
Use of imaging in dementia
27
Use of imaging in dementia John O’Brien Professor of Old Age Psychiatry NIHR National Specialty Lead for Dementia Department of Psychiatry University of Cambridge
Transcript of Use of imaging in dementia

Use of imaging in dementia
John O’Brien
Professor of Old Age Psychiatry
NIHR National Specialty Lead for Dementia
Department of Psychiatry
University of Cambridge

Brain imaging in dementia
• Rule out other brain disorders
• Assist with subtype diagnosis
• Stratify subjects for clinical trials/ treatments
• Outcome biomarker for clinical trials
• Investigate underlying neurobiology and
mechanismsResearch use
Clinical practice
Current imaging in Dementia
• Computed tomography (CT)
• Magnetic resonance imaging (MRI)
• Perfusion (HMPAO) SPECT
• Glucose (FDG) PET
• Dopamine (FP-CIT) SPECT
• Amyloid (PIB, florbetapir, flutemetamol, flurbetaben)
PET
• MIBG cardiac imaging
6/7 NICE Recommended

Dementia diagnosis in specialist dementia
diagnostic services
• Offer structural imaging to rule out reversible
causes of cognitive decline and assist with
subtype diagnosis, unless dementia is well
established and the subtype diagnosis is clear
• Do not rule out dementia based solely on the
results of CT or MRI scans
• Don’t forget coronal CT
(JOB recommended)
NICE Dementia guideline, June 2018 (www.nice.org.uk)

Diagnosing vascular dementia
• If the dementia subtype is uncertain and vascular
dementia is suspected, use MRI.
• Do not diagnose vascular dementia based solely
on vascular lesion burden
NICE Dementia Guideline, June 2018

Diagnosing Alzheimer’s disease
If the diagnosis is uncertain and Alzheimer’s disease is
suspected, consider either:
• FDG-PET (fluorodeoxyglucose-positron emission tomography)
- or perfusion SPECT (single-photon emission CT) if FDG-
PET is unavailable
or
• Examining CSF for phosphorylated-tau 181 and total tau and
either amyloid beta 1-42 or a ratio of amyloid beta 1-42 and
amyloid beta 1-40
NICE Dementia Guideline, June 2018

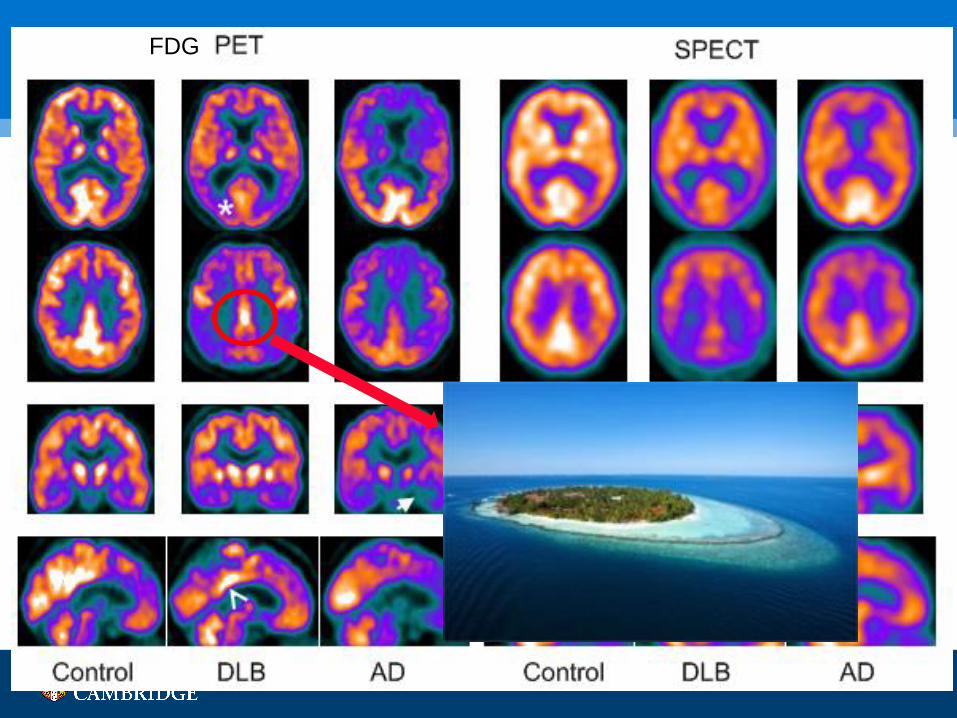
FDG
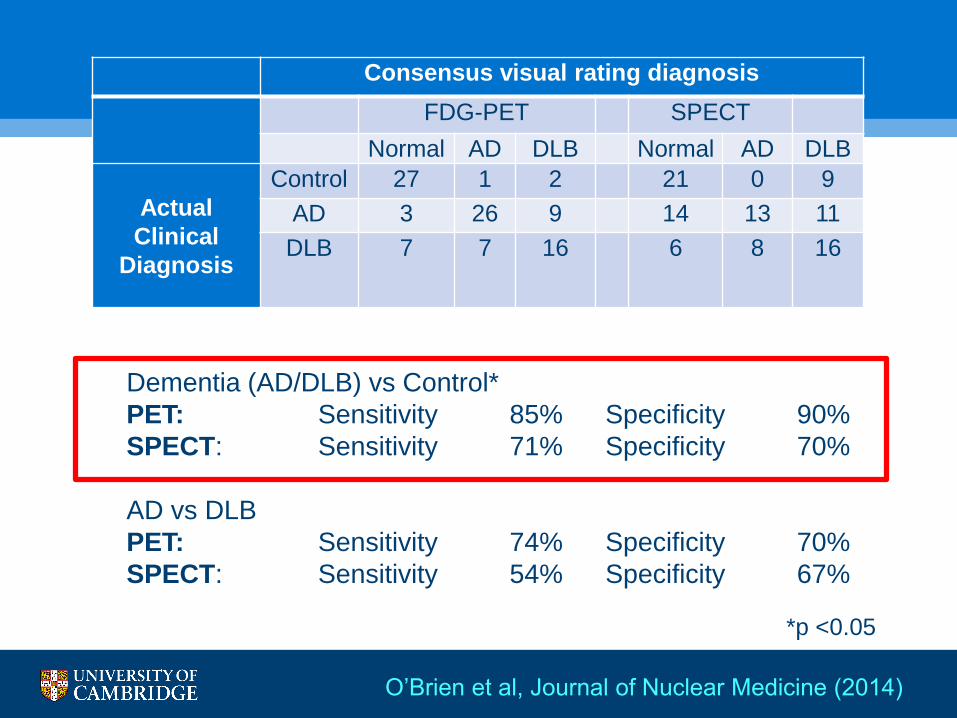
Consensus visual rating diagnosis
FDG-PET SPECT
Normal AD DLB Normal AD DLB
Actual
Clinical
Diagnosis
Control 27 1 2 21 0 9
AD 3 26 9 14 13 11
DLB 7 7 16 6 8 16
Dementia (AD/DLB) vs Control*
PET: Sensitivity 85% Specificity 90%
SPECT: Sensitivity 71% Specificity 70%
AD vs DLB
PET: Sensitivity 74% Specificity 70%
SPECT: Sensitivity 54% Specificity 67%
*p <0.05
O’Brien et al, Journal of Nuclear Medicine (2014)

Is PET more stressful than SPECT?
Bamford et al, 2015

0
10
20
30
40
50
60
70
80
90
100
Patients
Controls
Carers
Important factors associated with scan
Overall 97% rated PET and 91% SPECT as worthwhile
Bamford et al, 2015

Dopaminergic SPECT: a robust
biomarker for DLB
Pooled sensitivity 78%, specificity 90%
O’Brien et al, BMJ Open, 2014
Normal
DLB

Diagnosing dementia with Lewy bodies
• If the diagnosis is uncertain and dementia with Lewy
bodies is suspected, use 123I-FP-CIT SPECT
• If 123I-FP-CIT SPECT is unavailable, consider 123I-
MIBG cardiac scintigraphy
• Do not rule out dementia with Lewy bodies based
solely on normal results on 123I-FP-CIT SPECT or 123I-MIBG cardiac scintigraphy
NICE Dementia Guideline, June 2018
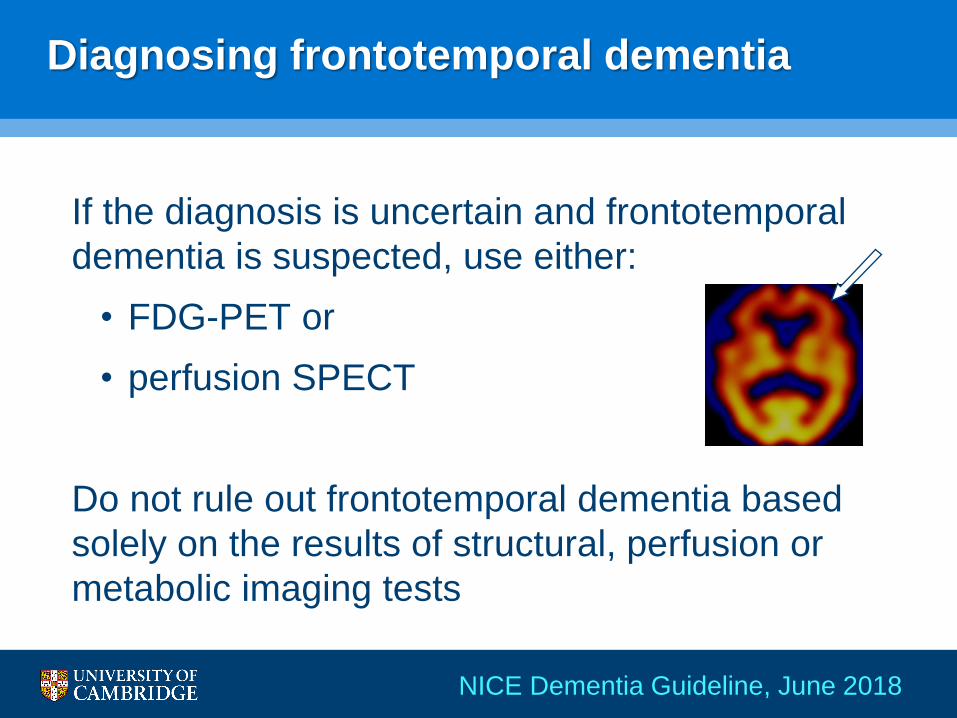
Diagnosing frontotemporal dementia
If the diagnosis is uncertain and frontotemporal
dementia is suspected, use either:
• FDG-PET or
• perfusion SPECT
Do not rule out frontotemporal dementia based
solely on the results of structural, perfusion or
metabolic imaging tests
NICE Dementia Guideline, June 2018

Amyloid imaging in Dementia
Negative scan:
normal
Positive scan:
Amyloid present
(AD, DLB, old age)
Flurbetapir
(Amyvid)
Flutametamol
(Vizamyl
Flurbetaben
(NeuraCeq)
3 commercially available Fluorine based ligands for AD diagnosis
What does NICE say about the use of
amyloid imaging?
NICE Dementia Guideline, June 2018
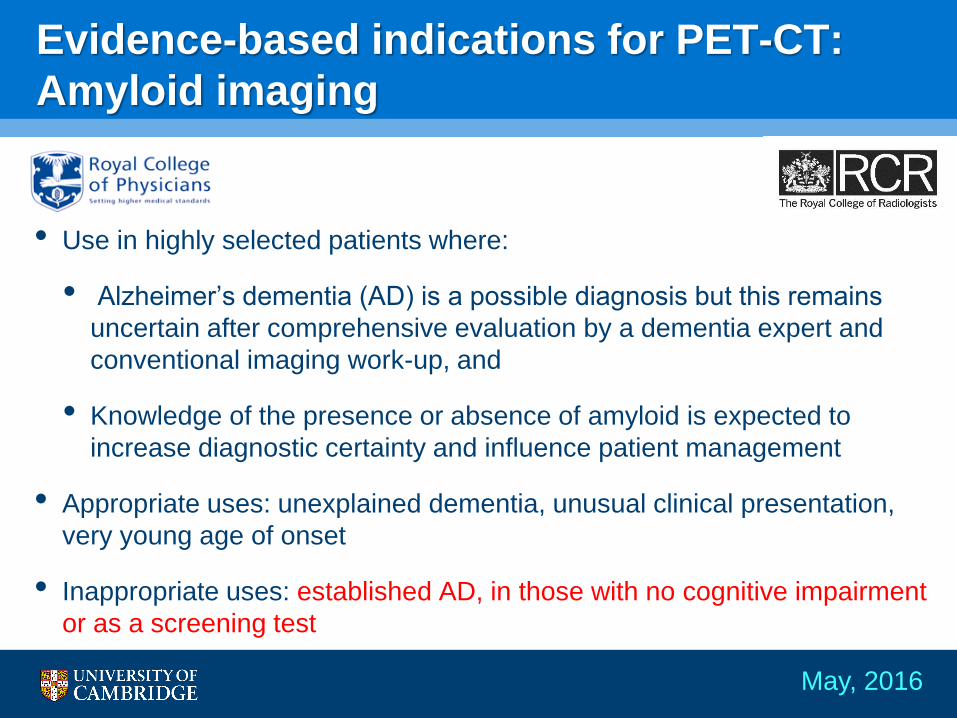
• Use in highly selected patients where:
• Alzheimer’s dementia (AD) is a possible diagnosis but this remains
uncertain after comprehensive evaluation by a dementia expert and
conventional imaging work-up, and
• Knowledge of the presence or absence of amyloid is expected to
increase diagnostic certainty and influence patient management
• Appropriate uses: unexplained dementia, unusual clinical presentation,
very young age of onset
• Inappropriate uses: established AD, in those with no cognitive impairment
or as a screening test
Evidence-based indications for PET-CT:
Amyloid imaging
May, 2016

Jansen et al, JAMA 2015
55 studies of 8694 people
Rates:
10% at 50 yo
20% at 70 yo
40% at 90 yo
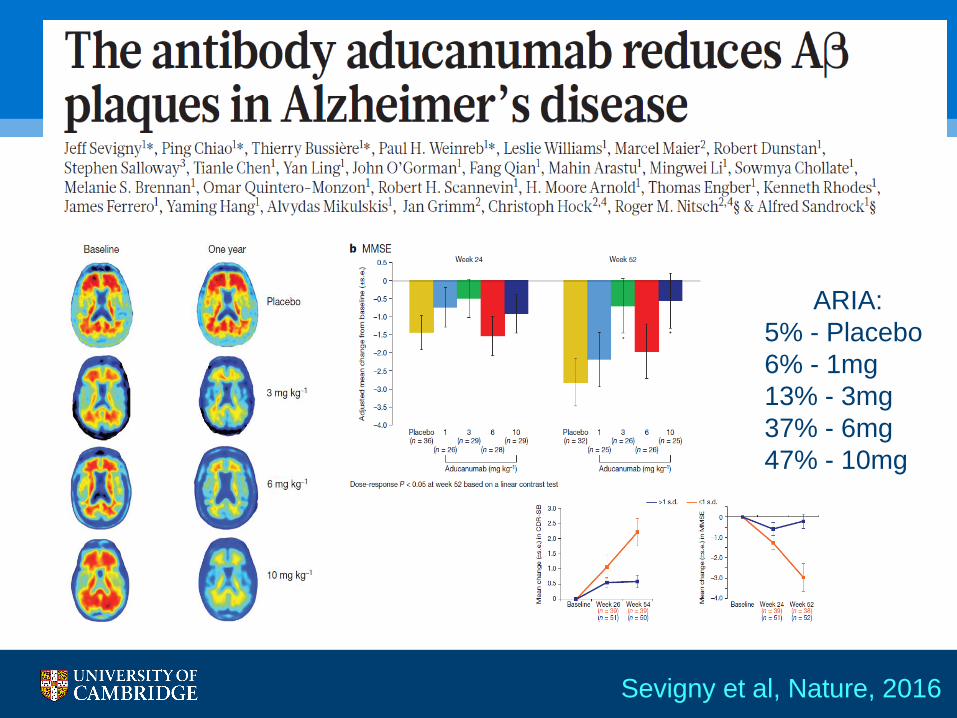
Sevigny et al, Nature, 2016
ARIA:
5% - Placebo
6% - 1mg
13% - 3mg
37% - 6mg
47% - 10mg

Imaging tau: the AD and the FTD spectrum
TAU TDP-43
AD
Courtesy of Matthew Jones, from BAP
Dementia Guidelines: O’Brien et al, 2017

Leuzy et al, Mol Psych, 2019
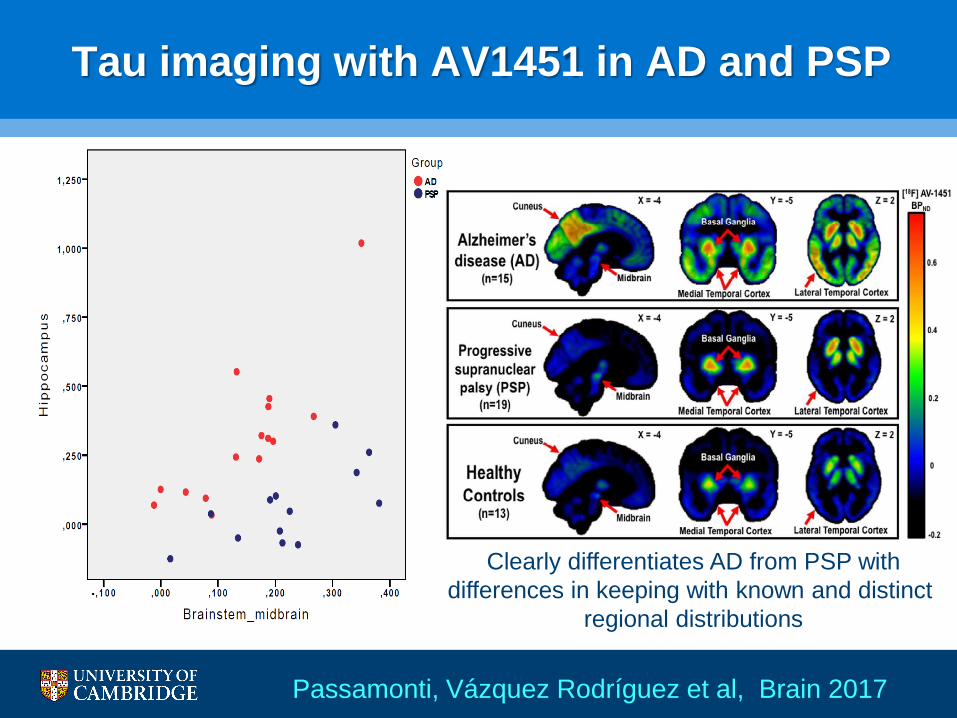
Tau imaging with AV1451 in AD and PSP
Clearly differentiates AD from PSP with
differences in keeping with known and distinct
regional distributions
Passamonti, Vázquez Rodríguez et al, Brain 2017

Imaging tau: the AD and the FTD spectrum
TAU TDP-43
AD
Bevan-Jones et al, 2017

But how early do brain imaging changes occur?
The PREVENT-Dementia study
• 5 site study, Cambridge, Imperial, Oxford, Dublin,
Edinburgh
• Aim to recruit 600-700 cognitively normal 40-59 yo
• Half of group have FH dementia (parent)/ half do not
• Comprehensive assessment over 3-4 visits
− Baseline physical, cognition, blood, urine and saliva
− Multi-modal MR scan
− Optional: Lumbar puncture for CSF, Amyloid PET, 7T
MRI
• Follow-up at 2 and 5 years
Ritchie et al, Alz and Dementia, 2017

P<0.001
Mean age 53, mean age
parental dementia 72
JNNP, 2020

Conclusions
• CT, MR, perfusion SPECT and Glucose PET are
established clinical tools
• FP-CIT and MIBG (heart) can assist with DLB
diagnosis
• Amyloid imaging available, not yet in wide clinical use;
tau and other ligands in development
• Brain imaging changes can be detected years
(decades) before dementia onset
• When ordering scans don’t forget other aspects
(referral form, report, MDTs)

Clinical Research Network
Join Dementia Research
● A nationwide service that helps
anyone in the UK find and take part in
vital dementia research studies.
● Supporting delivery of Government’s
Challenge on Dementia
What is Join Dementia Research?


















