant role in the future for the diagnosis
and management of venous thromboembolism.
MR Perfusion Imaging ◙ Contrast-based perfusion MRI is generally used in combination with
ultra-fast three dimensional MR angiography (3D MRA), demonstrating
contrast agent entering into the pulmonary circulation as well as imaging
of the vessel morphology. Techniques without or with parallel imaging
technology are effective. These permit both the identification of perfusion
defects and imaging of the vessel morphology, hence facilitating the
diagnosis of pulmonary vascular disease. Highly promising results have
been reported from the initial work in this field.
◙ A recent study of 33 patients evaluated the feasibility of MR perfusion for
short-term follow-up of patients with acute PE. The study also purposed to
evaluate temporal changes of pulmonary perfusion and thrombus
characteristics of a thrombus that might be helpful in determining the age
of the thrombus. All patients were examined by CT and, MRA, real-time
MRI and MR pulmonary perfusion imaging initially and 1 week after
treatment. A follow-up diagnostic work-up was feasible for all patients after
treatment. MRA and CT were concordant for a diagnosis of PE in all
patients. They have also indicated that MRI has potential role for
determining the age of embolic material. The technique currently has to be
considered experimental and its value in clinical practice remains to be
demonstrated.
Pulmonary Angriography
◙ Pulmonary angiography is considered the gold standard for the
diagnosis of PE, although recent evidence does not necessarily
always support that. Pulmonary angiography is an invasive
procedure and due to its costs and potential risks is usually reserved
for patients in whom more information or certainty of the diagnosis
of PE are necessary. Indications for angiographic evaluation of
patients suspected of having PE are the need to confirm the
diagnosis of PE in the presence of contraindications to
anticoagulation or if IVC filter placement or surgical embolectomy are
contemplated.
◙ In addition, patients with a high index of clinical suspicion but
nondiagnostic noninvasive studies and patients with pulmonary
hypertension of unknown cause commonly undergo the exam . The
unequivocal establishment of the diagnosis of PE in younger
patients facing life-long anticoagulation therapy or IVC filter
placement is another indication. With modern techniques and
nonionic contrast media, the risks of the procedure are exceedingly
low with major nonfatal complication rates less than 2% and a
mortality of the procedure of 0.1%.
Pulmonary Angriography
◙ Life threatening complications are typically secondary to acute cor
pulmonale in patients with pre-existing severe pulmonary
hypertension and failing right ventricle. Therefore, the measurement
of the right ventricular enddiastolic pressure (RVEDP) is mandatory
before performing the angiographic runs and if this is 20 mmHg or
higher it should be acknowledged that the patient has a significantly
higher risk of a serious complication and therefore either should not
have the study performed or have a superselective study using more
runs with smaller amounts of contrast.
◙ It has been shown that digital angiography helps to reduce both
time and amount of contrast necessary to perform pulmonary
angiography if compared to conventional cut-film angiography. It
also has been shown to have similar performance without sacrifices
in sensitivity or specificity
Pulmonary Embolism During Pregnancy
◙ The diagnosis of PE during pregnancy imposes special
challenges. Both CTPA and VQ scanning expose the mother and the
fetus to radiation, with the fetus being particularly susceptible. The
International Commission on Radiological Protection (ICRP) has
made recommendations regarding the minimization of radiation
exposure to both patient and fetus and many countries have
introduced legislation to this end. In general terms, the fetal dose is
much higher with VQ scanning than with CTPA (depending on the
protocol up to 200 times higher) (700 – 800 µGy, vs 3 – 131 µGy) while
the maternal dose is typically lower with VQ scanning (1.4 mSv
versus 2.2 – 6.0 mSv).
Pulmonary Embolism During Pregnancy
◙ This fetal dose advantage for CTPA even applies to protocols
specifically modified for pregnant patients like half-dose perfusion scans
(140 – 250 µGy). Other considerations are the somewhat higher risk for
the mother to develop breast cancer with CTPA and the lack of human
safety data for the effects of iodinated contrast media on the fetus,
although they approved to be safe in animal experiments. Therefore, any
search for PE in a pregnant patient should involve a thorough discussion
of the risks and benefits with the patient. If imaging is necessary with
ionizing radiation, the currently available data support the preferential use
of CTPA, if possible with a modified low-dose technique and limited
anatomical coverage.
Automated tube modulation should be used for all scans, regardless
if the patient is pregnant or not. However, as a first step, an
ultrasound of the legs is recommended as a surrogate test for
pulmonary embolism.
Pulmonary Embolism During Pregnancy
◙ The D-dimer concentration is usually increased in the second and
third trimester of the pregnancy and normalizes 4 to 6 weeks after
delivery. Thus, the test is clearly less useful during pregnancy. As
significant controversy exists on this topic and because no study
has ever validated a negative D-dimer test for t he exclusion of PE in
pregnancy, the use D-dimer testing as a stand-alone test to exclude a
PE can currently not be recommended in this setting.

Pulmonary Embolism During Pregnancy
◙ This fetal dose advantage for CTPA even applies to protocols
specifically modified for pregnant patients like half-dose perfusion scans
(140 – 250 µGy). Other considerations are the somewhat higher risk for
the mother to develop breast cancer with CTPA and the lack of human
safety data for the effects of iodinated contrast media on the fetus,
although they approved to be safe in animal experiments. Therefore, any
search for PE in a pregnant patient should involve a thorough discussion
of the risks and benefits with the patient. If imaging is necessary with
ionizing radiation, the currently available data support the preferential use
of CTPA, if possible with a modified low-dose technique and limited
anatomical coverage.
Automated tube modulation should be used for all scans, regardless
if the patient is pregnant or not. However, as a first step, an
ultrasound of the legs is recommended as a surrogate test for
pulmonary embolism.
Pitfalls of CTPA
◙ Anatomic Pitfalls: PA’s run with bronchi, PV’s run
independent, Unopacified veins, Mucoid impaction,
Lymphadenopathy and perivascular tissue, Other
pathologies (Shunts, Sarcomas)
◙ Imaging Artifacts: Streak artifacts, Motion artifacts,
Improper bolus timing, inconsistent (“fractured”) bolus
Edge-enhancing reconstruction algorithm, Inadequate
window settings, Patient size
Pitfalls of CTPA
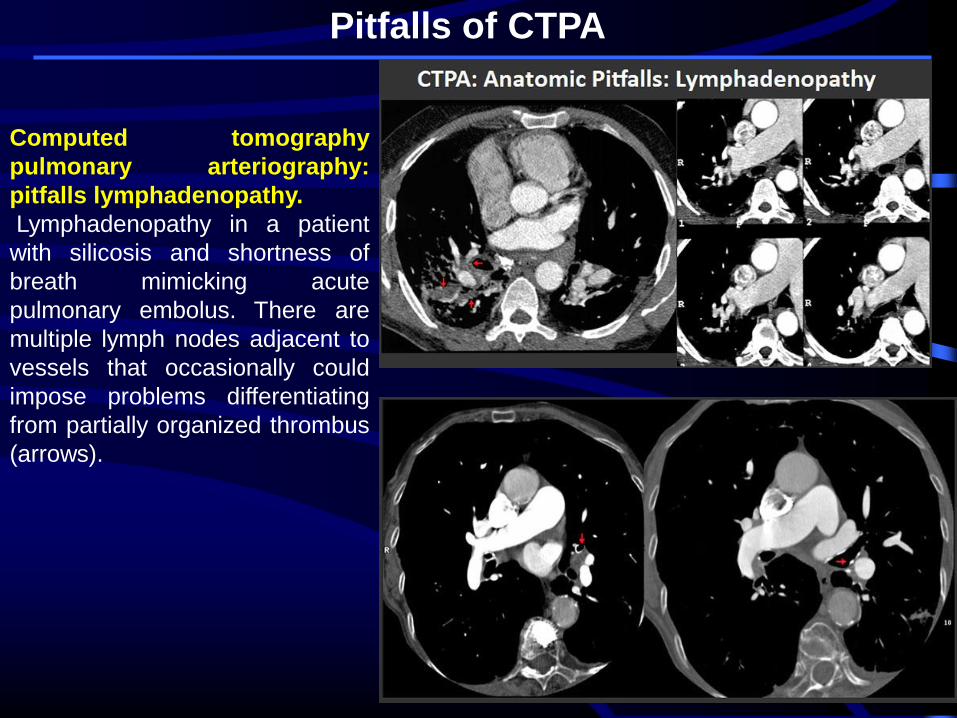
Computed tomography
pulmonary arteriography:
pitfalls lymphadenopathy.
Lymphadenopathy in a patient
with silicosis and shortness of
breath mimicking acute
pulmonary embolus. There are
multiple lymph nodes adjacent to
vessels that occasionally could
impose problems differentiating
from partially organized thrombus
(arrows).
Pitfalls of CTPA
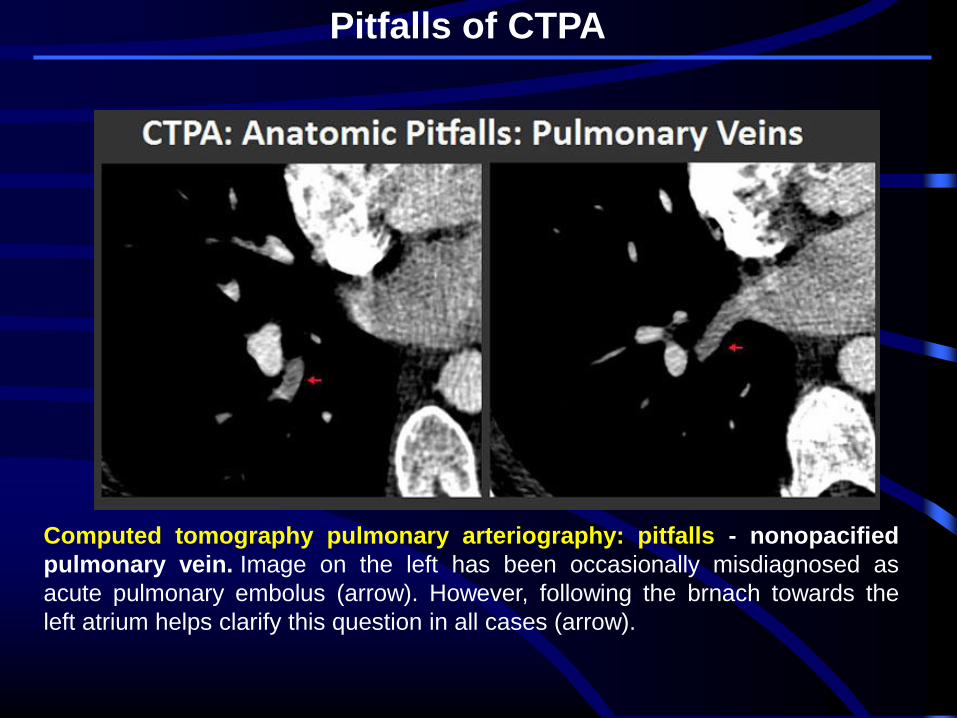
Computed tomography pulmonary arteriography: pitfalls - nonopacified
pulmonary vein. Image on the left has been occasionally misdiagnosed as
acute pulmonary embolus (arrow). However, following the brnach towards the
left atrium helps clarify this question in all cases (arrow).
Pitfalls of CTPA
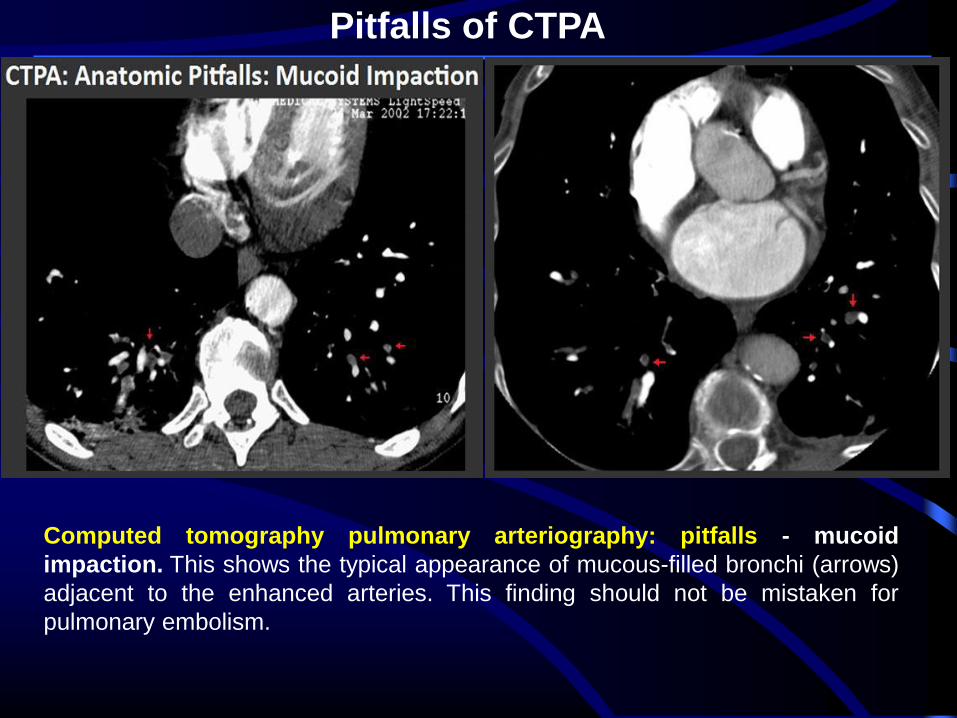
Computed tomography pulmonary arteriography: pitfalls - mucoid
impaction. This shows the typical appearance of mucous-filled bronchi (arrows)
adjacent to the enhanced arteries. This finding should not be mistaken for
pulmonary embolism.

Pitfalls of CTPA
Computed tomography pulmonary arteriography: pitfalls - volume
rendering. (Left) Pulmonary arteries that run in-plane parallel with bronchi can
occasionally appear less dense than the arteries running perpendicular to the imaging
plane. This is caused by partial volume averaging of the air-filled bronchi into the
pulmonary artery, thus artificially reducing its density (arrow). Reconstruction of the dataset
with thinner slices and/or oblique perpendicular multiplanar reconstructed images usually
help resolve this issue. (Right) True pulmonary embolus in a small branch to the middle
lobe running in-plane (arrow). There are also other emboli (arrowheads).
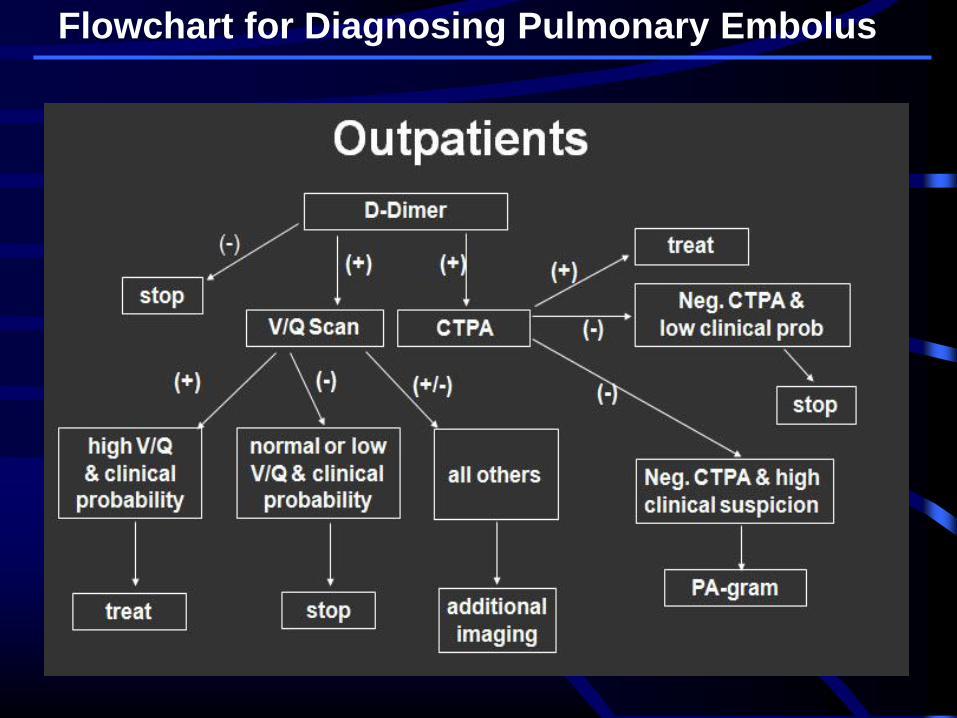
Flowchart for Diagnosing Pulmonary Embolus
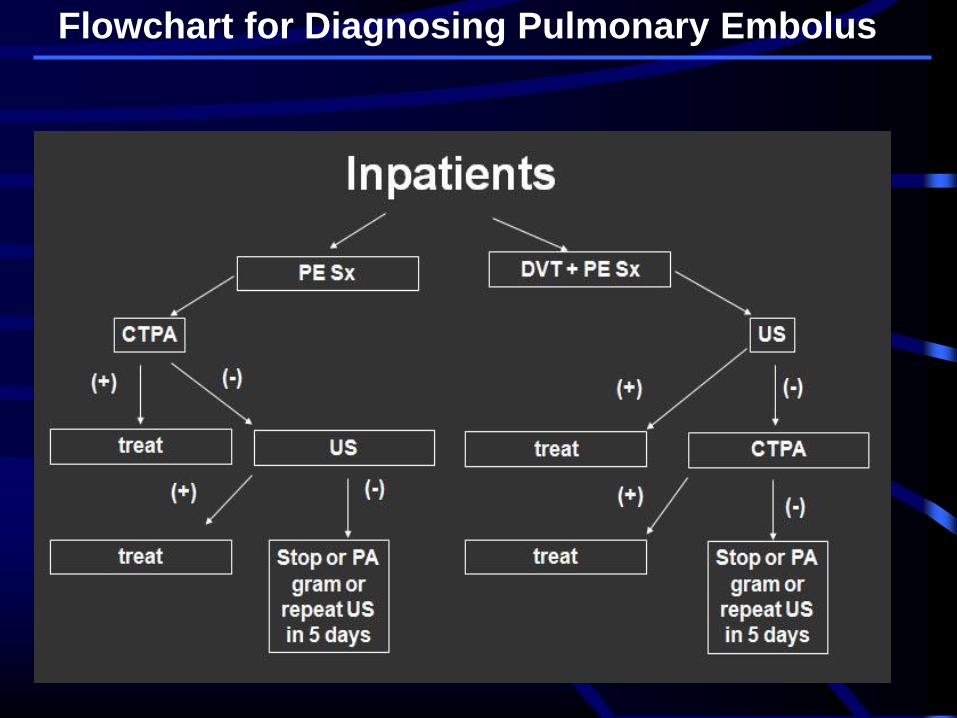
Flowchart for Diagnosing Pulmonary Embolus
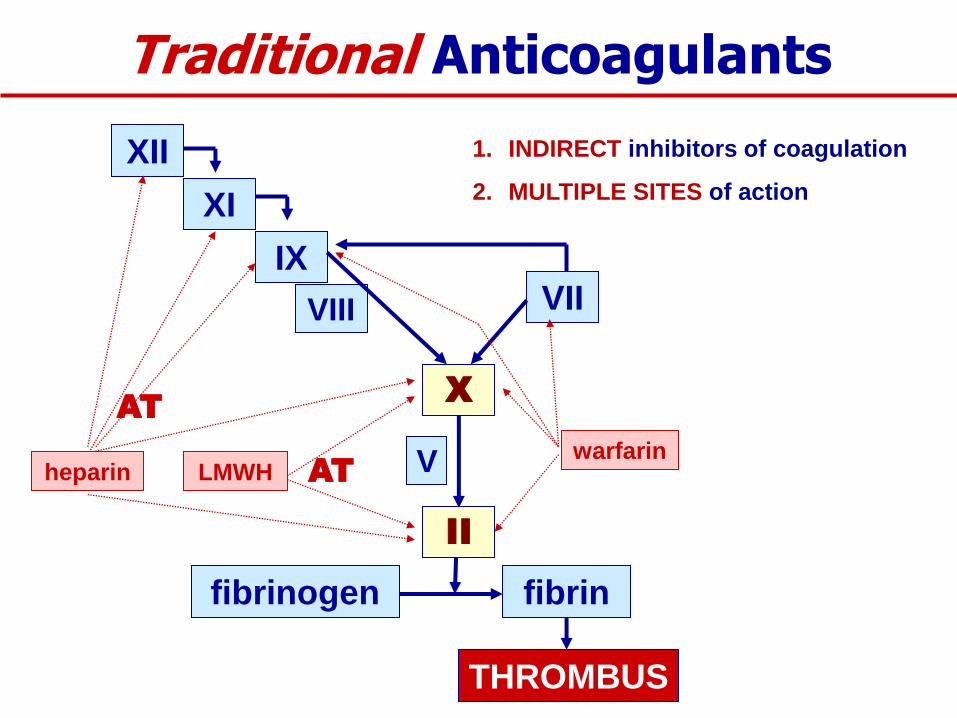
Traditional Anticoagulants
XII
XI
IX
VIII VII
V LMWH warfarin
X
heparin
1. INDIRECT inhibitors of coagulation
2. MULTIPLE SITES of action
THROMBUS
fibrinogen fibrin
II
AT
AT

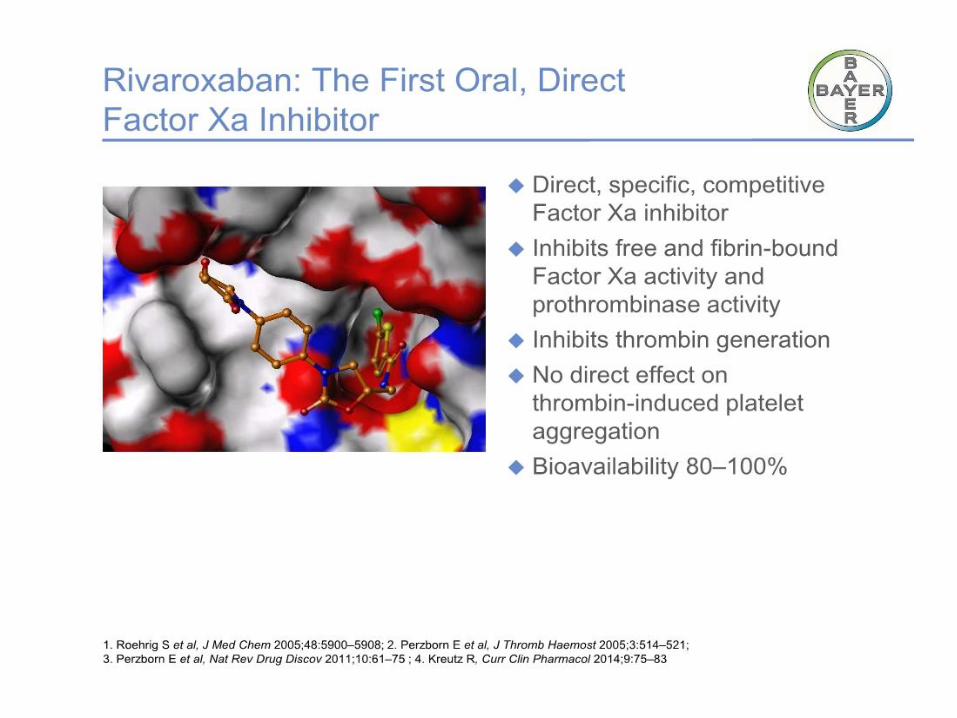
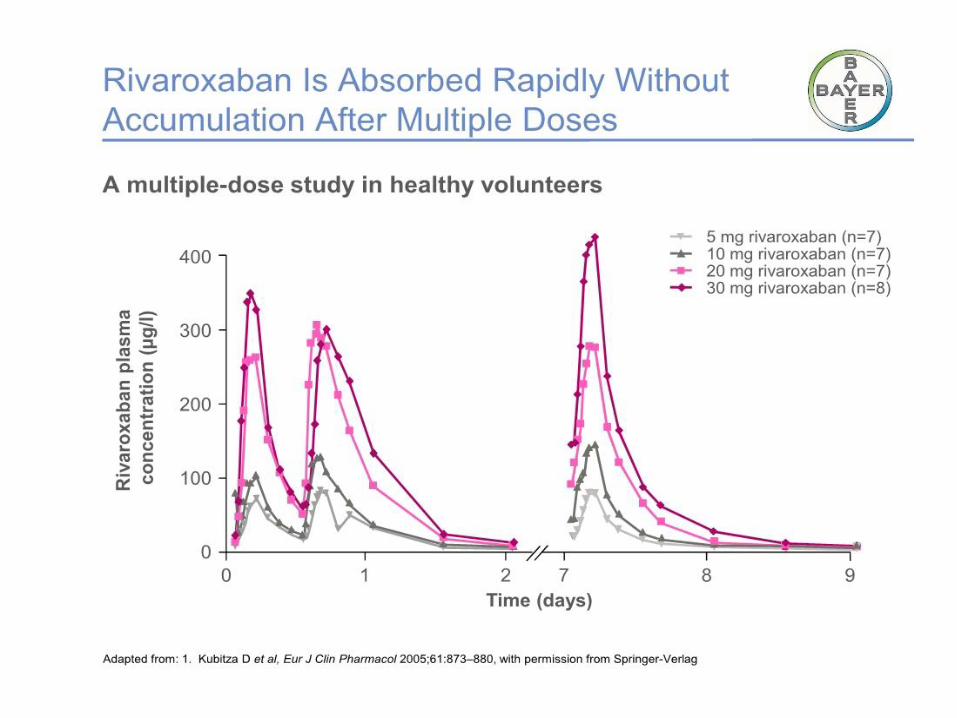
The new/novel oral anticoagulants (NOACs)
rivaroxaban (Xarelto®)
apixaban (Eliquis®)
dabigatran (Pradaxa®)
[edoxaban (Savaysa®)]
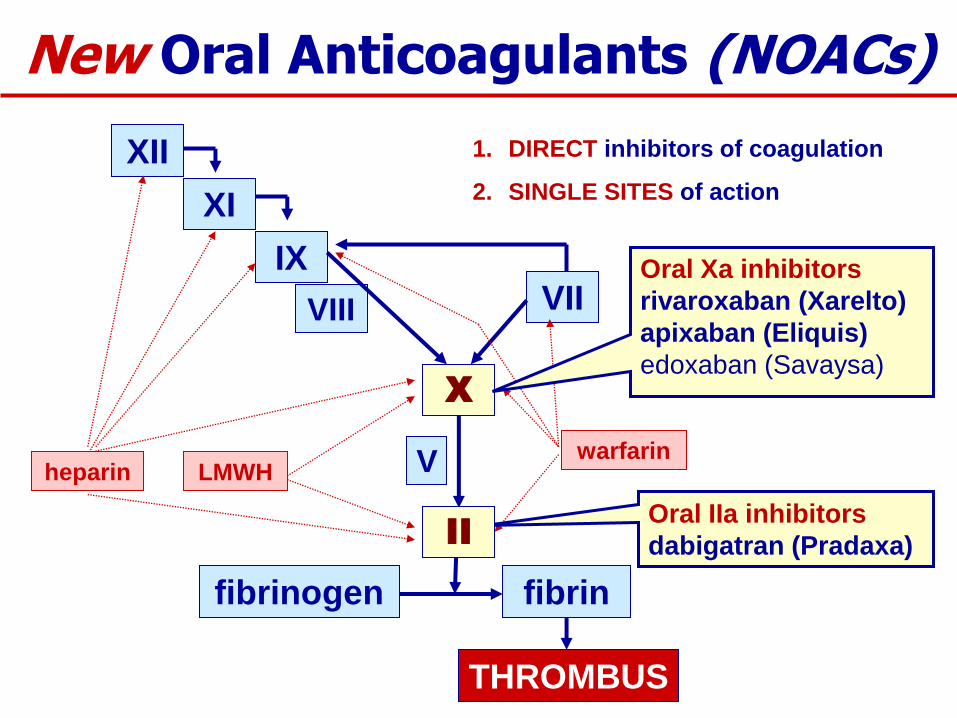
New Oral Anticoagulants (NOACs)
XII
XI
IX
VIII VII
V LMWH warfarin
X
Oral Xa inhibitors
rivaroxaban (Xarelto)
apixaban (Eliquis)
edoxaban (Savaysa)
Oral IIa inhibitors
dabigatran (Pradaxa)
heparin
1. DIRECT inhibitors of coagulation
2. SINGLE SITES of action
fibrinogen fibrin
II
THROMBUS

NOACs: Advantages
Property Advantages
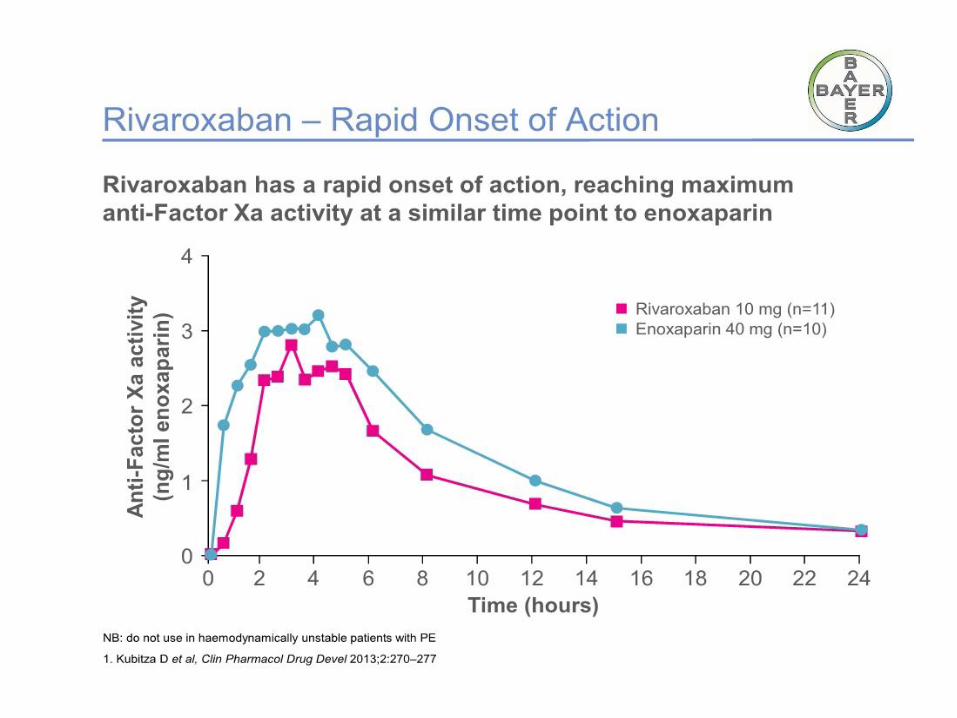
Rapid onset of action No need for IV/SC anticoag
Less variability in
anticoagulant effect
Fixed dose (or limited options)
No routine lab monitoring Convenient for patients, docs
Relatively rapid offset of
action
Simplifies pre-procedure Mx
Relatively inexpensive Generally affordable
All of the above Potential for greater/longer use
fewer thromboemboli

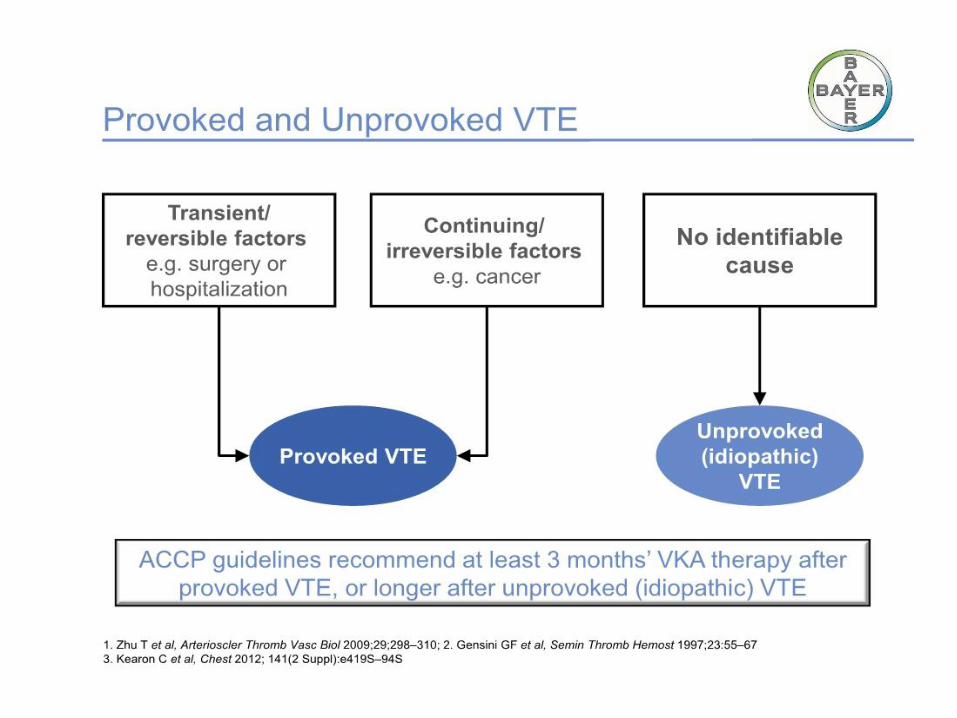
ACCP guidelines 2016
In patients with DVT of the leg or PE and
no cancer, as long-term (first 3 months)
anticoagulant therapy, we suggest
dabigatran, rivaroxaban, apixaban, or
edoxaban over vitamin K antagonist
(VKA) therapy (all Grade 2B).
Remarks: Initial parenteral anticoagulation
is given before dabigatran and edoxaban, is
not given before rivaroxaban and apixaban,

ACCP guidelines 2016
In patients with a proximal DVT of the leg or
PE provoked by surgery, we recommend
treatment with anticoagulation for 3 months
over (i) treatment of a shorter period (Grade
1B), (ii) treatment of a longer time-limited
period (eg, 6, 12, or 24 months) (Grade 1B),
or (iii) extended therapy (no scheduled stop
date) (Grade 1B)
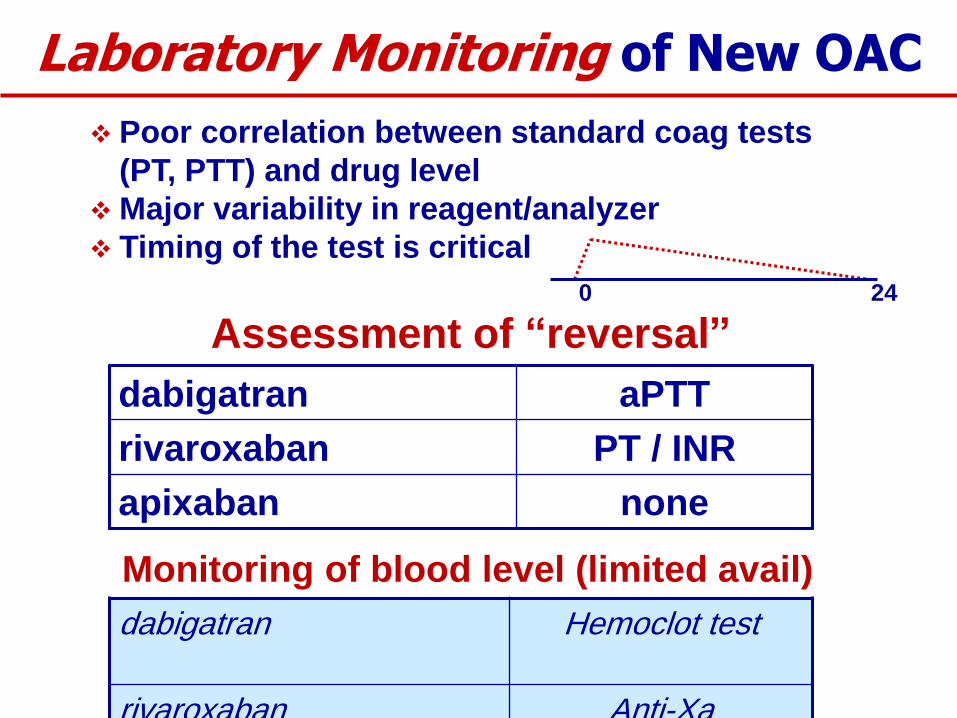
Laboratory Monitoring of New OAC
Assessment of “reversal”
dabigatran aPTT
rivaroxaban PT / INR
apixaban none
Monitoring of blood level (limited avail)
dabigatran Hemoclot test
rivaroxaban Anti-Xa
Poor correlation between standard coag tests
(PT, PTT) and drug level
Major variability in reagent/analyzer
Timing of the test is critical
0 24