Stage 2 Critical Elements for Urinary Incontinence, Urinary Catheter
Upload
maya-rentinaCategory
view
37download
8description

Urinary System
Dr. Ika Kartika, SpPA

Functional Anatomy of KidneyStructure and Function of NephronsRenal Blood Flow and its Regulation

Kidneys
• Kidneys are a pair of excretory organs situated on the posterior abdominal wall, extending from upper border of T12 to L3 vertebra
• Right kidney is slightly lower than the left• Each kidney is 11 cm long, 6 cm broad and 3 cm thick,
weight 150 g in males and 135 g in females• Capsules or coverings of kidneys - Fibrous capsule, Peri-
renal fat, Renal fascia and Para-renal fat• Coronal segment – cortex; medulla; renal sinus

Renal cortex Cortical lobules - which
form caps over the bases of the pyramids
Renal columns - which dip in between the pyramids
Renal medulla has 10 conical masses
called renal pyramids, their apices form renal papillae
Renal sinus Space that extends into kidney from hilus Contains branches of renal artery and renal vein Renal pelvis divides into 2-3 major calices and these in turn divide into 7-
13 minor calices, each minor calyx (cup of flower) ends in an expansion which is indented by 1-3 renal papillae

Kidney Location
Lateral to vertebral column high on body wall, under floating ribs in retro-peritoneal position

Sectional Anatomy
Cortex: outer layer, light reddish brow, granular appearance (due to many capillaries)
Medulla: darker striped appearance (due to tubules) Subdivided into distinct renal pyramids, terminating with a papilla. Separated by renal columns from the cortex.
Fig 26-3

Urine collection:
Ducts within each renalpapilla release urine into minor calyx
major calyx
renal pelvis
ureter

Histologically, each kidney is composed 1-3 million uriniferous tubules. Each consists of Secretory part - which forms urine is called nephron, functional
unit of kidney Nephrons open in to collecting tubules. Many such tubules unite
to form the ducts of Bellini which open into minor calicesArterial Supply One renal artery on each side arising from abdominal aorta At or near hilus, renal artery divides into anterior and
posterior branches giving rise to segmental arteriesLymphatics Lateral aortic nodesNerve Supply Renal plexus (an off shoot of coeliac plexus, T10-L1)

Circulation of renal blood flow
Renal artery divides serially into – interlobar artery arcuate interlobular arteries afferent arterioles capillary tufts of renal glomeruli into outer cortex efferent arterioles in juxtamedullary zone arterioles become vasa recta (closely applied to loop of henle)Venous drainage: Stelate veins interlobular veins arcuate veins interlobar veins

Two types of nephrons are present Cortical nephrons with short loop of Henle Juxtamedullary nephrons with long loops of Henle

Glomerulus - Five components Capillary endothelium – 70-100
nm fenestrations – restricts passage of cells
Glomerular basement membrane – filters plasma proteins
Visceral epithelium – podocytes with s foot processes with 25-60 nm gaps, permeability altered by contraction of foot processes
Parietal epithelium (Bowman’s capsule)
Mesangium (interstitial cells) – pericytes, structural support, phagocytosis, restricts bld flow in response to angiotensin-II
Filtr
atio
n ba
rrier

Filtration barrier - Size and charge selective
• Charge: all 3 layers contain negatively charged glycoproteins restricts passage of other negatively charge proteins
• Size: Molecules with radius <1.8 nm water, sodium, urea, glucose, inulin freely filtered
• >3.6 nm hemoglobin and albumin not filtered
• Between 1.8-3.6 cations filtered, anions not
• Glomerulonephritis negatively charged glycoproteins destroyed polyanionic proteins filtered proteinuria

Glomerular Filtration Rate (GFR) Normal GFR: in men = 125 ml/min, 10% lower in females Depends on permeability of filtration barrier Difference between hydrostatic process pushing fluid into
Bowman’s space and osmotic forces keeping fluid in plasma
GFR = Kuf [(Pgc – Pbs) – (gc – bs)Pgc & Pbs = Hydrostatic pressure in glomerular capillary and basement membrane gc & bs = plasma oncotic pressure in glomerular capillary and basement membraneKuf = Ultrafiltration coefficient reflects capillary permeability and glomerular surface area

Juxtaglomerular apparatus Macula densa – modified portion of thick ascending limb
which is applied to glomerulus at the vascular pole between the afferent and efferent arterioles containing chemoreceptor cells which sense tubular concentration of NaCl
Granular cells – Produce renin, which catalyses the formation of angiotensin modulates efferent and afferent arterial tone and GFR

Juxtaglomerular Apparatus
Macula densa +Juxtaglomerular cells (smooth
muscle fibers from afferent arteriole)
= Juxtaglomerular Apparatus
= Endocrine system structure (renin and EPO)

FunctionsNephron regulates Intravascular volume, osmolality, acid base balance,
excrete the end product of metabolism and drugs Urine is formed by combination of glomerular
ultrafiltration + tubular reabsorption and secretionNephron produces hormones Fluid homeostasis (renin, prostaglandins, kinins) Bone metabolism (1,25-dihydroxycholecalciferol) Hematopoiesis (erythropoietin) – produced by interstitial
cells in peritubular capillary bed (85% stimulus hypoxia

Tubuloglomerular feedback GFR
delivery of NaCl to distal tubule
Cl- sensed by macular Densa cells
Release of renin (from afferent arterioles)
Angiotensin
Arteriolar constriction
GFR and RBF

Normally, a balance is present between systems promoting renal vasoconstriction and sodium retention versus systems promoting renal vasodilation and sodium excretion.
Surgical stress, ischemia, and sepsis tip the balance in favor of vasoconstriction and sodium retention.
On the other hand, hypervolemia (or induction of atrial stretch) tips the balance in favor of vasodilation and sodium excretion.
Hormonal Regulation

Epinephrine & norepinephrine
Afferent arterial tone (directly & preferentially)
Marked in GFR prevented indirectly by release of renin and angiotensin-II

Renin angiotensin and Atrial natriuretic peptide (ANP) Hypotension or hypovolemia renin afferent arteriole
angiotensin II release of aldosterone from the adrenal cortex Volume reexpansion causes atrial distention release of ANP ANP inhibits the release of renin, renin's action on
angiotensinogen to form angiotensin II, angiotensin-induced vasoconstriction, stimulation of aldosterone secretion by angiotensin II, and action of aldosterone on collecting duct

Prostaglandins
Systemic hypotension and renal ischemia
Angiotensin induced prostaglandin synthesis (PGD2, PGE2 & PGI2)
Vasodilation (protective mechanism)

Neuronal Regulation
Sympathetic outflow from spinal cord
Celiac & renal plexus
1 receptors sodium reabsorption in
PCT
2 receptors Na+ reabsorption and
water excretion
Dopamine dilates afferent and efferent arterioles
(via D1 receptor activation)
Low dose dopamine partially reverses norepinephrine induced
renal vasoconstriction
Dopamine PCT Na+ reabsorption

Aldosterone Enhances Na+ K+ ATPase activity by number of open Na+
& K+ channels in luminal membrane Enhances H+ secreting ATPase on the luminal border od
intercalated cells Because principal cells reabsorb Na+ via an electrogenic
pump Either Cl- must be reabsorbed K+ must be secreted to maintain electroneutrality
intracellular K+ favours K+ secretion

Medullary collecting tubule Site of actiion of ADH or AVP (arginine vasopressin)
activates adenylate cyclase Dehydration ADH secretion luminal membrane
becomes permeable to water water is osmotically drawn out of tubular fluid passing through the medulla concentrated urine (upto 1400 mos)
Adequate hydration – suppressed ADH secretion fluid in collecting tubule passes through medulla unchanged and remains hypotonic (100-200 msom/l)
Hydrogen ion secreted are excreted in the form of titrable acids (phosphates) and ammonium ions


CONGENITAL•AGENESIS•HYPOPLASIA•ECTOPIC•HORSESHOE

AGENESIS

HYPOPLASIA

ECTOPIC (usually PELVIC)

HORSESHOE

CYSTIC DISEASES• CYSTIC RENAL “DYSPLASIA”• Polycystic Kidney Disease
–Autosomal DOMINANT (AD-ULTS)– Autosomal RECESSIVE (CHILDREN)
• MEDULLARY–Medullary Sponge Kidney (MSK)– Nephronopththisis-Medullary
• ACQUIRED (Dialysis-associated) cystic disease• Localized (SIMPLE) Renal cysts

• Renal Cysts in hereditary malformation syndromes (e.g tuberous sclerosis)
• Glomerulocystic disease• Extraparenchymal renal cysts

CYSTIC RENAL “DYSPLASIA”• ENLARGED• UNILATERAL or BILATERAL• CYSTIC• Have “MESENCHYME”• NEWBORNS• VIRAL, GENETIC (rare)

AUTOSOMAL DOMINANT• HEREDITARY, PKD1, PKD2• FOLLOWS AUTOSOMAL DOMINANT
PEDIGREE• COMPLEX GENETICS• RENAL FAILURE in 50’s

AUTOSOMAL RECESSIVE• CHILDHOOD• KIDNEYS LOOK EXACTLY LIKE THE
ADULT TYPE• PKHD1• PATIENTS WHO SURVIVE
CHILDHOOD OFTEN DEVELOP HEPATIC FIBROSIS

MEDULLARY CYSTS• MEDULLARY SPONGE KIDNEY (MSK),
usually an incidental finding on CT or US
• NEPHRONOPHTHISIS, cysts @ CMJ, hereditary (AR), progressive

ACQUIRED (DIALYSIS)

“SIMPLE” CYSTS• Cortical• Also called “retention” cysts• Also “acquired”• Incidental, asymptomatic• VERY very very common



CLINICAL MANIFESTATIONS OFRENAL DISEASES
The clinical manifestations of renaldisease can be grouped intoreasonably well-defined syndromes.
Some are peculiar to glomerulardiseases; others are present indiseases that affect any one of thecomponents.

Azotemia refers to an elevation of blood urea nitrogen and creatinine levels and is largely related to a decreased glomerular filtration rate (GFR).
Azotemia is produced by many renal disorders, but it also arises from extrarenal disorders.
Prerenal azotemia is encountered when there is hypoperfusion of the kidneys, which decreases GFR in the absence of parenchymal damage.
Postrenal azotemia can result when urine flow is obstructed below the level of the kidney. Relief of the obstruction is followed by correction of the azotemia
Terminology

When azotemia progresses to clinical manifestations and systemic biochemical abnormalities, it is termed uremia.
Uremia is characterized not only by failure of renal excretory function but also by a host of metabolic and endocrine alterations incident to renal damage.
There is, in addition, secondary gastrointestinal (e.g., uremic gastroenteritis), neuromuscular (e.g., peripheral neuropathy), and cardiovascular (e.g., uremic fibrinous pericarditis) involvement

The major renal syndromes : Acute nephritic syndrome is a glomerular
syndrome dominated by the acute onset of usually grossly visible hematuria (red blood cells in urine), mild to moderate proteinuria, azotemia, edema, and hypertension; it is the classic presentation of acute poststreptococcal glomerulonephritis.

The nephrotic syndrome due to glomerular disease characterized by heavy proteinuria (excretion of >3.5 gm of protein/day in adults), hypoalbuminemia, severe edema, hyperlipidemia, and lipiduria (lipid in the urine).
Asymptomatic hematuria or proteinuria, or a combination of these two, is usually a manifestation of subtle or mild glomerular abnormalities.

Rapidly progressive glomerulonephritis results in loss of renal function in a few days or weeks and is manifested by microscopic hematuria, dysmorphic red blood cells and red blood cell casts in the urinesediment, and mild-to-moderateproteinuria

Acute renal failure is dominated by oliguria or anuria (no urine flow), with recent onset of azotemia. It can result from glomerular injury (such as crescentic glomerulonephritis), interstitial injury, vascular injury (such as thrombotic microangiopathy), or acute tubular necrosis
Chronic renal failure, characterized by prolonged symptoms and signs of uremia, is the end result of all chronic renal diseases

Urinary tract infection is characterized by bacteriuria and pyuria (bacteria and leukocytes in the urine).
The infection may be symptomatic or asymptomatic, and it may affect the kidney (pyelonephritis) or the bladder (cystitis) only

Nephrolithiasis (renal stones) is manifested by
renal colic, hematuria,and recurrent stone
formation.
In addition to these renal syndromes, urinary
tract obstruction and renal tumors, discussed
later, represent specific anatomic lesions that
often have varied manifestations.

Schematic diagram of a lobe of a normal glomerulus

Glomerulus merupakan bagian dari nefron yang terletak dalam kapsul Bowman, mempunyai fungsi sebagai filter darah.
Setiap glomerulus terdiri dari anyaman kapiler yang kompleks yang menonjol di dalam ruang Bowman.
Kapiler glomerulus tersusun atas:• Sel endotel• Membran basalis• Sel epitel
GLOMERULUS

GLOMERULAR STRUCTURE


PENYAKIT GLOMERULUS
A. Glomerulonefritisprimer : Proliferatif yang difus dan akut Glomerulonefritis yang progresif
cepat Glomerulonefritis membran Nefrosis lipoid Glomerulosklerosis segmental
dan fokal Glomerulonefritis membrane
proliferatif Nefropati imunoglobulin A Glomerulonefritis kronik
B. Penyakit sekunder(sistemik) : Lupus erimatosus sistemik Diabetes melitus Amiloidosis sindr,.googpasture Poliarteritis nodosa Granulomatosis wagener Purpura henockschonlein Endokarditis bakteri

GLOMERULONEFRITISPROLIFERATIF DIFUS (PGN)
• Kelainan Glomerulus yang disebabkan oleh postinfeksi.• Kelainan ini biasanya berupa lesi akut setelah terjadi infeksi.• Beberapa organisme yang menyebabkan PGN, yaitu :
- Streptococcus ß-hemolitikus - Virus- Stafilokokus - Malaria- Meningokokus
-Toksoplasmosis- Pneumokokus -Skistosomiasis
• Morfologi : Pada umumnya, ginjal dapat normal atau sedikit membesar, permukaan korteks halus dan bebas jaringan parut.
• Mikroskop cahaya : glomerulus membesar, hiperseluler,disebabkan karena infiltrasi sel lekosit, proliferasi sel endothel dan mesangial

GLOMERULONEFRITISPROLIFERATIF DIFUS (PGN)
Pada stadium awal penyakit, mikroskop elektron menunjukkan kompleks
immun tersusun sebagai “punuk-punuk” subepitelial yang bersarang pada
GBM. Keadaan klinik : cenderung mendadak ditandai oleh malaise, demam ringan,
nausea, oliguri, azotemia, hypertensi ringan sampai sedang, proteinuria dan
hematuria (urine tampak coklat seperti asap tidak merah terang)

Dengan menggunakan mikroskop cahaya dapat dilihat adanya hiperseluler anyaman glomerulus yang seragam mengenai hampir semua glomeruli.

GLOMERULONEFRITISPROGRESIF CEPAT (RPGN)
Glomerulonefritis progresif cepat (RPGN) adalah suatu sindrom yang berhubungan dengan jejas glomerulus berat dan bukan suatu bentuk etiologik spesifik dari glomerulonefritis. Secara klinik, ditandai khas oleh :
• Oligouria berat.• Berkurangnya fungsi ginjal dengan cepat dan progresif.• Kematian karena gagal ginjal dalam beberapa minggu – bulan.

Kondisi sindrom RPGN dapat terjadi dan dikelompokan kedalam tiga kategori :• RPGN pasca-infeksi.Pasca infeksi streptokokus (1 sampai 2 % dari semua kasus) .
• GN disertai dengan penyakit sistemik.-SLE (Systemic Lupus Erimatosus)-Poliarteritis-Sindrom goodpasture-Granulomatosis wegener-Purpura Henoch-schohlein
• RPGN Primer atau idiopatik.

Morfologi :• Ginjal tampak membesar dan pucat.• Sering disertai pendarahan petekia pada permukaan korteks.
Keadaan Klinik :• Mula gejala RPGN sangat mirip dengan sindrom nefritik• Tetapi oligouria dan azotemia lebih menonjol.• 90% penderita menjadi anefritik dan membutuhkan dialisis
kronis/transplantasi.• Prognosis lebih baik dari pada mereka dengan presentase
kresen yang lebih tinggi.• Penggantian plasma berguna pada beberapapenderita, terutama
pasien dengan sindrom goodpasture.

GLOMERULONEFRITISPROGRESIVE CEPAT
Gambaran histologik ditandai secara khas oleh bentukbulan sabit pada kebanyakan glomeruli (GN kresentik).

GLOMERULONEFRITISMEMBRANOSA
• Merupakan kelainan kronis yang diperantarai oleh kompleks immun.
• Penderita dengan SLE merupakan kelompok lain yg penting;sekitar 10%
menderita MGN. Lebih dari 85% kasus, penyebabnya tidak diketahui
(glomerulonefritis membranosa idiopatik).
• Pada sebagian kasus mempunyai etiologi yang dapat diidentifikasikan
sebagai berikut : infektif : sifilis, malaria, hepatitis B. obat : penisilamin, emas, air raksa, heroin.

Pria lebih sering terkena dibandingkan wanita. Biasanya menunjukan gejala sindroma nefrotik atau adanya
proteinuria. Mengenai seluruh kelompok umur tetapi lebih sering pada
dewasa. Hipertensi ditemukan kadang- kadang saja pada pemeriksaan
klinik. Kira-kira 25% pasien mengalami penyakit progresif yang berakhir
dengan gagal ginjal.
Keadaan klinis dan prognosis :

• Dilihat dengan mikroskop cahaya, perubahan dasar tampak sebagai penebalan difus GBM.
• Dengan mikroskop elektron, dapat terlihat penebalan yang tampak disebabkan sebagian oleh pengendapan sub-epitelial yang bersarang pada GBM dan dipisahkan satu dengan lain oleh penonjolan kecil matriks GBM berbentuk ujung yang runcing (“gambaran paku dan kubah”).
• Mikroskopik fluoresen menunjukkan imunoglobulin yang tipikal granuler dan komplemen sepanjang GBM.
• Pemeriksaan imunopatologis menunjukkan adanya deposit granuler dari IgG dan C3 pada dinding kapiler yang menebal.
• Sesuai dengan berkembangnya penyakit, dinding menjadi lebih tebal akibat deposit
Morfologi :

Ini adalah gambaran glomerulonephritis membranosa yang diambil melalui mikroskop cahaya. Dalam gambar ini dapat dilihat bahwa lingkaran kapiler mengalami penebalan dan menonjol tetapi selularitas tidak mengalami pertambahan. Membranous GN adalah penyebab utama sindrom nefrotik pada orang dewasa.

Minimal Change Disease juga dikenal sebagai lipoid nephrosis, nama yang merefleksikan ada lemak di dalam sel epitel tubulus ginjal.
Kelainan yang relatif jinak ini adalah penyebab sindrom nefrotik yang paling sering pada anakanak.
Pada lipoid nephrosis, terjadi reduksi muatan negatif GBM karena hilangnya polianion glomerulus; yang selanjutnya memungkinkan aliran transmembran albumin serum, sehingga terjadi albuminuria.
Ditandai secara khas oleh glomeruli yang tampaknya normal dibawah mikroskop cahaya, tetapi tampak adanya kehilangan difus epitel taju kaki apabila dilihat dengan mikroskop elektron.
Nefrosis Lipoid (MCD)

Glomerulus tampak normal di bawah mikroskop cahaya. Apabila dilihat dibawah mikroskopelektron, maka dapat dilihat tidak adanya taju kaki epitel

Menyebabkan terjadinya sindroma nefrotik pada
10% anak- anak dan 15% dewasa. Patogenesisnya belum diketahui Gambaran klinis :
* Ditemukan bersama dengan sindroma nefrotik
atau proteinuria yang hebat
* Focal glomerulosclerosis cenderung kambuh lagi
pada ginjal yang ditransplantasikan.
FOCAL SEGMENTALGLOMERULOSCLEROSIS(FSGS)

Gambar diatas adalah glomerulus seorang pasien glomeruloskelerosis segmental dan fokal yang diwarnai dengantrichrome stain. Pada gambar ini dapat dilihat adanya desposisi kolagen ( yang berwana biru). Sekitar 1/6 dari kasus sindrom nefrotik pada anak-anak dan orang dewasa disebabkan oleh FSGS.

• Suatu bentuk glomerulonefritis proliferatif yang menunjukkan adanya proliferasi dan penebalan membran.
• Biasanya ditemukan pada anak besar dan orang dewasa muda. Perjalanan penyakit ini sangat lambat, tanpa remisi, dan berakhir dengan payah ginjal.
Keadaan klinik:• Gejala utama adalah sindrom nefrotik, namun dalam beberapa kasus dapat
hadir sebagai sindrom nefritik ataupun mempunyai ciri keduannya.• Prognosis MPGN rata-rata jelek.
MEMBRANO PROLIFERATIFGLOMERULONEPHRITIS(MPGN)

MPGN dibagi dalam dua bentuk kategori utama, yaitu : Tipe 1 MPGNDeposit tembus elektron terutama terlihat dalam regio subendotelial. Interposisi sel mesangial didalam reduplikasi membrana basalis juga merupakan suatu ciri yang konsisten. Tipe II MPGNBahan yang tembus elekton tidak teratur diendapkan tepat didalam GBM, menimbulkan penebalan ireguler yang jelas. Pada tipe II deposit-deposit itu juga ditemukan dalam kapsula bowman, membrana basalis tubuler, dan kapiler peritubuler
MEMBRANO PROLIFERATIFGLOMERULONEPHRITIS(MPGN)

Dengan mikroskop cahaya, GBM menebal dan terdapat proliferasi difus sel – sel mesangial dan suatu penambahan matriks mesangial. Perluasan mesangium ( sel – sel dan matriks ) berlanjut ke dalam kumparan kapiler perifer, menyebabkan reduplikasi membrana basalis.

Penyakit ginjal yang ditandai oleh adanya darah dalam urin,kadar serum Ig A yang meningkat,hipertensi,dan proteinuria ringan.
Disebabkan oleh inflamasi glomerolus dan deposit Ig A di jaringan ginjal. Menyerang anak-anak dan dewasa muda. Gambaran histologis: Proliferasi mesangial fokal ringan,dijumpai Ig A & C3
pada mesangium,ada bercak deposit paramesangial gelap,adanya gambaran mesangiokapiler yg kadang disertai nekrosis segmental
NEPHROPATHY Ig A


Merupakan glomerulonefritis tingkat terakhir (“end stage”) dengan kerusakan jaringan ginjal akibat proses nefritik dan hipertensi sehingga menimbulkan gangguan fungsi yang irreversible.
Dapat terjadi pada setiap usia, tetapi paling banyak pada dekade kedua hingga kelima. Tidak ada perbedaan pada jenis kelamin kecuali pada membranosa idiopathica, yang lebih sering ditemukan pada pria.
Kebanyakan GN kronik timbul secara samar-samar dan ditemukan hanya pada perjalanan lanjut.
GLOMERULONEFRITISKRONIK

Mikroskopik :- Kelainan glomerulus dapat terjadi karena proses nefritik dan oleh
hipertensi dan penyempitan vaskuler.- Tubulus biasanya atrofik atau menghilang (tubular loss) dan diganti oleh
jaringan ikat.- Interstisium menunjukkan penambahan jaringan ikat dan bersebukan sel
radang menahun. Beberapa kelompok tubulus yang berdilatasi dapat ditemukan.
- Arteri berukuran sedang dan kecil menunjukkan penebalan hialin pada intima dan media. Derajat kelainan vaskuler biasanya sesuai dengan kerasnya hipertensi dan perjalanan klinik.
Makroskopik :
Tampak ukuran ginjal biasanya mengecil (secondarycontracted kidney) dan simpai melekat sangat erat; bila dikupas terjadi dekortikasi. Permukaan luar granuler tidak teratur dan bopeng. Pada penampang kortex tampak menyempit.

Dapat dilihat pada gambar ini adalah ginjal yang mengalami atrofi dengan korteks yang menipis. Kenaikan serum kreatinin dan urea dapat digunakan sebagai tanda. Kebanyakan pasien juga mengalami hipertensi. Pada gambar diatas juga dapat di lihat kista kecil.

SLE merupakan penyakit sekunder ( sistemik ) yang berkaitan
dengan imunologik. SLE merupakan penyakit sistemik yang mengenai berbagai organ
seperti kulit, sendi, membran serosa, jantung dan paru, dimana
ginjal ikut terkena pada 70% kasus Sindrom klinik yang berhubungan dengan SLE yaitu :
1. Sindrom Nefrotik
2. Sindrom Nefritis
3. Sindrom Klinikopatologi
4. Glomerulonefritis Kronis ( GN Kronis )
5. Glomerulonefritis Fokal ( Proliferatif )
SISTEMIK LUPUSERITEMATOSUS (SLE)

Umum ditemukan penyakit glomerulus yang berhubungan dengan sistemik lupus erimatosus (SLE). Lupus nephritis mempunyai banyak manifestasi morfologis yang dapat ditemukan dengan renal biopsi. Umumnya, semakin banyak deposit kompleks imun maka semakin banyak ditemukan proliferasi seluler dan penyakit bertambah berat. Pada gambar ini dijumpai desposisi kompleks imun yang berat pada membran kapiler glomerulus yang menebal sehingga disebut gambaranwire-loop.

Nefropati diabetik (komplikasi diabetes) merupakan komplikasi menahun diabetes.
Kira-kira setelah 15 tahun menderita diabetes maka 10-30% penderita akan menunjukan gejala komplikasi ginjal.
Gejala paling awal adalah ditemukan protein dalam urin (proteinuria).
Bila proteinuria terjadi sangat hebat maka penderita dapat menderita kekurangan protein dalam darah yang mengakibatkan timbulnya sembab seluruh tubuh (sindroma nefrotik).
Bila penyakit terus berlangsung akhirnya timbul gagal ginjal terminal yang memerlukan pengobatan cuci darah atau cangkok ginjal.
DIABETES MELITUS

Gambaran histologis glomeropati diabetikum adalah penebalan dinding kapiler dan terjadi ekspansi matriks mesangial yang mengenai kapiler


Kidney diseases that involve structures in the kidney outside the glomerulus. These diseases generally involve tubules and/or the interstitium of the kidney
and spare the glomeruli. Tubulointerstitial nephritis (TIN)--is a group of inflammatory diseases of the
kidney that primarily involve the interstitium and tubules. Pyelonephritis ( pyelo means pelvis)-- tubulointerstitial nephritis with pelvis and
calyceal involvement.
Tubulointerstitial diseases??

Acute - usually suppurative inflammation involving pelvicalyceal system and parenchyma.
Chronic - involvement of pelvicalyceal system and parenchyma with prominent scarring.
Pyelonephritis

Acute pyelonephritis :mainly caused by bacterial infectionUrinary tract infection (Proteus,Klebsiella,Enterobacter, Pseudomonas,Stapylococcus albus).
Invasive procedure :eg.cystoscopy,catheterization.
GENDER--Incidence higher in women due to short urethra ( Ratio 1: 20) AND due to close proximity of urethra to anus.
Vesicourethral reflux Pregnancy DM,immunosuppression,immunodefisiency.
Aetiology of acute pyelonephritis


Ascending infectionBacteria from the LUT KIDNEYUrethral instrumentation (catheterization, cystoscopy ) act as a
predisposing factor. Hematogenous spread
Less commonsepticemia or infective endocarditis kidney
ObstructionOutflow obstruction or bladder dysfunction Causes incomplete emptying and increase residual volume
bacteria multiply without disturbance ascend upwards to infect the kidney Non obstructiveIncompetence of Vesicourethral orifice allows bacteria toascend the ureter into the pelvis of kidney (vesicourethralreflux)
Pathogenesis

Pain at the costovertebral angle Chills,fever and malaise Dysuria,frequency,urgency Urethral irritation Urinary findings from laboratory test
showing pyuria,bacteriuria.
Sign and symptoms

MORPHOLOGY(Gross)
Kidney, acute pyelonephritis - Gross, outer and cut surfacesNote: numerous, punctate, yellow foci over the cortical surface.
Question !! what is foci?? what are this foci composed of histologically??

It is a chronic tubulointerstitial inflammation involving renal parenchyma, pelvis and calyces associated with scarring.
non-obstructivereflux nephropathy
Obstructiveposterior urethral valves
Chronic pyelonephritisaetiology

Chronic obstructive pyelonephritisChronic obstruction Outflow obstruction (congenital /acquired) recurrent infection renal inflammation and renal scarring chronic pyelonephritis.
*congenital anomalies eg. Posterior urethral valves.*acquired eg.benign prostatic hyperplasia,stones.
Chronic reflux-associated pyelonephritis(Reflux nephropathy)more common cause of chronic pyelonephritiscongenital vesico urethral refluxreflux maybe bilateral/unilateral
Incompetence of Vesicourethral orifice allows bacteria toascend the ureter into the pelvis of kidney chronic reflux chronic pyelonephritis
Chronic pyelonephritis phatogenesis

Morphology
1.Kidney, chronic pyelonephritis 2. Kidney, chronic
pyelonephritis - Very low power The cortical surface correlates with the gross appearance, demonstrating elevations and depressions. The calyx appears dilated and deformed, and there is too much fibrous tissue in the interstitium.

Interstitial fibrosis Dilated,cast filled tubules Chronic inflammation.

Chronic inflammatory cells

1.Many dilated "colloid"-filled tubules are present. This phenomenon is known, appropriately enough, as thyroidization of the kidney. 2.markedly thickened arterial wall in the lower right of the image.

Laboratory test Pyuria and bacteriuria
USG to determine size and shape of
the kidney
Pyelogram is characteristis because it shows
the affected kidney to be assymetrically
Diagnosis

Acute drug induced tubulointerstitial nephritisadverse reaction to a drug ,begins abruptly, In most instances, occurs within days of exposure to the offending drug. Eg.* Antibiotics (eg, penicillins, cephalosporins, sulfa drugs, quinolones) ,
* NSAIDs * Diuretics (eg, thiazides, furosemide) * Allopurinol * Phenytoin * Rifampin * Interferon alfa
Drug induced interstitialnephritis
Chronic tubulointerstitial nephritis an insidious disease and most probably
represents the common final response pattern of the kidney to a variety of insults and agents.eg. Lead,drugs,(cyclosporine, cisplatin, and lithium) and metabolic disorders (hypercalcemia, and hyperoxaluria)Because of its insidious nature, chronic tubulointerstitial

Pathogenesis

Sign and symptoms
** A unique feature of allergic interstitial nephritis caused by NSAIDs is that patients may present with nephrotic syndrome. In such patients, massive proteinuria with hypoalbuminemia and edema are present in addition to the typical features of acute interstitial nephritis

Morphology
Abnormality in the interstitium. - pronounced edema - infiltration of inflammatory cell.

Acute tubular necrosis
Phatologically-destruction of tubular cell Clinically-acute suppression of renal failure. commonest cause of acute renalfailure Can be reversible with proper management. develops due to :
- direct poisoning of tubules (nephrotoxic lesions)
- renal ischemia (tubulorrhexic lesions)

Etiology & Pathogenesis
Ischemic in origin (Tubulorrhexic lesion)Prolonged ischemia due to :
1. Shock : postoperative, intra-operative, post-traumatic, septic,
hypotensive
2. Hemorrhage: postpartum hemorrhage, abruptio placentae
3. Other: severe burns, transfusion accidents, dehydration, heat stroke, crushing
injuries, non-traumatic rhabdomyolysis, paroxysmal
hemoglobinuria etc.

Direct effects of toxins (Nephrotoxic
lesion)Therapeutic agents : Antibiotics : Aminoglycosides, NSAIDs, chemotherapeutic agents, etc. Heavy metals: mercury, lead, gold etc. Radio contrast agents Multiple bee stings, scorpion bites etc
continuation


bilaterally enlarged & swollen kidney due
to edema Cut surface bulges and has a flabby
consistency widened & pale cortex dark & congested medulla
Gross pathology


dilated lumen with flattened epithelial cells Greatest change in proximal tubules, varies in two
forms1. loss of brush borders- proximal tubules2. evidence of regeneration of epithelial cells
hyaline, granular and pigmented casts interstitial edema & inflammation Intra-vascular collection of nucleated


depends upon underlying cause, over all mortality rate » 50%
post-traumatic (62%), post-operative (56%), medical (46 %), obstetric (17%)
Higher in older debilitated pts. & in pts.with multiple organ disease
good for uncomplicated and younger patients


RENALCIRCULATION
The renal circulation receives around 20% of the cardiac output.
It branches from the abdominal aorta and returns blood to the ascending vena cava.
It is the blood supply to the kidney, and contains many specialized blood vessels.



Renal artery stenosis-caused by atherosclerosis, fibromuscular dysplasia, Takayasu's arteritis (inflammatory of aorta and its branches), & posttransplantation stenosis.Symptoms :^ sudden onset of hypertension : before age 50 fibromuscular dysplasia-related stenosis after age 50 stenosis caused by atherosclerosis^ hypertension not responsive to 3/> blood pressure medications
^ increased urea in the blood^ unexplained kidney failure^ sudden kidney failure when first taking an angiotensin-converting enzyme (ACE) inhibitor medication for blood pressure and/or heart

A renal artery aneurysm- bulging, weakened area in the wall of an artery to the kidney small (<2cm) & discovered during diagnostic procedures.
Symptoms : generally asymptomatic hypertension >90% of persons with a renal artery
aneurysm dissecting aneurysms (caused by a tear in the inner
layer of the artery wall) flank pain and blood in the urine

Atheroembolic renal disease- a piece of plaque from the aorta / large arteriesbreaks off travels through the bloodstream blocking small arteries; renal arteries renal insufficiency in the elderly.Symptoms :- diarrhea - weight loss- confusion - fever- skin lesions; purpura - kidney failure- abdominal pain - muscle aches- mottling of the toes and feeta) Renal artery thrombosisb) Renal vein thrombosis

NEPHROSCLEROSIS

BENIGNNEPHROSCLEROSIS
Common in : Patients with end-stage renal diseasePathogenesis:Chronic hypertension damages small blood vessels, glomeruli, renal tubules, and interstitialTissues progressive renal failure : * Atrophic kidney finely granular surface (grain leather or pig skin) * Ischemic atrophy glomerulosclerosis, tubular atrophy, and interstitial fibrosis In arteries reduplication of the internal elastic lamina medial smooth muscle hyperplasia
Symptoms & Signs:
kidney function chronic renal failure develop
protein levels in the urine.
Signs of hypertension-related end-organ damage vasculature of the
eyes, skin, CNS, and periphery

Benign nephrosclerosis : the smaller arteries become thickened and narrowed leads to patchy ischemic atrophy focal loss of parenchyma granular appearance.
Arteriolar hyalinosis; insudation of plasmproteins & medial thickening


MALIGNANTNEPHROSCLEROSIS
Common in : blacks than whites.men during their 40s and 50swomen during their 30s.
Symptoms :headaches, nausea, vomiting, visual impairment(scotomas = spots).

Malignant nephrosclerosis focal smallhemorrhages due to essential hypertension(>300/150 mm Hg)


CHARACTERISTIC LESIONS

DIAGNOSIS
Physical examination :Benign nephrosclerosis: signs of decreased kidney function and have
elevated protein levels in the urine.Malignant nephrosclerosis: severe high blood pressure, kidney failure,
and visual disturbances. Ophthalmoscope damaged blood vessels in the back of the eye,
including bleeding, swelling, and a build-up of fluid. The heart may also be enlarged. Urine tests will show high levels of protein and clumps of red blood
cells. Blood tests high levels of a protein called renin produced by the
kidneys help control blood pressure. Computed tomography (CT) scan rule out other disorders that can
cause similar symptoms.

THROMBOTICMICROANGIOPATHIES
Pathogenesis & symptoms : Classic (Childhood) Hemolytic Uremic Syndrome :
Verocytotoxin-producing E. Coli Sudden onset after a gastrointestinal or flu-like prodromal episode of bleeding manifestations (hematemesis and melena) severe oliguria, hematuria, microangiopathic hemolytic anemia prominent neurological changes.
Adult Hemolytic Uremic Syndrome:Associated with infection & pregnancySecondary :
a. sclerodermab. systemic lupus erythematosusc. malignant hypertensiond. chemotherapeutic and immunosuppressive drugs(mitomycin & cyclosporin)
Thrombotic Thrombocytopenic Purpura :1. fever2. neurologic symptoms3. hemolytic anemia4. thrombocytopenia


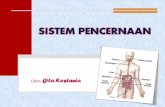
Dilatasi pelvis renalis dan calyces Atrofi progresif dan pembesaran kistik
ginjal Pelebaran ureter Dapat terjadi bilateral atau unilateral
tergantung tempat obstruksi
Hydronephrosis



Umumnya disebabkan obstruksi saluran air kemih
Obstruksi dapat terjadi pada setiap tempat dimulai dari ujung distal uretra sampai pelvis
Bersifat sebahagian sampai total Dapat berupa kelainan bawaan atau didapati
ETIOLOGI

A)Obstruksi
i) pada saluran kemih: katub kongenital pada uretra posterior, batu dan tumor
pelvis renalis
ii) pada dinding saluran kemih: hipertrofi pada dinding setempat, sriktura ureter
iii) dari luar yang menekan saluran kemih: tumor sekitar saluran kemih,hiperplasia
prostate, ateri renalis menekan ureter

B) Kelainan neuromaskular- misal nya akibat spina bifida, paraplegi, tabes
dorsalis, sklerosis multipel.
C) Kehamilan- terutama jelas pada primipara, terjadi pelebaran
fisiologik pada ureter dan pelvis, tekanan mekanik akibat uterus membesar.
D) Idiopatik

GAMBARAN MAKROSKOPIK
Ginjal tampak besar
Pelvis dan calyces melebar
Papil-papil mendatar serta membentuk cangkir,kistik kecil-kecil, multilokuler dan berhubungan dengan calyces dan pelvis melalui lubang-lubang yang lebar
Kortex lambat laun menipis dan atrofi, akhir nya berupa pita tipis

Ultrasonographic picture taken from a patient with left ureteral stone with hydronephrosis.


Tampak dilatasi pada susunan tubulus dengan sel epitel tubulus yang menjadi gepeng
Glomerulus tidak terjejas
Dilatasi mengenai tubuli recti
Tingkat lebih lanjut tubulus dan glomerulus menjadi atrofi dan diganti dgn jaringan ikat kemudian menghilang.
GAMBARAN MIKROSKOPIK

Flank pain Abdominal mass Nausea and vomiting Urinary tract infection Fever Dysuria Increased urinary frequency Increased urinary
SIMPTOM

UNILATERAL BILATERAL
DIAGNOSA

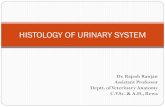
Papillary Carcinoma- Bladder
• Papillary carcinoma of urinary bladder
• grows outward rather than in
• Muscle layer is preserved
• Papillary projections – very diagnostic

Pyelonephritis
Pyonephrosis
Pyoureter
Gagal ginjal
KOMPLIKASI

i) Obstruksi akut pada saluran kemih bagian atas :- Insersi tuba nephrostomy
ii) Obstruksi kronik pada saluran kemih bagian atas:- Insersi ureteric stent atau pyeloplasty
iii) Obstruksi saluran kemih bagian bawah : - Insersi urinary catheter atau suprapubic catheter
PENGOBATAN

RENAL CYST
Cysts may be solitary or multiple, congenital or
acquired. A solitary cyst may stimulate a tumour. Congenital polycystic disease may not present
until adult life. Acquired cysts may be due to renal scarring.

TCC of Ureter
• Same system of grading and staging.
• Often bleed and see in urine

TCC of renal pelvis

• Lower urinary tract
• Pelvis, Ureters, Bladder& Urethra – lined by transitional epithelium (urothelium) – 2 to 3 cells thick - pelvis– 3 to 5 cells thick - ureters,– 3 to 7 cells thick - bladder– surface layer of flattened "umbrella cells"– apical plaques composed of specific proteins called uroplakins– Nests of urothelium or in-budding of the surface epithelium into the
mucosa lamina propria called as Brunn nests

• Ureters • retroperitoneal position• Retroperitoneal tumors or fibrosis trap and obstructing ureters• In female, lie close to the uterine arteries • 3 points of slight narrowing: – Uretero-pelvic junction– enter the bladder– cross the iliac vessels
Renal calculi may become impacted • Congenital anomalies• 1. Double ureters (derived from a double or split ureteral bud)
• 2. Uretero -pelvic junction obstruction– results in hydronephrosis (MCC)– presents in infants or children
• More in boys on left side

• 3. Diverticula= outpouchings of the ureteral wall & asymptomatic• 4. Dilation (hydroureter)= elongation, and tortuosity
a) Congenital hydroureter • neurogenic defect in the innervation of the ureteral musculature.
b) Megaloureter = Massive enlargement of the Ureter • due to a functional defect of ureteral muscle
• Inflammations = Ureteritis– component of UTI
• Forms of chronic ureteritis = ureteritis cystica ( Mucosa forms fine cysts, ureteritis follicularis small, grapelike clusters on granular mucosal surface)
• Tumors • Benign tumors
– Mesenchymal origin and most common are • fibro epithelial polyps and leiomyomas• more often on Left side
• Primary malignant tumors– TCC ( 6th – 7th decades of life, similar to those in renal pelvis calyces, and
bladder)

Ureteritis cystica

UreterOBSTRUCTIVE LESIONS
Intrinsic
Calculi Of renal origin, rarely more than 5 mm indiameter
Larger renal stones cannot enter ureters
Impact at loci of ureteral narrowing-ureteropelvic junction, where ureters crossiliac vessels, and where they enter bladder-and cause excruciating "renal colic"
Strictures Congenital or acquired (inflammations)
Tumors Transitional cell carcinomas arising in ureters
Rarely, benign tumors or fibroepithelial polyps
Blood clots Massive hematuria from renal calculi, tumors, orpapillary necrosis
Neurogenic Interruption of the neural pathways to the bladder

UreterOBSTRUCTIVE LESIONS
Extrinsic
Pregnancy Physiologic relaxation of smooth muscle or pressure on ureters at pelvic brim from enlarging fundus
Periureteral inflammation Salpingitis, diverticulitis, peritonitis, sclerosing retroperitoneal fibrosis
Endometriosis With pelvic lesions, followed by scarring
Tumors Cancers of the rectum, bladder, prostate, ovaries, uterus, cervix, lymphomas, sarcomas

• Sclerosing Retroperitoneal Fibrosis - URETERS• uncommon cause of ureteral narrowing or obstruction • leads to hydronephrosis in middle to late age• Causes– primary or idiopathic (Ormond disease)• 70% of cases no obvious cause• similar fibrotic changes in other sites (referred to as
mediastinal fibrosis, sclerosing cholangitis, and Riedel fibrosing thyroiditis
– Drugs (ergot derivatives, β-adrenergic blockers)– Adjacent inflammatory conditions (vasculitis, diverticulitis,
Crohn disease)– Malignant disease (lymphomas, urinary tract carcinomas).

• Urinary Bladder • Congenital anomalies • Diverticula= out pouchings
– Congenital– Acquired - with Prostatic enlargement – Complications = Infection, calculi, Rarely- carcinomas
• Exstrophy= developmental failure in the anterior wall of the abdomen and the bladder
• Increased risk of adenocarcinoma of the colon and bladder adenocarcinoma• Persistent urachus = connects the bladder with the umbilicus • Increased risk of cancers resembling colonic adenocarcinomas• CYSTITIS = inflammation of urinary bladder • Causes = Infections (MCC): E. coli, Proteus, TB, Candida, Chlamydia
• uncommon - Schistosomiasis– Radiation & chemotherapy – Prolonged catheterization
• Morphologic Types: – Acute or Chronic:

• Cystitis Special Forms • 1. Interstitial Cystitis (Hunner’s ulcer)
– Characterized by:• Painful chronic cystitis = dysuria • MC seen in women• Ulcers with inflammation & granulation tissue involving all layers• no bacterial infection • Mast cells are prominent• Unknown cause ( difficult to Rx)
• 2. Malacoplakia =Peculiar pattern of Cystitis • Characterized by = soft, yellow, slightly raised mucosal plaques• Pathogenesis= acquired defect in phagosome degradation• Histology = large, foamy macrophages , multinucleate giant cells and
interspersed lymphocytes • Michaelis - Gutmann bodies = Laminated mineralized concretions• Related to E.coli & Proteus infections
• 3. Squamous Metaplasia = response to injury– Stone in the bladder causes irritation leading to squamous cell carcinoma

Malacoplakia
macrophages withPAS positive cytoplasm
Michaelis-Gutmann bodies

Urethra INFLAMMATIONS• Gonococcal and nongonococcal urethritis• often accompanied by– cystitis in women – prostatitis in men
• Nongonococcal = Chlamydia & Mycoplasma• 25% to 60% of nongonococcal urethritis in men • 20% in women
• Reiter syndrome- triad of arthritis, conjunctivitis, and urethritis• Urethral caruncle = inflammatory lesion at external urethral
meatus in the female – extremely friable = break and bleed – cause ulceration of the surface and bleeding.– Surgical excision - cure

Occasionally, a simple renal cyst can reach a large size and mimic a tumor mass, though the difference is usually obvious with radiographic procedures. Such a large cyst can be complicated by hemorrhage or rupture.

Simple renal cysts Autosomal dominant polycystic kidney disease Autosomal recessive polycystic kidney disease Congenital nephrotic syndrome Renal dialysis-associated
Cysts in the kidney are classified as :



Autosomal dominant polycystic kidney disease affects up to 1 in 1000 people.
A definite diagnosis of ADPKD relies on imaging or molecular genetic testing.

AUTOSOMAL RECESSIVE(CHILDHOOD) POLYCYSTIC
Rare developmental anomaly Mutations in an unidentified gene localized to chromosome 6p Subcategories: perinatal, neonatal, infantile, juvenile Perinatal & neonatal : most common, Manifestation : present at birth,
young infants may die quickly from pulmonary or renal failure. Kidney : numerous small cysts in cortex & medulla, spongelike
appearance affect both kidney. Most cases : + multiple epithelium lined cysts in liver & proliferation of
portal bile ducts Patients who survive infancy will develop liver cirrhosis (congenital
hepatic fibrosis)