University of Malawi - Home page | UNICEF · 2019-06-07 · i Acknowledgements We would like to...
95
University of Malawi Centre for Social Research The Role of Health Surveillance Assistants (HSAs) in the Delivery of Health Services and Immunisation in Malawi Study carried out by John M. Kadzandira (MSc) and Wycliffe R. Chilowa (PhD) for, and on behalf of Government of Malawi UNICEF Ministry of Health and Population P.O. Box 30375 P.O. Box 30377 Lilongwe 3 Lilongwe 3 Funded by UNICEF December 2001
Transcript of University of Malawi - Home page | UNICEF · 2019-06-07 · i Acknowledgements We would like to...

University of Malawi
Centre for Social Research
The Role of Health Surveillance Assistants (HSAs) in the Delivery of Health Services and Immunisation in Malawi
Study carried out by
John M. Kadzandira (MSc) and Wycliffe R. Chilowa (PhD)
for, and on behalf of
Government of Malawi UNICEF Ministry of Health and Population P.O. Box 30375 P.O. Box 30377 Lilongwe 3 Lilongwe 3
Funded by UNICEF
December 2001

i
Acknowledgements
We would like to thank UNICEF and the Ministry of Health and Population for entrusting the Centre for Social Research of the University of Malawi with the development and implementation of this study. Particular mention needs to be made of Dr. Juan Ortiz and Mr. Augustine Munyimbili, both of UNICEF and Mr. Barlie Makumba and Dr. Wesley Sangala, both of the Ministry of Health, who shared their ideas during the conceptualization and design stages of the study. Secondly, we would also like to acknowledge the assistance of the District Environmental Health Officers and Maternal and Child Health Coordinators from Salima, Nkhotakota, Ntchisi and Dowa where the main study was carried out and Machinga where the pilot was conducted. We would like to thank them for working with us and for all the assistance they rendered to the study team. Special thanks go to all the HSAs and mothers who participated in the survey for welcoming us and to all those who would have participated but did not because of sampling brackets. Lastly, we would like to thank the following people: members of the research team for their dedication to their work {James Mwera (Supervisor), Effie Kamwendo, Isabella Khureya, Rose Chiwaya and Frank Palamuleni}; Mr. Kazembe for driving the research team safely and Messrs. Chiocha and Kwizombe, both of the CSR, for providing the statistical support services including data entry and cleaning.

ii
TABLE OF CONTENTS Acknowledgements .........................................................................................................i LIST OF ACRONYMS ......................................................................................................vi Executive Summary......................................................................................................vii 1.0 INTRODUCTION....................................................................................................1
1.1 Problem Statement.................................................................................................... 1 1.2 Research Question ..................................................................................................... 2 1.3 Study Objectives ........................................................................................................ 2
2.0 OVERVIEW OF HEALTH SERVICES AND IMMUNISATION IN MALAWI ....................3
2.1 Health Services in Malawi ........................................................................................ 3 2.2 Immunization in Malawi........................................................................................... 5 2.3 Government Policy on EPI............................................................................................ 6 2.4 Social Demand for Vaccination ..................................................................................... 6 2.5 Trends in Vaccination Coverage.................................................................................... 8
3.0 HISTORICAL BACKGROUND OF HSAs ....................................................................11
3.1 The Origin .............................................................................................................. 11 3.2 The position of the HSA in the Ministry of Health.................................................. 12 3.3 Primary Health Care and the HSA ........................................................................... 12
4.0 METHODOLOGY ......................................................................................................14
4.1 Survey approach ....................................................................................................... 14 4.2 Survey Tools............................................................................................................. 14 4.3 Sampling .................................................................................................................. 15
4.3.1 Sampling for the pilot survey........................................................................... 15 4.3.2 Sampling for the main field survey .................................................................. 15
4.3.2.1 Sampling for the household interviews ............................................................ 15 4.3.2.2 Sampling of Health Centres for the household interviews.................................. 16 4.3.2.3 Sampling of areas and allocation of sample size per Health Centre .................... 16 4.3.2.4 Sampling of households and Respondents.................................................. 16
4.3.3 Sampling of the HSAs ..................................................................................... 16 4.4 Presentation of the findings ................................................................................... 16
5.0 FINDINGS FROM KEY INFORMANT INTERVIEWS.................................................17
5.1 Summary of findings ................................................................................................. 17 5.2 Job Description of the HSA........................................................................................ 18 5.3 Tasks being carried by HSAs ..................................................................................... 18
5.3.1 Immunization, growth monitoring and health talks ................................................. 19 5.3.2 Village and Business premises inspection............................................................... 20 5.3.3 TB work ............................................................................................................. 20 5.3.4 Water source protection and chlorination .............................................................. 20 5.3.5 Family planning................................................................................................... 21 5.3.6 Treatment of minor illnesses and Vector control..................................................... 21 5.3.7 Implementing the DRF and the BMHI.................................................................... 21 5.3.8 Supervising VHWCs and TBAs .............................................................................. 21 5.3.9 Working with NGOs ............................................................................................. 22
5.4 How are HSAs supervised?........................................................................................ 22 5.5 Technical and Social Constraints affecting the work of HSA’s........................................ 23
5.5.1 Limited opportunities........................................................................................... 23 5.5.2 Low salary and other financial rewards.................................................................. 24 5.5.3 Lack of/inadequate transport................................................................................ 24

iii
5.5.4 Low immunisation skills ....................................................................................... 24 5.5.6 Limited training................................................................................................... 24 5.5.7 Poor accommodation ........................................................................................... 25
5.6 Factors affecting immunisation coverage ..................................................................... 25 5.7 Strengths and weaknesses of HSAs............................................................................ 26 5.8 Suggestions for improving the work of the HSA .......................................................... 26 5.9 How else could HSAs be utilized?............................................................................... 27
6.0 FINDINGS FROM INTERVIEWS WITH HSAs..........................................................28
6.1 Summary of findings ................................................................................................ 28 6.2 Background characteristics of the sampled HSAs......................................................... 29
6.2.1 Education ........................................................................................................... 29 6.2.2 Age and Marital status ......................................................................................... 30 6.2.3 Religion.............................................................................................................. 30 6.2.4 Proportion of HSAs trained in HSA work ................................................................ 30 6.2.5 Length of service as HSA ..................................................................................... 31 6.2.6 Distance to health centers or hospitals .................................................................. 31 6.2.7 Size of catchment area and population.................................................................. 31 5.3.8 Working with health and water committees ........................................................... 32
6.3 Tasks being conducted by the sampled HSAs.............................................................. 32 6.3.1 Knowledge and reception of Terms of Reference.................................................... 32
6.4 Tasks enjoyed most by HSAs..................................................................................... 33 6.5 Tasks where HSAs lacked skills.................................................................................. 34 6.5 Tasks on which the HSAs were consulted frequently by the community......................... 34 6.7 Reasons why some people do not consult HSAs .......................................................... 35
6.7.1 Access factors..................................................................................................... 36 6.7.2 Relevance........................................................................................................... 36 6.7.3 Service quality .................................................................................................... 36 6.7.4 Fitness ............................................................................................................... 36
6.9 Proportion of children brought for growth monitoring .................................................. 36 6.10 Work carried out in the previous month.................................................................... 37
6.10.1 Disease investigation and treating patients .......................................................... 37 6.10.2 Nutrition and health talks ................................................................................... 37 6.10.3 Water treatment................................................................................................ 37 6.10.4 Family planning................................................................................................. 37 6.10.5 Other tasks carried out in September 2001 .......................................................... 38
6.11 Other activities conducted by HSAs at their health centres ......................................... 38 6.12 How do HSAs respond to emergencies?.................................................................... 38 6.13 Working with NGOs and other government projects .................................................. 38 6.14 Supervision............................................................................................................ 39 6.15 Significant community based projects initiated by HSAs in their catchment areas ......... 39 6.16 HSA Membership to local committees....................................................................... 39 6.17 Source of information ............................................................................................. 40 6.18 What other tasks could HSAs perform?..................................................................... 40 6.19 Living conditions ................................................................................................. 41
6.19.1 Housing............................................................................................................ 41 6.19.2 Salary............................................................................................................... 42 6.19.3 Other benefits attached to the HSA work............................................................. 42
6.20 Constraints to effective performance ........................................................................ 43 6.20.1 Technical .......................................................................................................... 43 6.20.2 Socio-cultural constraints ................................................................................... 43 6.20.3 Replenishment of drugs and materials................................................................. 44
6.21 HSA relations with the local community and other staff at the health centre ................ 45

iv
6.22 Suggestions to improve the work of HSAs as put forward by the sampled HSAs ........... 45 7.0 VIEWS AND PERCEPTIONS OF MOTHERS AND CHILD CARETAKERS....................47
7.1 Summary of findings ................................................................................................ 47 7.2 Characteristics of the households from which the sampled mothers/caretakers came ..... 47 7.3 Knowledge of HSAs and their work ............................................................................ 49 7.4 Functions of the HSAs............................................................................................... 50 7.5 Mothers/caretakers rating of HSA performance and that of other health staff ................ 51 7.6 Proportion of mothers/caretakers consulting an HSA ................................................... 53 7.7 Response to last illness............................................................................................. 54 7.8 Constraints facing HSAs in their work......................................................................... 54 7.9 Suggestions for improving the work of HSAs............................................................... 55
8.0 IMMUNISATION PERFORMANCE OF THE SAMPLED CHILDREN............................56
8.1 Reasons for late reception of vaccines or no receipt at all ............................................ 57 8.2 Place of receipt ........................................................................................................ 58
9.0 CONCLUSIONS AND RECOMMENDATIONS...........................................................60
9.1 Overall Conclusions ................................................................................................... 60 9.2 Overall Recommendations......................................................................................... 61 9.3 Specific recommendations to improve immunisation coverage rates .......................... 62
10. References.............................................................................................................63

v
List of Tables
Table 1: Percentage of children 12-23 months who had received specific vaccines by 12 months of age ........................................................................................................................ 10
Table 2: Background characteristics of the sampled HSAs...................................................... 29 Table 3: Training status of the sampled HSAs ...................................................................... 30 Table 4: Tasks contained in ToRs served to HSAs ................................................................. 33 Table 5: HSA Task preferences and level of skills ................................................................. 34 Table 6: Tasks for which most villagers consulted HSAs ........................................................ 35 Table 7: Activities carried out by HSAs at health centers ....................................................... 38 Table 8: NGOs and projects with which some of the sampled HSAs were working.................... 39 Table 9: Descriptive summary of housing conditions for the sampled HSAs ............................. 41 Table 10: Technical and socio-cultural constraints to HSA work cited by HSAs ........................ 44 Table 11: Availability of drugs and other materials among the sampled HSAs ......................... 45 Table 12: HSA rating of their relations with various groups of people...................................... 45 Table 13: Activities being implemented by HSAs as reported by mothers/caretakers ............... 51 Table 14: Mother’s/caretakers rating of HAS performance an a few selected activites............... 52 Table 15: Mothers rating of health staff that are commonly met at health centers .................. 53 Table 16: Activities for which HSAs were consulted most ....................................................... 53 Table 17: Constraints facing HSAs reported by women from Salima ....................................... 54 Table 18: Immunisation status of the sampled children in Salima .......................................... 57 Table 19: Main reasons cited by mothers/caretakers in Salima as to why their children received
certain vaccines very late or never received at all .......................................................... 58 Table 20: Places where various vaccines were received by the sampled children...................... 59
List of Figures Figure 1:Number of HSAs (trained and untrained in 8 HCs that were visited in Salima, Nkhotakota, Ntchisi
and Dowa Districtcs (October-November 2001)..................................................................... 24 Figure 2: Reasons given by HSAs as to why some people in their catchment areas do not consult
them (October-November 2001) ................................................................................... 35 Figure 3: Educational levels of the sampled mothers in Salima (November 2001)..................... 48 Figure 4: Population distribution of the sampled households .................................................. 49

vi
LIST OF ACRONYMS ADEHO Assistant District Environmental Health Officer
AEHO Area Environmental Health Officer
CHN Community Health Nurse
DDEHO Deputy District Environmental Health Officer
DEHO District Environmental Health Officer
EHA Environmental Health Assistant
EHO Environmental Health Officer
GOM Government of Malawi
HC Health Centre
HAS Health Surveillance Assistant
JCE Junior Certificate
KAP Knowledge, Attitudes and Practices
KII Key Informant Interviews
MCH Maternal and Child Health
MOHP Ministry of Health and Population
MSCE Malawi Schools Certificate Examinations
NGO Non-Governmental Organisation
PHC Primary Health Care
PO/CTO Professional Officer/Chief Technical Officer
PSLC Primary School Leaving Certificate
SAEHO Senior Assistant Environmental Health Officer
SC Subordinate Class
SSI Semi-Structured Interviews
STO Senior Technical Officer
TA Technical Assistant
VHC Village Health Committee

vii
Executive Summary
In October and November 2001, the Centre for Social Research (CSR) of the University of Malawi conducted a survey to assess the role of Health Surveillance Assistants (HSAs) in the delivery of health services and immunisation in Malawi and to explore the various constraints to their work. The survey was initiated jointly by the Government of Malawi (Ministry of Health) and UNICEF who also provided funding for all the activities related to the survey. Salima District was purposively selected for the study on the basis of its low immunisation coverage rates as reported in the DHS report of 20001. A total of 61 HSAs belonging to 14 health centres and 325 mothers/female child caretakers from catchment areas of nine health centres were randomly sampled and interviewed during the stated period. Sixty extra HSAs were also randomly sampled and interviewed in Nkhotakota, Ntchisi and Dowa districts (20 from each) so as to provide simple comparisons during analysis of the HSA data from Salima.
The general picture arising out from this survey is that HSA’s, formerly recruited as
temporary ‘Smallpox Vaccinators’ in the 1960’s and as ‘Cholera Assistants’ in mid 1970’s have contributed greatly to the delivery of preventive health services in rural areas of Malawi. Over time, they have formed an extensive network of ground staff bridging the formal health services and the community. They are responsible for about 60% of all vaccination that are given to underfive children in the rural areas. Their contribution has enabled the country to virtually eliminate and/or reduce prevalence rates of the highly infectious but preventable diseases namely: measles, polio, diptheria, pertusis, smallpox and tetanus. They also play a very significant role in detecting disease outbreaks and in providing assistance to the victims.
The job description of an HSA is very comprehensive and has continued to change over the
years as new interventions are introduced into the health sector. Currently, HSA tasks at community level include child (and mother) vaccination, growth monitoring, sanitation, water source protection and water treatment, disease surveillance, village and business inspection, health and nutrition talks and supervising traditional birth attendants and village health and water committees. Other tasks include providing family planning methods (condoms, pills and depo provera), implementing the Bakili Muluzi Health Initiative and the Drug Revolving Fund, following up TB patients and other health related tasks as advised by the government or NGOs.
In terms of time allocation, immunisation, growth monitoring and health talks occupy over
40% of the total HAS’s time, followed by sanitation and water protection activities (25%). Village talks about HIV/AIDS and family planning (FP) are also being carried out. Condoms, pills and injection (Depo provera) were the three FP methods being provided by sampled HSAs. Apart from working in the villages, some HSAs provide assistance at their health centres like manning the dispensary and dressing room, cleaning utensils, sterilizing needles and messengerial work. Treatment of minor illnesses, however, is not being carried out by most HSAs because of drug supply problems.
Most of the sampled HSAs (>30%) said that they enjoyed doing health talks and giving
immunisation compared to TB work and HIV/AIDS talks. Tasks in which most of the sample HSAs reported to lack skills included disease investigation, family planning, water treatment and administration of vaccines, particularly BCG and DPT.
1 It was perceived (during study concept) that the benefits from replicating the study in other districts would not justify the costs that would be incurred.

viii
On average, the sampled HSAs lived about 5km from their health centres although others
lived more that 20km away. The average population being served by the sampled HSAs was 2364 people but about 35% of them were serving more than 2500 people (maximum of 9500 for one HSA in the Salima district). The average distance to furthest villages for the sampled HSAs was reported to be 6km with the maximum being 17km.
While the HSA network is very extensive and considerably old, findings from this survey have
provided indications and evidence of undercoverage. Some sections in some catchment areas are not reached by HSAs mainly due to accessibility and mobility problems and, not all HSAs are implementing all the tasks as contained in their terms of reference. Six of the 325 mothers sampled had never previously heard of nor seen an HSA. Sanitation, growth monitoring, immunisation, family planning and health talks were cited by 60-88% of the sampled mothers while the rest said they had never heard of these activities being carried out in their villages, even after probing. This suggests that some pockets of households in the various communities are never reached by HSAs or that some tasks contained in the HSA Terms of Reference (ToRs) are not being implemented at all.
Most of the mothers sampled (>80%) who had interacted with an HSA before, applauded
those HSAs very highly for the work they were doing in their areas. However, some mothers felt that HSAs performance was being affected because of side effects in the case of vaccination, frequent shouting at mothers, boasting that they know more than villagers, irregular visits, infidelity and non-availability of drugs. Only 30% of the sampled mothers said that they had consulted an HSA before for some assistance other than immunisation, growth monitoring and heath talks. Access factors accounted for 54% of all the reasons why some mothers had never consulted the sampled HSAs followed by quality of service(21%), relevance (19%) and problems with scheduling (6%).
The survey also identified a number of constraints that are affecting the performance of
HSAs in the delivery of health services. Common constraints that were cited included mobility (transport) problems (69%), poor remuneration, no promotion and low status given to HSAs in the civil service (84%), irregular supply of vaccines and drugs (65%) and lack of protective clothing and stationery (65%). At the time of the survey, only 5 of the 121 sampled HSAs had antimalarial drugs, while 4 had antibiotics and 4 had pain relievers. On the other hand, condoms were available to 41 HSAs, child weighing scales to 59 HSAs and Oral Rehydration Sachets to 33 HSAs.
In addition to the above constraints, most HSAs are untrained (19% of the sampled HSAs)
and supervision is inadequate and irregular. This is mainly due to mobility problems, limited and irregular refresher courses and poor telecommunication systems.
Overall support to preventive health services has been declining over the years and this
mentality has trickled down to the district and health centre levels where preventive services are given little attention. Infact, some resources, notably vehicles, are diverted away to other sections.
On immunisation coverage, our findings indicate that over 80% of the 418 sampled children
had received all the vaccines for which they were eligible. As such, coverage in general was not bad but the problem was with the timing as most of children received the various vaccines very late. The findings also revealed a set of administrative and logistical hurdles to immunisation work, mainly at a level above than that of HSAs. These hurdles include lack of transport to carry vaccines, unavailability of some vaccines, non-functioning refrigerators and lack of paraffin, geographical inaccessibility especially during rainy season, high dropouts

ix
because of side effects of some vaccines, and inactive Village and Health Committees. Other problems include incorrect scheduling of immunization sessions (morning hours only when mothers are busy with other activities), laziness of mothers and cultural beliefs.
OVERALL RECOMMENDATIONS The overall recommendation being made by this report calls for increased support towards preventive health services and reorientation of priorities in budgetary allocation towards training and technical support in the Ministry of Health and Population so that infection and exposure rates are reduced. Specific recommendations are that:
o More HSAs must be recruited, trained and deployed to rural areas to reduce the workload among those currently in service;
o HSAs must be served with clear ToRs at the time of their recruitment and whenever new tasks are being introduced to the old ToRs. They should be thoroughly oriented in the various tasks that are contained in the ToRs through regular training and induction courses;
o There are some tasks in which the sampled HSAs said they lacked skills and knowledge. These areas (vaccinations, disease surveillance, HIV/AIDS and family planning talks, tallying and report writing) need to be properly addressed during HSA training and refresher courses;
o The level of supervision to the HSAs should be increased. This could motivate the HSAs as well assessing the HSAs levels of commitment to their work for onward recommendations to other benefits such further training and promotion;
o Measures must be taken against those HSAs not performing as expected and those who abuse their clients either verbally or immorally;
o (Despite being overloaded with tasks) HSAs could also be utilised to provide meat inspection services at community level if trained and oriented to do so. A lot of livestock are slaughtered every day, which are sold and consumed without any certification;
o Transport and mobility problems be reduced by provision of push bikes to HSAs and motor cycles to their supervisors on an ownership scheme. This would ensure that each HSA takes care of his/her bicycle or motorcycle as personal property. An annual maintenance allowance for the push bikes and motor cycles should also be provided to the HSAs;
o The position of HSAs be reviewed in terms of rank, salary scale and other allowances (for example housing, risk and duty allowances) and that opportunities for upward mobility be provided through further training and promotions. It is thus further recommended that some places should be reserved for serving HSAs during intake for the Degree/Diploma in Environmental Health Sciences at the University of Malawi, so that HSAs are given an opportunity.
To achieve these objectives, there is need for collaboration among various stakeholders (government, multilateral agencies, NGOs and the private sector) in terms of HSA training, development and provision of refresher courses and transport. This could be achieved through an independent and autonomous National Health Surveillance Programme (NHSP) with responsibility for HSA recruitment, training, deployment, supervision and monitoring. The NHSP could also provide advisory services to the various stakeholders that require the services of HSAs. Moreover, the HSA further training programme proposed above could be channeled through this proposed NHSP. As a way forward, the MoHP should develop a “Strategy Paper” that will outline plans for the future development HSAs in the country.

x
Specific recommendations to improve immunisation coverage rates
o In view of the fact that most mothers do not take their babies for vaccination or drop-out early because of side effects of some vaccines, it is recommended that new and better methods of administering the various vaccines should be researched, particularly DPT;
o Vaccines should be made available in all Health Centres at all times. Damaged and non-functioning refrigerators and vehicles should be repaired. The national EPI and the NHSP proposed above should, also assist HCs with fuel for vehicles and motor cycles. This would enable vaccines to be brought to mobile clinics on time thus maintaining the cold chain;
o The national EPI programme, which is mandated to promote immunisation activities in Malawi should also intensify civic education especially in rural areas on the importance of immunisation;
o Medical staff should accompany HSAs during vaccination to allow for the treatment of minor illnesses. This could be attracting some mothers/caretakers whose children are sick including those whose children who have not finished receiving their vaccinations.
1
1.0 INTRODUCTION In June 2001, the Centre for Social Research was approached by UNICEF to undertake a study that would provide answers to the apparent low immunization coverage rates that have been thought of as arising out of Health Surveillance Assistants taking on almost everything at community level. A study concept paper was developed and circulated to other stakeholders including the Ministry of Health, who also made their suggestions to the overall study design and approach. This resulted in shifting the focus of the study from sorely looking at whether immunisation coverage rates have been declining as a result of HSAs taking on almost everything at community level to assessing their contribution in the delivery of health services in general and their working conditions. For nearly a decade, Malawi has enjoyed very high immunization coverage rates of over 80%. Polio is virtually eradicated and measles is nearly eliminated. There are many possible factors to this high success. However, we do not have the evidence and documentation on those factors and the magnitude of their contribution. The latest DHS (2000) has reported a substantial decrease on immunization coverage rates, a 10% drop from around 80% to 70%. This drop is something to worry about very seriously. There might be many causes that can be attributed to the decline. It was therefore seen as very useful to document these causes so as to address them in project planning, implementation, monitoring and further evaluation. One of the most important factors that has been suggested to be responsible for the previous high immunisation coverage rates and the recent drop in these rates is the role that the Health Surveillance Assistants play in service delivery. In the past, most HSAs have been dedicated to support immunization services. Of late however, they have been seen as the "super health worker" capable of doing everything at community level. For example, they are very often asked to implement the whole of the health sector plan at community level. This apparently has taken the HSA away from supporting immunization services and may have resulted in a significant impact on immunization coverage. In itself this occurrence might not be too negative in that the HSA is moving away from supporting vertical interventions towards a more comprehensive and integrated support to service delivery. If this would be the case, the drop on immunization coverage would be a painful price to pay for a better reform. The feeling is that the HSAs are moving away from immunization to other vertical interventions that offer more incentives. Both UNICEF and the Ministry of Health have for some time been planning to carry out an evaluation of the role, contributions and efficiency of the HSA in service delivery from a historical point of view. It was thought that given the recent developments discussed above, now was an opportune time to conduct an evaluation of the roles of HSAs.
1.1 Problem Statement
The problems of the formal health services in Malawi have been documented widely. Findings from current studies reveal a myriad of failures in the supply of most health services. Access to formal services is impinged by distance and financial factors, service quality is extremely very poor and is highly characterized by drug and staff shortages, poor infrastructure and irreverence and negligence among health staff (Kadzandira & Mvula 2001, Namate, L, (2000). Immunization services seemed to be the only successful public health intervention in the country with over 80% coverage rates by antigen in the last couple of years. The decline in immunization rates documented in the 2000 DHS (by about 10%) is not only worrisome but also an observation that requires urgent investigation for intervention. Studies by Chilowa et. al (1997, 1998, 2000, 2001) have discerned a declining EPI performance between 1992 and 1996 in terms of full coverage

2
rates at the right age and as recommended by the World Health Organisation (WHO). The reasons for this decline have been enumerated in these reports and papers.
1.2 Research Question
The research question being posed by this study is as follows: “could the decline in the immunization coverage be as a result of the changing roles of Health Surveillance Assistants (HSAs) from that of full support to immunization to that of ‘super health worker’ capable of doing everything at community level?” While the change may be beneficial in as far as utilisation of human resources is concerned, the reverse may also be true. For example, the workload of the HSAs might have subsequently increased and as a result, s/he may choose to practice those other tasks of higher rewards at the expense of immunization. Much is not known on the ground and the suggested argument is mere guesswork. Non-availability of vaccines in some areas plus other logistical problems, poor management and priority not being given to preventive services could be alternative explanations. It was, therefore felt necessary to carryout a historical evaluation on the roles, contributions and efficiency of the HSA in terms of service delivery, particularly those related to immunization and growth monitoring. The findings of such a study could be document for policy purposes. Most health evaluation studies conducted in Malawi have focussed on the delivery of the health services or immunization in general. There is little data on the roles of the HSAs and how the reforms that have swept many sectors in the public services may have affected the delivery of the health services, in particular those related to immunization and primary health care. It was therefore imperative that a study focusing on the aspect of health care be conducted to guide health policy. Findings from the study would provide insight into the implementation of the national health plan.
1.3 Study Objectives
This study conducted an evaluation of the role, contributions and efficiency of the HSAs in the delivery of health services with particular focus on immunisation and primary health care. The study therefore assessed the historical roles of the HSAs, their origin, how their roles have changed over time and the impact that these changes have had on achievements in the health sector. Specifically, the objectives for the evaluation were:
to explore the historical roles of the HSAs in the delivery of health services; to determine the effectiveness (quantity and quality of work) of the HSA in the sector with
particular attention to immunisation and primary health care activities; to assess the working conditions and constraints against the efficiency of the HSAs work; to assess the community’s response to the HSA; and, to explore other health areas where the HSA can be utilised within the context of Primary
Health Care (PHC) without necessarily putting additional strain on him/her.

3
2.0 OVERVIEW OF HEALTH SERVICES AND IMMUNISATION IN MALAWI
2.1 Health Services in Malawi
Health care services in Malawi are provided on both a formal and informal basis, with the latter being provided by traditional healers, traditional birth attendants, local vendors and shops. Formal health services are structured around six levels, namely: health posts, health centres, rural hospitals, district hospitals, central hospitals and specialist hospitals. These formal services are delivered by the Government, Christian Health Association of Malawi (CHAM), non-governmental organisations (NGOs), private practitioners, and some large companies. The Ministry of Health and Population is the largest provider of the formal health services responsible for about 40% of the facilities while 19% are CHAM facilities. Local authorities manage 8% and the rest are managed by the private sector or NGOs (Chilowa and Munthali 1999). Services at community level include outreach activities (mainly primary health care type of activities) conducted through mobile clinics held either in public places or at manned or unmanned health posts. Most health centres on the other hand offer curative and maternal services. District hospitals are referral centres for health centres and they also service the local town population offering both in-patient and out-patient services. Central hospitals act as district hospitals for their own districts. They are different from district hospitals in that they provide specialist referral care for their respective regions. Lastly, specialist hospitals offer very specific services such as mental health services and in-patient care for leprosy and tuberculosis patients. Malawi’s health sector is facing problems of inadequate and inefficient allocation of resources as well as the other problems associated with the delivery of its services. The country’s health indicators are very poor and have continued to decline in the last decade. Prior to the 1980’s government clearly regarded health improvements as an aid to increased productivity of labour and not as a basic need. In the 1980s, the overall health policy was reviewed. The new concern was to raise the level of health of all Malawians by reducing the incidence of disease in the population. Particular attention was to be paid to the provision of services to mothers and children, including nutrition and child spacing. Primary Health Care (PHC), which was adopted in 1978, was to be the basic philosophy behind service delivery. It was believed that, through the use of the PHC approach, the more common diseases such as malaria and diarrhoea would be prevented or treated at home, thus obviating the need for hospitalisation and its associated costs. The adoption of PHC was viewed as an attempt to shift health care from the hospital to the community. In the long run this approach to health care was projected to be less expensive for the state than hospital-based care. However, the implementation of PHC has been slow and does not seem to have gone much beyond sensitisation of communities and the formation of village health committees (VHCs). The reasons for the slow progress in the implementation of PHC could be attributed to a number of factors including lack of appropriately qualified personnel, inadequate funding, the difficult of coordinating the activities of multiple government departments involved in health-related work, and possible resistance to the approach by some influential medical professionals who fear losing control over health care delivery to `under qualified' personnel. Government development policies for the 1990s were set out in the Statement of Development Policies 1987-96. It announced that the country would continue to place a high priority on economic growth as a means of realising an acceptable standard of welfare for its people.

4
Growth would be realised through increased productivity in the exploitation of the country's natural and human resources. Social sector expenditure would continue to be tightly controlled. It had become clear to the World Bank in the 1980s that economic growth did not automatically translate into higher standards of living for a country's population; deliberate effort had to be made to remove barriers that prevented certain segments of the population from enjoying the benefits of economic growth. Under World Bank guidance, the Malawi Government in May 1990 adopted a development strategy that sought to achieve economic growth while at the same time attempting to reduce poverty. Among the strategies the government was advised to adopt were: the removal of constraints placed upon growth in the informal sector, extension of licenses to smallholders, growing of high value tobacco, particularly burley tobacco, general expansion of the primary school programme to enable children of poorer households to attend school; and general expansion of primary health care services in rural areas. Permitting production of burley tobacco by smallholders was designed to improve rural incomes, while the opening up of the informal sector was designed to enable smallscale entrepreneurs to set up businesses and create employment for people who could not be absorbed into the formal employment sector. The latter marked the first formal recognition of the fact that alternative sources of income to smallholder agricultural production needed to be explored in the context of rapid population growth and increasing land scarcity. Although the health sector adopted PHC as the philosophy behind health delivery, little headway seems to have been made to make it applicable country-wide. New health units are being built, largely with donor assistance, and more are promised. These health units, when they have resources, provide curative services as well as maternal and child care services. For a village community in Malawi to have a health unit is a visible symbol of their community's development. Pressure will, therefore, continue on the government to provide more health units. In 1995 71% of the Malawi population lived within a 5km radius of a health unit, which is remarkable by African standards. But proximity to a health unit does not always mean access to health care. Due to the economic difficulties the government has been going through these last few years, many health units experienced recurrent drug shortages. At various times, patients have had to be turned away without treatment from most health establishments. A preventive approach to health would limit the incidence of disease, perhaps at a lower cost than hospital-based health care. This might ultimately contribute to a healthier population than the current curative approach. However, the practice in the Ministry of Health and Population has been and is still, to allocate the lion’s share of the budget to curative services, seconded by overheads with only a meager going to preventive services, which is the priority area (World Bank 2001). It is hoped that this practice will change for the better and requisite resources will begin to be allocated where the priority lies, i.e. preventive services. The Malawi Government recognizes that, despite the fact that the health service delivery is largely funded by the public sector, donor agencies are also playing a major role as a source of financing for health care services. The amount of resources that the Government puts into the health sector is not adequate to cater for the health needs of Malawi's growing population. This is exemplified by the general lack of essential drugs and medical equipment in Government health facilities and the drifting of medical personnel either into the private sector or to other countries because of poor remuneration. As in all government departments, the recurrent budget in the MoHP is generally inadequate to meet the needs of the growing population. Hence, the Ministry relies on donor aid from both bilateral and multilateral agencies.

5
2.2 Immunization in Malawi
The goal of immunization programmes is the sustainable control of vaccine preventable infectious diseases. The sustainability of any health intervention, such as the vaccination programme, ultimately depends not simply on public compliance but also on public demand. This demand encompasses widespread acceptance of the prevention programme and a willingness to pay for it, either through direct community funding or through government subsidies obtained from taxes, or as it has been for Malawi, through donor funding as a stopgap measure. The Demographic and Health Survey (DHS) of 1992 indicated that over 82% of all children aged 12-23 months had received all the recommended vaccination, 67% before their first birthday as recommended by the World Health Organization (WHO). In comparison, the 1995 Malawi Social Indicators Survey (MSIS) showed that 75% of children aged 12-23 months at the time of the survey had all the recommended vaccines, 61% before their first birthday, a slight drop from the 1992 figures. What was significant in the MSIS was that the figures for those children who had been vaccinated by 12 months of age for BCG, DPT and were considered "fully" immunized, showed a statistically significant drop from the 1992 DHS. This was the first time a drop had been recorded. Similarly, the 1996 Malawi Knowledge, Attitudes and Practices in Health Survey (MKAPHS) reported that complete vaccination at any time before the survey among children aged 12-23 months was 81%, while 55% of children were reported to have been fully vaccinated before their first birthday. The 2000 DHS results revealed that overall, 70% of all children aged 12-23 months had all the recommended vaccination, 54% before their first birthday. These results confirm the contention that there has been a discernible downward trend in the Expanded Programme on Immunization (EPI) performance. As regards the official view of coverage figures in Malawi, coverage of children with the basic EPI vaccines appears to have reached upwards of 80 percent, but unfortunately this is by antigen and by the time of the survey. The recommended coverage figures are those where the children aged 12-23 months should have been fully vaccinated by their first birthday (i.e. by 12 months). These have been consistently lower in Malawi indicating the poor EPI performance over the years due to various problems as will be elucidated below. UNICEF and other donor agencies have funded studies on immunization coverage, EPI disease surveillance and monitoring and evaluation of EPI. However, there is general lack of information regarding compliance with and social demand for immunization services, quality of care and sustainability of vaccination services. Even where the availability of vaccination services are known and accessible, they are often under-utilized. Several authors have noted that certain factors affect demand and, hence, coverage and sustainability. Such factors include availability and accessibility of services, quality of health education, vaccine potency, educational level of the mother (and the father), societal beliefs, attitude of health workers to users and community's perception of vaccination services (Heggenhoegen, 1995; Streefland, 1995; Nichter, 1995). As will be discussed below, there are variations in immunization coverage rates in Malawi basically because of variations in people’s cultural and social lifestyles. Official reporting of immunization figures in Malawi is flawed in the sense that the coverage rates that are usually reported are those by antigen, and by the time of the survey, which are obviously higher. However, the correct figures recommended by WHO to be reported are those of children 12-23 months old that have been fully vaccinated by their first birthday. These have been consistently lower in Malawi from 1989. By reporting these it will assist Government policy makers to appreciate where things are going wrong and facilitate them to respond effectively.

6
The current official reporting of artificially inflated immunisation rates has allowed government to become complacent and to believe that the EPI performance is on track.
2.3 Government Policy on EPI
The Government of Malawi’s health policy aims at raising the level of health of all Malawians through the provision of a sound health care delivery system. One of the strategies that Government has instituted to effect the health policy is the strengthening and expansion of the maternal and child health programmes. The Expanded Programme on Immunization (EPI), which is an attempt to coordinate and expand a number of individual immunization programmes, has been fully integrated into the Maternal and Child Health (MCH) programme. It has been suggested that by fully immunizing children, the spread of EPI diseases shall be stopped thereby saving the lives and protecting the future health of children. The EPI aims at immunizing children against diseases such as measles, poliomyelitis, tuberculosis, diphtheria, pertussis and tetanus through vaccination. A plan for EPI was drawn in 1978 in collaboration with the World Health Organization. Through the EPI, four types of vaccines are given to children namely measles, polio, BCG against tuberculosis and DPT against diphtheria, pertussis and tetanus. For a child to be considered fully immunized s/he should have received one dose of BCG vaccine, one dose of measles vaccine, three doses of DPT and three doses of polio vaccine. If the vaccination schedule is to be adhered to, a child should have received all vaccines and be considerede fully immunized by the age of 12 months. In Malawi, the policy regarding EPI aims to:
immunize all children under the age of twelve months with the goal of reducing morbidity and mortality as a result of the six preventable and infectious diseases; and
immunize all pregnant women and females of child bearing age in order to protect the unborn children against neonatal tetanus and the mother against tetanus (Ministry of Health and Population : EPI Unit, 1994).
The MoHP is responsible for vaccination activities in Malawi. The head of the EPI is the National Programme Manager who reports to the Controller of Preventive Health Services. Under the National Programme Manager are the National Logistics/Cold Chain Officer and the Central EPI Stores Officer. At regional level, there is a Regional EPI Officer and a Cold Chain Officer. At district level the MCH Coordinator is responsible for the day-to-day running of the immunization programme and reports to the District Environmental Health Officer. A Health Assistant oversees the EPI activities at the health centre level and in most cases the HSAs are the ones who are responsible for vaccinating the children. These HSAs are ideally supposed to live within the community.
2.4 Social Demand for Vaccination
Immunization has been recognized and accepted as one of the most important components in the prevention and control of communicable diseases. It is a basic health service, therefore, it has been integrated into the health care delivery system of the MoHP in Malawi. Despite the tremendous progress that has been made in the prevention of vaccine preventable diseases through vaccination, there is still a lot of controversy surrounding the introduction of vaccination programmes in developing countries. Some of the issues raised by the clients of vaccination programmes include the development of side effects after a child has been

7
vaccinated and misconceptions that vaccination are for family planning purposes and not for disease prevention as advocated by the vaccinating regimes. It is not only in Malawi where such controversies have arisen. In India, for example, the Muslim minority fear that the Hindu majority may be covertly introducing family planning through vaccination programmes so that their population should never outnumber that of the Hindus for political reasons (Nichter 1995). Some people perceive vaccination as a threat to traditional values, and it has been contended that after receiving the protection of vaccines and foreign medicines the population would be civilized in the western sense at the expense of their moral and ethnic identity (Nichter, 1995). Research has shown that socio-economic factors also affect peoples’ utilization and acceptance of health services, use of folk remedies and self-medications. Socio-economic status can also create a feeling of social distance between the health practitioners and clients; impoverished persons feel less at ease in medical settings than more affluent persons (Mechanic, 1974). Such beliefs, practices and misconceptions can adversely affect the demand for vaccination services, hence, immunization coverage. An important point of attention is the appropriateness of the provision of vaccination. Firstly, this concerns the so-called technical quality of care: whether providers of vaccination do their work bio-medically correct and complete, using existing professional knowledge and standards. Secondly, it regards the way in which the providers relate to their clients whether their relation is characterized by "...privacy, confidentiality, informed choice, concern, empathy, honesty, tact and sensitivity" (Donabedian, 1988,17-44). This is the interpersonal quality of care. Thirdly, the perceived quality of care is also an issue. The perceptions that the users and the providers have of the technical and interpersonal quality of care. The mothers/caretakers who attend vaccination sessions may be called acceptors. Acceptance of vaccination does not imply necessarily that it is based on a bio-medically correct and complete understanding of vaccination. In fact, at local level, within certain groups or village societies, vaccination cultures prevail, which include knowledge, beliefs, practices and experiences with regard to vaccination. Such local cultures include past experiences of side effects of vaccines, rumours about intended use of vaccination for improper purposes, experiences of epidemics, preferences for certain medical technologies, folk aetiologies of vaccine preventable diseases, various lay explanations about the efficacy of vaccination (this may, for instance, be considered disease specific or rather boosting general health improvement). Besides the clients' behaviour being grounded in the local vaccination culture, it is also related to personal experiences and the individual vaccination history. This concerns, for instance, the personal history of side effects of certain vaccines. Health services provide vaccination as a preventive health intervention and usually require that the mothers attend vaccination sessions at certain places at certain times. The way in which compliance with the vaccination rules and regulations is encouraged may be called a vaccination regime. Such a vaccination regime may be promotive, encouraging compliance through health education and supportive follow-up activities (e.g. home visits), or it may be prescriptive, emphasizing control through sanctions, manipulation of public opinion, or use of local power structures (e.g. reminding mothers through the mediation of a village chief). Vaccination regimes may also combine promotive and prescriptive elements (Chilowa and Munthali, 1999). The actual provision of vaccinations, be it in static health centre settings or in outreach conditions, is a set of behavioural patterns of providers and consumers, based on rules, regulations, expectations, experiences and assumptions of all involved. This may be termed the vaccination practice, which may be characterized and experienced as being campaign like (For example, the vaccination practice can include unfamiliar locations and different timings, as in the case of the National Immunization Days (NID's) or it can be more routine, with familiar staff, using fixed timings at fixed locations.

8
Non-acceptance of vaccinations may be defined as a situation when potential users do not come to vaccination sessions when invited to do so. There may be various reasons behind this and it is important to distinguish them. Firstly, non-acceptance may be based on misunderstanding due to, for example, to lack of information or negligence. Secondly, the mother may be willing but unable to attend due to, for instance, pressing tasks, lack of travel money and social obligations such as a funeral in the village. Thirdly, a parent may be refusing to allow vaccinations. There may be different reasons for such individual behaviour including the conviction that the vaccination is not necessary or is harmful. It may also be based on previous experiences of side-effects of the vaccines or rude behaviour of the providers. Fourthly, non-acceptance may be a collective response by a number of parents. This may be the case when a joint religious conviction stands in the way of vaccination, or when a certain rumour (e.g. about vaccination being related to family planning practices) leads to a collective reaction of non-acceptance. Vaccination programmes are intended to continue over a long period of time. Their sustainability can be defined in two ways. Firstly, by emphasizing the financial (financial sustainability) and political (political sustainability) support necessary to maintain immunization activities at the required scale and standard. Secondly, by stressing the relationship to high levels of coverage and defining sustainability as sustained high rates of coverage.
2.5 Trends in Vaccination Coverage
A number of evaluations have been carried out in Malawi since 1980 aimed at determining coverage rates as well as progress that the Immunization programme has made towards immunizing children and mothers. It will be noted that Malawi has made considerable progress in immunisation coverage rates since the Expanded Programme on Immunization (EPI) was officially launched in 1978/79. In 1980 that the MoHP carried out an evaluation of the EPI in three districts, namely Mzimba, Lilongwe and Thyolo. The immunization coverage rates ranged from 66 percent to 79 percent for BCG, 23 percent to 50 percent for the third dose of polio, 40 percent to 51 percent for the third dose of DPT and 58 percent to 64 percent for measles. Percentages of fully immunized children ranged from 20 to 39 percent. National immunization coverage rates for 1982 were 69 percent for the third dose of DPT, 72 percent for the third dose of polio, 70 percent for measles and 82 percent for BCG (Chilowa et al 1999). The proportion of fully immunized children was 55 percent. These results showed that there was an improvement over those figures obtained in 1980. Nsanje, a district in Southern Malawi, was among other districts in which surveys aimed at determining coverage rates were conducted in 1988. The evaluation revealed that 59 percent of the children were fully immunized that year. During the 1991 evaluation,77 percent of the 211 children were fully immunized. The coverage for each antigen were as follows: 95 percent for BCG, 80 percent for DPT3, 83 percent for Polio and 86 percent for measles. Approximately 1% of the children were not immunized at all and 22 percent were partially immunized. During the same survey, 210 women were interviewed of which 91 percent had received TT1, 79 percent TT2, 35 percent TT3, 12 percent TT4 and 5 percent TT5 (Ministry of Health and Population, 1991). A survey that was carried out in Lilongwe by Chilowa et al (1991) showed that 55 percent of the 210 children in the sample were fully immunized, 42 percent partially immunized and 3 percent not immunized. The coverage for each antigen was as follows: 92 percent for BCG, 58 percent for DPT3, 56 percent for Polio 3 and 49 percent for measles.

9
During the 1992 Demographic and Health Survey (DHS) that was conducted by the National Statistical Office (NSO), 97 percent of the children in Malawi aged between 12 and 23 months were vaccinated against tuberculosis and about 95 percent received the BCG vaccination by the age of 12 months. This information was based on availability of vaccination cards as well as the mothers' report. Immunization coverage for the first dose of polio and first dose of DPT was 97 percent. However, coverage declined after the first dose with 94 percent and 88 percent receiving the second and third doses respectively, yielding a drop-out rate of about 9 percent for the DPT and polio vaccines. As reported, 86 percent of children aged 12 - 23 months had been vaccinated against measles, 70 percent before their first birthday. Overall 82 percent of all children aged 12-23 months had all the recommended vaccines at the time of the survey, 67 percent of whom had received before their first birthday. Approximately three percent of the children aged 12-23 months had not received any vaccination. The 1992 DHS also revealed that children from urban areas (87 percent) had a slightly better immunisation coverage rates than rural based children (81 percent). Complete coverage increased with maternal education from 76 percent among children of uneducated mothers to 96 percent among children of mothers with some secondary education. The Malawi Social Indicators Survey (Chilowa et al 1995), revealed for the first time in a decade that there was a significant drop in immunization coverage rates in Malawi. The survey revealed that 61% of the children aged 12-23 months were fully immunized by their first birthday (compared to 67 percent reported in the 1992 DHS). Seventy five percent for the same age group (82 percent in 1992) were fully immunized at the time of the survey. The figures for individual antigens were higher. For those children who were fully immunized by their first birthday, coverage for BCG was at 91 percent, polio 80 percent, DPT 76 percent and measles 70 percent. Comparisons with coverage recorded in 1992 during the DHS survey indicate that apart from measles, whose rate has been maintained at 70 percent, the rates for all other antigens have gone down. One explanation could be the unavailability of some vaccines especially DPT and Measles during some periods in the country, as a result of both financial and logistical reasons. The downward trend in EPI performance could be a consequence of the effects of the cash budget on service delivery for which there has been anecdotal evidence through the EPI's field monitoring trips. Measles is the most likely antigen to have the lowest coverage by 12 months of age since the window of opportunity to receive this vaccination before the first birthday is narrow, even under the best of circumstances. Thus, any decrease in number of possible contacts (such as decreased outreach clinic visits) is likely to affect measles coverage first. The fact that DPT is less than OPV coverage is probably due to the three months-long DPT vaccine shortage which occurred in early 1995.

10
Table 1: Percentage of children 12-23 months who had received specific vaccines by 12 months of age
Fully Vaccinated
BCG DPT* OPV* Measles Number of children in the Sample
Malawi 61 (2.3) 91 (1.1) 76 (1.8) 80 (1.7) 70 (2.1) 975
Region North Centre South
67 (4.5) 58 (2.9) 62 (4.0)
93 (2.4) 91 (1.5) 92 (1.7)
83 (3.0) 71 (2.9) 80 (2.8)
81 (3.4) 78 (2.5) 83 (2.7)
71 (4.7) 71 (2.6) 69 (3.7)
186 438 351
District Chitipa Karonga Rumphi Mzimba Nkhata-Bay
81 (7.6) 52 (11.6) 74 (5.0) 63 (7.0) 74 (13.1)
92 (4.7) 100 (0.0) 88 (7.0) 91 (4.3) 98 (2.7)
93 (3.9) 78 (8.2) 87 (7.3) 78 (3.7) 90 (8.4)
89 (4.6) 74 (7.4) 86 (7.7) 77 (5.5) 90 (8.4)
84 (7.2) 59 (8.7) 67 (8.9) 71 (9.1) 81 (9.1)
33 24 29 72 28
Kasungu Mchinji Lilongwe Dowa Nkhota-Kota Salima Dedza Ntcheu Ntchisi
59 (10.3) 41 (12.3) 50 (4.8) 57 (6.8) 59 (12.6) 68 (6.0) 72 (5.8) 80 (6.8) 30 (8.0)
97 (2.2) 89 (5.1) 86 (4.1) 91 (3.6) 88 (4.5) 98 (1.9) 89 (2.7) 97 (0.9) 88 (4.1)
78 (8.6) 62 (7.2) 62 (5.5) 71 (11.5) 77 (7.7) 70 (5.0) 80 (4.7) 87 (5.4) 59 (5.7)
87 (4.7) 62 (8.7) 71 (5.4) 80 (8.9) 73 (10.5) 85 (1.6) 85 (2.4) 88 (4.2) 67 (3.4)
66 (7.4) 51 (14.2) 69 (4.7) 75 (4.4) 68 (9.6) 74 (6.8) 80 (2.9) 83 (6.4) 50 (8.7)
35 34 127 47 33 43 36 40 43
Mangochi Machinga Zomba Mwanza Blantyre Mulanje Thyolo Chiradzulu Chikwawa Nsanje
63 (9.6) 35 (10.6) 73 (7.2) 64 (11.4) 71 (6.4) 58 (12.9) 63 (13.9) 79 (10.3) 56 (10.7) 58 (21.3)
94 (3.8) 89 (4.9) 91 (5.3) 92 (4.2) 94 (3.3) 87 (7.4) 87 (5.3) 100 (0.0) 98 (2.1) 83 (3.6)
88 (7.0) 54 (6.8) 80 (2.5) 72 (8.2) 91 (4.6) 78 (8.4) 83 (11.3) 87 (8.9) 78 (10.2) 71 (10.1)
77 (10.1) 77 (8.5) 77 (4.7) 83 (4.9) 89 (5.1) 81 (7.9) 86 (10.6) 93 (7.2) 91 (4.4) 78 (5.0)
69 (7.8) 48 (12.9) 81 (2.5) 78 (6.9) 74 (6.1) 58 (12.9) 72 (14.9) 82 (8.6) 80 (5.8) 56 (17.4)
37 37 49 41 53 23 23 22 30 36
Residence Urban Rural
69 (7.6) 60 (2.4)
86 (5.8) 92 (1.0)
78 (7.4) 76 (1.9)
79 (7.5) 80 (1.7)
78 (7.6) 69 (2.1)
108 867
Sex Male Female
59 (2.9) 62 (2.8)
90 (1.8) 93 (1.4)
75 (2.6) 76 (2.3)
80 (2.5) 80 (2.0)
68 (2.7) 72 (2.5)
482 491
* Three doses of DPT and Polio Percent Standard Errors (SE percent) in Brackets. Source : Chilowa, et. al (1996).

11
3.0 HISTORICAL BACKGROUND OF HSAs
3.1 The Origin Malawi was hit by an outbreak of smallpox in the period before the early 1960s, a situation to which the Ministry of Health (MoH) responded by recruiting a cadre of temporary staff whom it called ‘Smallpox Vaccinators’ specifically to deal with the outbreak. Just as smallpox was almost obliterated (in 1973), there was a cholera outbreak in the country particularly in the Southern District of Nsanje. Village Health Committees (VHCs) were established in all the villages to deal with the outbreak comprising untrained volunteer individuals from within the various villages. There was therefore a need to employ Cholera Assistants who would train the various VHCs as well as helping in the actual control and preventive measures against further spread of the outbreak. Thus, the Vaccinators were deployed to Nsanje (Namilaza 1998), from where they were redeployed to do similar work in other districts of the country because the outbreak had spread throughout the country. Other Cholera Assistants were recruited as well. The recurring cholera outbreaks were put to rest around the early 1980’s. The MoHP then wanted to boot out all the Cholera Assistants and cease their recruitment because it was thought that there was going to be no further requirements for their services. However, the preventive section of the Ministry successfully negotiated for their retention, under a new mandate of ‘surveying’ factors and behaviours that put people’s health at risk and providing primary assistance before referring complicated cases to health centers and hospitals, hence the name ‘Health Surveillance Assistants’. Over the years, the mandate of HSAs has widened considerably. The position of HSAs remained temporal and officially non-existent in the structure of the Ministry of Health until 1995 when it was decided to make it permanent and equivalent to Subordinate Class II (SC II). The policy at the time when the position of HSA was being regularized was that aspiring applicants should possess a minimum qualification of a Malawi Junior certificate (JCE) and a maximum of the Malawi Schools Certificate (MSCE)2. They were all, on recruitment, at the level of SC II. According to the Human Resources Development Plan for the Environmental Section of the MoHP, each HSA has an opportunity of being promoted to the position of Environmental Health Assistant (EHA) after pursuing a short in-service training for about 12 months following successful performance in one’s work (GoM 1997). To ensure a high quality of services, all HSAs are required to undergo an intensive 8-week HSA induction course3 before being considered for the position. The course is planned for every two years for about 300 new candidates countrywide. Upon deployment, one HSA is expected to serve a population of about 2,000-2,500 people (6000 HSAs for the whole country).
2 The current civil service human resource policy though does not recruit JC holders anymore. 3 The induction course is based on a curriculum developed in 1987 which, according to the Acting Chief Environmental Officer based at the Ministry of Health, may be outdated considering the trend of events in the health sector. The course does not incorporate participatory approaches

12
3.2 The position of the HSA in the Ministry of Health HSAs are under the Environmental Health Section of the Ministry of Health and Population. Each district is expected to have a District Environmental Health Officer (DEHO) and his/her deputy (DDEHO) to manage all the preventive public health activities in the District (Appendix 1). The DEHOs report to their respective Regional Environmental Health offices who also report to the office of the Chief Environmental Health Officer based at the MoHP headquarters. Below the DDEHO are four Assistant District Environmental Health Officers (ADEHO) responsible for Health and Safety, Water and Sanitation, Food Hygiene and Quality Control, and Vector and Disease Control, respectively. The four ADEHOs are at PO/CTO grade. Moving down the organogram, there are Area Environmental Health Officers (AEHOs) at PO/CTO grade whose numbers in a district vary depending on the population of the district. The AEHOs are direct supervisors4 of the Senior Assistant Environmental Health Officers (SAEHOs) whose position is at STO grade (each AEHO supervising about two SAEHOs) while the SAEHOs are direct supervisors of Assistant Environmental Health Officers at TO grade. Each TO supervises about two EHAs who are at the level of Technical Assistant (TA). EHAs are supposed to be the immediate supervisors of the HSAs (each supervising about 5 HSAs or a total population of about 10,000 people). The HSA is the point of contact between the formal health service delivery system and the community. As such, information and new ideas in the preventive health sector that trickle down the ladder from the Ministry and from research has to be implemented at community level via the catalytic functions of the HSA. However, as will be noted in the findings from the field survey, the HSA also receives instructions from and implements activities on behalf of a wider range of health service providers including Community Health Nurses (CHNs), NGOs and other government departments. In terms of training, HSAs undergo an 8-week training programme at several PHC centers countrywide, whereas EHAs undergo a 2-year training programme at the Malawi College of Health Sciences. AEHOs undergo a 3-year training at MCHS while EHOs undergo a 4-5 year training programme at the Malawi Polytechnic in Blantyre.
3.3 Primary Health Care and the HSA
Malawi endorsed the Alma Ata declaration on achieving ‘Health for All by 2000’ using the Primary Health Care (PHC) approach in 1979 (Bennet & Cole-King 1982; Msukwa 1987; Russell & Reynolds 1984). Malawi therefore committed itself to the concept of PHC, which revolves around the active participation of local communities in meeting their health needs and simultaneously the development of basic health infrastructure and services to provide accessible supporting health care which penetrates into all rural areas. The PHC approach is a complete departure from an ‘Extension Approach’, where health workers diagnosed health problems for the community and taught them ways of dealing with the problems. The extension approach led to overgeneralization of health problems and their associated risk factors across communities. In general terms, PHC addresses the main health problems in the communities through providing promotive, preventive, curative and rehabilitative services with active community involvement and at a cost that is affordable. PHC includes, education concerning prevailing health problems,
4 Specific duties of the various officers are detailed in GoM, Ministry of Health and Population 1997: “Human Resource Development: Environmental Health Section”

13
promotion of food supply and proper nutrition, adequate supply of safe water and basic sanitation, Maternal and Child Health (MCH) care including family planning, immunization against major diseases, treatment of common diseases and injuries, promotion of mental health and provision of essential drugs. From 1980-1989, the Government of Malawi had been setting up PHC infrastructure and implementing capacity building activities at national, regional and district levels (GoM 1999). In 1984, the GoM decided to involve HSAs (who were at this time only involved in selected immunization and cholera control activities) in working with VHCs in promoting the health of their communities. Over the years there has never been any comprehensive evaluation of the PHC implementation in the various local communities. A more recent assessment of HSAs knowledge, attitudes and practices (KAP) of the PHC approach revealed that HSAs lacked knowledge of the approach (Chitimbe 1998). Only about 15% of the 74 HSAs who were included in the study were able to define and explain how the approach works. The study also observed that most HSAs had no basic training and very few had attended refresher courses. It also concluded that some of the HSAs were using the PHC approach unknowingly.

14
4.0 METHODOLOGY
4.1 Survey approach
The survey, which was cross-sectional and explorative in nature, was conceptualized jointly by the MoHP, UNICEF and the Centre for Social Research of the University of Malawi as indicated above. Salima District was purposively selected for the main survey because it recorded low immunization coverage rates as reported in the MDHS of 2000. The other three Districts (Nkhotakota, Ntchisi and Dowa) were included for the purpose of providing backup data for simple comparison purposes and were thus purposively selected based on logistical consideration. After the study tools were drafted, four Research Assistants (RAs) and 1 Supervisor were recruited and trained for about three days prior to a pilot survey in Machinga District. The four RAs conducted household interviews while the Supervisor interviewed HSAs. As the study progressed, the supervisor was joined by the rest after they had completed the household interviews. The two Principal Investigators conducted the Key Informant Interviews (KII) as well the literature review.
4.2 Survey Tools5
Three principal methods namely KII, Semi-structured Interviews (SSI) and a Literature Review were used in the survey. Key Informants included DEHOs in the four Districts, Supervisors of HSAs at community level and the Acting Chief Environmental Health Officer at the Ministry of Health. In total, 14 Key Informants were interviewed in the four districts. The informants were asked to give their experiences in working with HSAs, the perceived strengths and weaknesses of HSAs and the type of supervisory support that they are providing to the HSAs. Based on their experiences, they were also asked to suggest ways of improving the work of HSA and what they feel could be reasons for reduced immunization coverage in some areas of the country. In the SSI, individual interviews were held with 121 HSAs from the four districts and 325 mothers/caretakers of children under the age of five years from Salima district. In the HSA questionnaire, HSAs were asked about their job description, tasks, which they were implementing in their catchment areas, and technical and social constraints which they were facing in their job. They were also asked to evaluate themselves in terms of achievements which they had made in their areas. Furthermore, the HSAs were also asked to state their general working conditions, their relations with the communities and to suggest was of improving the work of HSAs in the country. The mothers were asked about their experiences in working/or not working with HSAs, the range of services they access through HSAs and immunization status of their children. The literature review focused mainly on the two areas namely, immunisation and the historical impact of the HSAs in Malawi. In the process, it was learnt that literature on immunisation is readily available while literature about on HSAs is scanty and not properly articulated.
5 The questionnaires and KII guides are attached at the end as appendices 5, 6 and 7

15
4.3 Sampling
The section below discusses how the various respondents were sampled/selected starting with the pilot survey. Lessons learnt during the pilot directly fed into the main survey.
4.3.1 Sampling for the pilot survey A pilot survey was conducted to test the various draft survey tools and to assess the feasibility and relevance of the proposed sampling plan. A total of 18 household interviews were conducted in Matandika village, one of the villages in the catchment area of Machinga Health Centre. Households for inclusion were selected on the basis of having a child aged between 3-59 months, as some sections of the questionnaire were asking about child immunizations. This was the first point of departure from the sampling plan indicated in the proposal, which suggested that households to be included in the sample would be derived after conducting an initial village census which would be used for screening purposes. The second point of departure was the definition of geographical boundary for the study areas. The pilot survey used catchment area of a health center as the study geographical area (as opposed to census EA) and a list of HSAs as sampling frame for HSAs while a list of villages for one selected HSA as frame for sampling the village to be included in the pilot. Main lessons learnt from the pilot survey therefore were that:
sampling households using the Enumeration Areas (EAs) as defined by the National Population and Housing Census would not have been the best approach to capture people’s views and experiences in working (or not working) with Health Surveillance Assistants because chances are that one HSA covers several EAs. Conducting the household interviews in one EA would have therefore meant capturing views, reactions and experiences of 325 interviewees concerning one HSA, a situation that would be grossly misleading;
Conducting preliminary community censuses for screening purposes was not feasible considering the time and budgetary constraints of the survey;
Most HSAs and their supervisors (Senior HSAs and Health Assistants) do not keep immunization records because they are submitted to the office of Maternal and Child Health Coordinator (MCH) once they are compiled. They don’t retain any copies because of stationery problems.
Lessons cited above necessitated alterations to the study design i.e. sampling of households and collection of immunization statistics for the main survey. Furthermore, immunization statistics kept by MCH Coordinators do not indicate the proportions conducted by HSAs.
4.3.2 Sampling for the main field survey 4.3.2.1 Sampling for the household interviews
A multi-stage cluster sampling technique was adopted. The first stage was the sampling of health centers in whose catchment areas the questionnaires were to be administered followed by the sampling of HSA catchment areas, villages and households respectively.

16
4.3.2.2 Sampling of Health Centres for the household interviews
Salima District has 18 health centres, one District hospital and about 175 HSAs. A total of nine health centres (50%) were sampled for the household interviews. Salima and Kaphatenga HCs were classified as HCs serving the peri-urban population because of their close proximity to the District Headquarters although some of the HSAs who report to the two centres serve very remote communities. Thus, Salima and Kaphatenga HCs were therefore purposively selected on that basis. The other seven rural HCs namely Lifuwu, Kaundu, Golomoti6, Mchoka, Thavite, Chipoka and Khombedza were randomly sampled from the remaining 17 rural HCs. 4.3.2.3 Sampling of areas and allocation of sample size per Health Centre
One third of the household interviews (109) were conducted in the catchment areas of the two peri-urban HCs, while the remaining 216 were conducted in the rural HCs. Allocation of sample size per health centre for the nine sampled HCs was proportionate to the number of HSAs serving in the catchment areas of each health centre. From each of the nine health centres, catchment areas of 2 to 5 HSAs, depending on number of HSAs at the HC were randomly sampled and included in the survey. A list of villages in these areas was drawn and about 1 to 2 villages were sampled. Allocation of sample sizes for each of the sampled catchment areas and villages was proportional to their population sizes. 4.3.2.4 Sampling of households and Respondents
Starting at an approximated central point in a village, the 4 RAs were moved in four different directions from each other (at right angles) holding interviews at any household that had a child aged between 3 and 59 months. RAs moved towards their respective directions until the sample size for the village was reached. Interviews were held with either mothers or female caretakers of the child (or children) alone or sometimes in the presence of their spouses.
4.3.3 Sampling of the HSAs A total of 121 HSAs were interviewed from the four districts (61 in Salima and 20 in each of the other 3 districts namely Nkhotakota, Ntchisi and Dowa). In Salima, the HSAs were randomly sampled from 14 Health Centres (including the 9 HCs where the household interviews were conducted). In the other Districts, the HSAs were sampled from 4 to 5 randomly sampled HCs.
4.4 Presentation of the findings
Findings from the field survey are presented in three different chapters. Findings from interviews with Key informants are discussed in chapter 5 while findings from interviews with HSAs and mother/child caretakers are discussed in chapters 6 and 7 respectively. Each is beginning with a summary of findings which are followed by a detailed discussion of the findings. Overall conclusions and recommendations are presented in chapter 8.
6 Golomoti, Mtakataka and Mua are in Dedza District but for administration purposes of the Ministry of Health, they report to Salima DHO.

17
5.0 FINDINGS FROM KEY INFORMANT INTERVIEWS This chapter presents findings from discussions with the Acting Chief Environmental Officer (based at the Ministry of Health headquarters), DEHOs and other supervisors of HSAs from the four districts that were included in the survey. The findings will be discussed under five sub-headings namely: Job description of the HSA, type of supervision provided, technical and social constraints affecting the work of the HSAs, factors affecting immunisation coverage and suggestions for improving the work of the HSAs. In total, 14 interviews were conducted across the four districts.
5.1 Summary of findings
The general picture that came out of the various KIIs is that HSAs are very crucial to achieving healthy communities in Malawi. They are the only health staff that work at the grassroots level in implementing health related activities on behalf of both the Government and the NGO sector. Because of the widened scope of operations at community level, HSAs are overloaded. The current workload of HSAs includes immunizations (up to 90% of all child immunizations), village and business premises inspection, water source protection and water chlorination, family planning, sanitation, running the drug revolving fund and the Bakili Muluzi health initiative, forming and supervising VHCs, supervising Traditional Birth Attendants (TBAs) and implementing health programes for some NGOs. Frequently, HSAs are not oriented when new interventions are being introduced. Furthermore, HSAs basic courses have become haphazard and irregular and many HSAs remain untrained. Currently very few HSAs have attended a refresher course. The major strengths that exist among HSAs include team spirit and cooperation, knowledge of local culture, language and the environment, timeliness and perseverance in harsh conditions and during times of delayed payments. Their weaknesses include incidences of overindulgence in alcohol, the fact that many of them stay very far from their catchment areas, limited knowledge of report writing and limited skills especially in immunization and disease investigation. Externally the major constraint that was mentioned across the board was the lack of vision and peripheral support for preventive health services in Malawi. Over the years there has been reduced support towards preventive services and even at the District Health Office (DHO) level, there is limited support for preventive services. Furthermore, HSA work has limited opportunities and there are basically very minute chances of upward mobility. Moreover, salaries are very low and they do not take into consideration of ones’ qualification. In addition, refresher courses and transport remain unavailable and HSAs reside in poor looking houses and are inadequately supplied with drugs for common diseases and water treatment chemicals. Arising out of the KII is the recommendation that in order to improve the work of HSAs in Malawi, a review of the HSA position should be undertaken with the aim of making it more attractive and responsive to academic qualifications and one’s achievements. It is also recommended that the budgetary allocation to the preventive health sector in the MoHP should be increased and that current vision and strategies in the Ministry be re-oriented. It is further recommended that extra HSAs be recruited in order to reduce the workload of each HSA. Moreover, transport should be improved and drugs should be supplied regularly. Lastily, the MoHP should explore possibilities of inter-country visits for field HSAs so that they could learn and exchange lessons across countries.

18
Factors contributing to low immunization coverage in Malawi could include lack of transport for carrying vaccines, unavailability of some vaccines, geographical inaccessibility of some areas especially during rainy season, the HSAs workload, high dropout rates because of side-effects of some vaccines and inactive VHCs. Other factors could include wrong scheduling of immunization sessions (morning hours only when mothers are busy with other activities), non-functioning of refrigerators and the lack of paraffin at some health centers. The following sections carry detailed findings from the KIIs starting with the activities relative to their job description, that the HSAs were reportedly implementing in the areas where the survey was carried out.
5.2 Job Description of the HSA
Appendix 2 is an official job description of an HSA as stipulated in the Human Resources Development Plan of the Environmental Health section of the Ministry of Health (GoM 1997). However, discussions with the various HSA Supervisors revealed that HSAs are also involved in other activities, government-driven or not (usually with a health orientation) outside their job description. According to the informants, the HSAs are, therefore, overloaded. They have a lot of tasks to implement, some of them very new to the HSAs and therefore they do not have time to concentrate on a particular task or a group of tasks. The ‘overload’ was mentioned by the informants as one of the many factors that might have affected immunization services in their respective areas because they assign only 1-2 days in a month for immunization, the rest being for other activities.
5.3 Tasks being carried by HSAs
Informants were asked to cite the various tasks which were being implemented by HSAs under their jurisdiction. Box 1 below gives a list of the activities that were cited. In reality, it would seem that the activities that HSAs are actually doing on the ground exceed those contained in their job description. Basically this is because new activities are continuously being introduced, which have to be implemented at community level. HSAs provide the only human resource link at that level. Furthermore to this, several NGOs and other government projects in the health sector also utilize the HSAs to implement their activities (taking advantage of the existing human resource structure). With the exception of the DRF and the BMHI, all other activities exist in all the areas (although some pockets in some areas are being missed out). Usually, where the DRF is in operation, the BMHI was reported not to exist because the two use different approaches, in that the DRF has some elements of cost-sharing while the BMHI is free.

19
Box 1: Activities being implemented by HSAs in the 12 sampled HCs as reported by their supervisors (October-November 2001)
Immunization Growth monitoring Health and HIV/AIDS talks Village inspection Business premises inspection Sanitation Formation of Village Health Committees & AIDS Toto clubs Supervising VHCs and health volunteers Aids counseling Follow-up of TB patients Water source protection and water chlorination Disease surveillance Family planning Implementing the BMHI and/or DRF Supervising TBAs Referring malnourished children for rehabilitation Detecting and reporting disease outbreaks
5.3.1 Immunization, growth monitoring and health talks The policy of the EPI, which was launched in Malawi in 1979, is to immunize all children under the age of 12 months. The goal of the programme is to reduce morbidity and mortality rates due to the six infectious but preventable diseases namely tuberculosis, poliomyelitis, pertussis, tetanus, diphtheria and measles. Immunizations are also given to pregnant mothers and all females in the reproductive age bracket (15-49 years of age) in order to protect the unborn babies against neonatal tetanus and the mother against tetanus. HSAs are the major providers of the immunizations particularly for children. Estimations provided by the various informants suggest that HSAs are responsible for over 90% of vaccination that are provided to underfive children in rural Malawi, the rest being provided at the HCs and in other private clinics including Banja La Mtsogolo (BLM). Each HSA runs 1-3 outreach clinics in a month in his/her catchment area during which immunizations are conducted. Vaccines are brought to the outreach clinics (by HSA supervisors) on the day of the immunizations from the respective HCs because HSAs do not have the equipment to maintain the cold chain. Talks on health problems affecting the community usually precede growth monitoring and immunization activities. In some communities, local health volunteers assist HSAs with the weighing of children and the recording of the on the health cards. However, the informants also indicated that most VHCs are not adequately functioning as some of the volunteers got demoralized due to financial expectations which never materialised.

20
5.3.2 Village and Business premises inspection HSAs inspect villages to determine people’s accessibility to sanitary facilities (excreta and solid waste disposal) and to survey the risk behaviour of the people in terms of their health. Based on the findings from such inspectorate visits, HSAs plan for health and advisory talks for the communities, which are sometimes conducted at organized village gatherings or at household level. HSAs also teach and demonstrate to the community on the construction and usage of san plats, usually in collaboration with some NGOs. Moreover, HSAs also inspect business premises for observance of sanitary practices but have no powers to close down any business that disregards or does not satisfy sanitary regulations. The informants also indicated that remarkable achievement has been made in the various communities in terms of accessing sanitary facilities because of the HSAs. For example, HSAs in Salima (Thavite HC) were reported to have motivated communities to construct and access sanitary facilities. According to the informant at the HC, access rates for pit latrines and bath shelters in 2000 were 30% and 35% respectively. At the time of the study, the rates had gone up to 44% and 58% respectively.
5.3.3 TB work During the village and household inspectorate visits, HSAs also identify suspected TB patients and advise them to visit HCs for examination. In addition, they
o collect sputum from the suspects for examination at HCs. o provide follow-up visits to TB patients who have been discharged from hospital but who
are continuing their treatment at home, to ensure that they are following the advice from the hospital
o follow up on TB treatment defaulters o collect TB drugs at the HCs on behalf of patients in their catchment areas
5.3.4 Water source protection and chlorination In communities that have a communal water source, for example a tank, HSAs are responsible for the protection of that source in liaison with local field staff from the Ministry of Water Development. At other times, the HSAs work hand-in-hand with communities, sometimes using the village health and water committees (VHWCs), to identify community sections that urgently need boreholes and they communicate this information to the responsible offices including the respective Members of Parliament. Furthermore, HSAs also:
o teach communities on borehole and well protection; o treat borehole and wells with Chloride of Lime; and, o in other communities which have no boreholes and tap water, they train VHWCs in
preparing chlorine solutions and the treatment of water in the homes (if the water isnot treated at source).
Main problems that were reported to be hampering HSAs efforts on water treatment included irregular supply of chlorine and, for some, lack of the basic knowledge of water treatment.

21
5.3.5 Family planning On family planning (FP), HSAs work as motivators and distributors of FP methods in the communities. According to the informants, HSAs distribute condoms (as a contraceptive) and pills to the communities. In some communities, there are community-based distributors who are supervised by HSAs. In isolated cases HSAs were also reported giving birth control injections (Depo provera) to some local women, usually on the recommendation from the HCs to which they report. During growth monitoring and other village health talks, HSAs also teach communities about fertility issues and their relevance in terms of the safety and health of mothers and their children.
5.3.6 Treatment of minor illnesses and Vector control Ideally, HSAs are supposed to have access to drugs for minor illnesses, which are to be given out to community members once they approached the HSA. According to the respondents, some HSAs were not doing this activity basically because of problems with drug supply. As such, people in their communities have since stopped approaching them when ill because they (usually) have been turned away without any assistance. In vector control, mosquitoes and snails are the main target. Ideally, HSAs are supposed to be provided with the necessary chemicals for use in vector control. In the event that chemicals are not provided, HSAs only provide talks to the communities on environmental sanitation. It was also mentioned that some NGOs are using the HSAs to sell their products to the people on a commercial basis e.g. mosquito nets
5.3.7 Implementing the DRF and the BMHI The Bamako Initiative of 1987 by the Ministers of Health of WHO African region called for community financing of health services after noting that African national budgets were failing to support PHC activities. They recommended the setting up of village-based DRFs so that communities that are very far from health facilities have a continuous supply of low-priced drugs for common ailments, particularly malaria. Ideally, DRFs are run by a community based health promoter or VHC members who receive a 1-2 week basic training in drug administration. HSAs are advisors and supervisors of the health promoter or VHC regarding the management of DRFs. The BMHI is a more recently refined and detracted strategic component of the PHC, whereby drugs are disbursed at no cost to communities that are very far from health facilities. Ideally the BMHI operates in places where DRFs are not operating as it targets those communities that cannot sustain the DRF because of their poverty. As with the DRFs, the BMHIs are run by the community and HSAs are supposed to act as advisors only. However, according to the informants, HSAs are also involved in the actual drug disbursement under both schemes, a situation that creates conflict between HSAs and communities especially if the two schemes are being implemented in nearby communities.
5.3.8 Supervising VHWCs and TBAs

22
Most villages in Malawi have village health and water committees (which are supervised by HSAs) whose functions are disease surveillance and detection of outbreaks, health talks, community sensitization and organization, growth monitoring and protection of water sources. Traditional birth attendants (TBAs) are ideally supposed to be supervised by community health nurses because of the nature of their jobs. However, because there are very few CHNs or none at all in most HCs, HSAs take on the job of supervising the TBAs.
5.3.9 Working with NGOs Formal health services in Malawi are provided by quite a big array of players including the government, religious institutions, NGOs, big companies and the private sector. Informal service providers include traditional healers, local injectors, TBAs, local shops and vendors. The Ministry of Health and Population is the only formal service provider that has an extensive network that adequately infiltrates into the rural and remote areas using the HSAs. It is because of this, that most NGOs with health-related purposes utilize HSAs to implement their activities because most of them usually have few staff for that purpose. These NGOs are actively supporting and implementing immunizations, growth monitoring, water and sanitation, food security and nutrition activities. All these activities fall within the job mandate of an HSA. In return, HSAs benefit from these NGOs in the form of short training courses, duty and training allowances and access to new information. In the 12 HCs where HSA supervisors were interviewed, the following NGOs were identified: Save the Children Fund (UK), Salima Aids Support Organisation (SASO), Action-Aid, Sight Savers and World Vision International (WVI). Save the Children Fund UK was identified in 7 of the 12 HCs and was promoting and supporting sanitary activities by providing materials for dome slab and san plats construction and rehabilitation. HSAs were involved in the identification of beneficiary villages and supervision of the communities in the construction works. Action Aid was identified in one HC and was supporting and implementing water and sanitation activities, HIV/AIDS awareness and prevention (called Stepping Stones) and had made a donation of beds and mattresses to the health centre and the installation of electricity. This NGO also donated bicycles to the HSAs. Sight Savers was also identified in one HC and was assisting those people who have trachoma.
5.4 How are HSAs supervised?
HSAs are directly supervised by Health Assistants (HAs) and in their absence, by Senior Health Surveillance Assistants (SHSAs). Each HSA prepares a monthly work plan which indicates the work that s/he will do in that particular month including dates for outreach/mobile clinics. Based on the plans of several HSAs, the supervisors prepare their own plans for monitoring and supervision. The ‘ideal’ situation is that the supervisors are expected to sporadically (and sometimes regularly) visit the HSAs in their catchment areas to see what they are doing and to learn about their problems directly and talking to some local people about their experiences with the HSAs. However, because of transport problems, the reverse happens. Most HSAs go to their supervisors to submit activity reports and are visited on immunisation dates because there is usually a vehicle or motorbike available on that day to carry vaccines to outreach clinics. None of the HA’s and SHSA’s who were interviewed indicated that s/he had a checklist that would be used when supervising the HSAs. The HA’s and SHSA’s report to and are supervised by the

23
DEHOs. DEHO’s usually do not interact directly with HSAs except for those who report to the district hospital.
5.5 Technical and Social Constraints affecting the work of HSA’s
A range of technical and social constraints were cited by the various informants regarding the work of HSAs in their areas (Box 2).
Box 2: Technical and social constraints facing HSAs as cited by supervisors
Limited opportunities Low salary and other financial rewards Lack of/inadequate transport Lack of immunisation skills (BCG & DPT) Limited supervision Limited training Lack of equipment and stationery Poor accommodation Resistance from local leaders No drugs for common illnesses
5.5.1 Limited opportunities The various informants raised three related but important issues on this topic. Firstly, all HSAs, regardless of their school qualifications and whether one has undergone an induction course or not, are recruited at SC II, a position that is equivalent to a watchman or a messenger in the civil service. This, according to the informants, is demotivating to some HSAs especially those with MSCE certificates because their counterparts who are recruited in other administrative positions join the civil service at CO grade and have more other opportunities than HSAs. For example, HSAs are not considered when reviewing conditions of service for professional staff in the MoHP. Annual leave days for HSAs are also similar to those for ground staff i.e. 21 days which, according to the informants, are not adequate for the HSAs to rest adequately. Secondly, starting salaries for MSCE and JCE certificate holders is uniform regardless of one’s qualification and whether one has attended an induction course or not. Related to this, salaries for Senior HSAs who are supervisors of fellow HSAs are not adjusted to reflect the promotion. One SHSA in Salima said:
“what has changed to me is the title from HSA to SHSA and my job description to that of supervisor …… my salary is the same ….I thought this time I would be promoted to TA grade”
Thirdly, the informants indicated that the HSA system is so closed that there are virtually no opportunties (blackout) for further training which would promote upward mobility in the professional development of HSAs. Promotions are scanty and almost based on a lottery system.
“… Once recruited as an HSA, you will be an HSA forever …. There is a complete blackout of chances of being trained and later promoted” - SHSA, Salima

24
5.5.2 Low salary and other financial rewards HSA wages are very low. Housing and duty allowances (usually not more than K1000 per month) are also very low. They are not provided with lunch and transport allowances (or opportunities to claim T&T for using their bicycles) when they work in distant places. The informants also said that HSAs are not paid risk allowances despite the nature of their job i.e. collecting sputum specimens and other samples and transporting them from the villages to health centres for analysis. For example, Kaphatenga HC had treated 119 cholera cases in 1999 which resulted in 1 death, 256 cases in 2000 (2 deaths) and 115 cases of scabies in 2001 all of which were identified and handled by HSAs.
5.5.3 Lack of/inadequate transport HSAs and SHSAs cover wide catchment areas, on average 5-10km for HSAs and 10-20Km for SHSAs. Transport in the form of motorbikes for SHSAs and bicycles (push bikes) for HSAs or transport allowances are not provided. This was reported to be common especially among the newly recruited HSAs
“we use borrowed bicycles” - SHSA, Ntchisi Some areas are therefore not visited by the HSAs. Some informants indicated that pushbikes which were given out to some HSAs, were all damaged because they were misused by the HSAs as they were taken to be the property of the government. Spare parts are not been provided by the MoH and are beyond the affordability of HSA wages.
5.5.4 Low immunisation skills SHSAs cited a general lack of vaccination skills among HSAs (both trained and untrained HSAs) particularly in relation to the administration of BCG and DPT vaccines. This, according to the informants causes some mothers to stop bringing their children for immunizations because of abscesses and other side effects that result thereafter.
5.5.6 Limited training Figure 1 shows the numbers of both trained and untrained HSAs in 8 of the 12 health centers where discussions were heard with HSA supervisors. Four HCs did not provide the breakdown as the informants were not very sure of the actual situation. Untrained HSAs were present in all the 8 HCs. According to the informants, these untrained HSAs are supposed to be given ‘on the job training’ by their fellow HSAs and are expected to work for some period before attending a formal induction course.
Figure 1:Number of HSAs (trained and untrained in 8 HCs that were visited in Salima, Nkhotakota, Ntchisi and Dowa Districtcs (October-November 2001)

25
10
3
11
3
8
2
10
4
5
2
12
5
9
2
12
4
0
2
4
6
8
10
12
Number
Thavite
Mcoka
Mwansam
bo
Msenjere
Kamson
ga
Chakhaz
aKhuw
i
Kaphate
nga
Health Centre
Figure : Number of HSAs (Trained and untrained) in 8 Health Centres that were visited (November 2001)
TotalTrainedUntrained
The informants also stated that training is usually not provided to the HSAs when a new intervention is being introduced, as such, HSAs implement such functions on a ‘trial and error’ basis, a situation that is dangerous considering that HSAs work directly with people and they have a great influence in people’s health decisions.
5.5.7 Poor accommodation The informants indicated that most HSAs have no government houses. They live in rented houses, which are of substandard quality. Some HSAs live very far from their catchment areas (at trading centres) because there are no houses to rent in the catchment area.
5.6 Factors affecting immunisation coverage
Two extreme viewpoints were captured on this topic. Some informants (3 SHSAs, 1 DEHO and 1 MCH Coordinator) refuted and labeled it as an allegation that immunisation coverage rates are declining as reported in the DHS report of 2000. They advanced two arguments. Firstly, immunisation data in most health centres is not properly collected and collated and therefore not reliable. Related to this, the 2000 DHS data collection exercise was also characterized by a lot of errors and the denominators that were used could have been misleading. The second argument raised by the opponents was more mathematical. They contended that children are immunised against the 6 killer diseases, which have been wiped out and no cases have been reported in recent times. This, according to the opponents was an indicator that more children are being immunised hence, they did not subscribe to the fact that immunisation coverage rates were declining.

26
Those who agreed that immunisation coverage has been declining cited several factors that could be contributing to this decline, at least in their catchment areas. These factors are summarized as follows:
No transport (no vehicles or no fuel) to carry vaccines from HCs to mobile clinics, and no bicycles for HSAs);
Non-functioning of refrigerators in most HCs and scarcity of spare parts; Broken needles and syringes; Unavailability of some vaccines (e.g. BCG and Polio) over long periods of time in some HCs
and even at national level; High dropouts mainly because of side effects of vaccines, particularly DPT; Geographical inaccessibility of some areas especially during the rainy season; Lack of cooperation at HCs i.e. Immunisation services are left for public health staff only.
Nurses and other health staff refuse to assist; ‘Missed opportunities’ i.e. children who are not immunised and have come to HCs for other
treatment are let to go home without taking advantage of this opportunity; Religious beliefs preventing vaccination especially among the Zionists; Cancellation of outreach clinics mainly due to vehicle breakdowns, fuel problems and
shortage of vaccines. This was reported to demoralize mothers even if they were interested. (For example, in Dowa, parents were reported as having gone to HCs to inquire why an outreach clinic was cancelled);
Most growth monitoring volunteers who were there 5-10 years ago stopped assisting once their training was suspended in 1995;
Inactive village health and water committees; Local people confuse immunizations as a family planning strategy; Bad attitude of staff at HCs; Busy schedules for mothers especially during the rainy season. Mobile clinics are usually
conducted in the morning when the mothers are busy in the fields; and, Non-participation of men/fathers.
5.7 Strengths and weaknesses of HSAs
The informants were also asked to explain the weaknesses and strengths among their HSAs. Strengths that were reported included:
o Team spirit and cooperation; o Knowledge of local culture, language and the environment because HSAs usually work in
their home environment; o Timely completion of tasks and submission of reports; and, o Perseverance, considering the type of work they are doing vis-à-vis their remuneration
and other social rewards. Weaknesses that were reported to be common among some HSAs included:
o Over indulgence in alcohol and general negligence of duty; o Disrespect for SHSAs; o HSAs residing very far from their catchment areas; and, o Low report writing skills.
5.8 Suggestions for improving the work of the HSA

27
Based on their experiences in working with HSAs or as HSAs, the key informants were asked to suggest ways of improving both the work of HSAs in the delivery of health services and the general welfare of HSAs. Box 3 gives the various suggestions that were put forward.
Box 3 : Suggestions for improving the work of HSAs as put forward by supervisors
Provide opportunities for upgrading courses and promotions Review HSA grade in the civil service to respond to one’s
academic qualifications and length of service Provide pushbikes to HSAs and motor cycles to senior HSAs on
an ownership scheme to enhance proper care Consider paying T&T to HSAs for using their personal pushbikes Improve salaries for HSAs and introduce a different
remuneration level for SHSAs Provide uniform and other protective clothing especially during
the rainy season Promote inter-country visits for HSAs Provide longer and more practical induction and refresher
courses Provide recognized certificates after completion of the induction
course Reduce the HSA : Population ratio to less than 1:2000
Ensure that medical staff should accompany HSAs during outreach clinics
Encourage regular information flow Provide regular supply of fuel and stationery
5.9 How else could HSAs be utilized?
The informants indicated that although HSAs are overloaded with tasks, they could also be used in meat inspection if properly trained. A lot of livestock are slaughtered in the villages, which are then sold to consumers without being inspected because there are no Veterinary Assistants in their areas. HSAs could intervene in the system to ensure that the meat being sold from the slaughtered animals is suitable for human consumption.

28
6.0 FINDINGS FROM INTERVIEWS WITH HSAs A total of 121 HSAs from 30 health centers in 4 districts namely Salima (61), Nkhotakota (20), Dowa (20) an Ntchisi (20) were interviewed to get their views and perceptions regarding their own work.
6.1 Summary of findings
Of the 121 HSAs who were interviewed, 65% possessed the Malawi Schools Certificate of Education (MSCE) while 3.3% had a primary school leaving certificate. Overall, 19% of the HSAs were not formally trained in HSA work. However, the proportion of untrained HSAs was higher among MSCE holders compared to the holders of the Junior Certificate (JC). On average, the sampled HSAs lived about 5km from their health centres although others lived more than 20km away. Accommodation for most of the sampled HSAs was very poor and pathetic, many reside very far from shopping centres and markets, bus stations and telecommunication facilities. The average population being served by the sampled HSAs was 2364 people but about 35% of them were serving more than 2500 people (maximum of 9500 for one HSA in Salima district). Average distance to furthest village in their catchment areas for the sampled HSAs was 6km with a maximum of 17km. About 83% of the sampled HSAs said that they had received terms of reference for their position at the time of recruitment while the rest had not. The rate of non-receivers was higher among the untrained HSAs (56.5%) compared to the trained HSAs (8.2%). The findings also revealed that the tasks that are being implemented by most of the sampled HSAs include immunisation, growth monitoring, village inspection, assisting VHWCs, water protection and treatment, sanitation and nutrition and health talks. In terms of time allocation, immunisation, growth monitoring and health talks occupy over 40% of the HSA’s total time followed by sanitation and water protection activities (25%). Treatment of minor illnesses is not being carried out by most HSAs because of problems with drug supply. Village talks about HIV/AIDS and family planning do take place. Condoms, pills and injection (Depo provera) were the three FP methods being provided by HSAs. Apart from working in the villages, some HSAs provided assistance at their health centres such as manning the dispensary and dressing room, cleaning hospital utensils, sterilizing needles and messengerial work. Most of the sampled HSAs (>30%) prefer involvement in health talks and immunisation compared to TB work and HIV/AIDS talks. Most of the HSAs also reported having more skills in health talks, immunisation and sanitation compared with other tasks such as TBA supervision. Tasks in which most HSAs reported to lack skills included disease investigation, family planning, water treatment and giving immunisation particularly, BCG and DPT. The sampled HSAs were being consulted often by their local communities for assistance with water treatment, treatment of minor illnesses, family planning and transport for patients/dead bodies and gloves for cleaning dead bodies. Access factors account for 54% of the reasons why some people had never consulted the sampled HSAs compared to service quality (21%), relevance (19%) and problems with scheduling (6%). Being community based and residing in the villages, HSAs also have other social obligations and roles to play such as membership to local committees for example funeral and church groups and cash credit groups. Apart from implementing government work, HSAs provide the channel for delivering services supplied by most NGOs in the health sector. Although their monthly salaries varied with length of service, the data revealed that the salaries were not responsive to one’s level of education attainment. Technical constraints cited by most of the HSAs included lack of transport (69%), lack of storage and carrying equipment for vaccines (65%), lack of protective clothing (65%) limited supervision (25%) and irregular supply

29
of vaccines and drugs (60%). At the time of the survey, only 5 of the 121 HSAs had antimalarial drugs and 4 had antibiotics, 4 had pain relievers. Similarly, condoms were available to just 41 HSAs, child weighing scales to 59 HSAs and ORS sachets to 33 HSAs. Social constraints included low remuneration and limited opportunities, lack of refresher courses, poor roads, poor telecommunication, cultural values of the community and poor relations with supervisors. Details pertaining to the various issues summarised above are discussed in the subsections below.
6.2 Background characteristics of the sampled HSAs
Table 2 provides a summary of the background characteristics of the sampled HSAs. Of the 121 HSAs who were included in the survey, 72 (59.5%) were male while 40.5% (49) were female.
Table 2: Background characteristics of the sampled HSAs
Sex of HSA Characteristic Males % (n=72) Females % (n=49)
Total %
Education level
Standard 8 Form 2 Form 4
2.8 38.9 58.3
4.1 22.4 73.5
3.3 32.3 64.5
Marital status Married
Single (never married) Widowed
Divorced/separated
86.1 9.7 1.4 2.8
67.3 26.5
0 6.1
78.5 16.5 0.8 4.1
Religion Christianity
Islam Watch Tower/Zion/Apostle
Traditional
84.7 12.5 1.4 1.4
98.0 2.0 0 0
90.1 8.3 0.8 0.8
Received HAS basic training? Yes No
86.1 13.9
73.5 26.5
81.0 19.0
6.2.1 Education The minimum academic qualification among the sampled HSAs was the Malawi Primary Schools Leaving Certificate (PSLC) while the maximum was the Malawi Schools Certificate of Education (MSCE). Sixty-five percent of the sampled HSAs possessed the MSCE, 73.5% for females and 58.3% for males. In comparison, there were proportionately more male HSAs holding JCE certificates (34.7%) compared to females (22.4%), a situation that was reversed among MSCE holders. The high proportion of MSCE holders among female HSAs than males could be a result of the gender differences in employment opportunities in Malawi. It may be that the other high paying

30
jobs are not available easily to women, a situation that might have forced most female MSCE holders to join the HSA scheme in desperation.
6.2.2 Age and Marital status About 79% of the sampled HSAs were married, 17% were single (never married before) while the rest were either divorced or separated. One of the male HSAs in the sample was widowed. The age range of the sampled HSAs was 38 years, a minimum of 20 years, maximum of 58 years and a mean of 29.6 years. Only one HSA in the sample was over the mandatory age for retirement in the civil service of 55 years while about 91% of the 121 HSAs were below the age of 40 years.
6.2.3 Religion Religious denominations were classified into four categories in a deliberate attempt to explore whether followers of some religious affiliations do not work as health workers. The findings indicate that religious affiliation does not necessarily prevent some one from taking up the HSA work although the numbers of HSAs belonging to some religions in the sample was dismal. This may just reflect their being relatively few and sparsely located in the sampled districts, and perhaps the country as a whole. Christians formed about 91% of the sample while Moslems were about 8%. One of the 121 HSAs was neither a Christian nor a Moslem, but belonged to a traditional cult known as Gule Wamkulu also called ‘Mpingo wa Aaroni’.
6.2.4 Proportion of HSAs trained in HSA work According to the Human Resource Development Policy of the MoHP, about 300 new HSAs are supposed to be recruited and trained every year before being deployed to serve in various parts of the country. The training, which is 8 weeks long, covers a wide range of issues particularly those contained in the terms of reference for HSAs including work ethics. Basically, the training is conducted to ensure that the quality of services being delivered to the rural masses by the HSAs is of high standard and promotes healthy living among most Malawians. Eighty-one percent of the sampled HSAs indicated that they had attended the HSA induction course while 19% had not attended. When cross tabulations of their academic qualifications and whether one had attended the induction course (or not) were completed, it was found that all the PSLCE certificate holders in the sample had attended the HSA induction course. On the other hand, about 11% of the JC holders and 24% of the MSCE certificate holders had not attended the course (Table 3). Although the proportion of untrained HSAs seemed to be higher among MSCE certificate holders compared to those possessing JCE certificates, the differences in the proportions were not statistically significant at p=0.05 level, suggesting that being trained does not depend on whether a candidate holds a MSCE or JCE certificate but is subject to chance. Is therefore possible that the same observation could be true for PSLCE certificate holders.
Table 3: Training status of the sampled HSAs (October-November 2001)
Academic qualification
Trained (%)
Not trained (%)
Total (n)
Standard 8
Form 2 Form 4
100 88.9 75.6
0
11.1 24.4
4 39 78

31
Total
81%
19%
121
6.2.5 Length of service as HSA Appendix 3 provides a summary of descriptive statistics for various variables. The minimum length of service as an HSA among the sampled HSAs was a quarter of a year (3 months), maximum was 21 years and the mean was about 6 years. About 22 percent of the sampled HSAs had been in service for not more than one year. The average length of service in the catchment areas where the survey team met the sampled HSAs was about 3 years.
6.2.6 Distance to health centers or hospitals Distances to the HCs have implications on reporting frequency, supervision and availability of materials as usually those staying very far are disadvantaged. In this survey, HSAs were asked to estimate distances to the HCs or hospitals to which they report and the time that elapses when walking or cycling. The average distance to HCs was found to be about 5 km, a minimum of 0.05 km and a maximum of 30 km. Further analysis of the data showed no significant differences in the mean, minimum and maximum distances in the four districts under study. About 68% of the sampled HSAs lived not more than 5 km from their HCs while about 13% lived more than 10 km from their HCs.
6.2.7 Size of catchment area and population The average number of villages per HSA was found to be about 7 to 8 villages with an average population of 2364 people (Appendix 3). These fall within the recommended coverage scales of the MoHP of about 10 villages and about 2000-2500 people per HSA. However, about 36% of the HSAs served more than the recommended maximum population of 2500. The maximum population for one HSA in Salima district was 9500 people. In Nkhotakota, Dowa and Ntchisi districts, the maximum population for an HSA were 5000, 4000 and 6000 people respectively. The findings further show that distances from the HC did not vary with the size of the population being served by an HSA as those HSAs serving the highest populations in the four districts lived not very far from the HCs, 7km in Salima, 8km in Dowa and less than 1km in Nkhotakota and Ntchisi respectively. This finding seems to suggest that population size may not have been the key criteria that was used to assign HSAs to the various catchments. Other criteria like topographical features might have been used as well. The HSAs were also asked to estimate distances to the furthest villages in their catchments and the time it takes to walk or cycle to those villages7. The average distance to the furthest village was about 6km, a minimum of 0.5km and maximum of 17km respectively. On average, the HSAs indicated that it takes them about 2 hours to walk to the furthest villages and about a quarter of an hour to cycle there (Appendix 3). On the usual mode of mobility (travel) by when working, about 55% indicated that they use pushbikes while about 44% walk to their respective duty points. Only one HSA used a motor cycle when working.
7 This is linked to the mobility of residents of those villages in terms of consulting the HSAs when a need arises.

32
According to the sampled HSAs, almost all villages in their catchments are visited at least once a month. The average number of visits per village was two with a minimum of one visit and a maximum of 15 visits per village per month. When the HSAs are grouped according to number of villages covered, the data does not seem to suggest that HSAs covering fewer villages make more visits per village. This might indicate that a visit to a village does not necessarily last for a full day and may depend upon one’s planning system to cover all the households in a catchment including those small pockets found in the peripherals.
5.3.8 Working with health and water committees The HSAs were asked to state the number of health and water committees which they had established in their catchments, and the total committees with which they are working. About 22.3% said they had never established any committee while the rest indicated that they had established some committees. The numbers of the newly established committees ranged form1 to 22 with an average of 3 VHWCs per HSA. All the HSAs indicated that the various VHWCs were assisting them with activities related to sanitation, disease surveillance, growth monitoring, water source protection and water treatment and village and business premises inspection.
6.3 Tasks being conducted by the sampled HSAs
The sampled HSAs were asked if they had received terms of reference at the time they started as HSAs. Those who acceded, they were further asked to state the types of tasks that were prescribed therein. Finally, the HSAs were also asked to state what types of tasks they were implementing in their catchment areas.
6.3.1 Knowledge and reception of Terms of Reference ToRs are used to describe the contractual obligations, duties and responsibilities and expectations of interested parties in an activity so that all those concerned enter into an agreement and sign for it with a common understanding. In this particular case, those individuals who are interested to work as HSAs are (upon being recruited as HSAs) supposed to be served with the ToRs. These ToRs allow them to know exactly what is expected of them and what they should expect in return from the employer (MoHP) in terms of both technical and logistical support, as well as remuneration. In the survey HSAs were asked whether they were served with TORs when they were taking the HSA job and what types of tasks were prescribed therein. About 83% of the HSAs acceded that they received the ToRs while about 17% said they did not. When cross-tabulated against HSA training background, the proportion of those HSAs that were not served with TORs is significantly higher among those HSAs who had never gone through the induction course (56.5%) compared to their counterparts (8.2%). This finding is somewhat worrying because it might indicate some disorganization in the whole process of recruitment and induction (or it may be pointing out problems with the HSAs themselves). Ideally, the HSA induction course revolves around their TORs. The expectation was that all the HSAs that had gone through the course, knew their TORs A list of tasks was tabulated in the HSA questionnaire and Research Assistants were instructed to tick against all those tasks which the HSAs recited on their own without prompting. When they

33
had finished recalling what was contained in the original TORs, the RA’s then probed for the other tasks in the table that were not mentioned by the respondents. The aim of this process was to firstly assess if the HSAs still remembered their TORs and secondly to develop a simple indicator of tasks that are frequently carried out and preferred by HSAs. Table 4 below gives a summary of tasks which the HSAs conceded to have been contained in their ToRs.
Table 4: Tasks contained in ToRs served to HSAs
Tasks Task was contained in the ToRs (%)
Proportion of HSAs who listed the task after promted (%)
Immunizations 99.2 13.2 Water protection and treatment 99.2 33.9 Village inspection 98.3 16.5 Nutrition and health talks 98.3 31.4 Sanitation 98.3 44.6 Growth monitoring 97.5 19.8 Formation and assisting water and health committees 95.9 52.1 Nutritional supplementation 73.6 84.3 Treatment of minor ailments 56.2 79.3 Family planning 50.4 81.8 Running a drug revolving fund (DRF) 21.5 93.4 Prescribing drugs at HC 2.5 95.0 The data presented in the table above suggests that immunizations, growth monitoring, village inspections, working with VHCs, sanitation, water protection, nutrition and health talks were according to most of the sampled HSAs the common activities contained in the ToRs they joined the HSA work. Family planning, running the DRF and prescribing drugs at a HC were rarely mentioned by the sampled HSAs. When cross-tabulated against length of service, the data revealed that these functions were mostly reported by HSAs with less than 6 years of service (78%). As indicated earlier, there is a standard job description for an HSA to which new activities are continuously being added (over time) as new developments in the health sector are introduced. The fact that mostly those with less than six years experience reported these activities as being part of their ToRs could reflect this trend.
6.4 Tasks enjoyed most by HSAs
The HSAs were asked to select one task they enjoy performing above all others. Immunisation and health talks topped the list of tasks that are liked most, followed at some distance by sanitation activities (Table 5). Perhaps immunizations and health talks were both rated highly because the two are usually conducted concurrently. Most HSAs indicated that almost 40% of their time is dedicated to immunisation and growth monitoring. The number of days that are usually time-tabled for immunisation and growth monitoring by the HSAs ranged from 1 to 22 per month (Appendix 3). Working with or following-up on TB patients and HIV/AIDS talks scored the lowest followed by family planning, water treatment and disease investigation in that order. The low score for TB work is not very surprising because there are a lot of risks involved, particularly when collecting sputum specimen for examination. Most HSAs complained that they are not provided with protective clothing including gloves for this work. The low scores on HIV/AIDS and family planning issues could possibly be due to ethical and socio-cultural complexities as few people are comfortable to discuss such issues.

34
Table 5: HAS Task preferences and level of skills (October-November 2001
Task enjoyed most by HSAs
%
Task with a lot of skills according to HSAs
%
Task lacking skills according to HSAs
%
Health talks 36.4 Immunizations 33.9 Disease investigation 16.7 Immunizations 34.7 Health talks 28.9 Family planning 14.2 Sanitation 14.9 Sanitation 14.0 Health talks 10.8 Growth monitoring 4.1 Water treatment 6.6 Water treatment 10.8 Disease investigation 2.5 Disease investigation 5.8 Immunisation 9.2 Supervising VHCs 2.5 Family planning 5.0 TB work 8.3 Water treatment 1.7 Growth monitoring 2.5 Sanitation 8.3 Family planning 1.7 Supervising VHCs 1.7 Vector control 7.5 HIV/AIDS talks 0.8 TBA supervision 0.8 HIV/AIDS talks 6.7 TB work 0.8 None 0.8 Supervision of TBA/VHCs 4.1 Working at HC 1.7 Nutrition 1.6 Growth monitoring 0.8
6.5 Tasks where HSAs lacked skills
The HSAs were asked to mention one task in which they felt that they lacked adequate knowledge and skills or where they had problems when working. The common tasks that were cited included methods of disease surveillance and reporting, family planning and water treatment (Table 5). This data could indicate areas where training of HSAs and refresher courses should focus on. As such, in may be necessary that during the planning and delivery of future training and refresher courses for HSAs, emphasis should be placed in these areas.
6.5 Tasks on which the HSAs were consulted frequently by the community
The sampled HSAs were asked to estimate the proportion of people in their catchment areas who consults their services, excluding immunisation and growth monitoring. Half of the sampled HSAs (50%) estimated that more than half of their catchment population does not consult them. The minimum estimate of the population which consults them was 2% of the catchment while the maximum was 97% and a mean of about 45%. In order to highlight the particular activities for which HSAs are being consulted, a list of possible tasks was tabulated in the questionnaire and the HSAs were required to answer ‘yes’ or ‘no’ for each task. Consider Table 6 below. The results showed that most HSAs in the sample were being consulted frequently for treatment of minor illnesses, water chlorination, disease outbreaks and for family planning methods. Another important service, which HSAs said they perform in their catchment areas was certifying death and providing gloves for cleaning the corpse. And being the only health personnel that people see amidst them, HSAs are people’s only source of hope and assistance when diseases strike or when death occurs. They are therefore consulted to assist with transport to take patients to health centres and hospitals and to provide transport for dead bodies. As noted by Chilowa and Munthali (1999), HSAs have social roles and obligations that they have to fulfill in their communities. These include amongst others, providing cash credit to people and joining local committees.

35
Table 6: Tasks for which most villagers consulted HSAs in SA, KK, NS and DA Districts (October-November 2001)
Task or service Proportion of HSAs (%)
Water chlorination/treatment 91.7 Treatment of minor illnesses 88.4 Disease outbreaks 86.6 Family planning 80.2 To provide gloves for cleaning dead bodies (corpses) 50.4 Transport for patients 47.9 Nutrition advice 20.0 Sanitation 15.0 To certify death 11.6 Counseling 10.0 Vector control 9.9 Transport for funerals 8.3 Health education 7.5 Installation of boreholes 7.5 Cash credit 5.0
6.7 Reasons why some people do not consult HSAs
An array of reasons was cited by the HSAs as to why some people in their catchments do not consult their services. These have been clustered into four broader categories namely: access constraints, quality constraints, fitness in terms of people’s socio-cultural systems and relevance (Figure 2).
Figure 2: Reasons given by HSAs as to why some people in their catchment areas do not consult them (October-November 2001)
Access54%
Fitness6%
Relevance19%
Quality21%

36
6.7.1 Access factors According to the sampled HSAs, some people in their catchment areas do not consult their services because of distances and impassable rivers in the rainy season (40%). The reason arises because some HSAs do not stay in their catchment areas because there no good houses available. Some HSAs also suggested that some HSAs bahave in a boastful manner and shout at the villagers (8%). It was also suggested that in catchments that are close to a health centre, most people prefer going to the HC rather than visiting an HSA (4%). Furthermore, it was also indicated that some people had never been in a situation that required assistance from an HSA and thus have never contacted them.
6.7.2 Relevance The sampled HSAs indicated that most people see no justification in visiting an HSA especially those who stay very far because most of the HSAs do not have drugs in stock (10%). Furthermore, the HSAs also noted that some people, particularly men feel that HSAs are there for women and children only because they are mostly seen in an area during growth monitoring and immunisation (5%). Laziness and shyness among some people were also reported by the HSAs as making some people to fail to consult an HSA for a service.
6.7.3 Service quality According to the sampled HSAs, their services have been dwindling over the past years because they lacked support from government. They usually have no drugs such that their assistance is valued lowly compared to what other health service providers in the same areas can afford to offer e.g. traditional healers and local vendors/shops. Living conditions of HSAs are also poor and their houses are often dilapidated. This has an effect on the way the community evaluates their services as they may be judged on such other external parameters.
6.7.4 Fitness Some religions do not recognize any hospital service as important to their people. According to the HSAs, members belonging to these religions do not consult them as they do not fit into their life styles. Further to this, the HSAs also said that some HSAs work for only half of a day (in the morning) when people are busy with farming, hence conflicting with local calendars.
6.9 Proportion of children brought for growth monitoring
The HSAs were also asked to estimate the proportion of underfive children who are brought to them for growth monitoring and immunisation. About 33% of the HSAs said that less than half of the children in their catchment areas are brought to such sessions. The estimates ranged from 10% to about 97% and there were basically very little differences between HSAs from the four districts. None of the HSAs was sure of a 100% coverage rate. The main reasons that were cited for non-attendance to growth monitoring and immunisation are laziness and ignorance of the mothers (69.7%), distance (15.8%), fearing the side-effects of vaccines, (5.3%), cultural

37
reasons (5.3%) and non-availability of supplementary food (3.9%). On distances, the HSAs were also asked whether they run mobile clinics in their catchment areas. About 61 percent said they do while the rest said they do not, basically because people stopped coming to such clinics as they had no drugs to treat sick children and/or supplementary foods to give to malnourished children.
6.10 Work carried out in the previous month
The HSAs were also asked about tasks they had carried out in the month of September 2001. Only 6 of the 121 HSAs indicated that they had not conducted any immunisation. The rest had given immunisation to various numbers of children ranging from 9 to 600 children. About 54% of the HSAs had vaccinated less than 100 children. Number of immunisation and growth monitoring sessions that were conducted by these HSAs ranged from 1 to 26 sessions.
6.10.1 Disease investigation and treating patients Approximately 36% of the HSAs had not conducted any disease investigation and nearly 62% of the HSAs had not issued any drugs (medicines) to their communities. About 51% of the HSAs had not worked at their health centres while the rest had served various numbers of patients at their HCs ranging from 20 to 960.
6.10.2 Nutrition and health talks About 54% of the HSAs conducted nutrition talks in their catchment areas while about 10% did not have (general) health talks with their people in the month of September 2001. Sixty three percent of those who had health talks, included HIV/AIDS in their talks.
6.10.3 Water treatment Water protection and treatment is either conducted at source and/or at home before being consumed. Nearly 75% of the HSAs did not do any water protection works in their catchment areas in the month of September. This could be due to the fact that water-borne infections and water contamination are usually very low in the months of June to late October. However, 26 HSAs had treated various numbers of wells/tanks in their catchments ranging from 1 to 20 tanks/wells. In terms of water treatment at household level, 37 of the 121 HSAs had assisted over 5000 households with water treatment.
6.10.4 Family planning Three FP methods namely condoms, pills and Depo provera (injection) were reportedly given out by some HSAs in the month of September 2001. 71 of the 121 HSAs had issued various numbers of condoms to people in their catchments. Numbers of clients ranged from 1 to about 400 people with no major differences between the four districts. Clients for pills ranged from 1 to 26 but one HSA in Salima had a total of 840 clients. 22 HSAs had clients for Depo provera ranging from 1 to 35 people. The 22 HSAs were from all the four districts.

38
6.10.5 Other tasks carried out in September 2001 Seven of the 121 HSAs supervised TBAs, three in Salima and one each in Ntchisi and Dowa and two in Nkhotakota. One HSA conducted village registration while 4 HSAs did some TB work. Other tasks that were conducted included (food) shop inspections, HIV counseling and formation of borehole protection committees.
6.11 Other activities conducted by HSAs at their health centres
HSAs are obliged to assist in different ways at their HCs at least once or twice a month. Table 7 below gives a list of activities that are also carried out by the sampled HSAs at their HCs. In the months of September and October, most of the HSAs said they assisted in providing immunisation (to mothers and children),giving health talks and performing growth monitoring functions. On family planning, the HSAs said that they were involved in providing condoms, birth control pills and Depo provera.
Table 7: Activities carried out by HSAs at health centers in Salima, Nkhotakota, Dowa and Ntchisi (September-October 2001)
Activity Proportion of HSAs Immunizations 90.9 Health talks 88.4 Sterilizing equipment 86.8 Growth monitoring 86.0 Providing family planning methods 23.5 Cleaning materials and washing 17.4 Mail collection/Messenger 12.5 Manning the dispensary/injection and dressing room 10.7 Writing reports 7.8 Giving food supplements 2.0 Prescribing drugs 1.7
6.12 How do HSAs respond to emergencies?
Emergency circumstances such as floods and disease outbreaks are common in most parts of the country. HSAs are among the first people to note such events and to report to their HCs. In the visited catchment areas, outbreaks of scabies, diarrhoea, dysentery and cholera were reported to have occurred in the past 2-3 years. In response, HSAs indicated that they firstly conduct a quick community survey in order to determine the magnitude of the outbreak and its cause(s). The survey also helps to identify the groups of people who have been affected and the locations where they reside. If the problem and its causes have been identified, the HSAs then set-up temporary clinics in the affected areas and go to their HCs to get the necessary drugs apart from giving health talks. Complicated cases are referred to HCs.
6.13 Working with NGOs and other government projects
Overall, approximately forty three percent of the sampled HSAs indicated that they were implementing activities on behalf of NGOs or other government departments apart from the normal government HSA work (54% in Salima, 40% in Dowa, 33% in Nkhotakota and 21% in Dowa). All the programmes had either a health or nutritional purpose (Table 8). About 77% of the programmes/projects were NGO funded while about 22% were funded by a government department. The community was funding only one of the projects.

39
In terms of time allocation, the sampled HSAs reported that government HSA work was allocated more time compared to other projects, an average of 60-75% of total working time for government work. None of the HSAs who worked on another projects indicated that s/he was receiving an extra salary from the project but about 32% said they benefited from training and training allowances. About 36% of those HSAs who were working for another project were also benefiting from duty allowances, ranging from K100 to about K1,500 per month.
Table 8: NGOs and projects with which some of the sampled HSAs were working
Name of programme or sponsor Number of HSAs
Water & sanitation 30
Bakili Muluzi Health Initiative (BMHI) 9
Stepping Stones (ACTION-AID) 7
Nutrition project 5
Save the Children Fund (UK) 4
Family planning programme 4
Community Based Care Project 3
Bilharzia control project 2
Salima AIDS Support Organisation (SASO) 1
MACOHA mobile clinic 1
Tifere Zina radio programme 1
6.14 Supervision
Nearly 51% of the sampled HSAs were supervised by senior HSAs, 39% by HAs while about 8% and 2% were supervised by either an Environmental Health Assistant or a Medical Assistant. When asked about what is usually done during supervision, about 76% said that they hold person to person discussions with their supervisors as well as submitting monthly progress reports. The rest (24%) said their supervisors had never visited them.
6.15 Significant community based projects initiated by HSAs in their catchment areas
The sampled HSAs were asked to cite significant community projects, which they have initiated in their catchment areas for which the local community applauds them. About 44% of the HSAs cited none. The rest cited various projects and organisations including VHWCs, HIV/AIDS awareness clubs, orphan care groups, borehole construction and maintenance committees, dome slab/san plats projects and underfive care groups. In these projects, the roles of the HSAs were said to those of a supervisor, educator, counselor and facilitator.
6.16 HSA Membership to local committees
HSAs live within local communities. They therefore (together with other extension workers and teachers) have social obligations to fulfill. About 18% of the sampled HSAs indicated that they were in an executive committee of a local club or association. The clubs to which HSAs belonged ranged from development committees to financial clubs (e.g. SACCO) and to charity organizations like orphan care groups and funeral and church committees.

40
6.17 Source of information
The HSAs were asked about their regular source of new information about developments in the health sector and areas of their work. About 84% indicated that their supervisors were their regular source of information while 6.6% said their workmates provided them with such information. Five percent of the HSAs said radio was their regular source of information. The rest cited workshops (2%), hospital in-charge (1.7%), and official circulars and memos (0.8%). This confirms that HSAs are usually not oriented to new interventions when such such interventions are being introduced.
6.18 What other tasks could HSAs perform?
The HSAs were also asked to suggest tasks, which they felt they could also perform in their catchments without necessarily exerting more pressure on their schedules. The suggested tasks were as follows:
Meat inspection; Conducting and assisting child deliveries; Conducting adult literacy classes; Gender sensitization workshops; and Teaching modern farming methods.
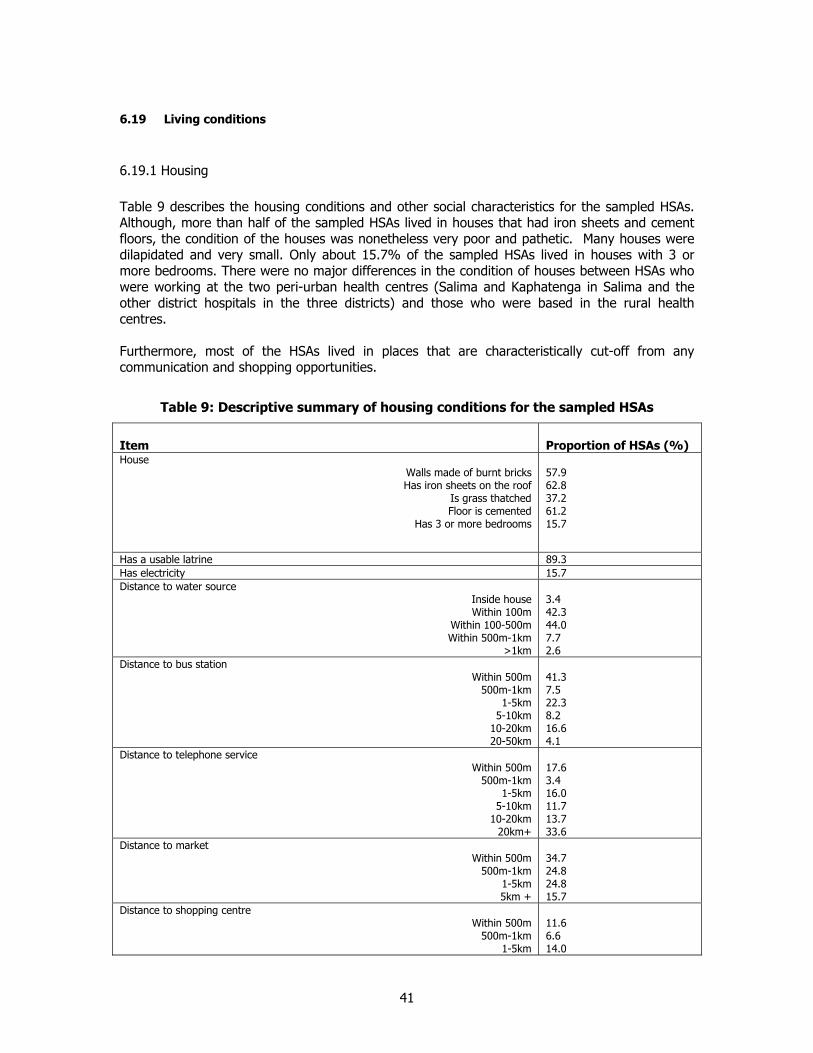
41
6.19 Living conditions
6.19.1 Housing Table 9 describes the housing conditions and other social characteristics for the sampled HSAs. Although, more than half of the sampled HSAs lived in houses that had iron sheets and cement floors, the condition of the houses was nonetheless very poor and pathetic. Many houses were dilapidated and very small. Only about 15.7% of the sampled HSAs lived in houses with 3 or more bedrooms. There were no major differences in the condition of houses between HSAs who were working at the two peri-urban health centres (Salima and Kaphatenga in Salima and the other district hospitals in the three districts) and those who were based in the rural health centres. Furthermore, most of the HSAs lived in places that are characteristically cut-off from any communication and shopping opportunities.
Table 9: Descriptive summary of housing conditions for the sampled HSAs
Item
Proportion of HSAs (%)
House Walls made of burnt bricks Has iron sheets on the roof
Is grass thatched Floor is cemented
Has 3 or more bedrooms
57.9 62.8 37.2 61.2 15.7
Has a usable latrine 89.3 Has electricity 15.7 Distance to water source
Inside house Within 100m
Within 100-500m Within 500m-1km
>1km
3.4 42.3 44.0 7.7 2.6
Distance to bus station Within 500m
500m-1km 1-5km
5-10km 10-20km 20-50km
41.3 7.5 22.3 8.2 16.6 4.1
Distance to telephone service Within 500m
500m-1km 1-5km
5-10km 10-20km
20km+
17.6 3.4 16.0 11.7 13.7 33.6
Distance to market Within 500m
500m-1km 1-5km 5km +
34.7 24.8 24.8 15.7
Distance to shopping centre Within 500m
500m-1km 1-5km
11.6 6.6 14.0

42
5-10km 10km +
9.1 58.7
6.19.2 Salary The recommended minimum wage per day for ground staff in Malawi is currently pegged at about K50 per day, which translates to about K1500 per 30-day calendar month. Taking this as a base, about 3% of the sampled HSAs were getting less than the recommended minimum wage8. The minimum reported salary was K1046.00 while the maximum was K3820.75 per month and the average was K1809.81. When the question of salary was posed to most HSAs, their immediate reaction was that their salaries were not sensitive to their education levels and that they do not change over time. If this was the case, there is therefore a need to revisit the scenario and make the conditions sensitive to people’s qualifications. Indeed, when the reported salaries were explored by HSA academic qualifications and length of service as HSA, the results do not show any consistency in the salary levels9. The expectation would have been that MSCE holders should start at a higher salary level than both JCE and PLCSE certificate holders. Salary differences among holders of a similar certificate would exist based on the length of service as HSA. The data seems to reveal that some JCE certificate holders get a higher salary than MSCE holders of the same length of service. Only among JCE holders did the expected trend exist in that length of service differentiated their salary levels.
6.19.3 Other benefits attached to the HSA work Apart from the question of salaries, the HSAs were also asked to state if they had other benefits attached to their work. Housing and duty allowances were also mentioned by some of the HSAs. Approximately 10% of the HSAs said that they received a housing allowance of less than K1000 per month while about 89% said their housing allowance was and has been, K1000 for the past 3-4 years. Ninety five percent of the HSAs said they also received a duty allowance every month. The allowances that were reported ranged from K200 to about K550 per month. Approximately 37% of the HSAs indicated that they had government bicycles and of these, 10% said their bicycles were in working condition while the rest said their bicycles were damaged and they had no spare parts to repair them. The HSAs who had received HSA induction course before (81%) were also asked whether they had attended a refresher course in the past 3 years. About 46% of them acceded and 80% of these, said they had attended only one refresher course while about 16% had attended two times. The remainder had attended three such courses. When they were asked about the funders of refresher courses to which they had gone, about 90% said the MoH funded the courses. This was also true for those who had gone to more than one course. The refresher courses for the remaining HSAs were funded by NGOs working in the various catchment areas. 6.19.4 Farming 8 The nature of HSA work makes it sensible to calculate the salary for a 30-day calendar month because they work almost everyday and oftentimes outside normal working hours 9 This observation is only indicative and therefore needs to be treated with caution as usually people do not disclose their actual salaries

43
Another hidden benefit of the HSA system is their access to farming land because of their proximity to chiefs who own customary land. These farming activities supplement some of the gaps that are left by the government salary. When asked whether they had land for farming, 73.6% said they had some parcel of land. However, about 51% of those who had land, held not more than 1 acre of land and about 35% had just 2 acres only.
6.20 Constraints to effective performance
6.20.1 Technical Mobility problems, lack of vaccine storage and carrying equipment and protective clothing were cited by over 65% of the sampled HSAs as constraints to effective performance (Table 10). Mobility problems also prevented some of the HSAs from coovering some of the villages in their catchment areas and in addition, to go their HCs to collect drugs and other necessary provisions for their work including vaccines. As discussed above, Malawi has in the recent past experienced several emergency situations including disease outbreaks. About 45% of the HSAs also cited lack of emergency kit as a constraint that prevents them from containing outbreaks in the catchments. Absence of supervision or rudeness of some supervisors were also cited as affecting HSAs work as they lacked guidance on some of the most important issues.
6.20.2 Socio-cultural constraints Low remuneration, lack of promotion, no refresher courses and poor road network were cited by over 50% of the sampled HSAs as social constraints to their work (Table 10). The first three were singled out as direct demotivators. Those who mentioned that their age was a constraint were all above 45 years of age and they talked mainly of traveling to some of their villages, which are very far. Four males and three females complained that their sex affected their work. The male HSAs said that some women in their catchment areas do not attend HSA functions on allegations that the HSAs behave immorally while the females said they usually have problems interacting with men in their catchment areas. In relation to marital status, single HSAs said they had problems especially when dealing with family planning issues as some people felt that the HSAs were not fit to discuss marriage issues since they were not married themselves.

44
Table 10: Technical and socio-cultural constraints to HSA work cited by HSAs from Salima, Nkhotakota, Ntchisi and Dowa (November 2001)
Constraint
Proportion of HSAs (%)
Technical
Mobility problem (no transport) No storage and carrying facilities for vaccines
Lack of protective clothing Inadequate stationery
No emergency kit No supervision
Rudeness of supervisors Irregular supply of vaccines Lacking immunization skills
69.4 65.0 65.0 45.0 35.0 25.0 10.0 25.0 5.0
Social constraints
Low remuneration No promotion
Poor road network No refresher courses
Poor telecommunication Cultural values of the community
Poor relations with the community Working in remote areas
Poor relations with supervisor My age
My marital status My gender My religion
84.3 60.3 56.2 54.0 33.9 16.7 14.0 14.0 9.1 9.1 6.6 6.6 5.0
6.20.3 Replenishment of drugs and materials As noted in Table 10 above, most HSAs cited irregularity in the supply of drugs and other materials as a constraint to their work. When asked about the frequency of replenishing of their drug stocks, about 88% of the 121 sampled HSAs said they had never been issued with drugs at any time since they started working as HSAs while the rest (12%) said they replenish their drug stocks monthly. Those who had ever been supplied with drugs also said that usually they are undersupplied in terms of what they had requested for. Table 11 below gives a summary of drugs and materials, which some HSAs had in stock at the time of the survey. As would be noted, most HSAs had weighing scales, condoms and ORS sachets as compared to other materials. In the absence of tally sheets, most of the HSAs do not keep any records of immunization and other services which they do every month.

45
Table 11: Availability of drugs and other materials among the sampled HSAs in SA, KK, NS and DA (November 2001)
Drugs/Materials
No. of HSAs
Quantity
Anti-Malarial drugs 5 Average of 167 adult doses (70 minimum and 370 maximum) Antibiotics 4 Average of 55 adult doses (10 minimum and 100 maximum)
Pain relievers (pain killers) 4 Not specified Eye ointment 1 Not specified Vitamin A capsules 5 Not specified
ORS sachets 33 Range of 2-1500 sachets (50% with < 20 sachets) Weighing scales 59 Average 4
Condoms 41 Minimum of 5 condoms and maximum of 1747 (50% with <150) Ovulet pills 2 Average 300
Lefiminol Pills 2 Average 507
Syringes 4 Average 5 Needle sterilizers 11 Range 1-5
Tally sheets 2 Average of 3 High test hydro chlorine 3 Not specified
6.21 HSA relations with the local community and other staff at the health centre
HSAs belong and report to fixed health centers or hospitals, where their supervisors and other curative health staff are stationed. They are ideally supposed to reside within their catchment areas where they interact with extension workers from other government departments, some NGO staff and the local community. The sampled HSAs were asked to rate their relations with the various groups of people whom they interact (Table 12).
Table 12: HSA rating of their relations with various groups of people
Rating (% of HSAs) Group of people Good Fair Bad Never interacted before Clinical Officers 57.0 28.1 5.8 9.1 Nurses and Midwives 62.8 28.1 5.0 4.1 Health Assistant 71.1 7.4 1.7 19.8 Lab Technicians 26.4 4.1 1.7 67.8 MoH District/HQ staff 62.0 27.3 7.4 3.3 Other Extension workers 70.8 16.7 3.3 9.2 Local community 71.1 28.1 0.8 0
6.22 Suggestions to improve the work of HSAs in Malawi as put forward by the sampled HSAs
A total of twelve proposals were put forward by a number of the sampled HSAs on how their work could be improved (Box 4). Provision of adequate and reliable transport, regular refresher courses, protective clothing (raincoats and gum boots), stationery, salary and house allowance increments and provision of emergency kits to HSAs were the main suggestions which were put forward by the HSAs.

46
Box 4: Proposals made by HSAs to improve HSA work in Malawi (Oct-Nov 2001)
Provide HSAs with transport Allow HSAs to attend regular refresher courses Provide HSAs with protective clothing Increase salaries and house allowances Provide HSAs with emergency kit Construct houses for HSAs Ensure that HSAs have adequate supervision Promote hardworking HSAs Preventive health section should stand on its own Introduce HSA loan scheme Re-introduce training for VHCs to assist HSAs
47
7.0 VIEWS AND PERCEPTIONS OF MOTHERS AND CHILD CARETAKERS
7.1 Summary of findings
A total of 325 mothers/child caretakers from catchment areas of nine health centres were interviewed about their experiences in working and staying with HSAs in their areas. Approximately 98% of the mothers/child caretakers who were interviewed knew or had heard about HSAs. Those who had never heard about HSAs were all from the catchment area of Salima district hospital10. Evidence of undercoverage was imminent from the data that was collected. Sanitation, growth monitoring, immunisation, family planning and health talks were cited by 60-88% of the sampled mothers/caretakers as being carried out in their areas while the rest said they had never heard that these activities were being carried out in their villages. The other HSA tasks as contained in the HSAs ToRs were cited by very few of the mothers/caretakers. In general, the HSAs were rated highly in terms of their performance in the various activities. However, some mothers/caretakers felt that their performance was being affected due to the abscesses after vaccinations, frequent shouting at mothers/caretakers, boasting that they know more than villagers, irregular visits, infidelity and non-availability of drugs. Only 30% of the mothers said that they had consulted an HSA for assistance other than immunisation, growth monitoring and heath talks. Those who knew about HSAs but had never consulted them cited access problems and frequent unavailability of drugs as the reasons for not consulting their HSAs. The following subsections give detailed findings from the interviews with the mothers/child caretakers.
7.2 Characteristics of the households from which the sampled mothers/caretakers came
A questionnaire was administered to a total of 325 mothers/caretakers drawn from 23 villages, randomly sampled from the catchment areas of nine health centers in Salima district (Appendix 4). The age range of the respondents was 39 years, a minimum age of 16 years and maximum of 55 years. The highest academic class completed by the respondents was form 4 (2%) while 38.5% had never been to school (Figure 3).
10 the reason why some individuals had never heard about HSAs could be because they resided close to Salima hospital. As such they find it more convenient to go to the hospital than to approach an HSA

48
Figure 3: Educational levels of the sampled mothers in Salima (November 2001)
Figure : Educational level of the sample mothers, Salima (November 2001)
No education38%
Std 1-424%
Std 5-832%
Form 1-24%
Form 3-42%
Approximately eighty six percent of the households in which interviews took place were male headed while the rest were female headed (14 percent). The figure for female headed households in the sample was lower than the national estimate of about 30%. In terms of religious affiliation, about 69 percent of the household-heads were Christian, 22% were Muslim, 5.8% belonged to the “Nyau cult” and about 3.1% did not follow any religion. About 3.1% of the household heads were reported to be Pagan worshippers. The trend is not very different for the sampled mothers/caretakers as about 75% of them were Christian, 22% were Muslim and the rest belonged to the other religions cited above. The 325 households from the sampled mothers came contained approximately1653 people, giving an average household size of 5.1 but in some households, there were more than nine members. Figure 4 shows the age-sex distribution of the population of the sampled households. Proportionately, most people were in the age ranges of 15-30 years (30%) and 0-5 years (28.3%).

49
Figure 4: Population distribution of the sampled households
Figure : Population (Age-Sex) distribution of the sample households
30.2
26.428.3
25.1 24.7 24.925.3
34.8
30
18.2
13.215.7
1.2 0.9 1
0
5
10
15
20
25
30
35
40
Males Females TotalAge groups and sex
prop
rtion
(%)
0-5 6-14 15-30 31-60 60+
As indicated above, households for inclusion in the survey were sampled on the basis of having at least one child under the age of five years. This was the case because one of the aims of this survey was to explore reasons why some children are immunized very late or are not immunized at all. There were a total of 457 underfive children in the 325 households that were visited, giving an average of 1.4 children per household (maximum of 3). About 62.8% of the households had one child under the age of five years, while 33.8% and 3.4% of the households had 2 or 3 underfive children respectively. When the mothers/caretakers were asked about their relationships with the children, about 98% of them indicated that they were the mothers of the, 1% were their grandchildren while the rest were either their aunts/uncles or their sisters/brothers.
7.3 Knowledge of HSAs and their work
The first question regarding the work of HSAs was asking the mothers/caretakers if they had ever heard of HSAs and if so, whether there was one who works in their village and what activities s/he was implementing. Approximately 98% of the mothers/caretakers acceded that they had heard of an HSA and of these, 91.8% (n=293) said that an HSA worked in their village. The six mothers/caretakers who said they had never heard about an HSA were all from one catchment area close to Salima District hospital. They belonged to three different villages belonging to one HSA. When their education level was traced, four of the mothers were among those that had never been to school while two were in the Std. 5-8 category. The data further reveals that three of the six mothers were Christians (non Watch Tower) while the other three were Muslims.

50
7.4 Functions of the HSAs
As alluded to previously, the mothers/caretakers were also asked to cite the various activities that HSAs were conducting in their respective villages or in the nearest villages. A list of activities was tabulated in the questionnaire and Research Assistants were instructed to tick against all the HSA activities that would be cited by the mothers on their own and then probe for the rest of he activities. The aim of probing was to capture all the various activities that were being implemented after determining the proportion of mothers who easily remembered that their HSA was implementing a particular activity in their village (Table 13). The number of women who spoke about various activities varied. This was so because other women chose not to comment on other activities. Some activities such as vitamin A supplementation, reporting emergencies, treatment of common illnesses and development projects were mentioned by some of the women independently as they were not included in the original list of activities that were pre-coded. The data presented in Table 13 provides evidence that HSAs were indeed implementing a number of activities in most areas that were visited. Sanitation, water treatment, growth monitoring, immunizations and health talks scored highly when mothers were answering the question pertaining to which type of activities were being implemented by their HSAs. However, a closer look at the data reveals evidence of under coverage. In most communities, some pockets are not reached by the HSAs. About 34% of the mothers/caretakers did not know that their HSAs were implementing immunization activities right within their areas. For growth monitoring, 28.4% expressed ignorance that their HSAs were carrying out this activity. For disease investigation, only 19% indicated that their HSAs were doing it meaning that about 81% of the mothers were not aware if their HSAs were doing any disease investigation in their villages. Using citation of an activity without probing as a yardstick of determining what activities were being appreciated by the visited communities, sanitation and growth monitoring appear to be the type of activities that might qualify.

51
Table 13: Activities being implemented by HSAs as reported by mothers/caretakers from Salima (October-November 2001)
Activities N Proportion of mothers who said ‘yes’
Proportion who cited without prompting
Proportion of mothers who cited after prompting
Immunizations 292 66.4 29.4 70.6 Growth monitoring 292 71.6 41.2 58.8 Disease investigation 290 19.0 6.9 93.1 Health talks 292 66.4 24.7 75.3 Water treatment 292 81.5 25.3 74.7 Sanitation 292 88.0 64.7 35.3 Vector control 292 11.6 1.4 98.6 Running the DRF 292 6.8 3.1 96.9 Family planning 292 64.0 16.6 83.4 Nutritional clinics 288 28.8 6.2 93.8 Working with VHCs 284 44.0 6.0 94.0 Vitamin A supplementation 56 All* - Reporting emergencies 56 All* - Treatment of illnesses 56 All* - Development projects 56 All* - Disaster preparedness 56 All* - * denotes activity added to the predetermined list after mothers cited it
7.5 Mothers/caretakers rating of HSA performance and that of other health staff
After discussing the various activities that HSAs were implementing in the various villages, the mothers/caretakers were then asked to rate the performance of their HSAs on a few common activities. They were further asked to give reasons for their rating. Three ratings namely poor, fair and good were purposively designated and uniformly applied for each activity. Table 14 carries findings from this subjective exercise. The number of women who evaluated the HSAs on the various activities kept changing. This was basically because some women did not comment on some activities either because they had never taken place in their village or because they were not very sure of what to say. Most HSAs were rated highly by the mothers/caretakers. Issues of timeliness, regular visits, elaborate and clear explanations, good behaviour and administering vaccinations without bad side effects were the common reasons which were given for rating their HSAs highly. These are issues that matter most in people’s lives and in decision-making on whether to approach an HSA or not. On the other hand those HSAs who make irregular visits, shout at mothers, whose vaccinations result in side effects, those who boas to know a lot, reluctant to explain more about certain issues, those who commit adultery and those who are selfish were rated poorly. Therefore, if the participation of communities in HSA work is to be improved, these are the issues that need redress as they act as social barriers to accessing the services being implemented by HSAs.

52
Table 14: Mother’s/caretakers rating of HSA performance an a few selected activites, Salima (October-November 2001).
(n=number of respondents) Rating (%) Reasons Activity (n in brackets)
Poor Fair Good Poor Fair Good Immunization (n=193) 3.1 8.8 88.1 Abscesses Shouts at mothers Always on time
No abscesses Notifies next date
Growth monitoring (n=205) 1.0 4.4 94.6 Shouts at mothers
Explains results Weighs properly
Disease investigation (n=53) 11.5 11.5 76.9 Gives lame excuses No feedback
Irregularly conducted
Gives drugs before outbreaks
Health talks (n=190) 1.1 13.2 85.8 Boasts to know more
Teaches as if not interested Reluctant to explain HIV/AIDS
Very clear explanations
Water treatment (n=236) 3.4 15.3 81.4 Irregularly conducted
Drugs given on time Explains clearly
Sanitation (n=258) 7.4 20.2 72.5 Never gives feedback
Irregular visits Very elaborate
Family planning (n=173) 1.7 6.9 91.3 Refuses about side effects
Secretive Motivates people Very clear when explaining
Nutritional clinics (n=84) 14.3 10.7 75.0 No food given Never carried out now
Provides food Very clear
General behaviour (n=275) 2.9 3.6 93.5 Adultery and selfishness
Always on time Hears our views
The mothers/caretakers were also asked to rate (good, fair, poor) the other staff they usually meet whenever they visit a HC that is close to them terms of the assistance they provide and their general behaviour. Table 15 below gives findings from this exercise. Nurses and Clinicians/HA’s (a Dokotala) were commonly met by the sample mothers at their nearest health facilities and about 51% said even HSAs were also met at the HC. The Dokotalas were rated highly on both assistance and attitude towards patients compared to the nurses. The poor rates, which were given to all the staff, were mainly due to bad behaviour and arrogance apart from nepotism and non-availability of drugs. Kadzandira and Mvula (2001) made similar observations in a qualitative study on gaps analysis in social service provisioning in Malawi. Issues of staff negligence, nepotism, arrogance, non-availability of drugs and non-observance of schedules were cited in all 16 sites where the study was conducted. These are issues that are continuously diverting people away from accessing formal health services in the country and they need urgent redress. Chilowa et al (2001) also noted that in the two weeks prior when their survey was conducted, over 60% of the sampled households visited either a local vendor/shop or an injector when a member of their household fell ill.

53
Table 15: Mothers rating of health staff that are commonly met at health centers (Salima, November 20010
N=325 Nurse (s) Clinician/Health
Assistant HSA
Yes 72.5 85.2 51.4 Met at HC? No 27.5 14.8 48.6 Good 61.8 70.5 48.3 Fair 8.6 12.0 1.8 Poor 1.8 2.5 0.9
Assistance
No rating 27.7 15.1 48.9 Good 54.2 70.2 45.5 Fair 12.3 12.0 4.0 Poor 5.8 2.8 1.5
Attitude
No rating 27.7 15.1 48.9
7.6 Proportion of mothers/caretakers consulting an HSA
Only about 30% of the mothers/caretakers who knew HSAs in the 23 sampled villages accepted to have consulted an HSA in the past 12 months for a service other than immunization, health talks or growth monitoring. The rest said they did contact any HSA. When asked why they never consulted an HSA, almost half (49.6%) said that their HSAs are difficult to be found and that they stick to their work schedules. The rest either said that they had never met a situation that called for HSA assistance (30%) or that they resided close to a health center. Those who had approached an HSA were asked about the type of service they wanted from him/her and whether they received it or not. Table 16 shows the type of services for which HSAs were consulted. It should be noted that the sampled mothers/caretakers mainly approached an HSA when they sought treatment for an illness or needed to obtain family planning methods. HSAs therefore provide good channels for reaching most of the rural masses with health interventions, in a country that has poor health infrastructure and few qualified personnel.
Table 16: Activities for which HSAs were consulted most
Type of assistance Proportion of mothers (n=98) Treatment of illness 84.9 Purchasing drugs 1.1 Water treatment 7.5 Counseling 7.5 Supplementation 25.0 Family planning methods 75

54
7.7 Response to last illness
The mothers were asked if any member of their household fell ill in the 12 months prior to the survey and what first action they took in response to the illness. Ninety seven percent of the mothers acceded that some members fell ill in the specified period. Regarding the first action that was taken, about 48% of the mothers said they rushed to the nearest HC, 28% bought medicines from local shops/vendors while about 18% approached an HSA. The rest either visited a traditional healer, private clinic or did nothing as a first response. Those who did not approach an HSA at first were asked why this was the case. Two major reasons were advanced. The first reason was that their HSAs usually had no drugs and the second reason was that their HSAs stayed very faraway and therefore was not easily accessible.
7.8 Constraints facing HSAs in their work
Mothers pointed out several constraints that prevent HSAs from performing well (Table 17). Poor community participation was one of the constraints mentioned. The other constraints relate directly to the MoHP including great workload for HSAs, irregular supply of drugs and vaccines, poor remuneration, HSAs staying very far from their catchment areas and lack of supervision. All these issues need to be addressed directly by the MoHP.
Table 17: Constraints facing HSAs reported by women from Salima (November 2001)
Constraints Proportion of mothers Too much work 34.5 Poor community participation 22.6 Bad roads 13.1 Irregular supply of drugs 12.5 Stays very far 9.5 Personal negligence 8.0 Irregular supply of vaccines 4.5 No supervision 3.1 No supply of drugs 2.4 Poor remuneration 2.4 Irregular supply of water treatment chemicals 1.7 Theft/selling of drugs 0.3

55
7.9 Suggestions for improving the work of HSAs
The sampled mothers/caretakers put forward an array of suggestions and proposals on how the work of HSAs could be improved. The suggestions and proposals were as follows: a). to Government and her partners
• increase salaries for HSAs in order to motivate them; • provide regular supervision to the HSAs; • provide pushbikes to HSAs; • provide good housing for HSAs; • thoroughly train HSAs before deploying them; • provide refresher courses to HSAs; • recruit more HSAs to reduce current workload; • punish HSAs when reported to be misbehaving; • provide drugs to HSAs to distribute at village level; • provide water treatment chemicals to HSAs throughout the year.
b). to HSAs
• must make frequent pre-arranged visits to communities; • should motivate villagers to construct shelters in all villages; • should intensify community sensitization campaigns; • should be development oriented; • should have drugs during growth monitoring sessions; • should provide feedback to community on any investigation made; • should set up VHCs in all the villages; • should also be making door-to-door visits.
c). for the community
• should be empowered to monitor, evaluate and take action on an HSA; • should assist in constructing shelters and houses for HSAs
56
8.0 IMMUNISATION PERFORMANCE OF THE SAMPLED CHILDREN The child immunisation schedule for Malawi stipulates that BCG, a vaccine for Tuberculosis is supposed to be given to any child at birth while DPT 1 should be given at 6 weeks of age or just thereabouts. DPT 2 and DPT 3 follow DPT 1 but with a 4 week period in between each. Polio 0 is supposed to be given to the child within 6 weeks of birth, while Polio 1 comes 4 weeks later followed by doses of Polio 2 and Polio 3 at intervals of 4 weeks respectively. Lastly, children are expected to receive the last vaccine against measles at nine months of age or later but nor more than 12 months of age (and not before nine months). However, following discussions with some health staff in the visited health centres, it was stated that polio 1 and DPT 1 are usually given on the same date and that the schedule starts at about 6 weeks of age usually because polio 0 is usually not available in most health centres. In this survey, a total of 423 children under the age of five years were identified and their dates of birth were verified from their health passport booklets or cards. Five of the 423 children were removed from the sample because of date recording errors whereby the dates in the booklets/cards either indicated that they started receiving vaccination before they were born or their birth dates were not recorded. As part of this analysis, steps were taken to prevent wrongly classifying children as non-recipients or late receivers by regrouping the children according to their age as evident from their dates of birth. Ages (in weeks) of all the 418 children were calculated from the date of interview as:
Child age (in weeks) = (DoI – DoB) / 7, (where DoI is date of interview and DoB is date of birth) For DPT 1 and Polio 1, all children who were less than 6 weeks of age were purposively removed from the sample because they were officially not eligible for the vaccines. Similarly, for DPT 2 and Polio 2, all children who were less than 10 weeks of age were also screened out while for DPT 3 and Polio 3, all children who were less than 14 weeks of age were screened out. For measles, a general frequency table was produced in order to observe if some children received the vaccines before the recommended age (nine months as recommended by WHO) The data presented in Table 18 suggests that immunisation coverage among the sampled children was generally good. Only about 16.8% of the eligible children had not received DPT 3 by the time of the survey, 18.4% had not received Polio 3, 11.7% and 8.9% had not received measles and BCG vaccines respectively. A child is said to be fully immunised if s/he has been given three doses of polio vaccine, three doses of DPT vaccine, one dose of BCG and one dose of measles. Taking this definition, it was observed that the rate of full immunisation coverage among the 196 children in the sample who were 9 months old or more was in excess of 88%. While the coverage rate seems good, the question is whether the children received the vaccines on time or not. Of all the 403 children who were eligible to receive DPT 1 and Polio 1, only about 22% and 23 % received DPT 1 and Polio 1 within the period when the two vaccines were due respectively. About 70% received their DPT 1 vaccine injections later than the recommended age for reception. For measles, about 60% of the 196 eligible children (by age) received their vaccine within the recommended time period of 9-12 months of age while 7.1% received it earlier, 21.4% received it very late and 11.7% had not received it by the time of the survey. BCG was the worst when considering reception beyond the recommended time. Over 80% of the 418 children received it beyond two weeks from birth, the maximum being 40 weeks from birth. One explanation that was suggested by one health staff member at one HC was that BCG vaccines come in doses of three children such that if one child is born, it cannot be vaccinated until two more new or unvaccinated children are available because once the BCG container is opened, the remaining vaccines become sterile.

57
Table 18: Immunisation status of the sampled children in Salima (October-November 2001)
Type of vaccine Never received Received earlier Received on time Received late
n % n % n % n %
Total n
BCG
37 8.9
*************
45 10.8
336 80.4
418
19 4.7 35 8.7 55 13.6 294 73.0 403
35 9.1 261 68.0 15 3.9 73 19.0 384
DPT 1
2
3 63 16.8 249 66.4 4 1.1 59 15.7 375
27 6.7 38 9.4 56 13.9 282 70.0 403
37 9.6 276 71.9 11 2.9 60 15.6 384
Polio 1
2
3 69 18.4 234 62.4 6 1.6 66 17.6 375
Measles
23 11.7
14 7.1
117 59.7
42 21.4
196
8.1 Reasons for late reception of vaccines or no receipt at all
In general, immunisation coverage rates among the sampled children were generally good (over 80%) but the problem was late reception of the various vaccines. Several reasons were put forward for receiving the various vaccines very late including laziness of the mothers/caretakers themselves, non-availability of vaccines at their health centres or at their HSAs, fearing side-effects and long distances to the immunisation centres (Table 19). The finding that most of the mothers/caretakers either took their children for vaccination very late (or never took them at all) might reveal weaknesses in the immunisation campaigns both at national and district levels as well as at the level of the HSAs themselves. This situation needs to be urgently addressed. The issue of side-effects also needs careful attention by medical researchers so that other ways of administering the vaccines are researched. Other reasons for late reception or no reception at all include such reasons as mothers/caretakers not being advised by health personnel and HSAs on the next dates for other immunization, not being advised that a child must be vaccinated soon after birth and alleged mistakes in recording on the cards.

58
Table 19: Main reasons cited by mothers/caretakers in Salima as to why their children received certain vaccines very late or never received at all (October-November 2001)
Type of vaccine
Reasons for late reception Proportion of mothers/ caretakers
Reasons for not receiving at all
Proportion of mothers/ caretakers
BCG
N/A
N/A
Mother always busy and laziness
No vaccines at HC and HSA
Long distance to centres Other reasons
66.6 16.8 8.3 8.3
Polio 1/DPT 1
Mother always busy/laziness No vaccines at HC/HSA Long distance to centres Fearing side effects Child born at TBA Other reasons
46.6 28.3 3.2 1.5 0.6 19.8
Long distance to centres Mother busy/lazy
33.5 62.5
Polio 2/DPT 2 Mother busy/lazy No vaccines at centre/HSA Long distances Interrupted by pregnancy Other reasons
37.8 30.1 3.7 0.4 28.0
Mother busy/lazy Fearing side effects Long distances
70.6 17.6 11.8
Polio 3/DPT 3 Mother busy/lazy No vaccines at HC/HSA Long distances Fearing side effects Interrupted by pregnancy Other reasons
50.2 24.2 5.0 0.5 0.5 19.6
Mother busy/lazy No vaccines Long distances Fearing side effects Other reasons
85.3 5.9 2.9 2.9 2.9
Measles Mother busy/lazy No vaccines at HC/HSA Long distances Other reasons
55.0 34.0 1.0 10
Mother busy/lazy No vaccines Long distances Fearing side effects Other reasons
70.6 11.7 2.9 2.9 11.8
8.2 Place of receipt
For each vaccine that the 418 children in the sample received, they were asked to state where they received them, whether at a fixed government health facility or at a mobile clinic and/or from any other place like private clinics (Table 20). Over 50% of all the vaccination which were given to the sampled children were administered at a fixed government health facility either a health centre, clinic or a hospital, while 48% were received from a mobile clinic. While it is well known that nearly all vaccination that are given at a mobile clinic are administered by HSAs, it is not clear as to what proportion of the vaccination that are given at fixed health facility are administered by the HSAs and by the other staff. Data that would illustrate this was not available even at the DHO offices.
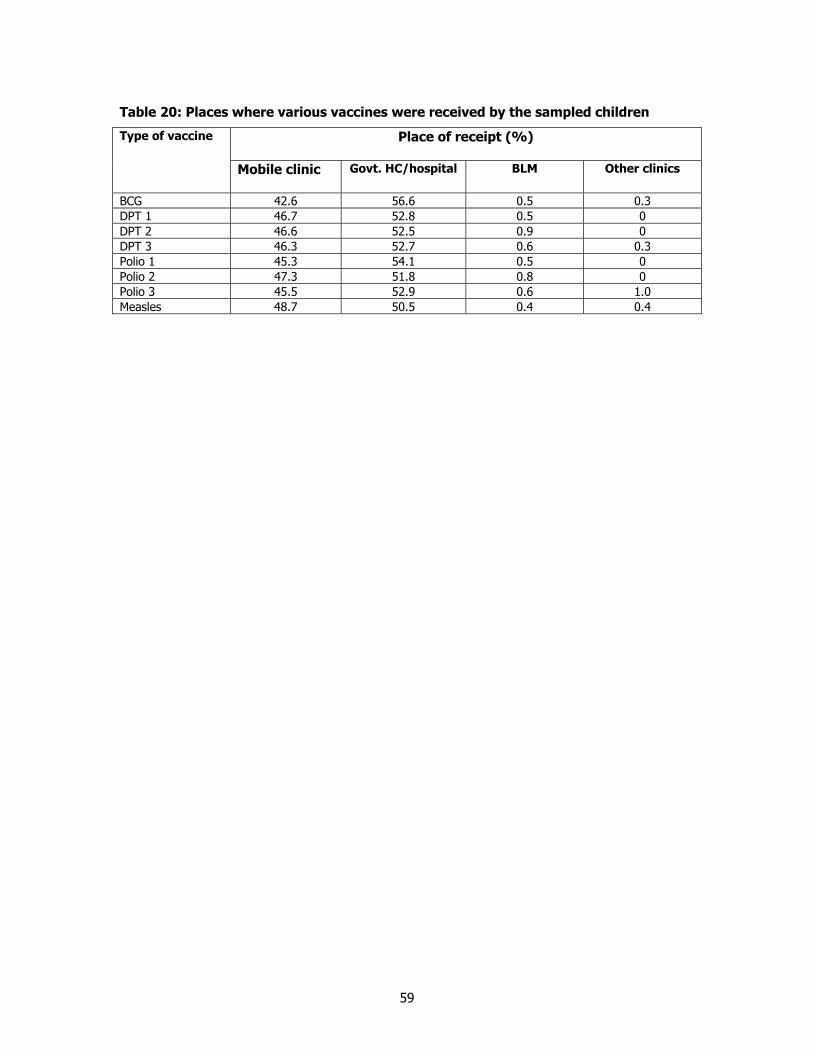
59
Table 20: Places where various vaccines were received by the sampled children
Place of receipt (%) Type of vaccine
Mobile clinic Govt. HC/hospital BLM Other clinics
BCG 42.6 56.6 0.5 0.3 DPT 1 46.7 52.8 0.5 0 DPT 2 46.6 52.5 0.9 0 DPT 3 46.3 52.7 0.6 0.3 Polio 1 45.3 54.1 0.5 0 Polio 2 47.3 51.8 0.8 0 Polio 3 45.5 52.9 0.6 1.0 Measles 48.7 50.5 0.4 0.4

60
9.0 CONCLUSIONS AND RECOMMENDATIONS This chapter presents an overall summary of major issues in line with the terms of reference and objectives of the survey as outlined in the introduction.
9.1 Overall Conclusions
o Overall, HSA’s, formerly recruited as temporary ‘Smallpox Vaccinators’ in the 1960’s and as ‘Cholera Assistants’ in mid 1970’s have contributed greatly to the delivery of preventive health services in rural areas of Malawi. Over time they have formed an extensive network of ground staff bridging the formal health services and the community. They are responsible for about 60% of all vaccination that are given to children under the age of five years in the rural areas. Their contribution has enabled the country to virtually eliminate and/or reduce prevalence rates of the highly infectious but preventable diseases namely: measles, polio, smallpox, diptheria, pertusis, tetanus and tuberculosis. They also play a very significant role in detecting disease outbreaks and in providing assistance to the victims.
o The job description of an HSA is very extensive and has continued to change over the
years as new interventions are introduced into the health sector. Currently, HSA tasks at community level include child (and mother) vaccination, growth monitoring, sanitation, water source protection and water treatment, disease surveillance, village and business inspection, health and nutrition talks and supervising traditional birth attendants and VHWCs. Other tasks include providing family planning (condoms, pills and depo provera), implementing the BMHI and the DRf, following up TB patients and other health related tasks as advised by the government or NGOs. While it is true that HSAs are overloaded in terms of work, this overloading may not have necessarily contributed to the declining immunisation coverage in most parts of the country. Other factors may also have played a significant role.
o While the HSA network is very extensive and considerably old, the findings from this
survey indicate evidence of undercoverage. Some sections in some catchment areas are not reached by HSAs mainly due to accessibility and mobility problems. While it is true that some pockets of households in some catchment areas are not reached by HSAs, not all HSAs are implementing all the tasks as contained in their terms of reference. Six of the 325 sampled mothers/caretakers had never previously heard of nor seen an HSA. In terms of tasks being carried out in the catchment areas, none of the tasks contained in the HSA TORs was identified by all the sampled mothers/catetakers, even after probing.
o The survey also identified a number of constraints that are affecting the performance of
HSAs in the delivery of health services. Common constraints that were cited included mobility (transport) problems (69%), poor remuneration, no promotion and low status given to HSAs in the civil service (84%), irregular supply of vaccines and drugs (65%) and lack of protective clothing and stationery (65%). Apart from these constraints, most HSAs are untrained (19%), supervision is inadequate and irregular mainly because of mobility problems, limited and irregular refresher courses and poor telecommunication systems. Overall support to preventive health services has been declining over the years and this has trickled down to the district and health centre levels where preventive services are given little attention. In fact, some resources, notably vehicles, are diverted away to other sections.
o Data on immunisation coverage for the 418 children sampled revealed that over 80% of
the children had received the vaccines they were eligible to. General coverage was

61
therefore not very bad but timing of reception was the problem as most of the sampled children received various vaccines very late. The lateness in receiving various vaccines was not necessarily due to the heavy workload of the HSAs, but a set of both administrative and logistical hurdles, mainly at a higher level above that of an HSA. These hurdles include: lack of transport to carry vaccines, unavailability of some vaccines, non-functioning refrigerators, lack of paraffin at some health centers, geographical inaccessibility of some areas especially during rainy season, high dropouts because of side effects of some vaccines and inactive VHCs. Other factors include incorrect scheduling of immunization sessions (morning hours only when mothers are busy with other activities), laziness of mothers and cultural beliefs.
9.2 Overall Recommendations
The overall recommendation being made by this report calls for increased support towards preventive health services and reorientation of priorities in budgetary allocation towards training and technical support in the Ministry of Health and Population so that infection and exposure rates are reduced. Specific recommendations are that:
o More HSAs must be recruited, trained and deployed to rural areas to reduce the workload among those currently in service;
o HSAs must be served with clear ToRs at the time of their recruitment and whenever new tasks are being introduced to the old ToRs. They should be thoroughly oriented in the various tasks that are contained in the ToRs through regular training and induction courses;
o There are some tasks in which the sampled HSAs said they lacked skills and knowledge. These areas (vaccinations, disease surveillance, HIV/AIDS and family planning talks, tallying and report writing) need to be properly addressed during HSA training and refresher courses;
o The level of supervision to the HSAs should be increased. This could motivate the HSAs as well assessing the HSAs levels of commitment to their work for onward recommendations to other benefits such further training and promotion;
o Measures must be taken against those HSAs not performing as expected and those who abuse their clients either verbally or immorally;
o (Despite being overloaded with tasks) HSAs could also be utilised to provide meat inspection services at community level if trained and oriented to do so. A lot of livestock are slaughtered every day, which are sold and consumed without any certification;
o Transport and mobility problems be reduced by provision of push bikes to HSAs and motor cycles to their supervisors on an ownership scheme. This would ensure that each HSA takes care of his/her bicycle or motor cycle as personal property. An annual maintenance allowance for the push bikes and motor cycles should also be provided to the HSAs;
o The position of HSAs be reviewed in terms of rank, salary scale and other allowances (for example housing, risk and duty allowances) and that opportunities for upward mobility be provided through further training and promotions. It is thus further recommended that some places should be reserved for serving HSAs during intake for the Degree/Diploma in Environmental Health Sciences at the University of Malawi, so that HSAs are given an opportunity.
To achieve these objectives, there is need for collaboration among various stakeholders (government, multilateral agencies, NGOs and the private sector) in terms of HSA training, development and provision of refresher courses and transport. This could be achieved through an

62
independent and autonomous National Health Surveillance Programme (NHSP) with responsibility for HSA recruitment, training, deployment, supervision and monitoring. The NHSP could also provide advisory services to the various stakeholders that require the services of HSAs. Moreover, the HSA further training programme proposed above could be channeled through this proposed NHSP. As a way forward, the MoHP should develop a “Strategy Paper” that will outline plans for the future development HSAs in the country.
9.3 Specific recommendations to improve immunisation coverage rates
o In view of the fact that most mothers do not take their babies for vaccination or drop-out
early because of side effects of some vaccines, it is recommended that new and better methods of administering the various vaccines should be researched, particularly DPT;
o Vaccines should be made available in all Health Centres at all times. Damaged and non-functioning refrigerators and vehicles should be repaired. The national EPI and the NHSP proposed above should, also assist HCs with fuel for vehicles and motor cycles. This would enable vaccines to be brought to mobile clinics on time thus maintaining the cold chain;
o The national EPI programme, which is mandated to promote immunisation activities in Malawi should also intensify civic education especially in rural areas on the importance of immunisation;
o Medical staff should accompany HSAs during vaccination to allow for the treatment of minor illnesses. This could be attracting some mothers/caretakers whose children are sick including those whose children who have not finished receiving their vaccinations.

63
10. References
Bennet F.J. & Cole-King S. 1982: Guidelines for the Development of Primary Health Care. Report
1/82. PHC, EARO, UNICEF, MoH (LL) Chilowa W.R. & Munthali A.C. 1999: Immunisation in Malawi. Heit Spinhuis (Netherlands). Chilowa W.R. & Munthali A.C. 1998: Immunisation Services in Malawi: A Situational Analysis.
University of Malawi (Centre for Social Research) Chilowa, W.R. et al 1996: Malawi Social Indicators Survey 1995. Centre Social Research, Zomba,
Malawi Chitimbe E.G. 1998: Determination of Knowledge, Attitudes and Practices of the Primary Health
Care Approach by HSAs in Balaka and Blantyre Districts. BSc in Environmental Health Dissertation. University of Malawi (Polytechnic)
Donabedian, A. 1988: The Quality of care: How can it be assessed? JAMA 260 (12): 1743-1748.
Green, P. & Streefland Heggenhougen, H.K. 1995: Social demand and sustainability of vaccination programmes: a
comparative perspective. Paper for the research planning conference, Social science and immunisation project, Rajendrapur, Bangladesh
Makumba B. & Tauzie B.T. 2000: Hygiene Knowledge, Attitudes and Practices (KAP) for Water
and Sanitation Sector. Ministry of Health (Lilongwe) Mechanic, D. 1974: Politics, Medicine and Social Science. John Wilkey and Sons. New York Ministry of Health and Population – EPI Unit 1994: Expanded Programme on Immunisation Msukwa L.A.H. 1987: PHC in Malawi: A Search for Relevance. University of Malawi Namilaza D.M. 1998: An Assessment of the Health Surveillance Assistants Work Performance
after Training in Ntchisi, Mponela (Dowa) and Kasungu Districts. BSc in Environmental Health, University of Malawi (Polytechnic)
National Statistics Office 1994: Demographic and Health Survey 1992. Macro International Inc.,
Calverton, USA ___________________ 1997: Malawi knowledge, attitudes and practices in health survey 1996.
Zomba, Malawi Nichter, M. 1995: Vaccination in the third world: A consideration of community demand. Social
science and medicine 41(5): 617-633 Russell S.S. & Reynolds J. 1984: Operations Research Methods: Community Financing Streefland, P.H. 1995: Enhancing coverage and sustainability of vaccination programmes: An
explanatory framework with special reference to India. Social science and medicine 41 (5): 647-657

64
Appendix 1: Organogram of the District Environmental Health Office
DEHO
4 DDEHO's
Several AEHO's CTO/PO at Area level
Several SAEHO's STO
Several Health Assistants (TA/STA)
5 HSA's (SCII) for each HA
Point of contact
COMMUNITY

65
Appendix 2: Job description of a Health Surveillance Assistant (SCII) as documented in GoM (1997): Human Resource Development, MoH (Environmental Health Section), pages 21-22
HEALTH SUVILLANCE ASSISTANT (SCII)
Duties –
1. The HSA as a health worker serves as a linkage between fixed district health services and the
community;
2. The HSA works directly with village/ community leaders in identifying and providing services
by the community/- works with community health workers and volunteers from other
ministries in providing environmental and personal services; collaborates with Enrolled
community Health Nurse, Medical Assistant and reports to Environmental Health Assistant;
3. In community settings according to an assigned catchment area [2000-2,500 population];
4. Conducts community assessment within his assigned catchment area;
5. Works with the community in solving community;
6. Conducts village inspections;
7. Observes for and reports disease outbreaks;
8. Works with others in providing immunisation;
9. Maintains equipment utilised on the job;
10. Facilitates formation and training of Village Health Committees [VHCs] and volunteers;
11. Improves the quality of water by protecting shallow wells & chlorinating untreated water;
12. Treats minor illnesses;
13. Conducts growth monitoring;
14. Supervises VHCs and volunteers;
15. Refers patients and suspects to nearest health unit;
16. Writes monthly workplans; and,
17. Carries out any other duties as may be assigned to him/her by his/her immediate
supervisor

66
Appendix 3: Summary statistical descriptives of some selected variables
n Minimum Maximum Mean
Age of HSAs 121 20 58 29.6
Length of service as HSA 121 0.3 21 5.5
Length of service in current catchment area 121 o.1 15 2.9
Distance to Health Centre for reporting 121 0.1 30 4.9
Number of villages covered 121 1 27 7
Distance to furthest village in catchment area 121 1 17 5.8
Estimated time to walk to furthest village (minutes) 121 15 300 103
Estimated time to cycle to furthest village 121 7 150 46
Estimated population being served 121 518 9500 2364
Estimated population under 5 years of age 121 20 2500 490
Number of water and health committees formed 121 0 25 4
Total number of VHCs working with 121 1 25 6
Number of visits made to each VHC in a month 121 1 8 2
Number of visits made per village per month 121 1 15 3
Days for immunization functions in a month 87 1 22 2.3
Time spent on immunization (% of total time) 87 1 33 12.8
Days for growth monitoring in a month 95 1 22 2.9
Time spent on growth monitoring (%) 95 1 30 10.8
Days spent on disease investigation in a month 93 1 15 3.5
Time spent on disease investigation (% of total time) 93 2 50 12.0
Days for village health talks in a month 118 1 20 5.8
Time spent on village health talks (% of total time) 118 1 34 18.3
Time spent working at Health Centre (% of total time) 109 1 50 16.4
Days for nutrition talks/demonstration in a month 92 1 12 2.7
Time spent on nutritional talks/demo (% of total time) 92 1 15 6.2
Days implementing DRF in a month 8 1 4 2.4
Days doing sanitation work in a month 118 1 18 4.9
Time spent on sanitation (% of total time) 118 2 80 15.6
Days supplying FP methods in a month 69 1 30 6.4
Time spent on FP (% of total time) 69 1 29 7.5
Time spent on water treatment (% of total time) 102 0.5 31 8.0

67
Appendix 4: List of Health Centres that were visited, number of HSAs, Key Informants and Mothers interviewed (October-November 2001)
Health Centre Number of HSAs Number of Mothers KII Salima Kaphatenga 8 49 1 Salima hospital 13 60 2 Mchoka 4 31 1 Khombedza 5 42 Thavite 4 36 1 Lifuwu 2 14 Kaundu 2 19 Golomoti 6 32 Chipoka 5 41 Chitala 2 Maganga 3 Makioni 3 Chinguluwe 3 Chagunda 1 Salima District Totals 61 325 5 Nkhotakota Nkhotakota 5 1 Benga 3 Mwansambo 5 1 Msenjere 5 1 Alinafe Rehabilitation (CHAM) 2 Nkhotakota District Totals 20 3 Ntchisi Ntchisi hospital 5 1 Kamsonga 4 1 Malomo 5 Khuwi 2 1 Mndinda 1 Chinthembwe 3 Ntchisi District Totals 20 3 Dowa Dowa Hospital 5 1 Chakhaza 5 1 Thonje 5 Mponela 1 Chinkhwiri 4 Dowa District Totals 20 2 Overall Totals 121 325 13

68
Appendix 5: HSA Questionnaire
Questionnaire code: __________ Initials of Research Assistant: ________ Date: ____________2001 Name of the HSA: ____________
BACKGROUND VARIABLES
1. Age of the HSA _________ 2. Sex (M=1, F=2) _________ 3. Religion of the HSA _________
1. Christianity 2. Islamic 3. Watch Tower/Zion/Apostolic faith 4. Traditional 5. Other, specify ____________________
4. Marital status _________
1. Married 2. Single (never married) 3. Widowed 4. Divorced/Separated
5. Highest academic qualification (indicate class e.g. std. 6) _________ 6. When did you receive HSA training (year)? _________ 7. Length of service as HSA (years) _________ 8. Length of service in this catchment area (years) _________ 9. Health Centre/Hospital to which HSA reports _________ 10. Distance to the Health Centre/Clinic/Hospital _________Km 11. District _________

69
B. FUNCTIONAL ROLES OF THE HSA 1. How many villages do you cover? _________ 2. What is the distance to the furthest village in your catchment area? _________Km 3. What is the usual mode of transport that you use in your work? _________
1. Bicycle 2. Walking 3. Public vehicles e.g. Matola, minibuses 4. Other, specify _______________________________
4. Please estimate time taken (on average) to cycle to the furthest village from your house _________ Hours and __________ Minutes
5. Please estimate time taken (on average) to walk to the furthest village from your house ________ Hours and _________ Minutes
6. Estimated population served __________ 7. Population under the age of 5 years __________ 8. How many visits do you make per village in a month? ___________ 9. How many health committees have you formed since you started working in this area?
____________ 10. How many health committees do you work with (Total)? ____________ 11. How many visits do you make to each committee (on average) in a month? ___________ 12. At the time of starting as an HSA, were you served with terms of reference? 1. Yes 2. No 13. What specific functions were contained in the terms of reference? PROBE FOR ALL!
Role/Function 1=Yes 2=No
1=Probed for 2= Not probed
Immunization Village inspection and disease investigation Growth monitoring Community based treatment of minor illnesses Formation of and assisting village health groups Nutritional supplementation Nutrition and health talks at the clinic/Health centre Prescribing drugs at the HC Water treatment Sanitation (e.g. latrine and san plats construction) Family planning Running the drug revolving fund (DRF) Vector control (e.g. mosquitoes and snails) Other, specify ____________________

70
14. Mention the roles/functions that you are actively implementing in your catchment area and roughly estimate the amount of time spent on each (out of 100%) Function/Role 1 = Yes
2 = No How many days in a month do you do these functions?
Time allocation per month (%)
Immunization Growth monitoring Disease investigation Village health talks/inspection Working at HC Nutrition talks/demonstration Drug revolving fund Vector control Sanitation HIV/AIDS talks Family planning Water treatment Other, specify _____________ 14. Which of the roles above do you enjoy most when performing) ___________ 15. Among the listed activities, where do you more skills? ___________ 16. Which of the roles above do you find difficulties with in terms of skills? ____________ 17. How many (or how much) of the following activities/functions have you performed in the last month of September? Function/Role Number or
frequency Immunization (number of children immunized) Growth monitoring sessions Disease investigation (Number of days used) Village health talks/inspection (Number of days used) Number of patients issued with drugs in the village Number of patients served at the HC/clinic where you report Nutrition talks/demonstration (number of sessions) HIV/AIDS talks (number of sessions) Water treatment (number of beneficiary households)
Condoms (number of clients) Pills (Number of clients)
Family planning methods
Other, specify
18. What other areas of health service would you also work on without necessarily straining on your work schedules? __________________________________ __________________________________ __________________________________

71
19. For what functions are you mostly consulted/approached by the local community? -Probe for all
Function 1=Yes 2=No
Primary treatment of illnesses e.g. Malaria, diarrhoea Water chlorination/treatment Disease outbreaks To certify death or provide gloves for cleaning dead body Transport for patients Transport for funerals Family planning Other, specify
20. What proportion of the catchment population consults you for PHC assistance? _______ % 21. Why do you think the other proportion does not consult you? (multiple responses possible)
___________________________________________________________________ ___________________________________________________________________
22. Are you a member of any local committee? (1=Yes, 2=No) ___________ 23. If yes in 23 above, name the committee(s) – multiple responses possible
______________________________________________________________________ 24. Do you run a mobile clinic in your catchment area? 1=Yes 2=No ____________ 25. If yes, what proportion of underfive children do you think are brought for growth monitoring? 26. For what main reason do you think are some mothers in your catchment area not bringing their children?
1. Distance 2. Absence of supplementary food handouts 3. Cultural reasons 5. Fearing effects of immunizations 6. Laziness
27. Is there any project or programme that you are also working with? (1=Yes, 2= N) _______ 28. If yes, mention the programme(s)
_________________________________________________________________ _________________________________________________________________
29. Mention the funding agency 1. Government 2. Donor/NGO 3. Community 4. Other, specify ______________________________
30. Indicate your time allocation: Time allocation (%) Government HSA work ____________ Other projects ____________ 31. How do you benefit from this project?
Type of benefit 1=yes 2=No Number how much/month?
Salary
Training
Allowances
Other, specify
32. What other activities do you do at the health centre or hospital where you report to?

72
(1=Yes, 2=No) Cleaning/washing Health talks Prescribing drugs Running the dispensary/injection/dressing room Immunization Growth monitoring Sterilization of needles Messenger/mail collection Other, specify
33. How do you respond during emergencies like floods and disease outbreaks?
_______________________________________________________________ _______________________________________________________________ 34. What significant community based project(s) have you initiated in your catchment area?
_______________________________________________________________ _______________________________________________________________ 35. What roles do you play in its/their activities?
______________________________________________________________

73
C. WORKING CONDITIONS AND LOGISTICAL/SUPERVISORY SUPPORT 1. What is the condition of your house and housing environment
Item 1=Yes 2=No Wall is made of burnt bricks Is roofed with iron sheets Is grass thatched Floor is cemented Has three or more bedrooms Distance to nearest safe water source (in metres) Has usable latrine Has electricity Distance to bus station (m or km) Distance to telephone facilities (m or KM) Distance to market (m or km) Distance to nearest shopping centre e.g. the Boma
2. How much is your government salary per month? MK _____________ 3. Apart from the government salary, what other benefits do you have attached to your HSA work? Type of benefit 1=yes
2=No If it is a cash allowance, how much per month?
Transport
Field allowance – for working in the field
House
Training
***********************
4. Do you have a parcel of land for farming? 1=Yes 2=No 5. If yes in question 4 above, please indicate acreage _______ Acres 6. Have you attended any refresher course since 1995? 1=Yes 2=No ___________ 7. If yes, how many? ___________ 8. If yes, who funded your attendance? __________
Source of Funding Number of courses in last 3 years
Ministry of health NGO working in the area Other government project

74
9. What is your regular source of information about new developments in the health sector? Choose one only!
Source of information Tick for one only
Refresher courses Supervisors Workmates TV Radio Newsletters Newspapers Other, specify
10. Technically, what is the major constraint that prevents the performance of your functions? Choose one only!
Constraint Tick once only Irregular supply of vaccines No storage and carriage facility for vaccines Irregular/no supply of drugs Irregular supply of water treatment chemicals No supervision Mobility problems (e.g. no transport) No emergency kit to deal with outbreaks or emergencies Inadequate stationery
11. How often do you replenish your drug stocks?
1. As need arises 2. Weekly 3. Bi-weekly 4. Monthly 5. Every 2 months 6. Other, specify ___________________
12. How long does it usually take for drugs to be delivered to you after requesting? _________ days or ____________ weeks
13. Make your comment on the quantity of drugs that are usually supplied to you ________ 1. Usually supplied in requested quantities 2. Usually supplied in quantities less than requested 3. Usually supplied in quantities more than requested

75
14. What drugs and materials do you have at this time in stock? Drugs/medicines or materials 1=Yes
2=No How many adult doses?
Anti-malarial drugs (doses)
Antibiotics (Number of tablets) Weighing scales (number) Pain killers (how many tablets?) ORS sachets (how many?) Condoms (number) Others, specify
15. Who is your immediate supervisor? __________________ 16. What is usually done during supervisory sessions? (circle all relevant responses)
1. Man to man discussions 2. Progress reports are submitted 3. Supervisor talks to some local people and local leaders 4. Other, specify _______________________________________
17. How often do you submit progress reports to your supervisor? ___________ 18. Please rate your relations with the following categories of staff and people:
Category of staff/people 1=good, 2=Fair, 3=bad 4=never interacted before
Clinicians Nurses/midwives Health Assistants Laboratory Technicians MoHP District/headquarters staff Local community Extension workers from other Departments/NGOs
19. What social demotivating factors do you face in your work?
Factor 1=Yes 2=No
1=probed for 2=mentioned
Low remuneration Poor relations with the community Poor relations with supervisors No promotion No refresher courses Working out of town in remote areas Poor telecommunication system Poor road networks My gender My age My marital status My religion Cultural values of the community – specify
20. What suggestions do you have for the improvement of HSA work in Malawi ________________________________________________________________ ________________________________________________________________ 21. Why do you think are immunization coverage rates going down in the country?
________________________________________________

76
________________________________________________

77
Appendix 6: Questionnaire for Mothers/ Care takers of Underfive Children
Date of Interview: ________________ 2001 Interviewer: ________________________
Checked by Supervisor: ___________________ Village: ______________ 1. Name of Mother/care taker: _______________ Highest class attained ____________ 2. Age: __________ 3. List of household members Name Sex
1=Male 2=Female Age
4. Number of children under the age of five ___________ 5. Relationship to Child 1: __________ Child 2: __________ Child 3: ____________ 1= Mother 2=Grandparent 3=Aunt 4=Sister
5=Other relative 6= Non-relative 6. Sex of household head: ______________ (1=Male 2=Female) 7. Religious affiliation of the household head ________
1= Christianity 2= Islam 3=Watch Tower 4= Apostolic faith/believer /Zion 5= Traditional 6= Other (specify) _______________
8. Religious affiliation of mother/care taker (Codes above) _________
KNOWLEDGE ABOUT HSAS
9. Have you ever heard of an HSA? (1=yes, 2=No) ________ 10. Is there an HSA who works in your village? (1=yes, 2=No) _________ 11. Are you related to the HSA? (1=Yes 2=No) _________

78
12. If an HSA works in your area, what activities is s/he doing? Note to Researcher – Please probe for all and indicate whether probed for or mentioned by respondent alone Function of HSAs 1=Yes
2=No 1=mentioned by respondent 2= Probed for
Immunization Growth monitoring Disease investigation Health talks HIV/AIDS talks Water treatment Sanitation activities e.g. latrines Vector control e.g. snails, mosquitoes Running the drug revolving fund Family planning Nutritional clinics Working with health committees Other, specify
13. For all activities that the HSA is doing, please rate his/her performance (1=Poor, 2=Fair, 3=Good) on them and
general behaviour Function of HSA Rate Reason Immunization Growth monitoring Disease investigation Health talks HIV/AIDS talks Nutritional clinics Water treatment Sanitation activities Family planning Working with health committees General behaviour 14. When you go to a health centre/clinic that is close to you, which staff do you meet?
Rate them in terms of Staff 1= YES 2= NO
Assistance Attitude
Nurse Clinician/Health Assistant HSA
Ratings: 1=Good 2=Fair 3=Bad 15. Have you ever gone to an HSA for assistance? (1=Yes 2=No) ________ 16. For what do you usually approach an HSA? Type of assistance/meeting 1= YES 2= NO Illnesses (free drugs) To purchase drugs Water treatment Health advice/counseling Other (Specify) ________________
17. How many times have you approached an HSA in the last 12 months? ____________ 18. What do you think are the major constraints facing the HSA in his/her work? Constraint 1= YES 2= NO Irregular supply of vaccines Irregular supply of water treatment chemicals No supply of supply (none at all) Irregular supply of drugs No supervision Personal negligence

79
Theft/selling of drugs (by HSA) Poor remuneration Other (Specify) ______________
19. Was any member of your household sick in the last 12 months? 1=Yes 2=No _______

80
20. When that member of your household fell ill, what first action did you take? 1. Went to shops/vendors to purchase drugs 2. Rush to a Health centre 3. Went to Hospital 4. Approached HSA 5. Visited a Traditional healer 6. Visited a Local injector 7. Other _(Specify)__________________
21. Why is the main reason why to took the action above? Reason 1= YES 2= NO or write N/A for Not Applicable Health facility is very far Health centre always has no drugs NO HSAs in the village/or nearby Cheap drugs Drugs are always available Nearest service Other (Specify) ______________
22. What suggestions do you have for improvement on the work of HSAs?

81
Child Information (Underfives) Child 1 (oldest) Name of child _____________ 15. Date of Birth ____________ 16. Place of Birth ____________
1=Hospital/HC 2=Home 3=TBA 4= Other ______
If you are not the mother of the child, does the mother live here? 1=Yes 2= No Please record the following information regarding the child’s immunization schedules (from the Card) Immunization Schedule
Number Date of receipt
Weeks from birth/last vaccine. Months from birth for measles
Place of receipt -codes-
Why not on time -codes-
Why not received -codes-
BCG 1 2
DPT
3 0 1 2
Polio
3 Measles Codes for no immunization or late reception Place of receiving Immunization
1. Long distance to immunization centres 1. Health centre 2. Fearing that their child will become sick 2. Mobile clinic 3. Laziness of mother/caretaker 3. Other, specify _____________ 4. Interrupted by (ashamed of) another pregnancy 5. Mother/Caretaker always busy 6. There were no vaccines at the health centre/hospital 7. HSA had no vaccines 8. Religious domains/beliefs 9. Child was born at a TBA 10. Other (Specify)______________________________
If reason for not receiving BCG on time was (9) above, did the TBA advise you to take the child to a clinic/hospital for the vaccine? 1=Yes 2=No ___________

82
Child 2 Name of child _____________ 15. Date of Birth ____________ 16. Place of Birth ____________
1=Hospital/HC 2=Home 3=TBA 4= Other ______
If you are not the mother of the child, does the mother live here? 1=Yes 2= No Please record the following information regarding the child’s immunization schedules (from the Card) Immunization Schedule
Number Date of receipt
Weeks from birth/last vaccine. Months from birth for measles
Place of receipt -codes-
Why not on time -codes-
Why not received -codes-
BCG 1 2
DPT
3 0 1 2
Polio
3 Measles Codes for no immunization or late reception Place of receiving Immunization
1. Long distance to immunization centres 1. Health centre 2. Fearing that their child will become sick 2. Mobile clinic 3. Laziness of mother/caretaker 3. Other, specify _____________ 4. Interrupted by (ashamed of) another pregnancy 5. Mother/Caretaker always busy 6. There were no vaccines at the health centre/hospital 7. HSA had no vaccines 8. Religious domains/beliefs 9. Child was born at a TBA 10. Other (Specify)______________________________
If reason for not receiving BCG on time was (9) above, did the TBA advise you to take the child to a clinic/hospital for the vaccine? 1=Yes 2=No ___________

83
Child 3 Youngest Name of child _____________ 15. Date of Birth ____________ 16. Place of Birth ____________
1=Hospital/HC 2=Home 3=TBA 4= Other ______
If you are not the mother of the child, does the mother live here? 1=Yes 2= No Please record the following information regarding the child’s immunization schedules (from the Card) Immunization Schedule
Number Date of receipt
Weeks from birth/last vaccine. Months from birth for measles
Place of receipt -codes-
Why not on time -codes-
Why not received -codes-
BCG 1 2
DPT
3 0 1 2
Polio
3 Measles Codes for no immunization or late reception Place of receiving Immunization
1. Long distance to immunization centres 1. Health centre 2. Fearing that their child will become sick 2. Mobile clinic 3. Laziness of mother/caretaker 3. Other, specify _____________ 4. Interrupted by (ashamed of) another pregnancy 5. Mother/Caretaker always busy 6. There were no vaccines at the health centre/hospital 7. HSA had no vaccines 8. Religious domains/beliefs 9. Child was born at a TBA 10. Other (Specify)______________________________
If reason for not receiving BCG on time was (9) above, did the TBA advise you to take the child to a clinic/hospital for the vaccine? 1=Yes 2=No ___________

84
CENTRE FOR SOCIAL RESEARCH HSA STUDY INTERVIEW GUIDE FOR HSA SUPERVISORS 1. Identification details
Name of interviewee For how long have you been a supervisor? An HSA? Number of HSAs supervised? How many have attended induction courses? How many have received refresher
courses? How many refresher courses have you received in the last 3-5 years? Total population served? How many children under the age of five? Distance to furthest village in your catchment area? Nearest distance? Your usual mode of transport Salary? How much housing allowance? Risk allowance? Other allowances?
2. What functions are HSAs under your supervision implementing in the catchment area? How many days in a month
does each allocate to immunizations and growth monitoring? 3. What technical constraints are HSAs facing? 4. What socio-cultural problems are they facing? 5. In what areas do you observe weaknesses among your HSAs? How about strengths? 6. How do you provide your supervision? (individually? During growth monitoring only? Are any reports submitted? Do
they retain copies of the reports? etc.) 7. What factors do you think would be contributing to the general decline in the coverage of immunizations in Malawi?
(problems with HSAs? Their workload? Mothers/caretakers? Supply of vaccines? Logistics? etc.) 8. Are there any NGOs that are working in your catchment area? How do they involve HSAs? What contributions do
HSAs make to their activities? How is the HAS work related to the objectives of the NGOs? How are HSAs remunerated?
9. What suggestions would you make to improve the work of HSAs? To improve immunization coverage rates? Delivery of general health services?