Use of Intravenous Mannitol in Postperfusion …circ.ahajournals.org/content/27/4/699.full.pdfUse of...
7
Use of Intravenous Mannitol in Postperfusion Oliguria-Anuria By SAFUiI ATTAR, M.D., FRANCIS J. BORGES, M.D., R. ADAMS COWLEY, M.D., WILLIAM G. ESmOND, M.D., NORAIAN HOLLINGSWORTH, M.D., AND EMIL BLAIR, M.D. PREVIOUS EXPERIENCE indicates that renal failure following cardiopulmonary bypass caan lead to morbidity and mortality. Doberneek and associates' have indicated that a satisfactory techniieal operative procedure may be nullified by acute renal failure. These authors report the incideniee of acute renal failure after open-heart operation using ex- tracorporeal circulation as 3 per cent in a thousand patienits. There was an associated mortality of 86.7 per cent in 30 patients ex- perieneing postperfusion oliguria, azotemia, and hyperkalemia. In order to evaluate our experience with renal failure followinog cardiopulmonary by- pass, and the influence of intravenous man- nitol on oliguria-anuria experienced during this procedure, the following investigation was carried out. Methods To date, we have performled 158 open-heart pro- cedures for repair of congenital and acquired car- diac lesions. Of these, 33 patients had associated deep hypothermia (10 to 22 C.), with and without complete circulatory occlusion. The remaining 125 patients had moderate hvpothermia (30 to 32 C.) throughout the bypass procedure. A disposable disk oxygenator-heat exchanger system and 360- degree spring-loaded pumllp were used.2 No specific preoperative preparations or evalu- ation of renal function were undertaken other than routine urinalysis and measurem-tent of blood urea nitrogen (BUN) and seruni electrolytes. All pa- tients were in the usual preoperative fasting state, begun at midnight prior to operation. Anesthesia was iniduced by sodium pentothal and mlaintained in most instances with nitrous oxide and oxygen, fluothane (0.5 to 1 per cent), and suceinyleholine. From the Departments of Surgery, Medicine, and Aniesthesiology, University of Maryland School of Medicine, Baltimore, Maryland. Supported by U. S. Public Health Service Grant 5348 and U. S. Army Research and Development Grant DA-49-007-MD-674. Circulation, Volume XXVII, April 1963 In adults, a Foley catheter was inserted prior to anesthesia; children were catheterized imme- diately after induction of anesthesia. The rate of urine flow was monitored by continuous collection of urine in a graduated cylinder. In the early phase of the study, the urinary flow during the entire operation was collected as a single specimien. Because of the occurrence of oliguria during the operation, we began ilonitoring the urine flow at 15-i minute intervals throughout the entire operative procedure (fig. 1). In all instances, postoperative urinary flow was monitored at hourly intervals. All patients who developed oliguria, defined here as 0.25 ml./i mm. (360 ml./day) or less for two hours or longer, received a priming dose of 50 ml. of 20 per cent mannitol (10 Gm.). If urine flow did not increase within 30 minutes, a second dose of 10 Gm. was administered. If no response was ob- tained within an hour, no further mannitol was administered. When urine flow increased to 0.5 ml./nmin. or more, mannitol infusion was titrated against urine flow to mlaintain urinary flow at approximiiately 1 nml./min. Administration of 20 per cent intravenous miiannitol at 0.5 to 1 ml./min. was usually adequate to provide a urinary flow of 1 to 1.5 ml./min. In no instance was more than 140 Gm. of mannitol administered in 24 hours. Amounts beyond 200 Gm. in 24 hours are not ree- omniended because of the possibility of producing circulatory overload, clinical symptomiis resemiibling water intoxication, hyponatreiimia, or irreversible renal tubular damage. In this study, we have applied the principle of acute functional renal failure as proposed by Barry.3 Barry defines acute renal failure as the suddeni inability of the kidneys to vary urinary vol- umire and content appropriately in response to homeostatic needs. He classifies it into two major parts: functional renal failure, which is precipi- tated by extrarenal factors and is immediately reversible by arresting the renal action of these factors, since no organic lesions are present; and organic renal failure, which may be preceded by functional failure, but is not inmmnediately reversi- ble by arresting action of the extrarenal precipi- tating factors. Renal failure is maintained by organic renal lesions. Barry suggests that mannitol infusion nmay prevent the progression of func- tional to total organic failure. 699 by guest on July 3, 2018 http://circ.ahajournals.org/ Downloaded from
Transcript of Use of Intravenous Mannitol in Postperfusion …circ.ahajournals.org/content/27/4/699.full.pdfUse of...

Use of Intravenous Mannitol in PostperfusionOliguria-Anuria
By SAFUiI ATTAR, M.D., FRANCIS J. BORGES, M.D., R. ADAMS COWLEY, M.D.,WILLIAM G. ESmOND, M.D., NORAIAN HOLLINGSWORTH, M.D.,
AND EMIL BLAIR, M.D.
PREVIOUS EXPERIENCE indicates thatrenal failure following cardiopulmonary
bypass caan lead to morbidity and mortality.Doberneek and associates' have indicated thata satisfactory techniieal operative proceduremay be nullified by acute renal failure. Theseauthors report the incideniee of acute renalfailure after open-heart operation using ex-tracorporeal circulation as 3 per cent in athousand patienits. There was an associatedmortality of 86.7 per cent in 30 patients ex-perieneing postperfusion oliguria, azotemia,and hyperkalemia.
In order to evaluate our experience withrenal failure followinog cardiopulmonary by-pass, and the influence of intravenous man-nitol on oliguria-anuria experienced duringthis procedure, the following investigationwas carried out.
MethodsTo date, we have performled 158 open-heart pro-
cedures for repair of congenital and acquired car-diac lesions. Of these, 33 patients had associateddeep hypothermia (10 to 22 C.), with and withoutcomplete circulatory occlusion. The remaining 125patients had moderate hvpothermia (30 to 32 C.)throughout the bypass procedure. A disposabledisk oxygenator-heat exchanger system and 360-degree spring-loaded pumllp were used.2No specific preoperative preparations or evalu-
ation of renal function were undertaken other thanroutine urinalysis and measurem-tent of blood ureanitrogen (BUN) and seruni electrolytes. All pa-tients were in the usual preoperative fasting state,begun at midnight prior to operation. Anesthesiawas iniduced by sodium pentothal and mlaintainedin most instances with nitrous oxide and oxygen,fluothane (0.5 to 1 per cent), and suceinyleholine.
From the Departments of Surgery, Medicine, andAniesthesiology, University of Maryland School ofMedicine, Baltimore, Maryland.
Supported by U. S. Public Health Service Grant5348 and U. S. Army Research and DevelopmentGrant DA-49-007-MD-674.
Circulation, Volume XXVII, April 1963
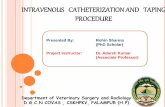
In adults, a Foley catheter was inserted priorto anesthesia; children were catheterized imme-diately after induction of anesthesia. The rate ofurine flow was monitored by continuous collectionof urine in a graduated cylinder. In the earlyphase of the study, the urinary flow during theentire operation was collected as a single specimien.Because of the occurrence of oliguria during theoperation, we began ilonitoring the urine flow at15-iminute intervals throughout the entire operativeprocedure (fig. 1). In all instances, postoperativeurinary flow was monitored at hourly intervals. Allpatients who developed oliguria, defined here as0.25 ml./imm. (360 ml./day) or less for two hoursor longer, received a priming dose of 50 ml. of20 per cent mannitol (10 Gm.). If urine flow didnot increase within 30 minutes, a second dose of10 Gm. was administered. If no response was ob-tained within an hour, no further mannitol wasadministered. When urine flow increased to 0.5ml./nmin. or more, mannitol infusion was titratedagainst urine flow to mlaintain urinary flow atapproximiiately 1 nml./min. Administration of 20per cent intravenous miiannitol at 0.5 to 1 ml./min.was usually adequate to provide a urinary flow of1 to 1.5 ml./min. In no instance was more than140 Gm. of mannitol administered in 24 hours.Amounts beyond 200 Gm. in 24 hours are not ree-omniended because of the possibility of producingcirculatory overload, clinical symptomiis resemiiblingwater intoxication, hyponatreiimia, or irreversiblerenal tubular damage.
In this study, we have applied the principle ofacute functional renal failure as proposed byBarry.3 Barry defines acute renal failure as thesuddeni inability of the kidneys to vary urinary vol-umire and content appropriately in response tohomeostatic needs. He classifies it into two majorparts: functional renal failure, which is precipi-tated by extrarenal factors and is immediatelyreversible by arresting the renal action of thesefactors, since no organic lesions are present; andorganic renal failure, which may be preceded byfunctional failure, but is not inmmnediately reversi-ble by arresting action of the extrarenal precipi-tating factors. Renal failure is maintained byorganic renal lesions. Barry suggests that mannitolinfusion nmay prevent the progression of func-tional to total organic failure.
699
by guest on July 3, 2018http://circ.ahajournals.org/
Dow
nloaded from

0TTTAR, BORGES, CO WLEY, ESMOND, HOLILJNGSWORTII, BLAIR
BUN 11 mg O/.No 129 mEqK 4.3 mEg
I^ _.a.I%
TEP401TEMP 35-fC 30 *
25-3L2L PUMP PUMPL ON OFF
33 28 31 29 1 8131 III 126 130 136 1324.5 5.3 5.3 36 4.7 4.21.7 2.2 1.9 .9 2.0 23 1.8.64 .58 .65 1.2 82 1.1 1.3
IN -I.9L0- .64
100ANESTHESIA-- )1
2.0 H/ ...........
............ M m
V.R. WF 50REPAIR OF RECURRENT
I.A.S.D. _
= 2.6 mEq
4 5 6 7 8 9 10 11 12 13 14 .7/2Y/62 ;1
Figure 1Patient V. R.-Oliguria during repair of re'-urrent interatrial septal defect.
In an attenlpt to circumvent the rare, but fatal,problem of postperfusion hypothermic renal fail-ure, we began to apply the above principle to theoliguric-anuric state associated with cardiopulnmo-nary bypass. For purposes of clarity, renal failureis considered functional when: (1) urine flow is0.25 ml./min. or less for two hours or longer; (2)oliguria is progressive and becomes associated withbiochemical changes characteristic of renal failure,i.e., azotemia, hyperkalemia, and acidosis; (3) oli-guria is reversible; and (4) oliguria is not asso-
ciated with any demonstrable renal tubular changescharacterized by degenerative changes of hypoxienephrosis and/or acute tubular necrosis as demon-strated by light microscopy. When these criteriaoccurred in association with demonstrable tubulardegenerative changes, organic renal failure was
considered to be present.
ResultsIn the 158 patients studied, 19 were found
to fulfill our criteria of acute renal failure.Seventeen patients fell into the functionalgroup, and 2 into the organic; 7 were chil-dren and 12 adults (table 1). None of thesepatients demonstrated abnormal findings inthe urine or serum BUN level preoperatively.The oliguria-anuria was most common in inter-ventricular septal defects (six patients) andmitral insufficiency (four patients) (table 1).
However, organic renal failure followed aorticvalvulotomy in patient E.S., and repair of
interventricular septal defect in patient C.Z.Deep hypothermia was utilized in eight pa-
tients with complete circulatory occlusionranging from 4 to 45 minutes. High flowrates were utilized even at lower tempera-tures to avoid the development of metabolicacidosis.2The onset of oliguria in relation to the
anesthesia and bypass was important (fig. 2).Five patients had onset of oliguria shortlyafter anesthesia: one prior to the pump, threecoincidental with the pump, six in the imme-
diate postperfusion period, and four duringthe first 48 hours after operation. The dura-tion of the oliguric-anuric period varied from2 to 45 hours. In four children, the oliguria(0.05 to 0.15 ml./min.) lasted from 2.5 to 16hours and ended with spontaneous diuresis. Inthe remaining three children, who died, the oli-guria persisted in two until death and was
reversed in patient D.D. with the use ofmannitol. In the adult group, nine patientsreceived mannitol, with good diuretic re-
sponse (1 ml./min. or more) in eight; threedied in functional renal failure.
Circulation, Volume XXVII, April 1963
UI
-
C. .
700
kgI' I"I'e1 /2 18/3
by guest on July 3, 2018http://circ.ahajournals.org/
Dow
nloaded from

SYMPOSIUM ON CARDIOVASCULAR SURGERY
CA
C-C)
rn0000
CO
P. -Il
0
ct
AH0
be
005
P- f)
f C/C Cf
Cr Cr Cr-000,0000 0_ 0_
000Z5050
0; 0
o oCr
0
CO
r,)a)
U1
0CO
a)
0 C)
oC_
.,-
0)
Cr0
54r
0;
0V0H
(1p-00
be5
ct
v
1-5
(.)
0
Z
T2
C)
.~;_
Z
LO
P-
Go
AC:0-
C)
00ct
a)
A0CO
.-
C-)
CIZ0
C)
C)
_4 C:CZ
9 1=
C-. (:,00
co
a) aD)
0) 0 0 a) 0~>q z1~1z
ClCl
CO
CA
CAO
0
Cr 0
rn _ a
_.-4r 0-C.0Cr.OOF-C
0
'H-
0
'H0a-
0
0*'Hai
t- L--cl CO C in rH C 00 C0 10r-H CA>C a Cl Cl1 co
Cl10 Cl Cl 00 I> CO I O C
Cl H Cl 10
Az
°o5
CO O P>
5n 000zZ
._
F-4
.0H
F--
0,.
C) 0z
Cl
CO
rn
C1
-
U.'H0
a)
F-q
.0l
p
0o
C Cr(1 Cr0A 0> 0> 0>
0 Oi00
0
AbeS00O.C,s
0 ;M.n 0
cO Q
0)>0t
0),A_
0
F-0H
z
0
0
F1-O~ob--.I
. *j5-, -
0-
O) 04-
av -
0 4
rn
Cr
*-
0) 0~> z1
10
Cil 00 C ClCOy:6 CO O CO
00-I
'H0l
0
0rn5-
0
-
a)0
00
.H
0)A-
00
05z
00
a)
10 CO CO In 4 Cl 0 00 O0-i co Cl Cl Cl0 - Cl Cl
CO r I> CO CO I- CO HCl Cl C]l t co 10
'HG Z. ZC, C PI rj
Ci)
¢6
0O0
Ct EPH
C' e4--E-- o
0C.)00
.S .~
(1 ct
't on.,- m@ Pv g
. 0 4, 0 ', E-4 )o
-e .- Pm m 14~~
Circulation, Volume XXVII. April 1963
701
+ Cl
04 n
.,O
Cl
zev S
0t
00a
c: 0 >
0-;* A2
CI
4-a
0V
r.
S0a
0_I
r-
C
0u1= oA
%.
CH0
o
aL)
C
0
0za)
0
cr
0
.
CO
0s
0
0
0
0v
,_-
0
0
0
0c
r;
0
0,
CO
0qA:
CI)
~110
¢F0
*0
A)0)
0tV
F-0H
0
0
IIH/
._
0,
0t0
F-
00H0
II
0cOCl
WI
C)
a)
r00._2ruR
ci .. P4 P. P4 P. .?. (-5 P4 G6 P.a. P4 P. .,: .. 9 .i .. gi P4 P4 .11
HiGd
i-
by guest on July 3, 2018http://circ.ahajournals.org/
Dow
nloaded from

ATTAR, BORGES, COWLEY, ESMOND, HOLLINGSWORTH, BLAIR
Figure 2Graph illustrating urinary flow, ml. amm., as plotted against time of onset of oliguria.Origin of arrow indicates degree of oliguria; length of arrowic indicates duration of oligii-ria; height of arro,w indicates degree of diuretic response.
DiscussionOliguria-anuria and acute renal failure fol-
lowing open-heart operations have been at-tributed to various factors, including trans-fusion reactions, polybrene, inadequate andprolonged perfusions, and deep hypothermiawith eirculatory occlusion. In the presentstudy, it became apparent that the onset ofoliguria-anuria in cardiac patients was relatednot only to the pump perfusion, but also tothe induction of anesthesia. This is accountedfor by the further decrease in an alreadylowered cardiac output in patients with mitralstenosis, mitral insufficiency, and aortic in-sufficiency. The three patients (fig. 2) whodeveloped oliguria-anuria during pump per-fusion were all cooled to deep levels of hypo-thermia (13 to 21 C.) and had completecirculatory arrest for 4 to 21 minutes. Theurinary flow was found to drop with the lower-ing of temperature and would not improve,despite mannitol, until rewarming. Those pa-
tients who developed renal failure in the post-perfusion and early postoperative periodswere found to have the following in common:(1) episodes of hypotension during and afteroperation; (2) the use of vasopressors, specifi-cally norepinephrine, to combat shock; (3)cardiac arrest in two patients; and (4) onlytwo patients, E.S. and C.S., had an elevatedfree plasma hemoglobin lev,el (120 to 300 mg.per cent), compared with an average of 50mg. per cent in the remaininog 17 patients.
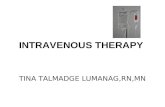
The first patient in this group who receivedmannitol was E.S. (fig. 3). He had an aorticvalvulotomy under deep hypothermia (15 to10 C.) for two hours during which the meanarterial blood pressure was between 30 and40 mm. Hg. Serum hemolysis was 290 mg.per cent at the completion of perfusion. Hehad severe oliguria (0.18 ml. mm.) duringoperation, followed by 4a5 hours of total anu-ria, renal failure, and death. Such an episodeof renal ischemia, elevated plasma hemoglobin
Circulation, Volume XXVII, April 1963
702
by guest on July 3, 2018http://circ.ahajournals.org/
Dow
nloaded from

SYMPOSIUM ON CARDIOVASCULAR SURGERY
40-j35-
TEMP 230iBUN I4mg% 13 77
C 20 Co2 28mEq 1015- No 146mEq 128 124
S0- K 4.6 m Eq I N-1. L 334
0- .13 .02HEMOLYSIS -290mg /0
3,FLOW 2] x E.Sm.-WM 47
LIN 0Xtii0'/FAORTIC VALVULOTOMY -5/25/61Nn-=
_ 10%1. MANNITOL-0.5 L
0.5L-10/.MDIED
W,20*/. 1M- 0.2 L 3:00 PM.
I I I I I I I II
0 2 3 4 5 6 7 8 9 11 13 15 6 12 18 24 6 12 18l< 5/25 *I. 5/26 ).I 5/27 I
HOURSFigure 3
Patient E. S., aortic valvulotomy. Postoperative oliguria refractory to intravenousmannitol.
level, and oliguria has been reported to pro-
duce acute tubular necrosis in dogs.4'One of us
(Dr. Borges) had been using intravenous 20per cent mannitol for the production of uri-nary flow in the treatment of postoperativeoliguria-anuria. The intravenous administra-tion of 140 Gm. of niannitol to E.S. after 15hours of anuria was unsuccessful in inter-rupting his anuria and preventing organicrenal failure. The delay between the onset ofanuria and the initiation of mannitol therapywas felt to be of paramount importance in hisfailure to respond to mannitol titration.
Since then, eight other patients have re-
ceived mannitol between 2 and 14 hours afterthe onset of oliguria-anuria, with an average
waiting period of five hours. The response was
immediate and diuresis between 0.50 and 2.50ml./min. was obtained (fig. 1). Titration ofmannitol was then maintained to keep theurinary flow at 1 ml./min. or higher, as de-scribed under Methods. There was no hypona-tremia, circulatory overloading, or convul-Circulation, Volume XXVII, April 1963
sions. Six other patients with oliguria-anuria(0 to 0.1 ml./min.), for an average period of35 minutes, were also given mannitol, butwere excluded from this study because theydid not fulfill the criteria of functional renalfailure. It is interesting to note that fourchildren who had functional renal failure fora period varying from 2.5 to 21 hours recov-ered spontaneously, in contradistinction tothree adults who had oliguria from 7 to 34hours and died in renal failure.An attempt was made to evaluate renal
function during cardiopulmonary bypass bydetermination of glomerular filtration (endog-enous creatinine clearance) and renal plasmaflow (para-aminohippurate clearance) in twopatients; however, the lack of a steady urinaryflow throughout the operation rendered theclearance meaningless. Nevertheless, Barry etal. have demonstrated that mannitol infusionincreases renal plasma flow and restores glo-merular filtration rate and urinary flow ratein diseased kidneys.6 In addition, it has been
URINE 0.8-07-
FLOW 0o6-
0.3-
0.1 1 b d " --- '' --
........... -----
*I I I I ! I I
703
-1 n-L.
by guest on July 3, 2018http://circ.ahajournals.org/
Dow
nloaded from

ATTAR, BORGES, COWLEY, ESMOND, HOLLINGSWORTH, BLAIR,
shown, experimentally, to protect the kidneysagainst pigment, epinephrinie, and mallettrauma. If this is so, then hypertonic manni-tol infusion would seem to be a direct attackon the immediate cause of acute renal failure.namely, renal ischemia and the more remotefactors of hypoxia, interstitial edema, tubularcollapse, tubular cast obstruction, and intra-capillary thrombosis found in experimentalacute renal failure. One or all of these factorsmay be operating during cardiopulmonary-bypass operations. We therefore believe thatthe use of mannitol in open-heart operations isindicated when functional renal failure isdemonstrated.
SummaryWe have applied the principle of acute
functional renal failure in the managementof the oliguric-anuric state encountered in 19of 158 patients undergoing open-heart opera-tions. Mannitol was administered to nine pa-tients who experienced acute renal failure,with successful diuresis and restoration ofkidney function in eight.
AcknowledgmentThe authors wish to express their appreciation to
Dr. Colin Wood for the interpretation of histologicalslides, and to Dr. L. D. Beetol and Dr. T. A. Garrett,from Baxter Laboratories, Inc., Morton Grove, Illinois,for kinidly supplying the mannitol used in this investi-gation.
References1. DOBERNECK, R. C., REISER, M. P., AND LILLEHEI,
C. W.: Acute renal failure after openi heartsurgery. J. Thoracic & Cardiovas. Surg. 43:441, 1962.
2. ES-MOND, W. G., ATTAR, S., AND COWLEY, R. A.:Profound hypothermia with simplified equip-ment. J. Thoracic & Cardiovas. Surg. 42: 563,1961.
3. BARRY, K. G., AND MALLOY, J. P.: Oliguric renalfailure. J.A.M.A. 179: 510, 1962.
4. LITWIN, M. S., WALTER, C. W., AND JACKSON, N.:Experimental production of acute tubular ne-crosis in dogs. S. Forum 10: 370, 1959.
5. BORGES, F. J.: Use of intravenous niannitol intreatment of the acute oliguric-anuric state.Presented at Symposium on Mannitol, WalterReed Army Hospital, February 3, 1962.
6. BARRY, K. G., DOBERNECK, R. C., AND MCCORMICK,G. J.: Effect of hypertonic mannitol infusionon renal clearance of PAH and inulin in man.Clin. Res. 10: 245, 1962.
Circulation, Volume XXVII, April 1963
704
by guest on July 3, 2018http://circ.ahajournals.org/
Dow
nloaded from

ESMOND, NORMAN HOLLINGSWORTH and EMIL BLAIRSAFUH ATTAR, FRANCIS J. BORGES, R. ADAMS COWLEY, WILLIAM G.
Use of Intravenous Mannitol in Postperfusion Oliguria-Anuria
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1963 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.27.4.699
1963;27:699-704Circulation.
http://circ.ahajournals.org/content/27/4/699located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. and Rights Question and Answer
Permissionsthe Web page under Services. Further information about this process is available in thewhich permission is being requested is located, click Request Permissions in the middle column ofClearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of the CopyrightCirculationoriginally published in Requests for permissions to reproduce figures, tables, or portions of articlesPermissions:
by guest on July 3, 2018http://circ.ahajournals.org/
Dow
nloaded from