URGENZE ADDOMINALI NEI PAZIENTI TRAPIANTATI · PDF file“It is now estabilished that...
19
URGENZE ADDOMINALI NEI PAZIENTI TRAPIANTATI L’addome acuto nei pazienti con trapianto renale Dr. Sergio SANTELLA U.O. Chirurgia Generale e d’Urgenza Direttore Dr. Francesco BUCCOLIERO Roma 15 Ottobre 2014 Ospedale M. Bufalini - Cesena
Transcript of URGENZE ADDOMINALI NEI PAZIENTI TRAPIANTATI · PDF file“It is now estabilished that...

URGENZE ADDOMINALI NEI PAZIENTI TRAPIANTATI L’addome acuto nei pazienti con trapianto renale
Dr. Sergio SANTELLA U.O. Chirurgia Generale e d’Urgenza Direttore Dr. Francesco BUCCOLIERO
Roma 15 Ottobre 2014
Ospedale M. Bufalini - Cesena

Roma 15 Ottobre 2014
Ospedale M. Bufalini - Cesena GENERAL MED IC INE / R EV I EW ART I C L E
Care of the Renal Transplant Recipient in the
Emergency Department
KK Venkat, MDArvind Venkat, MD
From the Division of Nephrol-ogy, Department of Medicine,Henry Ford Hospital, Detroit,MI (KK Venkat); and the De-partment of Emergency Medi-cine, University of CincinnatiCollege of Medicine, Cincinnati,OH (A Venkat).
0196-0644/$30.00
Copyright ! 2004 by the AmericanCollege of Emergency Physicians.
doi:10.1016/j.annemergmed.2004.05.019
End-stage renal disease is becoming more common in the United States because of theaging of the population and the increased prevalence of predisposing conditions suchas diabetes and hypertension. Renal transplantation is the preferred treatment forpatients with end-stage renal disease. This article reviews the medical problems thatmight bring renal transplant recipients to the emergency department, the informationemergency physicians should be aware of in evaluating and treating these patients, andthe critical importance of close communication between emergency and transplantphysicians in treating them.
[Ann Emerg Med. 2004;44:330-341.]
I N T R O D U C T I O N
It is now established that renal transplantation is the best therapy for end-stage renaldisease.1-3 Renal transplantation offers a better quality of life and confers greater longevitythan long-term dialysis. The susceptibility of renal transplant recipients to a variety ofurgent and serious medical problems is well known to emergency physicians. Renaltransplantation in the elderly is becoming more common, and transplant programs areincreasingly accepting patients with significant comorbidities for transplantation.4,5
Diabetic nephropathy accounts for approximately 40% of the diseases leading to renaltransplantation.6 Diabetic patients are significantly more prone to complications afterrenal transplantation. Because of organ shortage, the waiting period for cadaverictransplantation is increasing, which adds to the dialysis-related comorbidities in patientsat transplantation.7 The currently available immunosuppressive drugs are more potentthan those available in the past. Although this availability has resulted in a lower incidenceof rejection, it has contributed to a greater incidence of medication-related problems.8
These factors are likely to increase the utilization of emergency medical services by renaltransplant recipients.
Medical care of renal transplant recipients in the emergency department (ED) posesa number of challenges. The spectrum of medical complications in this population isdifferent from that in the general population. Also, the classical presentation of commonmedical disorders may be modified by immunosuppressive medications. Adverse effects ofthe immunosuppressants may cause unusual problems that may not be recognized asmedication related. The commonly used antirejection medications have a number of druginteractions that, if not recognized, may lead to serious complications. It is essential thatemergency physicians have a good understanding of the special factors involved in treatingrenal transplant recipients. In this review, we present a discussion of these factors and
3 3 0 ANNALS OF EMERGENCY MEDIC INE 44 : 4 OCTOBER 20 04
Roma 15 Ottobre 2014
Ospedale M. Bufalini - Cesena
“It is now estabilished that renal transplantation is the best theraphy for end-stage renal disease. Renal transplantation offers a better quality of life and confers greater longevity than long-term dialysis. Diabetic nephropathy accounts for approximately 40% of the disease leading to renal transplantation. Diabetic patients are significantly more prone to complications after renal transplantation.
Venkat, Ann Emerg Med 2004

Roma 15 Ottobre 2014
Ospedale M. Bufalini - Cesena
Medical problems that might bring renal transplant recipients to the Emergency Department. Ø Immunosoppressive medications; Ø Renal and urinary tract problems; Ø Surgical complications affecting the allograft; Ø Fever; Ø Cardiovascular disorders; Ø Hypertensive urgencies and emergencies; Ø Pulmonary problems; Ø Gastrointestinal problems; Ø Hepatobiliary and pancreatic disorders; Ø Neurologic and psychologic disorders; Ø Hematologic disorders; Ø Muscoloskeletal and articular complications; Ø Cutaneous problems; Ø Common electrolyte abnormalities; Ø New-onset posttransplant diabetes mellitus; Ø Stress-dose corticosteroid coverage.
Venkat, Ann Emerg Med 2004

Roma 15 Ottobre 2014
Ospedale M. Bufalini - Cesena
Renal and urinary tract problems in renal transplant recipients Ø Acute renale failure:
• Acute cyclosporine or tacrolimus nephrotoxicity; • Acute rejection; • Differentiation between these 2 disorders may be difficult without allograft biopsy; • Ultrasonography of the allograft may demonstrate hydronephrosis (urgent
percutaneous nephrostomy) or peritransplant fluid collection; • Doppler ultrasonography may demonstrate lack of blood flow (prompt surgical
exploration to salvage the transplant); Ø Chronic allograft nephropaty (chronic rejection):
• Recurrence of native renal disease; • Development of de novo renal disease in the kidney transplant;
Ø Gross or microscopic hematuria; Ø Urinary tract infection.
Venkat, Ann Emerg Med 2004

Roma 15 Ottobre 2014
Ospedale M. Bufalini - Cesena
Surgical complications affecting the allograft Ø Acute occlusion of the transplant renal artery or vein:
• Doppler ultrasonography or radioisotopic scanning demonstrate lack of blood flow (prompt surgical exploration may result in salvage of the allograft in a small fraction of patients);
Ø Peritransplant hematomas: • Early post-operative complication or in the setting of perioperative anticoagulation; • Rarely, severe acute reject may cause swelling and rupture of the transplanted
kidney; CT scan is the best diagnostic test. Immediate surgical exploration is required and usually leads to allograft nephrectomy;
Ø Urinary leak: • Urine extravasation and acute renal failure, caused by the disruption of the ureteric
anastomosis to the bladder; it is best diagnosed by the demonstration of a peritransplant fluid collection on sonography. Institution of Foley catether drainage, followed by prompt surgical intervention, is required.
Venkat, Ann Emerg Med 2004

Roma 15 Ottobre 2014
Ospedale M. Bufalini - Cesena
Surgical complications affecting the allograft Ø Lymphocele:
• Asymptomatic, incidentally detected during ultrasonography: conservative treatment; • Larger symptomatic (pain over the allograft, acute renal failure by pressure on the
ureter, urinary frequence by pressure oon the bladder, lower-extremity edema by pressure of the iliac veins): percutaneous drainage;
Ø Obstructive uropathy: • In the early posttransplant period the common cause is a technical problem with the
ureteric anastomosis to the bladder; stenosis of the transplanted ureter as a result of ischemia or previous rejection, may cause obstruction months or years after transplant. The best diagnostic test is the documentation of hydronephrosis by ultrasonography. Percutaneosus nephrostomy of the allograft, followed by anterograde stenting through the nephrostomic tube. Elective surgical correction of the obstruction is usually required;
Ø Bleeding after renal allograft biopsy: • Severe hematuria may require blood transusion and angiographic embolization of
bleeding vessel.
Venkat, Ann Emerg Med 2004

Roma 15 Ottobre 2014
Ospedale M. Bufalini - Cesena
Gastrointestinal, hepatobiliar and pancreatic disorders. Ø Disorders of the gastrointectinal tract are common after renal transplantation, occurring in 3%
to 30% of recipients, and may affect any part from the oral cavity to the large bowel. Ø The severity of acute abdominal conditions such as upper gastrointestinal
perforation or colonic diverticular rupture may be blunted by immunosuppressants, such as corticosteroids.
Ø Even apparently mild pain should be prompt imaging studies such as an acute abdominal series or CT scanning in renal transplant recipients.
Ø Abnormalities in liver function tests occur frequently in renal transplant recipients. Ø The clinical presentation of acute cholecystitis may be blunted by
immunosuppressive therapy, especially corticosteroids. Ø The incidence and severity of acute pancreatitis appear to be increased in renal
transplant recipient.
Venkat, Ann Emerg Med 2004

Roma 15 Ottobre 2014
Ospedale M. Bufalini - Cesena
highlight the complexity of caring for these patients,which necessitates close communication between emer-gency and transplant physicians.
S U R G I C A L A N A T O M Y O F K I D N E Y
T R A N S P L A N T A T I O N
The transplanted kidney is placed in the right or left lowerquadrant of the abdomen. Except in obese persons, thetransplant is easily palpable on abdominal examination.The transplant renal artery is anastomosed to theipsilateral internal or external iliac artery, the renal vein tothe internal or external iliac vein, and the transplant ureterto the bladder.9 Generally, a single kidney is transplanted.When small, pediatric, or older cadaveric donor kidneyswith age-related loss of renal function are transplanted,both kidneys from a donor might be placed in a singlerecipient to provide adequate functional renal mass.
Unlike living donor transplants that functionimmediately after transplant, approximately 30% ofcadaveric transplants have delayed graft function becauseof more prolonged ischemic cold preservation.10 Con-tinued dialytic support is required until delayed graftfunction resolves.
I M M U N O S U P P R E S S I V E M E D I C A T I O N S
Renal transplant recipients require lifelongimmunosuppression to prevent rejection. Before 1983,immunosuppression consisted of a combination of
azathioprine and corticosteroids. The cyclosporine erabegan in November 1983. Themost popular cyclosporine-based regimen is ‘‘triple’’ therapy with cyclosporine,azathioprine, and corticosteroids.8 Since the mid-1990s,the number of available immunosuppressants hasincreased. Current ‘‘triple’’ regimens include cyclosporine-microemulsion or tacrolimus, mycophenolate mofetil orazathioprine, and corticosteroids.11 Sirolimus becameavailable in 1999, and its incorporation intoimmunosuppression protocols is evolving.12
Immunosuppressant minimization protocols are be-coming increasingly popular. These protocols involve‘‘triple’’ therapy for 3 to 12 months after transplant,followed by withdrawal of 1 of the 3 drugs to minimizelong-term adverse effects.13 The most commonly with-drawn drug is corticosteroids. Thus, a patient presentingto the ED may be receiving a combination of 2 drugs only.Comments in the rest of this article about the effects ofcorticosteroids apply only to patients indefinitely receiv-ing this drug. Table 1 shows the doses and target bloodlevels of currently available immunosuppressants. Drugadverse effects are presented in Table 2.
In addition to the above maintenance agents, antilym-phocyte antibodies are widely used in renal transplantrecipients.14,15 Information on these antibodies is pre-sented in Table 3. Initial therapy of rejection involves theadministration of intravenous corticosteroids (methyl-prednisolone 250 to 1,000 mg daily for 3 days ordexamethasone 100 mg daily for 3 days).16 Sudden death,probably because of serious cardiac arrhythmias, has been
Table 1.Currently approved maintenance immunosuppressive medications.
Medication Typical Dose Initial/Maintenance Target Blood Level (Trough)
Cyclosporine (Sandimmune or generic) 5–6 mg/kg PO Q12; maintenance dosedetermined by blood level
250–400 ng/mL (initial)125–200 ng/mL (long term)
Cyclosporine microemulsion (Neoral orgeneric)
4–5 mg/kg PO Q12; maintenance dosedetermined by blood level
250–400 ng/mL (initial)125–200 ng/mL (long term)
Tacrolimus (Prograf) 0.1 mg/kg PO Q12; maintenance dosedetermined by blood level
10–20 ng/mL (initial)5–10 ng/mL (long term)
Azathioprine (Imuran or generic) 1.5–2.5 mg/kg PO QD (adjusted for bloodcounts)
Blood level monitoring not used in clinicalpractice
Mycophenolate mofetil (CellCept) 1.0–1.5 g PO Q12 (adjusted according togastrointestinal adverse effects and bloodcounts)
Blood level monitoring not used in clinicalpractice
Prednisone, prednisolone,methylprednisolone
0.5 mg/kg/day (initial)0.1 mg/kg/day (long term)
Blood level monitoring not used in clinicalpractice
Sirolimus (Rapamune) 2–5 mg PO QD (adjusted according to level) 10–20 ng/mL (initial)5–15 ng/mL (long term)
PO, By mouth; Q12, every 12 h; QD, once daily.
CARE O F RENAL TRANSP LANT REC I P I ENTS IN TH E EMERGENCY DEPARTMENT Venkat & Venkat
OCTOBER 200 4 44 : 4 ANNALS OF EMERGENCY MEDIC INE 3 3 1highlight the complexity of caring for these patients,which necessitates close communication between emer-gency and transplant physicians.
S U R G I C A L A N A T O M Y O F K I D N E Y
T R A N S P L A N T A T I O N
The transplanted kidney is placed in the right or left lowerquadrant of the abdomen. Except in obese persons, thetransplant is easily palpable on abdominal examination.The transplant renal artery is anastomosed to theipsilateral internal or external iliac artery, the renal vein tothe internal or external iliac vein, and the transplant ureterto the bladder.9 Generally, a single kidney is transplanted.When small, pediatric, or older cadaveric donor kidneyswith age-related loss of renal function are transplanted,both kidneys from a donor might be placed in a singlerecipient to provide adequate functional renal mass.
Unlike living donor transplants that functionimmediately after transplant, approximately 30% ofcadaveric transplants have delayed graft function becauseof more prolonged ischemic cold preservation.10 Con-tinued dialytic support is required until delayed graftfunction resolves.
I M M U N O S U P P R E S S I V E M E D I C A T I O N S
Renal transplant recipients require lifelongimmunosuppression to prevent rejection. Before 1983,immunosuppression consisted of a combination of
azathioprine and corticosteroids. The cyclosporine erabegan in November 1983. Themost popular cyclosporine-based regimen is ‘‘triple’’ therapy with cyclosporine,azathioprine, and corticosteroids.8 Since the mid-1990s,the number of available immunosuppressants hasincreased. Current ‘‘triple’’ regimens include cyclosporine-microemulsion or tacrolimus, mycophenolate mofetil orazathioprine, and corticosteroids.11 Sirolimus becameavailable in 1999, and its incorporation intoimmunosuppression protocols is evolving.12
Immunosuppressant minimization protocols are be-coming increasingly popular. These protocols involve‘‘triple’’ therapy for 3 to 12 months after transplant,followed by withdrawal of 1 of the 3 drugs to minimizelong-term adverse effects.13 The most commonly with-drawn drug is corticosteroids. Thus, a patient presentingto the ED may be receiving a combination of 2 drugs only.Comments in the rest of this article about the effects ofcorticosteroids apply only to patients indefinitely receiv-ing this drug. Table 1 shows the doses and target bloodlevels of currently available immunosuppressants. Drugadverse effects are presented in Table 2.
In addition to the above maintenance agents, antilym-phocyte antibodies are widely used in renal transplantrecipients.14,15 Information on these antibodies is pre-sented in Table 3. Initial therapy of rejection involves theadministration of intravenous corticosteroids (methyl-prednisolone 250 to 1,000 mg daily for 3 days ordexamethasone 100 mg daily for 3 days).16 Sudden death,probably because of serious cardiac arrhythmias, has been
Table 1.Currently approved maintenance immunosuppressive medications.
Medication Typical Dose Initial/Maintenance Target Blood Level (Trough)
Cyclosporine (Sandimmune or generic) 5–6 mg/kg PO Q12; maintenance dosedetermined by blood level
250–400 ng/mL (initial)125–200 ng/mL (long term)
Cyclosporine microemulsion (Neoral orgeneric)
4–5 mg/kg PO Q12; maintenance dosedetermined by blood level
250–400 ng/mL (initial)125–200 ng/mL (long term)
Tacrolimus (Prograf) 0.1 mg/kg PO Q12; maintenance dosedetermined by blood level
10–20 ng/mL (initial)5–10 ng/mL (long term)
Azathioprine (Imuran or generic) 1.5–2.5 mg/kg PO QD (adjusted for bloodcounts)
Blood level monitoring not used in clinicalpractice
Mycophenolate mofetil (CellCept) 1.0–1.5 g PO Q12 (adjusted according togastrointestinal adverse effects and bloodcounts)
Blood level monitoring not used in clinicalpractice
Prednisone, prednisolone,methylprednisolone
0.5 mg/kg/day (initial)0.1 mg/kg/day (long term)
Blood level monitoring not used in clinicalpractice
Sirolimus (Rapamune) 2–5 mg PO QD (adjusted according to level) 10–20 ng/mL (initial)5–15 ng/mL (long term)
PO, By mouth; Q12, every 12 h; QD, once daily.
CARE O F RENAL TRANSP LANT REC I P I ENTS IN TH E EMERGENCY DEPARTMENT Venkat & Venkat
OCTOBER 200 4 44 : 4 ANNALS OF EMERGENCY MEDIC INE 3 3 1

Roma 15 Ottobre 2014
Ospedale M. Bufalini - Cesena
“There is no evidence that asymptomatic potential transplant recipients require screening for diverticular disease, peptic ulceration or gallbladder stones.” ü Colonic perforation due to diverticular disease after renal transplantation is rare with modern immunosuppressive regimes utilizing low dose corticosteroids. Furthermore, in a retrospective study in wich all transplant candidates aged more than 50 years underwent screening, none of the patients with significant diverticular disease had symptomatic disease post-transplantation. Patient with clinically significant disease should be assessed and managed according to standard practice. ü Peptic ulceration is now rarely a serious problem and there is no published evdience from the recent era to support a role for screening and intervention before transplantation. ü Most transplant centers ignore incidental cholelitiasis and there is no published evdience from the recent era to support a role for screening and intervention before transplantation.
British Transplantation Society Guidelines

Roma 15 Ottobre 2014
Ospedale M. Bufalini - Cesena

Roma 15 Ottobre 2014
Ospedale M. Bufalini - Cesena
the diagnostic criteria for infection orsystemic inflammation should be revised,we adhere to several principles. The cri-teria should be broadly useful both toclinicians caring for patients at the bed-side and to researchers designing obser-vational studies and clinical trials to im-prove the understanding of sepsis and itsoptimal treatment. The criteria should besensitive enough to identify most patientswith the syndrome, while minimally sac-rificing inevitable specificity. The criteriashould not be so cumbersome that clini-cians will resist a commitment to mem-ory or application. Any laboratory-dependent criteria should use assays thateither are widely available now or arelikely to be generally available in the nearfuture. The criteria should be applicableto adult, pediatric, and neonatal patients.
Infection. We defined infection as apathologic process caused by the invasionof normally sterile tissue or fluid or bodycavity by pathogenic or potentially patho-genic microorganisms. This definition,essentially the same one used in the 1992document, is not perfect. For example,colitis caused by Clostridium difficile, re-sults from overgrowth of this organism inthe colon, which is certainly not sterile.Furthermore, the clinical manifestationsof C. difficile colitis are not caused by thebacteria invading normally sterile tissuesbut, rather, by the cytopathic effects of anexotoxin secreted by the organism. It isalso important to point out that, fre-quently, infection is strongly suspectedwithout being microbiologically con-firmed. Accordingly, sepsis (i.e., infectionand the systemic response to it) may onlybe strongly suspected, without being mi-crobiologically confirmed.
Systemic Inflammation in Responseto Infection. Because of the limitations ofSIRS discussed above, we included a listof possible signs of systemic inflamma-tion in response to infection (Table 1).Ultimately, this scheme seeks to codifythe physical and laboratory findings thatprompt an experienced clinician to con-clude that an infected patient “looks sep-tic.” Findings indicative of early organdysfunction may be the first symptomsnoted by clinicians when making this as-sessment. It is for this reason that weincluded findings such as hemodynamicinstability, arterial hypoxemia, oliguria,coagulopathy and altered liver functiontests among the list of criteria that can beused to establish the diagnosis of sepsis.
It is important to emphasize that noneof the findings in Table 1 is specific for
sepsis. A high cardiac output is com-monly observed following major surgicalprocedures or multiple trauma. Arterialhypotension can be caused by many con-ditions other than sepsis, such as acuteleft ventricular failure secondary to AMIor hemorrhage. Coagulopathy can bedrug-induced and is associated withmany different diseases, in addition tosepsis. It is important that as a practitio-ner “checks off the boxes” to establish thediagnosis of sepsis, only findings thatcannot be easily explained by othercauses be included. The thresholds cho-sen in Table 1 merits discussion. We havenot chosen thresholds for each of thecriteria that are consistently abnormal indegree. The proposition is whetherthresholds similar in degree of abnormal-ity confer similar prediction in sepsis.
As a result, the group turned towardthe day-to-day “reality” for bedside clini-cians. Group consensus concluded that
few, if any, patients in the early stages ofthe inflammatory response to infectionare diagnosed with sepsis via four arbi-trary criteria. Instead, the clinician goesto the bedside, identifies myriad symp-toms, and regardless of an evident infec-tion, declares the patient to “look septic.”If no obvious source of infection exists,the clinician then initiates a search for aninfectious origin of the signs and symp-toms associated with sepsis. The use ofthe word “some” reflects the clinical re-ality at the bedside, rather than an arbi-trary list invented for the purpose of clin-ical trial entry criteria. Should thedefinition of sepsis reflect reality as seenat the bedside, thereby facilitating a clin-ical diagnosis, or should the definitionenable investigators to develop clear andsimple entry criteria for clinical trials? Itwas the opinion of the group that facili-tating a bedside diagnosis should haveprimacy over research entry criteria.
Table 1. Diagnostic criteria for sepsis
Infection,a documented or suspected, and some of the following:b
General variablesFever (core temperature !38.3°C)Hypothermia (core temperature "36°C)Heart rate !90 min#1 or !2 SD above the normal value for ageTachypneaAltered mental statusSignificant edema or positive fluid balance (!20 mL/kg over 24 hrs)Hyperglycemia (plasma glucose !120 mg/dL or 7.7 mmol/L) in the absence of diabetes
Inflammatory variablesLeukocytosis (WBC count !12,000 $L#1)Leukopenia (WBC count "4000 $L#1)Normal WBC count with !10% immature formsPlasma C-reactive protein !2 SD above the normal valuePlasma procalcitonin !2 SD above the normal value
Hemodynamic variablesArterial hypotensionb (SBP "90 mm Hg, MAP "70, or an SBP decrease !40 mm Hg in adults
or "2 SD below normal for age)Sv!O2 !70%b
Cardiac index !3.5 L!min#1!M#23
Organ dysfunction variablesArterial hypoxemia (PaO2/FIO2 "300)Acute oliguria (urine output "0.5 mL!kg#1!hr#1 or 45 mmol/L for at least 2 hrs)Creatinine increase !0.5 mg/dLCoagulation abnormalities (INR !1.5 or aPTT !60 secs)Ileus (absent bowel sounds)Thrombocytopenia (platelet count "100,000 $L#1)Hyperbilirubinemia (plasma total bilirubin !4 mg/dL or 70 mmol/L)
Tissue perfusion variablesHyperlactatemia (!1 mmol/L)Decreased capillary refill or mottling
WBC, white blood cell; SBP, systolic blood pressure; MAP, mean arterial blood pressure; Sv!O2,mixed venous oxygen saturation; INR, international normalized ratio; aPTT, activated partial throm-boplastin time.
aInfection defined as a pathologic process induced by a microorganism; bSvO2 sat !70% is normalin children (normally, 75–80%), and CI 3.5–5.5 is normal in children; therefore, NEITHER should beused as signs of sepsis in newborns or children; cdiagnostic criteria for sepsis in the pediatricpopulation are signs and symptoms of inflammation plus infection with hyper- or hypothermia (rectaltemperature !38.5 or "35°C), tachycardia (may be absent in hypothermic patients), and at least oneof the following indications of altered organ function: altered mental status, hypoxemia, increasedserum lactate level, or bounding pulses.
1252 Crit Care Med 2003 Vol. 31, No. 4
the development of clear and simple en-try criteria for clinical trials. Participantsbelieve that the facilitation of bedside di-agnosis should have priority over stan-dardized sepsis entry criteria for clinicaltrials. A standardized set of signs andsymptoms that may aid enrollment intorandomized trials remains to be devel-oped. Our conclusions can be summa-rized as follows (Table 3).
1. Current concepts of sepsis, severesepsis, and septic shock remain usefulto clinicians and researchers. Until fur-ther evidence arises that justifies alter-ing these categories that describe thehost response to infection, they shouldremain as described 10 yrs ago.2. These definitions do not allow forprecise staging or prognostication ofthe host response to infection.3. While SIRS remains a useful con-cept, the diagnostic criteria for SIRSpublished in 1992 are overly sensitiveand nonspecific.4. An expanded list of signs and symp-toms of sepsis may better reflect theclinical response to infection.5. The operational definitions of sepsismay be refined and tested in the futureas we increase our understanding ofthe immunologic and biochemicalcharacteristics of these conditions.6. We hypothesize that improvementsin the management of critically ill pa-tients with serious infections may fol-low the development of a staging sys-tem for sepsis that can bettercharacterize the syndrome on the basisof predisposing factors and premorbidconditions, the nature of the underly-ing infection, the characteristics of thehost response, and the extent of theresultant organ dysfunction.
The fact that no new definitions forsepsis are introduced in this conferencereport is noteworthy. This document re-flects a process whereby a group of ex-perts revisited the 1992 sepsis consensusdefinitions and found that apart from ex-panding the list of signs and symptoms ofsepsis to reflect clinical bedside experi-ence, no evidence exists to support anychange in the definitions. This lack ofevidence serves to underscore the chal-lenge for clinicians and researchers stillpresent in diagnosing sepsis in 2003 andalso provides the basis for introducingPIRO as a hypothesis-generating modelfor future research.
REFERENCES
1. Members of the American College of ChestPhysicians/Society of Crit Care Med Consen-sus Conference Committee: American Col-lege of Chest Physicians/Society of Crit CareMed Consensus Conference: Definitions forsepsis and organ failure and guidelines forthe use of innovative therapies in sepsis. CritCare Med 1992; 20:864–874
2. Marshall JC: SIRS and MODS: What is theirrelevance to the science and practice of in-tensive care? Shock 2000; 14:586–589
3. Vincent J-L: Dear SIRS, I’m sorry to say thatI don’t like you. Crit Care Med 1997; 25:372–374
4. Ramsay G, Gerlach H, Levy MM, et al: Aninternational sepsis survey: A Study of doc-tors’ knowledge and perception about sepsis.Crit Care Med 2003; 31:
5. Nomenclature and Criteria for Diagnosis ofIschemic Heart Disease: Report of the JointInternational Society and Federation of Car-diology/World Health Organization TaskForce on Standardization of Clinical Nomen-clature. Circulation 1979; 59:607–609
6. Falahati A, Sharkey SW, Christensen D, et al:Implementation of serum cardiac troponin Ias marker for detection of acute myocardialinfarction. Am Heart J 1999; 137:332–337
7. Antman EM, Grudzien C, Mitchell RN, et al:Detection of unsuspected myocardial necro-
sis by rapid bedside assay for cardiac tropo-nin T. Am Heart J 2002;133:596–598
8. Puleo PR, Meyer D, Wathen C, et al: Use of arapid assay of subforms of creatine kinase MBto diagnose or rule out acute myocardialinfarction. N Engl J Med 2002; 331:561–566
9. Myocardial infarction redefined—A consen-sus document of The Joint European Societyof Cardiology/American College of Cardiol-ogy Committee for the Redefinition of Myo-cardial Infarction. J Am Coll Cardiol 2000;36:959–969
10. Taniguchi T, Koido Y, Aiboshi J, et al:Change in the ratio of interleukin-6 to inter-leukin-10 predicts a poor outcome in pa-tients with systemic inflammatory responsesyndrome. Crit Care Med 1999; 27:1262–1264
11. Ueda S, Nishio K, Minamino N, et al: In-creased plasma levels of adrenomedullin inpatients with systemic inflammatory re-sponse syndrome. Am J Respir Crit Care Med1999; 160:132–136
12. Stoiser B, Knapp S, Thalhammer F, et al:Time course of immunological markers inpatients with the systemic inflammatory re-sponse syndrome: Evaluation of sCD14, sV-CAM-1, sELAM-1, MIP-1 alpha and TGF-beta2. Eur J Clin Invest 1998; 28:672–678
13. Hietaranta A, Kemppainen E, PuolakkainenP, et al: Extracellular phospholipases A2 inrelation to systemic inflammatory responsesyndrome (SIRS) and systemic complicationsin severe acute pancreatitis. Pancreas 2002;18:385–391
14. Takala A, Jousela I, Olkkola KT, et al: Sys-temic inflammatory response syndromewithout systemic inflammation in acutely illpatients admitted to hospital in a medicalemergency. Clin Sci (Lond) 1999; 96:287–295
15. Sablotzki A, Borgermann J, Baulig W, et al:Lipopolysaccharide-binding protein (LBP)and markers of acute-phase response in pa-tients with multiple organ dysfunction syn-drome (MODS) following open heart surgery.Thorac Cardiovasc Surg 2001; 49:273–278
16. Harbarth S, Holeckova K, Froidevaux C, et al:Diagnostic value of procalcitonin, interleu-kin-6, and interleukin-8 in critically ill pa-tients admitted with suspected sepsis. Am JRespir Crit Care Med 2001; 164:396–340
17. Duflo F, Debon R, Monneret G, et al: Alveolarand serum procalcitonin: Diagnostic andprognostic value in ventilator-associatedpneumonia. Anesthesiology 2002; 96:74–79
18. Angus DC, Linde-Zwirble WT, Lidicer J, et al:Epidemiology of severe sepsis in the UnitedStates: Analysis of incidence, outcome, andassociated costs of care. Crit Care Med 2001;29:1303–1310
19. Marshall JC, Cook DJ, Christou NV, et al:Multiple organ dysfunction score: A reliabledescriptor of a complex clinical outcome.Crit Care Med 1995; 23:1638–1652
20. Ferreira FL, Bota DP, Bross A, et al: Serialevaluation of the SOFA score to predict out-
Table 3. 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
Primary consensus points! The current concepts of sepsis, severe sepsis, and septic shock seem to be robust definitions
and should remain as described 10 yrs ago.! Current definitions do not allow for precise staging of the host response to infection.! Signs and symptoms of sepsis are more varied than the initial criteria established in 1991.! A list of these signs and symptoms, for the diagnosis of sepsis is presented.! The future lies in developing a staging system that will characterize progression of sepsis. A
new system, PIRO, is proposed for characterizing and staging the host response to infection.
SCCM, Society of Critical Care Medicine; ESICM, European Society of Intensive Care Medicine;ACCP, American College of Chest Physicians; ATS, American Thoracic Society; SIS, Surgical InfectionSociety; PIRO, stratifies patients on the basis of their predisposing conditions, the nature and extentof the insult—in the case of sepsis, infection, the nature and magnitude of the host response, and thedegree of concomitant organ dysfunction.
1255Crit Care Med 2003 Vol. 31, No. 4
Roma 15 Ottobre 2014
Ospedale M. Bufalini - Cesena
Surviving Sepsis Campaign Bundles The Surviving Sepsis Campaign Bundles are the core of the sepsis improvement efforts. Using "bundles" simplifies the complex processes of the care of patients with severe sepsis. A bundle is a selected set of elements of care distilled from evidence-based practice guidelines that, when implemented as a group, have an effect on outcomes beyond implementing the individual elements alone. TO BE COMPLETED WITHIN 3 HOURS: 1) Measure lactate level 2) Obtain blood cultures prior to administration of antibiotics 3) Administer broad spectrum antibiotics 4) Administer 30 ml/kg crystalloid for hypotension or lactate ≥4mmol/L TO BE COMPLETED WITHIN 6 HOURS: 5) Apply vasopressors (for hypotension that does not respond to initial fluid resuscitation) to maintain a mean arterial pressure (MAP) ≥65 mm Hg 6) In the event of persistent arterial hypotension despite volume resuscitation (septic shock) or initial lactate ≥4 mmol/L (36 mg/dL): - Measure central venous pressure (CVP)* - Measure central venous oxygen saturation (ScvO2)* 7) Remeasure lactate if initial lactate was elevated* *Targets for quantitative resuscitation included in the guidelines are CVP of ≥8 mm Hg; ScvO2 of ≥70%, and normalization of lactate.
Surviving Sepsis Campaign: International guidelines for management of severe sepsis and septic shock: 2012.
Dellinger et al: Crit Care Med. 2013; 41:580-637

Roma 15 Ottobre 2014
Ospedale M. Bufalini - Cesena
Recommendations: Initial Resuscitation and Infection Issues - Source Control 1. A specific anatomical diagnosis of infection requiring consideration for emergent source control be sought and diagnosed or excluded as rapidly as possible, and intervention be undertaken for source control within the first 12 hr after the diagnosis is made, if feasible (grade 1C). 2. When infected peripancreatic necrosis is identified as a potential source of infection, definitive intervention is best delayed until adequate demarcation of viable and nonviable tissues has occurred (grade 2B). 3. When source control in a severely septic patient is required, the effective intervention associated with the least physiologic insult should be used (eg, percutaneous rather than surgical drainage of an abscess) (UG). 4. If intravascular access devices are a possible source of severe sepsis or septic shock, they should be removed promptly after other vascular access has been established (UG).
Surviving Sepsis Campaign: International guidelines for management of severe sepsis and septic shock: 2012. Dellinger et al: Crit Care Med. 2013; 41:580-637

Roma 15 Ottobre 2014
Ospedale M. Bufalini - Cesena
Conclusions Ø Renal transplant recipients frequently utilize ED services because of their proneness to a variety of emergency medical problems. Ø Key to achieving a reduction in mortality from severe sepsis is not just standardized evidence based treatment, but equally important, the early recognition of sepsis. Ø The importance of close monitoring in the sepsis patient population cannot be underestimated; later development of hypotension in patients who were normotensive at ED triage is not the only indication of severe sepsis. Awareness of organ dysfunction other than hypotension is equally important. Frequent observations for changes in vital signs will lead to early recognition and improved outcomes. Ø Initial resuscitation and early control of the source of infection, provide the better care for critically ill patients; to achieve te best results, critical care physicians and surgeons must have adequate knowledge of patients characteristics and therapeutic options.
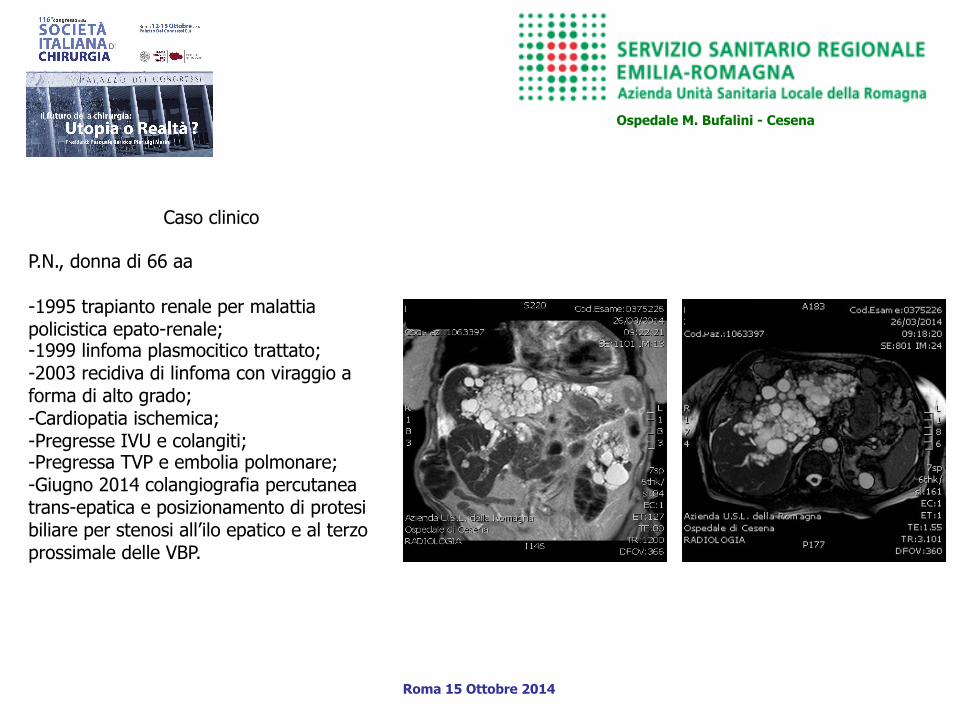
Caso clinico
P.N., donna di 66 aa - 1995 trapianto renale per malattia policistica epato-renale; - 1999 linfoma plasmocitico trattato; - 2003 recidiva di linfoma con viraggio a forma di alto grado; - Cardiopatia ischemica; - Pregresse IVU e colangiti; - Pregressa TVP e embolia polmonare; - Giugno 2014 colangiografia percutanea trans-epatica e posizionamento di protesi biliare per stenosi all’ilo epatico e al terzo prossimale delle VBP.
Ospedale M. Bufalini - Cesena
Roma 15 Ottobre 2014

Caso clinico
2/7/2014 Ricovero in Nefrologia per f-up - Dopo alcune ore dal ricovero, comparsa
di dolore addominale; - 3/7/2014 ore 1 circa - Consulenza chirurgica: addome non
trattabile ai quadranti superiori; - PA 100/55; - FC 108 bpm; - WBC 23.320; - PCR 191.
- Ecografia e TC addominale, comparsa di versamento peri-epatico, tra le anse del piccolo intestino e nello scavo pelvico.
Ospedale M. Bufalini - Cesena
Roma 15 Ottobre 2014
SIRS DA COLEPERITONEO IN ESITI DI PTC E POSIZIONAMENTO DI PROTESI BILIARE 3/7/2014 ore 12: Intervento chirurgico urgente laparoscopia esplorativa, toilette e drenaggi.


Roma 15 Ottobre 2014
Ospedale M. Bufalini - Cesena
MERCOLEDI’ 15 OTTOBRE ORE 11.30 – 13.00
SALA CAMPIDOGLIO
URGENZE ADDOMINALI NEI PAZIENTI TRAPIANTATI SEGRETARIO DI SESSIONE: D. Krizzuk MODERATORI: P. Chirletti, F. Baldoni RELAZIONI R. Caronna – La malattia da graft versus host S. Santella – L’addome acuto nei pazienti con trapianto renale G. Casciaro – L’emorragia digestiva nei pazienti con trapianto di fegato G. Sganga – Le sepsi nei pazienti trapiantati Invitati alla discussione: M. Biffoni; F. Consorti; F. La Rocca
... grazie per la cortese
attenzione!