UPDATES ON THE MANAGEMENT OF INGUINAL HERNIA IN ADULTS.
64
UPDATES ON THE MANAGEMENT OF INGUINAL HERNIA IN ADULTS
-
Upload
genesis-streat -
Category
Documents
-
view
221 -
download
0
Transcript of UPDATES ON THE MANAGEMENT OF INGUINAL HERNIA IN ADULTS.

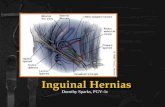
UPDATES ON THE MANAGEMENT OF INGUINAL HERNIA IN ADULTS


INTRODUCTION Most common general surgical procedure
Goals Provide long-lasting closure of pelvic floor defect Reduce pain Improve quality of life
Lack of consensus Optimum repair technique Prosthetic mesh

QUESTIONS?
Should all inguinal hernias be repaired?
What kind of mesh?
Endoscopic approach or open surgery?
TEP vs TAPP?
To fix or not to fix? (In endoscopic approach)

MYOPECTINEAL ORIFICE OF FRUCHARD A single weak point where all groin hernias originate from
Only consists of transversalis fascia Superior – Conjoint tendon Inferior – Cooper’s ligament (Pectineal) Medial – Rectus muscle Lateral – Illiopsoas muscle

ANATOMY

QUESTIONS?
Should all inguinal hernias be repaired?
What kind of mesh?
Endoscopic approach or open surgery?
TEP vs TAPP?
To fix or not to fix? (In endoscopic approach)

SHOULD ALL HERNIAS BE REPAIRED? All hernias should be repaired due to risk of incarceration or strangulation


THE EVIDENCE
Definite indications for surgery include Strangulation Incarceration Symptomatic
What about asymptomatic or minimally symptomatic patients?

THE EVIDENCEAuthor Published
YearStudy Size Follow up Conversion
RateHernia
Accident
Fitzgibbons et al
2013 254 10 years 68% 2.4%
O’Dwyer et al 2011 160 7.5 years 72% 2.5%
Fitzgibbons RJ, Jr, Giobbie-Hurder A, Gibbs JO, et al. Watchful waiting vs repair of inguinal hernia in minimally symptomatic men: a randomized clinical trial. JAMA. 2006;295:285–292Fitzgibbons RJ Jr, Ramanan B et al. Long-term results of randomized controlled trial of a nonoperative strategy (watchful waiting) for men with minimally symptomatic inguinal hernias. Ann Surg. 2013 Sep;258(3):508-15. O’Dwyer PJ, Norrie J, Alani A, et al. Observation or operation for patients with an asymptomatic inguinal hernia: a randomized clinical trial. Ann Surg. 2006;244:167.Chung L, Norrie J, O’Dwyer P. Long-term follow-up of patientswith a painless inguinal hernia from a randomized clinical trial. Br J Surg. 2011;98:596–599.
Watchful waiting Safe and acceptable
70% of patients symptoms will increase Surgery

SHOULD ALL HERNIAS BE REPAIRED? Current Recommendation Older men/comorbidities consider watchful waiting strategy
Younger patients encourage elective repair

QUESTIONS?
Should all inguinal hernias be repaired?
What kind of mesh?
Endoscopic approach or open surgery?
TEP vs TAPP?
To fix or not to fix? (In endoscopic approach)

LIGHTWEIGHT VS HEAVYWEIGHT Lightweight mesh (Large porous mesh) Weight reduced large pore >1 mm in size Minimal foreign body reaction Lighter, more pliable and more comfortable ↓ Shrinkage
Heavyweight mesh (Small porous mesh) Closely knitted with small pores less than 1 mm size ↑ Surface area ↑ Intense foreign body reaction ↑ Shrinkage

THE EVIDENCE
3 Meta-analyses (2012): Sajid et al, Uzzaman MM et al, Smietanski M et al
Current Recommendation Lightweight meshes - ↓ chronic pain and ↓ foreign body feeling (early follow up)
No difference in chronic pain in long term follow up >3 years
Recurrence rate not increased

QUESTIONS?
Should all inguinal hernias be repaired?
What kind of mesh?
Endoscopic approach or open surgery?
TEP vs TAPP?
To fix or not to fix? (In endoscopic approach)

ENDOSCOPIC APPROACH OR OPEN SURGERY? Proven benefit for recurrent hernias In terms of recurrence and chronic pain
Also proven beneficial for bilateral hernias
But what about primary unilateral inguinal hernias?

THE EVIDENCE – META-ANALYSISAuthor Journal Studies Patient
no.Repair type Recurrenc
eChronic
painComplications Return to Work
(days)
EU Hernia Trialist (2002)
Hernia 25 4165 Lap vs Lichtenstein No difference
Lap < Open More serious Cx in lap
N/A
Memon (2003)
British Journal of Surgery
29 5588 Lap vs Open No difference
N/A Lap < Open Lap < Open
NICE Guidelines
(2004)
37 5560 Lap vs Open mesh repair
No difference
Lap < Open No difference Lap < Open
Schmedt (2005)
Surgical Endoscopy
23 4550 Lap vs Open No difference
Lap < Open Lap < OpenMore serious Cx
in lap
Lap < Open
Kuhry (2007)
(Systemic review)
Surgical Endoscopy
23 4231 TEP vs Open No difference
N/A No difference Lap < Open
O’Reilly (2012)
Annals of Surgery
27 7161 Lap vs Open Lap > Open Lap < Open No difference N/A
Koning (2013)
PLOS ONE 13 5404 TEP vs Lichtenstein No difference
No difference
No difference N/A
European Hernia Society
Guidelines (2009/2014)
Hernia 8 (FU
>48mths)
2399 Lap vs Lichtenstein No difference
No difference
N/A N/A

WHAT DOES THIS ALL MEAN?
Difficult to interpret
Heterogeneity of the studies Open repair included studies performing Bassini, Shouldice etc Discrepancy in laparoscopic experience
Bassini
Shouldice
Master Techniques in Surgery: Hernia. Jones B Daniel. 2012.

BEST OPTIONS FOR PRIMARY UNILATERAL HERNIA REPAIR Current Recommendation Open Lichtenstein and laparoscopic hernioplasty
No difference between recurrence rate
Possible ↓ acute and chronic pain in laparoscopic hernioplasty

QUESTIONS?
Should all inguinal hernias be repaired?
What kind of mesh?
Endoscopic approach or open surgery?
TEP vs TAPP?
To fix or not to fix? (In endoscopic approach)

TEP OR TAPP?
TEP = Totally extraperitoneal technique
TAPP = Transabdominal pre-peritoneal technique
What’s the difference?

Zollinger’s Atlas of Surgical Operations 9th Edition

Master Techniques in Surgery: Hernia. Jones B Daniel. 2012.

TEP
Hernia Surgery Simplified. Kuber, Sachin. 2013.

TEP
Master Techniques in Surgery: Hernia. Jones B Daniel. 2012.

TEP
Master Techniques in Surgery: Hernia. Jones B Daniel. 2012.

TEP
Hernia Surgery Simplified. Kuber, Sachin. 2013.

TAPP
Hernia Surgery Simplified. Kuber, Sachin. 2013.

TAPP
Master Techniques in Surgery: Hernia. Jones B Daniel. 2012.

Master Techniques in Surgery: Hernia. Jones B Daniel. 2012.

Master Techniques in Surgery: Hernia. Jones B Daniel. 2012.

Master Techniques in Surgery: Hernia. Jones B Daniel. 2012.

TEP OR TAPP?
Cochrane Review 2005 Insufficient data Most were non-randomized studies Conclusion back then: No differences between TEP and TAPP
What is the conclusion now, 10 years later?

TEP VS TAPP
Systemic Review by Bracale et al (2012) Indirect comparison
Operative time Post-op complications Post-op pain Recurrence
TEP and TAPP were equivalent
Bracale U, Melillo P, Pignata G, et al. Which is the best laparoscopic approach for inguinal hernia repair: TEP or TAPP? A systematic review of the literature with a network meta-analysis. Surg Endosc 2012;26(12):3355–66.

TEP VS TAPP
Two RCTs – Gong et al (2011) and Bansal et al (2012) Chronic pain Quality of life Return to normal activities Recurrence
TEP and TAPP were comparable
Gong K, Zhang N, Lu Y, Zhu B, Zhang Z, Du D, Zhao X, Jiang H (2011) Comparison of the open tension-free mesh-plug, transabdominal preperitoneal (TAPP), and totally extraperitoneal (TEP) laparoscopic techniques for primary unilateral inguinal hernia repair: a prospective randomized controlled trial. Surg Endosc 25:234–239Bansal VK, Misra MC, Babu D, et al. A prospective, randomized comparison of long-term outcomes: chronic groin pain and quality of life following totally extraperitoneal (TEP) and transabdominal preperitoneal (TAPP) laparoscopic inguinal hernia repair. Surg Endosc 2013;27(7):2373–82.

TEP OR TAPP
Current Recommendation Both TEP and TAPP provide favorable outcomes
Decision based on surgeon’s preference and expertise

QUESTIONS?
Should all inguinal hernias be repaired?
What kind of mesh?
Endoscopic approach or open surgery?
TEP vs TAPP?
To fix or not to fix? (In endoscopic approach)

TRIANGLE OF PAIN
CORONA MORTIS
Master Techniques in Surgery: Hernia. Jones B Daniel. 2012.
TRIANGLE OF DOOM


Master Techniques in Surgery: Hernia. Jones B Daniel. 2012.

TYPES OF FIXATION
Traumatic mesh fixation Endoscopic staplers
Atraumatic mesh fixation Fibrin/tissue glue
Hernia Surgery Simplified. Kuber, Sachin. 2013.

MESH FIXATION VS NO FIXATION – META-ANALYSES
Author Journal Studies
Patient no.
Repair type Recurrence
Post-op Pain
Complications
Chronic pain
Tam KW et al
(2010)
World Journal of Surgery
6 932 TEP No difference
No difference
No difference
N/A
Tang YJ et al (2011)
Surgical Endoscopy
6 772 TEP No difference
No difference
No difference
N/A
Sajid MS et al
(2012)
International Journal of Surgery
8 1386 TEP(one study with
TAPP)
No difference
No difference
No difference
No difference

TAPP
Only one RCT comparing mesh fixation and no fixation 502 patients Median follow up of 16 months
No statistical difference Operative time Chronic pain Recurrence
Smith AI, Royston CM, Sedman PC (1999) Stapled and nonstapled laparoscopic transabdominal preperitoneal (TAPP) inguinal hernia repair. A prospective randomized trial. Surg Endosc 13(8):804–806

TO FIX OR NOT TO FIX
Current Recommendation Traumatic mesh fixation in TEP is unnecessary in most cases

CONCLUSION
Should all inguinal hernias be repaired?
What kind of mesh?
Endoscopic approach or open surgery?
TEP vs TAPP?
To fix or not to fix? (In endoscopic approach)

THE END

THE IDEAL MESH Not physically modified by body tissue fluids
Chemically inert
Flexible and moldable
Not causing hypersensitivity
Resistant to mechanical strain over long time
Should not cause foreign body inflammation or allergic reactions
High tensile strength
Capable of being fabricated in the form required
Can be sterilized
Noncarcinogenic
Should not prone to bacterial seeding and infection
Barrier to adhesion
Cost-effective
Readily available

MOST COMMON MATERIALS USED Polypropylene Ie. Prolene, Marlex
Polyester Ie. Dacron, Mersilene

WHAT MATERIAL?
No evidence on what type of material is better.

ATRAUMATIC MESH FIXATION VS
MECHANICAL FIXATION

ATRAUMATIC FIXATION VS MECHANICAL FIXATION Comparable results Recurrence, operative time, post-operative complications and length of hospital stay.
Two RCTs (Lovisetto F et al (2007) and Olmi S (2007) Decreased post-operative pain for glue fixation
No meta-analyses to compare
- Lau H (2005) Fibrin sealant vs. mechanical stapling for mesh fixation during endoscopic extraperitoneal inguinal hernioplasty: a randomized prospective trial. Ann Surg 242(5):670–675- Lovisetto F, Zonta S, Rota E, Mazzilli M, Bardone M, Bottero L, Faillace G, Longoni M (2007) Use of human fibrin glue (Tissucol) vs. staples for mesh fixation in laparoscopic transabdominal preperitoneal hernioplasty: a prospective, randomized study. Ann Surg 245(2):222–231. - Olmi S, Scaini A, Erba L, Guaglio M, Croce E (2007) Quantification of pain in laparoscopic transabdominal preperitoneal (TAPP) inguinal hernioplasty identifies marked differences between prosthesis fixation systems. Surgery 142(1):40–46.- Boldo E, Armelles A, Perez de Lucia G, Martin F, Aracil JP, Miralles JM, Martinez D, Escrig J (2008) Pain after laparoscopic bilateral hernioplasty: early results of a prospective randomized double-blind study comparing fibrin vs. staples. Surg Endosc 22(5):1206–1209. - Fortelny RH, Petter-Puchner AH, May C, Jaksch W, Benesch T, Khakpour Z, Redl H, Glaser KS (2012) The impact of atraumatic fibrin sealant vs. staple mesh fixation in TAPP hernia repair on chronic pain and quality of life: results of a randomized controlled study. Surg Endosc 26(1):249–254.

MESH OR NON-MESH
Not much controversy
Many studies have documented a 50-75% reduction rates with the addition of mesh to an inguinal hernia repair With mesh
Most studies report recurrence rates in the 2-5% range with long-term follow up Lower rates of chronic pain
- EU Hernia Trialists Collaboration. Mesh compared with non-mesh methods of open groin hernia repair: systematic review of randomized controlled trials.Br J Surg 2000;87(7):854–9. - Scott NW, McCormack K, Graham P, et al. Open mesh versus non-mesh for repair of femoral and inguinal hernia. Cochrane Database Syst Rev 2002;(4):- EU Hernia Trialists Collaboration. Repair of groin hernia with synthetic mesh: meta-analysis of randomized controlled trials. Ann Surg 2002;235(3):322–32.- Amato B, Moja L, Panico S, et al. Shouldice technique versus other open techniques for inguinal hernia repair. Cochrane Database Syst Rev 2012;(4):- Grant AM, EU Hernia Trialists Collaboration. Open mesh versus non-mesh repair of groin hernia: meta-analysis of randomised trials based on individual patient data. Hernia 2002;6(3):130–6.

CONTRALATERAL DISSECTION: HOW FAR? The incidence of incipient unsuspected contralateral hernia is 11.2 -20%
Laparoscopic hernia repair (TAPP) has a major advantage of allowing the surgeon to explore the site contralateral to the clinically diagnosed hernia without any additional dissection steps
In TEP- Advantages and disadvantages
Recommendations The systemic exploration of the contralateral side using the TEP technique is controversial. Further studies are needed

WHAT IS THE MOST COST-EFFECTIVE OPERATION? From the perspective of the hospital, an open mesh procedure is the most cost-effective operation in primary unilateral hernias
From a socioeconomic perspective, an endoscopic procedure is probably the most cost-effective approach for patients who participate in the labour market.
Conclusions with respect to cost issues should be interpreted with care since local expertise, the used instrumentation (disposable vs reusable instruments, type of anaesthesia) and local health care/insurance issues (eg. Day surgery vs overnight stay, public vs private hospital setting) play a role to determine direct costs
Sociocultural differences with respect to work resumption increase the difficulty in interpretation when evaluating total costs

ANTIBIOTICS
In open mesh repair in low risk patients and a low incidence of wound infection, antibiotic prophylaxis does not significantly reduce the number of wound infections
In the presence of high incidence of wound infection (>5%) there is a significantly benefit of antibiotic prophylaxis. NNT 22 (Class IA evidence)
European Hernia Society Guidelines Update 2014

ILIOINGUINAL NERVE
Prophylactic resection of the ilioinguinal nerve does not reduce the risk of chronic pain after open hernia surgery
Level IA evidence
A more recent meta-analysis of all RCTs on preservation vs routine division of the ilioinguinal nerve during open mesh repair for the prevention of chronic pain showed no difference at 6 and at 12 months Chen CS, Lee HC, Liang HH, Kuo LJ, Wei PL, Tam KW (2012) Preservation vs. division of ilioinguinal nerve on open mesh repair of
inguinal hernia: a meta-analysis of randomized controlled trials. World J Surg

CHRONIC PAIN
Evidence from two RCTs show that chronic pain diminishes over time
In a 10 year follow up study of an RCT including 300 patients comparing mesh vs non-mesh repair for a primary inguinal hernia Incidence of pain 6 months postoperatively was between 10-15% None of the patients suffered from persistent pain and discomfort interfering with daily activity
Another RCT comparing endoscopic TEP vs Lichtenstein repair in 1370 patients 21.7% had chronic pain at 1 year 18.8% chronic pain at 5 years

MESH DEVICES
PHS and Plug and Patch (mesh plug) result in comparable outcome (recurrence and chronic pain) as the Lichtenstein technique (1-4 year follow up)

COMPARISON BETWEEN POLYESTER AND POLYPROPYLENE
Small RCTs have shown similar results in regards to postoperative pain and quality of life
Amount of chronic pain was similar too

REFERENCES
Fitzgibbons RJ, Jr, Giobbie-Hurder A, Gibbs JO, et al. Watchful waiting vs repair of inguinal hernia in minimally symptomatic men: a randomized clinical trial. JAMA. 2006;295:285–292
Fitzgibbons RJ Jr, Ramanan B et al. Long-term results of randomized controlled trial of a nonoperative strategy (watchful waiting) for men with minimally symptomatic inguinal hernias. Ann Surg. 2013 Sep;258(3):508-15.
O’Dwyer PJ, Norrie J, Alani A, et al. Observation or operation for patients with an asymptomatic inguinal hernia: a randomized clinical trial. Ann Surg. 2006;244:167.
Chung L, Norrie J, O’Dwyer P. Long-term follow-up of patientswith a painless inguinal hernia from a randomized clinical trial. Br J Surg. 2011;98:596–599.
Sajid MS, Leaver C, Baig MK, Sains P (2012) Systematic review and meta-analysis of the use of lightweight vs. heavyweight mesh in open inguinal hernia repair. Br J Surg 99(1):29–37.
Uzzaman MM, Ratnasingham K, Ashraf N (2012) Meta-analysis of randomized controlled trials comparing lightweight and heavyweight mesh for Lichtenstein inguinal hernia repair. Hernia.
Smietanski M, Smietanska IA, Modrzejewski A, Simons MP, Aufenacker TJ (2012) Systematic review and meta-analysis on Heavy and lightweight polypropylene mesh in Lichtenstein inguinal hernioplasty. Hernia 16(5):519–528
Nikkolo C, Murruste M, Vaasna T, Seepter H, Tikk T, Lepner U (2012) 3-year results of randomised clinical trial comparing lightweight mesh with heavyweight mesh for inguinal hernioplasty. Hernia 16(5):555–559.
Smietanski M, Bury K, Smietanska IA, Owczuk R, Paradowski T (2011) 5-year results of a randomised controlled multi-centre study comparing heavy-weight knitted vs. low-weight, nonwoven polypropylene implants in Lichtenstein hernioplasty. Hernia 15(5):495–501.
Bury K, Smietanski M (2012) 5-year results of a randomized clinical trial comparing a polypropylene mesh with a poliglecaprone and polypropylene composite mesh for inguinal hernioplasty. Hernia 16(5):549–553.

REFERENCES Treadwell J, Tipton K, Oyesanmi O, et al. Surgical options for inguinal hernia: comparative effectiveness review. Comparative effectiveness review No.
70 (Prepared by the ECRI Institute evidence-based Practice Center under Contract No. 290-2007-10063.) AHRQ publication No. 12-EHC091-EF. Rockville (MD): Agency for Healthcare Research and Quality; 2012
McCormack K, Wake BL, Fraser C, et al. Transabdominal pre-peritoneal (TAPP) versus totally extraperitoneal (TEP) laparoscopic techniques for inguinal hernia repair: a systematic review. Hernia 2005;9(2):109–14.
Bittner R, Arregui ME, Bisgaard T, et al. Guidelines for laparoscopic (TAPP) and endoscopic (TEP) treatment of inguinal Hernia [International Endohernia Society (IEHS)]. Surg Endosc 2011;25:2773–843.
Wake BL, McCormack K, Fraser C, et al. Transabdominal pre-peritoneal (TAPP) vs totally extraperitoneal (TEP) laparoscopic techniques for inguinal hernia repair. Cochrane Database Syst Rev 2005;(1):CD004703.
McCormack K, Wake B, Perez J, et al. Laparoscopic surgery for inguinal hernia repair: systematic review of effectiveness and economic evaluation. Health Technol Assess 2005;9(14):1–203, iii–iv.
Shah NR, Mikami DJ, Cook C, et al. A comparison of outcomes between open and laparoscopic surgical repair of recurrent inguinal hernias. Surg Endosc 2011;25(7):2330–7.
Sevonius D, Gunnarsson U, Nordin P, et al. Recurrent groin hernia surgery. Br J Surg 2011;98(10):1489–94.
Bignell M, Partridge G, Mahon D, et al. Prospective randomized trial of laparoscopic (transabdominal preperitoneal-TAPP) versus open (mesh) repair for bilateral and recurrent inguinal hernia: incidence of chronic groin pain and impact on quality of life: results of 10 year follow-up. Hernia 2012;16(6): 635–40.
Gopal SV, Warrier A. Recurrence after groin hernia repair-revisited. Int J Surg 2013;11(5):374–7.

REFERENCES Yang J, Tong da N, Yao J, et al. Laparoscopic or lichtenstein repair for recurrent inguinal hernia: a meta-analysis of randomized controlled trials. ANZ J Surg
2013;83(5):312–8.
Simons MP, Aufenacker ET, Bay-Nielsen M, et al. European Hernia Society guidelines on the treatment of inguinal hernia in adult patients. Hernia 2009; 13:343–403.
Bittner R, Arregui ME, Bisgaard T, et al. Guidelines for laparoscopic (TAPP) and endoscopic (TEP) treatment of inguinal Hernia [International Endohernia Society (IEHS)]. Surg Endosc 2011;25:2773–843.
McCormack K, Wake BL, Fraser C, et al. Transabdominal pre-peritoneal (TAPP) versus totally extraperitoneal (TEP) laparoscopic techniques for inguinal hernia repair: a systematic review. Hernia 2005;9(2):109–14.
Sajid MS, Ladwa N, Kalra L, et al. A meta-analysis examining the use of tackerfixation versus no-fixation of mesh in laparoscopic inguinal hernia repair. Int J Surg 2012;10(5):224–31.
Tolver MA, Rosenberg J, Juul P, et al. Randomized clinical trial of fibrin glue versus tacked fixation in laparoscopic groin hernia repair. Surg Endosc 2013; 27(8):2727–33.
Kaul A, Hutfless S, Le H, et al. Staple versus fibrin glue fixation in laparoscopic total extraperitoneal repair of inguinal hernia: a systematic review and metaanalysis. Surg Endosc 2012;26(5):1269–78.
Fortelny RH, Petter-Puchner AH, Glaser KS, et al. Use of fibrin sealant (Tisseel/Tissucol) in hernia repair: a systematic review. Surg Endosc 2012;26(7):1803–12.
Sajid MS, Ladwa N, Kalra L, et al. A meta-analysis examining the use of tacker mesh fixation versus glue mesh fixation in laparoscopic inguinal hernia repair. Am J Surg 2013;206(1):103–11.
Lau H (2005) Fibrin sealant vs. mechanical stapling for mesh fixation during endoscopic extraperitoneal inguinal hernioplasty: a randomized prospective trial. Ann Surg 242(5):670–675
Lovisetto F, Zonta S, Rota E, Mazzilli M, Bardone M, Bottero L, Faillace G, Longoni M (2007) Use of human fibrin glue (Tissucol) vs. staples for mesh fixation in laparoscopic transabdominal preperitoneal hernioplasty: a prospective, randomized study. Ann Surg 245(2):222–231.

REFERENCES Olmi S, Scaini A, Erba L, Guaglio M, Croce E (2007) Quantification of pain in laparoscopic transabdominal preperitoneal (TAPP) inguinal hernioplasty
identifies marked differences between prosthesis fixation systems. Surgery 142(1):40–46.
Boldo E, Armelles A, Perez de Lucia G, Martin F, Aracil JP, Miralles JM, Martinez D, Escrig J (2008) Pain after laparoscopic bilateral hernioplasty: early results of a prospective randomized double-blind study comparing fibrin vs. staples. Surg Endosc 22(5):1206–1209.
Fortelny RH, Petter-Puchner AH, May C, Jaksch W, Benesch T, Khakpour Z, Redl H, Glaser KS (2012) The impact of atraumatic fibrin sealant vs. staple mesh fixation in TAPP hernia repair on chronic pain and quality of life: results of a randomized controlled study. Surg Endosc 26(1):249–254.
Bansal VK, Misra MC, Babu D, et al. A prospective, randomized comparison of long-term outcomes: chronic groin pain and quality of life following totally extraperitoneal (TEP) and transabdominal preperitoneal (TAPP) laparoscopic inguinal hernia repair. Surg Endosc 2013;27(7):2373–82.
Bracale U, Melillo P, Pignata G, et al. Which is the best laparoscopic approach for inguinal hernia repair: TEP or TAPP? A systematic review of the literature with a network meta-analysis. Surg Endosc 2012;26(12):3355–66.
EU Hernia Trialists Collaboration. Mesh compared with non-mesh methods of open groin hernia repair: systematic review of randomized controlled trials. Br J Surg 2000;87(7):854–9.
Scott NW, McCormack K, Graham P, et al. Open mesh versus non-mesh for repair of femoral and inguinal hernia. Cochrane Database Syst Rev 2002;(4):
EU Hernia Trialists Collaboration. Repair of groin hernia with synthetic mesh: meta-analysis of randomized controlled trials. Ann Surg 2002;235(3):322–32.
Amato B, Moja L, Panico S, et al. Shouldice technique versus other open techniques for inguinal hernia repair. Cochrane Database Syst Rev 2012;(4):
Grant AM, EU Hernia Trialists Collaboration. Open mesh versus non-mesh repair of groin hernia: meta-analysis of randomised trials based on individual patient data. Hernia 2002;6(3):130-6.