Venous thromboembolism in pregnancy - sfai.se...2018/05/02 · Prof Beverley Hunt, Guy’s & St...
53
Prof Beverley Hunt, Guy’s & St Thomas’ NHS Foundation Trust Kings College, London Medical Director of Thrombosis UK Twitter @bhwords Venous thromboembolism in pregnancy
Transcript of Venous thromboembolism in pregnancy - sfai.se...2018/05/02 · Prof Beverley Hunt, Guy’s & St...

Prof Beverley Hunt, Guy’s & St Thomas’ NHS Foundation Trust
Kings College, LondonMedical Director of Thrombosis UK
Twitter @bhwords
Venous thromboembolism in pregnancy


VTE in pregnancy
VTE in 1/1000 pregnancies
>70% of DVT in left side
>70% ileofemoral
>70% post-phlebitic syndrome
How to diagnose?
How to treat?
How to prevent?

Pregnancy is a prothrombotic state
Increased venous stasis
Endothelial changes
Hypercoagulable changes
• Increased levels of fibrinogen, Factor Vc, Factor VIIIc and vWF*
• Reduced levels of total and free Protein S• Activated Protein C sensitivity ratio falls• Increased levels of PAI-1 and PAI-2 from placenta†
• Gradual increase in Prothrombin Factor 1 +2, TAT‡ and D-dimers
• Persist for up to 6 weeks post-partum
*vWF = von Willebrand Factor; †PAI = plasminogen activator inhibitor; ‡TAT = thrombin antithrombin



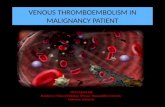
Distribution of VTE in pregnancy & puerperium
Jacobsen et al. Am J Obstet Gynecol 2008;198(2):233.e1–7
49.3% of VTE occurred during the first 6 weeks
postpartum
VTE incidence:1st trimester: 10.1%2nd trimester: 10.4%3rd trimester: 28.4%
12 24 36 1 6 12
VTE
(n)
0102030405060708090
Antepartum PostpartumWeeks Delivery

Rate of venous thromboembolism per 100 000 person years by weeks after discharge during antepartum period: 12 events in weeks 1-2 after discharge, 7 events in weeks 3-4
after discharge, and 12 events in weeks 5-10 after discharge.
Sultan A et al. BMJ 2013;347:bmj.f6099©2013 by British Medical Journal Publishing Group
HOSPITAL ACQUIRED VTE & PREGNANCY

Weeks Postpartum
VTEOR
95% CI
0-6 12.1 7.9 to 18.6
7-12 2.2 1.4 to 3.3
13-18 1.6 1.0 to 2.5
18-24 0.9 0.5 to 1.4
Kamel et al New Engl J Med Feb 2014

Treatment
Prevention
The RCOG guidelines

Sharp and statistically significant fall in mortality rate: 1.94 (95% CI 1.43-2.63) per 100,000 maternities 2003-5
0.79 (95% CI 0.49-1.25 ) per 100,000 maternities 2006-8.
Thrombosis & thromboembolismMortality rates 1985-87 to 2006-08
RCOG Thromboprophylaxis Guideline 2004 (an + post vd)
RCOG Working Party thromboprophylaxis gynaecology and obstetrics. 1995 (post CS)

Risk factor for VTE aOR 95% CIPrevious VTE 1 24.8 17.1-36
Age > 35 4 1.3 1.0-1.7
BMI > 30 21
5.34.4
2.1-13.53.4-5.7
Smoking 3 2.7 1.5-4.9Parity >3 4 2.4 1.8-3.1
Medical Conditions1
Sickle cell disease, SLE, Heart disease, anaemia, infection, Hyperemesis
2.0 – 8.7
2.51 2.0-3.2Immobility 3 7.7 (an)
10.8 (pn)3.2-194-28.8
Pre-eclampsia3
+Fetal Growth Restricition3.15.8
1.8-5.32.1-16
ART 3 4.3 2.0-9.4
Twins3 2.6 1.1-6.2
APH 1 2.3 1.8-2.8
PPH 3 4.1 2.3-7.3
Caesarean section 4 3.6 3.0-4.3
Varicose veins 2.4 1.04-5.4
Transfusion1 7.6 6.2-9.4
1.James et al 2006; 2.Larsen et al 2007; 3.Jacobsen et al 2008; 4.Lindqvist et al 1999
Any woman with THREE or more (TWO or more if admitted) current or persisting risk factors should receive prophylactic LMWH antenatally.
Any woman with TWO or more current or persisting risk factors should receive prophylactic LMWH postpartum.

Graduated compression stockings
Only 1,000 patients in clinical trials
Never shown to reduce the risk of death due to PE
The CLOT study Dennis M et al, Lancet 2009; 373: 19582,500 stroke ptsThigh length anti-embolic stockings v nothing10% v 9.5% VTE rate on USS BUT5% with stockings had skin problems
Do not offer stockings to patients who have:Suspected peripheral arterial diseasePeripheral arterial bypass graftingPeripheral neuropathy or other causes of sensory impairmentAny local condition in which stockings may cause damageKnown allergy to material of manufactureCardiac failure/severe leg oedemaUnusual leg size or shapeIf arterial disease suspected seek expert opinionEncourage them to wear them day and night until they no longer have reduced mobilityRemove daily for hygiene purposes and to inspect skin 2-3 times a day for integrity or sensory impairment and discontinue if problems develop.

GAPS: Graduated compression as an Adjunct to Pharmacoprophylaxis
in Surgery
3,250 moderate risk surgical patients receive LMWH +/-stockings
Primary outcome: symptomatic & asymptomatic vTE

Page 15
National register-based cohort study, 1995 to 2005.All Danish pregnancies conceived by IVF (n = 18 787)48 cases VTE
VTE incidence- 3 fold increase in pregnancies after IVF; especially in the first trimester and in the first 6 weeks post-partum.

Cumulative incidence of VTE in the puerperal period in IVF pregnancies, and reference pregnancies.
Hansen A et al. Hum. Reprod. 2014;29:611-617
© The Author 2014. Published by Oxford University Press on behalf of the European Society of Human Reproduction and Embryology. All rights reserved. For Permissions, please email: [email protected]

Difficulties in diagnosing VTE in pregnancy:
Wells score and D-dimer not validated in pregnancy
Non-thrombotic causes of symptoms such as leg swelling and shortness of breath are common in pregnancy
“Maintain a low threshold for performing objective testing”

Systemic review & meta-analysis of pregnant patients referred for suspected PE to Emergency
Kline et al, Academic Emergency Medicine 2014;21:949-59
Identified 17 studies with 25,339 patients
506 were pregnant 4.1% positive imaging
Non-pregnant – 12.4% positive
Conclusion: In the ED setting physicians test for PE in pregnant pts at a low threshold, resulting in a low rate of VTE diagnosis.

11 studies of poor quality looking at 1300+ pregnant women
Scanning with either CTPA or V/Q appeared to be appropriate for excluding PE in pregnancy, but comparative studies necessary
But they noted:
Only 3% of all women scanned had a PE
Cochrane review: scanning imaging techniques for the exclusion of PE in pregnancy
van Mens et al Jan 2017

Radiation doses for diagnosing PE in pregnancy
CTPA V only V/QEffe
Effective dose 21 mSiv 1.04 1.29
Breast absorbed 44 mGy 0.28 0.37
Uterus absorbed 0.48 mGy 0.25 0.40
Some authorities say risk of breast cancer increases by 10% if CTPA used in fertile women
From Detection of pulmonary embolism during pregnancy:comparing radiation doses of CTPA and pulmonary
scintigraphy.Astani et al. Nucl Med comm 2014;35: 704

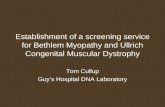
V/Q SPECT – how it works
Camera head rotates around patient

CT VQSPECT
Roach et al Seminars Nuclear Medicine 2010:40:455-466
Co-registered CTPA/perfusion SPECT showing perfusion defects corresponding with bilateral PE
14

Head to Head: VQ SPECT & CTPA in suspected PE
Reinharz: JNM 2004: 45: 1501-8
n Sensitivity Specificity
VQ SPECT 81 97% 91%CTPA 4-slice 81 86% 98%
Gutte JNM 2009:50: 1987-92
n Sensitivity Specificity
VQ SPECT 81 97% 88%CTPA 16-slice 81 68% 100%
V/Q SPECT plus low dose CT raised specificity to 100% (Gutte et al, 2009)
5

Difficulties in diagnosing PE in pregnancyDiPEP: Diagnosis of Pulmonary Embolism (PE) in
Pregnancy
ISRCTN: 21245595
REC ref: 14/LO/1695
HTA ref: 13/21/01
This project is funded by the National Institute for Health Research Health Technology Assessment Programme (13/21/01)
The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the Health Technology Assessment Programme, NIHR, NHS or the Department of Health.

Aims
Develop new rule to select pregnant or postpartum women with suspected PE for imaging
Estimate the diagnostic accuracy of expert-derived clinical decision rules
Test existing Clinical Decision Rules (Wells, Geneva, PERC) in a pregnant population used for a non-pregnant population
Explore the diagnostic value of biomarkers
DiPEP study

Design: Multicentre, case-control design in the UK
Suspected PE- Prospective data collection (n=250), across from 11 NHS Trusts
Diagnosed PE- UK-wide Obstetric Surveillance System (UKOSS), retrospective data collection (n=150)
Inclusion criteria: Pregnant and Postpartum women (42 days) requiring diagnostic imaging for PE.
Exclusion Criteria: women with PE diagnosed as an incidental finding, requiring life support at presentation, diagnosed with PE earlier in the current pregnancy, aged <16 years, unable to give informed consent, previously recruited to the study
Data Collection: Standard clinical assessment, potential predictor variables, diagnostic test results and management
Suspected PE: Blood sample, 30 day follow up (medical records and patient questionnaire
Methods

No blood sample for UKOSS (cases) as consent cannot be obtained retrospectively.
We anticipated that only a small number (~5) of those with suspected PE would actually have PE.
To increase statistical power to estimate sensitivity of biomarkers, data collection and blood sample collected on pregnant and postpartum women diagnosed with DVT (~20)
Reference standard classification
All Suspected PE and Diagnosed PE classified as PE present or PE absent based on the results of diagnostic imaging, thromboembolic events, evidence of treatment for PE, and adverse events
Two independent assessors (and 3rd adjudicator), blind to clinical predictors and blood results
Methods cont.

Planned analyses
D-Dimers (ELISA)D-dimers (Innovance)Plasmin-antiplasmin assay (PAP)
Prothrombin fragment 1+2 (PF 1 +2)
Thrombin GenerationProthrombin time (PT)Activated partial thromboplastin time (APTT)Clauss FibrinogenSoluble Tissue Factor (sTF)Troponin IB-type natriuretic peptideC- Reactive Protein (CRP)MRproAMP
Biomarkers; Existing CDR’s;
Simplified Geneva ScoreWellsPERC
The accuracy of each index test was assessed by reporting and comparing the sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV). The combined sensitivity and specificity was assessed plotting Receiver Operating Characteristic (ROC) curves
(LASSO) regression modelling, recursive partitioning to create data derived rulePerformance of consensus derived CDR

Recruitment period: February 2015- September 2016
Recruitment totals
Suspected PE n= 324
Diagnosed PE n= 198
Diagnosed DVT n=18
Primary analysis classifications
PE- 181
No PE- 259
Exclude- 82
Biomarkers data;
Women who received anticoagulation prior to blood sampling (n=240) have APTT and ETP results removed
Results
Figure 1: Suspected PE recruitment

Heart rate

Respiratory rate

Oxygen saturation

Performance of existing rules
Score AUCPERC 0.586Simplified Revised Geneva 0.514
Wells 0.525

Biomarkers

Marker False -ve
False +ve
True -ve
True +ve Sensitivity Specificity PPV NPV FPR FNR FDR Accuracy
Clauss Fibrinogen 18 0 241 0 0 1 0 0.931 0 1 0 0.931D-Dimer (ELISA) 16 8 237 2 0.111 0.967 0.2 0.937 0.033 0.889 0.8 0.909D-Dimer (Innovan) 16 6 239 2 0.111 0.976 0.25 0.937 0.024 0.889 0.75 0.916Plasmin (Antiplasmin) 16 5 240 2 0.111 0.98 0.286 0.938 0.02 0.889 0.714 0.92
Soluble Tissue Factor 18 0 245 0 0 1 0 0.932 0 1 0 0.932
Troponin 18 0 247 0 0 1 0 0.932 0 1 0 0.932Aprothombin 3 0 60 0 0 1 0 0.952 0 1 0 0.952Prothombin (Time) 18 1 236 0 0 0.996 0 0.929 0.004 1 1 0.925Prothombin Fragments 18 0 245 0 0 1 0 0.932 0 1 0 0.932
Thrombin Generation (Endogenous Potential)
3 0 60 0 0 1 0 0.952 0 1 0 0.952
Thrombin Generation (Lag Time)
3 0 60 0 0 1 0 0.952 0 1 0 0.952
Thrombin Generation (Peak) 3 0 60 0 0 1 0 0.952 0 1 0 0.952
Thrombin Generation (Time to Peak)
3 0 60 0 0 1 0 0.952 0 1 0 0.952

D-dimer (ELISA) and (Innovance)

D-dimer ELISA values according to gestation

:
Clinical prediction scores used outside of pregnancy are NOT suitable in pregnancy
Single biomarkers are not helpful in diagnosing or excluding PE in pregnancy
Conclusion

DiPEP Thank you!
Barts Health NHS Trust
Bolton NHS Foundation Trust
Bradford Teaching Hospitals NHS Foundation Trust
Hull and East Yorkshire Hospitals NHS Trust
The Leeds Teaching Hospitals NHS Trust
Central Manchester University Hospitals NHS Foundation Trust
We would like to extend our thanks to the following sites:
Nottingham University Hospitals NHS Trust
Portsmouth Hospitals NHS Trust
Royal Berkshire NHS Foundation Trust
Sheffield Teaching Hospitals NHS Foundation Trust
Guy’s and St Thomas’ NHS Foundation Trust

Why are we not using MR direct thrombus imaging to diagnose DVT in pregnancy? Moody A et al
MR direct thrombus imaging in comparison to venography in imaging DVT
N. BDoppler ultrasound:Operator dependentPoor in calf & pelvis

Fetal risks of coumarins in pregnancy
Teratogenic 1–2% risk of: Hare lip and cleft palateBone abnormalities
Between 6-14 weeks
Risk of fetal haemorrhagein 2nd and 3rd trimesters due to hepatic immaturity
Risk greatest if maternal dose > 5mgs
BUT coumarins remain the preferred option in women with mechanical valves and previous catastrophic or cerebral antiphospholipid syndrome

Fetal risks of DOACs in pregnancy
Unknown effects in humans
What to do if require long term anticoagulation & want to get pregnant?
ISTH recommendation-switch to warfarin preconceptually
BUT
Switching from unknown fetal risk to known fetal risk!
Switch to LMWH?
Stay on DOAC & switch as soonas pregnant

In pregnancy: use LMWH in preference to UFH
At least equivalent efficacyMore practical
Longer half-life than UFHReliable pharmacokinentics compared with UFH
Better safety……

Safety and efficacy of LMW heparins in pregnancyC Nelson Piercy, I Greer, Blood 2005; 106: 401
• 2,777 pregnancies included in a systematic review.174 patients for VTE, 2603 for thromboprophylaxis or adverse
pregnancy outcome• No maternal deaths
• Recurrent VTE and arterial thrombosis in 0.86% and 0.5%• Bleeding in 1.98%, allergic skin reaction in 1.8%• No cases of HITT
• Osteoporotic fracture in 0.04%• Live births in 94%

Current problems with LMWHs during pregnancy
LMWHs are still unlicensed for use in pregnancy
Dosing
Monitoring
Regional anaesthesia
Formulation

LMW heparin dosing in pregnancy
In treatment of VTE practice has been dictated by experience outside of pregnancy but pharmacokinetics are different due to improved renal function
e.g. enoxaparin 1 mg/kg b.i.d. vs 1.5 mg/kg in non-parous women
Lessons from surveys: Voke et al Brit J Haem 2007; 139: 545-58
126 antenatal VTE events
Once daily LMWH in 66%, twice daily in 31%
Outcomes- no recurrences, no deaths
? Can one reduce the dose to an intermediate dose after 6-8 weeks?
Continue for 6 weeks post-partum/switch to a vitamin K antagonist

Should LMW heparin be monitored in pregnancy?
LMWH has reliable pharmacokinetics unlike UF heparin and warfarin.
Studies would suggest this is true in pregnancy.
What is the target value?
Ultimately efficacy should be judged by clinical outcome studies NOT anti-Xa levels attained
…and does monitoring anti-Xa levels produce a reliable results?

LMWH (S01/10) u/ml

Regional anaesthesia, anticoagulants and pregnancy
Risk of spinal or epidural haematomas described in elderly with intermediate dose LMWH
Full anticoagulation is an absolute contraindication
Proceed if:
• Last dose of LMWH 24 hours prior to procedure and
• Normal clotting screen and platelet count >75x109/L

LMWH: Preservatives & supply
Tinzaparin (syringes): none
(multi-dose vial): benzyl alcohol
(20,000iu/ml) : Na metabisulphite [stabiliser]
Dalteparin (syringes): none
(multi-dose vial): benzyl alcohol
Other problems: previous USA alert on degree of sulphation
intermittent supply

Other agents for treatment of VTE in pregnancy
UFH (need larger doses than non-parous)Danaparoid — monitor with anti-Xa levels, safe to breastfeed
(few reports)Recombinant hirudin- case report in pregnancy, no adverse
outcomeFondaparinux — minor transplancental passageDOACs –direct oral anticoagulants — little human dataIVC filters — temporary or permanent – only necessary if
recent DVTEmergency thromboembolectomy

Post thrombotic syndrome70% have post thrombotic syndrome after iliofemoral
DVT- We are entering a new age of endovascular
management of post- thrombotic syndrome- watch this space!!
Management in future pregnancies?
The aftermath Page 52

Still a major modern problem in pregnancy
Can we find better diagnostic tools to reduce the exposure to radiation?
LMWH is here to stay – can there be more trials?
Ultimately prevention is better than treatment…..
VTE in pregnancy Page 53