Venous thromboembolism prophylaxis using the Caprini score · 250 I. Golemi, J.P. Salazar Adum and...
50
Disease-a-Month 65 (2019) 249–298 Contents lists available at ScienceDirect Disease-a-Month journal homepage: www.elsevier.com/locate/disamonth Venous thromboembolism prophylaxis using the Caprini score Iva Golemi, MD a,∗ , Juan Pablo Salazar Adum, MD a , Alfonso Tafur, MD, MS, RPVI b , Joseph Caprini, MD, MS, RVT c a Department of Medicine, NorthShore University HealthSystem, Evanston, IL, USA b Department of Medicine, Division of Cardiovascular Medicine, NorthShore University HealthSystem, USA c The University of Chicago Pritzker School of Medicine, Evanston, IL, USA a r t i c l e i n f o a b s t r a c t Venous thromboembolism (VTE) including pulmonary em- bolism (PE) and deep vein thrombosis (DVT) is one of the leading causes of preventable cardiovascular disease in the United States (US) and is the number one preventable cause of death following a surgical procedure. Post-operative VTE is associated with multiple short and long-term complications. We will focus on reviewing the many faces of VTE in detail as they represent common challenging scenarios in clinical practice. © 2018 Elsevier Inc. All rights reserved. PART ONE: THE MANY FACES OF VENOUS THROMBOEMBOLISM INCLDING RISK FACTORS Introduction Venous thromboembolism (VTE) is the number one preventable cause of death following a surgical procedure. 1 Anticoagulant prophylaxis postoperatively saves lives without increas- ing bleeding deaths. 2 Surgeons are understandably reluctant to employ these drugs for fear of bleeding complications which in some cases can result in poor clinical outcomes. 1 This re- view will demonstrate the value of individual risk assessment to tailor the use of anticoagulant ∗ Corresponding author: Address: 2650 Ridge Ave, Evanston, IL 60201, USA. E-mail addresses: [email protected] (I. Golemi), [email protected] (J.P. Salazar Adum), [email protected] (A. Tafur), [email protected] (J. Caprini). https://doi.org/10.1016/j.disamonth.2018.12.005 0011-5029/© 2018 Elsevier Inc. All rights reserved.
Transcript of Venous thromboembolism prophylaxis using the Caprini score · 250 I. Golemi, J.P. Salazar Adum and...
Disease-a-Month 65 (2019) 249–298
Contents lists available at ScienceDirect
Disease-a-Month
journal homepage: www.elsevier.com/locate/disamonth
Venous thromboembolism prophylaxis using
the Caprini score
Iva Golemi, MD
a , ∗, Juan Pablo Salazar Adum, MD
a , Alfonso Tafur, MD, MS, RPVI b , Joseph Caprini, MD, MS, RVT
c
a Department of Medicine, NorthShore University HealthSystem, Evanston, IL, USA b Department of Medicine, Division of Cardiovascular Medicine, NorthShore University HealthSystem, USA c The University of Chicago Pritzker School of Medicine, Evanston, IL, USA
a r t i c l e i n f o
a b s t r a c t
Venous thromboembolism (VTE) including pulmonary em-
bolism (PE) and deep vein thrombosis (DVT) is one of the
leading causes of preventable cardiovascular disease in the
United States (US) and is the number one preventable cause
of death following a surgical procedure. Post-operative VTE is
associated with multiple short and long-term complications.
We will focus on reviewing the many faces of VTE in detail
as they represent common challenging scenarios in clinical
practice.
© 2018 Elsevier Inc. All rights reserved.
PART ONE: THE MANY FACES OF VENOUS THROMBOEMBOLISM INCLDING RISK FACTORS
Introduction
Venous thromboembolism (VTE) is the number one preventable cause of death following
a surgical procedure. 1 Anticoagulant prophylaxis postoperatively saves lives without increas-
ing bleeding deaths. 2 Surgeons are understandably reluctant to employ these drugs for fear
of bleeding complications which in some cases can result in poor clinical outcomes. 1 This re-
view will demonstrate the value of individual risk assessment to tailor the use of anticoagulant
∗ Corresponding author: Address: 2650 Ridge Ave, Evanston, IL 60201, USA.
E-mail addresses: [email protected] (I. Golemi), [email protected] (J.P. Salazar Adum),
[email protected] (A. Tafur), [email protected] (J. Caprini).
https://doi.org/10.1016/j.disamonth.2018.12.005
0011-5029/© 2018 Elsevier Inc. All rights reserved.

250 I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298
p
o
d
c
e
f
c
d
r
t
p
d
e
p
a
p
d
f
c
t
i
p
M
p
t
o
P
t
t
s
5
t
e
r
V
2
V
m
m
t
t
m
u
N
T
“
rophylaxis. Patients with a low risk for thrombotic complications can be spared from the use
f anticoagulants without increasing thrombosis event rates and death from this serious disor-
er. High-risk patients who are at great risk for developing thrombotic episodes including death
an be targeted using appropriate drug regimes. These patients need drug prophylaxis for the
ntire period they are at risk in order to achieve the best results. Randomized control trial data
rom 160 centers over a 30-year period in 43,0 0 0 patients demonstrate that 7–10 days of anti-
oagulants is the proper course of prophylaxis to prevent most VTE events. 2–5 However, thirty
ays of prophylaxis has been shown to be more effective and is recommended for the highest
isk patients especially those with cancer and a previous VTE. 6 The popular policy of adminis-
ering anticoagulants only during hospitalization or until the patient is ambulatory has not been
roven to prevent most thrombotic events. A significant number of patients develop VTE after
ischarge from the hospital and often are not protected with anticoagulants. 7 The most pow-
rful risk associated with surgical patients is a history or family history of thrombosis. 8 These
atients are particularly prone to fatal VTE events and often patients are not specifically queried
bout this history. Those identified with this past history are often not protected due to the
erceived low risk of simple surgical procedures. Understanding that a minor surgical proce-
ure may be associated with a major thrombotic risk is not well understood. The incidence of
atal VTE events even in young people having so called “minor surgical procedures” is far too
ommon and almost totally preventable if their risk was properly assessed. 9 , 10 The administra-
ion of appropriate anticoagulant prophylaxis for the period of time that they remain at-risk
s relatively uncommon. This review will discuss these issues and illustrate the value of these
rinciples based on the vast body of available literature that exists today.
ajor public health concern
The precise number of people affected by DVT/PE is unknown, although as many as 60 0,0 0 0
eople could be affected (1 to 2 per 1,0 0 0) each year in the United States. 11 Estimates suggest
hat 60,0 0 0–10 0,0 0 0 Americans die of DVT/PE including 10 to 30% of people who will die within
ne month of diagnosis. Sudden death is the first symptom in about 25% of people who have a
E. 12 Among people who have had a DVT, one-half will have long-term complications including
he post-thrombotic syndrome, which presents with swelling, pain, discoloration, and scaling in
he affected limb. A number of other complications can also occur and will be subsequently de-
cribed. One-third of people with DVT/PE will have a recurrence within 10 years. Approximately
to 8% of the U.S. population has one of several genetic risk factors (inherited thrombophilias)
hat increase the risk for thrombosis. 13
Venous thromboembolism (VTE) is a major health problem, with over one million events
very year in Europe. 14 The annual incidence of fatal pulmonary emboli across Western Eu-
ope was estimated via an epidemiological model when the annual estimates for symptomatic
TE events were estimated to be 465,715 (404,664–538,189) cases of deep-vein thrombosis,
95,982 (242,450–360,363) cases of pulmonary embolism (PE), and 370,012 (300,193–483,108)
TE-related deaths. Of these deaths, an estimated 27,473 (7%) were diagnosed as being ante-
ortem; 126,145 (34%) were sudden fatal PE, and 217,394 (59%) followed undiagnosed PE. Al-
ost three-quarters of all VTE-related deaths were from hospital-acquired VTE. The estimated
otal number of VTE events (DVT and PE: 148 per 10 0,0 0 0 and 95 per 10 0,0 0 0, respectively) in
he EU is higher than that reported for US communities. Sandler et al demonstrated that pul-
onary embolism is a frequent complication in hospital patients with 10% of 2388 patients who
nderwent autopsy having died from PE. 15
eed for increased awareness
The International Society of Hemostasis and Thrombosis reported on the occasion of World
hrombosis Day (October 13th). This date was chosen since it was Professor Virchow’s birthday.
Thrombosis including VTE, ischemic heart disease, and ischemic stroke is a major contributor

I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298 251
to the global health burden.” The authors estimate that one of every 4 deaths worldwide are
due to these thrombotic events. In the US alone, the Center for Disease Control and Prevention
estimated that there were more than 50 0,0 0 0 adult hospitalizations with the diagnosis of VTE
each year from 20 07–20 09. VTE is responsible for more deaths each year than breast cancer, HIV
disease, and motor vehicle crashes combined. Furthermore, approximately 60% of VTE cases are
associated with a recent hospital stay, and the World Health Organization (WHO) patient safety
program found that hospital-associated VTE was the leading cause of death and disability as-
sociated with hospitalization among all countries and accounted for more deaths and disability
than nosocomial pneumonia, catheter-related bloodstream infections and adverse drug events.
Public awareness of VTE remains low with only 44% and 54% of respondents in a global survey
were aware that most cases are preventable. An important education goal of the World Throm-
bosis Day is to equip patients and family with the adequate knowledge to advocate for VTE
preventions especially in high risk settings like hospitalization. 16
The many faces of VTE
There is a group of physicians who believe the only important postoperative venous throm-
botic issue is symptomatic and fatal pulmonary emboli during hospitalization. 17 The following
section summarizes the numerous issues associated with a postoperative thrombosis including
short and long-term complications. These issues represent compelling rationale to prevent “The
Many Faces Of VTE” rather than just focus on only one aspect of this enormous health problem.
Pulmonary emboli (PE)
Pulmonary emboli (PE) represent the most dramatic of the thrombotic events and fatal em-
boli are seen in 1–5% of those with > 4 risk factors. One-third of all fatal events present as sud-
den death. The mortality in those that survive the initial event approaches 17% at 3 months. 18 , 19
Non-fatal pulmonary emboli may be severe and some massive events may dictate fibrinolytic
therapy occasionally associated with serious bleeding. The Pulmonary Embolism Response Team
concept (PERT) represents integrated and multidisciplinary teams designed to provide the best
standard of care for patients suffering from acute PE. These teams are becoming more com-
mon in clinical practice and it may soon become a new standard of care in patients with PE.
Kabherl et al reported on a 30 month follow up on patients for whom PERT was activated. Even
though PERT was initially conceptualized for patients with higher risk PE they found out that
the PERT team was incredibly valuable for patients with low risk PE or with complex/unstable
issues without confirmed PE. PERT has the ability to quickly mobilize resources that benefit pa-
tients, save lives, and provide efficient and prompt care. 20
Chronic pulmonary hypertension
One of the most serious consequences that patients who suffer and survive a PE is chronic
pulmonary hypertension. Chronic thromboembolic pulmonary hypertension (CTEPH) etiology re-
mains poorly understood but is thought to most often result from obstruction of the pulmonary
vascular bed by non-resolving thromboemboli. 21 , 22 Chronic emboli can result after acute or
recurrent PE or DVT. Increased pulmonary vascular resistance (PVR) leads to progressive pul-
monary hypertension and right heart failure. In the non-occluded areas, pulmonary arteriopa-
thy manifests in small to medium-sized muscular pulmonary arteries as intimal cellular prolif-
eration with focal disruption of the internal elastic lamina and media by “glomeruloid” small
vascular channels. These channels ramify into alveolar septal capillaries, can be indistinguish-
able from pulmonary arterial hypertension (PAH) and can contribute to disease progression. 23
The incidence of CTEPH is unknown, and it remains controversial if CTEPH is a direct conse-
quence of acute PE, but studies suggest that incidence of CTEPH may be 1% −3.8% within 2 years
of acute pulmonary embolism. 22 A prospective international registry reported a history of PE
252 I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298
i
c
f
a
n
e
t
s
i
p
t
2
a
H
i
n
r
w
T
d
e
s
a
m
c
s
l
C
s
a
B
m
D
t
f
t
o
h
s
b
S
r
n 74.8%, and a history of DVT in 56.1% of CTEPH patients, thus labeling CTEPH as a chronic
omplication of VTE. 22 Some risk factors for CTEPH and VTE include: previous splenectomy, in-
ected ventriculo-atrial shunts, indwelling venous catheters and leads, thyroid replacement ther-
py, cancer, and chronic inflammatory states. 22
Symptoms are absent in the initial phases of CTEPH and once symptomatic, symptoms are
onspecific and clinically indistinguishable from PAH, PE, or acute PE superimposed on pre-
xisting CTEPH. 22 Right-sided heart failure can manifest at later stages of the disease secondary
o right ventricular functional impairment. The incidence after a PE remains low, thus routine
creening for CTEPH is not feasible. 22 , 24
Without treatment, the prognosis of CTEPH is poor and depends on the hemodynamic sever-
ty of pulmonary HTN. 25 , 26 In contrast with other pulmonary hypertension subgroups CTEPH is
otentially curable by surgical intervention. 22 Pepke-Zaba et al reported results from an interna-
ional prospective registry of 679 newly diagnosed patients ( ≤ 6 months) who were followed for
years. 427 patients (62.9%) were considered operable while 247 (36.4%) were non-operable,
nd 5 (0.7%) had no operability data.
Operable patients did not differ from non-operable patients relative to symptoms, New York
eart Association class, and hemodynamics. At the time of CTEPH diagnosis, 37.7% of patients
nitiated at least 1 pulmonary arterial hypertension–targeted therapy (28.3% operable, 53.8%
on-operable). Pulmonary endarterectomy was performed with a 4.7% documented mortality
ate. This study concluded that given the similarities between the groups, careful diagnostic
orkup is necessary to assess which patients will be good candidates for operative procedures.
hey also noticed that patients in the operable group were more likely to have thrombophilic
isorders. This registry data highlights the importance of previous venous thromboembolism
vents as a causal factor for the development of CTEPH, along with a significant role for as-
ociated medical risk factors as coexisting mechanisms in the disease process. The registry data
lso indicate that, although pulmonary endarterectomy can be performed with a low in-hospital
ortality rate, operability rates may vary considerably across centers and countries. 27
Removal of the obstructive material from the pulmonary vasculature is the treatment of
hoice to alleviate pulmonary obstruction and reduce resistance, but in 50% of patients the ob-
tructions are technically inaccessible, or the risk/benefit ratio is unfavorable. 22 , 28 Lately, bal-
oon pulmonary angioplasty (BPA) has emerged as a valuable treatment option for inoperable
TEPH.
The ELOPE study indicates that almost half of PE patients can be considered to have a post-PE
yndrome characterized by exercise limitation at 1 year which impairs their quality of life (QOL)
nd degree of dyspnea. Predictors of post-PE syndrome include male sex, younger age, higher
MI and smoking. Cardiopulmonary exercise testing (CPET) or 6-minute-walk test (6MWT) at 1
onth many help to identify patients with higher risk for post-PE syndrome at 1 year. 29
eep vein thrombosis (DVT)
Deep vein thrombosis (DVT) is a serious and sometimes life-changing event for many pa-
ients. Major DVT requires appropriate anticoagulation treatment for months or in many cases
or years when the event results from an unknown cause. The use of anticoagulants may dic-
ate refraining from contact sports, or activities such as skiing, and other winter sports for fear
f excessive bleeding in case of injury. Rarely the use of anticoagulants may be associated with
eparin-induced thrombocytopenia with or without thrombosis. 30 Warfarin-induced skin necro-
is is also a rare but potentially devastating complication. 31 Venous gangrene with limb loss may
e a result of these complications.
ilent venous thromboembolism
Borow reported that 66% of patients having surgery who had a previous DVT suffer a recur-
ent event without postoperative prophylaxis. 32 The incidence of recurrent DVT in those with
I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298 253
previous asymptomatic events is unknown but likely to be greater than those without that his-
tory. One study enrolled 150 high-risk patients in an internal medicine service with consecutive
hospitalization for another diagnosis, not DVT, who underwent Doppler US of the lower extrem-
ities. Four and one-half percent of patients were diagnosed with proximal DVT and 16% with
distal DVT (dDVT). Female sex, elevated age and renal and electrolyte abnormalities were sig-
nificantly associated with dDVT (p = 0.014, p = 0.009 and p = 0.046, respectively). Decreased mo-
bility was independently associated with dDVT [OR 7.97 (95% CI 2.42–26.27), p = 0.001)]. A high
mortality rate, for non-VTE-related causes, was found, especially in the first week, among dDVT
patients. 33 Another study evaluated 294 patients over a 24-month period in a surgical inten-
sive care unit. Prevalence of DVT was 7.5% in this population and no clinical signs of DVT were
present. DVT was identified within major vessels including iliac vein 1.7%, common femoral vein
2.7%, superficial femoral vein 2% and popliteal vein 1%. In this study age, APACHE II score ≥ 12
and emergent procedure were identified as risk factors for presence of DVT. 34 Another study
included 71 patients who underwent total hip arthroplasty (THA) and 30 patients who under-
went total knee arthroplasty to study the prevention of asymptomatic DVT with fondaparinux
prophylaxis. In patients who received fondaparinux for 14 days after THA surgery, the incidence
of DVT was 0% on the day of the surgery, 13.6% at day 1, 27.1% at day 4, and 11.9% at day 14.
In patients who received fondaparinux for 14 days after TKA surgery, the incidence of DVT was
4.2% on the day of surgery, 50.0% at day 1, 58.3% at day 4, and 20.8% at day 14. The incidence of
DVT after THA or TKA surgery at day 14 was significantly reduced compared to that at day 4. 35
Asymptomatic DVT remains an understudied entity and more data is necessary to understand
its prevalence and clinical significance.
Post-Thrombotic syndrome (PTS)
Incidence ranges from 25–50% following DVT and the clinical manifestations may not be ap-
parent for 2–5 years after the DVT. In a considerable portion of patients, the thrombus fails to
resolve resulting in obstructive changes or valvular incompetence years after the event. 22 This
syndrome can occur in cases of not only proximal DVT but calf DVT and asymptomatic DVT.
Chronic complications from DVT and/or PE can occur. PTS is associated with symptoms and
signs that can vary between patients but most frequently include: pain, heaviness, cramps and
persistent swelling of the affected extremity. Edema, telangiectasia, hyperpigmentation, lipoder-
matosclerosis and ulceration might be present. Prognosis depends on the affected anatomic seg-
ment and the patency of the involved vessel. 22 Proximal DVT has an increased risk for develop-
ing PTS compared with calf or popliteal vein DVT. 22 , 36 Iliofemoral DVT carries a higher risk of
recurrence, and the incidence of PTS is high despite anticoagulation. 37 PTS is diagnosed based
on clinical symptoms and venous duplex US. Symptoms can be exacerbated by exercise and im-
prove with rest. 22 Different scoring systems for PTS exist including The Villalta scale, Ginsberg
score, and Brandjes score. 38 The Villalta score combined with a venous disease-specific quality-
of-life questionnaire is considered the current gold standard for diagnosis and classification of
PTS. 38
Use of elastic compression stockings (ECS) after DVT is the first treatment choice to prevent
PTS by reducing leg edema, promoting venous blood return and improving venous pump func-
tion. 22 Several studies have shown the benefits of using ECS. 39 Brandjes et al. observed a 50% re-
duction in the incidence of PTS due to ECS. 40 Elastic compression stockings are also helpful once
PTS has developed as they increase fibrinolytic activity, stimulate collateral formation and help
prevent venous ulceration. 22 , 41 Aspirin 300 mg daily was tested in a small RCT and improved
rates of ulcer healing. 42 Pentoxifylline is a xanthine derivative that has been used for several
decades in the symptomatic management of intermittent claudication. 43 It also influences mi-
crocirculatory blood flow and oxygenation in ischemic tissues even though the mechanism is
uncertain. 44 In a Cochrane literature review of 12 trials 864 participants were included to as-
sess the role of pentoxifylline in treating venous leg ulcers. Pentoxifylline is more effective than
placebo in terms of complete ulcer healing (RR 1.70, 95% CI 1.30 to 2.24). Pentoxifylline plus
254 I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298
c
2
n
c
a
E
c
r
p
f
d
u
t
m
l
s
d
1
p
A
a
t
m
t
t
a
V
i
t
h
l
p
w
g
v
b
l
8
a
a
o
l
s
h
o
t
t
ompression stockings is more effective than placebo plus compression (RR 1.56, 95% CI 1.14 to
.13). Pentoxifylline in the absence of compression appears to be more effective than placebo or
o treatment (RR 2.25, 95% CI 1.49 to 3.39). More adverse effects were reported in people re-
eiving pentoxifylline (RR 1.56, 95% CI 1.10 to 2.22). Nearly three-quarters (72%) of the reported
dverse effects were gastrointestinal including nausea, indigestion and diarrhea. 44
Several years ago a large placebo controlled randomized trial was published indicating that
CS do not prevent PTS in the first 2 years in patients with a first proximal DVT 45 The authors
onclude-“ECS did not prevent PTS after a first proximal DVT, hence our findings do not support
outine wearing of ECS after DVT .” This statement is misleading since many physicians routinely
rescribe ECS to control the acute symptoms of pain, swelling, heaviness, and other symptoms
requently associated with acute DVT. I would have preferred a statement saying that the trial
oes not support the routine use of ECS to prevent PTS, but these stockings may indeed be
seful to control the patient’s symptoms. A number of methodological issues exist with this
rial and are best summarized in an editorial commenting on this trial. 46 It is apparent that
ore research is needed to identify the role of ECS for the prevention of PTS.
In selected patients with PTS surgical or endovascular treatments can be performed to re-
ieve symptoms. 22 Percutaneous transdermal recanalization of the iliac venous outflow tract by
tent angioplasty is an emerging trend for treatment of PTS. 22 The CaVent study tested Catheter-
irected thrombolysis (CDT) using Alteplase to reduce PTS and the absolute risk reduction was
4.4%. 47 PTS has been associated with higher healthcare expenses and worse quality of life of
atients and its adverse impact is comparable with diabetes and congestive heart failure. 22 , 48 , 49
large NIH supported clinical trial has recently been completed comparing standard antico-
gulation to pharmaco-mechanical fibrinolysis. “(catheter-mediated or device-mediated intra-
hrombus delivery of recombinant tissue plasminogen activator and thrombus aspiration or
aceration, with or without stenting). The primary outcome was development of the post-
hrombotic syndrome between 6 and 24 months of follow-up. The study showed that the addi-
ion of pharmaco-mechanical catheter-directed thrombolysis to anticoagulation did not result in
lower risk of the post-thrombotic syndrome but did result in a higher risk of major bleeding. 50
enous insufficiency-induced lymphedema
Lymphedema is classified into primary and secondary types. Primary lymphatic dysfunction
s of congenital or idiopathic origin. Secondary lymphedema is from damage to lymphatic struc-
ures from parasites, surgery, radiation, infection, most commonly cellulitis or chronic venous
ypertension due to chronic venous disease (CVD). 51 , 52 Up to 1/3 of patients with CVD will have
ymphatic dysfunction by isotope lymphangiography suggesting that secondary lymphedema is
robably more common than the primary variety. Treatment of lymphedema is a necessary step
hen treating extremity ulcers. 51 , 53 Raju et al concluded that clinical features, isotope lymphan-
iography, routine duplex imaging, and venography (sensitivity 61%) cannot reliably rule out a
enous cause for lymphedema and suggested that intravascular ultrasound IVUS (sensitivity 88%)
e routinely used. Swelling improved significantly after stent placement with significant pain re-
ief [complete swelling relief was 16% and 44% ( P < 0.001); pain relief at 40 months was 87% and
3%, respectively ( P = 0.3), with 65% and 71%, experiencing complete pain relief in the abnormal
nd normal lymphangiographic groups]. 51
Compression stockings can be helpful for lymphedema management. 51 There is little data
bout the optimal amount of pressure needed for edema reduction. The International Society
f Lymphology recommends the highest level tolerated; however, Partsch suggests that even
ow pressures can achieve significant lymphedema reduction. 53 Inelastic compression bandages
hould be applied at the start of treatment for patients with chronic edema, as they provide
igh pressures both when standing and walking. They also have a strong massaging effect and
ffer intermittent compression during walking and a low pressure when lying down, and tend
o be well tolerated by the patient over time due to the reduction in edema which decreases
he leg circumference. However, inelastic systems retain stiffness, thereby maintaining effective
I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298 255
pressure in the upright position for several days. 53 The commonly used elastic (ACE) bandages
are ineffective for reducing edema, and swelling may increase with these bandages in place. 54
One of the major issues with compression stockings is noncompliance among patients even
in the presence of severe symptoms, and medical supervision and patient education have not re-
sulted in better compliance. Manual drainage and decongestive therapy are effective techniques
when properly administered. Massage techniques do not correct the basic pathology, however,
and intensive lifelong daily compliance is necessary. In venous lymphedema, it is best used in
conjunction with correction of venous pathology. 53
A most important compression modality for the treatment of leg swelling including lym-
phedema is Velcro compression. A number of devices are available which consist of overlapping
Velcro straps made from inelastic material. They are quite easy to apply and remove, and as the
leg swelling decreases they can be tightened to further reduce leg swelling.
Paradoxical embolus
Paradoxical embolism (PDE) describes the passage of venous or right-sided cardiac thrombus
into the arterial systemic circulation. 55 PDE should be suspected in cases where ischemic stroke
occurs in the absence of conventional risk factors for cerebral vascular disease indicating an al-
ternative mechanism. Forty percent of strokes have no identifiable or proven cause. This occurs
most commonly through an intracardiac defect at the atrial level, but it can also occur via in-
terventricular or pulmonary arteriovenous malformations. 55 , 56 It has been suggested that PDE
could account for as many as 47,0 0 0 unexplained ischemic strokes in young patients each year.
In a small retrospective study with 13 patients with PDE, saline solution contrast echocardiogra-
phy was used as a useful method to demonstrate patent foramen ovale (PFO). Treatment varied,
but all patients received anticoagulation initially with heparin. The duration of therapy was in-
dividualized with patients receiving 6–12 months of anticoagulation. Surgical embolectomy was
performed for 8 patients presenting with limb-threatened ischemia. Intravenous unfractionated
heparin was administered followed by oral anticoagulation. An IVF filter was placed below the
renal veins and no acute limb loss was reported. One patient had surgical closure of PFO with
right atrial thrombectomy. 55 PFO rates are higher in cryptogenic stroke than in the general popu-
lation. In a meta-analysis of 23 case-control studies the odds ratio for PFO in cryptogenic stroke
patients compared with those with stroke from known cause was 2.9 (95% CI 2.1–4.0) which
was similar to Handek et al who prospectively studied 503 consecutive acute stroke patients
and observed that compared with stroke from a determined cause, the PFO rate in cryptogenic
stroke is significantly greater. 56 , 57 Another prospective study of 504 patients investigated the
presence of patent foramen ovale (PFO) in patients younger and older than 55. Two hundred
twenty seven patients with cryptogenic stroke were compared with 276 patients with known
causes of stroke. All patients received transesophageal echocardiogram for PFO evaluation in-
cluding the 131 younger patients.
Concluding that there is an association between the presence of patent foramen ovale and
cryptogenic stroke between both older and younger patients odds ratio, 3.70; 95% CI, 1.42 to
9.65; P = 0.0 08) and the older group (odds ratio, 3.0 0; 95% CI, 1.73 to 5.23; P < 0.001) 57
The above data reflect the enormous burden on society as a result of the many faces of VTE,
and these disorders provide compelling evidence for employing appropriate thrombosis prophy-
laxis to patients based on their level of risk. Balancing the risks of thrombosis and bleeding in
each individual is critical to minimize adverse postoperative events. The authors wish to em-
phasize that deaths from prophylactic anticoagulation are extremely rare, while deaths from
withholding anticoagulation for “at-risk” patients are common. Data published over the last 4
decades will support these strong statements.
Risk assessment
Evaluation of the individual patient represents a complex problem. A list of individual risk
factors that are associated with VTE have been known for a long time. 19 Over the years new

256 I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298
f
a
p
e
v
V
(
t
m
e
r
f
V
f
q
t
t
C
p
i
p
m
fi
e
p
m
s
s
i
o
a
v
r
a
r
V
p
a
d
t
d
1
1
f
o
o
actors have appeared that increase the risk of a thrombotic event. It is a daunting task to review
ll of these factors but if one fails to account for a potentially important risk factor, appropriate
rophylaxis for that level of risk may not be prescribed. The result may be a serious or fatal VTE
vent. Complicating this analysis is that the tendency of these factors to result in thrombosis
aries; i.e, bedrest is not as strong a risk factor as cancer or major surgery. A past history of
TE was identified as one of the greatest risks for developing a VTE postoperatively. 7 Borow
1981) found that in patients not receiving prophylaxis, there was a 66% chance of recurrent
hrombosis postoperatively in those with a past VTE history. Young age is associated with a
inimal increase in risk compared to older patients where the risk is quite substantial. 58 Howel
t al demonstrated that congestive heart failure was an independent risk factor for VTE, and the
isk increased with decreasing left ventricular ejection fraction. 59 Summarizing, the more risk
actors present the higher incidence of VTE. The more potent the risk factor, the more likely a
TE will result. A past history of VTE or current malignancy are among the most powerful risk
actors that may result in a postoperative thrombotic event.
For many years there was little understanding of how these various risk factors interact in a
uantitative manner to determine the position of each patient along a continuous spectrum of
hromboembolic risk. During this era, clinical trial data in specific surgical populations was used
o estimate risk according to the type and complexity of the surgical procedure. 60
onsensus guidelines vs. Clinical judgment
We discourage blindly following consensus guidelines without first determining whether the
atients in studies used to develop the guidelines fit a particular patient in question. As seen
n the quote below the guidelines emphasize the importance of careful clinical analysis of the
atients’ risk before deciding about the prophylaxis strategy for that individual. This means one
ay not follow the guideline recommendations for an individual patient because their risk pro-
le has not been tested in clinical trials. These trials commonly exclude very high-risk patients
specially those with a history or family history of thrombosis, or multiple comorbidities. These
atients must be protected due to their level of risk. The Caprini score provides an acceptable
ethod to calculate individual risk, and recommend a prophylactic program tied to the final
core. The Boston Hospital system described later in the chapter is a good example of how this
ystem works. 61
The CHEST Guidelines included the following statement: “In this review, thromboprophylaxis
s recommended for groups of patients for whom the benefits of this intervention appear to
utweigh the risks. Decisions about prescribing thromboprophylaxis for the individual patient
re best made by combining knowledge of the literature (including the recommendations pro-
ided herein) with clinical judgment, the latter based on specific knowledge about each patient’s
isk factors for VTE, the potential for adverse consequences with thromboprophylaxis, and the
vailability of various options within one’s center.
Since most thromboprophylaxis studies excluded patients who were at particularly high
isk for either VTE or adverse outcomes, their results may not apply to those with previous
TE or with an increased risk of bleeding. In these circumstances, clinical judgment may ap-
ropriately warrant use of a thromboprophylaxis option that differs from the recommended
pproach.”62
The following quote from the CHEST 2012 guidelines may help to clarify the spirit of this
iscussion. 63 “A Cochrane systematic review analyzed data from six randomized trials involving close
o 1,500 patients who required lower-leg immobilization for at least 1 week and comparing once-
aily LMWH vs no thromboprophylaxis continued, typically, until the cast or brace was removed.27 We identified an additional multicenter study that has remained published only in abstract form28 and updated the meta-analysis by performing our own analysis. We did not extract the data
ound in the Cochrane review. PE was diagnosed in two of 585 patients in the placebo group and
ne of 576 in the LMWH group. Results failed to demonstrate or exclude a beneficial effect of LMWH
n symptomatic DVT (RR, 0.34; 95% CI, 0.09–1.28), and two major bleeding events were seen with
I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298 257
LMWH vs none in the placebo group. The patient population was quite heterogeneous, and
patients with a higher risk for VTE were excluded. Detailed information was not provided
with regard to immobility. ”
Based on that text the summary statement in the guidelines is as follows:
“3.0. We suggest no prophylaxis rather than pharmacologic thromboprophylaxis in patients
with isolated lower-leg injuries requiring leg immobilization (Grade 2C).”
Let us now try to apply those guidelines to an individual patient.
Clinical vignette
A 60-year-old male was struck by a car while riding his bicycle. He suffered a compound
fracture of the ankle involving both bones and requires an external fixator to stabilize the frac-
ture until the wound heals and definitive surgery can be done. His mother had a DVT and his
sister suffered a non-fatal pulmonary embolus. Patient has limited mobility due to the hardware
and painful nature of the injury.
He is very high-risk due to the nature of his injury, marked immobility, and family history of
thrombosis. Anticoagulant prophylaxis in my view is required in this situation and selecting an
approach not recommended in the guidelines may be life-saving.
The patient had a pulmonary embolus and died 10 days after the injury. He did not receive
anticoagulant prophylaxis. The surgeon defended his approach stating the guidelines do not rec-
ommend anticoagulant prophylaxis. Hypothetically if you were that surgeon would you provide
prophylaxis to a future patient you encounter with the same set of clinical circumstances? This
type of patient with these characteristics has not been tested in clinical trials. The clinician must
use judgment, knowledge of risk factors, experience, and in some cases common sense to pro-
vide protection for the patient. In the final analysis, the decision to use anticoagulant prophy-
laxis is based on carefully weighing the evidence for thrombosis vs. bleeding, and providing the
safest course of action for the patient. It also stands to reason, but not often mentioned, that
the prophylaxis for thrombosis needs to be continued as long as the patient remains at risk. In
the case of braces and casts that period continues until these devices have been removed and
the patient is ambulating normally.
Those who have practiced for any length of time fully realize that individual patient decisions
are based on clinical judgment and experience as well as the guidelines. When the individual
patient does not fit the criteria outlined in the guidelines, or when following the guidelines
results in a poor clinical outcome, a different course of action is warranted. Clinical experience
over the years continues to refine this process.
Risk factors associated with the development of VTE
Age
Borow (1981) studied the relationship of age to the development of DVT and found a linear
relationship. 7 The incidence of DVT in those 40–60 years of age was 20%, and in those 61–
70 years of age the incidence was 36.4%, while when patients 71 years of age or more this
incidence rose to 62.5%. He also reported that in patients receiving prophylaxis the incidence of
DVT although lower overall, doubled in patients 61–70 years, and tripled in those 71 years of
age and above.
Anderson and colleagues conducted a community-wide study in 16 short-stay hospitals to
examine the incidence and case-fatality rates of DVT and PE in patients during an 18-month
period starting in July 1985. There were 151,349 acute-care discharges from the 16 hospitals and
VTE was found in 1372 patients (0.9%). Furthermore, the proportion of patients with clinically
suspected DVT in whom the diagnosis was confirmed by objective testing increased with the

258 I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298
n
a
P
s
O
d
i
i
e
a
o
t
s
O
y
s
B
o
o
g
2
2
[
a
t
s
l
a
o
o
–
H
o
p
c
t
w
w
b
e
umber of risk factors. The incidence of thrombosis was 100% in patients who had 5 risk factors
nd were suspected clinically of having a DVT. They found that the incidence rates of DVT and
E increased exponentially with age. These incidence rates increase with age and rising Caprini
core that assigns points based on the age of the patient beginning with age over 40 years.
besity
Obesity is a common finding in the population with a prevalence of 20–25% and has been
efined as a body mass index (BMI) ≥ 30 kg/m
2 . Studies have shown that the risk of thrombosis
s increased twofold in these patients. On the other hand, women with a BMI > 25 kg/m
2 are at
ncreased risk for developing thrombosis, and if they are taking oral contraceptive a synergistic
ffect occurs increasing their risk by 10-fold. The thrombotic risk is increased with advanced
ge, but adjustment for clotting factor levels were shown not to affect the risk estimate for
besity. 64 White and colleagues, using an administration database in patients who underwent
otal hip arthroplasty, found that a body-mass index of 25 kg/m
2 or greater was associated with
ubsequent re-hospitalization for thromboembolism. 65
Obesity has emerged as a global health issue and there is moderate association with VTE.
besity appears to be associated with increased risk for first occurrence of VTE. 66 In a metanal-
sis of 8125 patients with VTE and 23,272 control patients indicated that the likelihood of first
pontaneous VTE among obese patients was more than twice that of individuals with normal
MI (odds ratio (OR) = 2.33; 95% confidence interval (CI), 1.68 – 3.24). 67
Increase in BMI above normal values has been reported to be associated with rising risk
f VTE. One study of 87,226 women in the Nurses’ Health Study showed that the relative risk
f unprovoked PE is raised by 8% per 1 kg/m
2 increase in BMI and approaches nearly six fold
reater risk in individuals with BMI ≥ 35 (p < 0.001). 68 In a large Danish study that enrolled
9,340 women and 26,674 men found that VTE was [HR: 1.45 ((1.03–2.05)], [HR: 1.81 (1.27–
.56)], [HR: 2.82, (1.96–4.04)] in females and [HR: 0.98, (0.73–1.31)], [HR:1.32 (0.98–1.79)] and
HR: 1.72 (1.27–2.33)] in men with BMIs of 23.7 – 26.3 (24.4 – 26.8), 26.3 – 29.9 (26.8 – 29.4),
nd > 29.9 ( > 29.4) respectively after adjusting for age, physical activity, smoking, height, choles-
erol, hypertension, diabetes mellitus, and use of hormone replacement therapy. 69
Several studies have indicated a relationship between obesity and VTE recurrence. 66 In one
tudy 1107 patients were followed for an average of 46 months after termination of anticoagu-
ation therapy and they found the frequency of recurrent VTE was 9.3% (95% CI, 6.0% – 12.7%)
mong patients with a normal BMI and 17.5% (95% CI, 13.0% – 22.0%) among patients who were
bese. 70
The association between VTE-related mortality and PE has yet to be explained. Unexpectedly,
besity appears to be protective and associated with lower mortality among patients with PE
the so called “obesity paradox”71
istory of VTE
Individuals who have suffered a previous VTE event are at increased risk for developing an-
ther thrombosis including a fatal pulmonary embolus. This factor is particularly important in
atients requiring surgery, subject to prolonged immobilization, or serious illness especially can-
er. In an observational study of 1231 patients, Anderson and colleagues reported that 19% of
hese individuals had a prior history of thrombosis. 72 In another case-controlled study, patients
ere eight times more likely to suffer a recurrent event during a high-risk period than those
ithout a VTE history. 73 Borow & Goldson many years ago reported in a large venographic-
ased study that 66% of patients with a prior history of VTE suffered a recurrent event postop-
ratively. 74 , 75
I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298 259
Family history of VTE
Family history of thrombosis has been the most neglected risk factor and is frequently not
even asked preoperatively. Several widely used thrombosis risk assessment models in medical
patients do not even include family history. Studies show that family history is a risk indica-
tor for a first venous thrombosis regardless of the other risk factors identified in an individual
patient. In clinical practice family history may be more useful for risk assessment than throm-
bophilia testing. 76 Family history of VTE may reflect family genetic risk factors. We know that
carriers of one or more genetic risk factors are at increased risk of the first venous thrombosis,
particularly when exposed to environmental triggers. These triggers may include surgery, muscle
ruptures or sprain, immobilization, plaster cast, extended bed rest, hospitalization, pregnancy or
puerperium, use of oral contraceptives or hormonal therapy, diagnosis of malignancy, etc. The
relative risk of thrombosis increases with the number of risk factors identified. The combination
of a genetic and acquired risk factor can result in a risk 60-fold higher than for those with no
known risk factors and a negative family history. One study showed a positive family history
increased the risk of venous thrombosis more than twofold regardless of the risk factors precip-
itating the thrombosis. 76 In that same study 29.7% of patients with a positive family history had
a genetic risk factor when tested. In addition, the chance of finding a genetic risk factor was up
to 36.1% for patients with several affected relatives. The authors also concluded that the relative
risk associated with a positive family history was of similar magnitude as the risk associated
with a genetic risk factor. The authors conclude that in clinical practice, family history may be
more useful for risk assessment than thrombophilia testing.
One extremely important and valuable case-cohort study was done to determine the famil-
ial risk of VTE in first, second, and third-degree relatives of affected individuals. 77 This was the
Swedish Multi-Generation Register which was linked to Hospital Discharge Register data for the
period 1987–2009, and involved 183,515 individuals. The authors found an increased VTE risk
among not only first-degree relatives but also second and third degree relatives and non-biologic
relatives. They concluded that the genetic component of the familial clustering of VTE is strong.
We agree with the authors that the family history is potentially useful for clinical VTE risk as-
sessment even in second and 3rd degree relatives.
Ambulation
This risk factor has been difficult to standardize but a practical working definition has been
published a number of years ago when studies not only tracked symptomatic events but also
used venography to identify asymptomatic DVT. The authors defined ambulation as the abil-
ity to independently walk a distance of > 10 m [30 feet]). The authors studied thrombosis pro-
phylaxis in medical patients using two doses of low molecular weight heparin compared to a
placebo group. 78 They compared enoxaparin with placebo for the prevention of venous throm-
boembolism in acutely ill medical patients. 78 Another study published a few years ago sheds
light on this issue. 56 The authors examined the relationship between the use of prophylaxis, VTE
risk, and ambulatory status. They found that despite becoming ambulatory, patients remained at
risk and benefited from the use of low molecular weight heparin prophylaxis 40 mg daily. This
makes sense since ambulation does not affect underlying risk factors but removes only the risks
of bedrest. Furthermore, the mean duration of prophylaxis was 7.6 days. The authors comment
that data are lacking to support the concept of stopping pharmacologic prophylaxis when the
patient is ambulatory or discharged after a short hospitalization. The period of time demon-
strating efficacy for thrombosis prophylaxis in hospitalized patients is at least one week. This
agrees with more than one hundred-sixty studies done over the last 30 years establishing ef-
ficacy as 7–10 days. 3–5 There is considerable data in over 1 million patients to suggest that a
short course of one or two days of prophylactic anticoagulation is ineffective in reducing the
incidence of venous thrombosis. 79–81 These data will be dealt with more completely in another
260 I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298
s
s
C
M
o
s
s
i
o
m
t
t
t
o
a
a
s
t
c
i
c
t
i
t
a
a
i
b
i
ection. The Caprini score defines bedrest as inability to ambulate 30 feet (10 M), and walking a
hort distance to the bathroom or sitting in the chair does not qualify as ambulation using the
aprini score.
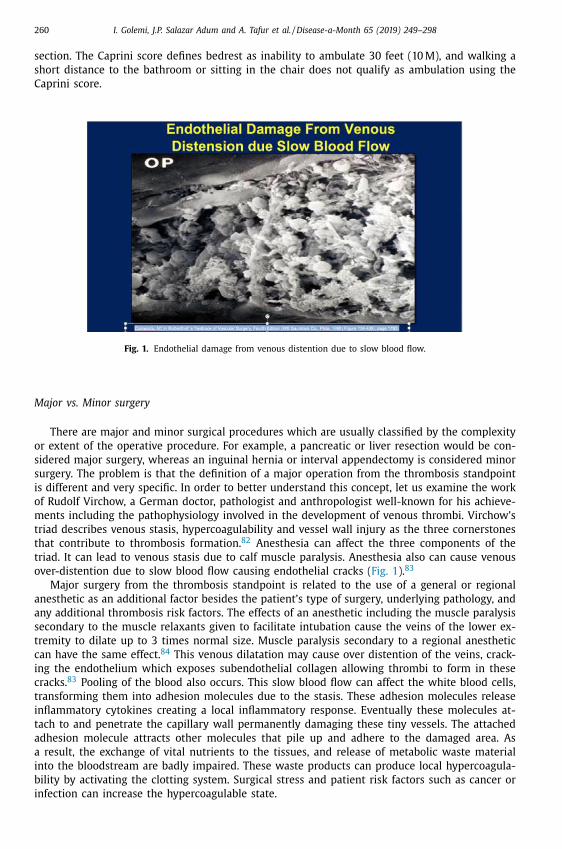
Fig. 1. Endothelial damage from venous distention due to slow blood flow.
ajor vs. Minor surgery
There are major and minor surgical procedures which are usually classified by the complexity
r extent of the operative procedure. For example, a pancreatic or liver resection would be con-
idered major surgery, whereas an inguinal hernia or interval appendectomy is considered minor
urgery. The problem is that the definition of a major operation from the thrombosis standpoint
s different and very specific. In order to better understand this concept, let us examine the work
f Rudolf Virchow, a German doctor, pathologist and anthropologist well-known for his achieve-
ents including the pathophysiology involved in the development of venous thrombi. Virchow’s
riad describes venous stasis, hypercoagulability and vessel wall injury as the three cornerstones
hat contribute to thrombosis formation. 82 Anesthesia can affect the three components of the
riad. It can lead to venous stasis due to calf muscle paralysis. Anesthesia also can cause venous
ver-distention due to slow blood flow causing endothelial cracks ( Fig. 1 ). 83
Major surgery from the thrombosis standpoint is related to the use of a general or regional
nesthetic as an additional factor besides the patient’s type of surgery, underlying pathology, and
ny additional thrombosis risk factors. The effects of an anesthetic including the muscle paralysis
econdary to the muscle relaxants given to facilitate intubation cause the veins of the lower ex-
remity to dilate up to 3 times normal size. Muscle paralysis secondary to a regional anesthetic
an have the same effect. 84 This venous dilatation may cause over distention of the veins, crack-
ng the endothelium which exposes subendothelial collagen allowing thrombi to form in these
racks. 83 Pooling of the blood also occurs. This slow blood flow can affect the white blood cells,
ransforming them into adhesion molecules due to the stasis. These adhesion molecules release
nflammatory cytokines creating a local inflammatory response. Eventually these molecules at-
ach to and penetrate the capillary wall permanently damaging these tiny vessels. The attached
dhesion molecule attracts other molecules that pile up and adhere to the damaged area. As
result, the exchange of vital nutrients to the tissues, and release of metabolic waste material
nto the bloodstream are badly impaired. These waste products can produce local hypercoagula-
ility by activating the clotting system. Surgical stress and patient risk factors such as cancer or
nfection can increase the hypercoagulable state.
I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298 261
This hypercoagulability may be compounded by other risk factors most notably a past his-
tory or family history of thrombosis, the tendency to develop significant or fatal VTE may be
quite likely. If the legs are in stirrups, or straps around the legs are tight, venous stasis may be
increased. Complete extension of the knee may compress the popliteal vein, further promoting
venous stasis; and this process is known as the popliteal entrapment syndrome. 85 This phe-
nomenon narrows or completely closes the popliteal vein which results in diverting the blood
flow through the superficial veins of the leg bypassing the popliteal fossa resulting in slowing
blood flow out of the leg. That is why it is important to put a pillow under the knees during the
operation to prevent complete extension of the knee.
The reverse Trendelenburg (head up) position used for many laparoscopic procedures along
with elevated intra-abdominal pressure due to distension of the abdominal cavity with gas in-
tensifies venous stasis further distending the veins. These mechanisms represent Virchow’s triad
of venous stasis, vascular injury, and hypercoagulability and have been shown many years ago
to represent causative factors for venous thrombosis. Pneumatic compression during the proce-
dure helps to minimize these changes. The longer the procedure, the more these changes can
occur. Tourniquets during surgery can also have these effects. The clinical proof of these con-
cepts starts with the work of Dr. Borow showing how the length of surgery affects the incidence
of VTE. The longer the surgical procedure, the more these factors can intensify and lead to a ve-
nous thrombosis. 7 , 32 The Caprini score assigns 2 points for any anesthetic over 45 minutes and
this is considered major surgery from the thrombosis viewpoint despite the fact that the surgical
procedure is considered minor. Some authors add an extra point for surgery longer than 2 hours,
and the Boston Studies (Cassidy et al) score 5 points if the operation lasts 6 hours. 86 A surgi-
cal procedure might be considered minor, but can pose major thrombotic risks if the anesthetic
lasts more than one hour. 74
Length of surgery
Operations that lasted from 1–2 hours were associated with a 20% DVT incidence in the con-
trol group. The incidence rose to 46.7% for operations lasting between 2–3 hours, and the in-
cidence rose to 62.5% for operations over 3 hours. One must remember that at that time in
the early 1980’s fibrinogen scanning with venographic confirmation was the best method for
determining the total incidence of DVT in a patient population. This included a large number
of asymptomatic events. Furthermore, thrombosis prophylaxis was not the standard of care, so
most patients were not receiving prophylaxis. Studies during this era looking at venographically
documented thrombosis in patients not receiving prophylaxis were of immense value in justify-
ing the administration of anticoagulants to surgical patients. The incidence of bleeding problems
was minuscule compared to the results achieved reducing the incidence of postoperative throm-
bosis. Borow’s landmark study involved studying five methods of prophylaxis for the preven-
tion of postoperative venous thrombosis. The groups were (1) control, (2) low-molecular weight
dextran, (3) mini-dose heparin, (4) bilateral pneumatic compression devices, (5) and elastic com-
pressive stockings. DVT was evaluated using fibrinogen scanning confirmed by venography. Over-
all, 36% of patients, in the control group suffered a DVT. All of the treatment groups lowered the
incidence of DVT including aspirin.
Laparoscopic surgery
A great number of procedures are done with a more minimal approach including
laparoscopically-assisted surgical procedures and arthroscopic surgery. Despite the advantages
including earlier ambulation, decreased pain and discomfort, these procedures still represent a
risk of thrombosis due to the anesthetic and length of surgery. Nguyen and his group from the
Department of surgery, University of California Irvine published a very interesting study compar-
ing the VTE incidence between open and laparoscopic approach for four common surgical pro-

262 I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298
c
d
i
i
l
s
h
n
h
d
c
p
t
C
q
p
i
t
t
t
i
c
i
l
r
p
m
q
t
V
d
s
C
c
h
b
a
o
P
t
r
a
o
t
t
p
p
edures. These included appendectomy, cholecystectomy, anti-reflux surgery, and gastric bypass
uring the period of time between 2002 and 2006. He studied a total of 138,595 patients hav-
ng one of these surgical procedures. Overall the thrombosis incidence was significantly higher
n the open cases compared with the laparoscopic cases (P < 0.01). The incidence of VTE after
aparoscopic surgery continues to be lower than that of open surgery even when the data are
tratified according to the level of severity of illness. This study corrected an earlier opinion we
ad regarding adding 2 points to the score if the procedure was done laparoscopically, and we
o longer add extra points for this minimally invasive approach. We do not reduce the score
owever since the score also reflects time of anesthesia. The approach is only one factor that
etermines thrombotic risk and careful overall risk assessment needs to be done to properly
haracterize risk.
We feel that this was an excellent study although these types of investigations where all the
atients are grouped together without very careful individual risk assessment may not reflect
he true nature of individual thrombotic risk.
linical vignette
A 75-year-old obese male having a laparoscopic cholecystectomy for acute cholecystitis re-
uiring a two-hour anesthetic, may not reflect the thrombotic risk of the average younger, la-
aroscopic cholecystectomy patient in this series. If this patient had a past history or fam-
ly history of VTE, that would increase the risk even further (Caprini score = 9). Therefore, al-
hough this series showed a lower overall risk of VTE for the average laparoscopic cholecys-
ectomy patient compared to the equivalent open cholecystectomy patient, that may not hold
rue when individual risk assessment is employed since a much higher level of risk may ex-
st in individual patients such as this example. The concept of evaluating thrombotic risk ac-
ording to type of procedure may be important but only when taken in the context of the
ndividual risk factors of a given patient. We have seen many examples where the overall
ow incidence of thrombosis for an individual procedure changes drastically when individual
isk assessment is applied. This patient would benefit from 30 days of LMWH prophylaxis
ostoperatively.
Reza Fazl Alizadeh and his colleagues, again from the University of California Irvine Depart-
ent of Surgery continue to do pioneering research in this area and have published a subse-
uent study involving 750,159 patients from the period of 2005 to 2014. They used the Na-
ional Surgical Quality Improvement Program database and looked at the overall incidence of
TE within 30 days of operation. Overall incidence of VTE was 0.32% in patients with benign
isease who underwent laparoscopic abdominal operations including colorectal surgery, bariatric
urgery, cholecystectomy, esophageal surgery, abdominal wall hernia repair, and appendectomy.
olorectal surgery had the highest incidence of VTE (1.12%) and was associated with signifi-
antly the longest length of stay and operative times. Those patients who develop thrombosis
ad a higher mortality and worse outcomes compared to those who did not suffer a throm-
otic event. They concluded that laparoscopic colorectal procedures for benign disease represent
higher risk for the development of thrombosis compared with other laparoscopic abdominal
perations. This study had some limitations since the National Surgical Quality Improvement
rogram database does not include details about past history of thrombosis, family history of
hrombosis, type of prophylaxis postoperatively, dose of any anticoagulants used, and does not
ecord the length of any of these prophylactic treatments. We know that all of these variables
ffect the VTE incidence for an individual.
Another individual patient factor is conversion from the laparoscopic approach to an open
peration. This factor needs to be considered when assessing the patient risk. Excessive opera-
ive time that may be associated with certain laparoscopic robotic procedures also may increase
he level of risk. The Boston group has assigned a higher score to patients who have operative
rocedures lasting 5 hours or more. Their impressive results using the score tied to a mandatory
rophylaxis protocol will be discussed later in this chapter.
I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298 263
Previous major surgery
Landmark studies of Borow, 18% of patients developing a postoperative thrombosis had a
past history of a major surgical procedure at some previous time. When the Caprini score was
designed, we considered those procedures done within one month to be a minor risk factor (1).
Cancer
Cancer is a major risk factor leading to the development of VTE and approximately 20% of pa-
tients with cancer will develop this complication. The score does not stratify between different
types of cancer thus there is expected variation in rate as some cancers have higher associated
risk for developing VTE. 87 VTE is also recognized as one of the leading causes of death in cancer
patients. Rates of thrombosis vary widely depending upon the type of cancer, with the high-
est rates observed in brain, pancreatic, gastric cancer, and a variety of hematologic malignan-
cies. Patients with cancer have an increased level of thrombotic risk especially when additional
risk factors are present. 88 The Khorana and Vienna scores are two additional scores that try to
predict risk of VTE in cancer patients, but neither of them is validated for perioperative risk.
Khorana score aims to identify ambulatory patients with cancer at increased risk of VTE by us-
ing two clinical variables (tumor site and body mass index) and three laboratory measurements
(platelet, hemoglobin and leukocytes). Vienna score is a modification of the Khorana score (ad-
dition of biomarkers D-dimer and soluble P-selectin). 89
Chemotherapy
The prothrombotic state associated with malignant tumors has been shown to be further
increased by chemotherapy. This is a complex issue since frequently central lines are necessary
for the continued administration of these drugs which also increases the thrombotic risk. Many
times, chemotherapy is used for patients with metastasis which in itself is also a risk factor for
thrombosis. The type of chemotherapy also influences the risk of incidental VTE which appears
more frequent in patients receiving platin-based drugs. However, with the multiple changes in
the agents it is hard to individualize the expected risk with each agent. 90
Thrombophilia
Thrombophilia is a congenital or acquired condition that is characterized by an imbalance in
the hemostasis producing a hypercoagulable state. It is often diagnosed by a first episode of VTE
associated with increased risk of recurrence. It is recognized in about 50% of subjects who had
experienced a VTE.
Hereditary thrombophilia
The most common entities of hereditary thrombophilia include antithrombin deficiency, pro-
tein C deficiency, protein S deficiency, resistance to activated protein C due to the mutation of
Factor V Leiden, and G20210A mutation in the prothrombin gene (FII G20210A). These defects
increase the chance of a VTE. Hereditary causes of VTE should be suspected in recurrent or
life-threatening thromboembolism, young age ( < 45 years old), multiple abortions or stillbirths,
family history of VTE, or where there are no obvious acquired risk factors. 91 In a prospective
cohort study of 202 patients with colorectal cancer were stratified in those with thrombotic
mutations (PTM + ) and without thrombotic mutations (PTM-). These patients were screened for

264 I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298
f
t
l
m
i
c
r
i
d
8
G
t
q
(
7
F
A
a
p
p
e
b
β
r
P
l
actor V Leiden and prothrombin G20210A mutations which are the 2 most common defects in
he western population. Coagulation markers including platelet counts, fibrinogen and D-dimer
evels were measured and symptomatic VTE was observed. In the post-prophylactic period 2–12
onths after surgery symptomatic VTE was observed. In the prophylactic period VTE incidence
n PTM + and PTM - was 0% and 1.6% respectively (p = 0.73). Levels of coagulation markers were
omparable in both patient cohort within 28 days postoperatively. In the post-prophylactic pe-
iod, VTE incidence in PTM + and PTM – was 15% and 5.5% respectively. There was significantly
ncreased incidence of lower extremity DVT in patients with factor V Leiden (17.6%). 92
Antithrombin deficiency was initially described by Egeberg in 1965. 93 Protein C and S
eficiency were found to be a cause of hereditary thrombophilia as reported in the early
0s. 94 , 95 Factor V Leiden mutation related to activated protein C resistance and the mutation
20210A on the prothrombin gene were identified as causes of hereditary thrombophilias in
he early 90’s. 96 These are the 2 most common defects. Unprovoked VTE occurs more fre-
uently in patients with hereditary thrombophilia than patients without thrombophilia HR 22.3
P = 0.003) and the presence of hereditary thrombophilia increases the risk of VTE approximately
-fold. 97
Other causes of thrombophilia are elevated concentration of coagulation factors (FVIII, FIX,
XI), deficiency of FXII or hyperhomocysteinemia.
cquired thrombophilia
The most common causes of acquired thrombophilia are antiphospholipid syndrome (APS),
cquired deficiency of natural inhibitors of coagulation, myeloproliferative syndromes and the
resence of the mutation JAK2V617F, and nocturnal paroxysmal hemoglobinuria.
APS is a condition that increases the risk of vascular occlusion and is frequently seen in
atients with pregnancy complications. It is an autoimmune disorder characterized by the pres-
nce of antibodies directed against proteins and phospholipids such as antiphospholipid anti-
odies (aPL) or anticardiolipid antibodies (aCL) or antibodies against the β2 glycoprotein I (anti-
2GPI) of IgG or IgM class.
The acquired deficiency of natural coagulation inhibitors (AT, PC or PS) are also independent
isk factors for VTE ( Table 1 ).
aroxysmal Nocturnal Hemoglobinuria (PNH)
Paroxysmal nocturnal hemoglobinuria (PNH) is a rare, potentially life-threatening hemato-
ogic disorder characterized by chronic intravascular hemolysis caused by uncontrolled activa-
Table 1
Thrombophilia testing recommendations.
Recommendations Explanation
Do not test with concomitant VTE event Test at completion of anticoagulant therapy for provoked VTE Test after
treatment for acute event for unprovoked VTE, if cessation of
anticoagulant therapy is considered and test results might change
management.
Do not test when receiving anticoagulation
therapy
Test when warfarin has been stopped for a minimum of 2 weeks,
DOAC has been stopped for 2 days or longer and UFH or LMWH for
antithrombin levels has been stopped for more than 24 hours
Do not test if VTE is provoked by strong
risk factors
Risk factors are trauma, surgery, immobility, severe illness
Consider testing VTE episodes at a young age in association with no clear provoking
factors Strong family history of VTE
Recurrent VTE
Modified from: Connors et al. 98

I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298 265
tion of the terminal complement pathway. Complement systems and coagulation systems are
closely integrated with each influencing the activity of the other. 99 Clinical manifestations may
include involvement of unusual sites of thrombosis especially (hepatic (Budd-Chiari being one of
the most common sites), mesenteric, cerebral (superior sagittal sinus thrombosis, dermal veins).
Thrombophilia is a major cause of morbidity and mortality in PNH. When thrombosis occurs, in-
definite anticoagulation is recommended. This disease is also associated with breakthrough and
recurrent thrombosis. The physician should have a high index of suspicion in cases of throm-
bosis at unusual sites, breakthrough thrombosis on adequate therapy, and excessive abdominal
pain associated with well-treated visceral thrombosis such as portal vein or mesenteric throm-
bosis.
Eculizumab is a new available drug that controls intravascular hemolysis in PNH and inhibits
the complement system. This drug needs to be given life-long. 99 It enables patients who may
die in their 30’s to have a normal life span. In a study including 195 patients that were followed
for 66 months 3-year survival was estimated to be 97.6% with patients showing reduction in
lactate dehydrogenase levels reflecting inhibition of chronic hemolysis. Thromboembolic events
decreased by 818%, with 96.4% of patients remaining thromboembolic event free. Transfusion
independence increased by 90.0% from baseline, with the number of red blood cell units trans-
fused decreasing by 54.7%. 100 Eculizumab was well tolerated, with no evidence of cumulative
toxicity and a decreasing occurrence of adverse events over time. 100
History of superficial venous thrombosis
The incidence of superficial venous thrombosis (SVT) varies in different populations from 3%
to 11%. 101–103
The prevalence during the third decade of life is 0.05/10 0 0 per year and 0.31/10 0 0 per
year in men and women respectively. It increases during the eighth decade of life to 1.8/10 0 0
per year and 2.2/10 0 0 in men and women respectively. SVT is more common in women (50–
70%). 101 , 104 , 105
The development of SVT in patients who concomitantly have varicose veins ranges from 4–
59%, 101 , 105–107 whereas SVT in patients without varicose veins is found in approximately 5–10%
of all cases. 105 , 108 , 109 SVT is a risk factor for the development and recurrence of DVT and it
may even coexist with DVT in 6–53% of patients and the most common presentation is exten-
sion from the great saphenous vein into the femoral vein. 75 , 103 , 105 , 106 , 110–121 SVT above knee is
associated with 17–19% incidence of DVT versus SVT located below the knee segment has an
incidence of DVT in 4–5% of patients. 112 , 122 , 123 SVT is a risk factor for DVT and recurrent PE. PE
has been seen in a wide range from 1.5 to 33% of patients with SVT. It has been reported in
18% of patients when the SVT was involved in the great saphenous vein above the knee and 4%
when in the small saphenous vein. 103 , 105 , 108 , 117 , 124
The diagnosis of SVT should include a complete duplex scan with full evaluation of the entire
deep venous system of the leg.
Varicose veins
Varicose veins are an entity within the spectrum of chronic venous disease (CVD); the pre-
sentation may vary from spider telangiectasias to reticular veins, and true varicosities. It affects
approximately 23% of adults in the US and it is more commonly seen in women and older adults.
Varicose veins affect approximately 22 million women and 11 million men between the ages of
40 to 80 years. 125 The prevalence increases to 80% in men and 85% in women if all forms of
varicose veins are included (spider telangiectasias, reticular veins and true varicosities). 126
Risk factors for varicose veins include estrogen exposure (female), lifestyle (prolonged sitting
or standing, smoking), acquired (obesity, pregnancy, DVT, age) and inherited (family history, tall
height, congenital syndromes that affect venous pressure, valvular incompetence and venous ob-

266 I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298
s
t
t
i
i
a
r
v
p
i
p
R
a
T
p
i
p
I
r
o
e
r
t
N
V
i
v
p
[
C
a
v
e
p
f
D
e
p
p
m
m
s
c
truction). The major mechanisms resulting in varicose veins include venous valvular incompe-
ence, venous hypertension, inflammation, structural changes in the vein wall and shear stress.
Varicose veins may advance in severity and extent if causative factors are not corrected and
reatment is not initiated. Advanced forms of chronic venous insufficiency may develop includ-
ng lower extremity edema and venous ulceration. Varicose veins were associated with a 7-fold
ncreased risk of DVT in a large observational cohort study. 127
Management options include lifestyle modifications, compression therapy, local/endovascular
blative therapies and surgical interventions. The majority of patients with varicose veins will
equire a multisystemic approach.
A retrospective evaluation of prospectively collected data undergoing procedures for varicose
eins from March 2008 until June 2014 was completed. Patient clinical severity scores pre- and
ost-procedure, treatment choice and perioperative complications were collected. Venous clin-
cal severity scores improved more with radiofrequency ablation + trans illuminated powered
hlebotomy as compared to radiofrequency ablation alone. (3.8 ± 3.4 vs. 3.2 ± 3.1, p = 0.018).
egarding deep venous thrombosis, there was no significant difference between radiofrequency
blation + trans illuminated powered phlebotomy in patients vs. radiofrequency ablation alone.
his study demonstrated that ablation of axial reflux plus trans illuminated powered phlebotomy
roduces improved outcomes as measured by venous clinical severity score, with slight increases
n minor post-operative complications and should be strongly considered as initial therapy when
atients present with significant symptomatic varicose veins and superficial venous insufficiency.
mplementation of a standardized thromboprophylaxis protocol with individual risk assessment
esults in few significant thrombotic complications among high-risk patients, thus potentially
bviating the need for routine post-operative duplex. 128
Königsbrügge et al demonstrated that the presence of varicose veins is associated with an
levated risk of VTE in cancer patients. In a prospective cohort study 1270 cancer patients were
ecruited and followed for 590 days. Sixty-six patients (5.2%) had a history of VTE, superficial
hrombophlebitis was seen in 79 patients (6.2%), and varicose veins seen in 160 patients (12.6%).
inety-eight patients (7.7%) developed VTE during follow-up. The hazard ratios for the risk of
TE in patients with a history of VTE or superficial thrombophlebitis were 1.44 (95% confidence
nterval: 0.67–3.07) and 1.94 (1.04–3.61), respectively, and 2.01 (1.26–3.21) in those with varicose
eins. In multivariate analysis including history of VTE, history of superficial thrombophlebitis,
resence of varicose veins, and other patient-related factors, the presence of varicose veins (2.10
1.29–3.41]) remained significantly associated with an increased risk of VTE. 129
hronic Venous Disease (CVD)
CVD is a very common problem affecting more than 25 million adults in the United States
nd more than 6 million with more advanced venous disease. 130
The most common manifestations of CVD are telangiectasias, reticular veins, and varicose
eins. Chronic venous insufficiency (CVI) is a condition in which the venous system of the lower
xtremities is affected. It is associated with persistent ambulatory venous hypertension causing
ain, edema, skin changes, and ulcerations. The edema seen in CVI is dependent and pitting. The
orefoot is often spared to help distinguish it from other causes of edema such as lymphedema.
ue to the obstruction of lymphatic drainage, lymphedema leads to accumulation of fluid that
xtends into the foot and toes.
Lipedema is characterized by accumulation of fatty tissues instead of fluid, therefore it is not
itting and often spares involvement of the feet, usually with a cuff of tissue at the ankle.
Post thrombotic syndrome (PTS) is characterized by lower extremity pain upon standing, de-
endent edema, and development of tender induration of the subcutaneous tissues (lipoder-
atosclerosis). The clinical picture of PTS is nonspecific, as clinical conditions other than DVT
ay result in a similar constellation of signs and symptoms of the lower extremity, including
uperficial venous insufficiency, trauma and obesity. Pruritus and eczematous skin changes are
ommonly seen. Ulceration of the affected area arises in a considerable number of patients. In
I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298 267
some patients these changes may result in permanent disability. PTS is often triggered by mi-
nor trauma, and is mostly chronic and indolent with a high recurrence rate. Rarely, patients
with persistent obstruction may experience venous claudication, which mimics arterial claudi-
cation. 131
It is known that venous hypertension may be a precursor of PTS. Patients with extensive
thrombosis including major involvement of the iliofemoral segment, frequently have venous hy-
pertension. Venous hypertension can be modified by appropriate compression garments includ-
ing stockings and Velcro devices. 132 Appropriate compression modalities including GEC stockings
are a necessity to control pain and edema, frequently on a permanent basis. 133
Leg swelling and Lymphedema
Swelling of distal leg characterized by loss of definition of the normal bony prominences
about the ankle. This can be seen with PTS, venous insufficiency, or lymphedema.
Chronic venous insufficiency which does not involve the foot so the veins of the foot are
visible. Lymphedema presents with a hump over the dorsum of the foot which obliterates the
venous pattern, along with a positive Stemmer’s sign (inability to pinch the tissue at the base
of the toes). When considering this risk factor, we score one point for either one or both legs
affected with swelling from any cause.
Stroke
Stroke remains the third leading cause of death in the United States. 134 DVT commonly de-
velops in patients admitted to hospital with acute stroke, and may then lead to PE. 135 It is as-
sociated with increased mortality and long-term morbidity. 136
The estimated rate of DVT in hospitalized patients who have a stroke is 20% −50% and two
thirds of these are calf DVTs. 62 , 137 The risk of fatal PE is estimated to be 4.9-fold higher in
immobilized patients with a neurological disease. 138 In a 19-year study period that analyzed
deaths from the United States Bureau of the Census Compressed Mortality File, demonstrated
that the corrected rate of fatal PE among patients with ischemic stroke ranges from 1.5% to
2.1%. 139 Recurrent venous thromboembolism (VTE) is also more common in patients with limb
paresis following stroke. 140 The risk is even higher in patients with brain tumors presenting as
stroke. 141
Inflammatory bowel disease
Data suggest that most patients with inflammatory bowel disease (IBD) have active disease
at the time of the diagnosis of VTE. 142 , 143
It has been shown that patients with active IBD have a three-fold increase in risk of VTE and
that has led to the use of thromboprophylaxis as the standard of care for patients in the hospi-
tal. 144 Approximately 50% of VTE episodes developing concomitantly with IBD occur in patients
who have been hospitalized within the past 3 months. 145
In a cohort study from the General Practice Research Database, 13,756 patients with inflam-
matory bowel disease and 71,672 matched controls were included in the analysis. Patients with
IBD had a higher risk of VTE versus control group (HR 3 • 4, 95% CI 2 • 7–4 • 3; p < 0 • 0 0 01; AR 2 • 6per 10 0 0 person-years). It was seen that at the time of a flare, this increase in risk was much
higher (8 • 4, 5 • 5–12 • 8; p < 0 • 0 0 01; 9 • 0 per 10 0 0 person-years). Interestingly, the relative risk at
the time of a flare was higher in non-hospitalized patients (15 • 8, 9 • 8–25 • 5; p < 0 • 0 0 01; 6 • 4 per
10 0 0 person-years) compared to hospitalized patients (3 • 2, 1 • 7–6 • 3; p = 0 • 0 0 06; 37 • 5 per 10 0 0
person-years). 146

268 I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298
Fig. 2. Surgical specimen of colon in IBD.
f
S
t
w
o
p
a
p
t
w
s
s
A
o
r
h
M
Figure 2 is an illustration of advanced inflammatory bowel disease in a surgical specimen
rom a diseased colon.
epsis- Infection requiring IV antibiotics
The association between acute infection and VTE is of paramount clinical importance due
o the high rates of both entities. Acute infection it is associated with systemic inflammation
hich may increase the risk of VTE causing at least one or even more of the three components
f Virchow triad: venous stasis, hypercoagulability and vessel wall injury. 146–148
In a population-based case–control study conducted in Denmark, of approximately 15,0 0 0
atients diagnosed with a first VTE episode in the hospital during the period 1999–2009 among
ll cases of hospital-diagnosed infections and community prescriptions for antibiotics 1 year
receding the VTE were evaluated. Schmidt, et al, found that, skin, intra-abdominal, respira-
ory tract, urinary tract and bacteremic infections diagnosed in hospital or treated as outpatient
ere associated with twofold increased VTE risk. The authors observed that this association was
trongest within the first 2 weeks after the onset of the infection, and gradually lessening sub-
equently. 149
cute Myocardial Infarction
Acute myocardial infarction is associated with a transient increased VTE risk independently
f traditional atherosclerotic risk factors. The estimate was particularly high for PE. Rinde et al
ecruited 29,506 participants with a median follow up of 15.7 years. This Study concluded that
ighest risk of PE was observed in the first 6 months after the MI (HR 8.49; 95% CI 4.00–18.77).
I explained 6.2% of the PEs in the population (population attributable risk) and 78.5% of the
I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298 269
PE risk in MI patients (attributable risk). 150 In an older study 89 patients were followed after an
acute MI and 27% of patients developed VTE. These patients were more likely to be over 60 years
old and had a previous history of angina and developed congestive heart failure with significant
dysrhythmias. 151 In a large population-based case controlled Danish study, inpatient diagnosis of
heart disease was associated with a markedly increased risk factor for venous thromboembolism.
The relative risk was particularly high for isolated pulmonary embolism without a concurrent
diagnosis of primary deep venous thrombosis. There was an increased risk with myocardial in-
farction especially if MI occurred less than three months after VTE. The risk extended beyond 3
months past the initial hospitalization for heart disease; however, the association got weaker. 152
In 41,259 patients with VTE from the RIETE registry 22,633(55.6%) experienced a provoked VTE.
Those with provoked events were more likely to have diabetes (OR 1.04; 95%; CI: 1.02 - 1.07),
history of coronary artery disease (OR: 1.03; CI: 0.9–1.2), or prior stroke (OR 1.09; CI:1.06–1.1).
During follow-up, patients with provoked VTE were 32% more likely to develop major adverse
cardiac events (MACE) and major adverse limb events (MALE) than patients with non-provoked
VTE (hazard ratio [HR]: 1.32; 95% CI: 1.1–1.5). The association was strong with recent immobility
(HR: 1.37; 95% CI: 1.5–12.1), and cancer (HR: 1.7; 95% CI: 1.4–1.9), but not for other risk factors
for VTE. After adjusting for multiple conventional cardiovascular risk factors, provoked VTE was
independently associated with an increased risk for MACE (HR Adj: 1.39; 95% CI: 1.1–1.7). Cancer
remained an adjusted predictor for both MACE (HR Adj: 1.7, 95% CI: 1.4–2.1) and MALE (HR Adj:
2.1; 95% CI: 1.01–4.6) outcomes. 153
Serious lung disease
Several lung conditions have been associated with VTE. Chronic obstructive pulmonary dis-
ease (COPD) is a leading cause of mortality and morbidity worldwide that is characterized by
systemic inflammation. COPD patients are at increased risk of VTE because of immobilization,
heightened systemic inflammation, cigarette smoking and venous stasis. The overall reported
prevalence of VTE during COPD exacerbation ranges from 5% to 29%. 154 VTE remains underdiag-
nosed in this population because it can present similarly to COPD exacerbation. Post mortem
studies of COPD patients have found pulmonary embolism (PE) in 28% −51% of cases. 155 , 156 Fur-
thermore, increased COPD severity is associated with VTE severity when measured in terms
of lung function impairment [OR] moderate: mild = 1.16; 95% confidence intervals [CIs] = 1.03, 1.32)
or medication usage (OR severe: mild/ moderate = 1.17; 95% CIs = 1.06, 1.26). However, there is no evi-
dence that frequent exacerbation is associated with greater risk of VTE OR = 1.06; 95% CIs = 0.97,
1.15). 157
Idiopathic Pulmonary fibrosis (IPH) poses a higher risk for VTE. Sprunger et al used data
from National Center for Health Statistics from 1988–2007 and identified 218,991 patients with
pulmonary fibrosis. Risk of VTE in pulmonary fibrosis was 34% higher than in the background
population and 44% and 54% greater for patients with COPD and lung cancer respectively. Pa-
tients with VTE died at a younger age than patients with IPH alone (females: 74.3 versus 77.4
years (p < 0.0 0 01); males: 72.0 versus 74.4 years (p < 0.0 0 01). 158
Pneumonia is also associated with an increase in VTE. 159 Pneumococcal infection specifically
has been associated with host coagulation/anticoagulation stimulated by components of the bac-
terial cell wall. 160 The cell wall also stimulates an inflammatory response including recruitment
of leukocytes, cytokine production such as TNFa, IL-1 and IL-05 reducing barrier function and
exposing extracellular matrix. 161 , 162 This leads to exposure of subendothelial tissue factor which
in combination with circulating factor VII induces coagulation. 159 Platelet activating factor (PAF)
has also been implicated in pneumococcus-associated VTE. 163 In a large multicenter database
of surgical patients it was shown that preoperative pneumonia may increase risk of developing
venous thrombosis DVT, OR:8.20 (95% CI 6.75–9.96) and PE, OR: 5.07 (95% CI 3.63–7.07). 164
A prospective population-based ARIC cohort concluded that obstructive spirometry patterns
(COPD pattern, low FEV1 and low FEV1/FVC) are associated with elevated risk of VTE (HR 1.35,

270 I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298
9
s
1
C
b
t
H
f
s
a
r
S
s
t
D
I
m
r
o
9
C
i
(
f
p
C
h
b
s
i
H
p
o
a
5% CI 1.08–1.68). Patients with respiratory symptoms and normal spirometric results also had
ignificantly increased risk of VTE (HR 1.40, 95% CI 1.12–1.73).
Restrictive lung disease pattern was not significantly related with increased risk of VTE (HR
.52, 95% CI 0.93–2.49). 165
ongestive heart failure
Patients with reduced cardiac function are thought to have a higher risk of venous throm-
oembolism (VTE). Thromboembolic events in hospitalized patients with heart failure (HF) seem
o be under-recognized and can contribute to increased mortality and morbidity. 166 More severe
F as defined by high NT-proBNP was associated with increased risk of VTE. 167 Congestive heart
ailure has been described as a significant risk factor for VTE in bariatric surgery. 168 In a retro-
pective analysis of the National Inpatient Sample database from 2005–2014 patients with VTE
nd heart failure had higher length of hospitalization. There was also an upward trend of VTE
elated hospitalization among patients with HF. 169
leep apnea
Sleep apnea can also be associated with VTE. In a systematic review of 15 studies obstructive
leep apnea was found to be an independent factor of VTE with risk of DVT or PE being two-
hree-fold higher in patients with obstructive sleep apnea than those without. 170
iabetes
VTE incidence appears to be 2 times higher among diabetic patients < 65YO vs no diabetes. 171
n a population-based study patients with diabetes who develop venous thromboembolism are
ore likely to suffer a complicated course and diabetes was an independent predictor for recur-
ent vein thrombosis. 172 A Taiwanese study with 56,158 patients concluded that the incidence
f VTE was higher in Type 2 diabetes mellitus (T2DM) patients than in controls [adj HR: 1.44
5% CI 1.27–1.63). The risks of DVT (aHR = 1.43, 95% CI = 1.23–1.65) and PE (adjHR = 1.52, 95%
I = 1.22–1.90. 173 In one study that included 358 patients undergoing total knee arthroplasty the
ncidence of DVT 14 days after TKA was significantly higher with than without diabetes OR: 2.71
95% CI 1.183–6.212, p = 0.018). 174
Metabolic syndrome is associated with increased plasma levels of fibrinogen, factor VII and
actor VIII potentially leading to a hypercoagulable state. 175 In a case control study a total of 200
atients, metabolic syndrome was independently associated with idiopathic DVT (OR 1.94; 95%
I 1.04, 3.63). 176 Prevalence of metabolic syndrome in recurrent venous thromboembolism was
igher than in controls in a study of 116 patients with confirmed recurrent venous thromboem-
olism [OR:2.1 (95% CI 1.2, 3.7)]. 177 In another case control study in Korean population metabolic
yndrome was associated with VTE (OR: 1.56; 95% CI: 1.07 to 2.27, P = 0.020) and especially with
diopathic VTE (OR: 1.71; 95% CI: 1.04 to 2.81, P = 0.033). 178
ypertension
Hypertension can also be a risk factor for DVT. In a metanalysis of 16 articles regarding hy-
ertension, including 68,955 males and 53,057 females, this factor was associated with DVT after
rthopedic surgery (OR 2.89, 95% CI 2.18–3.83, Z = 7.38, P < 0.05). Hypertension was also associ-
ted with an increase of VTE patients in newly diagnosed lung cancer OR 1.8; 95% CI 1.0–3.3). 179
I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298 271
Central Venous Access
Catheter-related thrombosis is a common complication of all anatomical sites and especially
smaller veins. Presence of catheter within the lumen of a vein decreases flow and can created
stasis leading to thrombosis. Nifong et al used fluid mechanics to calculate relative flow rates as a
function of the ratio of the catheter to vein diameters. They determined that there is a decrease
in fluid flow rate with catheter size ( < 0.001). PICCs in particular may contribute to substantial
decrease in venous flow as much as 93%. 180
Several studies have indicated that catheters are associated with increased risk of thrombo-
sis. The MITH study included 299 patients with catheter-related thrombosis. Upper extremity
DVT constituted 51% of all deep vein thrombosis. The use of central venous catheters (CVC)
was associated with a 14.0-fold increased risk of upper extremity DVT (95% CI, 5.9–33.2). 181
Post mortem examination of catheterized veins vs controls in 72 autopsied patients showed that
in the catheters sheath fibril and staph can adhere to fibrin producing enzymes that promote
thrombogenesis. 182 In an 18-month long study, 208 central venous catheters including jugular
and subclavian were analyzed with duplex sonography less than 24 hours after catheter removal.
Mean duration of catheterization was 9 days. In these patients, catheter-related thrombosis was
33% with 42% localized in the internal jugular vein and 10% in subclavian veins. 183 In patients
with catheter associated staph aureus bacteremia, 48 patients had venous duplex US and out-
comes were assessed at 12 weeks. Thrombosis by US was present in 71% of patients. 184 In a
prospective study of 105 patients undergoing chemotherapy having ≥ 2 positive cultures was as-
sociated with thrombosis (71% vs 3% in patients with negative or single positive culture). 185 In a
case study CVC related thrombosis was associated with paradoxical embolism through a patent
foramen ovale. 186 Thrombosis of a CVC can also lead to a superior venacava syndrome. 187
Peripheral Inserted Central Catheters (PICC) lines can cause trauma to the vein wall and pre-
dispose patients to upper extremity venous thrombosis. 188 PICC lines complications versus cen-
tral venous catheters were analyzed in surgical patients. PICC lines did not differ from infectious
complications with central venous catheters and thrombotic complications appeared more sig-
nificant in PICC lines, also appearing earlier after catheterization. 189
Hip, Leg, or pelvic fracture
The incidence of DVT is higher in patients with proximal extremity fractures than distal ex-
tremity fractures. In one study 102 patients underwent lower extremity venography 9 days af-
ter operative fixation and followed for 6 weeks. The overall incidence of clinically occult DVT
was 28% with 40% in the femoral shaft, 43% in the tibial plateau, 22% in the tibial shaft and
12.5% in the tibial plateau. 190 Multiple injured patients with pelvic fracture are at an increased
risk of venous thrombosis. The incidence of pulmonary emboli in these patients has been re-
ported to be from 0.5 to 8.3%. In a prospective study 198 patients with pelvic trauma were
followed for 3 years. The incidence of pulmonary embolism was related to the Injury Severity
Score ISS (ISS < 15 = 0% vs ISS > 15 = 4%, P < 0.05). 191 In a Canadian study of 349 patients with
major trauma, DVT occurred in 58% of the single cohort with major trauma who did not re-
ceive prophylaxis. Patients with highest risk were those with injures of the lower extremities
and spinal cord that were followed over 2 years. DVT was associated with spinal cord injury,
fracture of the femur or tibia. 192 Britt et al. reviewed the incidence of lower extremity DVT in
1093 patients with pelvic and lower extremity fractures. They found an incidence of 13% DVT
and patients with DVT (1.3% PE),15% in patients with both pelvic and lower extremity fractures
(0.99% PE), and 9% in patients with lower extremity fractures only (0.63% PE). 193
Lower extremity DVT can occur in patients with lower extremity trauma not undergoing
surgery. The lower extremity DVT in patients with brace or immobilization can be from 0–
17%. 194 , 195 Use of prophylaxis in these patients significantly reduces the incidence of VTE but
there is wide variation between physicians using anticoagulants. 195 , 196

272 I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298
o
r
u
t
w
p
M
u
r
h
h
b
a
T
t
i
d
m
7
K
a
i
l
p
f
s
h
e
n
p
c
D
c
I
a
A
s
o
o
a
t
t
c
Patients treated with surgery following lower extremity trauma have a reported risk of 2.1%
f DVT despite being anticoagulated with LMWH in the first 24 hours of admission. 197 , 198 A
etrospective review of 57,0 0 0 ankle traumas revealed a rate of 0.05% due to VTE. 199 In patients
ndergoing surgery for hip or femur fracture DVT presence was 10%. 200
Upper extremity trauma is also related to a higher risk of VTE. Incidence of VTE reported in
hese patients is 1–5%. 197 In a recent study between trauma patients, rate of VTE in patients
ith upper extremity trauma was reported to be 4.95% similar to the rate of VTE of all trauma
atients. 201
ultiple trauma with involvement of different organ systems
Trauma is also a risk factor for VTE. The incidence of VTE after injuries depends on the pop-
lation being described, nature of their injuries and prophylactic measures used. 202 Patients at
isk have an incidence of DVT that ranges from 10–20% and PE 1–2%, but mortality can be as
igh as 20–50%. 202 Geerts et al performed a prospective study in 349 patients and 58% of them
ad clots. 192 The occurrence of VTE during post-traumatic hospitalization is associated with mor-
idity and mortality. In a study from the German Trauma Surgery registry, 7937 were included
nd from them 146 developed clinically relevant VTE events with an overall incidence of 1.8%.
wo-thirds of the VTE events occurred in the first 3 weeks of admission while patients were ei-
her receiving mechanical or chemical prophylaxis. Multivariate analysis identifies injury sever-
ty score, number of operative procedures, pelvic injury and concomitant disease as indepen-
ent risk factors for VTE. Presence of VTE was also associated with higher frequency of sepsis,
ultiple organ failure and prolonged hospital stay. Mortality in the VTE group was 13.7% vs
.4% in the non VTE group (P-0.004). Presence of PE was associated with mortality of 25.7%. 203
nudson et al used the American College of Surgeons national trauma data bank and found that
ge ≥ 40, pelvic fracture, LE fracture, spinal cord injury with paralysis, ventilator days, venous
njury, shock on admission and major surgery were associated with VTE. 202 Ratan et al ana-
yzed 5,151,617 patients in Nationwide Readmission Database from 2010–2014 and 1.2% of these
atients were readmitted within one year with VTE. The yearly cost of one-year readmission
or VTE was $256.9 million accounting for one-third of the cost. 204 The risk assessment profile
core (RAP) identifies trauma patients at risk for DVT. In the prospective study there were 102
igh-risk (64%) and 58 low-risk (36%) individuals studied. Eleven of the high-risk group (10.8%)
xperienced the development of DVT (asymptomatic, 64%). None of the low-risk group was diag-
osed with DVT. Five of the 16 RAP factors were statistically significant for DVT. Eliminating pro-
hylaxis and Doppler scans in low-risk patients resulted in a total savings of $18,908 in hospital
harges. The RAP score correctly identified trauma patients at increased risk for development of
VT, and despite prophylaxis the high-risk group warranted surveillance scans. 205
A recent study using hospital discharge data in a pediatric population from 19 states indi-
ated that DVT occurred at a rate of 0.77 per 10 0 0 discharged among injured patients. 206 , 207
n a pediatric trauma population risk factors included older age, injuries to the head, thorax,
bdomen, lower extremity, spinal cord injury and use of central catheters. 202
cute spinal cord injury (paralysis)
VTE remains a cause of significant mortality in patients with spinal cord injuries. Venous sta-
is is a major concern in these patients as well as DVT. These patients exhibit all 3 components
f Virchow’s triad and the incidence of DVT is reported to be greater than 50% with incidence
f final PE as high as 5%. 208 Prevalence of DVT has been described to range from 14–100%. 209 In
retrospective chart review of 151 patients with spinal cord injury (SCI) 17 (11%) had symp-
omatic VTE (9 PEs, 6 lower extremity DVT, 1 upper extremity DVT, and 1 with DVT and PE). In
he univariable analyses, male sex and having other sites of injuries along with SCI were signifi-
ant risk factors. In stepwise Cox modeling, independent risk factors were other sites of injuries

I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298 273
(hazard ratio [HR] 6.07, 95% confidence interval [CI] 1.89–19.47, p = 0.002), age (HR 1.05 per year,
95% CI 1.02–1.08, p = 0.002) and the presence of leg paresis (HR 2.7, 95% CI 0.72–10.54, p = 0.14),
whereas hypertension appeared to reduce the risk (HR 0.18, 95% CI 0.04–0.78, p = 0.02). 210 In a
metanalysis of 23 studies, there was strong evidence to support use of LMWH for thrombophy-
laxis. 208
VTE remains a common complication following spinal cord injury. Because patients with SCI
might not report the initial symptoms that are associated with VTE oftentimes the initial pre-
sentation includes extensive DVT and PE including sudden death. Furthermore, DVT in patients
with spinal cord injury resolves more slowly and can lead to chronic venous occlusion. Early
thromboprophylaxis is the most effective way to reduce the burden of this complication in the
spinal cord injury patient population. Clinical practice guidelines are in place to guide clinicians
in management of VTE in this patient population. 211
Risk factors affecting female patients
VTE is a specific reproductive health risk for women. There is a synergistic effect between
thrombophilia and various reproductive risk factors. VTE in women occurs during pregnancy,
with the use of reproductive hormones and as a consequence of ovarian stimulation. In preg-
nancy, the risk of VTE is increased ∼5 fold while the use of combined hormonal contra-
ception (CHC) doubles the risk including contraceptive pills containing desogestrel, gestodene
and drospirenone when compared with levonorgestrel. Hormone replacement therapy (HRT)
increases the VTE risk 2–4 fold. In women who are at high risk, CHC and HRT should be
avoided.
Pregnancy increases the risk of VTE 4-5-fold over that in the non-pregnancy state. 212 , 213 VTE
can occur at any trimester in pregnancy but is more common during the first half of preg-
nancy. 214 DVT during pregnancy is more common in the left leg compared to the right. This
might be a consequence of May-Thurner syndrome in which the left iliac vein is compressed by
the right iliac artery. 215 Also 12% of DVT’s are in pelvic veins and VTE remains common in the
post-partum period. 216 In a 30-year-population-based study, Heit et al concluded the risk of VTE
and pulmonary embolism was 5-fold to 15-fold respectively in the postpartum period compared
to during pregnancy. 213
In a large primary care database containing 376,154 pregnancies ending in live birth or still-
birth, pregnancy ending in stillbirth was associated with a 6-fold increase in the rate of VTE
compared with a live-birth outcome. In the postpartum phase still birth was the strongest risk
factor with VTE (AR, 24 4 4/10 0 0 0 0 person-years; IRR, 6.2/10 0, 0 0 0 person-years). 217
Recurrent miscarriages affect 2–5% of women. 218 , 219 The cause of recurrent miscarriage is
only identified in 50% of patients. 220 Thrombophilic disorders nowadays are thought to play a
part in the cause of recurrent miscarriages, particularly the antiphospholipid antibody syndrome
(ACA) syndrome. 221 Women who are thought to have higher risk of thrombophilia prior to preg-
nancy show an increased risk of thrombotic events during pregnancy and/or abortion. 222
Estrogen influences hemostasis by increasing the levels of clotting factors (VII, VIII, X, fibrino-
gen) and plasminogen and lowering antithrombin III and protein S levels and altering activated
protein C (ACP) resistance which decreases factor V activity. 223 In a large case control study
that compared VTE risk associated with levonorgestrel containing pills (2nd generation) and 3rd
generation pills (desogestreol, gestodene) included 1524 cases and 1750 controls. Overall OCPs
were associated with a fivefold increased risk of VTE. The risk was lower with levonorgestrel-
containing pills (odds ratio [OR] 3.6; 95% CI 2.9–4.6) when compared with pills containing des-
ogestrel (OR 7.3; 95% CI 5.3–10), gestodene (OR 5.6; 95% CI 3.7–8.4), drospirenone (OR 6.3; 95%
CI 2.9–13.7), or cyproterone acetate (OR 6.8; 95% CI 4.7–10). The risk for VTE was highest in the
first 3 months of use (OR 12.6; 95% CI 7.1–22.4), but even at 1 year a fivefold increased risk was
detected. Among those who used the pill for at least 2 years, the risk was still elevated with
desogestrel- (OR 1.9; 95% CI 1.3–2.9) and gestodene- (OR 1.5; 95% CI 0.9–2.6) containing pills
when compared with levonorgestrel-containing pills. 224

274 I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298
i
c
i
r
C
r
h
a
r
2
0
d
E
P
R
t
t
c
p
d
t
e
a
t
p
m
t
a
h
r
p
r
C
p
p
s
c
l
s
a
b
T
u
In a systematic review of progesterone only contraception (POCs) did not suggest an increase
n odds of venous or arterial events with use of most POCs. Limited evidence suggested in-
reased odds of VTE with use of injectables and use of POCs for therapeutic indications. 225
Hormonal therapy is also a risk factor for VTE in women. Route of hormonal therapy is also
mportant in risk for VTE. Oral but not transdermal estrogens are associated with a higher risk of
ecurrent VTE in postmenopausal women [HR, 1.0; 95% CI, 0.4–2.4, transdermal and [HR 6.4; 95%
I, 1.5–27.3, oral therapy]. 226 Treatment with tamoxifen has also been associated with increased
isk of VTE. In a Danish population study of 16,289 women found that patients taking tamoxifen
ave a higher risk of VTE. The 5-year risk of DVT/PE was 1.2% for women receiving tamoxifen
nd 0.50% for women not receiving tamoxifen. Women treated with tamoxifen were at a higher
isk for DVT/PE during the first 2 years after exposure (RR, 3.5; 95% confidence interval [95% CI],
.1–6.0). Subsequently, their risk was not found to be substantially increased (RR, 1.5; 95% CI,
.88–2.5). Older women taking tamoxifen appeared to be at higher risk than younger women
uring the first 2 years of exposure. 227
ND OF PART ONE
ART TWO: RISK ASSESSMENT USING THE CAPRINI SCORE
isk assessment models (RAM’s)
A variety of RAM’s have been proposed ranging from those looking at a few major factors
o very detailed models designed to capture all of the important factors that could lead to a
hrombotic event. Most of these models attempted to simplify the assessment process by in-
luding only the most frequently associated factors known to increase the incidence of VTE. The
roblem with this approach is many patients with risk factors not included in the model may be
enied prophylaxis but remain at high risk. Scores such as the Padua score and Improve score
hat do not include family history of thrombosis, or obstetrical-related complications, are good
xamples. These scores do identify most of the patients that are “at risk” for VTE but anytime
patient with family history of thrombosis, or history of an obstetrical complication is encoun-
ered, the patient may be misclassified. We began development of a RAM designed for surgical
atients in 1986 inspired by the work of Professor Maxwell Borow who demonstrated that the
ore risk factors, the more likely the patient would suffer a thrombosis. He further observed
hat there was a linear relationship between the age of the patient and the length of surgery
nd development of a postoperative thrombosis. 7 , 32 He also reported that 25–40% of patients
aving an operative procedure lasting over one hour developed a postoperative thrombosis. The
ate was even higher when additional risk factors were present. He further documented that a
hysical method of compression when combined with an anticoagulant resulted in a very low
ate of postoperative thrombosis.
aprini risk model
Risk assessment is the first step in preventing death and disability from VTE. A multidisci-
linary team put together a list of common risk factors and weighted these factors assigning a
oint score to each factor based on the literature of the day. The points were totaled, and the
core correlated with the 30 and 60 days clinically evident VTE events ( Fig. 1 ). This system ac-
ounted for most of the risk factors known at the time to be associated with VTE. The underuti-
ization of VTE prophylaxis seems to be a global problem. In a large international cross-sectional
tudy across 32 countries, 39.5% only of at-risk medical patients received VTE prophylaxis. 228 On
national level, in 2011 around 20 0 0 VTE events and 940 deaths have been avoided in England
y implementing a compulsory VTE risk assessment tool developed by British investigators. 229
hat tool like the Caprini score includes family history of VTE as a risk factor.
The Caprini RAM was first published in 1991. This model was subsequently modified and
pdated to its most widely used version in 2005 to reflect new evidence and improved
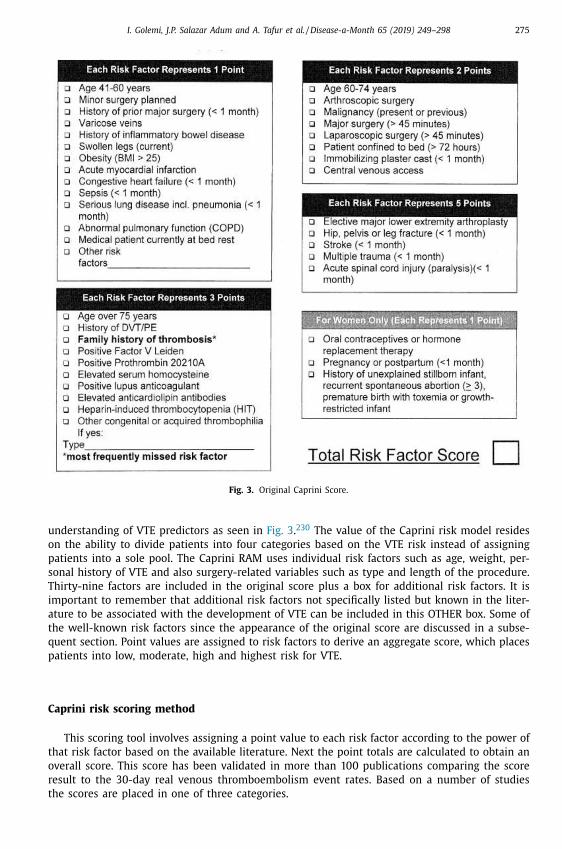
I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298 275
Fig. 3. Original Caprini Score.
understanding of VTE predictors as seen in Fig. 3 . 230 The value of the Caprini risk model resides
on the ability to divide patients into four categories based on the VTE risk instead of assigning
patients into a sole pool. The Caprini RAM uses individual risk factors such as age, weight, per-
sonal history of VTE and also surgery-related variables such as type and length of the procedure.
Thirty-nine factors are included in the original score plus a box for additional risk factors. It is
important to remember that additional risk factors not specifically listed but known in the liter-
ature to be associated with the development of VTE can be included in this OTHER box. Some of
the well-known risk factors since the appearance of the original score are discussed in a subse-
quent section. Point values are assigned to risk factors to derive an aggregate score, which places
patients into low, moderate, high and highest risk for VTE.
Caprini risk scoring method
This scoring tool involves assigning a point value to each risk factor according to the power of
that risk factor based on the available literature. Next the point totals are calculated to obtain an
overall score. This score has been validated in more than 100 publications comparing the score
result to the 30-day real venous thromboembolism event rates. Based on a number of studies
the scores are placed in one of three categories.

276 I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298
3
f
i
t
s
c
b
t
o
w
o
o
t
v
i
t
i
j
a
o
s
T
r
a
H
a
s
s
c
i
f
T
a
p
s
m
t
p
s
l
t
t
m
t
s
c
a
Low-risk patients are spared anticoagulant prophylaxis postoperatively since the incidence of
0-day clinically evident venous thromboembolism events is less or equal to the risk of bleeding
rom anticoagulation. Different set points for this low-risk group have been established depend-
ng upon the population studied. In general, those patients with a score of less than five fall into
his category. As many as 50% of patients fall into this category although a recent meta-analysis
uggests this number may even be higher. 231
Standard-risk patients are those that have a risk score reflecting a VTE incidence that ex-
eeds the incidence of bleeding events using anticoagulation. Point totals in this group average
etween five and eight although those numbers may shift slightly depending on the population
ested. We feel that there is strong evidence that patients in this group require 7 to 10 days
f anticoagulant prophylaxis postoperatively. This opinion is based on the premise that patients
ho are at risk to develop venous thromboembolic events need to be protected for the period
f time that has been shown in the literature to effectively prevent thrombosis. This large body
f evidence will be discussed in a subsequent section. The results of all of these trials indicate
he appropriate period is at least 7–10 days.
High-risk patients are those whose point totals indicate that they are at great risk to develop
enous thromboembolism postoperatively, and merit anticoagulant protection for 30 days. There
s strong evidence in the literature that 30 days of prophylaxis are more effective than shorter
ime periods in patients who are at very high risk for thrombosis which would include people
n this group. Point totals for these patients are > 8 for general surgery, 10 or greater for total
oint replacement, and 12 or more following hip fracture.
The process of collecting these data has evolved over time, and we now feel that the most
ppropriate method is to have the patient fill out a patient friendly questionnaire prior to the
perative day. Patients are encouraged to complete the document in the presence of their family
o that thorough historical perspectives including family history of thrombosis can be uncovered.
he patient should then submit this form ahead of time especially using the electronic medical
ecord portal or other means so that at the time of the admitting history and physical, the
ppropriate healthcare provider can double check the form and ask a few final questions.
Some of the critiques of the Caprini RAM are its complexity and its time-consuming process.
owever, a patient-completed form of the Caprini RAM was recently devised and tested . 232 The
uthors demonstrated an almost perfect correlation between patient and physician-completed
cores. Having the patient fill out the form with their family removes the onus of exten-
ive patient questioning and simplifies the face-to face encounter with the admitting physi-
ian. Collecting all of these data using the EMR and linking the score to a treatment plan is
deal ( Fig. 4 ).
Fuentes and colleagues in a multistep process developed and validated this patient friendly
orm that is highly accurate compared to the same form being filled out by a trained physician.
heir studies have shown that the average patient can complete a form in about five minutes,
nd the physician or healthcare provider completing and checking the document can accom-
lish that task in another five minutes. The authors have found that patients often fail to an-
wer family history questions correctly, and do not understand how to calculate the BMI. Fe-
ale patients often do not understand the questions regarding obstetrical complications and
heir importance in the risk assessment process. The examiner can quickly correct these simple
roblems as well as look for certain physical findings. These include leg edema and clinically
ignificant varicose veins. Finally, the most important objection to collecting the Caprini score
ist of 39 variables has been resolved and this system is now published in four languages, with
ranslations into Thai, Turkish, and at least one Chinese dialect on the way. Paz et al validated
he Caprini score in Spanish, Arabic and Polish speaker languages and reported excellent agree-
ent comparing physician and patient results ( κ = 0.93) and high correlation 0.97 ( P < 0.01) for
he overall score. 232
One of the unique features of the scoring system is the dynamic nature of data collection pos-
ible. During hospitalization the score can be revised depending upon the appearance of certain
linical problems including infection, central lines for administration of antibiotics or chemother-
py, unexpected diagnosis of cancer, or emergent reoperation for anastomotic leaks, or infection.
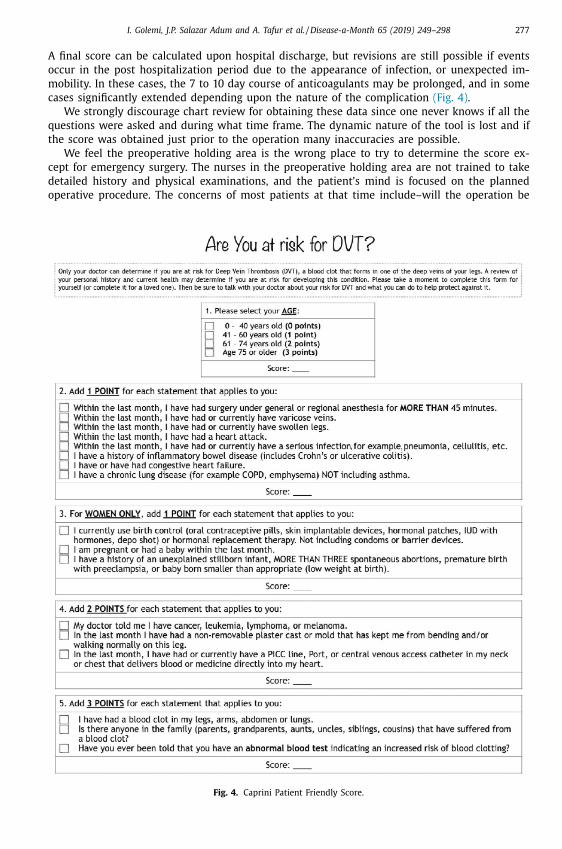
I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298 277
A final score can be calculated upon hospital discharge, but revisions are still possible if events
occur in the post hospitalization period due to the appearance of infection, or unexpected im-
mobility. In these cases, the 7 to 10 day course of anticoagulants may be prolonged, and in some
cases significantly extended depending upon the nature of the complication (Fig. 4) .
We strongly discourage chart review for obtaining these data since one never knows if all the
questions were asked and during what time frame. The dynamic nature of the tool is lost and if
the score was obtained just prior to the operation many inaccuracies are possible.
We feel the preoperative holding area is the wrong place to try to determine the score ex-
cept for emergency surgery. The nurses in the preoperative holding area are not trained to take
detailed history and physical examinations, and the patient’s mind is focused on the planned
operative procedure. The concerns of most patients at that time include–will the operation be
Fig. 4. Caprini Patient Friendly Score.
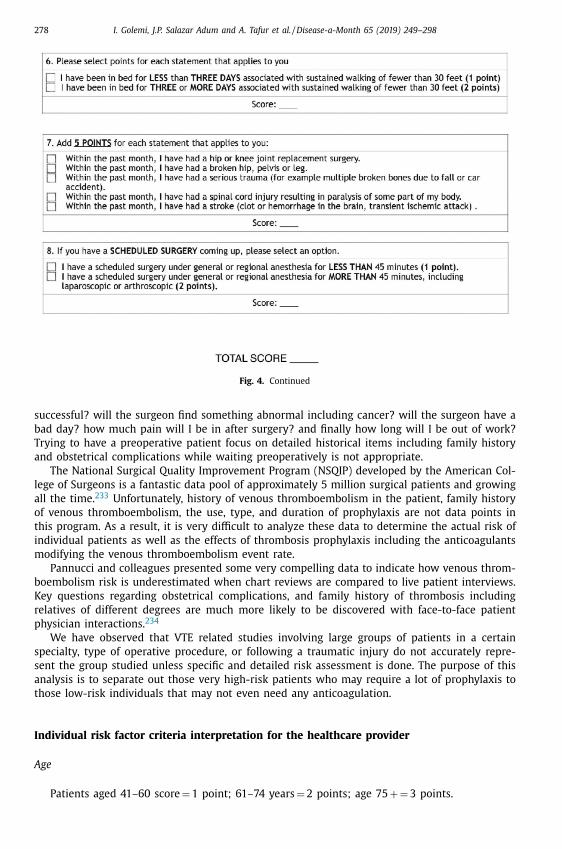
278 I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298
Fig. 4. Continued
s
b
T
a
l
a
o
t
i
m
b
K
r
p
s
s
a
t
I
A
uccessful? will the surgeon find something abnormal including cancer? will the surgeon have a
ad day? how much pain will I be in after surgery? and finally how long will I be out of work?
rying to have a preoperative patient focus on detailed historical items including family history
nd obstetrical complications while waiting preoperatively is not appropriate.
The National Surgical Quality Improvement Program (NSQIP) developed by the American Col-
ege of Surgeons is a fantastic data pool of approximately 5 million surgical patients and growing
ll the time. 233 Unfortunately, history of venous thromboembolism in the patient, family history
f venous thromboembolism, the use, type, and duration of prophylaxis are not data points in
his program. As a result, it is very difficult to analyze these data to determine the actual risk of
ndividual patients as well as the effects of thrombosis prophylaxis including the anticoagulants
odifying the venous thromboembolism event rate.
Pannucci and colleagues presented some very compelling data to indicate how venous throm-
oembolism risk is underestimated when chart reviews are compared to live patient interviews.
ey questions regarding obstetrical complications, and family history of thrombosis including
elatives of different degrees are much more likely to be discovered with face-to-face patient
hysician interactions. 234
We have observed that VTE related studies involving large groups of patients in a certain
pecialty, type of operative procedure, or following a traumatic injury do not accurately repre-
ent the group studied unless specific and detailed risk assessment is done. The purpose of this
nalysis is to separate out those very high-risk patients who may require a lot of prophylaxis to
hose low-risk individuals that may not even need any anticoagulation.
ndividual risk factor criteria interpretation for the healthcare provider
ge
Patients aged 41–60 score = 1 point; 61–74 years = 2 points; age 75 + = 3 points.
I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298 279
Minor surgery
Patients having surgery with an anesthesia time of less than 45 minutes = 1 point.
Past major surgery
Individuals having surgery with an anesthesia time of greater than 45 minutes during the
past month = 1 point.
Major surgery
Planned major surgery with an anesthesia time lasting longer than 45 minutes (including
laparoscopic and arthroscopic procedures) = 2 points.
Total hip or knee replacement
These operations are scored as 5 points each due to their high-risk nature. It should be un-
derstood if additional risk factors are present, that further increases the level of risk. It is a
misnomer to conclude that since all of these procedures are high risk, there is no need to risk
assess. It is important to understand as the level of risk escalates above what is seen in the av-
erage patient, the type, duration, and intensity of the thrombosis prophylaxis must be adjusted.
Patients with scores at the highest level may want to postpone or not have one of these elective
quality-of-life improving procedures.
Visible Varicose Veins
Patients with visible bulging veins would receive a score of 1. This risk factor does not refer to
a patient with spider veins or a patient with a history of surgically removed varicose veins. = 1
point.
Inflammatory Bowel Disease
History of Inflammatory Bowel Disease (IBD) and includes Crohn’s disease or ulcerative coli-
tis. This risk factor includes both active and inactive inflammatory bowel diseases such as ulcer-
ative colitis or regional ileitis. This would not include irritable bowel syndrome or diverticulo-
sis. = 1 point.
Swollen legs (current)
Swollen legs include pitting edema of any level, loss of definition of the bony prominences,
obscured surface foot veins, or indentation of the leg when a stocking is removed. This factor
refers to either one or 2 legs affected. = 1 point.
280 I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298
O
t
B
H
C
a
h
u
S
t
a
a
w
p
L
o
a
P
r
C
“
p
B
t
d
N
verweight or obese (Body mass index above 25 kg/m
2 )
This weight level was associated with patients developing symptomatic thrombosis readmit-
ed following total hip replacement and women developing thrombosis. 65 The combination of
MI 25 kg/m
2 and oral contraceptives increased the thrombotic risk 10-fold. 64 = 1 point.
eart attack
This refers to an acute myocardial infarction during the past 30 days. = 1 point.
ongestive Heart Failure
This risk factor includes patients who have had an episode within the last month. Addition-
lly, patients who are currently being treated with medication for CHF are included, even if they
ave not had an acute episode within the past month. An ejection fraction alone should not be
sed when determining if a patient qualifies for this risk factor. = 1 point.
erious infection (e.g. Pneumonia)
A “serious infection” is defined as a patient who requires hospitalization and intravenous an-
ibiotics for treatment. For example, if a patient has a cellulitis requiring hospitalization with IV
ntibiotics they would receive one point for this risk factor. Treatments that are less severe and
re managed on an outpatient basis with oral antibiotics are not included. Serious infections
ould include diverticulitis, bacterial infection of the bladder and lungs, and septicemia. = 1
oint.
ung disease (e.g. Emphysema or COPD)
In addition to emphysema or COPD these criteria also include any interstitial lung disease
r patients with abnormal pulmonary function tests. This would include, but not limited to,
ny patient with sarcoidosis, pulmonary fibrosis, pulmonary hypertension, and bronchiectasis.
atients who present with more than one diagnosis meeting the criteria for lung disease will
eceive a point for each diagnosis. For example, if the patient has a diagnosis of sarcoidosis and
OPD they would receive a total of 2 points for this risk assessment. Asthma is not considered a
lung disease” for the purpose of the risk assessment score. Additionally, patients with restrictive
ulmonary disease related to obesity would not be included in these criteria. = 1 each point.
ed rest (Restricted Mobility) [1 or 2 points depending on duration]
We define restricted mobility (bedrest) as any individual who is unable to ambulate con-
inuously more than 30 feet. We have chosen this definition based on the prospective ran-
omised, double-blind, placebo-controlled trial in MEDical patients with ENOXaparin (MEDE-
OX), which was a large prospective study where this definition was used. 78 The rate of VTE in

I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298 281
non-ambulatory medical patients without prophylaxis was 19.7% compared to 10.6%; (p = 0.03)
in those that were ambulatory without prophylaxis. 235 Furthermore, the incidence of VTE in
non-ambulatory patients in the LMWH group was reduced to 9.0% compared with 19.7% seen in
the placebo group [RR = 0.46; 95% CI,0.23 − 0.91; p = 0.02] (10.7% absolute risk reduction). In the
ambulatory group, VTE incidence was 3.3% with enoxaparin 40 mg compared with 10.6% in the
placebo group (RR = 0.31; 95% CI, 0.13 − 0.78; p = 0.008. The absolute risk reduction was 7.3%.
We assign one point to those fitting the definition of bedrest < 72 hrs. We realize that there
are other definitions regarding ambulation but we feel the above data are the most robust. 236
Critics ask why isn’t everyone who spends a night in bed sleeping also at risk? We would
answer that the bedrest in hospitalized patients is associated with their underlying disease pro-
cess. For example, a person who has congestive failure, severe pain, infection, stroke, etc. is at
bedrest because of their disease process. A normal person goes to bed to get necessary rest, not
because of a specific illness. Patients moving short distances to the bathroom or sitting in a chair
are not ambulatory according to this definition. Although we use the term medical patients at
bedrest, these scores apply to all patients.
Patients who are using a cane or walker for stability are not considered as having restricted
mobility if they are using their calf muscles for ambulation.
Patients who are unable to ambulate 30 feet continuously for > 72 hrs. receive 2 points total
for restricted mobility. (We do not add an additional point for the first 24 hrs.)
A patient who requires crutches and is non-weight bearing would pass the restricted mobility
criteria but would receive 2 points if they are not using calf muscles in one leg due to a brace,
boot, or cast even though they can ambulate 30 feet.
Non-Removable Plaster Cast Or Mold (Worn For > 72 Hours) That Prevents Leg Movement Within
The Last Month (2 points)
The intent of this criterion is to capture any limitation in leg mobility which would interfere
with calf muscle pumping action such as a leg brace or cast. 237 Remember that patients using
crutches who are non weight bearing on one leg would also be included. The use of an assistive
device for stability, such as a walker, would not meet the criteria if the patient is using their calf
muscles. = 2 points.
Confined to bed for 72 hours or more (unable to ambulate continuously 30 feet)
“Confined to bed” is confusing terminology and should be referred to as impaired mobility.
The patient is unable to ambulate continuously 30 feet. This would also apply to any patient
who is unable to ambulate using both leg muscles. For example, a patient who requires crutches
and is non-weight bearing would be considered as restricted mobility even though they can
ambulate 30 feet. Patients who are using a cane or walker for stability are not included in this
group if they are using their calf muscles for ambulation. Patients moving a short distance to
the bathroom or sitting in a chair are not ambulatory according to this definition. = 2 points.
Central Venous Lines
Tube in blood vessel in the neck or chest that delivers blood or medicine directly to the heart
within the last month (e.g. central venous access, PICC line, port). = 2 points.
Current Or Past Malignancies (Excluding Skin Cancer But Including Melanoma)
Whether the cancer diagnosis is remote or recent the patient will receive a score of 2. This
is because patients with a remote history of cancer are always at risk for occult metastasis
which would increase their risk for thrombosis. Every incidence of cancer is considered sepa-
rately and scored accordingly. For example, a patient who has a remote history of breast cancer
and is recently diagnosed with uterine cancer would receive a score of 4 (2 points for each
episode of cancer). For the purpose of this document Ductal Carcinoma in situ (DCIS) would
also receive a score of 2 as there is always the potential of an invasive cancer. Myelodys-
plastic Syndrome (MDS) would be scored as 2 points only if the disease requires chemother-
282 I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298
a
t
b
w
c
p
s
S
s
d
G
m
c
t
D
a
s
p
a
b
r
u
m
c
t
b
o
py treatment. The patient would also receive an additional point for the chemotherapy
reatment.
History of Blood Clots, Either DVT or PE. This Also Includes History of Superficial Venous Throm-
osis (SVT) = 3 points
Arterial blood clots are not included in the scoring. A CVA due to a paradoxical embolus
ould be given 3 points; however, a DVT must be documented by an objective measure in this
ase. Each episode of a DVT or PE is captured as a separate event for scoring. For example, a
atient with a medical history of DVT in 2014 and PE in 2015 would be given a cumulative
core of 6. However, PE and DVT events that occur simultaneously would be scored as 3 points.
VT must be captured and scored a 3 here as well. 238
Family History VTE = 3 points
Family history of VTE should include first-degree relatives (sibling, son/daughter, parent),
econd-degree relatives (maternal half-sibling, paternal half-sibling, niece/nephew), and third-
egree relatives (cousin). Younger age of first VTE and male relative increase the risk. 77
Personal or family history Of positive blood test indicating an increased risk Of blood clotting (e.g.
enetic Or Acquired Thrombophilia)
A patient will receive a score of 3 points for each genetic thrombophilia marker. If a family
ember has a proven genetic marker the patient will receive a score of 3 unless it has been
onfirmed that the patient does not have this genetic marker. Genetic (inherited) factors: Fac-
or V Leiden/Activated protein C resistance, Antithrombin III deficiency, Protein C & S deficiency,
ysfibrinogenemia, homozygous MTHFR, 20210A prothrombin mutation. Acquired factors: Lupus
nticoagulant, antiphospholipid antibodies, myeloproliferative disorders (including thrombocyto-
is), disorders of plasminogen and plasmin activation, Heparin-induced thrombocytopenia, hy-
erviscosity syndromes, homocysteinemia. Human immunodeficiency virus (HIV) infection is an
cquired thrombophilia. 239
Fracture of the Hip, Pelvis, Or Leg
Fractures requiring surgical repair would receive 5 points for the fracture and will also
e assessed additional points depending on the type of surgery. Patients undergoing an open
eduction and internal fixation (ORIF) would be given 2 points for “surgery over 45 min-
tes”. Patients requiring a hemi-arthroplasty would receive 5 points “for elective hip replace-
ent surgery”. For example, a patient with a fractured ankle undergoing an ORIF would re-
eive a score of 7; 5 points for the fracture and 2 points for the surgical repair. An addi-
ional 2 points would be added if a cast or brace is applied or the patient is non-weight
earing.
Serious trauma (E.G. Multiple Broken Bones Due To A Fall Or Car Accident) = 5 points
Now or within the past month. There is some overlap between this category and the previous
ne and only one of these categories should be chosen.
Spinal Cord Paralysis or Stroke = 5 points
Now or within the last month.
Women Only
Current use of birth control or Hormone Replacement Therapy (HRT)
This includes estrogen contraceptives of any type. This also includes estrogen-like drugs, in-
cluding raloxifene, tamoxifen, anastrozole, and letrozole. Exemestane has not been shown
to increase the risk for DVT. Additionally, estrogen plus progestin, and progestin with or
without estrogen are independent VTE risk factors. 240 Recent publications have shown
that there is no increased risk of DVT in men who are on long term testosterone ther-
apy, therefore, testosterone is excluded. = 1 point.

I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298 283
Pregnancy or postpartum In The Last Month = 1 point
History of unexplained stillborn infant, recurrent spontaneous abortion (more than 3), premature
birth with toxemia or growth r estricted infant = 1 point
Recurrent fetal loss is associated with antiphospholipid antibody syndrome, procoagulant
platelet microparticles and some inherited thrombophilias such as Factor V Leiden. There have
been reports of both heritable and acquired thrombophilias being associated with pre-eclampsia,
intrauterine growth restriction (IUGR) and abruption. However, these associations are not con-
sistently reported with hereditary thrombophilias. 241
Additional risk factors not specifically validated in the original Caprini model
A number of additional risk factors that have been associated with the development of VTE
although not specifically listed in the 2005 score should be considered as additional risks. Note
that there is a category for others in the original 2005 document and no audit has been done to
indicate what additional risk factors have been scored over the past 13 years. Each one may be
scored as one point.
Smoking 242 Smoking is defined as the inhalation of anything that burns, including tobacco,
marijuana, or vaping = 1 point.
BMI > 40 , 243 244 Individuals who are physically fit or athletes but very large are not exempt
from this risk factor. The increased body mass is associated with stress on the cardiovascular
and respiratory systems and thrombotic risk = 2 points.
Diabetes requiring insulin 173,173,172 Only insulin products are included in the risk assessment
score. This does not include any other oral or parenteral medications used for the treatment of
diabetes = 1 point.
Chemotherapy 90,245 Chemotherapy treatments used for any medical condition are included
in the scoring. For example, a patient receiving Methotrexate for Rheumatoid Arthritis, re-
gardless of the dose given, would receive a point for this risk assessment. Patients diagnosed
with essential thrombocytosis taking hydroxyurea would also receive a point here, in addi-
tion to 3 points for “personal history of positive blood test indicating increased risk for blood
clotting”.
Blood Transfusions 246 Add one point for one or more blood transfusions
Length Of Surgery Over 2 Hours 7 Actual current surgery time exceeding 2 hours, including
anesthesia time. Do not add to the “5” for total hip or knee replacement surgery (add 1 point).
Meta-analysis involving selected studies using the Caprini score
One of the most valuable features of the Caprini Score is the ability to protect low-risk pa-
tients from receiving anticoagulant prophylaxis. Multiple studies have shown that the incidence
of clinical thrombotic events in patients with a score of 4 or less is below 1%, 247 and Pannucci
has published a meta-analysis involving 13 studies (14,776 patients) showed that 75% of patients
had a score of 6 or less, and could be spared anticoagulant prophylaxis. 231 They also found that
these patients did not have a significant VTE risk reduction with chemoprophylaxis. On the other
hand, those individuals not receiving prophylaxis had a 14-fold variation in clinical VTE risk de-
pending upon their score (0.7% to 10.7%). These findings underscore the importance of knowing
the type, dose, and extent of thrombosis prophylaxis in a surgical population for proper overall
evaluation of VTE incidence.
One must remember that meta-analysis only analyzed 13 of over 100 studies as of this date.
CHEST 2012 guidelines suggest that a Caprini score of 5 or more is associated with up to a 6%
incidence of clinical VTE, and these individuals benefit from anticoagulant prophylaxis. 249
Leonardi has shown that the bleeding complications associated with anticoagulants are not
trivial. He found that the incidence of wound hematoma, mucosal bleeding, and those having
284 I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298
p
t
c
t
V
a
t
G
t
S
t
r
3
a
(
h
h
m
W
B
E
o
T
t
t
p
p
(
s
i
m
s
i
c
e
t
L
P
P
rophylaxis ranges from 2.0 to 5.5%. 250 These data emphasize the importance of using the score
o target truly at-risk individuals.
This meta-analysis is an excellent example of how the Caprini score works. The low risk
ategory comprises people who are spared of anticoagulation since the risk of bleeding exceeds
he risk of anticoagulants to prevent VTE. The second group of patients that have risks factors for
TE and prophylaxis is clearly warranted. The high and highest risk subgroups comprise patients
t high risk of thrombosis in whom extended thromboprophylaxis should be given after leaving
he hospital up to 30 days post discharge.
eneral and vascular surgery
Bahl and associates from the University of Michigan published a landmark study to validate
he Caprini score in a retrospective analysis. A total of 8,216 surgical patients from the National
urgical Quality Improvement Program were included (general, urology, and vascular surgery),
he majority (52.1%) of the patients were classified to the highest risk level; 36.5% were high-
isk, 10.4% as moderate risk, and 0.9% as low risk. The overall incidence of acquired VTE within
0 days post procedure was 1.44%. The incidence of DVT was associated with an increased risk
ccording to the level of the patient’s risk (highest risk level 1.94%); (high-risk patients 0.97%);
moderate risk patients 0.70%); and (low-risk patients 0%). The difference between high and
ighest risk levels was statistically significant ( p: 0.001). 247 The University of Michigan hospitals
ave used this risk assessment tool along with mandatory care pathways since 2008. Physicians
ust opt-out of the standard algorithm for using thrombosis prophylaxis during hospitalization.
ithout enforcing care pathways, they are often ignored.
enchmark study for reducing the VTE rate
Cassidy, et al, from the Boston Medical Center, the largest safety-net urban hospital in New
ngland, developed a strategy to reduce VTE complications using the Caprini RAM. The scores
btained indicated the nature and length of thromboprophylaxis including an outpatient setting.
he investigators used mechanical (pneumatic compression boots) and pharmacologic (unfrac-
ionated or low molecular weight heparin) as dictated by the risk stratification tool comparing
he National Surgical Quality Improvement Program VTE outcomes (DVT, PE) before and after ap-
lying the standardized risk-stratified protocol in conjunction with a postoperative mobilization
rogram.
The study resulted in decreasing the incidence of DVT observed by 84%, from 1.9% to 0.3%
p < 0.01), with implementation of VTE prevention efforts.
The PE incidence decreased 55%, from 1.1% to 0.5% (p < 0.01). Risk-adjusted VTE outcomes
teadily declined from an OR of 3.41 to 0.94 (p < 0.05). The authors concluded with the follow-
ng statement “A patient care program, emphasizing early postoperative mobilization along with
andatory VTE risk stratification and commensurate electronic prophylaxis recommendations,
ignificantly reduced the likelihood of VTE complications among our patients”. 61 Key elements
n this program centered on mandatory compliance with an opt-out clause for the physician
ombined with providing prophylaxis according to risk for the period of time shown in the lit-
rature to be efficacious. The highest risk patients (score 9 + ) received 30 days of LMWH and
here was 77% compliance in these patients. Patients with a score of 5–8 received 7–10 days of
MWH prophylaxis with a compliance rate of 89%.
lastic and reconstructive surgery
In a retrospective analysis from the Venous Thromboembolism Prevention Study Network,
annucci et al. investigated the validity of the Caprini RAM in plastic and reconstructive surgery
I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298 285
patients. A total of 1126 patients were included. The overall incidence of VTE was 1.69%. Patients
with a Caprini score 8 were significantly more likely to develop VTE when compared with pa-
tients with Caprini score of 3 to 4 (OR: 20.9, p 0.001), 5 to 6 (OR: 9.9, p 0.001), or 7 to 8 (OR:
4.6, p 0.015). Approximately 1 in 9 patients (11.3%) with Caprini score 8 had a VTE event. It was
noted that VTE risk was not limited to the immediate postoperative period (days 1–14) among
patients with Caprini score 7 to 8 or Caprini score 8. Among these high-risk patients, more than
50% of VTE events were diagnosed in the late postoperative period (days 15–60). 248
Trauma surgery
A single center, retrospective case-control study of 78 patients with VTE versus 156 non-VTE
patients who were randomly selected in a 2:1 ratio and admitted to the intensive care unit due
to their critically ill status was done. The Caprini RAM was used to obtain the VTE risk score
and VTE risk classification in critically ill VTE patients and non-VTE patients in order to prove
the validity of the Caprini RAM. Zhang et al., found that patients with VTE had a higher Caprini
score compared to the control group ( p < 0.001). Critically ill VTE patients classified at high risk
and very high accounted for 88.4% according to the Caprini RAM. Compared to low-risk patients,
the incidence risk of VTE patients at high-risk and very high-risk was significantly higher (OR:
2.042 in high-risk; OR: 11.681 in very high-risk patients). The logistic regression model identi-
fied eight risk factors in the Caprini RAM as predictors of VTE: bed-bound in internal medicine
wards, severe lung disease ( < 1 month), sepsis ( < 1 month), large operation ( < 1 month), ma-
lignant tumor, VTE personal history, VTE family history, and thrombosis with multiple trauma
( < 1 month). The authors concluded that the Caprini RAM was applicable for critically ill pa-
tients, and had good predictive value for risk of VTE. 251
Otolaryngology
One of the Boston University studies involved patients from the Otolaryngology Service.
Seven hundred and four patients were included in this study and the average score was 9.87 for
those patients suffering a VTE event. The score for those without thrombosis was 5.62. Patients
with a score of six and below did not suffer any thrombotic events. The incidence of throm-
bosis with a score of 7 to 8 was 3.01%percent while those with a score of greater than nine
was 13.16%. The authors concluded that a score of over eight predicts a high risk of thrombosis
despite chemoprophylaxis during the hospitalization. This is a good example of how the score
threshold should be derived in individual surgical specialties to target the use of prophylaxis
with anticoagulation to those at or above the threshold rather than a shotgun approach giving
anticoagulants to all postoperative patients. 252
Another study in 2016 otolaryngology patients from the University of Michigan demonstrated
the use of the Caprini Score to risk stratify this patient population. Those with the score of six
or less had a DVT incidence of 0.5% while those with a score of seven or eight the incidence
rose to 2.4%. Finally, in those with a score of > 8, the incidence of thrombosis was 18.3%. These
statistics were based on 30-day follow-up of the patients and in this study these patients did
not receive prophylactic anticoagulation. 253
Chest surgery
The Caprini score was evaluated in a retrospective study of 232 patients operated for lung
cancer from 2005–2013 at Boston University. All of the patients received inpatient prophylaxis
with UFH 50 0 0 units TID, and were followed for 60 days. The overall incidence of VTE at 60
days was 5.2%, and 33% of the events occurred post-discharge. No VTE events were seen with
286 I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298
p
h
t
t
p
c
s
p
g
p
e
3
d
t
(
b
p
t
O
f
W
o
t
c
a
p
C
g
e
w
p
i
o
s
w
w
s
a
p
a
c
o
e
r
s
a
r
atients scores of < 5, while 1.7% of patients had a VTE event with a score of 5–8. The very
igh-risk group with a score of 9 + had a 10.3% incidence of VTE events. The authors suggested
hat these data should result in establishing a policy for outpatient anticoagulant prophylaxis for
hose with high scores. 254
In another study from Boston University thromboembolism rates were compared using a
reintervention group of thoracic surgery patients retrospectively analyzed from 2005–2013 in-
luding some patients in the previous study. The patients included both those having lung
urgery as well as a group of esophagectomy patients. These patients all received inpatient pro-
hylaxis with UFH only (302 patients). This patient group was compared to a post-intervention
roup (64 patients) starting in 2014 which divided patients into 3 categories according to a
reviously established protocol in general surgery described elsewhere. The most important el-
ment of this protocol was continuing prophylaxis with LMWH beyond discharge for a total of
0 days. In addition, those with a BMI > 40 received 40 mg injections twice daily instead of once
aily in the lower weight patients. Provider adherence to the protocol was 100% and the pa-
ient adherence was 97.4%. The preintervention group had an incidence of VTE events of 7.3%
22/302), and the post intervention group had a VTE incidence of 3.2% 2/64. There were no
leeding complications and although these results are not statistically significantly different, the
ositive trend and high patient acceptance of extended prophylaxis, the authors felt, supports
his approach. 255
rthopedic surgery
A prospective study involving 92 fracture patients was done to evaluate clinical predictors
or preoperative DVT. Specifically, clinical signs, d -dimer, DVT risk assessment score both with
ells and Caprini scores and Doppler ultrasonography were done preoperatively. The incidence
f preoperative DVT was 16.3% and in these patients the Wells and Caprini scores were statis-
ically significantly higher than those not suffering a thrombosis (p < 0.05 all). 256 The authors
oncluded that patients with a Caprini score of 12 or more should be screened with a preoper-
tive ultrasound examination to rule out DVT.
A very recent publication involving 1078 patients has appeared comparing the results of a
rospective department-based protocol in patients undergoing total joint replacement to the
aprini risk assessment model retrospectively in the same patient group. 257 The investigators’
oal was to determine if the department protocol or the Caprini score would better identify VTE
vents after total joint replacement. All therapeutic decisions regarding thrombosis prophylaxis
ere based on the department protocol not the Caprini score. The department protocol divided
atients into low or high risk based on the presence or absence of one or more of the follow-
ng criteria. Patients were considered high risk if they had a VTE within the prior year, morbid
besity with a BMI greater than 40 with additional comorbidities, active malignancy, bilateral
taged total joint replacement, and inherited or acquired thrombophilia. If none of these criteria
ere present the patient was considered low risk. Total hip and knee replacement patients who
ere considered low risk received aspirin 325 mg twice daily for six weeks. Those patients con-
idered high risk received 12 days of a DOAC anticoagulant followed by twice daily aspirin for
n additional four weeks. At the conclusion of the study a retrospective chart review of every
atient was conducted and a Caprini score determined for each of these individuals. Statistical
nalysis indicated that the high-risk cutoff for the Caprini score was 10 or above.
Eight patients in this study suffered a symptomatic venous thromboembolic event and ac-
ording to the department protocol, 7 of these individuals were considered low risk receiving
nly aspirin prophylaxis. On the other hand, seven of the eight patients with the thrombotic
vent were correctly placed in the high-risk group with a Caprini score of 10 or more. Once the
esults of this study became available, the department protocol was abandoned in the Caprini
core is now used prospectively to classify these total joint replacement patients and provide
ppropriate prophylaxis. A large multicenter trial is being proposed to verify these preliminary
esults. We feel it is possible in the future, based on additional studies, to define the population
I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298 287
where aspirin is the most appropriate choice and selectively use the more powerful anticoagu-
lants where the risk is clearly greater.
Medical patients
A number of studies have addressed the Caprini score in medical patients over the past few
years. 258–265 These studies in many cases have compared the Caprini Score to the Padua Score
which has been recommended by CHEST 2012 for use in medical patients. CHEST consensus
leaders did not look at the Caprini score at that time despite several reports indicating the util-
ity of this score in medical patients. Since that time a number of reports have documented the
Caprini score as being more valuable in identifying patients at high risk for VTE. Several impor-
tant factors are recorded in the Caprini score that are missing in the Padua score and other more
recent scores proposed for use in medical patients. The most important missing factor in these
other scores is family history of thrombosis. This factor is discussed in detail elsewhere, and
represents a powerful predictor of VTE. Obstetrical complications are another important missing
question not addressed in other scores. These obstetrical complications may be associated with
the Antiphospholipid Antibody Syndrome which may be associated with an increased risk for
thrombosis. Another simple fact is no other risk scores look at as many variables, and we know
the more thorough a history and physical, the more comprehensive analysis of risk is possi-
ble. Unfortunately life is not simple and just looking at some common risk factors often results
in missing important variables. 266 The latest guidelines for thrombosis prophylaxis in medical
patients have just been published. They discuss the use of the Padua or IMPROVE scores but
acknowledge that –“Although optimal strategies for VTE risk assessment and decision making
on prophylaxis are yet to be identified, when clinicians and health care systems use these ASH
VTE guidelines, they should integrate VTE and bleeding risk assessments into clinical decision
making processes.” We assume that despite the number of publications addressing the Caprini
Score in medical patients none of that data was considered relevant for their review. 267 We look
forward to more studies using the Caprini score in this patient population. A number of large
hospitals have suggested that using a hospital-wide risk assessment tool is preferred for a num-
ber of practical reasons.
Bleeding Vs. Thrombosis
It is important to understand that skilled surgeons are rightfully concerned about postopera-
tive bleeding that may result from prophylactic anticoagulants. Certain bleeding events may be
associated with significant postoperative complications including infection, reoperation, or de-
creased functional outcomes in the case of total joint replacement procedures. While that’s a
major concern it is important to realize that bleeding deaths are very rare using prophylaxis.
Withholding anticoagulation and in surgical patients who are at significant risk may be associ-
ated with an increased incidence of fatal pulmonary embolism.
Kakkar and associates published a randomized prospective multicenter trial involving pro-
phylaxis against fatal pulmonary emboli using low-dose unfractionated heparin. 268 They en-
rolled 4121 patients undergoing major surgery in this trial. Anticoagulant prophylaxis was used
for one week, and objective endpoints including venography were employed. In the 24 centers
involved, 16 fatal pulmonary emboli occurred in the control group versus two patients in the
group treated with heparin prophylaxis for one week. The authors concluded that low-dose un-
fractionated heparin saved 7 lives for every 1,0 0 0 operated patients. The overall incidence of
deep vein thrombosis was reduced from approximately 30% in the controls to 10% in the treated
patients. No deaths from bleeding were observed in the patients receiving heparin prophylaxis.
Many surgeons were skeptical of these results since at that time (1975) it was unheard of to
give surgical patients anticoagulants which might result in postoperative bleeding. Public opin-
288 I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298
i
i
a
r
b
p
t
p
h
f
n
t
2
c
s
w
f
t
c
4
l
o
t
4
t
n
w
l
L
2
o
r
m
A
t
p
t
u
v
e
p
m
J
i
o
i
on changed when Rory Collins published the results from the analysis of 70 evenly random-
zed trials of perioperative unfractionated heparin compared to controls in general, orthopedic,
nd urological surgery. 269 There were over 12,0 0 0 patients in this study and the results were
emarkably similar to the original Kakkar trial 15 years earlier. The risk of fatal pulmonary em-
olism was reduced from 0.9% to 0.3% representing a 66% relative risk reduction in the treated
atients. The overall incidence of pulmonary emboli was 3% in the control group and 1.7% in
he treated subjects. There was no difference in bleeding deaths between controls and treated
atients. In 1988 one could conclude that in 94 centers around the world over a 15-year period
ighly statistically significant reduction of venous thromboembolism including deaths resulted
rom administering unfractionated heparin in small doses to postoperative patients. Of great sig-
ificance was the fact that there was no difference in bleeding deaths between the controls and
he treated patients. THE TREATMENT PERIOD FOR ALL OF THESE STUDIES WAS 7–10 DAYS.
A randomized double-blind comparison of LMWH with unfractionated heparin involving
3,078 surgical patients given prophylaxis for 5 to 20 days was carried out in 67 worldwide
enters and the results reported in 2005. 270 Autopsy adjudicated fatal pulmonary emboli repre-
ented the primary endpoint in the trial and occurred in 0.15% of patients in either group. There
ere no deaths from anticoagulant related bleeding in the 23,078 patients. One may conclude
rom these results that administration of one of these anticoagulants for at least five days prac-
ically eliminated the possibility of a fatal pulmonary embolus despite many patients at signifi-
ant risk for venous thromboembolism. The combined results of the above three trials involved
3,0 0 0 patients, 160 centers worldwide given anticoagulant prophylaxis for ONE WEEK estab-
ishing efficacy with objective diagnostic endpoints. Remember these studies were conducted
ver a 30-year period.
The CHEST 2012 guidelines reported on the results of a meta-analysis of 51 randomized con-
rolled trials comparing low molecular weight heparin to low-dose unfractionated heparin in
8,0 0 0 general and abdominal surgical patients who were treated for at least SEVEN days, and
he thrombotic risk was 30% lower in the low molecular weight heparin groups. 271 Unfortu-
ately, the CHEST 2012 consensus guidelines did not emphasize providing prophylaxis for one
eek despite the fact that this period was shown to be efficacious in these 51 trials they ana-
yzed.
ength of prophylaxis
The Surgical Care Improvement Program (SCIP) was a nationwide program established in
006 to improve surgical care. One of the initiatives involved the administration of a single dose
f anticoagulant medication within 24 hours of surgery to patients who were judged to be at
isk for venous thromboembolism and did not have a contraindication from bleeding (SCIP-VTE
easure). It was a required Joint Commission measure for all hospitalized surgical patients. 272
ltom and associates published a large trial involving 30,531 patients having surgery from 2006
o 2009 in a database linked with the Veterans Administration surgical quality improvement
rogram data. 80 Compliance with the measure was documented in 89.9% of the patients and
he incidence of venous thromboembolism in these patients was 1.4%. Noncompliance was doc-
mented in 10.1% of the patients, and the incidence of venous thromboembolism in these indi-
iduals was 1.3%. The authors concluded that there was no association between SCIP-VTE adher-
nce and the incidence of postoperative venous thromboembolism. Although those results were
ublished in 2012 this practice continues in many hospitals to this day despite the fact that this
easure has been discontinued by the centers for Medicare and Medicaid services.
A study involving 50 0,0 0 0 US venous thromboembolism events annually was reported by
ohn Heit from the Mayo Clinic in 2017. 79 Half of these events were related to hospitalization
n patients where near universal in-hospital VTE prophylaxis was provided. The mean duration
f hospital stay was 70 hours. The authors concluded that a short course of anticoagulant is
neffective in lowering the VTE rate.
I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298 289
Another study, this time following total joint replacement, found that the rate of pulmonary
emboli increased from 0.87% prior to the SCIP-VTE measure to 1.3% following implementation of
the measure. 273 The authors concluded that this measure was not successful in reducing com-
plications in total joint replacement patients.
The largest study demonstrating the discordance between SCIP-VTE adherence and postoper-
ative outcomes involves 779,922 patients followed for 30 days over a five-year period and re-
ported in 2017. 81 During that time adherence to the measure improved from 14.6% to 20%. The
postoperative DVT rate increased by 7.1% and the postoperative PE rate increased by 3.7%. The
authors concluded that short-term anticoagulant prophylaxis postoperatively does not lower the
VTE rate. Lowering the VTE rate after surgery requires at least one week as previously shown in
more than 160 centers over the past 40 years.
Extended prophylaxis
The RIETE worldwide database was queried in 2008 by Arcelus and colleagues and they re-
ported on the time course in clinical presentation of postoperative VTE using these registry data.
They observed that 77% of patients developed their thrombotic event after leaving the hospital
and 55% of these thrombotic events were diagnosed after prophylaxis was discontinued. 274 These
data emphasize the need for continued prophylaxis after hospitalization for at least a week or
in cases of very high risk up to 30 days postoperatively.
CHEST 2004 guidelines considered history of thromboembolism in the highest risk group of
patients along with cancer and indicated that the risk of thrombosis was as high as 40 to 80%
with a 1% to 5% chance of a fatality. 60 These data were based on objective endpoints including
asymptomatic thrombotic events. They recommended continuing thrombosis prophylaxis for 28
days on the basis of these event rates. The 2008 CHEST guidelines emphasized that patients
who have undergone major cancer surgery or have previously had VTE should be considered to
receive LMWH prophylaxis for 28 days. 275
The CHEST 2012 guidelines suggested that risk of VTE remains elevated for at least 12 weeks
following surgery. 249 This edition of the guidelines included three excellent studies including
one meta-analysis in patients having surgery for benign and malignant disease. All three studies
concluded that extended duration prophylaxis reduces the risk of symptomatic or asymptomatic
DVT by at least 50% and two of them reported that proximal DVT was reduced by 75%. The
CHEST authors reiterated their suggestion that for patients undergoing major cancer surgery 28
days of prophylaxis should be considered, but failed to include a past history of DVT in these
recommendations despite the fact that the prior two editions of the guidelines made that rec-
ommendation. We find that conclusion odd considering that the data in the 2012 guidelines
regarding extended prophylaxis was much more robust than in the previous editions. This in-
cluded the meta-analysis involving patients with both cancer and benign diseases. 276 We would
suggest based on all of these data as well as the excellent study from Boston University that
patients considered to be very high risk using the Caprini score should receive 30 days of anti-
coagulant prophylaxis with LMWH. The very high-risk group in that study and related studies in
the Boston Hospital system was defined as a score of > 8. 61 We also suggest that in an individual
population the very high-risk score be determined prospectively. Several orthopedic groups per-
forming joint replacement use a score of 10 + as the very high-risk category, 257 and one study
uses 12 + in hip fracture patients. 256
Conclusions
1. Avoid chart reviews since they depend on the accuracy of the data collection including did
the examiner ask all of the questions. Face-to-face encounters are critical as well as using
the patient-friendly form. Patients welcome the invitation to participate in their care.

290 I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298
1
A
R
2. Mandatory compliance must be enforced for prophylaxis protocols based on risk score
to have a lasting effect lowering the VTE rate. The physician should be given the opt-
out option based on individual clinical circumstances; otherwise, the protocol should be
automatic.
3. Use of clinical judgment to select a prophylaxis option in the face of patients with a history
or family history of VTE, or increased risk of bleeding, instead of relying on guidelines is
critical and may be lifesaving. The guidelines commonly exclude patients at high risk for VTE
as well as those with a past history or family history of VTE.
4. Understanding that bleeding deaths from the use of prophylaxis are very rare, while with-
holding anticoagulation in surgical patients “at risk” is associated with an increased risk of
fatal pulmonary emboli.
5. Administering anticoagulant prophylaxis to high risk patients for one week as shown in 160
trials involving 43,0 0 0 patients should be followed since that is the time period shown to be
efficacious for thrombosis prevention. It is important to avoid the temptation of short courses
of anticoagulants during brief hospital stays, or outpatients in high-risk individuals
6. Prescribe anticoagulant prophylaxis for at least 30 days in very high-risk individuals. It is
important to remember that most patients develop thrombosis after leaving the hospital,
and when short courses of anticoagulants are discontinued.
7. Ambulation has no effect on existing risk factors such as cancer or history of venous throm-
boembolism and only decreases the risk associated with immobility.
8. Remember that 66% of patients having surgery, who had a history of venous thrombosis suf-
fered a postoperative thrombosis when prophylaxis with anticoagulants was omitted.
9. Understand the value of family history as a risk indicator for venous thrombosis and pul-
monary emboli. Note that this is the most frequently missed or ignored risk factor which
can result in a serious postoperative thrombotic event. This history should include all 3 de-
grees of relatives.
0. Continue appropriate anticoagulant prophylaxis long-term in patients with ongoing risks
such as immobilization, infection, casts, rigid leg braces, or metastatic cancer.
cknowledgment
The authors wish to acknowledge Dr. Thomas Wakefield for reviewing this manuscript.
eferences
1. O’Donnell M , Weitz JI . Thromboprophylaxis in surgical patients. Can J Surg . 2003;46(2):129–135 . 2. Kahn SR , et al. Prevention of VTE in nonsurgical patients: Antithrombotic Therapy and Prevention of Thrombo-
sis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest . 2012;141(2
Suppl):e195S–e226S . 3. Haas S , et al. Prevention of fatal pulmonary embolism and mortality in surgical patients: a randomized double-blind
comparison of LMWH with unfractionated heparin. Thromb Haemost . 2005;94(4):814–819 . 4. Prevention of fatal postoperative pulmonary embolism by low doses of heparin. An international multicentre trial .
Lancet . 1975;2(7924):45–51 . 5. Collins R , et al. Reduction in fatal pulmonary embolism and venous thrombosis by perioperative administration of
subcutaneous heparin. Overview of results of randomized trials in general, orthopedic, and urologic surgery. N Engl
J Med . 1988;318(18):1162–1173 . 6. Brose KM , Lee AY . Cancer-associated thrombosis: prevention and treatment. Curr Oncol . 2008;15(Suppl 1):S58–S67 .
7. Borow M , Goldson H . Postoperative venous thrombosis. Evaluation of five methods of treatment. Am J Surg .1981;141(2):245–251 .
8. Rosendaal FR . Causes of venous thrombosis. Thromb J . 2016;14(Suppl 1):24 . 9. Cushman M . Epidemiology and risk factors for venous thrombosis. Semin Hematol . 2007;44(2):62–69 .
10. Rosendaal FR . Thrombosis in the young: epidemiology and risk factors. A focus on venous thrombosis. Thromb
Haemost . 1997;78(1):1–6 . 11. Centers for disease control and prevention (2014) Deep Vein Thrombosis (DVT) / Pulmonary Embolism (PE) — Blood
Clot Forming in a Vein. 12. Heit JA , et al. Estimated Annual Number of Incident and Recurrent, Non-Fatal and Fatal Venous Thromboembolism
(VTE) Events in the US. BLOOD . 2005:910 .

I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298 291
13. Beckman MG , et al. Venous thromboembolism: a public health concern. Am J Prev Med . 2010;38(4
Suppl):S495–S501 . 14. Agnelli G , et al. The management of acute venous thromboembolism in clinical practice - study rationale and pro-
tocol of the European PREFER in VTE Registry. Thromb J . 2015;13:41 .
15. Sandler DA , Martin JF . Autopsy proven pulmonary embolism in hospital patients: are we detecting enough deepvein thrombosis? J R Soc Med . 1989;82(4):203–205 .
16. ISTH Steering Committee for World Thrombosis Day . Venous thromboembolism: A Call for risk assessment in allhospitalised patients. Thromb Haemost . 2016;116(5):777–779 .
17. Johanson NA , et al. American academy of orthopaedic surgeons clinical practice guideline on. Prevention ofsymptomatic pulmonary embolism in patients undergoing total hip or knee arthroplasty. J Bone Joint Surg Am .
2009;91(7):1756–1757 .
18. Goldhaber SZ , Visani L , De Rosa M . Acute pulmonary embolism: clinical outcomes in the International CooperativePulmonary Embolism Registry (ICOPER). Lancet . 1999;353(9162):1386–1389 .
19. Anderson Jr FA , Spencer FA . Risk factors for venous thromboembolism. Circulation . 2003;107(23 Suppl 1):I9–16 . 20. Kabrhel C . Achieving Multidisciplinary Collaboration for the Creation of a Pulmonary Embolism Response Team:
Creating a Team of Rivals. Semin Intervent Radiol . 2017;34(1):16–24 . 21. Auger WR , et al. Chronic thromboembolic pulmonary hypertension. Clin Chest Med . 2007;28(1):255–269 x .
22. Winter MP , Schernthaner GH , Lang IM . Chronic complications of venous thromboembolism. J Thromb Haemost .2017;15(8):1531–1540 .
23. Grosse C , Grosse A . CT findings in diseases associated with pulmonary hypertension: a current review. Radiograph-
ics . 2010;30(7):1753–1777 . 24. Lang IM , Madani M . Update on chronic thromboembolic pulmonary hypertension. Circulation . 2014;130(6):508–518 .
25. Becattini C , et al. Incidence of chronic thromboembolic pulmonary hypertension after a first episode of pulmonaryembolism. Chest . 2006;130(1):172–175 .
26. Pengo V , et al. Incidence of chronic thromboembolic pulmonary hypertension after pulmonary embolism. N Engl JMed . 2004;350(22):2257–2264 .
27. Pepke-Zaba J , et al. Chronic thromboembolic pulmonary hypertension (CTEPH): results from an international
prospective registry. Circulation . 2011;124(18):1973–1981 . 28. Jenkins D . Pulmonary endarterectomy: the potentially curative treatment for patients with chronic thromboembolic
pulmonary hypertension. Eur Respir Rev . 2015;24(136):263–271 . 29. Kahn SR , et al. Functional and Exercise Limitations After a First Episode of Pulmonary Embolism: Results of the
ELOPE Prospective Cohort Study. Chest . 2017;151(5):1058–1068 . 30. Ahmed I , Majeed A , Powell R . Heparin induced thrombocytopenia: diagnosis and management update. Postgrad Med
J . 2007;83(983):575–582 .
31. Eby CS . Warfarin-induced skin necrosis. Hematol Oncol Clin North Am . 1993;7(6):1291–1300 . 32. Borow M , Goldson HJ . Prevention of postoperative deep venous thrombosis and pulmonary emboli with combined
modalities. Am Surg . 1983;49(11):599–605 . 33. Ciuti G , et al. Incidence and characteristics of asymptomatic distal deep vein thrombosis unexpectedly found at
admission in an Internal Medicine setting. Thromb Res . 2012;130(4):591–595 . 34. Harris LM , et al. Screening for asymptomatic deep vein thrombosis in surgical intensive care patients. J Vasc Surg .
1997;26(5):764–769 .
35. Yamaguchi T , et al. Incidence and time course of asymptomatic deep vein thrombosis with fondaparinux in patientsundergoing total joint arthroplasty. Thromb Res . 2010;126(4):e323–e326 .
36. Labropoulos N , et al. The effect of venous thrombus location and extent on the development of post-thromboticsigns and symptoms. J Vasc Surg . 2008;48(2):407–412 .
37. Gabriel F , et al. Incidence of post-thrombotic syndrome and its association with various risk factors in a co-hort of Spanish patients after one year of follow-up following acute deep venous thrombosis. Thromb Haemost .
2004;92(2):328–336 .
38. Soosainathan A , et al. Scoring systems for the post-thrombotic syndrome. J Vasc Surg . 2013;57(1):254–261 . 39. Partsch H . Compression therapy of the legs. A review. J Dermatol Surg Oncol . 1991;17(10):799–805 .
40. Brandjes DP , et al. Randomised trial of effect of compression stockings in patients with symptomatic proximal-veinthrombosis. Lancet . 1997;349(9054):759–762 .
41. Baldwin MJ , et al. Post-thrombotic syndrome: a clinical review. J Thromb Haemost . 2013;11(5):795–805 . 42. Tilbrook H , et al. Aspirin for Venous Ulcers: Randomised Trial (AVURT): study protocol for a randomised controlled
trial. Trials . 2015;16:513 .
43. McCarty MF , O’Keefe JH , DiNicolantonio JJ . Pentoxifylline for vascular health: a brief review of the literature. OpenHeart . 2016;3(1) .
44. Jull AB , et al. Pentoxifylline for treating venous leg ulcers. Cochrane Database Syst Rev . 2012;12 . 45. Kahn SR , et al. Compression stockings to prevent post-thrombotic syndrome: a randomised placebo-controlled trial.
Lancet . 2014;383(9920):880–888 . 46. Galanaud JP , Righini M , Quere I . Compression stockings to prevent post-thrombotic syndrome. Lancet .
2014;384(9938):129 . 47. Enden T , et al. Long-term outcome after additional catheter-directed thrombolysis versus standard treat-
ment for acute iliofemoral deep vein thrombosis (the CaVenT study): a randomised controlled trial. Lancet .
2012;379(9810):31–38 . 48. Kahn SR , et al. The influence of venous thromboembolism on quality of life and severity of chronic venous disease.
J Thromb Haemost . 2004;2(12):2146–2151 . 49. Roberts LN , et al. Post-thrombotic syndrome is an independent determinant of health-related quality of life follow-
ing both first proximal and distal deep vein thrombosis. Haematologica . 2014;99(3):e41–e43 .
292 I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298
50. Vedantham S , et al. Pharmacomechanical Catheter-Directed Thrombolysis for Deep-Vein Thrombosis. N Engl J Med .
2017;377(23):2240–2252 . 51. Raju S , Furrh JBt , Neglen P . Diagnosis and treatment of venous lymphedema. J Vasc Surg . 2012;55(1):141–149 .
52. Bollinger A , PH , Wolfe JHN . The Initial Lymphatics . Stuttgart, New York: G Thieme; 1985 .
53. Partsch H . Pathophysiology of Veno-Lymphatic Interaction in Leg Ulcers and Oedema ; 2012 2nd Jobst® Scientific Sym-posium .
54. Blecken SR , Villavicencio JL , Kao TC . Comparison of elastic versus nonelastic compression in bilateral venous ulcers:a randomized trial. J Vasc Surg . 2005;42(6):1150–1155 .
55. Travis JA , et al. Diagnosis and treatment of paradoxical embolus. J Vasc Surg . 2001;34(5):860–865 . 56. Maron BA , Shekar PS , Goldhaber SZ . Paradoxical embolism. Circulation . 2010;122(19):1968–1972 .
57. Handke M , et al. Patent foramen ovale and cryptogenic stroke in older patients. N Engl J Med .
2007;357(22):2262–2268 . 58. Anderson Jr FA , et al. A population-based perspective of the hospital incidence and case-fatality rates of deep vein
thrombosis and pulmonary embolism. The Worcester DVT Study. Arch Intern Med . 1991;151(5):933–938 . 59. Howell MD , Geraci JM , Knowlton AA . Congestive heart failure and outpatient risk of venous thromboembolism: a
retrospective, case-control study. J Clin Epidemiol . 2001;54(8):810–816 . 60. Geerts WH , et al. Prevention of venous thromboembolism: the Seventh ACCP Conference on Antithrombotic and
Thrombolytic Therapy. Chest . 2004;126(3 Suppl):338S–400S . 61. Cassidy MR , Rosenkranz P , McAneny D . Reducing postoperative venous thromboembolism complications with a
standardized risk-stratified prophylaxis protocol and mobilization program. J Am Coll Surg . 2014;218(6):1095–1104 .
62. Geerts WH , et al. Prevention of venous thromboembolism: American College of Chest Physicians Evidence-BasedClinical Practice Guidelines (8th Edition). Chest . 2008;133(6 Suppl):381S–453S .
63. Falck-Ytter Y , et al. Prevention of VTE in orthopedic surgery patients: Antithrombotic Therapy and Preventionof Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest .
2012;141(2 Suppl):e278S–e325S . 64. Abdollahi M , Cushman M , Rosendaal FR . Obesity: risk of venous thrombosis and the interaction with coagulation
factor levels and oral contraceptive use. Thromb Haemost . 2003;89:4 93–4 98 .
65. White RH , et al. Predictors of Rehospitalization for symptomatic venous thromboembolism following total hiparthroplasty.pdf. NEJM . 20 0 0;343(24):1758–1764 .
66. Yang G , De Staercke C , Hooper WC . The effects of obesity on venous thromboembolism: A review. Open J Prev Med .2012;2(4):499–509 .
67. Ageno W , et al. Cardiovascular risk factors and venous thromboembolism: a meta-analysis. Circulation .2008;117(1):93–102 .
68. Kabrhel C , et al. Prospective study of BMI and the risk of pulmonary embolism in women. Obesity (Silver Spring) .
2009;17(11):2040–2046 . 69. Severinsen MT , et al. Anthropometry, body fat, and venous thromboembolism: a Danish follow-up study. Circulation .
2009;120(19):1850–1857 . 70. Eichinger S , et al. Overweight, obesity, and the risk of recurrent venous thromboembolism. Arch Intern Med .
2008;168(15):1678–1683 . 71. Kalantar-Zadeh K , et al. Risk factor paradox in wasting diseases. Curr Opin Clin Nutr Metab Care .
2007;10(4):433–442 .
72. Anderson Jr FA , et al. Physician practices in the management of venous thromboembolism: a community-widesurvey.[ see comment ]. Journal of Vascular Surgery . 1992;16(5):707–714 .
73. Sammama MM . Epidemiology of Risk Factors of Deep Vein Thrombosis (DVT) of the lower limbs in communitypractice. Thromb haemost . 1993;69:763 .
74. Borow M , Goldson H . Postoperative venous thrombosis. Evaluation of five methods of treatment. American Journalof Surgery . 1981;141(2):245–251 .
75. Sobreira ML , et al. Prevalence of deep vein thrombosis and pulmonary embolism in superficial thrombophlebitis of
the lower limbs: prospective study of 60 cases. Int Angiol . 20 09;28(5):40 0–408 . 76. Bezemer ID , et al. The Value of Family History as a Risk Indicator for Venous Thrombosis. Arch Intern Med .
2009;169(6):610–615 . 77. Zoller B , et al. Familial risk of venous thromboembolism in first-, second- and third-degree relatives: a nationwide
family study in Sweden. Thromb Haemost . 2013;109(3):458–463 . 78. Samama MM , et al. A comparison of enoxaparin with placebo for the prevention of venous thromboembolism
in acutely ill medical patients. Prophylaxis in Medical Patients with Enoxaparin Study Group. N Engl J Med .
1999;341(11):793–800 . 79. Heit JA , et al. Effect of a near-universal hospitalization-based prophylaxis regimen on annual number of venous
thromboembolism events in the US. Blood . 2017;130(2):109–114 . 80. Altom LK , et al. Association between Surgical Care Improvement Program venous thromboembolism measures and
postoperative events. Am J Surg . 2012;204(5):591–597 . 81. Chang V , et al. Discordance between surgical care improvement project adherence and postoperative outcomes:
implications for new Joint Commission standards. J Surg Res . 2017;212:205–213 . 82. Virchow RKL . Gessamelte Abhandlungen zur wissenschaftlichen Medizin. Frankfurt am Main Meidinger .
1856:514–515 .
83. Comerota AC . Venous Dilatation and Endothelial Damage . Phila.: WB Saunders Co; 1995:1793 . 84. Coleridge-Smith PD , Hasty JH , Scurr JH . Venous stasis and vein lumen changes during surgery.pdf. British Journal of
surgery . 1990;77:1055–1059 . 85. Butros SR , et al. Venous compression syndromes: clinical features, imaging findings and management. Br J Radiol .
2013;86(1030) .

I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298 293
86. Cassidy MR , Rosenkranz P , McAneny D . Reducing postoperative venous thromboembolism complications: in reply
to Lau and colleagues. J Am Coll Surg . 2014;219(5):1103–1104 . 87. Fennerty T . Screening for cancer in venous thromboembolic disease. BMJ . 2001;323(7315):704–705 .
88. Ay C , et al. Prediction of venous thromboembolism in cancer patients. Blood . 2010;116(24):5377–5382 .
89. Pabinger I , et al. A clinical prediction model for cancer-associated venous thromboembolism: a development andvalidation study in two independent prospective cohorts. Lancet Haematol . 2018;5(7):e289–e298 .
90. Di Nisio M , et al. Incidental venous thromboembolism in ambulatory cancer patients receiving chemotherapy.Thromb Haemost . 2010;104(5):1049–1054 .
91. Seligsohn U , Lubetsky A . Genetic susceptibility to venous thrombosis. N Engl J Med . 2001;344(16):1222–1231 . 92. Ulrych J , et al. The impact of hereditary thrombophilia on the incidence of postoperative venous thromboembolism
in colorectal cancer patients: a prospective cohort study. European Surgery . 2018 .
93. Egeberg O . Inherited Antithrombin Deficiency Causing Thrombophilia. Thromb Diath Haemorrh . 1965;13:516–530 . 94. Griffin JH , et al. Deficiency of protein C in congenital thrombotic disease. J Clin Invest . 1981;68(5):1370–1373 .
95. Comp PC , Esmon CT . Recurrent venous thromboembolism in patients with a partial deficiency of protein S. N EnglJ Med . 1984;311(24):1525–1528 .
96. Dahlback B , Carlsson M , Svensson PJ . Familial thrombophilia due to a previously unrecognized mechanism charac-terized by poor anticoagulant response to activated protein C: prediction of a cofactor to activated protein C. Proc
Natl Acad Sci U S A . 1993;90(3):1004–1008 . 97. Mahmoodi BK , et al. A prospective cohort study on the absolute risks of venous thromboembolism and predic-
tive value of screening asymptomatic relatives of patients with hereditary deficiencies of protein S, protein C or
antithrombin. J Thromb Haemost . 2010;8(6):1193–1200 . 98. Connors JM . Thrombophilia Testing and Venous Thrombosis. N Engl J Med . 2017;377(23):2298 .
99. Hill A , Kelly RJ , Hillmen P . Thrombosis in paroxysmal nocturnal hemoglobinuria. Blood . 2013;121(25):4 985–4 996quiz 5105 .
100. Hillmen P , et al. Long-term safety and efficacy of sustained eculizumab treatment in patients with paroxysmalnocturnal haemoglobinuria. Br J Haematol . 2013;162(1):62–73 .
101. Leon L , et al. Clinical significance of superficial vein thrombosis. Eur J Vasc Endovasc Surg . 2005;29(1):10–17 .
102. Schonauer V , et al. Superficial thrombophlebitis and risk for recurrent venous thromboembolism. J Vasc Surg .2003;37(4):834–838 .
103. Decousus H , et al. Recent findings in the epidemiology, diagnosis and treatment of superficial-vein thrombosis.Thromb Res . 2011(127 Suppl 3):S81–S85 .
104. Decousus H , et al. Superficial vein thrombosis: risk factors, diagnosis, and treatment. Curr Opin Pulm Med .2003;9(5):393–397 .
105. Decousus H , et al. Superficial venous thrombosis and venous thromboembolism: a large, prospective epidemiologic
study. Ann Intern Med . 2010;152(4):218–224 . 106. Husni EA , Williams WA . Superficial thrombophlebitis of lower limbs. Surgery . 1982;91(1):70–74 .
107. Lutter KS , et al. Superficial thrombophlebitis diagnosed by duplex scanning. Surgery . 1991;110(1):42–46 . 108. Decousus H , et al. Fondaparinux for the treatment of superficial-vein thrombosis in the legs. N Engl J Med .
2010;363(13):1222–1232 . 109. Gillet JL , Allaert FA , Perrin M . Superficial thrombophlebitis in non varicose veins of the lower limbs. A prospective
analysis in 42 patients. J Mal Vasc . 2004;29(5):263–272 .
110. Unno N , et al. Superficial thrombophlebitis of the lower limbs in patients with varicose veins. Surg Today .2002;32(5):397–401 .
111. Lofgren EP , Lofgren KA . The surgical treatment of superficial thrombophlebitis. Surgery . 1981;90(1):49–54 . 112. Bergqvist D , Jaroszewski H . Deep vein thrombosis in patients with superficial thrombophlebitis of the leg. Br Med J
(Clin Res Ed) . 1986;292(6521):658–659 . 113. Skillman JJ , et al. Simultaneous occurrence of superficial and deep thrombophlebitis in the lower extremity. J Vasc
Surg . 1990;11(6):818–823 discussion 823-4 .
114. Lohr JM , et al. Operative management of greater saphenous thrombophlebitis involving the saphenofemoral junc-tion. Am J Surg . 1992;164(3):269–275 .
115. Jorgensen JO , et al. The incidence of deep venous thrombosis in patients with superficial thrombophlebitis of thelower limbs. J Vasc Surg . 1993;18(1):70–73 .
116. Blumenberg RM , et al. Occult deep venous thrombosis complicating superficial thrombophlebitis. J Vasc Surg .1998;27(2):338–343 .
117. Bounameaux H , Reber-Wasem MA . Superficial thrombophlebitis and deep vein thrombosis. A controversial associa-
tion. Arch Intern Med . 1997;157(16):1822–1824 . 118. Galanaud JP , et al. Predictive factors for concurrent deep-vein thrombosis and symptomatic venous thromboembolic
recurrence in case of superficial venous thrombosis. The OPTIMEV study. Thromb Haemost . 2011;105(1):31–39 . 119. Pulliam CW , Barr SL , Ewing AB . Venous duplex scanning in the diagnosis and treatment of progressive superficial
thrombophlebitis. Ann Vasc Surg . 1991;5(2):190–195 . 120. Prountjos P , et al. Superficial venous thrombosis of the lower extremities co-existing with deep venous thrombosis.
A phlebographic study on 57 cases. Int Angiol . 1991;10(2):63–65 . 121. Murgia AP , et al. Surgical management of ascending saphenous thrombophlebitis. Int Angiol . 1999;18(4):343–347 .
122. Chengelis DL , et al. Progression of superficial venous thrombosis to deep vein thrombosis. J Vasc Surg .
1996;24(5):745–749 . 123. Quenet S , et al. Factors predictive of venous thrombotic complications in patients with isolated superficial vein
thrombosis. J Vasc Surg . 2003;38(5):944–949 . 124. Gjores JE . Surgical therapy of ascending thrombophlebitis in the saphenous system. Angiology . 1962;13:241–243 .
125. Hamdan A . Management of varicose veins and venous insufficiency. JAMA . 2012;308(24):2612–2621 . 126. Bergan JJ , et al. Chronic venous disease. N Engl J Med . 2006;355(5):4 88–4 98 .
294 I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298
127. Muller-Buhl U , et al. Varicose veins are a risk factor for deep venous thrombosis in general practice patients. Vasa .
2012;41(5):360–365 . 128. Obi AT , et al. Outcomes associated with ablation compared to combined ablation and transilluminated powered
phlebectomy in the treatment of venous varicosities. Phlebology . 2016;31(9):618–624 .
129. Konigsbrugge O , et al. Presence of varicose veins in cancer patients increases the risk for occurrence of venousthromboembolism. J Thromb Haemost . 2013;11(11):1993–20 0 0 .
130. Beebe-Dimmer JL , et al. The epidemiology of chronic venous insufficiency and varicose veins. Ann Epidemiol .2005;15(3):175–184 .
131. Immelman EJ , Jeffery PC . The postphlebitic syndrome. Pathophysiology, prevention and management. Clin ChestMed . 1984;5(3):537–550 .
132. Mosti G. Progressive or degressive compression pressure profile in patients with chronic venous disorders of the
lower limb. Veins and Lymphatics . 2014;3(1) 2014. doi: 10.4081/vl.2014.2235 . 133. Partsch, H., Compression Therapy in Venous Leg Ulcers. 2007. 77–90.
134. Lloyd-Jones D , et al. Executive summary: heart disease and stroke statistics–2010 update: a report from the Amer-ican Heart Association. Circulation . 2010;121(7):948–954 .
135. Bounds JV , et al. Mechanisms and timing of deaths from cerebral infarction. Stroke . 1981;12(4):474–477 . 136. Kelly J , et al. Venous thromboembolism after acute ischemic stroke: a prospective study using magnetic resonance
direct thrombus imaging. Stroke . 2004;35(10):2320–2325 . 137. Turpie AG , et al. Double-blind randomised trial of Org 10172 low-molecular-weight heparinoid in prevention of
deep-vein thrombosis in thrombotic stroke. Lancet . 1987;1(8532):523–526 .
138. Laporte S , et al. Clinical predictors for fatal pulmonary embolism in 15,520 patients with venous thromboembolism:findings from the Registro Informatizado de la Enfermedad TromboEmbolica venosa (RIETE) Registry. Circulation .
2008;117(13):1711–1716 . 139. Skaf E , et al. Fatal pulmonary embolism and stroke. Am J Cardiol . 2006;97(12):1776–1777 .
140. Heit JA . Venous thromboembolism epidemiology: implications for prevention and management. Semin ThrombHemost . 2002(28 Suppl 2):3–13 .
141. Jenkins EO , et al. Venous thromboembolism in malignant gliomas. J Thromb Haemost . 2010;8(2):221–227 .
142. Solem CA , et al. Venous thromboembolism in inflammatory bowel disease. Am J Gastroenterol . 2004;99(1):97–101 . 143. Talbot RW , et al. Vascular complications of inflammatory bowel disease. Mayo Clin Proc . 1986;61(2):140–145 .
144. Bernstein CN , et al. The incidence of deep venous thrombosis and pulmonary embolism among patients with in-flammatory bowel disease: a population-based cohort study. Thromb Haemost . 2001;85(3):430–434 .
145. Novacek G , et al. W1138 A Nationwide Multicenter Study On Venous Thromboembolism in Inflammatory BowelDisease. Gastroenterology . 2008;134(4):A–641 .
146. Grainge MJ , West J , Card TR . Venous thromboembolism during active disease and remission in inflammatory bowel
disease: a cohort study. Lancet . 2010;375(9715):657–663 . 147. Smeeth L , et al. Risk of deep vein thrombosis and pulmonary embolism after acute infection in a community set-
ting. Lancet . 2006;367(9516):1075–1079 . 148. Bhagat K , et al. Endothelial "stunning" following a brief exposure to endotoxin: a mechanism to link infection and
infarction? Cardiovasc Res . 1996;32(5):822–829 . 149. Schmidt M , et al. Acute infections and venous thromboembolism. J Intern Med . 2012;271(6):608–618 .
150. Rinde LB , et al. Impact of incident myocardial infarction on the risk of venous thromboembolism: the Tromso Study.
J Thromb Haemost . 2016;14(6):1183–1191 . 151. Simmons AV , Sheppard MA , Cox AF . Deep venous thrombosis after myocardial infarction. Predisposing factors. Br
Heart J . 1973;35(6):623–625 . 152. Sorensen HT , et al. Heart disease may be a risk factor for pulmonary embolism without peripheral deep venous
thrombosis. Circulation . 2011;124(13):1435–1441 . 153. Golemi I , et al. Abstract 10672: Incidence of major adverse cardiovascular events among patients with provoked
and non-provoked venous thromboembolism: a review of the riete registry. Circulation . 2018;138(Suppl_1):A10672 .
154. Kim V , et al. Risk factors for venous thromboembolism in chronic obstructive pulmonary disease. Chronic ObstrPulm Dis . 2014;1(2):239–249 .
155. Baum GL , Fisher FD . The relationship of fatal pulmonary insufficiency with cor pulmonale, rightsided mural thrombiand pulmonary emboli: a preliminary report. Am J Med Sci . 1960;240:609–612 .
156. Mitchell RS , et al. Clinical and morphologic correlations in chronic airway obstruction. Aspen Emphysema Conf .1968;9:109–123 .
157. Morgan AD , et al. COPD disease severity and the risk of venous thromboembolic events: a matched case-control
study. Int J Chron Obstruct Pulmon Dis . 2016;11:899–908 . 158. Sprunger DB , et al. Pulmonary fibrosis is associated with an elevated risk of thromboembolic disease. Eur Respir J .
2012;39(1):125–132 . 159. Beckert L , Rahman A . Pneumonia and venous thromboembolism: Is the evidence catching up with the guidelines?
Respirology . 2015;20(5):695–696 . 160. Geelen S , Bhattacharyya C , Tuomanen E . Induction of procoagulant activity on human endothelial cells by Strepto-
coccus pneumoniae. Infect Immun . 1992;60(10):4179–4183 . 161. Heumann D , et al. Gram-positive cell walls stimulate synthesis of tumor necrosis factor alpha and interleukin-6 by
human monocytes. Infect Immun . 1994;62(7):2715–2721 .
162. Riesenfeld-Orn I , et al. Production of interleukin-1 but not tumor necrosis factor by human monocytes stimulatedwith pneumococcal cell surface components. Infect Immun . 1989;57(7):1890–1893 .
163. Cabellos C , et al. Differing roles for platelet-activating factor during inflammation of the lung and subarachnoidspace. The special case of Streptococcus pneumoniae. J Clin Invest . 1992;90(2):612–618 .
164. Masrouha KZ , et al. Preoperative pneumonia and postoperative venous thrombosis: A cohort study of 427,656 pa-tients undergoing major general surgery. World J Surg . 2016;40(6):1288–1294 .

I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298 295
165. Kubota Y , et al. Lung function, respiratory symptoms and venous thromboembolism risk: the Atherosclerosis Risk
in Communities Study. J Thromb Haemost . 2016;14(12):2394–2401 . 166. Ng TM , et al. Venous thromboembolism in hospitalized patients with heart failure: incidence, prognosis, and pre-
vention. Circ Heart Fail . 2010;3(1):165–173 .
167. Mebazaa A , et al. Predicting the risk of venous thromboembolism in patients hospitalized with heart failure. Circu-lation . 2014;130(5):410–418 .
168. Haskins IN , et al. Congestive heart failure is a risk factor for venous thromboembolism in bariatric surgery. SurgObes Relat Dis . 2015;11(5):1140–1145 .
169. Golemi ISA , Pablo Juan , Diaz Quintero Luis , Torres Christian , et al. Venous thromboembolism related mortalityin patients with heart failure: Analysis of the National Inpatient Sample database. Vascular Investgiation Therapy .
2018;1(1 (Supplement)October) .
170. Lippi G , Mattiuzzi C , Franchini M . Sleep apnea and venous thromboembolism. A systematic review. Thromb Haemost .2015;114(5):958–963 .
171. Leonard J , et al. Does diabetes type increase the odds of venous thromboembolism following traumatic injury?Trauma Surg Acute Care Open . 2016;1(1) .
172. Piazza G , et al. Venous thromboembolism in patients with diabetes mellitus. Am J Med . 2012;125(7):709–716 . 173. Chung WS , Lin CL , Kao CH . Diabetes increases the risk of deep-vein thrombosis and pulmonary embolism. A pop-
ulation-based cohort study. Thromb Haemost . 2015;114(4):812–818 . 174. Zhao Z , et al. Diabetes mellitus increases the incidence of deep vein thrombosis after total knee arthroplasty. Arch
Orthop Trauma Surg . 2014;134(1):79–83 .
175. Dentali F , Squizzato A , Ageno W . The metabolic syndrome as a risk factor for venous and arterial thrombosis. SeminThromb Hemost . 2009;35(5):451–457 .
176. Ageno W , et al. The metabolic syndrome and the risk of venous thrombosis: a case-control study. J Thromb Haemost .2006;4(9):1914–1918 .
177. Ay C , et al. Venous thromboembolism–a manifestation of the metabolic syndrome. Haematologica .2007;92(3):374–380 .
178. Jang Moon Ju , W-iC , Bang Soo-Mee , Lee Taeseung , et al. Metabolic Syndrome Is Associated With Venous Throm-
boembolism in the Korean Population. Arteriosclerosis, Thrombosis, Vascular Biology . 2009;29:311–315 . 179. Huang L , Li J , Jiang Y . Association between hypertension and deep vein thrombosis after orthopedic surgery: a
meta-analysis. Eur J Med Res . 2016;21 13-13 . 180. Nifong TP , McDevitt TJ . The effect of catheter to vein ratio on blood flow rates in a simulated model of peripherally
inserted central venous catheters. Chest . 2011;140(1):48–53 . 181. Winters JP , et al. Central venous catheters and upper extremity deep vein thrombosis in medical inpatients: the
Medical Inpatients and Thrombosis (MITH) Study. J Thromb Haemost . 2015;13(12):2155–2160 .
182. Raad II , et al. The relationship between the thrombotic and infectious complications of central venous catheters.JAMA . 1994;271(13):1014–1016 .
183. Timsit JF , et al. Central vein catheter-related thrombosis in intensive care patients: incidence, risks factors, andrelationship with catheter-related sepsis. Chest . 1998;114(1):207–213 .
184. Crowley AL , et al. Venous thrombosis in patients with short- and long-term central venous catheter-associatedStaphylococcus aureus bacteremia. Crit Care Med . 2008;36(2):385–390 .
185. van Rooden CJ , et al. Infectious complications of central venous catheters increase the risk of catheter-related
thrombosis in hematology patients: a prospective study. J Clin Oncol . 2005;23(12):2655–2660 . 186. Batsis JA , Craici IM , Froehling DA . Central venous catheter thrombosis complicated by paradoxical embolism in a
patient with diabetic ketoacidosis and respiratory failure. Neurocrit Care . 2005;2(2):185–188 . 187. Venturini E , Becuzzi L , Magni L . Catheter-induced thrombosis of the superior vena cava. Case Rep Vasc Med .
2012;2012 . 188. Goldhaber SZ . Peripherally inserted central catheters: bigger is not necessarily better. Chest . 2011;140(1):6–7 .
189. Turcotte S , Dube S , Beauchamp G . Peripherally inserted central venous catheters are not superior to central venous
catheters in the acute care of surgical patients on the ward. World J Surg . 2006;30(8):1605–1619 . 190. Abelseth G , et al. Incidence of deep-vein thrombosis in patients with fractures of the lower extremity distal to the
hip. J Orthop Trauma . 1996;10(4):230–235 . 191. Buerger PM , et al. Risk of pulmonary emboli in patients with pelvic fractures. Am Surg . 1993;59(8):505–508 .
192. Geerts WH , et al. A prospective study of venous thromboembolism after major trauma. N Engl J Med .1994;331(24):1601–1606 .
193. Britt SL , et al. The impact of pelvic and lower extremity fractures on the incidence of lower extremity deep vein
thrombosis in high-risk trauma patients. Winner of the Best Paper Award from the Gold Medal Forum. Am Surg .2003;69(6):459–463 discussion 464 .
194. Ettema HB , Kollen BJ , Verheyen CC , Buller HR . Prevention of venous thromboembolism in patients with im-mobilization of the lower extremities: a meta-analysis of randomized controlled trials. J Thromb Haemost .
2008;6:1093–1098 . 195. Testroote M , et al. Low molecular weight heparin for prevention of venous thromboembolism in patients with
lower-leg immobilization. Cochrane Database Syst Rev . 2014(4) . 196. Batra S , et al. Thromboprophylaxis following cast immobilisation for lower limb injuries–survey of current practice
in United Kingdom. Injury . 2006;37(9):813–817 .
197. Scolaro JA , Taylor RM , Wigner NA . Venous thromboembolism in orthopaedic trauma. J Am Acad Orthop Surg .2015;23(1):1–6 .
198. Sems SA , et al. Incidence of deep venous thrombosis after temporary joint spanning external fixation for complexlower extremity injuries. J Trauma . 2009;66(4):1164–1166 .
199. SooHoo NF , et al. Incidence and factors predicting pulmonary embolism and deep venous thrombosis followingsurgical treatment of ankle fractures. Foot Ankle Surg . 2011;17(4):259–262 .

296 I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298
2
22
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
00. Smith EB , Parvizi J , Purtill JJ . Delayed surgery for patients with femur and hip fractures-risk of deep venous throm-
bosis. J Trauma . 2011;70(6):E113–E116 . 201. Hsu JE , et al. Is upper extremity trauma an independent risk factor for lower extremity venous thromboembolism?
An 11-year experience at a Level I trauma center. Arch Orthop Trauma Surg . 2011;131(1):27–32 .
02. Knudson MM , Ikossi DG . Venous thromboembolism after trauma. Curr Opin Crit Care . 2004;10(6):539–548 . 03. Paffrath T , et al. Venous thromboembolism after severe trauma: incidence, risk factors and outcome. Injury .
2010;41(1):97–101 . 04. Rattan R , et al. Hidden Burden of Venous Thromboembolism After Trauma: A National Analysis. J Trauma Acute Care
Surg . 2018 . 05. Gearhart MM , et al. The risk assessment profile score identifies trauma patients at risk for deep vein thrombosis.
Surgery . 20 0 0;128(4):631–640 .
06. Vachirasrisirikul S , Laohapensang K . Incidence and Risk Factors of Venous Thromboembolism Following Major Ab-dominal Surgery. J Med Assoc Thai . 2016;99(6):665–674 .
207. Vavilala MS , et al. Risk factors for venous thromboembolism in pediatric trauma. J Trauma . 2002;52(5):922–927 . 08. Teasell RW, HT Aubut JL, et al. Venous Thromboembolism Following Spinal Cord Injury. Archives of physical medicine
and rehabilitation . 2009;90(2):232–245. doi: 10.1016/j.apmr.2008.09.557 . 09. Chiou-Tan FY , et al. Comparison of dalteparin and enoxaparin for deep venous thrombosis prophylaxis in patients
with spinal cord injury. Am J Phys Med Rehabil . 2003;82(9):678–685 . 210. Piran S , Schulman S . Incidence and risk factors for venous thromboembolism in patients with acute spinal cord
injury: A retrospective study. Thromb Res . 2016;147:97–101 .
211. . Prevention of Venous Thromboembolism in Individuals with Spinal Cord Injury: Clinical Practice Guidelines for HealthCare Providers, 3rd ed.: Consortium for Spinal Cord Medicine. Top Spinal Cord Inj Rehabil . 2016;22(3):209–240 .
212. Pomp ER , et al. Pregnancy, the postpartum period and prothrombotic defects: risk of venous thrombosis in theMEGA study. J Thromb Haemost . 2008;6(4):632–637 .
213. Heit JA , et al. Trends in the incidence of venous thromboembolism during pregnancy or postpartum: a 30-yearpopulation-based study. Ann Intern Med . 2005;143(10):697–706 .
214. Gherman RB , et al. Incidence, clinical characteristics, and timing of objectively diagnosed venous thromboembolism
during pregnancy. Obstet Gynecol . 1999;94(5 Pt 1):730–734 . 215. Ginsberg JS , et al. Venous thrombosis during pregnancy: leg and trimester of presentation. Thromb Haemost .
1992;67(5):519–520 . 216. Pabinger I , et al. Temporary increase in the risk for recurrence during pregnancy in women with a history of venous
thromboembolism. Blood . 20 02;10 0(3):1060–1062 . 217. Sultan AA , et al. Risk factors for first venous thromboembolism around pregnancy: a population-based cohort study
from the United Kingdom. Blood . 2013;121(19):3953–3961 .
218. Wilcox AJ , et al. Incidence of early loss of pregnancy. N Engl J Med . 1988;319(4):189–194 . 219. Clark DA , et al. Unexplained sporadic and recurrent miscarrage in the new millennium: a critical analysis of im-
mune mechanisms and treatments. Hum Reprod Update . 2001;7(5):501–511 . 20. Stephenson M , Kutteh W . Evaluation and management of recurrent early pregnancy loss. Clin Obstet Gynecol .
2007;50(1):132–145 . 221. Rai R , Regan L . Recurrent miscarriage. Lancet . 2006;368(9535):601–611 .
22. Robertson L , et al. Thrombophilia in pregnancy: a systematic review. Br J Haematol . 2006;132(2):171–196 .
23. Tchaikovski SN , Rosing J . Mechanisms of estrogen-induced venous thromboembolism. Thromb Res .2010;126(1):5–11 .
224. van Hylckama Vlieg A , et al. The venous thrombotic risk of oral contraceptives, effects of oestrogen dose and pro-gestogen type: results of the MEGA case-control study. BMJ . 2009;339:b2921 .
25. Tepper NK , et al. Progestin-only contraception and thromboembolism: A systematic review. Contraception .2016;94(6):678–700 .
26. Olie V , et al. Hormone therapy and recurrence of venous thromboembolism among postmenopausal women.
Menopause . 2011;18(5):4 88–4 93 . 227. Hernandez RK , et al. Tamoxifen treatment and risk of deep venous thrombosis and pulmonary embolism: a Danish
population-based cohort study. Cancer . 2009;115(19):4 4 42–4 4 49 . 28. Cohen AT , et al. Venous thromboembolism risk and prophylaxis in the acute hospital care setting (ENDORSE study):
a multinational cross-sectional study. Lancet . 2008;371(9610):387–394 . 29. Catterick D , Hunt BJ . Impact of the national venous thromboembolism risk assessment tool in secondary care in
England: retrospective population-based database study. Blood Coagul Fibrinolysis . 2014;25(6):571–576 .
30. Caprini JA . Thrombosis risk assessment as a guide to quality patient care. Dis Mon . 2005;51(2-3):70–78 . 231. Pannucci CJ , et al. Individualized venous thromboembolism risk stratification using the 2005 Caprini score to iden-
tify the benefits and harms of chemoprophylaxis in surgical patients: a meta-analysis. Ann Surg . 2017 . 32. Paz Rios LH , et al. Validation of a patient-completed Caprini risk assessment tool for Spanish, Arabic, and Polish
Speakers. Clin Appl Thromb Hemost . 2018;24(3):502–512 . 233. Sheils CR , et al. Evaluation of hospitals participating in the American College of Surgeons National Surgical Quality
improvement program. Surgery . 2016;160(5):1182–1188 . 34. Pannucci CJ , Fleming KI . Comparison of face-to-face interaction and the electronic medical record for venous throm-
boembolism risk stratification using the 2005 Caprini score. J Vasc Surg Venous Lymphat Disord . 2018;6(3):304–311 .
235. Amin AN , Girard F , Samama MM . Does ambulation modify venous thromboembolism risk in acutely ill medicalpatients? Thromb Haemost . 2010;104(5):955–961 .
36. Hull RD . Relevance of immobility and importance of risk assessment management for medically ill patients. ClinAppl Thromb Hemost . 2013;19(3):268–276 .
237. Nokes TJ , Keenan J . Thromboprophylaxis in patients with lower limb immobilisation - review of current status. BrJ Haematol . 2009;146(4):361–368 .
I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298 297
238. Roach RE , et al. The risk of venous thrombosis in individuals with a history of superficial vein thrombosis and
acquired venous thrombotic risk factors. Blood . 2013;122(26):4264–4269 . 239. Shen Y-MP , Frenkel EP . Thrombosis and a hypercoagulable state in HIV-infected patients. Clin Appl Thrombo-
sis/Hemostasis . 2004;10(3):277–280 .
240. Barsoum MK , et al. Is progestin an independent risk factor for incident venous thromboembolism? A popula-tion-based case-control study. Thromb Res . 2010;126(5):373–378 .
241. Greer IA . Thrombophilia: implications for pregnancy outcome. Thromb Res . 2003;109(2-3):73–81 . 242. Sweetland S , et al. Smoking, surgery, and venous thromboembolism risk in women: United Kingdom cohort study.
Circulation . 2013;127(12):1276–1282 . 243. Stein PD , Beemath A , Olson RE . Obesity as a risk factor in venous thromboembolism. Am J Med .
2005;118(9):978–980 .
244. Merkow RP , et al. Effect of body mass index on short-term outcomes after colectomy for cancer. J Am Coll Surg .2009;208(1):53–61 .
245. Simanek R , et al. High platelet count associated with venous thromboembolism in cancer patients: results from theVienna Cancer and Thrombosis Study (CATS). J Thromb Haemost . 2010;8(1):114–120 .
246. Spinella PC , et al. Duration of red blood cell storage is associated with increased incidence of deep vein thrombosisand in hospital mortality in patients with traumatic injuries. Crit Care . 2009;13(5):R151 .
247. Bahl V , et al. A validation study of a retrospective venous thromboembolism risk scoring method. Ann Surg .2010;251(2):344–350 .
248. Pannucci CJ , et al. Postoperative enoxaparin prevents symptomatic venous thromboembolism in high-risk plastic
surgery patients. Plast Reconstr Surg . 2011;128(5):1093–1103 . 249. Gould MK , et al. Prevention of VTE in nonorthopedic surgical patients: Antithrombotic Therapy and Prevention
of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest .2012;141(2 Suppl):e227S–e277S .
250. Leonardi MJ , McGory ML , Ko CY . The rate of bleeding complications after pharmacologic deep venous thrombosisprophylaxis. Arch Surg . 2006;141:790–799 .
251. Zhang XQ , et al. [Validity of Caprini Risk Assessment Scale for Assessing Risk of Venous Thromboembolism in
Hospitalized Critically Ill Patients]. Sichuan Da Xue Xue Bao Yi Xue Ban . 2015;46(5):732–735 . 252. Yarlagadda BB , et al. Venous thromboembolism in otolaryngology surgical inpatients receiving chemoprophylaxis.
Head Neck . 2014;36(8):1087–1093 . 253. Shuman AG , et al. Stratifying the risk of venous thromboembolism in otolaryngology. Otolaryngol Head Neck Surg .
2012;146(5):719–724 . 254. Hachey KJ , et al. Caprini venous thromboembolism risk assessment permits selection for postdischarge prophylactic
anticoagulation in patients with resectable lung cancer. J Thorac Cardiovasc Surg . 2016;151(1):37–44 e1 .
255. Sterbling HM , et al. Caprini Risk Model Decreases Venous Thromboembolism Rates in Thoracic Surgery CancerPatients. Ann Thorac Surg . 2018;105(3):879–885 .
256. Luksameearunothai K , et al. Usefulness of clinical predictors for preoperative screening of deep vein thrombosis inhip fractures. BMC Musculoskelet Disord . 2017;18(1):208 .
257. Kraus ES , et al. Implementation and Validation of the 2013 Caprini Score for Risk Stratification of ArthroplastyPatients in the Prevention]of Venous Thrombosis. Clin Appl Thromb Hemost . 2018:2019 In press .
258. Zhou HX , et al. Validation of the Caprini risk assessment model in Chinese hospitalized patients with venous
thromboembolism. Thromb Res . 2012;130(5):735–740 . 259. Zhou H , et al. Assessment of the Risk of Venous Thromboembolism in Medical Inpatients using the Padua Prediction
Score and Caprini Risk Assessment Model. J Atheroscler Thromb . 2018;25(11):1091–1104 . 260. Taha H , et al. Improving venous thromboembolism risk assessment compliance using the electronic tool in admitted
medical patients. BMJ Qual Improv Rep . 2015;4(1) . 261. Liu X , et al. Comparison between Caprini and Padua risk assessment models for hospitalized medical patients at
risk for venous thromboembolism: a retrospective study. Interact Cardiovasc Thorac Surg . 2016;23(4):538–543 .
262. Grant PJ , et al. Assessing the Caprini Score for Risk Assessment of Venous Thromboembolism in Hospitalized Med-ical Patients. Am J Med . 2016;129(5):528–535 .
263. Chen X , et al. Risk Assessment in Chinese Hospitalized Patients Comparing the Padua and Caprini Scoring Algo-rithms. Clin Appl Thromb Hemost . 2018 1076029618797465 .
264. Lukaszuk RF , et al. The comparison between Caprini and Padua VTE risk assessment models for hospitalised cancerpatients undergoing chemotherapy at the tertiary oncology department in Poland: is pharmacological thrombopro-
phylaxis overused? Contemp Oncol (Pozn) . 2018;22(1):31–36 .
265. Zhai Z , et al. VTE Risk Profiles and Prophylaxis in Medical and Surgical Inpatients: The Identification of ChineseHospitalized Patients’ Risk Profile for Venous Thromboembolism (DissolVE-2)-A Cross-sectional Study. Chest . 2018 .
266. Al-Ogaili A , et al. Venous Thromboembolism Risk Stratification: The Missing Link in Hospitalized Patients. JAtheroscler Thromb . 2018;25(11):1087–1088 .
267. Schunemann HJ , Cushman M , et al. American Society of Hematology 2018 guidelines for management of ve-nous thromboembolism- prophylaxis for hospitalized and nonhospitalized medical patients. Blood Advances .
2018;2:3198–3225 . 268. Kakkar VV . Prevention of fatal postoperative pulmonary embolism by low doses of heparin. An international mul-
ticentre trial. Lancet . 1975;2(7924):45–51 .
269. Collins R , et al. Reduction in fatal pulmonary embolism and venous thrombosis by perioperative administration ofsubcutaneous heparin. Overview of results of randomized trials in general, orthopedic, and urologic surgery. New
England Journal of Medicine . 1988;318(18):1162–1173 . 270. Haas S , et al. Prevention of fatal pulmonary embolism and mortality in surgical patients: a randomized double-blind
comparison of LMWH with unfractionated heparin. Thrombosis & Haemostasis . 2005;94(4):814–819 .
298 I. Golemi, J.P. Salazar Adum and A. Tafur et al. / Disease-a-Month 65 (2019) 249–298
271. Gould MK , et al. Prevention of VTE in Nonorthopedic Surgical Patients. Antithrombotic Therapy and Prevention
of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. CHEST .2012;141(2) Supp(supp):e227–e277 .
272. Bratzler DW , Hunt DR . The Surgical Infection Prevention and Surgical Care Improvement Projects. Clinical Infectious
Diseases . 2006;43:322–330 . 273. Rasouli MR , et al. Surgical care improvement project (SCIP): has its mission succeeded? J Arthroplasty .
2013;28(7):1072–1075 . 274. Arcelus JI , et al. Clinical presentation and time-course of postoperative venous thromboembolism: Results from the
RIETE Registry. Thromb Haemost . 2008;99:546–551 . 275. Geerts WH , Pineo GF , Heit JA . Prevention of venous thromboembolism: the Eighth ACCP Conference on Antithrom-
botic and Thrombolytic Therapy. Chest . 2008;133:381S–453S .
276. Rasmussen MS , Jorgensen LN , Jorgensen PW . Prolonged thromboprophylaxis with Low MolecularWeight heparin forabdominal or pelvic surgery (Review). Cochrane Database of Systemic Reviews . 2009(1):1–17 .