Updates In Pediatric Dermatology - American Academy of...
35
Updates In Pediatric Dermatology Dr. Adena Rosenblatt MD PhD Assistant Professor of Pediatric Dermatology University of Chicago Medicine
Transcript of Updates In Pediatric Dermatology - American Academy of...

Updates In Pediatric Dermatology
Dr. Adena Rosenblatt MD PhD Assistant Professor of Pediatric
Dermatology University of Chicago Medicine

Disclosures
• I have no relevant financial relationships with the manufacturers(s) of any commercial products(s) and/or provider of commercial services discussed in this CME activity.
• I do not intend to discuss an unapproved/investigative use of a commercial product/device in my presentation.

Learning Objectives
• Present new therapies for common pediatric dermatologic conditions
• Describe how to overcome barriers to implementing in practice

Acne
• 85% of adolescents and young adults between 12-24yo develop acne

Types of Acne

Guidelines of Care for Acne
Journal of the American Academy of Dermatology 2016 74, 945-973.e33DOI: (10.1016/j.jaad.2015.12.037)

Antibiotic Resistance Prevention
• Recent retrospective cohort study in the United Kingdom
• 62% of general practitioners (GP) prescribing oral antibiotics for acne did so without also prescribing a retinoid
• 29% of GPs prescribed oral antibiotics for greater that 6 mo course for acne

New Acne Treatments in Trial
• Topical minocycline foam appears to be effective and safe for the treatment of moderate to severe inflammatory acne in Phase 2 clinical trials.
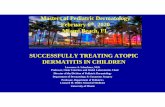
• Olumacostat glasaretil (OG) inhibits sebocyte lipid production is an effective and safe topical treatment for moderate to severe acne in Phase 2 clinical trials
• Of note, Differin (adapalene) 0.1% cream is now available over the counter

Fig 1. Acetyl coenzyme A carboxylase (ACC) effect on sebum production. CoA, Coenzyme A; HMG CoA, 3-hydroxy-3-methyl-
glutaryl-coenzyme A; OG, olumacostat glasaretil; TOFA, 5-(tetradecyloxy)-2-furancarboxylic acid.
Robert Bissonnette, Yves Poulin, Janice Drew, Hans Hofland, Jerry Tan
Olumacostat glasaretil, a novel topical sebum inhibitor, in the treatment of acne vulgaris: A phase IIa, multicenter,
randomized, vehicle-controlled study
Journal of the American Academy of Dermatology, Volume 76, Issue 1, 2017, 33–39
http://dx.doi.org/10.1016/j.jaad.2016.08.053

Periorificial Dermatitis
• Common condition in children
• Exacerbated by topical steroids
• +/- burning sensation • Standard treatment is
erythromycin x6wk, sometimes topical metronidazole or calcineurin inhibitors
• New study looks at efficacy of topical ivermectin (may be 2/2 demodex)

Atopic Dermatitis
• Most common chronic inflammatory skin condition
• Occurs in 10-15% of children
• Multifactorial pathogenesis but it is TH2 mediated
• Atopic Triad: AD, asthma, allergic rhinitis

Atopic Dermatitis

Types of Atopic Dermatitis

Atopic Dermatitis
• Guidelines of care for the management of atopic dermatitis in JAAD
• Emollients are mainstay for the treatment and maintenance of atopic dermatitis
• Bathing should be performed daily with mild, fragrance free soap
• Topical steroids are the mainstay for first line treatment in AD and topical calcineurin inhibitors can also be effective
• Refractory AD can be treated with phototherapy (ie nbUVB) or systemic treatment (ie cyclosporine, azathioprine, methotrexate)
• Probiotics may be mildly helpful but food avoidance is not recommended

New Treatment for Atopic Dermatitis
• Topical crisaborole 2% oint, a PDE 4 inhibitor, is effective for mild to moderate AD in Phase 3 clinical trial for children and adults
• Dupilumab, a human monoclonal antibody to IL-4 receptor alpha, is effective for moderate to severe AD in Phase 3 clinical trials in adults
• 5 year randomized trial found that pimecrolimus (elidel) cream was safe and effective for long term management of mild to moderate AD in infants

Contact Dermatitis In Children With Atopic Dermatitis
• Patch tested children with AD were younger and had a longer history of dermatitis compared to those without AD
• Increase frequency of reactions to:
– cocamidopropyl betaine (ie acne cleansers- panoxyl, clearasil, biore)
– wool alcohol/lanolin (ie Aquaphor)
– tixocortol pivalate
– Parthenolide (extract of feverfew, in Aveeno products)

2014 ISSVA Classification of Vascular Anomalies
Vascular Anomalies
Vascular
Tumors
Vascular Malformations
Simple Combined Of Major
Named
Vessels
Associated
With Other
Anomalies
Benign CM See Table 5 See text See Table 6
Locally
aggressive or
borderline
LM
VM
Malignant
AVM
Arteriovenou
s fistula

Vascular Lesions Benign vascular tumors
Infantile hemangioma/hemangioma of
infancy
Congenital hemangioma
Rapidly involuting CH (RICH)a
Noninvoluting CH (NICH)
Partially involuting CH (PICH)
Tufted angiomaa,b
Spindle cell hemangioma
Epithelioid hemangioma
Pyogenic granuloma (or lobular
capillary hemangioma)
Others
Locally aggressive or borderline
vascular tumors
Kaposiform hemangioendotheliomaa,b
Retiform hemangioendothelioma
Papillary intralymphatic
angioendothelioma, Dabska tumor
Composite hemangioendothelioma
Kaposi sarcoma
Others
Malignant vascular tumors
Angiosarcoma
Epithelioid hemangioendothelioma
Others
CMs
Cutaneous and/or mucosal CM (“port
wine” stain)
CM with bone and/or soft tissue
overgrowth
CM with CNS and/or ocular
anomalies (Sturge-Weber syndrome)
CM of CM-AVM
CM of microcephaly-CM (MICCAP)
CM of megalencephaly-CM-
polymicrogyria (MCAP)
Telangiectasia
Hereditary hemorrhagic
telangiectasia (HHT; different types)
Others
Cutis marmorata telangiectatica
congenita (CMTC)
Nevus simplex/salmon patch/ “angel
kiss,” “stork bite”
Others
LMs
Common (cystic) LMs
Macrocystic LM
Microcystic LM
Mixed cystic LM
Generalized lymphatic anomaly (GLA)
LM in Gorham-Stout disease
Channel-type LM
Primary lymphedema
Others
VMs
Common VM
Familial VM cutaneo-mucosal
(VMCM)
Blue rubber bleb nevus (Bean)
syndrome VM
Glomuvenous malformation
(GVM)
Cerebral cavernous
malformation (CCM; different
types)
Others
AVMs
Sporadic
In HHT
In CM-AVM
AVFs
Sporadic
In HHT
In CM-AVM
Others

Infantile Hemangiomas
• Benign vascular tumor
• Most present in the first few weeks of life (1/3 present at birth)
• More common in premature infants, females, mothers of AMA or with placental problems during pregnancy
• Growth phase (in 1st 6mo of life) plateau phase (1st few years of life) involution phase (3-10yo)

Types of Hemangiomas

Complications of Hemangiomas
• Functional compromise – Eye – Ear – Airway – Anogenital
• Ulceration • Permanent disfigurement
– Lip, tip of nose, parotid, anogenital
• Visceral lesions • Hypothyroidism • Associated syndromes or features

Management of Hemangiomas: Interventions
• Parental support and careful observation • Wound care when ulcerated • Propranolol is treatment of choice for
complicated lesions – Topical timolol gel: Might moderate proliferation;
might help heal ulcers • 2nd line options:
– Systemic corticosteroids, intralesional corticosteroids – Vincristine
– Pulsed dye laser – Embolization – Surgical excision

Infantile Hemangiomas
• Topical timolol is a safe and effective treatment for superficial, thin IH
• Oral propranolol has a safe profile with minimal AE if pt are screened properly for contraindications
• ~25% of patients on oral propranolol have rebound growth after d/c

Vascular Malformations

New Treatments for Vascular Anomalies
• Sirolimus (rapamycin) was efficacious and well tolerated for treatment of a variety of vascular anomalies in a phase 2 clinical trial
• Propranolol may be effective at low doses for the treatment of lymphatic anomalies in a recent retrospective case series

Psoriasis
• Chronic inflammatory skin condition affecting 4-5% of US population
• Multifactorial but it is TH1 mediated
• Guttate type is more common in children often following strep infection
• May be associated with arthritis and/or nail findings

Types of Psoriasis

Psoriasis Treatment
• Topical treatment: – Topical steroids – Topical vitamin D analogs – Topical calcineurin inhibitors – Tazorac (retinoid)
• Phototherapy: – nbUVB – Excimer laser – PUVA (not commonly used b/c risk of skin cancer)
• Systemic treatment: – Methotrexate – Cyclosporine – Acitretin – Biologics

Psoriasis
• Study showed a decrease in QOL of parents of children with psoriasis (ie sleep disruption, sadness, frustration, burden of care)
• Increased rates of psychiatric comorbid conditions in children with psoriasis (ie depression, substance abuse, eating disorders)
• Increased rates of metabolic syndrome in children with psoriasis

Psoriasis treatments and trials
• Approval for etanercept in children
• Investigation of biosimilars and other biologics in adults Guselkumab (anti IL 23 monoclonal ab) highly effective including adalimumab nonresponders
• Clinical trial is starting to investigate the efficacy of ixekizumab, (anti IL 17A monoclonal ab) for treatment of moderate to severe plaque psoriasis in children (approved in adults)

Alopecia areata
• Most common non-scarring alopecia
• T cell mediated autoimmune condition
• May have associated nail findings
• Clinical course is unpredictable
• May be associated with other autoimmune conditions
• Current treatments include: topical or intralesional steroids, squaric acid topical tx

Types of Alopecia areata

New Treatments for alopecia areata
• Tofacitinib, a JAK kinase inhibitor, was found to be effective in the treatment of alopecia areata in adolescents
• Clinical trial is underway to evaluate efficacy of topical JAK kinase inhibitor in adults with alopecia areata

Teledermatology
• Provides pediatric dermatology care remotely
• Dermatologist are able to identify the correct diagnosis most of the time through teledermatology
• It is best utilized with standardized history taking and photography
• Teledermatology is best for characteristic presentations of skin conditions and for follow up of previously diagnosed conditions

References • Puttgen K et al. Topical timolol maleate treatment of infantile hemangiomas. Pediatrics. Sept 2016 Vol 138 (3) • Leaute-Labreze C et al. Safety of oral propranolol for the treatment of infantile hemangiomas: as systematic review. Pediatrics. Oct 2016 138(4). • Shah SD et al. Rebound growth of infantile hemangiomas after propranolol therapy. Pediatrics Apr 2016 Vol 137 (4) • Wassef M et al. Vascular anomalies classification: recommendations from the international society for the study of vascular anomalies. Pediatrics Jul
2015 Vol 136 (1) • Tollefson MM et al. Impact of childhood psoriasis on parents of affected children. J Am Acad Dermatol. Feb 2017. 76 (2) • Todberg T et al. Psychiatric comorbidities in children and adolescents with psoriasis- a population-based cohort study. Br J Dermatol. Sept 2016. • Noguera-Morel L et al. Ivermectin therapy for papulopustular rosacea and periorificial dermatitis in children: A series of 15 cases. JAAD. Mar 2017 Vol
76 (3) 567-570. • Reich K et al. Efficacy and safety of guelkumab, an anti-interleukin-23 monoclonal antibody, compared with adalimumab for the treatment of
patients with moderate to severe psoriasis with randomized withdrawal and retreatment: Results from the phase III, double-blind, placebo- and active comparator- controlled VOYAGE 2 trial. JAAD. Mar 2017 Vol 76(3) 418-431
• Strober B. et al. Short and long-term safety outcomes with ixekizumab from 7 clinical trials in psoriasis> Etanercept comparisons and integrated data. JAAD. Mar 2017. Vol 76 (3) 432-440.
• Craiglow BG et al. Tofacitinib for the treatment of alopecia areata and variants in adolescents. JAAD. Jan 2017. Vol 76 (1) 29-32. • Bissonnette R et al. Olumacostat glasaretil, a novel topical sebum inhibitor, in the treatment of acne vulgaris: A phase IIa, multicenter, randomized,
vehicle-controlled study. JAAD. Jan 2017 Vol 76 (1). • Zaenglein AL et al. Guidelines of care for the management of acne vulgaris. JAAD. May 2016 Vol 74 (5) 945-973. • Shermer A et al. Topical minocycline foam for moderate to severe acne vulgaris: Phase 2 randomized double-blind, vehicle-controlled study results.
JAAD. June 2016. Vol 74 (6) • Barbieri JS et al. Duration of oral tetracycline-class antibiotic therapy and use of topical retinoids for the treatment of acne among general
practitioners (GP): A retrospective cohort study. JAAD. Dec 2016. Vol 75 (6) 1142-1150. • Jarnagin K et al. Crisaborole topical ointment, 2%: a nonsteroidal, topical, anti-inflammatory phosphodiesterase 4 inhibitor in clinical development for
the treatment of atopic dermatitis. JDD. Apr 2016 15 (4) 390-396. • Sidbury R et al. Guidelines of care for the management of atopic dermatitis: section 3. Management and treatment with phototherapy and systemic
agents. JAAD Aug 2014. 71 (2) 327-49 • Eichenfield LF et al. Guidelines of care for the management of atopic dermatitis: section 1. Diagnosis and assessment of atopic dermatitis. JAAD. Feb
2014 70(2) 338-51 • Sidbury R et al. Guidelines of care for the management of atopic dermatitis: section 4. Prevention of disease flares and use of adjunctive therapies
and approaches. JAAD Dec 2014 71 (6) 1218-1233 • Eichenfield LF et al. Guidelines of care for the management of atopic dermatitis: section 2. Management and treatment of atopic dermatitis with
topical therapies. JAAD Jul 2014 71(1) 116-32 • Simpson EL et al. Two phase 3 trials of dupilumab versus placebo in atopic dermatitis. N Engl J Med. Dec 2016. Vol 375 (24) 2335-2348 • Sigurgeirsson B et al. Safety and efficacy of pimecrolimus in atopic dermatitis: a 5-year randomized trial. Pediatrics. Apr 2015. Vol 135 (4) 597-606 • Adams DM et al. Efficacy and safety of sirolimus in the treatment of complicated vascular anomalies. Pediatrics. Feb 2016. Vol 137 (2) • Wu JK et al. Initial experience with propranolol treatment of lymphatic anomalies: a case series. Pediatrics. Sep 2016. Vol 138 (3) • Philp JC et al. Pediatric teledermatology consultation: relationship between provided data and diagnosis. Pediatr Dermatol. Sept 2013. Vol 30 (5) 561-
7 • Fogel AL and Teng JM. Pediatric teledermatology: a survey of usage, perspective, and practice. Pediatr Dermatol. May 2015. Vol 32 (3) 363-8